
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Oncol., 09 January 2024
Sec. Head and Neck Cancer
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1240913
This article is part of the Research TopicAdvances in Radiotherapy for Head and Neck CancerView all 15 articles
 Bianca Santo1
Bianca Santo1 Niccolò Bertini2*
Niccolò Bertini2* Carlo Guglielmo Cattaneo3
Carlo Guglielmo Cattaneo3 Sara De Matteis1
Sara De Matteis1 Paola De Franco1
Paola De Franco1 Roberta Grassi4
Roberta Grassi4 Giuseppe Carlo Iorio5
Giuseppe Carlo Iorio5 Silvia Longo6
Silvia Longo6 Luca Boldrini6
Luca Boldrini6 Antonio Piras7,8,9
Antonio Piras7,8,9 Isacco Desideri2Francesca De Felice3
Isacco Desideri2Francesca De Felice3 Viola Salvestrini10
Viola Salvestrini10Weight loss is a frequent occurrence among patients with head and neck cancer (HNC) and can be observed before, during, and after cancer treatment, especially radiation therapy (RT) with or without concurrent chemotherapy (CRT). Patients with HNC are at a high risk of malnutrition at the time of diagnosis, and nutritional support or intervention is often needed during and after RT or concurrent CRT. Given the severe consequences of malnutrition and cachexia on treatment outcomes, mortality, morbidity, and quality of life, it is essential to identify patients who are at higher risk of developing this condition. The nutritional status of patients is a crucial factor in terms of adherence to treatment and recovery. Malnutrition may have a significant impact on treatment outcomes and, consequently, tumor progression. However, in clinical practice, identifying and standardizing nutritional interventions can be challenging. In this commentary, we aim to identify the components of screening and assessment that are commonly used in both literature and clinical practice and suggest the appropriate timing for nutritional interventions in patients with HNC undergoing RT or CRT.
At the time of diagnosis, 35%–60% of head and neck cancer (HNC) patients are malnourished due to cancer-related impairment such as pain, obstruction, or loss of appetite (1, 2). Compared to patients with other primary neoplasms, HNC patients are at a higher risk of malnutrition due to the location of the tumor and the impact of the treatment-related side effects on quality of life (3, 4). Indeed, malnutrition can cause a range of clinical symptoms, including metabolic and electrolytic imbalances, immune system depression, and increased morbidity and mortality (5). Weight loss can lead to discontinue cancer treatments and to a negative impact on oncological outcomes, with approximately 55% of patients losing an additional 10% or more of their body weight during RT or CRT (5–7). This note aims to provide an overview on the role of nutritional counseling in HNC patients undergoing CRT, either in an exclusive or adjuvant setting.
Malnutrition screening is an essential component of multimodal care in HNC patients. It involves the systematic identification of patients who are at risk of malnutrition and the provision of appropriate interventions to prevent or treat malnutrition (8). In this regard, the European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines for screening suggests that the purpose of nutritional screening is to predict the outcome and the impact of nutritional intervention (9).There are no standardized guidelines regarding nutritional screening. Screening should occur at the time of diagnosis, before treatment begins, and at regular intervals throughout treatment and follow-up. This allows for early identification of malnutrition and timely intervention to prevent or treat it. Despite its acknowledged role, there are no standardized guidelines regarding nutritional screening.
The risk of malnutrition is frequent in HNC patients, and for this reason, it is mandatory to primarily identify patients at higher risk. Currently, standardized parameters are adopted, and although there is not a single assessment tool, we suggest that the use of a standardized assessment is essential to identify patients at risk at baseline. The commonly used nutrition assessment tools are the following:
1. Mini Nutrition Assessment (MNA) includes anthropometric, general, dietary, and autonomy of food self-assessments (self-perception of health and nutrition) (10–12).
2. Nutritional Risk Screening 2002 (NRS2002) detects the presence or the risk of undernutrition (9, 13).
3. Patient-Generated Subjective Globe Assessment (PG-SGA) is focused on the preeminent interdisciplinary patient assessment and allows for triaging of nutrition interventions (14).
4. Malnutrition Universal Screening Tool (MUST) is a five-step screening tool to identify malnourished adults (15, 16).
The appropriate nutritional assessment should be performed for all patients before CRT. For defining the severity of malnutrition, we recommend the use of the new GLIM (Global Leadership Initiative on Malnutrition) score, already adopted by ESPEN, ASPEN, FELANPE, and PENSA. In particular, the GLIM includes three phenotypical criteria (weight loss, low BMI, and reduced muscle mass) and two etiological criteria (reduced food intake or absorption and increased disease burden or inflammation) (17).
The aim of the nutritional intervention is to improve the subjective quality of life, enhance anti-tumor treatment effects, reduce the adverse effects of oncological care, prevent the interruption of therapy, and treat RT/CRT-related undernutrition. In this regard, Table 1 summarizes the main studies analyzing the impact of nutritional counseling and nutritional intervention strategies in HNC patients (18–32). The onset of oral mucositis in HNC patients during RT or CRT may result in weight loss and intensive dietary counseling, and oral nutrition support is recommended. This is also advised to prevent interruptions to CRT (33). There are different types of nutritional support that can be adopted to reach the needs of the patient. Main options of nutritional support are oral, enteral, and parenteral. Nutritional interventions include relaxation of previous therapeutic diets, to minimize further nutritional compromise and to positively influence quality of life outcomes (34). However, this may not necessarily be appropriate, due to the side effects and intensity of treatment regimens. Patients may require more intensive nutritional support methods from the beginning of treatment over and above traditional food fortification methods with the early use of oral nutrition support. The choice of feeding route in HNC patients will depend upon local arrangements; however, clinical considerations should include site of primary tumor, treatment plan and intent, predicted duration of enteral feeding, and patient choice (35, 36). Tube feeding is recommended if swallowing is impaired or if mucositis is anticipated, which may interfere with oral and/or pharyngeal functionality. If enteral feeding is expected to be required for longer than 4 weeks, then gastrostomy insertion is recommended but not in a prevention way, except for limited cases (37). The optimal method of tube feeding still remains unclear, and any approach should be discussed with the patient in order to ensure an individualized nutritional care. Moreover, the optimal screening and assessment for suitability and method of gastrostomy insertion by endoscopic, radiological, or surgical approach is essential. Assessment of co-morbidities and contraindications should be taken into account to prevent complications prior to oncological treatment (35, 36).
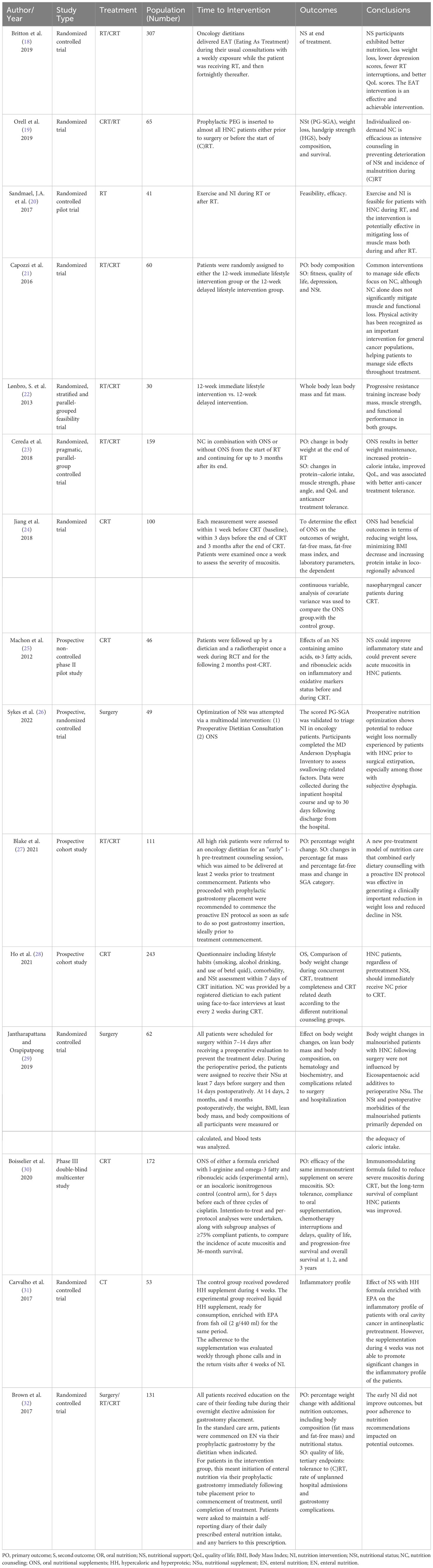
Table 1 Nutritional counseling and intervention strategies in HNC patients.
The type and volume of enteral nutrition will depend upon patients’ symptoms and current intake and is likely to change throughout and after treatment. There are no data to suggest a role for cancer-specific enteral formulae. Monitoring nutritional intervention is essential, as compliance with recommendations can be a problem and should be organized weekly during CRT. Supplementation with immunonutrient-enriched formulas such as arginine, nucleotides (RNA), and omega-3 fatty acids up to the end of (C)RT or until withdrawal in HNC patients during RT and CRT may improve or maintain nutrition status (37–39). Moreover, it can delay the onset of oral mucositis and reduce the incidence of severe oral mucositis (38–40). Much evidence is showing a possible beneficial effect of immunonutrition on the control of the onset of local recurrences of the disease after esophagectomy, an improvement in immunosurveillance mechanisms, and a reduction in inflammatory status. Finally, by modulating gene expression, the immunonutrition may make it easier for the body to adapt to systemic inflammation and oxidative stress induced by RCTs and may improve 3-year survival (25, 30, 41, 42). However, further studies focusing on the timing, dosage, and duration of immunonutrition in HNC patients are awaited.
In conclusion, HNC patients undergoing cancer treatment are at high risk of malnutrition before, during, and after oncological care. The nutritional screening, assessment, and support play a crucial role on the maintenance of nutritional status providing specific interventions such as oral nutritional supplements increasing dietary intake and preventing therapy-associated weight loss. It is well-reported in the literature that the interruption of CRT may contribute to worse oncological outcomes. In this regard, the present overview highlighted that an adequate nutritional screening, assessment, and interventions might increase the adherence of HNC patients to oncological treatments and encourages radiation oncologists to set up multidisciplinary care paths.
BS: Conceptualization, Methodology, Validation, Formal analysis, Data curation, Writing - original draft, Writing - review and editing, Supervision. NB: Methodology, Data curation, Writing – original draft, Writing – review and editing, Visualization. CC: Methodology, Data curation, Writing – original draft, Writing – review and editing, Visualization. SM: Methodology, Data curation, Writing – original draft, Writing – review and editing, Visualization. PF: Conceptualization, Validation, Formal analysis, Writing – review and editing, Visualization, Supervision. RG: Conceptualization, Validation, Formal analysis, Writing – review and editing, Visualization, Supervision. GCI: Conceptualization, Validation, Formal analysis, Writing – review and editing, Visualization, Supervision. SL: Data curation, Writing – original draft, Writing – review and editing. LB: Conceptualization, Validation, Formal analysis, Writing – review and editing, Visualization, Supervision. AP: Conceptualization, Validation, Formal analysis, Writing – review and editing, Visualization, Supervision. ID: Conceptualization, Validation, Formal analysis, Writing – review and editing, Visualization, Supervision. FF: Conceptualization, Validation, Formal analysis, Writing – review and editing, Visualization, Supervision. VS: Conceptualization, Methodology, Data curation, Writing – original draft, Writing – review and editing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer ND is currently organizing a Research Topic with the authors GCI, ID.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Isenring EA, Capra S, Bauer JD. Nutrition intervention is beneficial in oncology outpatients receiving radiotherapy to the gastrointestinal or head and neck area. Br J Cancer (2004) 91:447–52. doi: 10.1038/sj.bjc.6601962
2. Beer KT, Krause KB, Zuercher T, Stanga Z. Early percutaneous endoscopic gastrostomy insertion maintains nutritional state in patients with aerodigestive tract cancer. Nutr Cancer (2005) 52:29–34. doi: 10.1207/s15327914nc5201_4
3. Kruizenga HM, Wierdsma NJ, Van Bokhorst MAE, De van der Schueren MAE, Hollander HJ, Jonkers-Schuitema CF, et al. Screening of nutritional status in the Netherlands. Clin Nutr (2003) 22:147–52. doi: 10.1054/clnu.2002.0611
4. Datema FR, Ferrier MB, Baatenburg De Jong RJ. Impact of severe malnutrition on short-term mortality and overall survival in head and neck cancer. Oral Oncol (2011) 47:910–4. doi: 10.1016/j.oraloncology.2011.06.510
5. Ehrsson YT, Hellström PM, Brismar K, Sharp L, Langius-Eklöf A, Laurell G. Explorative study on the predictive value of systematic inflammatory and metabolic markers on weight loss in head and neck cancer patients undergoing radiotherapy. Support Care Cancer (2010) 18:1385–91. doi: 10.1007/s00520-009-0758-4
6. Silvestris N, Falzone L, Elasbali AM, Minoia C, Romito F, Dellino M, et al. Article 1270 psychological distress in outpatients with lymphoma during the COVID-19 pandemic. Front Oncol (2020) 1:1270. doi: 10.3389/fonc.2020.01270
7. Vera-Llonch M, Oster G, Hagiwara M, Sonis S. Oral mucositis in patients undergoing radiation treatment for head and neck carcinoma: Risk factors and clinical consequences. Cancer (2006) 106:329–36. doi: 10.1002/cncr.21622
8. Talwar B, Donnelly R, Skelly R, Donaldson M. Nutritional management in head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol (2016) 130:S32–40. doi: 10.1017/s0022215116000402
9. Kondrup J, Allison SP, Elia M, Vellas B, Plauth M. ESPEN guidelines for nutrition screening 2002. Clin Nutr (2003) 22:415–21. doi: 10.1016/S0261-5614(03)00098-0
10. Vellas B, Guigoz Y, Baumgartner M, Garry PJ, Lauque S, Albarede JL. Relationships between nutritional markets and the mini-nutritional assessment in 155 older persons. J Am Geriatr Soc (2000) 48:1300–9. doi: 10.1111/j.1532-5415.2000.tb02605.x
11. Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, et al. The mini nutritional assessment (mna) and its use in grading the nutritional state of elderly patients. Nutrition (1999) 15(2):116-22. doi: 10.1016/s0899-9007(98)00171-3
12. Villars H, Soto M, Morley JE. Overview of the MNA-Its history and challenges Aging Issues and Culture, Nationality, and Ethnicity View project The SITLESS project: Exercise Referral Schemes enhanced by Self-Management Strategies to battle sedentary behaviour in older adults View project (2005). Available at: https://www.researchgate.net/publication/6617786.
13. Kondrup J, Ramussen HH, Hamberg O, Stanga Z, Camilo M, Richardson R, et al. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin Nutr (2003) 22:321–36. doi: 10.1016/S0261-5614(02)00214-5
14. Correira Pereira MA, Santos CA, Almeida Brito J, Fonseca J. Evaluación global subjetiva del estado de nutrición generada por el paciente, albúmina y transferrina en pacientes con cáncer de cabeza o cuello alimentados por gastrostomía. Nutr Hosp (2014) 29:420–6. doi: 10.3305/nh.2014.29.2.7066
15. Boléo-Tomé C, Monteiro-Grillo I, Camilo M, Ravasco P. Validation of the malnutrition universal screening tool (MUST) in cancer. Br J Nutr (2012) 108:343–8. doi: 10.1017/S000711451100571X
16. Amaral TF, Antunes A, Cabral S, Alves P, Kent-Smith L. An evaluation of three nutritional screening tools in a Portuguese oncology centre. J Hum Nutr Diet (2008) 21:575–83. doi: 10.1111/j.1365-277X.2008.00917.x
17. Cederholm T, Jensen GL, Correia MITD, Gonzalez MC, Fukushima R, Higashiguchi T, et al. GLIM criteria for the diagnosis of malnutrition – A consensus report from the global clinical nutrition community. Clin Nutr (2019) 38:1–9. doi: 10.1016/j.clnu.2018.08.002
18. Britton B, Baker AL, Wolfenden L, Wratten C, Bauer J, Beck AK, et al. Eating as treatment (EAT): A stepped-wedge, randomized controlled trial of a health behavior change intervention provided by dietitians to improve nutrition in patients with head and neck cancer undergoing radiation therapy (TROG 12.03). Int J Radiat Oncol Biol Phys (2019) 103:353–62. doi: 10.1016/j.ijrobp.2018.09.027
19. Orell H, Schwab U, Saarilahti K, Österlund P, Ravasco P, Mäkitie A. Nutritional counseling for head and neck cancer patients undergoing (chemo) radiotherapy—a prospective randomized trial. Front Nutr (2019) 6:22. doi: 10.3389/fnut.2019.00022
20. Sandmæl JA, Bye A, Solheim TS, Stene GB, Thorsen L, Kaasa S, et al. Feasibility and preliminary effects of resistance training and nutritional supplements during versus after radiotherapy in patients with head and neck cancer: A pilot randomized trial. Cancer (2017) 123:4440–8. doi: 10.1002/cncr.30901
21. Capozzi LC, McNeely ML, Lau HY, Reimer RA, Giese-Davis J, Fung TS, et al. Patient-reported outcomes, body composition, and nutrition status in patients with head and neck cancer: Results from an exploratory randomized controlled exercise trial. Cancer (2016) 122:1185–200. doi: 10.1002/cncr.29863
22. Lonbro S, Dalgas U, Primdahl H, Overgaard J, Overgaard K. Feasibility and efficacy of progressive resistance training and dietary supplements in radiotherapy treated head and neck cancer patients-the DAHANCA 25A study. Acta Oncol (Madr) (2013) 52:310–8. doi: 10.3109/0284186X.2012.741325
23. Cereda E, Cappello S, Colombo S, Klersy C, Imarisio I, Turri A, et al. Nutritional counseling with or without systematic use of oral nutritional supplements in head and neck cancer patients undergoing radiotherapy. Radiother Oncol (2018) 126:81–8. doi: 10.1016/j.radonc.2017.10.015
24. Jiang W, Ding H, Li W, Ling Y, Hu C, Shen C. Benefits of oral nutritional supplements in patients with locally advanced nasopharyngeal cancer during concurrent chemoradiotherapy: an exploratory prospective randomized trial. Nutr Cancer (2018) 70:1299–307. doi: 10.1080/01635581.2018.1557222
25. MacHon C, Thezenas S, Dupuy AM, Assenat E, Michel F, Mas E, et al. Immunonutrition before and during radiochemotherapy: Improvement of inflammatory parameters in head and neck cancer patients. Support Care Cancer (2012) 20:3129–35. doi: 10.1007/s00520-012-1444-5
26. Sykes KJ, Gibbs H, Farrokhian N, Arthur A, Flynn J, Shnayder Y, et al. Pilot randomized, controlled, preoperative intervention for nutrition trial in head and neck cancer. Head Neck (2023) 45:156–66. doi: 10.1002/hed.27220
27. Blake C, Edwards A, Treleaven E, Brown T, Hughes B, Lin C, et al. Evaluation of a novel pre-treatment model of nutrition care for patients with head and neck cancer receiving chemoradiotherapy. Nutr Diet (2022) 79:206–16. doi: 10.1111/1747-0080.12714
28. Ho YW, Yeh KY, Hsueh SW, Hung CY, Lu CH, Tsang NM, et al. Impact of early nutrition counseling in head and neck cancer patients with normal nutritional status. Support Care Cancer (2021) 29:2777–85. doi: 10.1007/s00520-020-05804-3
29. Jantharapattana K, Orapipatpong O. Efficacy of EPA-enriched supplement compared with standard formula on body weight changes in malnourished patients with head and neck cancer undergone surgery: a randomized study. Head Neck (2020) 42:188–97. doi: 10.1002/hed.25987
30. Boisselier P, Kaminsky MC, Thézenas S, Gallocher O, Lavau-Denes S, Garcia-Ramirez M, et al. A double-blind phase III trial of immunomodulating nutritional formula during adjuvant chemoradiotherapy in head and neck cancer patients: IMPATOX. Am J Clin Nutr (2020) 112:1523–31. doi: 10.1093/ajcn/nqaa227
31. Carvalho TC, Cruz BCS, Viana MS, Martucci RB, Saraiva DCA, Reis PF. Effect of nutritional supplementation enriched with eicosapentaenoic acid on inflammatory profile of patients with oral cavity cancer in antineoplastic pretreatment: A controlled and randomized clinical trial. Nutr Cancer (2017) 69:428–35. doi: 10.1080/01635581.2017.1274406
32. Brown TE, Banks MD, Hughes BGM, Lin CY, Kenny LM, Bauer JD. Randomised controlled trial of early prophylactic feeding vs standard care in patients with head and neck cancer. Br J Cancer (2017) 117:15–24. doi: 10.1038/bjc.2017.138
33. Giddings A. Treatment interruptions in radiation therapy for head-and-neck cancer: Rates and causes. J Med Imaging Radiat Sci (2010) 41:222–9. doi: 10.1016/j.jmir.2010.08.002
34. Ravasco P, Monteiro-Grillo I, Vidal PM, Camilo ME. Impact of nutrition on outcome: A prospective randomized controlled trial in patients with head and neck cancer undergoing radiotherapy. Head Neck (2005) 27:659–68. doi: 10.1002/hed.20221
35. Talwar B, Findlay M. When is the optimal time for placing a gastrostomy in patients undergoing treatment for head and neck cancer? Curr Opin Support Palliat Care (2012) 6:41–53. doi: 10.1097/SPC.0b013e32834feafd
36. Bradley PT, Brown T, Paleri V. Gastrostomy in head and neck cancer: Current literature, controversies and research. Curr Opin Otolaryngol Head Neck Surg (2015) 23:162–70. doi: 10.1097/MOO.0000000000000135
37. NICE group. Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition. London: National Institute for Health and Care Excellence (NICE); NICE Clinical Guidelines (2022).
38. Reber E, Schönenberger KA, Vasiloglou MF, Stanga Z. Nutritional risk screening in cancer patients: the first step toward better clinical outcome. Front Nutr (2021) 8:603936. doi: 10.3389/fnut.2021.603936
39. Caccialanza R, Cereda E, Orlandi E, Filippi AR, Comoli P, Alberti A, et al. Immunonutrition in head and neck cancer patients undergoing chemoradiotherapy: an alternative approach for overcoming potential bias. Am J Clin (2021) 113(4):1053–54.
40. Caccialanza R, Cereda E, Klersy C, Nardi M, Masi S, Crotti S, et al. The efficacy of immunonutrition in improving tolerance to chemoradiotherapy in patients with head and neck cancer, receiving nutritional counseling: study protocol of a randomized, open-label, parallel group, bicentric pilot study. Ther Adv Med Oncol (2021) 13. doi: 10.1177/17588359211025872
41. Scarpa M, Kotsafti A, Fassan M, Scarpa M, Cavallin F, Nardi T, et al. Immunonutrition before esophagectomy: Impact on immune surveillance mechanisms. Tumor Biol (2017) 39:1–9. doi: 10.1177/1010428317728683
42. Talvas J, Garrait G, Goncalves-Mendes N, Rouanet J, Vergnaud-Gauduchon J, Kwiatkowski F, et al. Immunonutrition stimulates immune functions and antioxidant defense capacities of leukocytes in radiochemotherapy-treated head & neck and esophageal cancer patients: A double-blind randomized clinical trial. Clin Nutr (2015) 34:810–7. doi: 10.1016/j.clnu.2014.12.002
Keywords: head and neck, nutrition, chemotherapy, radiation therapy, weight
Citation: Santo B, Bertini N, Cattaneo CG, De Matteis S, De Franco P, Grassi R, Iorio GC, Longo S, Boldrini L, Piras A, Desideri I, De Felice F and Salvestrini V (2024) Nutritional counselling for head and neck cancer patients treated with (chemo)radiation therapy: why, how, when, and what? Front. Oncol. 13:1240913. doi: 10.3389/fonc.2023.1240913
Received: 16 June 2023; Accepted: 14 December 2023;
Published: 09 January 2024.
Edited by:
Dirk Van Gestel, Université libre de Bruxelles, BelgiumReviewed by:
Nerina Denaro, IRCCS Ca ‘Granda Foundation Maggiore Policlinico Hospital, ItalyCopyright © 2024 Santo, Bertini, Cattaneo, De Matteis, De Franco, Grassi, Iorio, Longo, Boldrini, Piras, Desideri, De Felice and Salvestrini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Niccolò Bertini, bmljY29sby5iZXJ0aW5pQHVuaWZpLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.