 Lucilla Crudele1†
Lucilla Crudele1† Fabio Novielli1†Carlo De Matteis1Stefano Petruzzelli1Patrizia Suppressa1Elsa Berardi1Gianfranco Antonica1
Fabio Novielli1†Carlo De Matteis1Stefano Petruzzelli1Patrizia Suppressa1Elsa Berardi1Gianfranco Antonica1 Giuseppina Piazzolla1
Giuseppina Piazzolla1 Carlo Sabbà1
Carlo Sabbà1 Giusi Graziano2
Giusi Graziano2 Antonio Moschetta1,3*
Antonio Moschetta1,3*- 1Department of Interdisciplinary Medicine, University of Bari “Aldo Moro”, Bari, Italy
- 2Center for Outcomes Research and Clinical Epidemiology (CORESEARCH), Pescara, Italy
- 3IINBB National Institute for Biostructure and Biosystems, Roma, Italy
Introduction: Thyroid cancer incidence is increasing, and adiposity-related conditions are gaining space in its pathogenesis. In this study, we aimed to detect any anthropometric, biohumoral, and clinical features that might be associated with thyroid nodule malignancy, potentially representing novel non-invasive markers of thyroid cancer.
Materials and methods: The study was conducted in a group of 142 consecutive outpatients (47 men and 95 women) who underwent fine-needle aspiration biopsy/cytology (FNAB/C) due to suspicion of malignancy from January 2018 to September 2022. We compared lipid and glycemic blood profiles as well as non-invasive liver fibrosis indexes such as aspartate aminotransferase (AST) to alanine aminotransferase (ALT) ratio (AAR), AST to platelet ratio index (APRI), and fibrosis index based on four factors (FIB-4) between patients with benign and malignant newly diagnosed nodules. Then, we performed receiver operating characteristic (ROC) analysis to assess their best cutoff values for discrimination of malignant nodules and chi-squared test to evaluate the association of specific dysmetabolic conditions with malignancy. To understand whether and to what degree dysmetabolic conditions increased the risk of thyroid nodule malignancy, we also calculated the odds ratio (OR) of the main biomarkers.
Results: After FNAB/C, 121 (85%) patients were diagnosed with benign thyroid nodules, while 21 (15%) individuals were diagnosed with thyroid cancer. Comparing patients with benign and malignant nodules, we found that individuals with thyroid cancer exhibited increased body mass index (BMI) (p = 0.048) and fasting plasma glucose (p = 0.046). Intriguingly, considering non-invasive scores for liver fibrosis, subjects with thyroid cancer presented increased AAR (p < 0.001) and APRI (p = 0.007), and these scores were associated with malignancy (p < 0.005) with OR = 7.1 and OR = 5, respectively. Moreover, we showed that only in the cancer group, low levels of vitamin D correlated with stigmata of impaired metabolism.
Discussion: In our study, AAR and APRI scores were associated with thyroid nodule malignancy and could be used to predict it and to speed up the diagnostic process. From a pathogenic point of view, we speculated that metabolic-associated fatty liver disease (MAFLD) along with hyperglycemia and vitamin D deficiency may represent putative drivers of thyroid carcinogenesis.
1 Introduction
The prevalence of palpable nodules is 5% in women and 1% in men living in iodine-sufficient parts of the world (1, 2), and an increase in thyroid cancer incidence, the most common endocrine neoplasm, has been observed in the last decades (3). In addition to familiarity and exposure to ionizing radiation, lifestyle changes and dietary habits play a significant role in the development of thyroid malignancy (4), and it has been even suggested that a healthier lifestyle may attenuate the deleterious influence of genetics on the risk of thyroid cancer (5). Indeed, obesity, diabetes, and metabolic syndrome (MetS) are characterized by a highly inflammatory microenvironment predisposing or promoting genetic instability, which underlies neoplastic transformation (6), consequently leading to increased thyroid cancer risk (7, 8). Fine-needle aspiration biopsy/cytology (FNAB/C) is the only procedure to discriminate benign from malignant nodules. Unfortunately, due to its invasiveness, it cannot be considered a screening tool. Thus, other non-invasive highly specific predictors of malignancy may be useful in clinical practice.
Similarly, liver biopsy is not feasible in all patients suspected of metabolic-associated fatty liver disease (MAFLD), the hepatic manifestation of adiposity that ranges from steatosis to liver fibrosis. Assessing the grade of liver fibrosis is critical because it can still be reversed via healthier dieting and lifestyle before progressing toward cirrhosis and hepatocellular carcinoma (9). For these reasons, nowadays, a number of non-invasive scores have gained validity as first-line tools in patients with hepatic fibrosis since they are immediate and not operator-dependent and can be used in the outpatient setting, differently from liver biopsy and transient elastography (10). Intriguingly, these scores have been proposed not only in the assessment of liver fibrosis per se but also as indirect markers of cardiovascular risk and diabetes (11, 12) and in predicting the development of MAFLD complications (13) and hepatic and extra-hepatic cancers (14). Aspartate aminotransferase (AST) to alanine aminotransferase (ALT) ratio (AAR), aspartate aminotransferase to platelet ratio index (APRI), and fibrosis index based on four factors (FIB-4) are among the most validated non-invasive indexes.
Hence, given the possible pathogenic association of adiposopathy with thyroid cancer onset, we considered a consecutive sample of 142 patients with newly diagnosed thyroid nodules who underwent FNAB/C with the aim of detecting any dysmetabolism-associated biomarker that might be associated with malignancy.
2 Materials and methods
2.1 Study population
Patients’ recruitment, anthropometric, biochemical, and clinical variables were registered continuously in the electronic health register of Metabolic Diseases of the Department of Interdisciplinary Medicine—Internal Medicine Division—”Aldo Moro” University of Bari (Bari, Italy) from January 2018 to September 2022. Participants underwent physical examination, biochemical assessment, and thyroid ultrasound. The study was conducted in a group of 142 consecutive outpatients (47 men and 95 women) who were diagnosed with thyroid nodules and underwent ultrasound-guided FNAB/C due to suspicion of malignancy according to ultrasound characteristics (1). Patients with acute diseases and neoplastic diseases with recent onset (less than 10 years) and/or under chemotherapy were excluded. The study was approved by the Ethics Committee (n.311, MSC/PBMC/2015) of the Azienda Ospedaliero-Universitaria Policlinico di Bari (Bari, Italy) in accordance with the requirements of the Declaration of Helsinki. Written informed consent for the use of clinical data was obtained from all participants in the study. In accordance with the approval of the Ethics Committee, only patients who were already 18 years or older were included.
2.2 Clinical and biochemical assessment
All participants underwent a detailed anamnesis and physical examination. Anthropometric assessment was performed using standardized procedures. To sum up, waist circumference (WC) was measured at the midpoint between the inferior part of the 12th costa and the anterior–superior iliac crest. Body mass index (BMI) was computed as weight (kg) divided by the height squared (m2), and BMI values (kg/m2) between 25 and 29.9 and over 30.0 were considered as overweight and obesity conditions, respectively. Morning blood samples were obtained from the antecubital veins after 12 hours of fasting. After blood clotting and centrifugation, serum was processed for analysis of biochemical markers of glucose and lipid metabolism. Liver and thyroid markers were also studied following standardized biochemical procedures. All biochemical measurements were centralized and performed in the ISO 9001-certified laboratories of the University Hospital of Bari. Diabetes mellitus (DM) was diagnosed according to international criteria: HbA1c (percentage of glycosylated hemoglobin) ≥6.5%, fasting plasma glucose (FPG) ≥126 mg/dl, and/or active treatment for DM. Non-invasive liver fibrosis scores were determined according to published formulas. AAR was calculated as AST divided by ALT. The cutoff value adopted was AAR < 1 for the identification of a fibrosis-free liver and AAR ≥ 1 for probable fibrosis. APRI score was calculated as AST/platelet count (×109/L) × 100. The cutoff values were as follows: APRI < 0.5 for no fibrosis, APRI ≥ 0.5 for liver fibrosis, and APRI ≥ 1.5 for probable cirrhosis. FIB-4 index was calculated as age × AST/platelet count (×109/L) × √ALT. The cutoff values adopted were as follows: FIB-4 < 1.45 for no or moderate fibrosis, 1.45 < FIB-4 < 3.25 for moderate fibrosis, and FIB-4 > 3.25 for extensive fibrosis or cirrhosis (15).
Thyroid ultrasound was performed with an Esaote MyLab 70 Gold ultrasound system with 10–15-MHz linear transducers. Thyroid nodules were defined according to international criteria as discrete lesions within the thyroid gland radiologically distinct from the surrounding thyroid parenchyma (1). The maximal diameter of nodules was measured in three planes: longitudinal, transverse, and anteroposterior. Fine-needle aspiration (FNA) was used after ultrasound for cytological diagnosis of nodules. The cytologic assessment was performed according to the SIAPEC-SIE 2014 guidelines. Malignancy was assumed in those diagnostic categories for which surgery was the suggested action (TIR3B, TIR4, and TIR5) (16).
2.3 Statistical analysis
Descriptive statistical analyses of the study sample were performed, and results were expressed as mean ± standard deviation (SD) for numerical data and as counts and percentages for categorical data. Comparisons of continuous clinical variables between two groups were performed by Student’s t-test.
The receiver operating characteristic (ROC) curves were used to determine the optimum cutoff level of AAR, APRI, BMI, and FPG in discriminating malignancy of thyroid nodules. Empirical ROC curves were plotted for these variables along with a calculation of the area under the curve (AUC) with 95% confidence intervals and one-sided upper p-values for the null hypothesis AUC = 0.5. Youden’s index, or equivalently, the highest sensitivity + specificity, was used to determine the optimal cutoff of each variable for the prediction of malignancy.
Contingency tables, chi-squared test, and Fisher’s exact test, if required, were used to study the association between categorical variables. The results were expressed as odds ratios with their relative 95% confidence interval (95% CI) and were graphically plotted in a forest plot.
Correlations among continuous variables were also analyzed and estimated using Spearman’s correlation coefficient (r). p-Values (p) lower than 0.05 were considered statistically significant. All analyses were performed using the NCSS 12 Statistical Software, version 12.0.2018 (NCSS, LLC Company, Kaysville, UT, USA) and GraphPad Prism, version 9.1.0 (GraphPad Software, San Diego, CA, USA).
3 Results
3.1 Clinical characterization of the study population
A total of 142 subjects (47 men and 95 women) with putative risk of metabolic diseases underwent thyroid ultrasound exam and were diagnosed with suspected malignant thyroid nodules, thus FNAB/C was performed. After FNAB/C, 121 patients (85%; 39 men and 82 women) were diagnosed with benign thyroid nodules, while 21 individuals (15%) were diagnosed with thyroid cancer (8 men and 13 women). As shown in Table 1, 106 (75%) patients had pathological WC according to the International Diabetes Federation (IDF) criterion for MetS diagnosis (17). A total of 71 patients (50%) were overweight (BMI ≥ 25 kg/m2), and 23 (16%) were obese (BMI ≥ 30 kg/m2). Moreover, 28 patients (20%) were affected by diabetes mellitus.
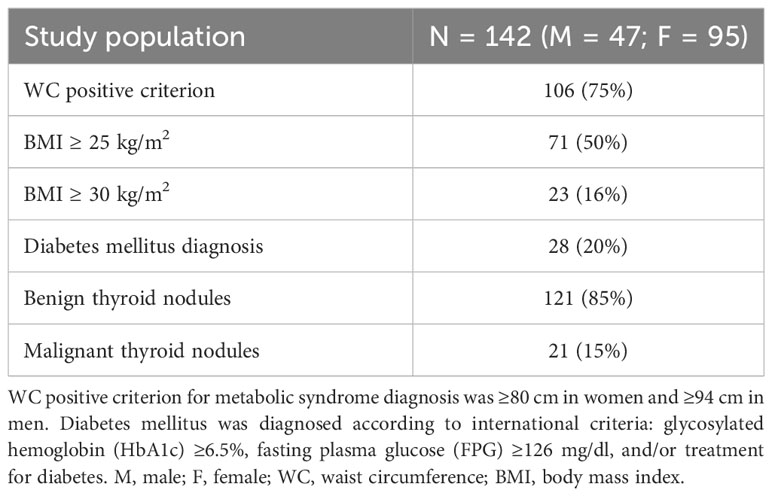
Table 1 Clinical characterization of the study population.
3.2 Clinical and biochemical variables characterizing patients with nodule malignancy
With the aim of identifying metabolic biomarkers associated with thyroid nodule malignancy, we compared groups of patients with benign and malignant nodules. First of all, we investigated whether sex could influence thyroid cancer susceptibility. We performed a chi-squared test finding that there was no significant association (p = 0.598, Supplementary Table 1). Age as well as WC did not significantly differ between the two groups, while patients with thyroid cancer exhibited increased BMI (p = 0.048) and FPG levels (p = 0.046). Lipid profile, 25-OH vitamin D, and thyroid function markers were not found to be statistically different between the two groups. Regarding transaminase levels, only AST was found to be significantly higher in the malignant group (p < 0.001) compared to subjects with benign nodules, albeit in the normal range of values. Intriguingly, considering non-invasive scores for liver fibrosis, subjects with thyroid cancer presented increased AAR (p < 0.001) and APRI scores (p = 0.007), while no difference was found for FIB-4 (Table 2).
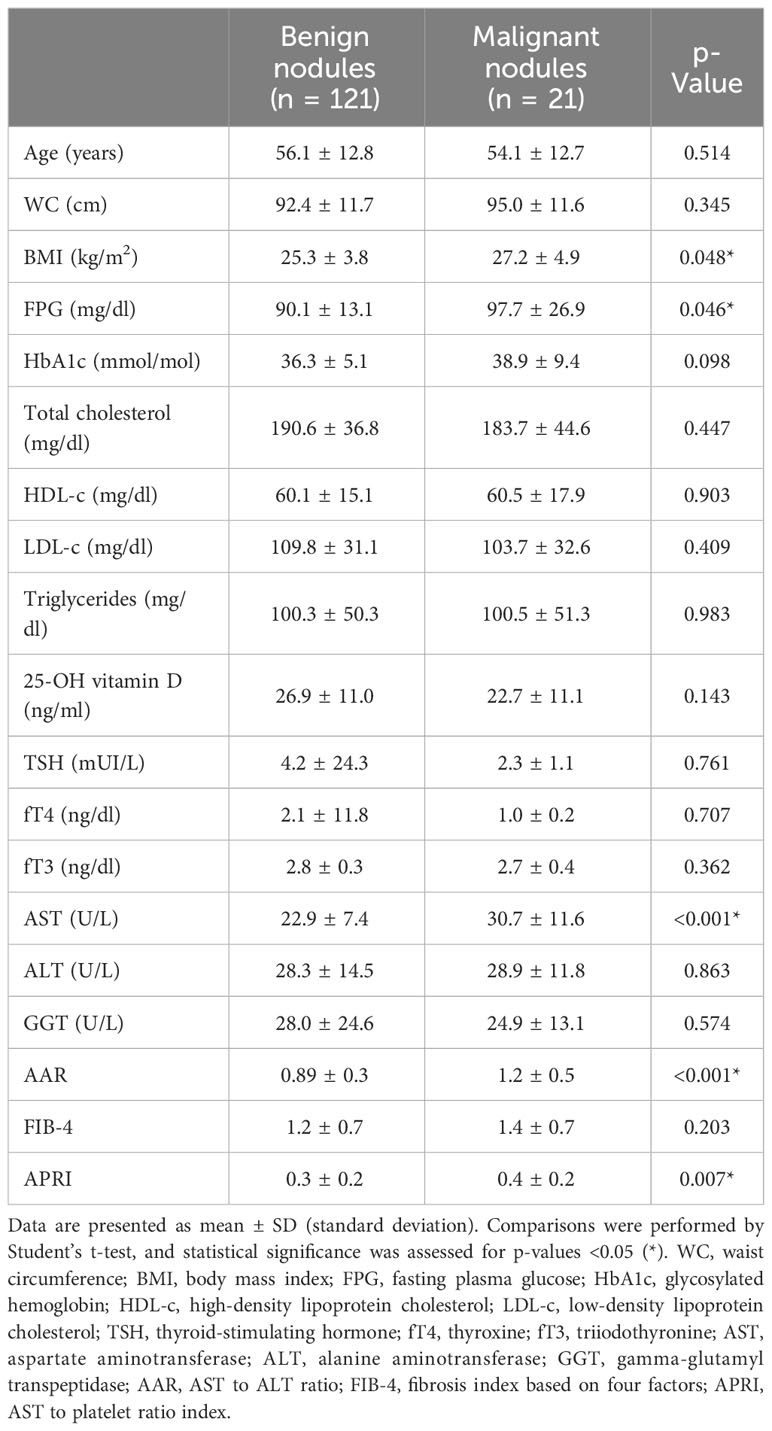
Table 2 Comparison of biochemical and clinical variables between subjects with benign nodules and malignant nodules.
3.3 Discrimination of nodule malignancy by metabolic biomarkers
We performed ROC curve analyses of AAR, APRI score, BMI, and FPG to define cutoff values for discrimination of thyroid nodule malignancy.
The empirical ROC curve of AAR (Figure 1A) was characterized by the largest AUC as well as the highest Youden’s index (sensitivity = 52%, specificity = 87%), with a cutoff value of 1.12 (p < 0.01). APRI score (Figure 1B) presented intermediate sensitivity and high specificity (48% and 85%, respectively), with a significant AUC (p < 0.01) and a cutoff value of 0.45. The empirical ROC curve of BMI (Figure 1C) showed high specificity (83%) but lower sensitivity than AAR and APRI scores in discriminating thyroid cancer, with a cutoff value of 29.01 (p = 0.058). Despite very high specificity (90%), FPG levels showed the lowest sensitivity (33%) and the smallest AUC (p = 0.131) in discriminating between benign and malignant nodules, with a cutoff value of 103 mg/dl (Figure 1D). Overall, these data highlight the strong ability of AAR and APRI to accurately discriminate thyroid nodule malignancy.
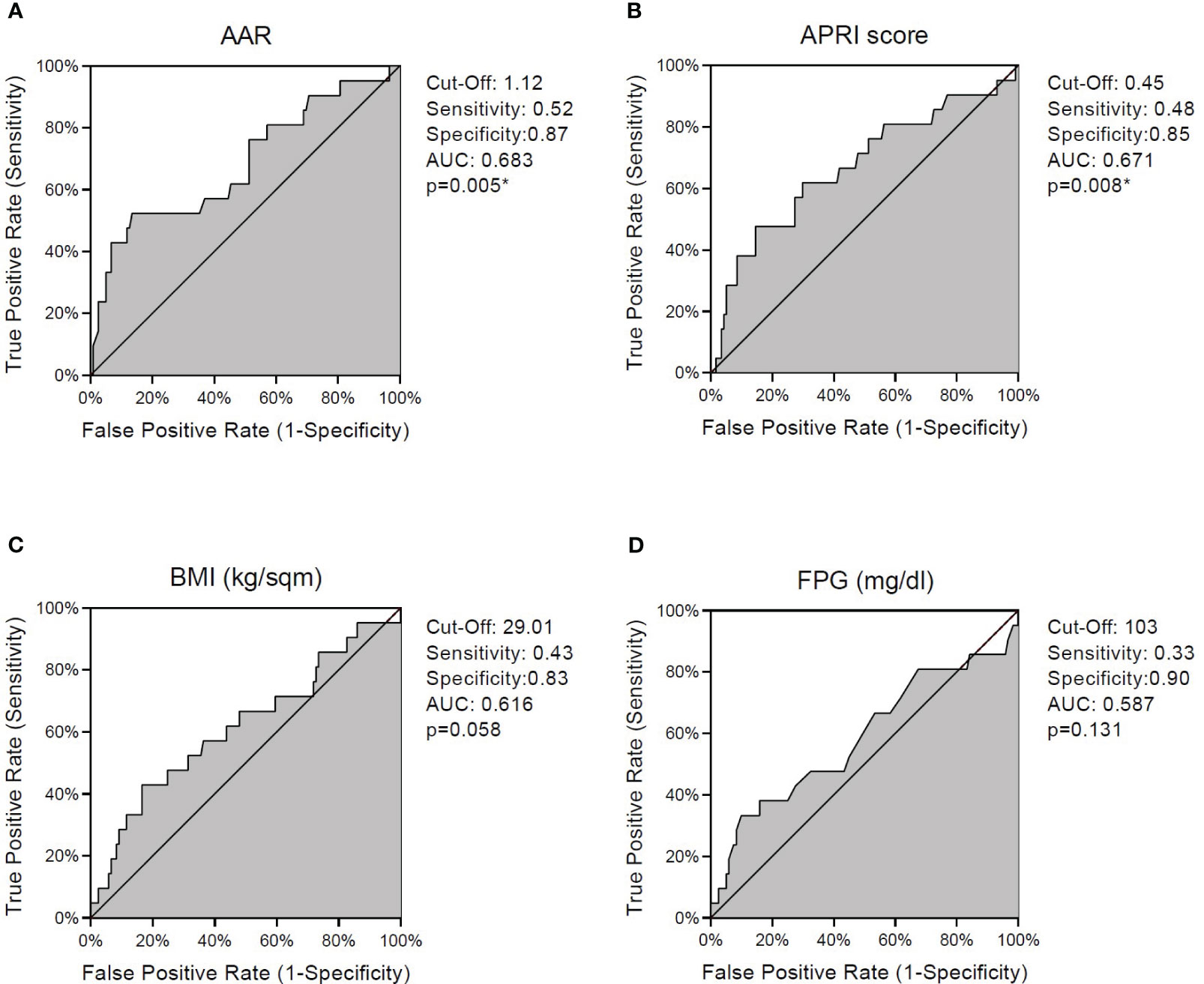
Figure 1 ROC curves for discrimination of thyroid nodule malignancy. Graphs indicate cutoff values with respective sensitivity and specificity levels and empirical estimation of area under curve (AUC) for AAR (A), APRI score (B), BMI (C), and fasting plasma glucose (D). (*) indicates significant p-values. ROC, receiver operating characteristic; AST, aspartate aminotransferase; ALT, alanine aminotransferase; AAR, AST to ALT ratio; APRI score, AST to platelet ratio index; BMI, body mass index; p, p-value.
3.4 Dysmetabolic condition-associated risk of malignancy
To understand whether and to what degree dysmetabolic conditions increased the risk of thyroid nodule malignancy, we calculated the odds ratio (OR) of main biomarkers, stratifying our population according to both internationally validated cutoff values and cutoff values that have been calculated through the analysis of our ROC curves even if not significant (Figure 2) (18).
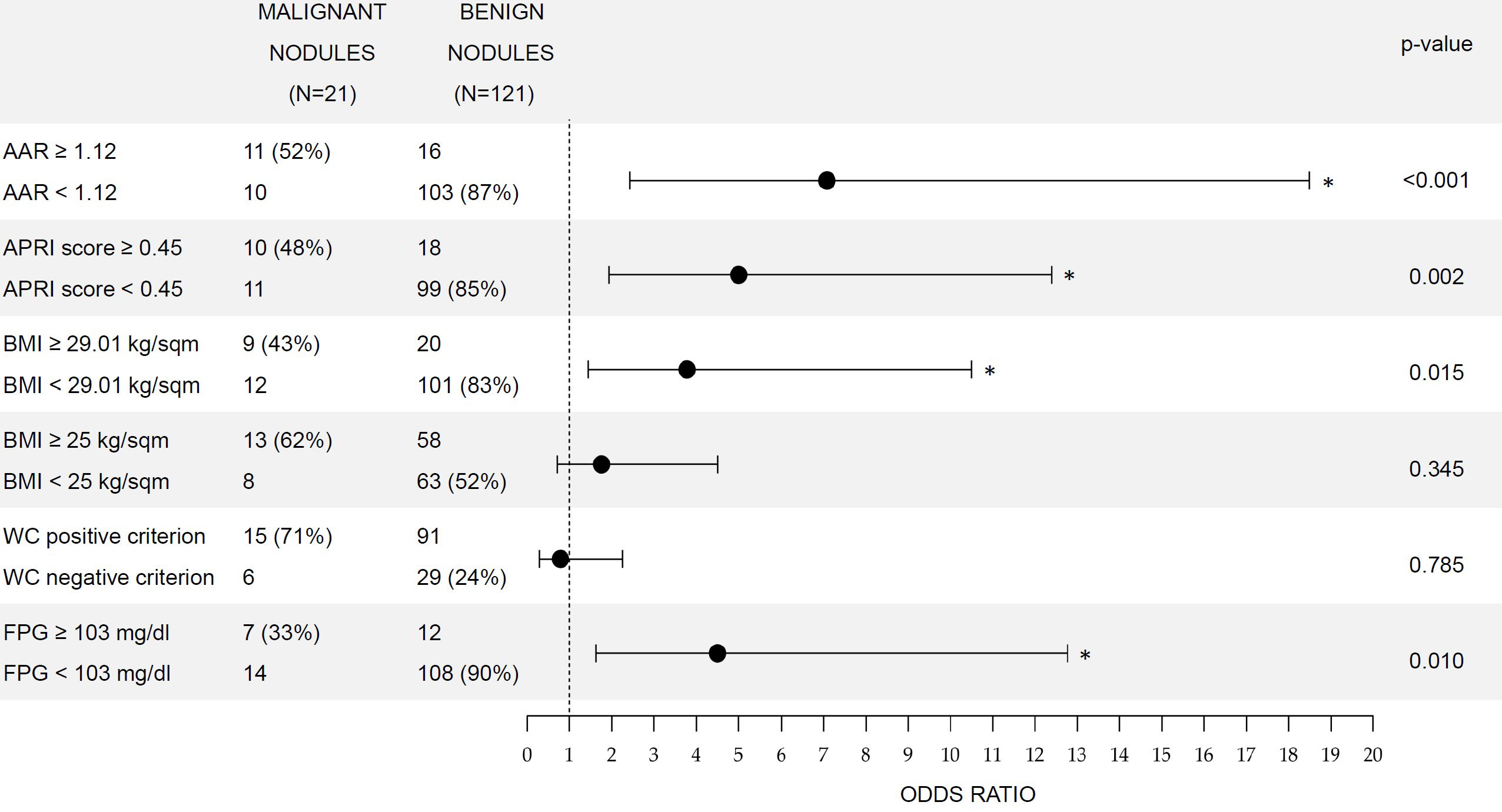
Figure 2 Comparison of odds ratio for thyroid cancer in patients with increased biomarkers. Contingency tables are presented on the left side of the picture. (%) in the second and third columns indicate, respectively, sensitivity and specificity. p-Value refers to chi-squared tests and (*) indicates significant p-values. Bars represent 95% CI for ORs. WC positive criterion for metabolic syndrome diagnosis was ≥80 cm in women and ≥94 cm in men. ORs, odds ratios; AST, aspartate aminotransferase; ALT, alanine aminotransferase; AAR, AST to ALT ratio; APRI score, AST to platelet ratio index; BMI, body mass index; WC, waist circumference; FPG, fasting plasma glucose.
Values of AAR above the international cutoff for the identification of liver fibrosis (AAR ≥ 1) indicate increased risk of malignancy with an OR of 2.13 (95% CI: 1.2–3.8), although the association in the chi-squared test was not significant (p = 0.077), while AAR values above the ROC cutoff of 1.12 showed the highest OR (7.1, 95% CI: 2.4–18.5), with a significant association (p < 0.001). Considering APRI, values above the international cutoff of 0.5 and the ROC cutoff of 0.45 were both associated (p < 0.05) with malignancy, with ORs of 6.6 (95% CI: 2.0–20.0) and 5 (95% CI: 1.9–12.6), respectively.
Regarding BMI, overweight condition (BMI ≥ 25 kg/m2) was not associated with thyroid cancer (p = 0.345). Conversely, systemic obesity (BMI ≥ 30 kg/m2) was associated (p = 0.047) with a risk of nodule malignancy (OR = 3.3, 95% CI: 1.2–8.9). Interestingly, an even higher risk (OR = 3.8, 95% CI: 1.5–10.5) was associated (p = 0.015) with BMI values above the ROC cutoff of 29.01 kg/m2. Surprisingly, visceral obesity assessed by WC was not associated (p = 0.785) with the risk of thyroid cancer in our study population.
Finally, FPG levels above the ROC cutoff value of 103 mg/dl were also found to significantly (p = 0.01) increase the risk of malignant nodules (OR = 4.5, 95% CI: 1.6–12.8).
3.5 Metabolic correlations among biomarkers in benign and malignant nodule populations
To further disclose how dysmetabolic conditions could affect the nature of thyroid nodules, we performed correlations among AAR, APRI, and biochemical metabolic biomarkers in patients with benign nodules and with cancer, separately (Figure 3).
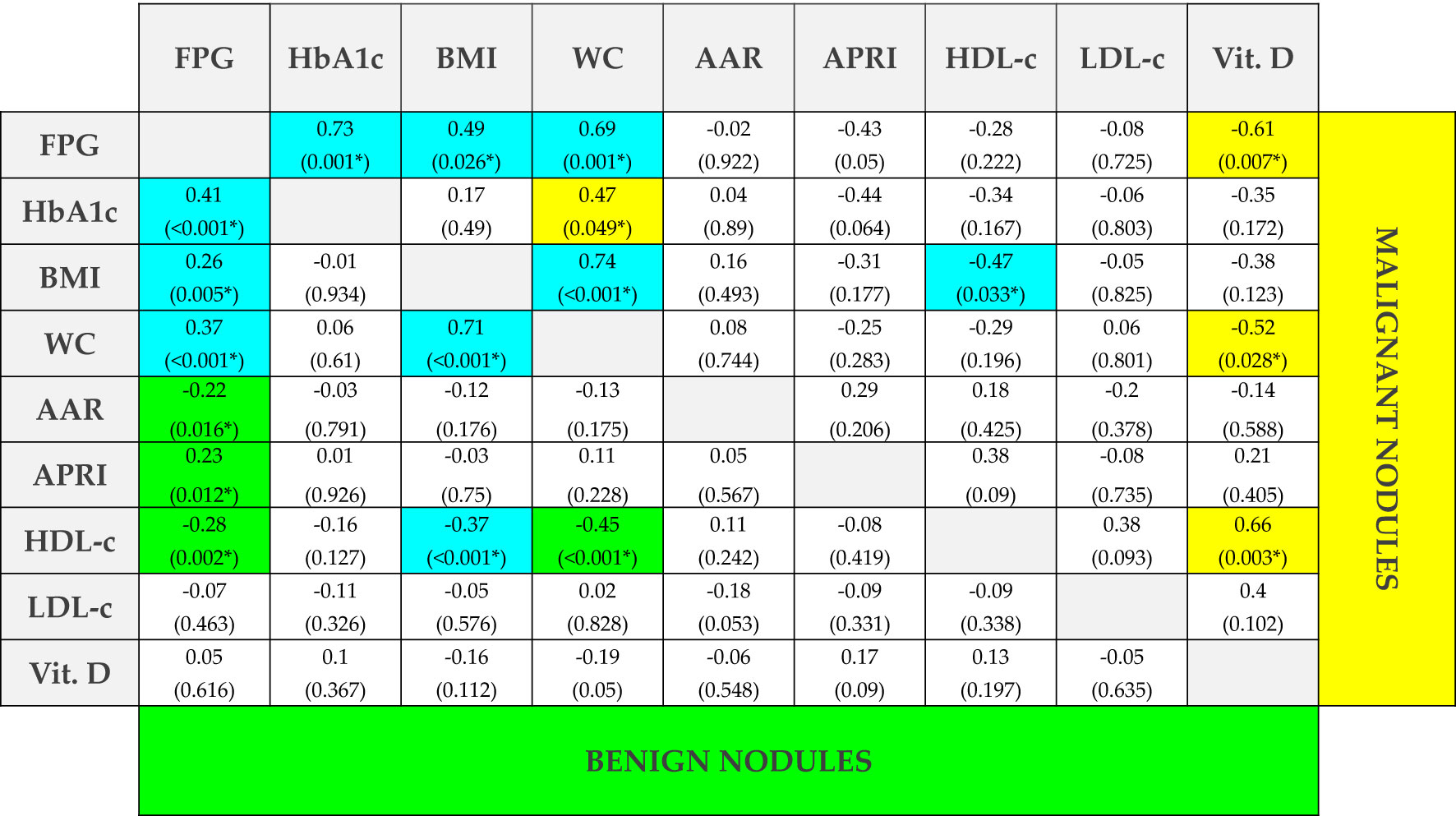
Figure 3 Spearman’s correlations among clinical and biochemical biomarkers in subjects with benign and malignant nodules. R and p-values (in brackets) of Spearman’s correlations among clinical and biochemical biomarkers. Statistical significance was assessed for p-values <0.05 (*). Blue cells represent correlations that are significant in both groups, yellow cells represent correlations that are significant only in patients with malignant thyroid nodules, and green cells represent correlations that are significant only in patients with benign nodules. FPG, fasting plasma glucose; HbA1c, glycosylated hemoglobin; BMI, body mass index; WC, waist circumference; AAR, AST to ALT ratio; APRI score, AST to platelet ratio index; HDL-c, high-density lipoprotein cholesterol; LDL-c, low-density lipoprotein cholesterol; Vit. D, 25-hydroxy vitamin D.
Regarding AAR and APRI, in the benign group, they both significantly (p < 0.05) correlated with FPG, although inversely (r = −0.22) and directly (r = 0.23), respectively. These results are in line with previous studies in subjects with a risk of diabetes (19, 20). Intriguingly, these correlations were both lost when considering cancer patients, suggesting that a metabolic derangement could be present in patients with cancer. To further investigate the other pathways that may be involved in cancer pathogenesis, we performed correlations among the other metabolic biomarkers. We found significant correlations of BMI with FPG (Figure 4A), WC (Figure 4B), and high-density lipoprotein cholesterol (HDL-c) (Figure 4C) in subjects with benign nodules, as well as in those with malignant ones. Furthermore, HDL-c showed statistically significant correlations with FPG (Figure 4D) and WC (Figure 4E) only in subjects with benign nodules, while HDL-c levels were observed to significantly correlate with BMI (Figure 4F) in both groups. Conversely, 25-OH vitamin D significantly correlated with FPG (Figure 4G), WC (Figure 4H), and HDL-c (Figure 4I) only in patients with malignant nodules, thus suggesting that its deficiency could play a crucial role in the development of thyroid malignancy.
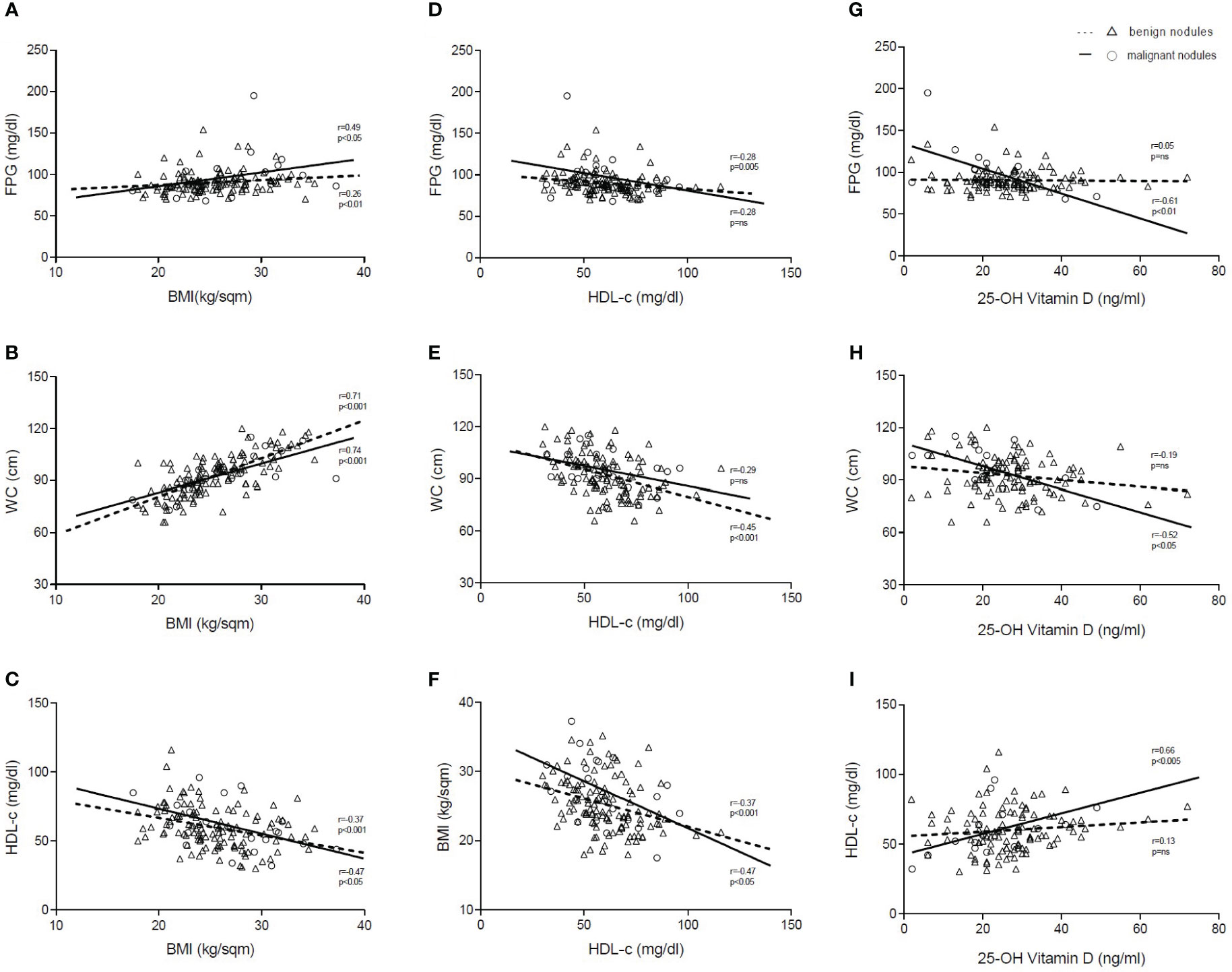
Figure 4 Correlations of BMI, HDL-c, and 25-OH vitamin D. Representation of Spearman’s correlations (r) of BMI (A–C), HDL-c (D–F), and 25-OH vitamin D (G–I) in patients with benign and malignant thyroid nodules. Statistical significance was assessed for p-values <0.05. Dashed lines indicate patients with benign nodules (Δ), and solid lines indicate patients with malignant nodules (o). FPG, fasting plasma glucose; WC, waist circumference; HDL-c, high-density lipoprotein cholesterol; BMI, body mass index; p, p-value; ns, not significant.
4 Discussion
In this study, we show for the first time that increased non-invasive liver fibrosis scores AAR and APRI are associated with thyroid cancer in patients with newly diagnosed thyroid nodules.
Although previous studies had investigated the possible role of AAR in predicting cancer incidence and mortality, to the best of our knowledge, this is the first study specifically pointing to the possible association between thyroid cancer and liver fibrosis indexes. Indeed, in a prospective Chinese study, baseline AAR was recently proposed for the prediction of the future development of cancer in a cohort of 9,946 participants, but unfortunately, no data were supplied for the specific cohort of thyroid cancer patients (21). Also, a retrospective Japanese study in 85,658 individuals investigated whether AAR may predict cancer onset, finding that a higher AAR increased the risk of cancer development, but only in men who were drinkers, while no association was detected in women and abstainer men. However, they did not register an appropriate number of thyroid cancer cases to speculate about specific correlations (22). Furthermore, similarly to a previous study exploring APRI association with thyroid autoimmune diseases (23), we confirm the usefulness of these scores in predicting a wide range of conditions, beyond liver fibrosis. However, there are some issues to be addressed.
In order to understand the reasons for this association, the first question is whether these scores possess a predictive and diagnostic power per se or if their increase mirrors the pathogenic involvement of MAFLD and liver fibrosis in thyroid carcinogenesis. Indeed, a recent study enrolling 352,911 participants showed that the presence of fatty liver was a significant risk factor for the development of thyroid cancer (24). It has been hypothesized that, as soon as hepatic steatosis progresses, leptin release may cause the death of macrophages and hepatocytes through CD8+ T lymphocytes, which could in turn promote the proliferation and invasiveness of tumors such as thyroid cancer (25).
Moreover, the loss of AAR and APRI correlations with FPG in patients with cancer underscores the involvement of other dysmetabolic conditions associated with fatty liver, such as obesity, impaired glycemia, and dyslipidemia.
In line with previous studies (26–30), we observed that BMI and increased FPG were both associated with malignancy. Chronic hyperglycemia has been observed to directly influence cancer cell growth through the promotion of oxidative stress (31), and increased reactive oxygen species (ROS) concentrations have been observed in thyroid cancer cells (32). We previously identified increased visceral adipose tissue and oxidative stress as predisposing conditions to impaired reverse cholesterol transport (RCT), a process in which HDL particles are critically involved (33). In this study, HDL level intriguingly shows significant correlations with FPG and WC only in subjects with benign nodules, while a significant direct correlation with 25-OH vitamin D, as previously reported (34, 35), was found only in patients with malignant nodules. On the one hand, the paradoxical uncoupling of cholesterol bioavailability and synthesis has already been shown in cancer cells (36). On the other hand, although the association of vitamin D levels with thyroid cancer onset is still being debated, our result strengthens the hypothesis that elevated serum levels of vitamin D hold a protective role toward thyroid malignancy (37) by inhibiting pro-tumorigenic inflammation (38). Nevertheless, given its role in the regulation of intestinal barrier integrity and control of innate and adaptive immunity in the gut (39), our result also suggests that lower levels of vitamin D may contribute to a worsening of the alterations of the gut microbiota typically observed in dysmetabolic subjects, thus tightening the relationship between metabolic diseases and thyroid cancer. Thus, one should consider that low vitamin D levels could increase the extra-hepatocytic inflammation process that dumps the progression of steatosis to fibrosis, also opening new perspectives on the utility of vitamin D supplementation in the prevention and treatment of MAFLD and supporting the metabolic interplay among hepatocyte infarction, imbalanced cholesterol metabolism, and cancer (40).
Our study has some limitations. First, the small size of our sample underlines the pressing need for further validation of AAR and APRI in a different cohort of metabolic subjects undergoing FNAB/C. Second, our data lacked potential important confounders, such as the use of antidiabetic and lipid-lowering drugs, which may influence the development of steatohepatitis and liver function, as well as anti-platelet treatment that may influence platelet count used for the calculation of APRI. Third, data on environmental risk factors and cancer susceptibility (41) were self-reported by patients, and no further detailed information was available. Finally, non-invasive scores should be correlated with liver ultrasound and elastography data to assess whether they represent the stigmata of liver dysfunction that eventually acts as a carcinogenesis trigger.
In conclusion, the strength of our study lies in the ability of non-invasive liver fibrosis scores AAR and APRI to assess the risk of malignancy in thyroid nodules of metabolic subjects. Thereby, on the one hand, in the future, exploring this association might lead to elaborate new scores to predict thyroid malignancy and to speed up the diagnostic process, also targeting patients who need to be offered FNAB/C of suspected nodules. On the other hand, future studies are needed to prove that reducing obesity, counteracting fatty liver-associated diseases and metabolic derangements, and supplementing vitamin D could probably prevent thyroid cancer onset at least in specific groups of patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee (n.311, MSC/PBMC/2015) of the Azienda Ospedaliero-Universitaria Policlinico di Bari (Bari, Italy). The studies were conducted in accordance with local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
Conceptualization, AM; methodology, LC, GG, and AM; software, LC, FN, and CM; formal analysis, FN, CM, SP, and GG; investigation, PS, EB, GA, GP, and CS; resources, LC and FN; data curation, FN, CM, and SP; writing—original draft preparation, FN; writing—review and editing, LC and AM; visualization, LC and FN; supervision, AM; project administration, AM; funding acquisition, LC, PS, and AM. All authors have read and agreed to the published version of the manuscript.
Funding
AM is funded by Italian Association for Cancer Research—AIRC IG 2019 Id 23239; EU-JPI HDL-INTIMIC—MIUR FATMAL; MIUR-PON “R&I” 2014–2020 “BIOMIS” cod. ARS01_01220; POR Puglia FESR—FSE 2014–2020, “INNOMA” cod. 4TCJLV4. AM and PS are funded by the National Recovery and Resilience Plan (NRRP), Mission 4 Component 2 Investment 1.3—Call for tender No. 341 of 15 March 2022 of Italian Ministry of University and Research funded by the European Union—NextGeneration EU; Project code PE00000003, Concession Decree No. 1550 of 11 October 2022 adopted by the Italian Ministry of University and Research, CUP D93C22000890001, Project title “ON Foods— Research and innovation network on food and nutrition Sustainability, Safety and Security—Working ON Foods”. LC is funded under the National Recovery and Resilience Plan (NRRP), Mission 4 Component 2 Investment 1.3—Call for tender No. 341 of March 15, 2022, of Italian Ministry of University and Research funded by the European Union—NextGeneration EU; Award Number: Project code PE0000015, Concession Decree No. 1243 of August 2, 2022, adopted by the Italian Ministry of University and Research, CUP H33C22000680006, Project title “Ageing well in an ageing society—A novel public-private alliance to generate socioeconomic, biomedical and technological solutions for an inclusive Italian ageing society—AGE-IT.
Acknowledgments
We thank the physicians and nurses of the Unità Operativa Complessa Universitaria di Medicina Interna “Cesare Frugoni” of the Azienda Ospedaliero—Universitaria Policlinico di Bari for their help and support during the study. Special thanks to Roberta Le Donne for her support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1233083/full#supplementary-material
References
1. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 american thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid (2016) 26:1–133. doi: 10.1089/thy.2015.0020
2. Kant R, Davis A, Verma V. Thyroid nodules: advances in evaluation and management. Am Fam Physician (2020) 102:298–304.
3. Hu J, Yuan IJ, Mirshahidi S, Simental A, Lee SC, Yuan X. Thyroid carcinoma: phenotypic features, underlying biology and potential relevance for targeting therapy. Int J Mol Sci (2021) 22:1950. doi: 10.3390/ijms22041950
4. Bogović Crnčić T, Ilić Tomaš M, Girotto N, Grbac Ivanković S. Risk factors for thyroid cancer: what do we know so far? Acta Clin Croat (2020) 59:66–72. doi: 10.20471/acc.2020.59.s1.08
5. Feng X, Wang F, Yang W, Zheng Y, Liu C, Huang L, et al. Association between genetic risk, adherence to healthy lifestyle behavior, and thyroid cancer risk. JAMA Netw Open (2022) 5:e2246311. doi: 10.1001/jamanetworkopen.2022.46311
6. Crudele L, Piccinin E, Moschetta A. Visceral adiposity and cancer: role in pathogenesis and prognosis. Nutrients (2021) 13:2101. doi: 10.3390/nu13062101
7. Matrone A, Ferrari F, Santini F, Elisei R. Obesity as a risk factor for thyroid cancer. Curr Opin Endocrinol Diabetes Obes (2020) 27:358–63. doi: 10.1097/MED.0000000000000556
8. Wang M, Gong W-W, Lu F, Hu R-Y, He Q-F, Yu M. The association between diabetes and thyroid cancer risk: a hospital-based case-control study in China. BMC Endocr Disord (2021) 21:21. doi: 10.1186/s12902-021-00684-y
9. Crudele L, De Matteis C, Piccinin E, Gadaleta RM, Cariello M, Di Buduo E, et al. Low HDL-cholesterol levels predict hepatocellular carcinoma development in individuals with liver fibrosis. JHEP Rep (2023) 5:100627. doi: 10.1016/j.jhepr.2022.100627
10. Berzigotti A, Tsochatzis E, Boursier J, Castera L, Cazzagon N, Friedrich-Rust M, et al. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis – 2021 update. J Hepatol (2021) 75:659–89. doi: 10.1016/j.jhep.2021.05.025
11. De Matteis C, Cariello M, Graziano G, Battaglia S, Suppressa P, Piazzolla G, et al. AST to Platelet Ratio Index (APRI) is an easy-to-use predictor score for cardiovascular risk in metabolic subjects. Sci Rep (2021) 11:14834. doi: 10.1038/s41598-021-94277-3
12. Crudele L, Novielli F, Petruzzelli S, Battaglia S, Giuliano AFM, Melodia R, et al. Liver fibrosis indices predict the severity of SARS-coV-2 infection. J Clin Med (2022) 11:5369. doi: 10.3390/jcm11185369
13. Önnerhag K, Hartman H, Nilsson PM, Lindgren S. Non-invasive fibrosis scoring systems can predict future metabolic complications and overall mortality in non-alcoholic fatty liver disease (NAFLD). Scand J Gastroenterol (2019) 54:328–34. doi: 10.1080/00365521.2019.1583366
14. Younes R, Caviglia GP, Govaere O, Rosso C, Armandi A, Sanavia T, et al. Long-term outcomes and predictive ability of non-invasive scoring systems in patients with non-alcoholic fatty liver disease. J Hepatol (2021) 75:786–94. doi: 10.1016/j.jhep.2021.05.008
15. Lazarus JV, Castera L, Mark HE, Allen AM, Adams LA, Anstee QM, et al. Real-world evidence on non-invasive tests and associated cut-offs used to assess fibrosis in routine clinical practice. JHEP Rep (2023) 5:100596. doi: 10.1016/j.jhepr.2022.100596
16. Nardi F, Basolo F, Crescenzi A, Fadda G, Frasoldati A, Orlandi F, et al. Italian consensus for the classification and reporting of thyroid cytology. J Endocrinol Invest (2014) 37:593–9. doi: 10.1007/s40618-014-0062-0
17. Alberti KGMM, Zimmet P, Shaw J. Metabolic syndrome–a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabetes Med (2006) 23:469–80. doi: 10.1111/j.1464-5491.2006.01858.x
18. Grund B, Sabin C. Analysis of biomarker data: logs, odds ratios, and receiver operating characteristic curves. Curr Opin HIV AIDS (2010) 5:473–9. doi: 10.1097/COH.0b013e32833ed742
19. Corbin KD, Pittas AG, Desouza C, Grdinovac KK, Herzig K-H, Kashyap SR, et al. Indices of hepatic steatosis and fibrosis in prediabetes and association with diabetes development in the vitamin D and type 2 diabetes study. J Diabetes its Complications (2023) 37:108475. doi: 10.1016/j.jdiacomp.2023.108475
20. Miyake Y, Eguchi H, Shinchi K, Oda T, Sasazuki S, Kono S. Glucose intolerance and serum aminotransferase activities in Japanese men. J Hepatol (2003) 38:18–23. doi: 10.1016/s0168-8278(02)00323-9
21. Chen W, Wang W, Zhou L, Zhou J, He L, Li J, et al. Elevated AST/ALT ratio is associated with all-cause mortality and cancer incident. Clin Lab Anal (2022) 36:e24356. doi: 10.1002/jcla.24356
22. Kobayashi D, Yamamoto K, Kimura T, Shimbo T. Aspartate aminotransferase/alanine aminotransferase ratio and subsequent cancer development. Cancer Med (2022) 11:798–814. doi: 10.1002/cam4.4473
23. Naguib R, Fayed A, Elkemary EZ, Naguib H. Evaluation of thyroid function and thyroid autoimmune disease in patients with non-alcoholic fatty liver disease. Clin Exp Hepatol (2021) 7:422–8. doi: 10.5114/ceh.2021.111169
24. Liu Z, Lin C, Suo C, Zhao R, Jin L, Zhang T, et al. Metabolic dysfunction-associated fatty liver disease and the risk of 24 specific cancers. Metabolism (2022) 127:154955. doi: 10.1016/j.metabol.2021.154955
25. Yang Z, Wei X, Pan Y, Xu J, Si Y, Min Z, et al. A new risk factor indicator for papillary thyroid cancer based on immune infiltration. Cell Death Dis (2021) 12:51. doi: 10.1038/s41419-020-03294-z
26. Hwang Y, Lee KE, Park YJ, Kim S-J, Kwon H, Park DJ, et al. Annual average changes in adult obesity as a risk factor for papillary thyroid cancer: A large-scale case-control study. Med (Baltimore) (2016) 95:e2893. doi: 10.1097/MD.0000000000002893
27. Youssef MR, Reisner ASC, Attia AS, Hussein MH, Omar M, LaRussa A, et al. Obesity and the prevention of thyroid cancer: Impact of body mass index and weight change on developing thyroid cancer - Pooled results of 24 million cohorts. Oral Oncol (2021) 112:105085. doi: 10.1016/j.oraloncology.2020.105085
28. Harikrishna A, Ishak A, Ellinides A, Saad R, Christodoulou H, Spartalis E, et al. The impact of obesity and insulin resistance on thyroid cancer: A systematic review. Maturitas (2019) 125:45–9. doi: 10.1016/j.maturitas.2019.03.022
29. Schmid D, Ricci C, Behrens G, Leitzmann MF. Adiposity and risk of thyroid cancer: a systematic review and meta-analysis. Obes Rev (2015) 16:1042–54. doi: 10.1111/obr.12321
30. Huang L, Feng X, Yang W, Li X, Zhang K, Feng S, et al. Appraising the effect of potential risk factors on thyroid cancer: A mendelian randomization study. J Clin Endocrinol Metab (2022) 107:e2783–91. doi: 10.1210/clinem/dgac196
31. Papachristoforou E, Lambadiari V, Maratou E, Makrilakis K. Association of glycemic indices (Hyperglycemia, glucose variability, and hypoglycemia) with oxidative stress and diabetic complications. J Diabetes Res (2020) 2020:7489795. doi: 10.1155/2020/7489795
32. Jelic MD, Mandic AD, Maricic SM, Srdjenovic BU. Oxidative stress and its role in cancer. J Cancer Res Ther (2021) 17:22–8. doi: 10.4103/jcrt.JCRT_862_16
33. Härdfeldt J, Cariello M, Simonelli S, Ossoli A, Scialpi N, Piglionica M, et al. Abdominal obesity negatively influences key metrics of reverse cholesterol transport. Biochim Biophys Acta Mol Cell Biol Lipids (2022) 1867:159087. doi: 10.1016/j.bbalip.2021.159087
34. De Matteis C, Crudele L, Cariello M, Battaglia S, Piazzolla G, Suppressa P, et al. Monocyte-to-HDL ratio (MHR) predicts vitamin D deficiency in healthy and metabolic women: A cross-sectional study in 1048 subjects. Nutrients (2022) 14:347. doi: 10.3390/nu14020347
35. Crudele L, Garcia-Irigoyen O, Cariello M, Piglionica M, Scialpi N, Florio M, et al. Total serum FGF-21 levels positively relate to visceral adiposity differently from its functional intact form. Front Endocrinol (Lausanne) (2023) 14:1159127. doi: 10.3389/fendo.2023.1159127
36. Bovenga F, Sabbà C, Moschetta A. Uncoupling nuclear receptor LXR and cholesterol metabolism in cancer. Cell Metab (2015) 21:517–26. doi: 10.1016/j.cmet.2015.03.002
37. Palanca A, Ampudia-Blasco FJ, Real JT. The controversial role of vitamin D in thyroid cancer prevention. Nutrients (2022) 14:2593. doi: 10.3390/nu14132593
38. Hansen CM, Binderup L, Hamberg KJ, Carlberg C. Vitamin D and cancer: effects of 1,25(OH)2D3 and its analogs on growth control and tumorigenesis. Front Biosci (2001) 6:D820–848. doi: 10.2741/hansen
39. Lu G, Yu X, Jiang W, Luo Q, Tong J, Fan S, et al. Alterations of gut microbiome and metabolite profiles associated with anabatic lipid dysmetabolism in thyroid cancer. Front Endocrinol (Lausanne) (2022) 13:893164. doi: 10.3389/fendo.2022.893164
40. Lo Sasso G, Celli N, Caboni M, Murzilli S, Salvatore L, Morgano A, et al. Down-regulation of the LXR transcriptome provides the requisite cholesterol levels to proliferating hepatocytes. Hepatology (2010) 51:1334–44. doi: 10.1002/hep.23436
Keywords: malignant thyroid nodule, liver fibrosis, thyroid cancer, BMI, obesity
Citation: Crudele L, Novielli F, De Matteis C, Petruzzelli S, Suppressa P, Berardi E, Antonica G, Piazzolla G, Sabbà C, Graziano G and Moschetta A (2023) Thyroid nodule malignancy is associated with increased non-invasive hepatic fibrosis scores in metabolic subjects. Front. Oncol. 13:1233083. doi: 10.3389/fonc.2023.1233083
Received: 01 June 2023; Accepted: 09 October 2023;
Published: 26 October 2023.
Edited by:
So Hee Kwon, Yonsei University, Republic of KoreaReviewed by:
Rhitajit Sarkar, National Institute of Diabetes and Digestive and Kidney Diseases (NIH), United StatesRunsheng Ma, First Affiliated Hospital of Zhengzhou University, China
Copyright © 2023 Crudele, Novielli, De Matteis, Petruzzelli, Suppressa, Berardi, Antonica, Piazzolla, Sabbà, Graziano and Moschetta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Moschetta, YW50b25pby5tb3NjaGV0dGFAdW5pYmEuaXQ=
†These authors share first authorship