 Ziming He
Ziming He Di Tang
Di Tang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 13 July 2023
Sec. Gastrointestinal Cancers: Hepato Pancreatic Biliary Cancers
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1230164
This article is part of the Research Topic Recent Advances in Diagnosis, Prognosis, and Therapy of Oncogenic Virus-driven Tumors View all 7 articles
Hepatitis B virus (HBV) is identified as a major risk factor for hepatocellular carcinoma (HCC), resulting in so-called hepatitis B virus-related hepatocellular carcinoma (HBV-related HCC). Hepatectomy for HCC is acknowledged as an efficient treatment strategy, especially for early HCC. Furthermore, patients with advanced HCC can still obtain survival benefits through surgical treatment combined with neoadjuvant therapy, adjuvant therapy, transcatheter arterial chemoembolization, and radiofrequency ablation. Therefore, preoperative and postoperative predictors of HBV-related HCC have crucial indicative functions for the follow-up treatment of patients with feasible hepatectomy. This review covers a variety of research results on preoperative and postoperative predictors of hepatectomy for HBV-related HCC over the past decade and in previous landmark studies. The relevant contents of Hepatitis C virus-related HCC, non-HBV non-HCV HCC, and the artificial intelligence application in this field are briefly addressed in the extended content. Through the integration of this review, a large number of preoperative and postoperative factors can predict the prognosis of HBV-related HCC, while most of the predictors have no standardized thresholds. According to the characteristics, detection methods, and application of predictors, the predictors can be divided into the following categories: 1. serological and hematological predictors, 2. genetic, pathological predictors, 3. imaging predictors, 4. other predictors, 5. analysis models and indexes. Similar results appear in HCV-related HCC, non-HBV non-HCV HCC. Predictions based on AI and big biological data are actively being applied. A reasonable prediction model should be established based on the economic, health, and other levels in specific countries and regions.
Primary liver cancer, in 185 countries and regions worldwide in 2020, is the sixth most commonly diagnosed cancer and the third leading cause of cancer death, with about 905,677 new cases and 830,180 deaths (Figure 1), 75%-85% of which are hepatocellular carcinoma (HCC) (1). As the main risk factor for HCC, a series of integrated global health sector strategies on hepatitis B virus (HBV) have been established at the 75th World Health Assembly, achieving global health impact with a significant reduction of new infections and mortality for the period 2022-2030 (2). HBV-related HCC refers to HCC caused by HBV, the main high-incidence area of which is the Asia-Pacific region, especially in China (3, 4). The pathogenesis is generally from the beginning of HBV infection, and then the occurrence of chronic hepatitis B (CHB), fibrosis, and cirrhosis, eventually leading to HCC. After HBV infection, the clinically common serum biomarkers include hepatitis B surface antigen (HBsAg), hepatitis B surface antibody, hepatitis B e antigen (HBeAg), hepatitis B e antibody, hepatitis B core antibody, and HBV DNA. As a new HBV infection biomarker, hepatitis B core-related antigen can still be detectable when HBV DNA level is undetectable or HBsAg is lost, because it is closely related to the presence of covalently closed circular DNA (cccDNA) in hepatocytes (5, 6). Hepatectomy is the main treatment strategy for early HCC, and even for advanced HCC combined with neoadjuvant therapy, adjuvant therapy, transcatheter arterial chemoembolization (TACE), and radiofrequency ablation (RFA). Besides the above biological indicators, numerous studies have focused on various preoperative and postoperative predictors to predict the prognosis of patients with feasible hepatectomy. This review summarizes various research results on preoperative and postoperative predictors of hepatectomy for HBV-related HCC over the past decade and previous landmark studies, including serology, molecular genomics, pathology, imaging, and other predictors (Tables 1–3), which are different from traditional factors of tumor status or liver function with the expectation of establishing correct disease prediction and guiding follow-up precise treatment.
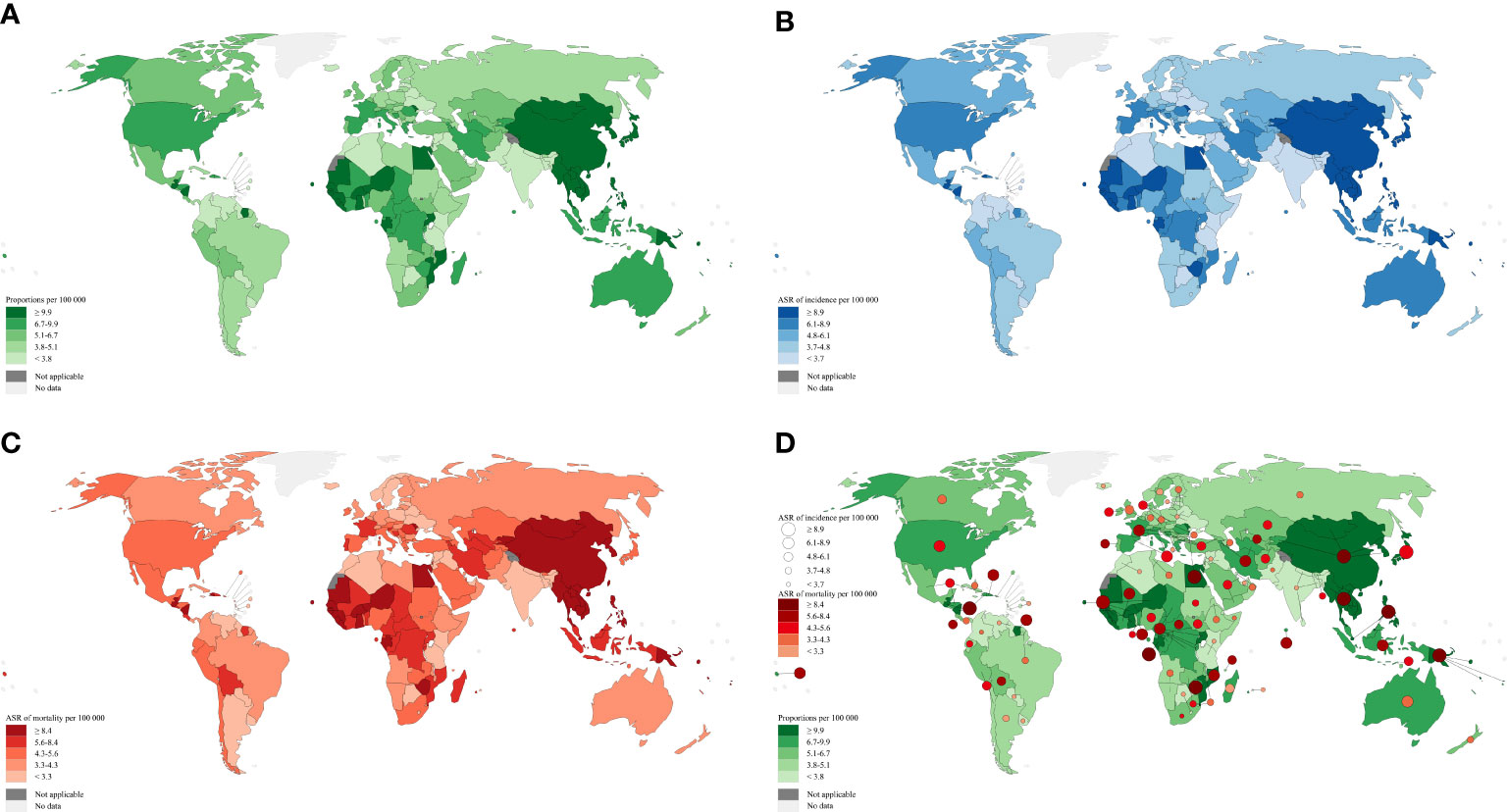
Figure 1 Global distribution map of liver cancer adapted from data source: GLOBOCAN 2020. Map production: IARC (http://gco.iarc.fr/today) World Health Organization. (A) Estimated number of prevalent cases (5-year) as a proportion in 2020. (B) Estimated age-standardized incidence rates in 2020. (C) Estimated age-standardized mortality rates in 2020. (D) Base map (A) + Size of the circle (B) + The color depth of circle (C).
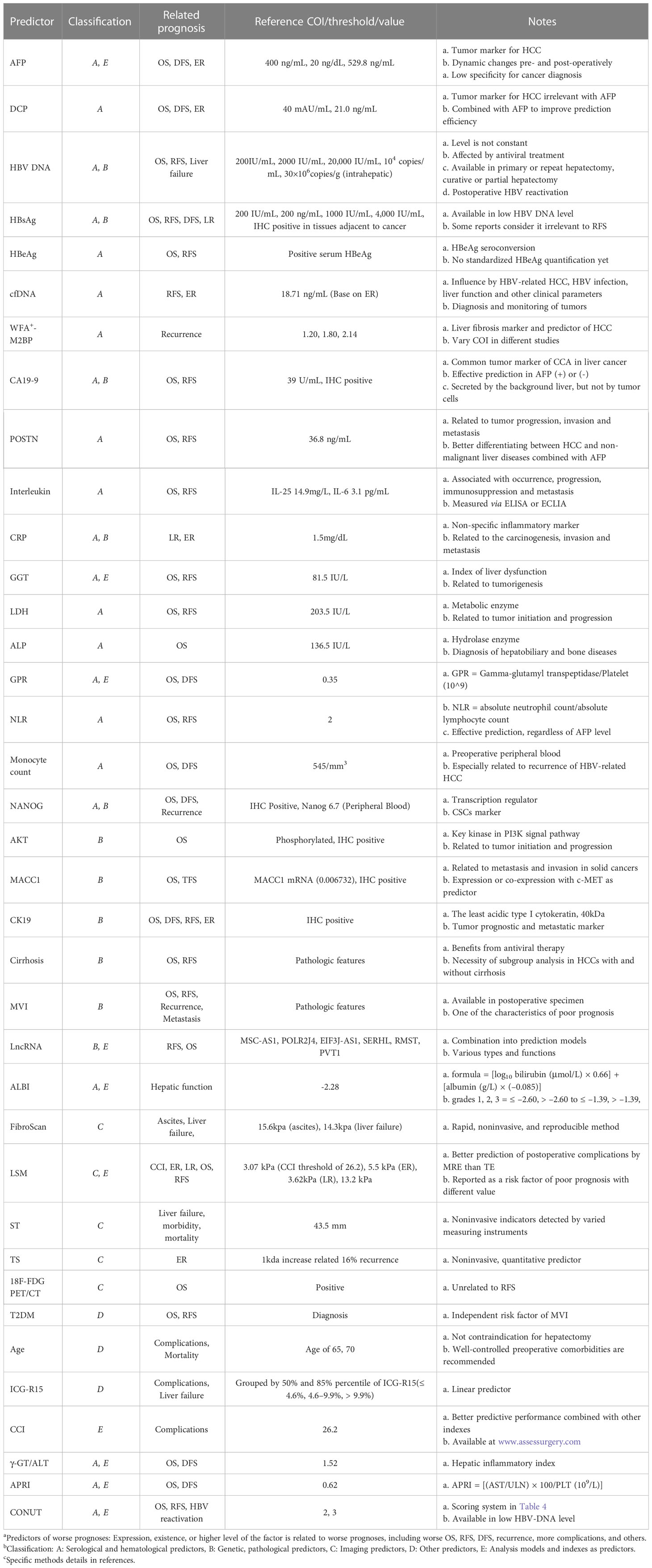
Table 1 Predictors of worse prognoses.
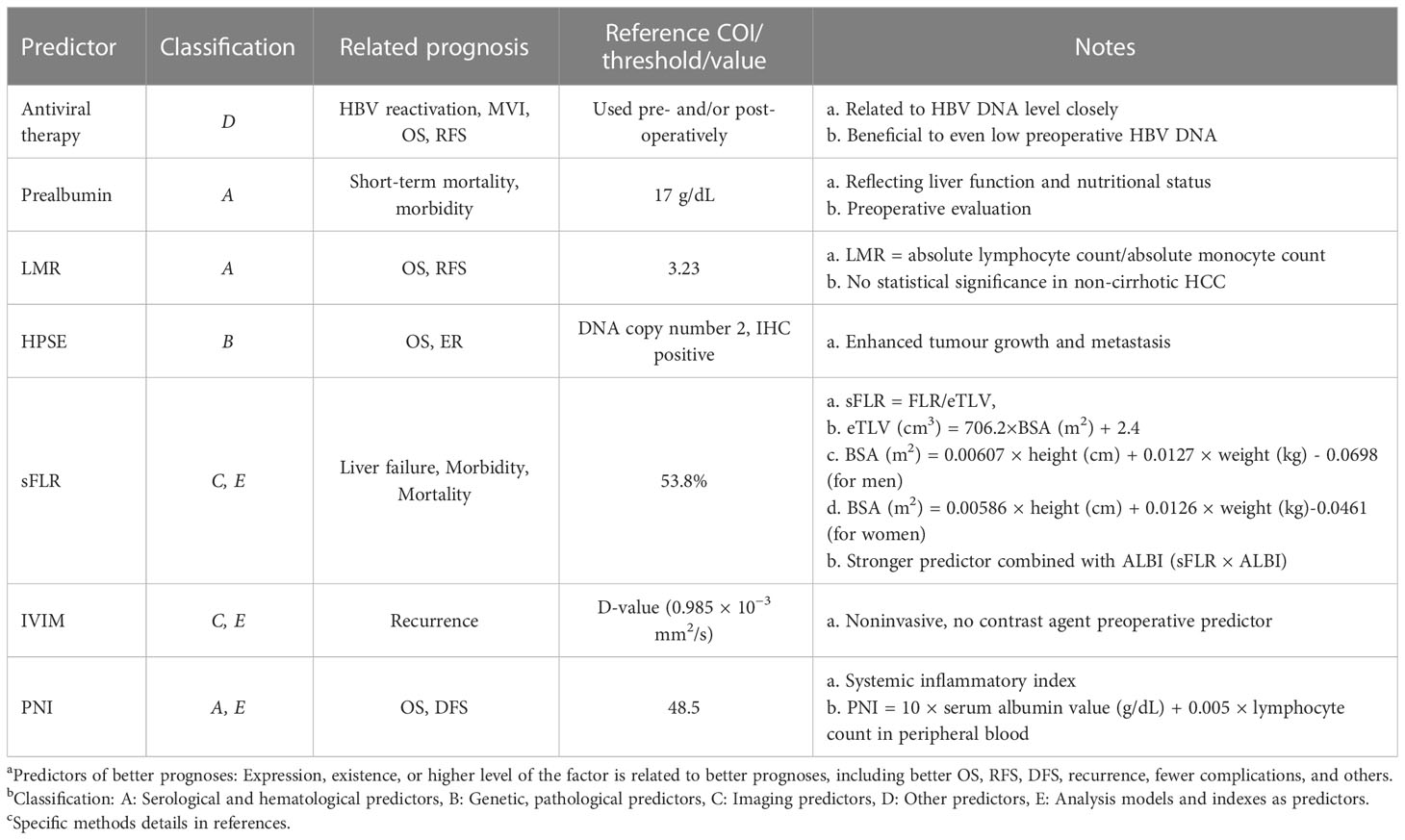
Table 2 Predictors of better prognoses.
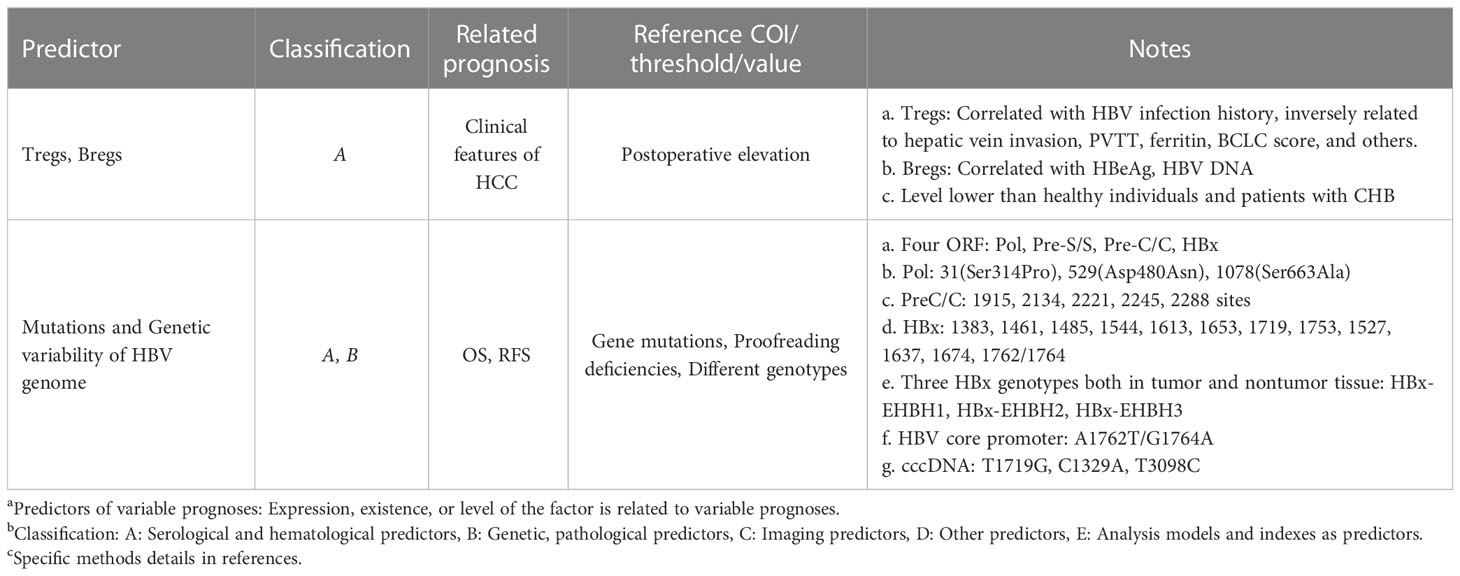
Table 3 Predictors of variable prognoses.
The pathogen of HBV belongs to the Hepadnaviridae family, with DNA as genetic material. The genetic material or components of HBV can be found in the infected individuals’ blood and liver tissue. The pathogenic mechanisms of HBV infection have been thoroughly researched (6, 7). The natural history of HBV-related HCC generally includes HBV infection, failure to trigger innate immunity, slow and weak adaptive immunity resulting in virus persistence, chronic hepatitis, fibrosis, cirrhosis, and eventually deterioration causing HCC (8).
Alpha-fetoprotein (AFP) is considered an important biomarker for early screening and diagnosis of HCC, so its prognosis prediction for hepatectomy is also of concern. Because of the dynamic changes in serum levels, AFP can serve as a stratification factor and prognostic predictor for treatment selection and recurrence prediction. A prospective study included 189 HBV-related HCC patients between 1995-2008 found that patients with preoperative AFP in the first quintile (1.4-4.1 ng/mL) had better overall survival (OS) and disease-free survival (DFS) than the other four groups (9). A retrospective study regarding 400 ng/mL as a cut-off value for AFP, demonstrated that AFP concentration higher than 400 ng/mL was an independent risk factor for shorter DFS and OS after HBV-related HCC hepatectomy, while its sensitivity and specificity were low (10).
In the surveillance and early diagnosis stage of HCC, des-γ-carboxy prothrombin (DCP) usually acts as a supplementary predictor to AFP (11). Given the low prognostic predictability of AFP, DCP can also be used as a complementary predictor of HBV-related HCC undergoing curative resection combined with AFP preoperatively. A retrospective analysis suggested that the AFP cut-off value for early recurrence (ER, within 2 years) after primary hepatectomy was 529.8 ng/mL, and DCP was 21.0 ng/mL (12). Another retrospective analysis suggested that high levels of AFP (≥20 ng/dL) and DCP (≥40 mAU/mL) were independent risk factors for tumor relapse and DFS in patients with HBV-related HCC after curative resection (13).
The detection of HBV DNA in serum is a significant biomarker of HBV infection and the most frequently used prognostic predictor of HBV-related HCC. Preoperative HBV DNA level [≥20,000 IU/mL (14), >104 copies/mL (15)] is associated with ER in patients with HBV-related HCC undergoing radical hepatectomy. The level of HBV DNA in patient’s serum often changes with the progression of the disease. Thus, the level of HBV DNA is not constant, which means that dynamic detection of HBV DNA level is meaningful. Analyzing HBV DNA levels before primary and repeated hepatectomies, a study found that when HCC relapses, low levels of HBV DNA suggest better prognoses, including primary and repeat hepatectomies (16). Preoperative low-level viremia (HBV DNA <2000 IU/mL) was associated with longer HCC recurrence intervals, and HBV DNA level ≥100 IU/mL was one of the independent risk factors for HBV-related HCC relapse (17). After hepatectomy for HBV-related HCC, HBV infection may persist in liver tissue, and liver dysfunction and even recurrence of liver cancer may occur. Preoperative HBV DNA level is related to the incidence of postoperative complications, especially the incidence of postoperative liver failure (18). Some research demonstrated that HBV-related HCC in patients with low preoperative HBV load (<2000 IU/mL) could emerge HBV reactivation after curative or partial hepatectomy (19, 20). In patients with HCC who underwent curative hepatectomy for non-cirrhotic liver, the prognosis of patients with HBV infection was worse than patients without HBV infection (21).
From the above studies, it can be inferred that preoperative use of antiviral therapy to reduce the preoperative HBV DNA level may be beneficial to improve the prognosis of patients with HBV-related HCC. A meta-analysis concluded that low viral load HBV-related HCC receiving antiviral therapy after curative hepatectomy could reduce viral reactivation and improve OS (22). HBV reactivation, which is associated with HCC recurrence, will occur in patients with HBV-related HCC after hepatectomy, even in those with undetectable HBV DNA before surgery. Therefore, some studies suggested that even if HBV DNA was not detected before surgery or HBV was reactivated after surgery, antiviral therapy should be used to reduce HBV reactivation and improve the prognosis after re-hepatectomy (23–25). In a multicenter retrospective study of patients with HBV-related HCC who underwent radical hepatectomy in China, it was suggested that postoperative antiviral therapy was an independent protective factor for 10-year survival rate (26). In addition to the direct effect of HBV on HCC progression, high serum HBV levels can also lead to poor outcomes in patients with HBV-related HCC by the association with microvascular invasion (MVI) (27). Antiviral therapy can be divided into preoperative and postoperative treatment. A retrospective cohort study suggested that a high preoperative HBV load is an independent risk factor for MVI, and that over 90 days of antiviral treatment before partial hepatectomy was associated with MVI reduction and lower early tumor recurrence rate (28). A randomized controlled trial demonstrated that after R0 hepatectomy for patients with preoperatively low serum HBV DNA (<2000 IU/mL), started receiving antiviral therapy (telbivudine tablets) 4-7 days after surgery could markedly reduce HCC recurrence (29).
Corresponding to HBV DNA, one of the multiple risk factors for late recurrence (LR, over 2 years) in patients with HBV-related HCC is preoperative HBsAg levels (≥4,000 IU/mL) (14). A retrospective analysis of 881 patients with HBV-related HCC who underwent curative hepatectomy, showed that preoperative and postoperative low level of HBsAg (<200 ng/mL) was correlated with better prognoses, while antiviral treatment might be beneficial to a high level of HBsAg (≥200 ng/mL) (30). Retrospective research in Taiwan suggested that HBsAg >200 IU/mL was an independent predictor of late recurrence (years 2 to 5), and HBsAg >50 IU/mL was an independent predictor of late mortality (over 5 years) (31). Meanwhile, HBsAg could serve as a monitor of antiviral therapeutic effect when HBV DNA level was low (<2000 IU/mL) (17). Original Investigation by Gang Huang, et al. demonstrated that preoperative serum HBsAg level over 1000 IU/mL was one of the independent risk factors for HCC recurrence in patients with low HBV DNA load (<200 IU/mL) receiving partial hepatectomy (32).
HBeAg seroconversion is common, and its quantification is not yet standardized (6). HBeAg level can also be down-regulated by peginterferon treatment and can be served as an efficacy indicator of the latter (33). Thus, the rate of HBeAg-positive patients with HCC is not high after a long progression from HBV infection. Nevertheless, a propensity score matching analysis about HCC undergoing hepatectomy and serum HBeAg suggested that positive serum HBeAg had a negative impact on tumor relapse and long-term survival (34).
Other detectable indicators in the blood may serve as preoperative and postoperative predictors, apart from the HBV particle component. Circulating cell-free DNA (cfDNA), which is highly fragmented DNA, exists in human blood circulation and is free from cells. Many studies have shown that the concentration of cfDNA was higher in the blood of cancer patients compared with healthy individuals (35), and a later study suggested that total plasma cfDNA levels could be used as a biomarker to predict ER of HBV-related HCC (36).
Studies have reported that Wisteria floribunda agglutinin-positive Mac-2-binding protein (WFA+-M2BP) was highly correlated with the development of hepatocellular carcinoma after HBV infection, whether or not receiving nucleos(t)ide analogues treatment (37, 38). A study from Korea showed that postoperative serum WFA+-M2BP was an independent risk factor of HBV-related HCC recurrence after curative hepatectomy, with cut-off value 2.14 obtaining maximized sensitivity and specificity (area under receiver operating characteristic curve, AUC = 0.632, P = 0.010) (39).
Carbohydrate antigen 19-9 (CA19-9) is generally considered a tumor marker of cholangiocarcinoma (CCA) (40). A study targeting HCC suggested that CA19-9 ≥39 U/mL predicted worse OS and RFS regardless of whether AFP was positive or negative in HBV-related HCC patients who underwent curative resection (41). Elevated CA19-9 levels in patients with HCC are a rare and interesting occurrence, as it is more common in cholangiocarcinoma, which is also a type of primary liver cancer. A recent study found that combined hepatocellular-cholangiocarcinoma (cHCC-CCA) is a rare primary liver cancer with clinical and pathological features of HCC and CCA (42). Half of cHCC-CCAs a may be misclassified as HCC. When CA19-9 levels are elevated, it is necessary to distinguish between HCC, CCA, or cHCC-CCA. Therefore, the predictive role and diagnostic value of CA19-9 cannot be ignored in clinical practice.
Periostin (POSTN) is an extracellular matrix protein. In addition to being related to allergic diseases and inflammatory diseases, more and more studies have shown that POSTN is abnormally expressed in a variety of cancers and related to the invasion and metastasis of tumor cells (43–45). Preoperative serum POSTN measured by enzyme-linked immunosorbent assay (ELISA) showed that high-level serum POSTN was associated with HCC progression and can serve as an independent worse prognostic predictor for OS and RFS (46). Detecting POSTN expression levels through immunohistochemistry (IHC) staining can reveal similar results, and combined with microvascular invasion can serve as an independent predictor for prognosis (47).
Members of the interleukin family are a class of cytokines produced by and act on a variety of cells in many ways. Studies indicated that abnormal expression of interleukin family members was associated with HBV-related HCC in initiation, progression, immunosuppression, and metastasis (48–50). A study that enrolled consecutive patients with HBV-related HCC who underwent hepatectomy from 2008 to 2015 suggested that IL-25 level ≥14.9 mg/L was an independent preoperative predictor of worse OS and RFS after liver surgery (51). Preoperative serum IL-6 level above 3.1 pg/mL was related to lower OS and RFS rates. When the level exceeded 3.7 pg/mL, a saturation effect occurred (52).
There are some other routine serological indicators tested before hepatectomy. C-reactive protein (CRP) is a non-specific inflammatory marker. Studies have shown that CRP overexpression verified by ELISA and IHC was related to the carcinogenesis, invasion, and metastasis of HBV-related liver cancer (53, 54). A retrospective study suggested that, in patients with HBV-related HCC, the saturation effect for preoperative serum CRP existed in 2.1 mg/dL, and the best cut-off value for CRP predicting ER and LR was 1.5 mg/dL (55).
Prealbumin, a small, short half-life protein synthesized by hepatocytes, is more sensitive than albumin when hepatocytes are damaged. An analysis from a Chinese multicenter database showed that patients in a group with low preoperative serum prealbumin level (17 mg/dL as cut-off value) had higher postoperative morbidity, mortality, and hepatic insufficiency (56).
A retrospective analysis for HBV-related HCC underwent curative liver resection found that gamma-glutamyl transpeptidase (GGT) and lactate dehydrogenase (LDH) were important independent prognostic factors of OS and RFS, while alkaline phosphatase (ALP) was an important independent predictor of OS, not RFS, with cut-off value 81.5 IU/L, 203.5 IU/L, 136.5 IU/L, respectively (57).
The gamma-glutamyl transpeptidase to platelet ratio (GPR) has been reported as an accurate non-invasive predictor for HCC development in patients with HBV infection (58). Combined with the preoperative serum fibrinogen index, GPR could better predict the prognosis of HBV-related HCC underwent hepatectomy as an effective non-invasive predictor (59).
As one of the most important organs in human blood circulation, the physiological function of the liver can be reflected in routine blood examinations. A meta-analysis including 17 studies demonstrated that preoperative Neutrophil-Lymphocyte ratio (NLR, the ratio of absolute neutrophil count to absolute lymphocyte count) was highly correlated with the prognosis of HCC (60). A report showed that preoperative peripheral NLR >2 was an independent risk factor of worse OS and DFS for patients with HBV-related HCC, regardless APF is normal or not (61).
As a parameter for evaluating inflammation in routine blood tests, high-level preoperative peripheral blood monocyte (≥545/mm3) has been reported as an independent risk factor for HCC undergoing hepatectomy, especially with HBV infection (62). Combined with absolute peripheral blood lymphocyte and monocyte counts, a low preoperative lymphocyte-to-monocyte ratio (LMR, <3.23) has been proven to serve as an independent prognostic factor in patients with HBV-related HCC who received curative resection (63).
A case-controlled study enrolled 36 patients with HCC, six patients with CHB as a control group, demonstrated that frequencies of peripheral regulatory T cells (Tregs) and regulatory B cells (Bregs) uplifted after liver resection. The research suggested that anti-Tregs and anti-Bregs combination treatments could improve the postoperative prognosis of HBV-related HCC (64).
Various test samples and indicators of HBV-related HCC patients are available clinically. The genetic and pathological factors can serve as predictors besides the indicators in serum (65).
The HBV genome encodes the following four proteins with overlapping open reading frames (ORF): the viral polymerase (Pol), the envelope protein (Pre-S/S), the core protein (Pre-C/C), and a multifunctional nonstructural protein called X (HBx) (7, 66, 67). Previous studies have confirmed that proofreading deficiencies of the HBV genome affect the occurrence, development, and prognosis of HBV-related HCC. The mutations at sites 31(Ser314Pro), 529(Asp480Asn), and 1078(Ser663Ala) in Pol were identified as independent predictors of survival in patients with HBV-related HCC after hepatectomy (68). The mutations of the PreC/C region at 1915, 2134, 2221, 2245, and 2288 sites have been reported as significant independent predictors of worse survival in patients with HCC who underwent tumor resection. Similar mutations related to postoperative survival in HCC were also present in the X gene (69, 70). A variety of HBX gene sequences that encode a 17kDa protein have been observed. A study by Qing-guo Xu, Hui Liu et al. demonstrated that three new genotypes, HBx-EHBH1 (HBx-E1), HBx-EHBH2 (HBx-E2), and HBx-EHBH3 (HBx-E3) could be identified in both the tumor and non-tumor tissues for patients with HBV-related HCC after liver resection. Among these genotypes, HBx-E2 detected from tissue or serum predicted better prognoses of patients with the intermediate stage (Barcelona Clinic Liver Cancer, BCLC stage B) HCC (71).
Another study analyzed HBV DNA in noncancerous part of HBV-related HCC tissue after tumorectomy and found that HBV basal core promoter mutation, like A1762T/G1764A mutation, as well as the amount of HBV DNA, were independent predictors for both OS and RFS (72).
The genetic material relaxed circular DNA (rcDNA) in the HBV nucleocapsid which exists in the cytoplasm is repaired to cccDNA after being transported into the nucleus as an episomal transcriptional template (7). The full-length cccDNA sequences of tumor and non-tumor tissues in HBV-related HCC patients from liver biopsy samples found that mutations T1719G, C1329A, and T3098C were related to different survival after surgery (73).
Long non-coding RNA (lncRNA) is a non-coding RNA with a length of more than 200 nucleotides, which is a research hotspot in epigenetics and oncology over the past decade. Studies have demonstrated the potential of lncRNAs as biomarkers for predicting and diagnosing HBV-related HCC and therapeutic targets (74, 75). A study based on Gene Expression Omnibus and The Cancer Genome Atlas databases constructed a prognostic nomogram combining the lncRNA signature and clinical characteristics showed that risk model with MSC-AS1, POLR2J4, EIF3J-AS1, SERHL, RMST, and PVT1 upregulated in HBV-related HCC tissues was significantly correlated with poor RFS (76).
In patients with HCC after a long period of HBV infection, the HBsAg level in serum does not remain unchanged because of seroclearance. There is a question as to whether HBsAg exists in tumor tissue or liver tissue, which can serve as a stable index. A study testing HBsAg expression by IHC in liver tissue microarrays which collected tissue approximately 2 cm away from the tumor after hepatectomy suggested that the HBsAg-positive group had a better OS than the negative group, but RFS was not statistically significant. HBsAg expression in liver tissue was an independent risk factor for patients with HBV-related HCC who underwent surgery (77).
AKT, a key kinase in PI3K signal pathway, is an important protein in cancer initiation and progression, so it is often used as an indicator in cancer research (78, 79). A study on double mutation A1762T/G1764A (TA) combined with other mutation(s) (TACO) and AKT showed that overexpression of TACO in HBV genome core promoter and phosphorylated AKT (pAKT) in HBV-related HCC tissues were independent predictors of poor prognosis after hepatectomy (80).
NANOG is a critical transcription regulator of embryonic stem (ES) cells with self-renewal and multilineage differentiation (81). Cancer stem cells (CSCs) share similar features with ES cells. Thus, NANOG has been reported to play an important role in CSCs’ abilities of stemness, unlimited self-renewal, metastasis, invasiveness, angiogenesis, and drug resistance (82). Numbers of NANOG-positive cells measured in peripheral blood (Nanog >6.7) and HCC tissues (positive-IHC) from patients, 90% of whom with HBV infection, showed a positive correlation to the worse prognosis for HCC patients after R0 resection (83).
High expression of heparinase (HPSE) has been reported in a variety of cancers and is also regarded as a significant regulator in the tumor microenvironment (84). The loss of heterozygosity, mRNA level, and protein expression of HPSE detected by SNP microarray, quantificational reverse transcription-polymerase chain reaction, and IHC, respectively, demonstrated that genetic alteration and decrease of HPSE expression were related to the poor outcome of HBV-related HCC (85).
As the term suggests, metastasis-associated in colon cancer 1 (MACC1) is generally correlated with the metastasis of colon cancer. Nevertheless, MACC1 has been reported to be associated with metastasis and invasion in multiple solid cancers after a decade of research (86–88). A retrospective study enrolled 354 patients with HBV-related HCC who underwent surgical resection and suggested that a high expression level of MACC1 in the tumor was correlated with poor prognosis and progression of HCC (89).
Cytokeratin 19 (CK19), with a molecular weight of 40kDa, is the least acidic type I cytokeratins (CKs) which has been considered a tumor prognostic and metastatic marker in varied cancers (90). A meta-analysis including 17 studies with 2943 patients showed that CK19 overexpression which was detected by IHC or IHC plus tissue microarrays was associated with HCC early recurrence and lower survival rate (91). A retrospective study based on two institutions’ data plotted nomogram of 2-year RFS and analyzed survival risk factors by Cox regression model showed that CK19 expression in tumor tissue detected by IHC after hepatectomy was an independent adverse factor for HBV-related HCC recurrence (92).
Liver cirrhosis is not inevitable in the development of HBV-related HCC. A study using the modified Ishak method to evaluate liver fibrosis of HBV-related HCC specimens after hepatectomy demonstrated that cirrhosis (Ishak stage 6) was an independent predictor of worse OS and RFS (93, 94). A long-term single-center follow-up study conducted in Japan from 1995 to 2013 showed differences in prognostic factors between HCC with cirrhosis (HCC-C) and HCC without cirrhosis (HCC-NC), and it was recommended an emphasis subgroup analysis of the two to achieve individualized treatment. The analysis suggested that the long-term prognosis of HCC-NC patients was better than that of HCC-C patients, and anti-viral therapy might be beneficial to HCC, especially HCC-C patients (95).
Microvascular invasion (MVI) generally is regarded as a predictor that reflects the tendency of invasion and metastasis causing recurrence or distant metastasis of HCC (96). A multicenter study from China that included 1517 HCC patients with MVI showed that the actual 5-year survival rate is 33% after hepatectomy, and some patients received other treatments after surgery (97). Another retrospective study from China included 2,508 patients with a solitary HBV-related HCC, suggesting that a wide resection margin is conducive to a better long-term prognosis for 929 patients with MVI (98). Because MVI can only be clearly diagnosed in postoperative specimens at present, follow-up treatment is necessary to improve long-term survival. Research about recurrent HBV-related HCC demonstrated that MVI (–) patients receiving re-resection or RFA could obtain longer survival than TACE, while no difference in MVI (+) patients (99).
With the development of imaging techniques and instruments, such non-invasive methods have been playing important roles in predicting the prognosis of patients preoperatively and postoperatively. Primary liver cancer is a type of cancer that can be clearly diagnosed through imaging and clinical manifestations in order to enter the treatment process as soon as possible. Therefore, imaging-related factors are important predictors that cannot be overlooked.
Computed Tomography, abbreviated as CT, is a commonly utilized imaging method for HCC diagnosis. A retrospective study enrolled 229 patients with three-dimensional CT reconstruction before curative hepatectomy demonstrated that albumin-bilirubin (ALBI) grade, which had been reported as a new assessment tool for hepatic function (100, 101), combined with standardized future liver remnant (sFLR) measured by CT could better predict prognosis of HBV-related HCC than separate indicators (102).
Liver ultrasound (US) combined with AFP are common methods for early screening and diagnosis of HCC. As a non-invasive ultrasonic examination, transient elastography (TE) is often used to measure liver fibrosis, cirrhosis, and stiffness, which are important reference factors for determining whether surgery can be performed and evaluating the possibility of liver failure after surgery. A prospective study applied TE assessed by FibroScan demonstrated that FibroScan value one week before surgery was an independent risk factor for predicting postoperative ascites, and liver failure, with a best cut-off value of 15.6 kpa, and 14.3 kpa, respectively (103). Besides liver stiffness measurement (LSM), a retrospective analysis found that splenic thickness (ST) measured by US was significantly associated with post-hepatectomy liver failure and an independent risk factor of postoperative morbidity and mortality in patients with HBV-related HCC (104).
It is reported that another implication for LSM by magnetic resonance elastography (MRE) based on magnetic resonance imaging (MRI) has better performance in detecting fibrosis and better postoperative prediction (evaluated by comprehensive complication index, CCI) in HCC than TE (105). A prospective study that collected HCC patients who were under Milan criteria and received MRE before treatment, including hepatectomy, RFA, or TACE showed that LSM by MRE could serve as an independent predictor of ER in patients with HCC under Milan criteria after treatment (106). LSM by MRE as a parameter of preoperative and postoperative prediction models for ER indicated a good predictive performance and served as an independent predictor of LR in HBV-related hepatocellular carcinoma patients (107). A study enrolling 263 patients with HBV-related HCC who underwent curative resection suggested that preoperative LSM ≥13.2 kPa was an independent risk factor causing worse OS and RFS (108). Another prospective study measured HCC tumor stiffness (TS) measured by MRE in patients with HBV infection before hepatectomy (median:6 days, range:1-30 days) suggested that TS and vascular invasion were risk factors of HCC ER analyzed by the multivariate Cox proportional hazard model (109). Intravoxel incoherent motion (IVIM) is a derivative model of diffusion-weighted imaging, which can assess water molecule diffusion and blood perfusion, and display both perfusion and diffusion information at the same time. Because no contrast medium is required, IVIM-based MRI has become a research hotspot in the imaging field related to tumors in recent years (110). D-value (true diffusion coefficient, <0.985 × 10−3 mm2/s) of tumors in HBV-related HCC patients obtained from preoperative IVIM models was reported as a risk factor for tumor recurrence after hepatectomy (111).
Positron emission tomography/computed tomography (PET/CT) is a combination of PET and CT, using F-18-fluoro-2-deoxy-glucose (18F-FDG) to reflect cellular metabolism, which can be used to diagnose tumors, neoplasm staging, and discover metastases. Studies have suggested that 18F-FDG PET/CT could be beneficial to the diagnosis of HCC metastasis and recurrence (112). Appropriate consistency of PET and CT texture features as 18F-FDG PET/CT radiomics signature could serve as an independent marker for estimation of MVI and DFS in patients with very-early- and early-stage HCC (113). A study involving patients with HBV-related HCC who received 18F-FDG PET/CT detection preoperatively between 2007 to 2014 showed that positive result is not related to recurrence but better OS (114).
In addition to various examination indexes, the patient’s general condition and basic characteristics before surgery are also effective predictors for preoperative evaluation of operation risk and prognosis, preoperative antiviral treatment mentioned above for instance.
It is generally acknowledged that MVI is a risk factor for metastatic tumor recurrence in HBV-related HCC leading to poor prognosis (96). A multicenter retrospective study in China found that HBV-associated HCC patients with type 2 diabetes mellitus (T2DM) had a higher risk of MVI occurrence, while non-T2DM patients had better OS and RFS (115). Since MVI can be only defined in postoperative specimens at present, incorporating preoperative T2DM evaluation is beneficial for establishing earlier predictive models and improving surgical protocols.
The age of HCC patients is also one of the important characteristics to predict the prognosis. A study enrolled HCC patients who underwent hepatectomy at Sun Yat-sen University Cancer Center from 1983 to 2006 suggested that HCC in the elderly (≥70 years) was less associated with HBV, less advanced, and less aggressive, compared with younger patients. Furthermore, the study concluded that pathological tumor-node-metastasis staging was the only independent predictor of OS in the elderly (116). Another retrospective study with a cut-off age of 65 years showed that compared with younger patients (<65 years), the elderly patients with HBV-related HCC had lower positive rates of serum HBsAg and HBeAg, lower levels of HBV DNA, but similar morbidity and levels of complications (117). Therefore, the above research indicated that age should not be considered a contraindication of hepatectomy. Hepatectomy is a safe and effective treatment for elderly patients without or with controllable complications before surgery.
The indocyanine green retention rate at 15 min (ICG-R15) is widely used in the clinic to evaluate liver function reserve before hepatectomy (118). A retrospective study that enrolled 354 HBV-related HCC patients who underwent initial hepatectomy suggested that preoperative ICG-R15 could better assess postoperative major complications and severe post-hepatectomy liver failure than Child-Pugh, MELD, and ALBI scores (119).
In addition to a single factor, some studies have found that analysis models or indexes combined with multiple single factors can better predict the prognosis of HBV-related HCC. This review adopts the relevant evaluation models, scoring models, and indexes that have been widely approved and applied.
Comprehensive Complication Index (CCI), which is based on the Clavien-Dindo classification (120) (www.assessurgery.com) can serve as an evaluation index combining all postoperative complications (121). A multicenter retrospective study suggested that models based on preoperative and postoperative CCI combined with other parameters could establish a more accurate prediction statistical model for patients with HBV-related HCC (122).
Systemic and hepatic inflammatory biomarkers have been reported as potential prognostic predictors for HBV-related HCCs. A study of systemic inflammatory markers and hepatic inflammatory markers, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), Prognostic Nutritional Index (PNI) (123), and aspartate aminotransferase-to-platelet ratio index (APRI), γ-glutamyl transferase (γ-GT)/alanine aminotransferase (ALT), respectively, showed that PNI and γ-GT/ALT were independent predictors of prognosis in patients with HBV-related HCC (124). (Formulations shown in Table 1, 2) The inflammation biomarkers mentioned above contain multiple indexes including platelet. Abnormal changes in peripheral platelet are usually correlated with liver diseases. A retrospective study of platelet-based indexes, including platelet count, PLR, and especially APRI indicated that the elevation of platelet-related inflammatory indicators was associated with cirrhosis and HBV infection, predicting worse OS and DFS (125).
The controlling nutritional status (COUNT) score is a scoring model for nutritional status proposed in 2005 by combining serum albumin, total cholesterol concentration, and total lymphocyte count (126). COUNT score is used to predict the prognosis of various tumors. Due to the included parameters related to liver nutritional function and HBV infection, COUNT can effectively serve as a prognostic factor for HBV-related HCC. It was reported that the preoperative COUNT score was a significant independent predictor of OS and an effective indicator of postoperative HBV reactivation in patients with HBV-related HCC (127, 128) (scoring system shown in Table 4).

Table 4 COUNT scoring system.
The main risk factors for HCC include chronic viral infections (HBV, HCV, HIV), metabolic risk factors (metabolic syndrome, obesity, type II diabetes, and non-alcoholic fatty liver disease), consumption of aflatoxin-contaminated foods, and smoking (1, 129, 130). In addition to HBV-related HCC, HCV-related HCC, and metabolism-related HCC also account for a large proportion and have significant global and regional distribution differences. Therefore, in the prevention and treatment strategies of HCC, it is essential to comprehend the prognostic predictors of HCC related to other risk factors.
Hepatitis C virus (HCV) is a major type of hepatitis, along with HBV, have been targeted in global health sector strategies for the period 2022-2030 (2). According to WHO statistics, an estimated 58 million people worldwide are infected with HCV. In 2019, about 290 000 people died from HCV, mainly due to cirrhosis and HCV-related HCC.
Numerous studies have shown that high HCV viral titer is associated with poor prognoses of HCV-related HCC (131, 132), which is similar to the relationship between HBV and HCC. HCV genotypes and serological clearance or not were reported to be unrelated to the long-term outcome of HCC (132, 133). WHO estimated about 15%-45% of individuals infected with HCV could occur spontaneous clearance without treatment. Unlike HBV, HCV is an RNA virus, which has a distinguished virus amplification mechanism. Therefore, the recommended antiviral therapy for HCV is direct-acting antiviral agents (DAAs). DAAs can result in nearly 100% sustained virological response (SVR), compared with approximately 50% with interferon-based treatments (134). Whether SVR is achieved preoperatively or postoperatively, it is associated with better prognoses of HCV-related HCC (135, 136). Further research suggested that preoperative SVR is more beneficial than postoperative SVR, with similar surgical outcomes but better postoperative liver function (137–139).
HCV-related HCC and HCV-related HCC have common prognosis predictors, such as AFP, DCP, fibrosis, cirrhosis, and diabetes mellitus (12, 140, 141). However, due to differences in tumor biology and characteristics baseline, the specific prediction results of predictors are not the same leading to different prognoses (142, 143). Therefore, in the study and treatment of HCC, patients with hepatitis virus infection need to be clearly classified and subgroup analyzed.
Non-HBV non-HCV HCC (NBNC-HCC) refers to patients with HCC who have not detected biomarkers of HBV and HCV, respectively, negative HBsAg and hepatitis C antibody (HCVAb) (144). NBNC-HCC commonly progress from non−alcoholic fatty liver disease (NAFLD), non−alcoholic steatohepatitis (NASH, a severe form of NAFLD), alcoholic liver disease (caused by heavy alcohol intake), exposure risk factors (such as aflatoxin, smoking) and other etiologies (such as primary biliary cirrhosis, autoimmune hepatitis, Wilson disease, Budd-Chiari syndrome) (1, 145).
The common cause of NBNC-HCC in high-income countries is NAFLD, of which the primary risk factor is metabolic syndrome including central obesity, dyslipidemia, hypertension, and diabetes mellitus (146, 147). During surgical treatment, a stable metabolic state is a crucial factor in the perioperative period. A retrospective study about major liver resection suggested that metabolic disorders would increase the risk of perioperative death in HCC patients (148). Meanwhile, HCC patients with metabolic syndrome have specific risks of postoperative complications and long-term survival benefits after surgery which means the necessity of perioperative regulation (149, 150). COUNT scoring system can also be an independent predictor of NBNC-HCC with ≥4 meaning worse OS and RFS (151). Compared with HBV-related and HCV-related HCC, although NBNC-HCC has different tumor characteristics and may have advanced tumors, DCP can serve as a diagnostic and prognostic predictor on both sides (152, 153).
A community-based prospective longitudinal study in Taiwan which is an HBV-endemic and HCV-endemic area found that high-level triglyceride (>150 mg/dL) was a decreased risk factor for HCC (154). A Subgroup Analysis of HCC patients grouped with HBV-related HCC (HBsAg+), HBV-related HCC (HCVAb+), NBNC-related HCC (HBcAb+), and pure NBNC-related HCC demonstrated that NBNC-related HCC patients with a history of HBV infection might have better survival than other groups (155). A multicenter retrospective study in France demonstrated that in NBNC-HCC patients with non-cirrhotic liver, stratified prediction can be performed based on the number (≤2 or >2) and size (≤10 or >10 cm, if less than 2 nodules) of nodules, with the potential to expand the range of patients who can undergo surgery (156). NBNC-HCC has a higher incidence rate in developed countries, which is related to the regional economy, diet, and medical level. With the popularization of vaccination and the development of the economy and medical treatment, the infection rates of HBV and HCV in some countries and regions have gradually decreased. At the same time, greater consideration should be given to NBNC-HCC.
With the development of artificial intelligence (AI), more and more AI technologies are being applied in medical and health services. For example, using omics data, machine learning (ML) and deep learning (DL) are used to predict metastasis (157). AI has been widely reported in the early diagnosis of HCC, such as the prediction model of HBV reverse transcriptase sequence combined with ML, establishing genome-wide interrogation of somatic copy number aberrations by ML as a non-invasive HCC detection, combining B-mode ultrasound with DL to identify AFP negative HCC (158–160). In terms of prognosis, artificial neural network model is helpful to preoperatively evaluate the HCC patients’ risk of liver failure and predict life quality after hepatectomy (161, 162). Based on DL of HCC pathological sections, new histological scoring methods can be established to predict tumor recurrence (163, 164). The combination of ML and CT radiomics can also predict the recurrence and MVI in solitary HCC (165, 166). Besides HBV-related HCC, ML can also be used to predict the risk of HCV-related HCC, assess DAA treatment for HCV, screen NAFLD in the general population, and select appropriate patients undergoing hepatectomy to replace liver transplantation (167–170).
Primary liver cancer is one of the most common cancers in the world, with approximately 75% - 85% of cases being HCCs (1). Cases of HCC caused by HBV infection are common in HBV-endemic areas, including East Asia, Southeast Asia, and countries in the south of the Sahara Desert, most of which are low- and middle-income countries. The current situation is closely related to the living habits of local people, regional economy and health levels. As a remarkable example, China, a region with a high prevalence of HBV and a high incidence of HCC, has benefited from the popularization of HBV vaccination since the 1990s and the HBV infection rate among millennials declined significantly. For the foreseeable future, it is expected that patients with HBV-related HCC in similar countries and regions will decrease with vaccine popularity, which is in line with global health sector strategies on viral hepatitis. In addition to early prevention, early diagnosis and treatment of HBV-related HCC are vital. Hepatectomy is the primary treatment method for early- and middle-stage HCC. Meanwhile, many clinical trials are conducted to convert resectable tumors from advanced HCC. Therefore, it is essential to assess the prognosis of patients with HBV-related HCC who are scheduled for surgical treatment during the perioperative period in order to establish correct disease expectations and develop personalized therapy.
Clinical applications tend to favor predictors that are simple, fast, and non-invasive. Indicators commonly used to predict the prognosis of HBV-related HCC, such as AFP and HBV DNA level in serum, imaging results by US and CT. Unfortunately, to our best knowledge, most predictors in various studies do not have standardized thresholds which may be related to individual characteristics, dynamic changes in disease, or perioperative differences. This situation implies that it is impossible to establish a simple prediction model for HBV-related HCC after hepatectomy. This review covers the research on the preoperative and postoperative predictors of HBV-related HCC after hepatectomy over the past decade. Researchers have studied more extensive numbers and types of predictors, including unconventional blood test factors, genetic and pathological predictors, and other predictors. Factors such as population differences, regional medical level differences, dynamic changes of various indicators, and mass medical data on the disease process are obstacles to accurately predicting the prognosis of HBV-related liver cancer after hepatectomy.
A variety of HCC prognostic systems have been proposed internationally, focusing on liver function, tumor size, lymph node metastasis, and distant metastasis. Commonly used in clinical practice include Barcelona Clinic Liver Cancer (BCLC) staging, United Network for Organ Sharing (UNOS) tumor node metastases (TNM) staging, Hong Kong Liver Cancer (HKLC) staging, and American Joint Committee on Cancer (AJCC) TNM staging. These evaluation standards have been applicable to a large number of clinical practices. These staging systems are significantly correlated with prognosis. However, prognosis is also influenced by other factors such as overall health status of the patient, pathological characteristics of tumors, and serum tumor marker levels. These factors further affect prognosis assessment and follow-up treatment choices in HCC patients. Only through a thorough evaluation can the prognosis of patients be accurately predicted and realized precise medicine. To sum up, it is important to study other factors that can influence prognosis due to the following reasons: 1. Limitations of staging: While staging systems provide valuable information about the tumor, they may not encompass all factors that can impact prognosis. Other factors such as overall health condition of the patient, tumor differentiation, pathological characteristics of tumors, and tumor marker levels, can also influence the prognosis. 2. Individual variations: HCC is a highly heterogeneous tumor, and patients can exhibit significant differences in disease characteristics and biological behavior. Therefore, relying solely on staging systems may not accurately predict the prognosis for each patient. Studying other factors can help better understand the specific circumstances of individual patients and provide a more accurate assessment of their prognosis. 3. Diverse treatment strategies: HCC can be treated through various methods including surgical resection, liver transplantation, radiofrequency ablation, radiation therapy, chemotherapy, etc. The impact of different treatment modalities on prognosis may vary depending on the patient’s disease characteristics and staging. Hence, studying other factors can help determine the optimal treatment strategy for achieving a better prognosis. 4. Personalized prognosis: HCC is a highly personalized disease, and the prognosis can differ for each patient. By studying other factors that influence prognosis, it becomes possible to provide patients with more personalized treatment and care, thereby improving their survival rates and quality of life.
In our opinions, single or several predictive factors or a fixed model in the past do not meet the trend of personalized and precise medicine in the future. We want to establish a prediction system beyond traditional staging-related factors. Incorporating more dimensional parameters for personalized prediction is a significant foundation for achieving personalized and precise medicine. The development of AI technology and its gradual application in the medical field may provide a solution to the above issues. AI has been used to predict metastasis and tumor recurrence, as well as evaluate the HCC patients’ risk of liver failure and life quality after hepatectomy (157, 161–164). It is expected that AI will become more widely used in the medical field and that the difficulties that hinder the establishment of the prediction model of prognosis in the perioperative period will be overcome within a few years. Our research aims to incorporate factors other than commonly used tumor status and liver function, such as HBV DNA, HBsAg, multiple tumor pathological features, imaging features, etc., and utilize big biological data and AI to make more accurate predictions and provide follow-up treatment plans. In the foreseeable future, more extensive and in-depth cooperation among medical institutions, regions, and even countries will be needed.
To our best knowledge, the relevant studies in a decade adopted in this review are summarized in Tables 1–4, and Figure 2. As we all know, there are plenty of preoperative and postoperative factors that can be served as prognostic predictors, but some predictors have no standardized threshold. This situation may be related to the endemic distribution characteristics of HBV-related HCC, which are affected by biological characteristics (e.g., race, HBV genotype), as well as economic, medical (e.g., vaccination, linkage to care), and other factors. With the development and application of big biological data and AI, we expect that future medicine can conduct big data research in combination with various preoperative and postoperative predictors of HBV-related HCC, reasonably use AI to make more accurate prognosis prediction, establish correct disease expectations, and guide precise medicine. Achieving this goal requires a wide range of regions, a large number of medical institutions, and medical personnel to work together, which is a small step toward promoting human health.
Figure 2 Various preoperative and postoperative predictors for the prognosis of HBV-related HCC.
Conception and design: ZH, DT. Collection, analysis and writing: ZH. Review and modification: DT. All authors contributed to the article and approved the submitted version.
This work was supported by Science, Technology and Innovation Commission of Shenzhen Municipality (JCYJ20220530144615034).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.

1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Global health sector strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections for the period 2022-2030. Geneva: World Health Organization (2022).
3. Xie DY, Ren ZG, Zhou J, Fan J, Gao Q. 2019 Chinese Clinical guidelines for the management of hepatocellular carcinoma: updates and insights. Hepatobil Surg Nutr (2020) 9(4):452–63. doi: 10.21037/hbsn-20-480
4. Sarin SK, Kumar M, Eslam M, George J, Al Mahtab M, Akbar SMF, et al. Liver diseases in the Asia-pacific region: a lancet gastroenterology & hepatology commission. Lancet Gastroenterol Hepatol (2020) 5(2):167–228. doi: 10.1016/S2468-1253(19)30342-5
5. Mak LY, Wong DK, Cheung KS, Seto WK, Lai CL, Yuen MF. Review article: hepatitis b core-related antigen (HBcrAg): an emerging marker for chronic hepatitis b virus infection. Aliment Pharmacol Ther (2018) 47(1):43–54. doi: 10.1111/apt.14376
6. Nguyen MH, Wong G, Gane E, Kao JH, Dusheiko G. Hepatitis b virus: advances in prevention, diagnosis, and therapy. Clin Microbiol Rev (2020) 33(2):e00046–19. doi: 10.1128/CMR.00046-19
7. Iannacone M, Guidotti LG. Immunobiology and pathogenesis of hepatitis b virus infection. Nat Rev Immunol (2022) 22(1):19–32. doi: 10.1038/s41577-021-00549-4
8. Arzumanyan A, Reis HM, Feitelson MA. Pathogenic mechanisms in HBV- and HCV-associated hepatocellular carcinoma. Nat Rev Cancer (2013) 13(2):123–35. doi: 10.1038/nrc3449
9. Blank S, Wang Q, Fiel MI, Luan W, Kim KW, Kadri H, et al. Assessing prognostic significance of preoperative alpha-fetoprotein in hepatitis b-associated hepatocellular carcinoma: normal is not the new normal. Ann Surg Oncol (2014) 21(3):986–94. doi: 10.1245/s10434-013-3357-z
10. Yang SL, Liu LP, Yang S, Liu L, Ren JW, Fang X, et al. Preoperative serum alpha-fetoprotein and prognosis after hepatectomy for hepatocellular carcinoma. Br J Surg (2016) 103(6):716–24. doi: 10.1002/bjs.10093
11. Kim DY, Han KH. Epidemiology and surveillance of hepatocellular carcinoma. Liver Cancer (2012) 1(1):2–14. doi: 10.1159/000339016
12. Meguro M, Mizuguchi T, Nishidate T, Okita K, Ishii M, Ota S, et al. Prognostic roles of preoperative alpha-fetoprotein and des-gamma-carboxy prothrombin in hepatocellular carcinoma patients. World J Gastroenterol (2015) 21(16):4933–45. doi: 10.3748/wjg.v21.i16.4933
13. Chon YE, Choi GH, Lee MH, Kim SU, Kim DY, Ahn SH, et al. Combined measurement of preoperative alpha-fetoprotein and des-gamma-carboxy prothrombin predicts recurrence after curative resection in patients with hepatitis-b-related hepatocellular carcinoma. Int J Cancer (2012) 131(10):2332–41. doi: 10.1002/ijc.27507
14. Sohn W, Paik YH, Kim JM, Kwon CH, Joh JW, Cho JY, et al. HBV DNA and HBsAg levels as risk predictors of early and late recurrence after curative resection of HBV-related hepatocellular carcinoma. Ann Surg Oncol (2014) 21(7):2429–35. doi: 10.1245/s10434-014-3621-x
15. Wang MD, Li C, Liang L, Xing H, Sun LY, Quan B, et al. Early and late recurrence of hepatitis b virus-associated hepatocellular carcinoma. Oncologist (2020) 25(10):e1541–e51. doi: 10.1634/theoncologist.2019-0944
16. Yan PG, Wang RY, Zhang J, Cong WM, Dong H, Yu HY, et al. Impact of preoperative hepatitis b virus levels on prognosis after primary and repeat hepatectomies for hepatocellular carcinoma patients-a retrospective study. J Gastrointest Surg (2018) 22(5):872–83. doi: 10.1007/s11605-017-3638-0
17. Sun F, Liu Z, Wang B. Correlation between low-level viremia and hepatitis b-related hepatocellular carcinoma and recurrence: a retrospective study. BMC Cancer (2021) 21(1):1103. doi: 10.1186/s12885-021-08483-3
18. Huang G, Lau WY, Shen F, Pan ZY, Fu SY, Yang Y, et al. Preoperative hepatitis b virus DNA level is a risk factor for postoperative liver failure in patients who underwent partial hepatectomy for hepatitis b-related hepatocellular carcinoma. World J Surg (2014) 38(9):2370–6. doi: 10.1007/s00268-014-2546-7
19. Sohn W, Paik YH, Cho JY, Ahn JM, Choi GS, Kim JM, et al. Influence of hepatitis b virus reactivation on the recurrence of HBV-related hepatocellular carcinoma after curative resection in patients with low viral load. J Viral Hepat (2015) 22(6):539–50. doi: 10.1111/jvh.12356
20. Huang G, Lai EC, Lau WY, Zhou WP, Shen F, Pan ZY, et al. Posthepatectomy HBV reactivation in hepatitis b-related hepatocellular carcinoma influences postoperative survival in patients with preoperative low HBV-DNA levels. Ann Surg (2013) 257(3):490–505. doi: 10.1097/SLA.0b013e318262b218
21. Zhou YM, Zhang XF, Li B, Sui CJ, Yang JM. Prognosis after resection of hepatitis b virus-related hepatocellular carcinoma originating from non-cirrhotic liver. Ann Surg Oncol (2014) 21(7):2406–12. doi: 10.1245/s10434-014-3505-0
22. Liu KX, Hong JG, Wu R, Dong ZR, Yang YF, Yan YC, et al. Clinical benefit of antiviral agents for hepatocellular carcinoma patients with low preoperative HBV-DNA loads undergoing curative resection: a meta-analysis. Front Oncol (2021) 11:605648. doi: 10.3389/fonc.2021.605648
23. Huang S, Xia Y, Lei Z, Zou Q, Li J, Yang T, et al. Antiviral therapy inhibits viral reactivation and improves survival after repeat hepatectomy for hepatitis b virus-related recurrent hepatocellular carcinoma. J Am Coll Surg (2017) 224(3):283–93 e4. doi: 10.1016/j.jamcollsurg.2016.11.009
24. Lee JI, Kim JK, Chang HY, Lee JW, Kim JM, Chung HJ, et al. Impact of postoperative hepatitis b virus reactivation in hepatocellular carcinoma patients who formerly had naturally suppressed virus. J Gastroenterol Hepatol (2014) 29(5):1019–27. doi: 10.1111/jgh.12472
25. Huang L, Li J, Lau WY, Yan J, Zhou F, Liu C, et al. Perioperative reactivation of hepatitis b virus replication in patients undergoing partial hepatectomy for hepatocellular carcinoma. J Gastroenterol Hepatol (2012) 27(1):158–64. doi: 10.1111/j.1440-1746.2011.06888.x
26. Li ZL, Yan WT, Zhang J, Zhao YJ, Lau WY, Mao XH, et al. Identification of actual 10-year survival after hepatectomy of HBV-related hepatocellular carcinoma: a multicenter study. J Gastrointest Surg (2019) 23(2):288–96. doi: 10.1007/s11605-018-4006-4
27. Wang Z, Duan Y, Zhang J, Lv Y, Wu S, Cheng M, et al. Preoperative antiviral therapy and microvascular invasion in hepatitis b virus-related hepatocellular carcinoma: a meta-analysis. Eur J Pharmacol (2020) 883:173382. doi: 10.1016/j.ejphar.2020.173382
28. Li Z, Lei Z, Xia Y, Li J, Wang K, Zhang H, et al. Association of preoperative antiviral treatment with incidences of microvascular invasion and early tumor recurrence in hepatitis b virus-related hepatocellular carcinoma. JAMA Surg (2018) 153(10):e182721. doi: 10.1001/jamasurg.2018.2721
29. Huang G, Li PP, Lau WY, Pan ZY, Zhao LH, Wang ZG, et al. Antiviral therapy reduces hepatocellular carcinoma recurrence in patients with low HBV-DNA levels: a randomized controlled trial. Ann Surg (2018) 268(6):943–54. doi: 10.1097/SLA.0000000000002727
30. Qiu JF, Ye JZ, Feng XZ, Qi YP, Ma L, Yuan WP, et al. Pre- and post-operative HBsAg levels may predict recurrence and survival after curative resection in patients with HBV-associated hepatocellular carcinoma. J Surg Oncol (2017) 116(2):140–8. doi: 10.1002/jso.24628
31. Lee IC, Lei HJ, Chau GY, Yeh YC, Wu CJ, Su CW, et al. Predictors of long-term recurrence and survival after resection of HBV-related hepatocellular carcinoma: the role of HBsAg. Am J Cancer Res (2021) 11(7):3711–25.
32. Huang G, Lau WY, Zhou W-p, Shen F, Pan Z-y, Yuan S-x, et al. Prediction of hepatocellular carcinoma recurrence in patients with low hepatitis b virus DNA levels and high preoperative hepatitis b surface antigen levels. JAMA Surg (2014) 149(6):519–27. doi: 10.1001/jamasurg.2013.4648
33. Fried MW, Piratvisuth T, Lau GK, Marcellin P, Chow WC, Cooksley G, et al. HBeAg and hepatitis b virus DNA as outcome predictors during therapy with peginterferon alfa-2a for HBeAg-positive chronic hepatitis b. Hepatology (2008) 47(2):428–34. doi: 10.1002/hep.22065
34. Shen J, Liu J, Li C, Wen T, Yan L, Yang J. The prognostic significance of serum HBeAg on the recurrence and long-term survival after hepatectomy for hepatocellular carcinoma: a propensity score matching analysis. J Viral Hepat (2018) 25(9):1057–65. doi: 10.1111/jvh.12911
35. Schwarzenbach H, Hoon DS, Pantel K. Cell-free nucleic acids as biomarkers in cancer patients. Nat Rev Cancer (2011) 11(6):426–37. doi: 10.1038/nrc3066
36. Wang D, Hu X, Long G, Xiao L, Wang ZM, Zhou LD. The clinical value of total plasma cell-free DNA in hepatitis b virus-related hepatocellular carcinoma. Ann Transl Med (2019) 7(22):650. doi: 10.21037/atm.2019.10.78
37. Kawaguchi K, Honda M, Ohta H, Terashima T, Shimakami T, Arai K, et al. Serum wisteria floribunda agglutinin-positive mac-2 binding protein predicts hepatocellular carcinoma incidence and recurrence in nucleos(t)ide analogue therapy for chronic hepatitis b. J Gastroenterol (2018) 53(6):740–51. doi: 10.1007/s00535-017-1386-2
38. Kim SU, Heo JY, Kim BK, Park JY, Kim DY, Han KH, et al. Wisteria floribunda agglutinin-positive human mac-2 binding protein predicts the risk of HBV-related liver cancer development. Liver Int (2017) 37(6):879–87. doi: 10.1111/liv.13341
39. Kim HS, Kim SU, Kim BK, Park JY, Kim DY, Ahn SH, et al. Serum wisteria floribunda agglutinin-positive human mac-2 binding protein level predicts recurrence of hepatitis b virus-related hepatocellular carcinoma after curative resection. Clin Mol Hepatol (2020) 26(1):33–44. doi: 10.3350/cmh.2018.0073
40. Rizvi S, Gores GJ. Pathogenesis, diagnosis, and management of cholangiocarcinoma. Gastroenterology (2013) 145(6):1215–29. doi: 10.1053/j.gastro.2013.10.013
41. Zhang W, Wang Y, Dong X, Yang B, Zhou H, Chen L, et al. Elevated serum CA19-9 indicates severe liver inflammation and worse survival after curative resection in hepatitis b-related hepatocellular carcinoma. Biosci Trends (2022) 15(6):397–405. doi: 10.5582/bst.2021.01517
42. Eschrich J, Kobus Z, Geisel D, Halskov S, Rossner F, Roderburg C, et al. The diagnostic approach towards combined hepatocellular-Cholangiocarcinoma-State of the art and future perspectives. Cancers (Basel) (2023) 15(1):301. doi: 10.3390/cancers15010301
43. Sonnenberg-Riethmacher E, Miehe M, Riethmacher D. Periostin in allergy and inflammation. Front Immunol (2021) 12:722170. doi: 10.3389/fimmu.2021.722170
44. Ikeda-Iwabu Y, Taniyama Y, Katsuragi N, Sanada F, Koibuchi N, Shibata K, et al. Periostin short fragment with exon 17 via aberrant alternative splicing is required for breast cancer growth and metastasis. Cells (2021) 10(4):892. doi: 10.3390/cells10040892
45. Yue H, Li W, Chen R, Wang J, Lu X, Li J. Stromal POSTN induced by TGF-beta1 facilitates the migration and invasion of ovarian cancer. Gynecol Oncol (2021) 160(2):530–8. doi: 10.1016/j.ygyno.2020.11.026
46. Lv Y, Wang W, Jia WD, Sun QK, Huang M, Zhou HC, et al. High preoparative levels of serum periostin are associated with poor prognosis in patients with hepatocellular carcinoma after hepatectomy. Eur J Surg Oncol (2013) 39(10):1129–35. doi: 10.1016/j.ejso.2013.06.023
47. Jang SY, Park SY, Lee HW, Choi YK, Park KG, Yoon GS, et al. The combination of periostin overexpression and microvascular invasion is related to a poor prognosis for hepatocellular carcinoma. Gut Liver (2016) 10(6):948–54. doi: 10.5009/gnl15481
48. Li N, Yamamoto G, Fuji H, Kisseleva T. Interleukin-17 in liver disease pathogenesis. Semin liver disease (2021) 41(4):507–15. doi: 10.1055/s-0041-1730926
49. Duan M, Hao J, Cui S, Worthley DL, Zhang S, Wang Z, et al. Diverse modes of clonal evolution in HBV-related hepatocellular carcinoma revealed by single-cell genome sequencing. Cell Res (2018) 28(3):359–73. doi: 10.1038/cr.2018.11
50. Zhang C, Gao Y, Du C, Markowitz GJ, Fu J, Zhang Z, et al. Hepatitis b-induced IL8 promotes hepatocellular carcinoma venous metastasis and intrahepatic treg accumulation. Cancer Res (2021) 81(9):2386–98. doi: 10.1158/0008-5472.CAN-20-3453
51. Chen SH, Wang X. A high preoperative serum IL-25 level is a negative prognosis predictor after liver resection for HBV-HCC. Front Oncol (2022) 12:858151. doi: 10.3389/fonc.2022.858151
52. Sheng T, Wang B, Wang SY, Deng B, Qu L, Qi XS, et al. The relationship between serum interleukin-6 and the recurrence of hepatitis b virus related hepatocellular carcinoma after curative resection. Med (Baltimore) (2015) 94(24):e941. doi: 10.1097/MD.0000000000000941
53. She S, Xiang Y, Yang M, Ding X, Liu X, Ma L, et al. C-reactive protein is a biomarker of AFP-negative HBV-related hepatocellular carcinoma. Int J Oncol (2015) 47(2):543–54. doi: 10.3892/ijo.2015.3042
54. Hosel M, Quasdorff M, Ringelhan M, Kashkar H, Debey-Pascher S, Sprinzl MF, et al. Hepatitis b virus activates signal transducer and activator of transcription 3 supporting hepatocyte survival and virus replication. Cell Mol Gastroenterol Hepatol (2017) 4(3):339–63. doi: 10.1016/j.jcmgh.2017.07.003
55. Zhao X, Luo J, Li B, Liu S, Li D. The association between preoperative serum c-reactive protein and hepatocellular carcinoma recurrence in patients with chronic hepatitis b virus (HBV) infection–a retrospective study. PloS One (2015) 10(1):e0116909. doi: 10.1371/journal.pone.0116909
56. Li JD, Diao YK, Li J, Wu H, Sun LY, Gu WM, et al. Association between preoperative prealbumin level and postoperative mortality and morbidity after hepatic resection for hepatocellular carcinoma: a multicenter study from a HBV-endemic area. Am J Surg (2021) 221(5):1024–32. doi: 10.1016/j.amjsurg.2020.08.036
57. Wu SJ, Lin YX, Ye H, Xiong XZ, Li FY, Cheng NS. Prognostic value of alkaline phosphatase, gamma-glutamyl transpeptidase and lactate dehydrogenase in hepatocellular carcinoma patients treated with liver resection. Int J Surg (2016) 36(Pt A):143–51. doi: 10.1016/j.ijsu.2016.10.033
58. Liu K, Huang Z, Yang S, Lin L, Zheng S, Zhang X, et al. The age, gamma-glutamyl transpeptidase and platelet index: a novel noninvasive model for predicting hepatocellular carcinoma in patients with hepatitis b virus-related liver cirrhosis. J Hepatocell Carcinoma (2022) 9:1057–63. doi: 10.2147/JHC.S386977
59. Dai T, Deng M, Ye L, Liu R, Lin G, Chen X, et al. Prognostic value of combined preoperative gamma-glutamyl transpeptidase to platelet ratio and fibrinogen in patients with HBV-related hepatocellular carcinoma after hepatectomy. Am J Trans Res (2020) 12(6):2984–97.
60. Wang Y, Peng C, Cheng Z, Wang X, Wu L, Li J, et al. The prognostic significance of preoperative neutrophil-lymphocyte ratio in patients with hepatocellular carcinoma receiving hepatectomy: a systematic review and meta-analysis. Int J Surg (2018) 55:73–80. doi: 10.1016/j.ijsu.2018.05.022
61. Fu SJ, Shen SL, Li SQ, Hua YP, Hu WJ, Liang LJ, et al. Prognostic value of preoperative peripheral neutrophil-to-lymphocyte ratio in patients with HBV-associated hepatocellular carcinoma after radical hepatectomy. Med Oncol (2013) 30(4):721. doi: 10.1007/s12032-013-0721-6
62. Shen SL, Fu SJ, Huang XQ, Chen B, Kuang M, Li SQ, et al. Elevated preoperative peripheral blood monocyte count predicts poor prognosis for hepatocellular carcinoma after curative resection. BMC Cancer (2014) 14:744. doi: 10.1186/1471-2407-14-744
63. Lin ZX, Ruan DY, Li Y, Wu DH, Ma XK, Chen J, et al. Lymphocyte-to-monocyte ratio predicts survival of patients with hepatocellular carcinoma after curative resection. World J Gastroenterol (2015) 21(38):10898–906. doi: 10.3748/wjg.v21.i38.10898
64. Chen T, Song D, Min Z, Wang X, Gu Y, Wei B, et al. Perioperative dynamic alterations in peripheral regulatory T and b cells in patients with hepatocellular carcinoma. J Trans Med (2012) 10:14. doi: 10.1186/1479-5876-10-14
65. Chen L, Zhang Q, Chang W, Du Y, Zhang H, Cao G. Viral and host inflammation-related factors that can predict the prognosis of hepatocellular carcinoma. Eur J Cancer (2012) 48(13):1977–87. doi: 10.1016/j.ejca.2012.01.015
66. Kramvis A, Kew MC. The core promoter of hepatitis b virus. J Viral Hepat (1999) 6(6):415–27. doi: 10.1046/j.1365-2893.1999.00189.x
67. Lee JY, Locarnini S. Hepatitis b virus: pathogenesis, viral intermediates, and viral replication. Clin Liver Dis (2004) 8(2):301–20. doi: 10.1016/j.cld.2004.02.009
68. Yin F, Xie Y, Fan H, Zhang J, Guo Z. Mutations in hepatitis b virus polymerase are associated with the postoperative survival of hepatocellular carcinoma patients. PloS One (2017) 12(12):e0189730. doi: 10.1371/journal.pone.0189730
69. Xie Y, Liu S, Zhao Y, Zhang L, Zhao Y, Liu B, et al. Precore/Core region mutations in hepatitis b virus DNA predict postoperative survival in hepatocellular carcinoma. PloS One (2015) 10(7):e0133393. doi: 10.1371/journal.pone.0133393
70. Xie Y, Liu S, Zhao Y, Guo Z, Xu J. X Protein mutations in hepatitis b virus DNA predict postoperative survival in hepatocellular carcinoma. Tumour Biol (2014) 35(10):10325–31. doi: 10.1007/s13277-014-2331-0
71. Xu QG, Yuan SX, Tao QF, Yu J, Cai J, Yang Y, et al. A novel HBx genotype serves as a preoperative predictor and fails to activate the JAK1/STATs pathway in hepatocellular carcinoma. J Hepatol (2019) 70(5):904–17. doi: 10.1016/j.jhep.2019.01.007
72. Yeh CT, So M, Ng J, Yang HW, Chang ML, Lai MW, et al. Hepatitis b virus-DNA level and basal core promoter A1762T/G1764A mutation in liver tissue independently predict postoperative survival in hepatocellular carcinoma. Hepatology (2010) 52(6):1922–33. doi: 10.1002/hep.23898
73. Jiao F, Long L, Ding S, Xie X, Jia L, Lu F. Complete genome sequencing and clinical analysis of intrahepatic hepatitis b virus cccDNA from HCC. Microb Pathog (2017) 109:49–55. doi: 10.1016/j.micpath.2017.04.028
74. Alfano V, Zeisel MB, Levrero M, Guerrieri F. The lncRNAs in HBV-related HCCs: targeting chromatin dynamics and beyond. Cancers (Basel) (2021) 13(13):3115. doi: 10.3390/cancers13133115
75. Wong CM, Tsang FH, Ng IO. Non-coding RNAs in hepatocellular carcinoma: molecular functions and pathological implications. Nat Rev Gastroenterol Hepatol (2018) 15(3):137–51. doi: 10.1038/nrgastro.2017.169
76. Gu JX, Zhang X, Miao RC, Xiang XH, Fu YN, Zhang JY, et al. Six-long non-coding RNA signature predicts recurrence-free survival in hepatocellular carcinoma. World J Gastroenterol (2019) 25(2):220–32. doi: 10.3748/wjg.v25.i2.220
77. He Z, Chen J, Wang J, Xu L, Zhou Z, Chen M, et al. Expression of hepatitis b surface antigen in liver tissues can serve as a predictor of prognosis for hepatitis b virus-related hepatocellular carcinoma patients after liver resection. Eur J Gastroenterol Hepatol (2021) 33(1):76–82. doi: 10.1097/MEG.0000000000001698
78. Revathidevi S, Munirajan AK. Akt in cancer: mediator and more. Semin Cancer Biol (2019) 59:80–91. doi: 10.1016/j.semcancer.2019.06.002
79. Song M, Bode AM, Dong Z, Lee MH. AKT as a therapeutic target for cancer. Cancer Res (2019) 79(6):1019–31. doi: 10.1158/0008-5472.CAN-18-2738
80. Chen L, Gu L, Gu Y, Wang H, Deng M, Stamataki Z, et al. HBV core promoter mutations and AKT upregulate s-phase kinase-associated protein 2 to promote postoperative hepatocellular carcinoma progression. Sci Rep (2016) 6:35917. doi: 10.1038/srep35917
81. Chambers I, Colby D, Robertson M, Nichols J, Lee S, Tweedie S, et al. Functional expression cloning of nanog, a pluripotency sustaining factor in embryonic stem cells. Cell (2003) 113(5):643–55. doi: 10.1016/S0092-8674(03)00392-1
82. Najafzadeh B, Asadzadeh Z, Motafakker Azad R, Mokhtarzadeh A, Baghbanzadeh A, Alemohammad H, et al. The oncogenic potential of NANOG: an important cancer induction mediator. J Cell Physiol (2021) 236(4):2443–58. doi: 10.1002/jcp.30063
83. Lei Y, Wang X, Sun H, Fu Y, Tian Y, Yang L, et al. Association of preoperative NANOG-positive circulating tumor cell levels with recurrence of hepatocellular carcinoma. Front Oncol (2021) 11:601668. doi: 10.3389/fonc.2021.601668
84. Jayatilleke KM, Hulett MD. Heparanase and the hallmarks of cancer. J Trans Med (2020) 18(1):453. doi: 10.1186/s12967-020-02624-1
85. Huang GL, Li BK, Zhang MY, Wei RR, Yuan YF, Shi M, et al. Allele loss and down-regulation of heparanase gene are associated with the progression and poor prognosis of hepatocellular carcinoma. PloS One (2012) 7(8):e44061. doi: 10.1371/journal.pone.0044061
86. Stein U, Dahlmann M, Walther W. MACC1 - more than metastasis? facts and predictions about a novel gene. J Mol Med (Berl) (2010) 88(1):11–8. doi: 10.1007/s00109-009-0537-1
87. Stein U. MACC1 - a novel target for solid cancers. Expert Opin Ther targets (2013) 17(9):1039–52. doi: 10.1517/14728222.2013.815727
88. Radhakrishnan H, Walther W, Zincke F, Kobelt D, Imbastari F, Erdem M, et al. MACC1-the first decade of a key metastasis molecule from gene discovery to clinical translation. Cancer Metastasis Rev (2018) 37(4):805–20. doi: 10.1007/s10555-018-9771-8
89. Qu JH, Chang XJ, Lu YY, Bai WL, Chen Y, Zhou L, et al. Overexpression of metastasis-associated in colon cancer 1 predicts a poor outcome of hepatitis b virus-related hepatocellular carcinoma. World J Gastroenterol (2012) 18(23):2995–3003. doi: 10.3748/wjg.v18.i23.2995
90. Mehrpouya M, Pourhashem Z, Yardehnavi N, Oladnabi M. Evaluation of cytokeratin 19 as a prognostic tumoral and metastatic marker with focus on improved detection methods. J Cell Physiol (2019) 234(12):21425–35. doi: 10.1002/jcp.28768
91. Sun DW, Zhang YY, Sun XD, Chen YG, Qiu W, Ji M, et al. Prognostic value of cytokeratin 19 in hepatocellular carcinoma: a meta-analysis. Clin Chim Acta (2015) 448:161–9. doi: 10.1016/j.cca.2015.06.027
92. Shuyao W, Mingyang B, Feifei M, Xiaoqin H. CK19 predicts recurrence and prognosis of HBV positive HCC. J Gastrointest Surg (2022) 26(2):341–51. doi: 10.1007/s11605-021-05107-w
93. Ishak K, Baptista A, Bianchi L, Callea F, De Groote J, Gudat F, et al. Histological grading and staging of chronic hepatitis. J Hepatol (1995) 22(6):696–9. doi: 10.1016/0168-8278(95)80226-6
94. Wang Q, Fiel MI, Blank S, Luan W, Kadri H, Kim KW, et al. Impact of liver fibrosis on prognosis following liver resection for hepatitis b-associated hepatocellular carcinoma. Br J Cancer (2013) 109(3):573–81. doi: 10.1038/bjc.2013.352
95. Yang SL, Liu LP, Sun YF, Yang XR, Fan J, Ren JW, et al. Distinguished prognosis after hepatectomy of HBV-related hepatocellular carcinoma with or without cirrhosis: a long-term follow-up analysis. J Gastroenterol (2016) 51(7):722–32. doi: 10.1007/s00535-015-1146-0
96. Zhang X, Li J, Shen F, Lau WY. Significance of presence of microvascular invasion in specimens obtained after surgical treatment of hepatocellular carcinoma. J Gastroenterol Hepatol (2018) 33(2):347–54. doi: 10.1111/jgh.13843
97. Chen ZH, Zhang XP, Feng JK, Li LQ, Zhang F, Hu YR, et al. Actual long-term survival in hepatocellular carcinoma patients with microvascular invasion: a multicenter study from China. Hepatol Int (2021) 15(3):642–50. doi: 10.1007/s12072-021-10174-x
98. Yang P, Si A, Yang J, Cheng Z, Wang K, Li J, et al. A wide-margin liver resection improves long-term outcomes for patients with HBV-related hepatocellular carcinoma with microvascular invasion. Surgery (2019) 165(4):721–30. doi: 10.1016/j.surg.2018.09.016
99. Chen SL, Xiao H, Xie ZL, Shen JX, Chen ZB, Wang YQ, et al. The presence of microvascular invasion guides treatment strategy in recurrent HBV-related HCC. Eur Radiol (2020) 30(6):3473–85. doi: 10.1007/s00330-019-06640-8
100. Hiraoka A, Kumada T, Michitaka K, Kudo M. Newly proposed ALBI grade and ALBI-T score as tools for assessment of hepatic function and prognosis in hepatocellular carcinoma patients. Liver Cancer (2019) 8(5):312–25. doi: 10.1159/000494844
101. Johnson PJ, Berhane S, Kagebayashi C, Satomura S, Teng M, Reeves HL, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol (2015) 33(6):550–8. doi: 10.1200/JCO.2014.57.9151
102. Zou H, Wen Y, Yuan K, Miao XY, Xiong L, Liu KJ. Combining albumin-bilirubin score with future liver remnant predicts post-hepatectomy liver failure in HBV-associated HCC patients. Liver Int (2018) 38(3):494–502. doi: 10.1111/liv.13514
103. Li C, Zhang J-Y, Zhang X-Y, Wen T-F, Yan L-N. FibroScan predicts ascites after liver resection for hepatitis b virus-related hepatocellular carcinoma: a prospective cohort study. Int J Surgery (2015) 20:21–5. doi: 10.1016/j.ijsu.2015.05.047
104. Chen X, Zou H, Xiong L, Huang SF, Miao XY, Wen Y. Predictive power of splenic thickness for post-hepatectomy liver failure in HBV-associated hepatocellular carcinoma patients. World J Surg Oncol (2017) 15(1):216. doi: 10.1186/s12957-017-1281-6
105. Bae JS, Lee DH, Yi NJ, Lee KW, Suh KS, Kim H, et al. Magnetic resonance elastography versus transient elastography in the prediction of complications after resection for hepatocellular carcinoma. Ann Surg (2022) 276(5):e466–e73. doi: 10.1097/SLA.0000000000004576
106. Cho HJ, Kim B, Kim HJ, Huh J, Kim JK, Lee JH, et al. Liver stiffness measured by MR elastography is a predictor of early HCC recurrence after treatment. Eur Radiol (2020) 30(8):4182–92. doi: 10.1007/s00330-020-06792-y
107. Zhang L, Chen J, Jiang H, Rong D, Guo N, Yang H, et al. MR elastography as a biomarker for prediction of early and late recurrence in HBV-related hepatocellular carcinoma patients before hepatectomy. Eur J Radiol (2022) 152:110340. doi: 10.1016/j.ejrad.2022.110340
108. Qi M, Chen Y, Zhang GQ, Meng YJ, Zhao FL, Wang J, et al. Clinical significance of preoperative liver stiffness measurements in primary HBV-positive hepatocellular carcinoma. Future Oncol (London England) (2017) 13(30):2799–810. doi: 10.2217/fon-2017-0281
109. Wang J, Shan Q, Liu Y, Yang H, Kuang S, He B, et al. 3D MR elastography of hepatocellular carcinomas as a potential biomarker for predicting tumor recurrence. J Magn Reson Imaging (2019) 49(3):719–30. doi: 10.1002/jmri.26250
110. Le Bihan D. What can we see with IVIM MRI? NeuroImage (2019) 187:56–67. doi: 10.1016/j.neuroimage.2017.12.062
111. Zhang Y, Kuang S, Shan Q, Rong D, Zhang Z, Yang H, et al. Can IVIM help predict HCC recurrence after hepatectomy? Eur Radiol (2019) 29(11):5791–803. doi: 10.1007/s00330-019-06180-1
112. Lin CY, Chen JH, Liang JA, Lin CC, Jeng LB, Kao CH. 18F-FDG PET or PET/CT for detecting extrahepatic metastases or recurrent hepatocellular carcinoma: a systematic review and meta-analysis. Eur J Radiol (2012) 81(9):2417–22. doi: 10.1016/j.ejrad.2011.08.004
113. Li Y, Zhang Y, Fang Q, Zhang X, Hou P, Wu H, et al. Radiomics analysis of [(18)F]FDG PET/CT for microvascular invasion and prognosis prediction in very-early- and early-stage hepatocellular carcinoma. Eur J Nucl Med Mol Imaging (2021) 48(8):2599–614. doi: 10.1007/s00259-020-05119-9
114. Kim JM, Kwon CHD, Joh JW, Sinn DH, Choi GS, Paik SW. Prognosis of preoperative positron emission tomography uptake in hepatectomy patients. Ann Surg Treat Res (2018) 94(4):183–9. doi: 10.4174/astr.2018.94.4.183
115. Zhang XP, Chai ZT, Feng JK, Zhu HM, Zhang F, Hu YR, et al. Association of type 2 diabetes mellitus with incidences of microvascular invasion and survival outcomes in hepatitis b virus-related hepatocellular carcinoma after liver resection: a multicenter study. Eur J Surg Oncol (2022) 48(1):142–9. doi: 10.1016/j.ejso.2021.08.010
116. Huang J, Li BK, Chen GH, Li JQ, Zhang YQ, Li GH, et al. Long-term outcomes and prognostic factors of elderly patients with hepatocellular carcinoma undergoing hepatectomy. J Gastrointest Surg (2009) 13(9):1627–35. doi: 10.1007/s11605-009-0933-4
117. Wang HQ, Yang J, Yan LN, Zhang XW, Yang JY. Liver resection in hepatitis b related-hepatocellular carcinoma: clinical outcomes and safety in elderly patients. World J Gastroenterol (2014) 20(21):6620–5. doi: 10.3748/wjg.v20.i21.6620
118. Kokudo T, Hasegawa K, Shirata C, Tanimoto M, Ishizawa T, Kaneko J, et al. Assessment of preoperative liver function for surgical decision making in patients with hepatocellular carcinoma. Liver Cancer (2019) 8(6):447–56. doi: 10.1159/000501368
119. Mai RY, Bai T, Luo XL, Wu GB. Indocyanine green retention test as a predictor of postoperative complications in patients with hepatitis b virus-related hepatocellular carcinoma. Ther Clin Risk Manage (2022) 18:761–72. doi: 10.2147/TCRM.S363849
120. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg (2004) 240(2):205–13. doi: 10.1097/01.sla.0000133083.54934.ae
121. Slankamenac K, Graf R, Barkun J, Puhan MA, Clavien PA. The comprehensive complication index: a novel continuous scale to measure surgical morbidity. Ann Surg (2013) 258(1):1–7. doi: 10.1097/SLA.0b013e318296c732
122. Bao M, Zhu Q, Aji T, Wei S, Tuergan T, Ha X, et al. Development of models to predict postoperative complications for hepatitis b virus-related hepatocellular carcinoma. Front Oncol (2021) 11:717826. doi: 10.3389/fonc.2021.717826
123. Pinato DJ, North BV, Sharma R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: the prognostic nutritional index (PNI). Br J Cancer (2012) 106(8):1439–45. doi: 10.1038/bjc.2012.92
124. Zhang T, Liu Z, Zhao X, Mao Z, Bai L. A novel prognostic score model based on combining systemic and hepatic inflammation markers in the prognosis of HBV-associated hepatocellular carcinoma patients. Artif Cells Nanomed Biotechnol (2019) 47(1):2246–55. doi: 10.1080/21691401.2019.1573174
125. Shen SL, Fu SJ, Chen B, Kuang M, Li SQ, Hua YP, et al. Preoperative aspartate aminotransferase to platelet ratio is an independent prognostic factor for hepatitis b-induced hepatocellular carcinoma after hepatic resection. Ann Surg Oncol (2014) 21(12):3802–9. doi: 10.1245/s10434-014-3771-x
126. Ignacio de Ulíbarri J, González-Madroño A, de Villar NG, González P, González B, Mancha A, et al. CONUT: a tool for controlling nutritional status. first validation in a hospital population. Nutricion hospitalaria (2005) 20(1):38–45.
127. Lin ZX, Ruan DY, Jia CC, Wang TT, Cheng JT, Huang HQ, et al. Controlling nutritional status (CONUT) score-based nomogram to predict overall survival of patients with HBV-associated hepatocellular carcinoma after curative hepatectomy. Clin Transl Oncol (2020) 22(3):370–80. doi: 10.1007/s12094-019-02137-4
128. Wang XB, Chen J, Xiang BD, Wu FX, Li LQ. High CONUT score predicts poor survival and postoperative HBV reactivation in HBV-related hepatocellular carcinoma patients with low HBV-DNA levels. Eur J Surg Oncol (2019) 45(5):782–7. doi: 10.1016/j.ejso.2018.11.007
129. Benson AB, D’Angelica MI, Abbott DE, Anaya DA, Anders R, Are C, et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Network (2021) 19(5):541–65. doi: 10.6004/jnccn.2021.0022
130. McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology (2021) 73 Suppl 1(Suppl 1):4–13. doi: 10.1002/hep.31288
131. Sasaki K, Shindoh J, Nishioka Y, Sugawara T, Margonis GA, Andreatos N, et al. Postoperative low hepatitis c virus load predicts long-term outcomes after hepatectomy for hepatocellular carcinoma. J Surg Oncol (2018) 117(5):902–11. doi: 10.1002/jso.25015
132. Shindoh J, Hasegawa K, Matsuyama Y, Inoue Y, Ishizawa T, Aoki T, et al. Low hepatitis c viral load predicts better long-term outcomes in patients undergoing resection of hepatocellular carcinoma irrespective of serologic eradication of hepatitis c virus. J Clin Oncol (2013) 31(6):766–73. doi: 10.1200/JCO.2012.44.3234
133. Shindoh J, Hasegawa K, Takemura N, Omichi K, Ishizawa T, Aoki T, et al. Hepatitis c viral load predicts tumor recurrence after curative resection of hepatocellular carcinoma regardless of the genotype of hepatitis c virus. Hepatol Int (2014) 8(1):112–20. doi: 10.1007/s12072-013-9507-3
134. Conti F, Buonfiglioli F, Scuteri A, Crespi C, Bolondi L, Caraceni P, et al. Early occurrence and recurrence of hepatocellular carcinoma in HCV-related cirrhosis treated with direct-acting antivirals. J Hepatol (2016) 65(4):727–33. doi: 10.1016/j.jhep.2016.06.015
135. Okamura Y, Sugiura T, Ito T, Yamamoto Y, Ashida R, Ohgi K, et al. The achievement of a sustained virological response either before or after hepatectomy improves the prognosis of patients with primary hepatitis c virus-related hepatocellular carcinoma. Ann Surg Oncol (2019) 26(13):4566–75. doi: 10.1245/s10434-019-07911-w
136. Shinkawa H, Hasegawa K, Arita J, Akamatsu N, Kaneko J, Sakamoto Y, et al. Impact of sustained virological response to interferon therapy on recurrence of hepatitis c virus-related hepatocellular carcinoma. Ann Surg Oncol (2017) 24(11):3196–202. doi: 10.1245/s10434-017-6008-y
137. Hsu PY, Liang PC, Huang CI, Hsieh MH, Tsai YS, Lin TC, et al. Effects of achieving SVR on clinical characteristics and surgical outcomes in patients who developed early-stage HCV-related hepatocellular carcinoma and received curative resection: preoperative versus postoperative SVR. Viruses (2022) 14(11):2412. doi: 10.3390/v14112412
138. Tanaka S, Shinkawa H, Tamori A, Takemura S, Uchida-Kobayashi S, Amano R, et al. Postoperative direct-acting antiviral treatment after liver resection in patients with hepatitis c virus-related hepatocellular carcinoma. Hepatol Res (2021) 51(11):1102–14. doi: 10.1111/hepr.13709
139. Tanaka S, Shinkawa H, Tamori A, Takemura S, Takahashi S, Amano R, et al. Surgical outcomes for hepatocellular carcinoma detected after hepatitis c virus eradiation by direct-acting antivirals. J Surg Oncol (2020) 122(8):1543–52. doi: 10.1002/jso.26184
140. Kim JM, Rhu J, Ha SY, Choi GS, Kwon CHD, Joh JW. Hepatectomy outcomes in patients with hepatitis c virus-related hepatocellular carcinoma with or without cirrhosis. Ann Surg Treat Res (2022) 102(1):1–9. doi: 10.4174/astr.2022.102.1.1
141. Kaneda K, Uenishi T, Takemura S, Shinkawa H, Urata Y, Sakae M, et al. The influence of postoperative glycemic control on recurrence after curative resection in diabetics with hepatitis c virus-related hepatocellular carcinoma. J Surg Oncol (2012) 105(6):606–11. doi: 10.1002/jso.22137
142. Lee JJ, Kim PT, Fischer S, Fung S, Gallinger S, McGilvray I, et al. Impact of viral hepatitis on outcomes after liver resection for hepatocellular carcinoma: results from a north american center. Ann Surg Oncol (2014) 21(8):2708–16. doi: 10.1245/s10434-014-3609-6
143. Sasaki K, Shindoh J, Nishioka Y, Margonis GA, Sugawara T, Andreatos N, et al. Impact of viral etiology on postoperative De novo recurrence after hepatectomy for hepatocellular carcinoma in cirrhotic patients. J Gastrointest Surg (2017) 21(3):487–95. doi: 10.1007/s11605-016-3344-3
144. Okamura Y, Sugiura T, Ito T, Yamamoto Y, Ashida R, Ohgi K, et al. Changes in patient background and prognosis after hepatectomy for hepatocellular carcinoma by hepatitis virus infection status: new trends in Japan. Ann Gastroenterol Surg (2021) 5(4):553–66. doi: 10.1002/ags3.12451
145. Nishikawa H, Osaki Y. Non-b, non-c hepatocellular carcinoma (Review). Int J Oncol (2013) 43(5):1333–42. doi: 10.3892/ijo.2013.2061
146. Degasperi E, Colombo M. Distinctive features of hepatocellular carcinoma in non-alcoholic fatty liver disease. Lancet Gastroenterol Hepatol (2016) 1(2):156–64. doi: 10.1016/S2468-1253(16)30018-8
147. Cauchy F, Belghiti J. A clinical perspective of the link between metabolic syndrome and hepatocellular carcinoma. J Hepatocell Carcinoma (2015) 2:19–27. doi: 10.2147/JHC.S44521
148. Zarzavadjian Le Bian A, Costi R, Constantinides V, Smadja C. Metabolic disorders, non-alcoholic fatty liver disease and major liver resection: an underestimated perioperative risk. J Gastrointest Surg (2012) 16(12):2247–55. doi: 10.1007/s11605-012-2044-x
149. Yoshida N, Takayama T, Midorikawa Y, Higaki T, Nakayama H, Moriguchi M, et al. Surgical outcomes in patients with hepatocellular carcinoma associated with metabolic syndrome. World J Surg (2015) 39(2):471–7. doi: 10.1007/s00268-014-2828-0
150. Chin KM, Prieto M, Cheong CK, Di Martino M, Ielpo B, Goh BKP, et al. Outcomes after curative therapy for hepatocellular carcinoma in patients with non-alcoholic fatty liver disease: a meta-analysis and review of current literature. HPB (Oxford) (2021) 23(8):1164–74. doi: 10.1016/j.hpb.2021.01.009
151. Tsunematsu M, Haruki K, Fujiwara Y, Furukawa K, Onda S, Matsumoto M, et al. Preoperative controlling nutritional status (CONUT) score predicts long-term outcomes in patients with non-b non-c hepatocellular carcinoma after curative hepatic resection. Langenbecks Arch Surg (2021) 406(1):99–107. doi: 10.1007/s00423-020-01987-9
152. Kaibori M, Ishizaki M, Matsui K, Kwon AH. Clinicopathologic characteristics of patients with non-b non-c hepatitis virus hepatocellular carcinoma after hepatectomy. Am J Surg (2012) 204(3):300–7. doi: 10.1016/j.amjsurg.2011.11.014
153. Hayashi M, Yamada S, Takano N, Okamura Y, Takami H, Inokawa Y, et al. Different characteristics of serum Alfa fetoprotein and serum des-gamma-carboxy prothrombin in resected hepatocellular carcinoma. In Vivo (2021) 35(3):1749–60. doi: 10.21873/invivo.12434
154. Chang TS, Hsu NT, Chen SC, Hsu IL, Lee MH, Lu SN. Non-b, non-c hepatocellular carcinoma in an HBV- and HCV-endemic area: a community-based prospective longitudinal study. Viruses (2022) 14(5):984. doi: 10.3390/v14050984
155. Omichi K, Shindoh J, Yamamoto S, Matsuyama Y, Akamatsu N, Arita J, et al. Postoperative outcomes for patients with non-b non-c hepatocellular carcinoma: a subgroup analysis of patients with a history of hepatitis b infection. Ann Surg Oncol (2015) 22(Suppl 3):S1034–40. doi: 10.1245/s10434-015-4845-0
156. Maulat C, Truant S, Hobeika C, Barbier L, Herrero A, Doussot A, et al. Prognostication algorithm for non-cirrhotic non-b non-c hepatocellular carcinoma-a multicenter study under the aegis of the French association of hepato-biliary surgery and liver transplantation. Hepatobil Surg Nutr (2023) 12(2):192–204. doi: 10.21037/hbsn-22-33
157. Albaradei S, Thafar M, Alsaedi A, Van Neste C, Gojobori T, Essack M, et al. Machine learning and deep learning methods that use omics data for metastasis prediction. Comput Struct Biotechnol J (2021) 19:5008–18. doi: 10.1016/j.csbj.2021.09.001
158. Chen S, Zhang Z, Wang Y, Fang M, Zhou J, Li Y, et al. Using quasispecies patterns of hepatitis b virus to predict hepatocellular carcinoma with deep sequencing and machine learning. J Infect Dis (2021) 223(11):1887–96. doi: 10.1093/infdis/jiaa647
159. Tao K, Bian Z, Zhang Q, Guo X, Yin C, Wang Y, et al. Machine learning-based genome-wide interrogation of somatic copy number aberrations in circulating tumor DNA for early detection of hepatocellular carcinoma. EBioMedicine (2020) 56:102811. doi: 10.1016/j.ebiom.2020.102811
160. Zhang WB, Hou SZ, Chen YL, Mao F, Dong Y, Chen JG, et al. Deep learning for approaching hepatocellular carcinoma ultrasound screening dilemma: identification of alpha-Fetoprotein-Negative hepatocellular carcinoma from focal liver lesion found in high-risk patients. Front Oncol (2022) 12:862297. doi: 10.3389/fonc.2022.862297
161. Mai RY, Lu HZ, Bai T, Liang R, Lin Y, Ma L, et al. Artificial neural network model for preoperative prediction of severe liver failure after hemihepatectomy in patients with hepatocellular carcinoma. Surgery (2020) 168(4):643–52. doi: 10.1016/j.surg.2020.06.031
162. Chiu CC, Lee KT, Lee HH, Wang JJ, Sun DP, Huang CC, et al. Comparison of models for predicting quality of life after surgical resection of hepatocellular carcinoma: a prospective study. J Gastrointest Surg (2018) 22(10):1724–31. doi: 10.1007/s11605-018-3833-7
163. Liu Z, Liu Y, Zhang W, Hong Y, Meng J, Wang J, et al. Deep learning for prediction of hepatocellular carcinoma recurrence after resection or liver transplantation: a discovery and validation study. Hepatol Int (2022) 16(3):577–89. doi: 10.1007/s12072-022-10321-y
164. Qu WF, Tian MX, Qiu JT, Guo YC, Tao CY, Liu WR, et al. Exploring pathological signatures for predicting the recurrence of early-stage hepatocellular carcinoma based on deep learning. Front Oncol (2022) 12:968202. doi: 10.3389/fonc.2022.968202
165. Ji GW, Zhu FP, Xu Q, Wang K, Wu MY, Tang WW, et al. Machine-learning analysis of contrast-enhanced CT radiomics predicts recurrence of hepatocellular carcinoma after resection: a multi-institutional study. EBioMedicine (2019) 50:156–65. doi: 10.1016/j.ebiom.2019.10.057
166. Liu P, Tan XZ, Zhang T, Gu QB, Mao XH, Li YC, et al. Prediction of microvascular invasion in solitary hepatocellular carcinoma </= 5 cm based on computed tomography radiomics. World J Gastroenterol (2021) 27(17):2015–24. doi: 10.3748/wjg.v27.i17.2015
167. Audureau E, Carrat F, Layese R, Cagnot C, Asselah T, Guyader D, et al. Personalized surveillance for hepatocellular carcinoma in cirrhosis - using machine learning adapted to HCV status. J Hepatol (2020) 73(6):1434–45. doi: 10.1016/j.jhep.2020.05.052
168. Park H, Lo-Ciganic WH, Huang J, Wu Y, Henry L, Peter J, et al. Machine learning algorithms for predicting direct-acting antiviral treatment failure in chronic hepatitis c: an HCV-TARGET analysis. Hepatology (2022) 76(2):483–91. doi: 10.1002/hep.32347
169. Yip TC, Ma AJ, Wong VW, Tse YK, Chan HL, Yuen PC, et al. Laboratory parameter-based machine learning model for excluding non-alcoholic fatty liver disease (NAFLD) in the general population. Aliment Pharmacol Ther (2017) 46(4):447–56. doi: 10.1111/apt.14172
Keywords: hepatitis B virus, hepatocellular carcinoma, predictor, preoperative, postoperative
Citation: He Z and Tang D (2023) Perioperative predictors of outcome of hepatectomy for HBV-related hepatocellular carcinoma. Front. Oncol. 13:1230164. doi: 10.3389/fonc.2023.1230164
Received: 28 May 2023; Accepted: 28 June 2023;
Published: 13 July 2023.
Edited by:
Mauro G. Tognon, University of Ferrara, ItalyReviewed by:
Giuseppe Fiume, Magna Græcia University of Catanzaro, ItalyCopyright © 2023 He and Tang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Di Tang, dGFuZ2RpQG1haWwuc3lzdS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.