 Pasquale Esposito1,2*
Pasquale Esposito1,2* Annarita Bottini2
Annarita Bottini2 Elvina Lecini2Francesca Cappadona1Michela Piaggio2Lucia Macciò2Carlo Genova2,3
Elvina Lecini2Francesca Cappadona1Michela Piaggio2Lucia Macciò2Carlo Genova2,3 Francesca Viazzi1,2
Francesca Viazzi1,2- 1Nephrology Unit, IRCCS Ospedale Policlinico San Martino, Genova, Italy
- 2Department of Internal Medicine, University of Genova, Genova, Italy
- 3UOC Clinica di Oncologia Medica, IRCCS Ospedale Policlinico San Martino, Genova, Italy
Introduction: Acute kidney injury (AKI) in cancer patients receiving immune checkpoint inhibitors (ICIs) may recognize multiple causes. Here, we reviewed cases of biopsy-proven acute tubulointerstitial nephritis (ATIN) to describe the clinical characteristics and outcomes of this condition.
Method: We conducted a pooled analysis of clinical cases of ICI-related biopsy-proven ATIN up to 1 May 2022. We collected data on clinical characteristics, AKI, biopsy findings, laboratory examinations, and renal outcomes.
Results: Eighty-five patients (61.4 ± 19 years, 56 male) were evaluated. Melanoma was the most prevalent diagnosis (51%), followed by non-small cell lung cancer (30%). ICI treatment consisted of PD-1, PDL-1 (nivolumab, pembrolizumab, atezolizumab), and CTLA-4 inhibitors (i) (ipilimumab) or combination PD-1i+CTLA4i. Renal toxicity developed after a median of four cycles of therapy. Fifty-one patients (65.5%) developed the most severe form of AKI- stage 3, including five patients requiring dialysis. All the 19 patients treated with dual ICI blockade developed AKI-stage 3, compared with 29 patients out of the 60 receiving a single agent (p<0.001). Most events were managed with corticosteroids associated with ICI withdrawal. In 15 patients ICI was restarted, but in six (40%) AKI recurred. Overall, 32 patients (40%) presented a complete renal recovery, which chance was inversely associated with dual ICI blockade (OR 0.15, 95CI 0.03-0.7, p=0.01).
Conclusion: ICI-related ATIN may develop late after the therapy initiation, presenting as severe AKI, particularly in patients with dual ICI blockade. Although this complication may be partially reversible, concerns remain about the renal function sequelae and the possibility of restarting ICI treatment.
Introduction
The systemic treatment with immune checkpoint inhibitors (ICIs) has revolutionized the management of multiple solid tumors, including melanoma and non-small cell lung cancer (NSCLC) (1). Notably, ICIs have been initially employed as single-agent regimens in advanced tumors; however, their use has been progressively extended to different settings, and novel combinations have emerged, including combinations of ICI and chemotherapy or combinations of multiple ICIs. Currently, the main immune checkpoints of therapeutic interest are the Programmed Death protein 1 (PD-1) and its ligand (PD-L1), as well as Cytotoxic T Lymphocyte Antigen 4 (CTLA-4) (2).
This treatment is not completely free from potential adverse events, which are strictly correlated with their mechanism of action (3). Indeed, disrupting the physiologic inhibitory effect of immune checkpoints might result in lymphocyte activation against multiple normal sites; such toxicities, collectively defined as immune-related adverse events (irAEs), may virtually involve any site, such as skin, gastroenteric tract, lungs, or kidneys (4).
Acute kidney injury (AKI) is a relatively uncommon irAE, but it has a relevant impact on involved patients (5). Indeed, AKI might translate into long-term renal dysfunction that might result in ineligibility to receive subsequent lines of treatment, such as chemotherapy, with a potential negative impact on patients’ outcomes from an oncological perspective (6). Notably, while clinical trials and published real-world data report immune-related renal toxicities, in most cases such events are only described as “creatinine increase” and renal biopsies are seldom performed (7, 8). Ideally, a renal biopsy might provide relevant data, both in terms of differential diagnosis and toxicity grading beyond the simple creatinine value, with a potential role in prognostic information (9). The most common histological finding in patients with ICI-related AKI is acute tubulointerstitial nephritis (ATIN), characterized by inflammation, infiltration of immune cells, and tubular damage (10). However, AKI in cancer patients is a multifaceted phenomenon that may recognize multiple causes, so the etiological definition is fundamental to address a proper clinical approach.
In this study, we reviewed case reports of biopsy-proven ATIN in patients treated with ICIs, to describe the clinical and laboratory characteristics and outcomes of this condition.
Methods
Search strategy, study selection, and data extraction
A literature search was conducted on PubMed for eligible studies published up to May 1, 2022, using the search terms [(Pembrolizumab OR Nivolumab OR Ipilimumab OR Atezolizumab OR Avelumab OR Durvalumab) AND (Nephritis)]. No filters were applied, and the text words could be in all fields of the articles. Data were independently extracted by two investigators (A.B. and E.L.) who carefully and manually scanned all the articles to identify cases of biopsy-proven ATIN A supervisor reviewed any discrepancies (P.E.). A total of 139 articles were identified by the search on PubMed, and 43 were eligible for analysis (7, 8, 11–51). The selection process was performed in two steps. In the first step, we analyzed articles, excluding those not presenting case reports/case series, not in English or not involving checkpoint inhibitors. Then, from this initial list, articles without renal biopsy, articles reporting other renal alterations, and those with insufficient clinical data were also excluded.
Of note, the list of papers excluded from the analysis also comprised the multicenter study by Gupta el. 2021 which evaluated more than 400 patients with ICI-related AKI (52). Indeed, although this cohort included 151 patients undergoing kidney biopsy (89% of them with ATIN), the authors did not provide detailed information to discern and characterize the clinical presentation and course of patients with biopsy-proven ATIN, with respect to patients with AKI from other etiologies.
The final list of eligible articles included 111 patients.
After the first article selection, as a second step, we analyzed individual patients, excluding 28 cases reporting only extra-renal toxicity, other renal alterations than ATIN, or cases without renal biopsy. Therefore, 83 patients were suitable for analysis, to whom we added two patients from our institution (who gave written informed consent to data collection), reaching a final number of 85 patients. (Supplementary Figure 1) The extracted data included patient demographics, comorbidities, home therapy, histology cancer, oncological therapy regimen, number of therapy cycles before renal toxicity, results of renal biopsy (in addition to ATIN, we recorded also the compresence of granulomas or acute tubular necrosis), baseline serum creatinine (sCr) and slope, clinical presentation (blood pressure, edema, hematuria), presence of other checkpoint inhibitor-induced toxicities, urinary analysis, ATIN treatment (dosage and duration), and decisions regarding restarting or interrupting ICIs therapy.
Definitions
We defined and graded AKI according to the Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline, based on changes in serum creatinine with respect to the pre-ICI value considered as baseline (53). We defined each stage as stages 1, 2, and 3.
These correspond to a serum creatinine increase of 1.5 to 1.9 times from the baseline value or a serum creatinine peak ≥ 0.3 mg/dL, 2 to 2.5 times, and 3 or more times their baseline creatinine or newly required renal replacement therapy (RRT). Urine output was not considered due to limited data availability.
Hematuria was defined as a red blood cell number of more than three per high-power field, and nephrotic proteinuria as proteinuria of more than 3.5 g/day. The outcome of toxicity was categorized into three classes: complete renal recovery in absence of AKI criteria (i.e., last serum creatinine < 1.5-fold baseline); no recovery if patients needed RRT, and partial recovery if, at the last evaluation, patients were not on RRT but failed to meet the criteria for complete renal recovery (54).
Finally, when present we consider the tumor radiological response that was reported as: complete response, partial response, and stable disease.
Statistical analysis
Descriptive and statistical analyses were performed on the whole of our center’s cases and those extracted from the literature.
Quantitative variables were represented by mean ± standard deviation (SD) or interquartile ranges (IQR) if they were not normally distributed (Shapiro Test).
Group analyses for continuous variables were performed by using the Student t-test or nonparametric Mann-Whitney test when appropriate. Comparisons of proportions were made using Fisher’s exact test. Univariate and multivariate logistic regression analysis was used to investigate predictor factors on AKI severity and renal function recovery.
The analyses were performed using Stata 13.1 (Stata Corporation, College Station, Tex, United States) used for computation. A 2-sided P value <0.05 was considered statistically significant.
Results
Patient characteristics
Eighty-five patients (56 males) with ICI-related biopsy-proven ATIN were analyzed. The mean age was 61.4 ± 19 years, and the most frequent comorbidities were hypertension (n=41), ischemic heart disease/atrial fibrillation (n=12), diabetes mellitus (n=8), and hypothyroidism (n=7). Forty-three patients (51%) had melanoma, 25 (30%) had non-small cell lung cancer (NSCLC), 8 had clear cell renal cell carcinoma (CRCC), and 9 had other types of cancer. ICI treatment consisted of PD-1 inhibitors nivolumab in 28 patients, pembrolizumab in 21 patients, PDL-1 inhibitor (atezolizumab) in 2 patients, and CTLA4 inhibitor (ipilimumab) in 9 patients, while 19 patients were treated with dual ICI blockade, nivolumab+ipilimumab. In six cases, the checkpoint inhibitor drug was not specified (Table 1). Eleven patients in the whole group were receiving chemotherapy combined with immunotherapy.
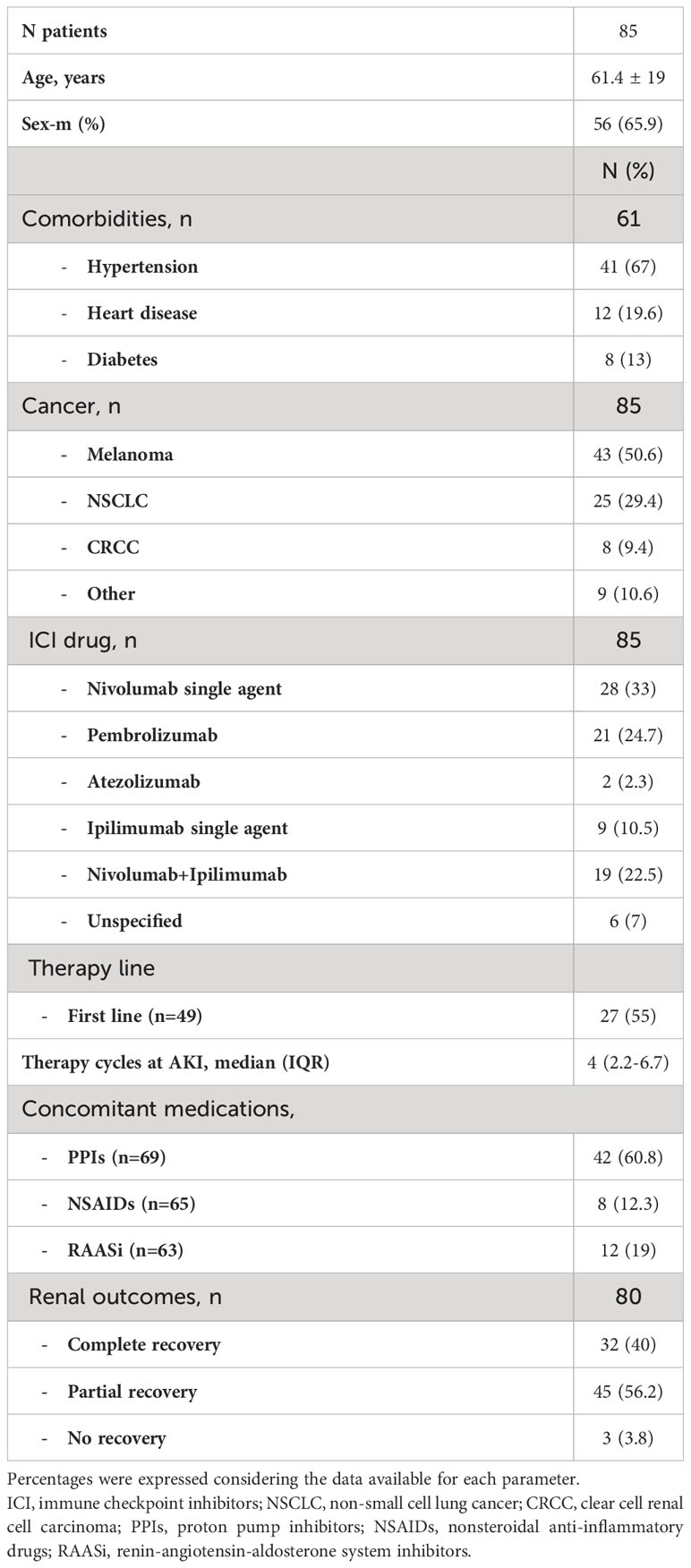
Table 1 Clinical and laboratory characteristics of patients evaluated in the pooled analysis.
Clinical presentation and ICI-related renal toxicity
The mean basal serum creatinine (available in 78 patients) was 0.8 ± 0.4 mg/dl.
Renal toxicity developed during the first line in 27 patients out of the 49 for whom data were available (55%). Instead, data on therapy cycles were present in 62 cases showing that AKI developed after a median of four cycles of therapy, but in most cases (n=48, 77%) after at least three treatment cycles. Eleven patients (14%) presented with AKI stage 1, 16 patients (20.5%) with stage 2, and 51 patients (65.5%) with AKI stage 3, including five patients requiring RRT. In 7 patients AKI stage was not reported, and it was not possible to evaluate the stage due to the lack of data on basal serum creatinine. Urinary sediment, available in 55 patients, showed: 36 patients with leukocyturia, 20 patients with hematuria, and 13 patients with casts. Five patients (9%) presented with nephrotic range proteinuria, and ten patients (18%) had gross hematuria. Data on the clinical presentation of renal toxicity were available for 41 patients, among them 7 presented with edema, 10 had fever, and 12 were hypertensive. AKI was accompanied by other ICI-related toxicity in 37/74 patients (50%), including 11 cases of autoimmune endocrinological disorders, 8 cases of skin toxicity, and 5 cases of autoimmune hepatitis. Due to the study design, kidney biopsy showed a histological picture of ATIN in all the patients (Supplementary Figure 2). According to the report of histological data, in 12 out of 61 patients (20%), interstitial granulomas were described, while ATN was present in 10 out of 71 patients (14%). Comparing patients with the more severe form of AKI (AKI 3) with those presenting milder renal dysfunction (AKI 1-2), we found no significant difference in patient demographic and clinical characteristics, such as in histological findings (Table 2).
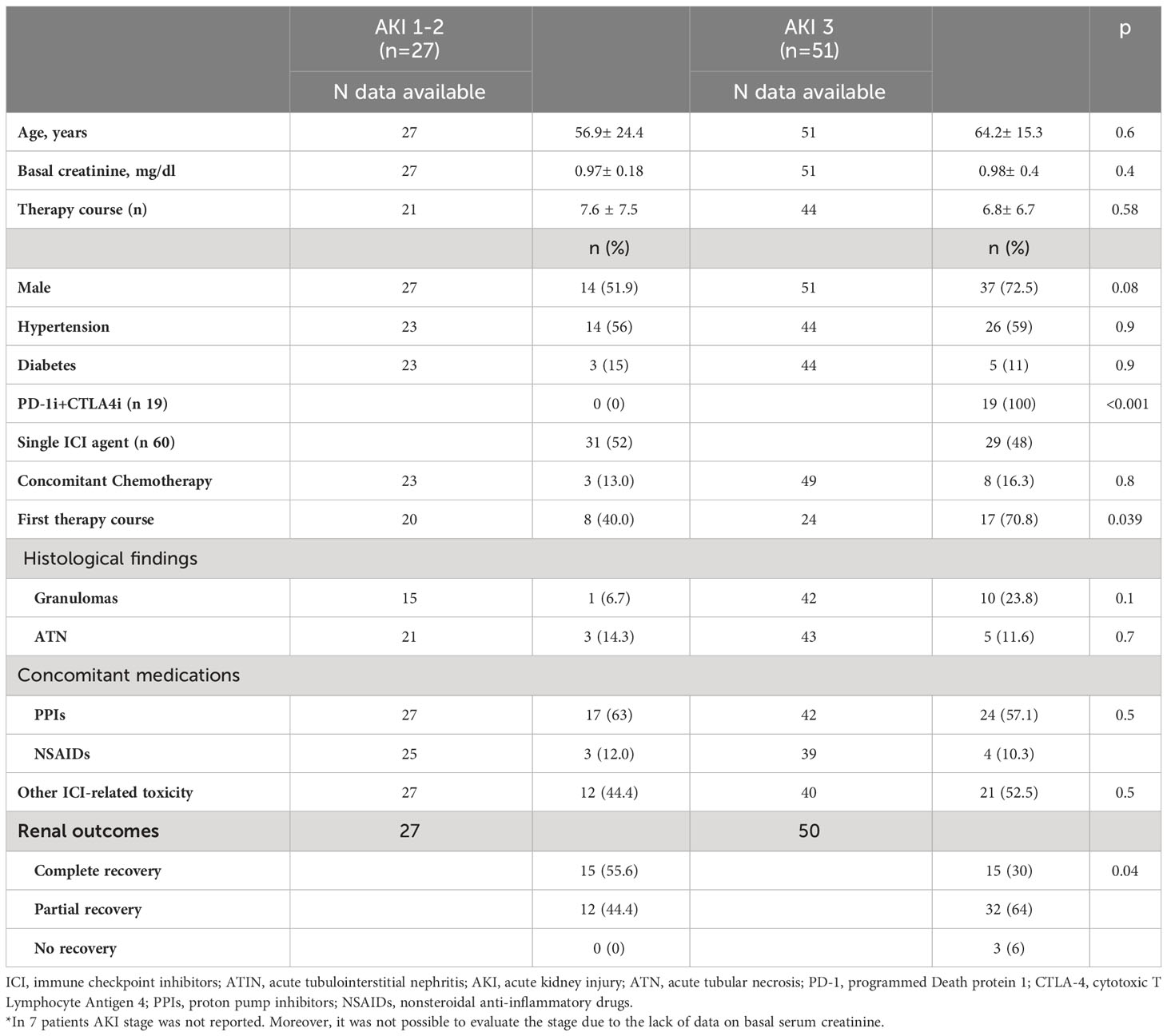
Table 2 Clinical and laboratory characteristics of patients with ICI-related ATIN according to the acute kidney injury severity.
Among AKI 3 patients, there was a significantly higher prevalence of patients at the first-line therapy (p=0.04). All the patients treated with the dual ICI blockade developed stage 3 AKI (100%), compared with 29 out of the 60 patients (48%) taking a single agent (p<0.001, Figure 1A).
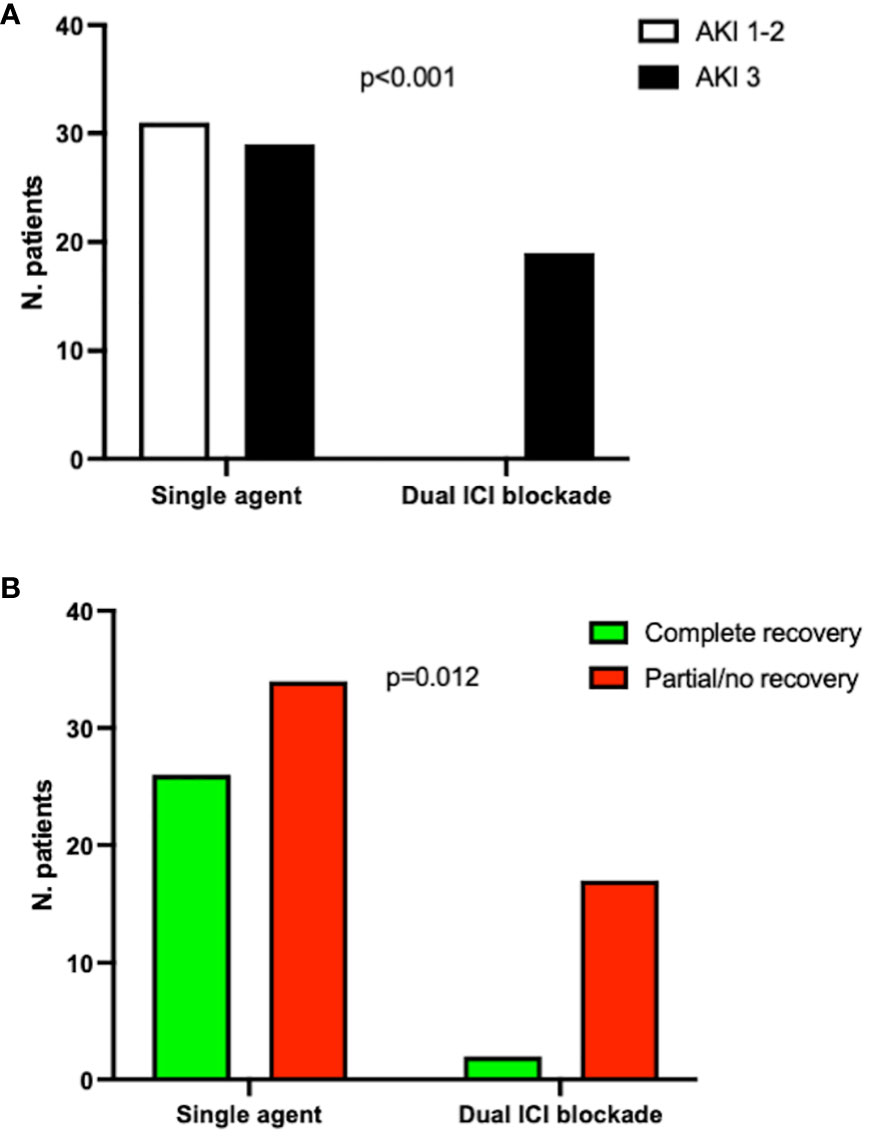
Figure 1 Prevalence of AKI stage 3 (A) and renal recovery (complete vs partial/no recovery) (B) in patients on single or dual ICI blockade. Fisher’s test. ICI, immune checkpoint inhibitors; AKI, acute kidney injury. Six patients were not included in this analysis due to the lack of data on specific ICI treatment prescribed.
Moreover, patients developing AKI stage 3 presented worse renal outcomes in terms of a significantly higher number of patients experiencing partial or no recovery of renal function.
Multivariate logistic regression analysis evaluating the risk of developing AKI stage 3 showed that when combined ICI treatment was considered in the analysis, other factors, such as age, sex, and therapy line lost significance (Supplementary Table 1).
Treatment of ICI-related ATIN
Data on ATIN treatment were reported in 84 patients. Among them, seventy-seven patients (91%) received immunosuppressive treatment, while seven patients did not receive any specific therapy.
All the treated patients received corticosteroids at different dosages, associated with mycophenolate mofetil in 5 patients and Rituximab in 1 case.
Excluding one patient still taking MMF three years after the onset of nivolumab-related toxicity, the mean duration of immunosuppressive treatment was 68.3 ± 49.3 days.
ICI treatment was withdrawn in 65 out of 69 patients with available data. Following renal function improvement, in 15 patients ICI therapy was restarted, and in six patients (40%) AKI recurred.
Renal outcomes
Renal outcomes were reported in 80 patients. Overall, at the last control (time ranging 7-1400 days after AKI diagnosis), 32 patients (40%) presented a complete renal recovery, 45 patients (56.2%) had a partial recovery, and 3 patients (3.8%) did not recover.
Complete renal recovery was observed only in 2 out of the 7 patients (28%) not treated with steroids, compared with 30 out of 77 treated patients (39%, p=ns).
Then, we found that among patients without complete recovery, there was a higher prevalence of dual ICI therapy and AKI stage 3 at the presentation (p=0.002 and 0.026, respectively), with no significant difference in other clinical characteristics (Table 3).
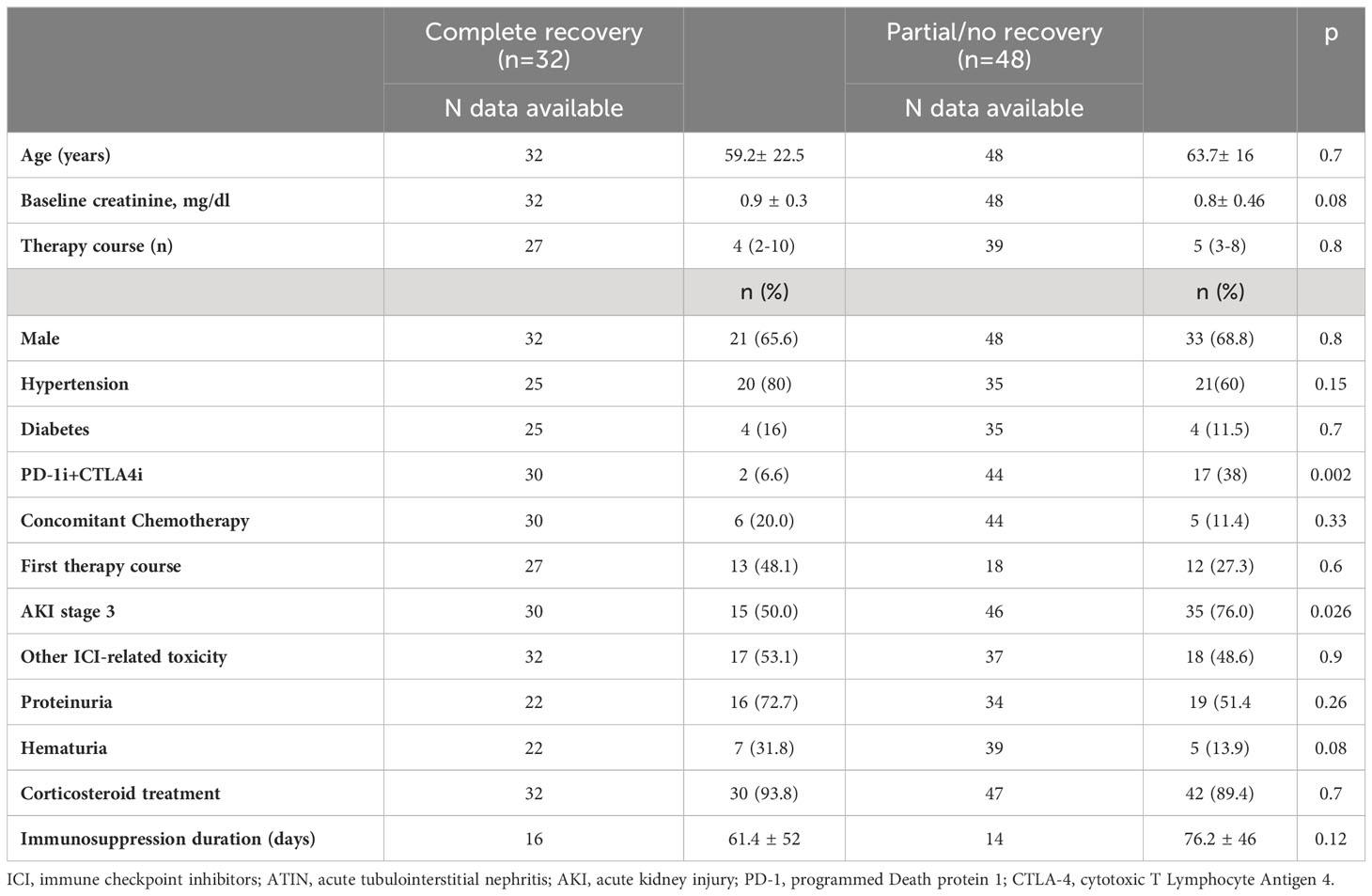
Table 3 Clinical and laboratory characteristics of patients with ICI-related ATIN according to the renal function recovery.
Conversely, a significantly higher percentage of patients taking a single ICI agent, 26 out of 60 (43%), had a complete renal recovery when compared with patients taking dual therapy (2 out of 19 (10%), p=0.01, Figure 1B). At univariate logistic regression, complete renal recovery was inversely associated with dual ICI blockade (OR 0.1, 95CI 0.02-0.5, p=0.006) and AKI 3 (OR 0.31, 95CI 0.1-0.9, p=0.04), but only the association with dual ICI therapy remained significant at multivariate analysis (Supplementary Table 2).
Finally, tumor radiological response was reported only in 33 cases, showing a complete response in seven patients (21.5%), a partial response in 10 patients (30%) and stable disease in the remaining 16 patients (48.5%).
Discussion
In this paper, we provide information about the risk profile, clinical presentation, and management of AKI due to ATIN occurring during ICIs. The rationale of this study moved from the observation that most of the previous reports on AKI during ICIs did not distinguish the various potential underlying causes, and there is limited data on patients undergoing kidney biopsies. This may be a relevant weakness since AKI in cancer patients may recognize multiple causes, including irAEs, volume depletion, obstructive nephropathy, hypercalcemia, and drug-related nephrotoxicity (55).
So, for example, only a part (151/429- 35%) of the large cohort of patients with ICI-related AKI, reported by Gupta et al., underwent kidney biopsy and, among them, almost 20% of the patients presented other nephropathies than ATIN (52).
So, conceivably the authors analyzed a heterogenic population, including an unknown number of patients without ATIN, which may explain some discrepancies we found comparing their results with our data. For example, Gupta et al. described a lower percentage of patients with AKI stage 3 (48.5 vs. 65.5% of our study). These differences may be at least in part influenced by different populations analyzed, further highlighting that proper discrimination of AKI etiologies is essential to define disease course and may have important clinical implications.
This is why, we focused our attention on cases of biopsy-proven ATIN, the most common histological presentation of renal irAEs during ICIs. This analysis allowed us to make many considerations that could help in guiding clinical decisions and future research.
First, we found that the timing of AKI development may be noteworthy. Indeed, as partially already reported, we observed that ATIN may develop also late in the history of cancer therapy, after several therapy cycles (56).
So, caution and awareness for the development of renal toxicity should be maintained throughout the whole course of therapy. Notably, it seems that dual ICI blockade with combined anti-PD-1 and anti-CTLA-4 treatment is associated with a significant risk of severe AKI and a reduced chance of renal recovery. This occurrence is not unexpected, as it is known that dual blockade is associated with an increased risk of irAEs compared to single-agent ICI (57). The potential elevated harmful effects of combination therapy may also explain the observation of an increased AKI severity in patients undergoing ICIs as first-line therapy. Indeed, combinations are typically administered at the first line, while patients treated in the second or further line usually receive single-agent PD-1/PD-L1 inhibitors (58). However, due to the limited number of cases, our data did not allow us to discriminate the nephrotoxic effects of the different ICI classes (CTLA4, PD-1, and PD-L1 inhibitors).
Almost all the patients included in this analysis were treated with corticosteroids, so we cannot quantify the impact of this treatment on the recovery of renal function in our cohort. However, as a matter of fact, corticosteroids are the cornerstone therapy in cases of ATIN of different etiologies (59). Moreover, general observations involving irAEs and immune-related renal impairment during ICIs confirm the effectiveness of corticosteroids (60). So, conceivably, a prompt corticosteroid initiation at the onset of renal toxicity might be instrumental to the resolution of the event, and this approach is not generally considered to disrupt the anti-neoplastic activity of ICIs. On the other hand, this is a fundamental point in favor of the renal biopsy. Indeed, apart from ATIN, other structural renal alterations may be found, which deserve different treatments and have various prognosis (61). Moreover, renal biopsy may guide differential diagnosis even when multiple drug-related nephrotoxicities are suspected (62) Finally, renal biopsy is important also to provide information on irAE severity and prognosis, which may assist in the following clinical management of the patient, such as the decision on ICI rechallenging (63).
Notably, our suggestions are not completely in line with the current recommendations from the American Society of Clinical Oncology (ASCO), which, although emphasizes the use of steroids for the treatment of suspected ICI-related AKI, suggest performing a kidney biopsy only in patients with severe AKI-stage 3 (64). Indeed, for the reasons above exposed we think that a kidney biopsy should be considered in almost all AKI patients fit for the procedure.
Looking at renal outcomes, we observed that in many patients renal recovery was not complete. This is an extremely relevant observation because permanent renal dysfunction in the case of patients with advanced cancer often results in further deterioration of quality of life and possibly a reduction of survival due to the worsened clinical condition and inability to receive further antineoplastic treatments. On the other hand, patients with potentially curable cancer could present the risk of developing chronic kidney disease (65). Finally, a further observation deserving of attention is the high recurrence rate of AKI after ICI reuse, which may have possible relevant clinical implications.
Remarkably, even in the analysis of the renal outcomes, we noticed significant differences in our patients when compared with those studied by Gupta et al. (52) In particular, they found better outcomes, with a higher rate of renal recovery and a lower rate of recurrence. Also, in this case, these dissimilarities could have been partially explained by the different populations evaluated, even if they could have been conditioned by the limitation of our study. Indeed, we are aware that the study has some weaknesses, mainly due to its retrospective design and collection of pooled data from the literature. So, although we sought uniform data collection and definitions, case reports from different authors usually lack the consistency of systematic data collection and may be biased from different diagnostic and clinical approaches (66). Moreover, our data are not representative of the general population of patients treated with ICIs, since, in this study, we intended to study the specific condition of ATIN. Furthermore, since there is a great heterogeneity in kidney biopsy policy among different centers, it is not possible to rule out that a selection bias occurred, mainly due to mild-moderate AKI cases who did not undergo kidney biopsy.
Finally, due to the lack of a control group and complete clinical and laboratory data, we could not evaluate the prevalence of other known risk factors for AKI, such as concomitant medications, hyperuricemia, and anemia, that may impact the susceptibility of developing kidney damage (67).
Surely, the evaluation of AKI timing, adverse effects of dual ICI blockade, and the long-term outcome of ATIN, such as the establishment of standardized therapeutic approaches, need prospective studies to be elucidated. Nevertheless, generating such data might be difficult due to the need for focused analysis including large cohorts of patients undergoing renal biopsy for AKI.
Conclusions
In conclusion, we found that ICI-related ATIN may develop at any stage of therapy in patients treated with ICIs. It may present as a severe form of AKI, particularly in patients with dual ICI blockade. This condition appears partially reversible, but concerns remain about the renal function sequelae and the possibility of restarting treatment after AKI resolution due to the risk of recurrence. Thus, we suggest that a simple but complete renal risk assessment should be included in the workup of patients undergoing ICI therapy, especially if a combined regimen is prescribed (68, 69). At the same time, monitoring renal function should be warranted throughout the whole course of immunotherapy, pointing out the fundamental contribution of renal biopsy in proper clinical management.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
PE, AB, CG contributed to conception and design of the study. AB, EL, MP organized the database. FC, LM performed the statistical analysis. PE wrote the first draft of the manuscript. CG, FV wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1221135/full#supplementary-material
References
1. Melosky B, Juergens R, Hirsh V, McLeod D, Leighl N, Tsao M-S, et al. Amplifying outcomes: checkpoint inhibitor combinations in first-line non-small cell lung cancer. Oncologist (2020) 25:64–77. doi: 10.1634/theoncologist.2019-0027
2. Cella E, Zullo L, Marconi S, Rossi G, Coco S, Dellepiane C, et al. Immunotherapy-chemotherapy combinations for non-small cell lung cancer: current trends and future perspectives. Expert Opin Biol Ther (2022) 22:1259–73. doi: 10.1080/14712598.2022.2116273
3. Wei SC, Duffy CR, Allison JP. Fundamental mechanisms of immune checkpoint blockade therapy. Cancer Discovery (2018) 8:1069–86. doi: 10.1158/2159-8290.CD-18-0367
4. Gumusay O, Callan J, Rugo HS. Immunotherapy toxicity: identification and management. Breast Cancer Res Treat (2022) 192:1–17. doi: 10.1007/s10549-021-06480-5
5. Borówka M, Łącki-Zynzeling S, Nicze M, Kozak S, Chudek J. Adverse renal effects of anticancer immunotherapy: A review. Cancers (Basel) (2022) 14:4086. doi: 10.3390/cancers14174086
6. Stengel B. Chronic kidney disease and cancer: a troubling connection. J Nephrol (2020) 23:253–62.
7. Meraz-Muñoz A, Amir E, Ng P, Avila-Casado C, Ragobar C, Chan C, et al. Acute kidney injury associated with immune checkpoint inhibitor therapy: incidence, risk factors and outcomes. J Immunother Cancer (2020) 8(1):e000467. doi: 10.1136/jitc-2019-000467
8. Hultin S, Nahar K, Menzies AM, Long GV, Fernando SL, Atkinson V, et al. Histological diagnosis of immune checkpoint inhibitor induced acute renal injury in patients with metastatic melanoma: a retrospective case series report. BMC Nephrol (2020) 21:391. doi: 10.1186/s12882-020-02044-9
9. Perazella MA. Kidney biopsy should be performed to document the cause of immune checkpoint inhibitor–associated acute kidney injury: commentary. Kidney360 (2020) 1:166–8. doi: 10.34067/KID.0001072019
10. Picciotto D, Genova C, Costigliolo F, Bottini A, Garibotto G, Viazzi F, et al. (2022). An updated focus on immune checkpoint inhibitors and tubulointerstitial nephritis. In: Interdisciplinary Cancer Research. Springer, Cham doi: 10.1007/16833_2022_80
11. Tanaka A, Ikinaga K, Kiyohara E, Tanemura A, Wataya-Kaneda M, Fujimura R, et al. Critical renal adverse event induced by nivolumab therapy in a stage IV melanoma patient. J Dermatol (2017) 44:727–8. doi: 10.1111/1346-8138.13538
12. Aya F, González-Navarro EA, Martínez C, Carcelero E, Arance A. Safe anti-programmed cell death-1 rechallenge with antibody switching after immune-related adverse events: brief communication. Immunotherapy (2021) 13:745–52. doi: 10.2217/imt-2020-0274
13. Anastasopoulou A, Diamantopoulos PT, Skalioti C, Liapis G, Psychogiou E, Ziogas DC, et al. The diagnosis and management of sarcoid-like reactions in patients with melanoma treated with BRAF and MEK inhibitors. A case series and review of the literature. Ther Adv Med Oncol (2021) 13:17588359211047348. doi: 10.1177/17588359211047349
14. Shirali AC, Perazella MA, Gettinger S. Association of acute interstitial nephritis with programmed cell death 1 inhibitor therapy in lung cancer patients. Am J Kidney Dis (2016) 68:287–91. doi: 10.1053/j.ajkd.2016.02.057
15. Izzedine H, Gueutin V, Gharbi C, Mateus C, Robert C, Routier E, et al. Kidney injuries related to ipilimumab. Invest New Drugs (2014) 32:769–73. doi: 10.1007/s10637-014-0092-7
16. Murakami N, Borges TJ, Yamashita M, Riella LV. Severe acute interstitial nephritis after combination immune-checkpoint inhibitor therapy for metastatic melanoma. Clin Kidney J (2016) 9:411–7. doi: 10.1093/ckj/sfw024
17. Cortazar FB, Marrone KA, Troxell ML, Ralto KM, Hoenig MP, Brahmer JR, et al. Clinicopathological features of acute kidney injury associated with immune checkpoint inhibitors. Kidney Int (2016) 90:638–47. doi: 10.1016/j.kint.2016.04.008
18. Cappelli LC, Gutierrez AK, Baer AN, Albayda J, Manno RL, Haque U, et al. Inflammatory arthritis and sicca syndrome induced by nivolumab and ipilimumab. Ann Rheum Dis (2017) 76:43–50. doi: 10.1136/annrheumdis-2016-209595
19. Belliere J, Meyer N, Mazieres J, Ollier S, Boulinguez S, Delas A, et al. Acute interstitial nephritis related to immune checkpoint inhibitors. Br J Cancer (2016) 115:1457–61. doi: 10.1038/bjc.2016.358
20. Escandon J, Peacock S, Trabolsi A, Thomas DB, Layka A, Lutzky J. Interstitial nephritis in melanoma patients secondary to PD-1 checkpoint inhibitor. J Immunother Cancer (2017) 5:3. doi: 10.1186/s40425-016-0205-2
21. Bottlaender L, Breton A-L, de Laforcade L, Dijoud F, Thomas L, Dalle S. Acute interstitial nephritis after sequential ipilumumab - nivolumab therapy of metastatic melanoma. J Immunother Cancer (2017) 5:57. doi: 10.1186/s40425-017-0261-2
22. Uchida A, Watanabe M, Nawata A, Ikari Y, Sasaki M, Shigemoto K, et al. Tubulointerstitial nephritis as adverse effect of programmed cell death 1 inhibitor, nivolumab, showed distinct histological findings. CEN Case Rep (2017) 6:169–74. doi: 10.1007/s13730-017-0269-y
23. Koda R, Watanabe H, Tsuchida M, Iino N, Suzuki K, Hasegawa G, et al. Immune checkpoint inhibitor (nivolumab)-associated kidney injury and the importance of recognizing concomitant medications known to cause acute tubulointerstitial nephritis: a case report. BMC Nephrol (2018) 19:48. doi: 10.1186/s12882-018-0848-y
24. Tabei A, Watanabe M, Ikeuchi H, Nakasatomi M, Sakairi T, Kaneko Y, et al. The analysis of renal infiltrating cells in acute tubulointerstitial nephritis induced by anti-PD-1 antibodies: A case report and review of the literature. Intern Med (2018) 57:3135–9. doi: 10.2169/internalmedicine.0444-17
25. Nakatani Y, Kawakami H, Ichikawa M, Yamamoto S, Otsuka Y, Mashiko A, et al. Nivolumab-induced acute granulomatous tubulointerstitial nephritis in a patient with gastric cancer. Invest New Drugs (2018) 36:726–31. doi: 10.1007/s10637-018-0596-7
26. Xipell M, Victoria I, Hoffmann V, Villarreal J, García-Herrera A, Reig O, et al. Acute tubulointerstitial nephritis associated with atezolizumab, an anti-programmed death-ligand 1 (pd-l1) antibody therapy. Oncoimmunology (2018) 7:e1445952. doi: 10.1080/2162402X.2018.1445952
27. Basnet S, Dhital R, Tharu B. Acute tubulointerstitial nephritis: A case report on rare adverse effect of pembrolizumab. Medicina (Kaunas) (2019) 55. doi: 10.3390/medicina55050176
28. Georgianos PI, Vaios V, Leontaridou E, Karayannopoulou G, Koletsa T, Sioulis A, et al. Acute interstitial nephritis in a patient with non-small cell lung cancer under immunotherapy with nivolumab. Case Rep Nephrol (2019) 2019:3614980. doi: 10.1155/2019/3614980
29. Ryuzaki M, Tokuyama H, Uchiyama K, Nakaya H, Hasegawa K, Miyashita K, et al. Acute interstitial nephritis with karyomegalic epithelial cells after nivolumab treatment-two case reports. Clin Med Insights Case Rep (2019) 12:1179547619853647. doi: 10.1177/1179547619853647
30. de Sousa Oliveira D, Mesquita JL, Garcia YDO, Rosales YMZ, Lemes RPG, Filho FDR, et al. Interstitial nephritis associated with nivolumab in a patient with hodgkin lymphoma. Rev Assoc Med Bras (1992) (2019) 65:934–6. doi: 10.1590/1806-9282.65.7.934
31. Shingarev R, Glezerman IG. Kidney complications of immune checkpoint inhibitors: A review. Am J Kidney Dis (2019) 74:529–37. doi: 10.1053/j.ajkd.2019.03.433
32. Shah N, Jacob J, Househ Z, Shiner E, Baird L, Soudy H. Unchecked immunity: a unique case of sequential immune-related adverse events with Pembrolizumab. J Immunother Cancer (2019) 7:247. doi: 10.1186/s40425-019-0727-5
33. Person F, Chahoud-Schriefer T, Fehrle W, Janneck M, Huber TB, Wiech T. Severe acute kidney injury due to nivolumab/ipilimumab-induced granulomatosis and fibrinoid vascular necrosis. J Immunother (2020) 43:29–31. doi: 10.1097/CJI.0000000000000296
34. Irifuku T, Satoh A, Tani H, Mandai K, Masaki T. Acute tubulointerstitial nephritis and IgM deposits on glomerular capillary walls after immunotherapy with nivolumab for metastatic renal cell carcinoma. CEN Case Rep (2020) 9:48–54. doi: 10.1007/s13730-019-00424-1
35. Oki R, Hirakawa Y, Kimura H, Honda K, Hinata M, Abe H, et al. Renal effects after pembrolizumab treatment for non-small cell lung carcinoma. Intern Med (2020) 59:977–81. doi: 10.2169/internalmedicine.3928-19
36. Taki T, Oda N, Fujioka Y, Mitani R, Tokura T, Takata I, et al. Successful treatment of non-small-cell lung cancer with atezolizumab following tubulointerstitial nephritis due to pembrolizumab. Intern Med (2020) 59:1639–42. doi: 10.2169/internalmedicine.4260-19
37. Hu Q, Hasuda H, Ueki K, Tsuchimoto A, Zaitsu Y, Tsuda Y, et al. Reintroduction of nivolumab in a patient with gastric cancer after improvement of nivolumab-induced acute interstitial nephritis: a case report. Int Cancer Conf J (2020) 9:127–32. doi: 10.1007/s13691-020-00418-2
38. Sise ME, Seethapathy H, Reynolds KL. Diagnosis and management of immune checkpoint inhibitor-associated renal toxicity: illustrative case and review. Oncologist (2019) 24:735–42. doi: 10.1634/theoncologist.2018-0764
39. Moliz C, Cavero T, Morales E, Gutiérrez E, Alonso M, Praga M. Renal damage secondary to check-point inhibitors. Nefrologia (2020) 40:206–8. doi: 10.1016/j.nefro.2019.05.004
40. Mukherjee A, Ghosh R. Pembrolizumab induced acute tubulointerstitial nephritis. Am J Ther (2022) 29(6):e722-e724. doi: 10.1097/MJT.0000000000001248
41. Thajudeen B, Madhrira M, Bracamonte E, Cranmer LD. Ipilimumab granulomatous interstitial nephritis. Am J Ther (2015) 22:e84–7. doi: 10.1097/MJT.0b013e3182a32ddc
42. Do TVC, Gudipati MK, Ganti SS, Depa J, Sajnani K. Immunotherapy: A case series. Cureus (2021) 13:e19726. doi: 10.7759/cureus.19726
43. Mitarai Y, Nakashima K, Fukunaga S, Ishikawa N, Ito T, Tsubata Y, et al. IgA nephropathy that developed as an immune-related adverse event of pembrolizumab complicated with interstitial nephritis. Intern Med (2022) 61:2013–7. doi: 10.2169/internalmedicine.7115-21
44. Gebauer E, Bechtel-Walz W, Schell C, Erbel M, Walz G, Hermle T. Development of nivolumab/ipilimumab-associated autoimmune nephritis during steroid therapy. Case Rep Nephrol Dial (2021) 11:270–4. doi: 10.1159/000517502
45. Ai L, Gao J, Zhao S, Li Q, Cui Y-H, Liu Q, et al. Nivolumab-associated DRESS in a genetic susceptible individual. J Immunother Cancer (2021) 9. doi: 10.1136/jitc-2021-002879
46. Aratani S, Sugano T, Shimizu A, Seike M, Kashiwagi T, Gemma A, et al. Clinicopathological characteristics of kidney injury in non-small cell lung cancer patients under combination therapy including pembrolizumab. CEN Case Rep (2022) 11:97–104. doi: 10.1007/s13730-021-00636-4
47. Noto-Kadou-Kaza B, Desbuissons G, Isnard CB. Association of acute interstitial nephritis with nivolumab in renal cell carcinoma: A case report. Indian J Nephrol (2021) 31:303–6. doi: 10.4103/ijn.IJN_62_20
48. Parza K, Dao K, Patel P, Scibelli N, Mangano A, Gondal M. Immunotherapy-induced acute tubulointerstitial nephritis. Cureus (2021) 13:e15358. doi: 10.7759/cureus.15358
49. Faieta A, Dancik T. Refractory acute interstitial nephritis in the setting of nivolumab therapy. Case Rep Nephrol (2021) 2021:6640154. doi: 10.1155/2021/6640154
50. Mulroy M, Ghafouri S, Sisk A, Ribas A, Goshtaseb R, Cherry G, et al. Acute interstitial nephritis and PR3-ANCA following reintroduction of pembrolizumab: a case report. Immunotherapy (2021) 13:283–8. doi: 10.2217/imt-2020-0223
51. Patel V, Elias R, Formella J, Schwartzman W, Christie A, Cai Q, et al. Acute interstitial nephritis, a potential predictor of response to immune checkpoint inhibitors in renal cell carcinoma. J Immunother Cancer (2020) 8. doi: 10.1136/jitc-2020-001198
52. Gupta S, Short SAP, Sise ME, Prosek JM, Madhavan SM, Soler MJ, et al. Acute kidney injury in patients treated with immune checkpoint inhibitors. J Immunother Cancer (2021) 9:3467. doi: 10.1136/jitc-2021-003467
53. Kellum JA, Lameire N. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care (2013) 17:204. doi: 10.1186/cc11454
54. Forni LG, Darmon M, Ostermann M, Oudemans-van Straaten HM, Pettilä V, Prowle JR, et al. Renal recovery after acute kidney injury. Intensive Care Med (2017) 43:855–66. doi: 10.1007/s00134-017-4809-x
55. Rosner MH, Perazella MA. Acute kidney injury in patients with cancer. N Engl J Med (2017) 376:1770–81. doi: 10.1056/NEJMra1613984
56. Draibe JB, García-Carro C, Martinez-Valenzuela L, Agraz I, Fulladosa X, Bolufer M, et al. Acute tubulointerstitial nephritis induced by checkpoint inhibitors versus classical acute tubulointerstitial nephritis: are they the same disease? Clin Kidney J (2021) 14:884–90. doi: 10.1093/ckj/sfaa027
57. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med (2015) 373:23–34. doi: 10.1056/NEJMoa1504030
58. Reck M, Ciuleanu T-E, Cobo M, Schenker M, Zurawski B, Menezes J, et al. First-line nivolumab plus ipilimumab with two cycles of chemotherapy versus chemotherapy alone (four cycles) in advanced non-small-cell lung cancer: CheckMate 9LA 2-year update. ESMO Open (2021) 6:100273. doi: 10.1016/j.esmoop.2021.100273
59. Perazella MA. Drug-induced acute kidney injury. Curr Opin Crit Care (2019) 25:550–7. doi: 10.1097/MCC.0000000000000653
60. Petrelli F, Signorelli D, Ghidini M, Ghidini A, Pizzutilo EG, Ruggieri L, et al. Association of steroids use with survival in patients treated with immune checkpoint inhibitors: A systematic review and meta-analysis. Cancers (Basel) (2020) 12:546. doi: 10.3390/cancers12030546
61. Kitchlu A, Jhaveri KD, Wadhwani S, Deshpande P, Harel Z, Kishibe T, et al. A systematic review of immune checkpoint inhibitor–associated glomerular disease. Kidney Int Rep (2021) 6:66–77. doi: 10.1016/j.ekir.2020.10.002
62. Perazella MA, Shirali AC. Immune checkpoint inhibitor nephrotoxicity: what do we know and what should we do? Kidney Int (2020) 97:62–74. doi: 10.1016/j.kint.2019.07.022
63. Seethapathy H, Herrmann SM, Sise ME. Immune checkpoint inhibitors and kidney toxicity: advances in diagnosis and management. Kidney Med (2021) 3:1074–81. doi: 10.1016/j.xkme.2021.08.008
64. Brahmer JR, Lacchetti C, Schneider BJ, Atkins MB, Brassil KJ, Caterino JM, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American society of clinical oncology clinical practice guideline. J Clin Oncol (2018) 36(17):1714–68. doi: 10.1200/JCO.2017.77.6385
65. Bhatraju PK, Zelnick LR, Chinchilli VM, Moledina DG, Coca SG, Parikh CR, et al. Association between early recovery of kidney function after acute kidney injury and long-term clinical outcomes. JAMA Netw Open (2020) 3:e202682. doi: 10.1001/jamanetworkopen.2020.2682
66. Nissen T, Wynn R. The clinical case report: a review of its merits and limitations (2014). Available at: http://www.biomedcentral.com/1756-0500/7/264.
67. Gérard AO, Barbosa S, Parassol N, Andreani M, Merino D, Cremoni M, et al. Risk factors associated with immune checkpoint inhibitor–induced acute kidney injury compared with other immune-related adverse events: a case–control study. Clin Kidney J (2022) 15:1881–7. doi: 10.1093/ckj/sfac109
68. Cosmai L, Porta C, Foramitti M, Perrone V, Mollica L, Gallieni M, et al. Preventive strategies for acute kidney injury in cancer patients. Clin Kidney J (2021) 14:70–83. doi: 10.1093/ckj/sfaa127
Keywords: immune checkpoint inhibitors, cancer, acute kidney injury, acute tubulointerstitial nephritis, pooled analysis, corticosteroids, renal biopsy, chronic kidney disease
Citation: Esposito P, Bottini A, Lecini E, Cappadona F, Piaggio M, Macciò L, Genova C and Viazzi F (2023) Biopsy-proven acute tubulointerstitial nephritis in patients treated with immune checkpoint inhibitors: a pooled analysis of case reports. Front. Oncol. 13:1221135. doi: 10.3389/fonc.2023.1221135
Received: 11 May 2023; Accepted: 12 October 2023;
Published: 23 October 2023.
Edited by:
Sree Bhushan Raju, Nizam’s Institute of Medical Sciences, IndiaCopyright © 2023 Esposito, Bottini, Lecini, Cappadona, Piaggio, Macciò, Genova and Viazzi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pasquale Esposito, UGFzcXVhbGUuZXNwb3NpdG9AdW5pZ2UuaXQ=