
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 25 August 2023
Sec. Thoracic Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1220248
This article is part of the Research Topic Editor's Challenge: Dr. Sara Pilotto - Modulating Tumor-Host Interplay through Lifestyle in Lung Cancer View all 3 articles
 Lotte van der Weijst1,2†
Lotte van der Weijst1,2† Renée Bultijnck1,2*†
Renée Bultijnck1,2*† Axel Van Damme2Vincent Huybrechts1,2
Axel Van Damme2Vincent Huybrechts1,2 Marc van Eijkeren1,2
Marc van Eijkeren1,2 Yolande Lievens1,2
Yolande Lievens1,2Introduction: To better understand the impact of stereotactic body radiotherapy (SBRT) and its treatment-related toxicity on early-stage non-small cell lung cancer (ES-NSCLC) patients, we conducted the Lung PLUS study in a real-world setting.
Methods: This is a monocentric prospective longitudinal study up to 12 months post-treatment, evaluating clinician- and patient-reported toxicity (resp. CTCAE and PRO-CTCAE), health-related quality of life (HRQoL) (EORTC QLQ-C30 and LC-13), activities of daily living (HAQ-DI) and functional exercise capacity (6 Minute Walking Test (6MWT)). A mixed model approach was applied to analyze the data.
Results: At baseline, clinicians and patients (n=51) reported mostly fatigue (63% vs 79%), cough (49% vs 75%) and dyspnea (65% vs 73%) of any grade. Dyspnea (p=.041) increased over time. Meaningful clinical improvements were particularly seen in pain, fatigue, and cough. Clinician reported clinically meaningful improvements and deteriorations over time in fatigue, cough, and dyspnea. Almost at every timepoint, more people reported deterioration to the clinician than improvement in aforementioned toxicities. Overall HRQoL (p=.014), physical (p=.011) and emotional (p<.001) functioning improved over time. At baseline, patients had a moderate daily functioning score and walked an average distance of 360 meters. No statistically significant differences were found in daily functioning and exercise capacity over time.
Conclusion: Our study showed an increase in patient-reported toxicity and dyspnea, without impacting functional status, following SBRT. Overall HRQoL, physical and emotional functioning improved over time. Understanding the impact of treatment on patient-reported outcomes is crucial to identify the needs/problems of patients to enhance their HRQoL.
Lung cancer is the most deadly of all cancers worldwide and is only preceded in incidence by breast cancer (1). The majority of lung cancer patients (85%) are diagnosed with non-small cell lung cancer (NSCLC) of which 20% is detected at an early stage (ES) (2). The standard treatment for ES-NSCLC is surgery, but for those unwilling or unsuitable for surgery due to age, multiple comorbidities and/or poor physical function, stereotactic body radiotherapy (SBRT) is the standard of care (3). However, the unadjusted overall survival rates of SBRT at 1, 3 and 5 years are 83%, 57% and 41% respectively, which is lower than those historically observed in surgical candidates (2).
The poor survival rates of ES-NSCLC patients who are medically inoperable and treated with SBRT can be attributed to the fact that this patient population is often older, has multiple severe co-morbidities and a low performance status, as reported in previous studies (4). Although population-based and randomized controlled studies have proven the benefit of SBRT, the extent of this benefit in frail patients is frequently questioned (5, 6). Indeed, SBRT can lead to acute and late toxicities (7, 8), which can potentially affect the health-related quality of life (HRQoL) of these patients (9, 10). Yet, it is not always easy to disentangle toxicities from lung cancer symptoms, or even symptoms of intercurrent diseases, such as chronic obstructive lung disease (COPD) (8, 11). Whereas these symptoms and toxicities are usually clinician-scored, symptoms and toxicities directly reported by the patients may be different and more reliable. Hence, there is growing interest in patient-reported outcomes (PROMs). It has been recognized that the combination of PROMs and clinician-scored data provides more accurate knowledge of patient’s wellbeing (12).
HRQoL is an important measure of the impact of disease and treatment on patient’s overall wellbeing. It covers different aspects of a person’s life, including physical, psychological, social, sexual and spiritual functioning. However, HRQoL can be difficult to interpret because it is such a complex concept. HRQoL is often captured with PROMs (13).
Lastly, lung cancer and its treatments may also have a substantial impact on a patient’s functional and physical wellbeing, subsequently influencing their HRQoL (14). Lung cancer patients are particularly at risk for exercise intolerance, muscle fatigue, impaired lung functions and pulmonary complications (15). Furthermore, baseline physical wellbeing and physical exercise capacity are prognosticators for treatment response and survival in lung cancer (16). This may aid in decision-making regarding the most optimal therapy.
Ample research has been conducted on PROMs in ES-NSCLC patients receiving SBRT (17–25). However, none of these studies collected comprehensive data on patient-reported HRQoL, symptoms, toxicity and daily living activities along with clinician-scored toxicity data, nor were data collected in a real-world setting. Real-world evidence provides inclusive data on the heterogeneous lung cancer population. As patients receiving SBRT are characterized by poor performance status and co-morbidities, these patients are frequently excluded from clinical trials (26). The REQUITE project included a large group of ES-NSCLC patients treated with SBRT in the real-world setting, but did not collect patient-reported toxicities (9, 10). Therefore, there is a need for further research that collects comprehensive patient-reported data in a real-world setting to improve our understanding of the impact of SBRT on ES-NSCLC patients.
The Lung PLUS study is a real-life, prospective, longitudinal study that investigated PROMs (symptoms, toxicities, HRQoL and activities of daily living) along with clinician-scored symptoms and toxicity, and functional exercise capacity in ES-NSCLC patients receiving SBRT. Hereby, we present both baseline and longitudinal data related to symptoms, toxicity, HRQoL, and activities of daily living. Additionally, we compare the symptoms/toxicities scored by patients and clinicians and examine whether HRQoL and physical functioning have an impact on survival.
For this monocentric prospective, longitudinal cohort study, we recruited ES-NSCLC patients without any other malignancies in the 5 years leading up to the NSCLC diagnosis. Additionally, we only included patients with an Eastern Cooperative Oncology Group (ECOG)/World Health Organisation (WHO) performance status of ≤2, who underwent SBRT at Ghent University Hospital (GUH) in Belgium. The study was approved by GUH’s ethical committee (EC 2017/0517), and all patients provided written informed consent before enrolling in the study.
Data concerning patient and tumor characteristics were collected at baseline, whereas details regarding SBRT were obtained at the end of radiotherapy.
Patient-reported symptom and toxicity data on pain, fatigue, dyspnea, cough and dysphagia were collected with the Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE) (27).
Clinicians scored lung cancer-related symptoms (fatigue, cough and dyspnea) and radiotherapy-induced toxicities (dysphagia, esophagitis, hemoptysis, chest wall pain, pneumonitis and radiotherapy-dermatitis) with the Common Terminology Criteria for Adverse Events (CTCAE) (28).
The patient-reported and clinician-scored data collected during the baseline assessment were categorized as symptom data, while the data obtained at subsequent time points were classified as toxicity data (29).
HRQoL data was collected with the European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core 30 items (QLQ-C30) and the EORTC Quality of Life Questionnaire Lung Cancer 13 items (QLQ-LC13) (30–32). The QLQ-C30 evaluates five functional domains (physical, role, emotional, cognitive, and social), nine cancer-related symptoms, global health and quality of life. The QLQ-LC13 measures lung cancer-specific symptoms.
Data was collected from both patient-reported and clinician-scored sources prior to the initiation of radiotherapy, as well as at 1, 3, and 12 months following SBRT treatment. These specific time points were chosen as they align with the follow-up consultations that patients receive at Ghent University Hospital (GUH). Additionally, patient-reported HRQoL, functional status and toxicity data was collected at 6 and 9 months post-treatment. Functional exercise capacity was measured before the start of radiotherapy, and at 3 and 12 months with the six-minute walk test (6MWT). Participants were asked to walk self-paced for six minutes on a hard flat straight surface. The 6MWT was performed according to previously published recommendations (33).
Daily functioning was measured using the self-administered health assessment questionnaire disability index (HAQ-DI). This questionnaire evaluates activities of daily living over the past week across eight categories, including dressing and grooming, arising, eating, walking, hygiene, reaching, gripping and errands and chores. Data on specific aids, devices utilized for assistance or whether help was needed from another person were captured as well (34). Survival data, defined as the time between study inclusion and death as a result of any cause, was additionally collected. Two-year survival data was available for all patients.
Patient- and clinician-scored toxicities were calculated by subtracting baseline scores from follow-up scores.
HRQoL data of the EORTC QLQ-C30 and LC13 was calculated following the guidelines of the EORTC (31). Functional scales, global quality of life, and health status scores that are higher in value indicate better functioning. Conversely, symptom scales that have higher scores indicate a greater presence of symptoms. HRQoL data was regarded as missing if at least half of the items were missing from the EORTC QLQ-C30 and LC13 questionnaires. In the analyses, only data on the different domains and overall HRQoL was included. For the purposes of this study, a meaningful clinical important difference (MCID) was defined as a score difference of at least 10 points within a patient between 2 different time points (35).
A MCID in functional capacity was defined as any change in walking distance that exceeded the initial distance by 9.5% (36). Daily functioning status of the HAQ-DI was calculated using following the guidelines of the questionnaire (37). Data was considered missing if more than two of the eight categories were missing. The total score is between 0 and 3.0, in 0.125 increments. An increase in score indicates worsening of functioning, with 0 indicating no functional impairment and 3 indicating complete impairment. Scores of 0 to 1 are considered to represent mild to moderate difficulty, 1 to 2 moderate to severe disability, and 2 to 3 severe to very severe disability. A minimal clinically important difference was defined as 0.22 (38).
For patient, treatment, and tumor characteristics, as well as for changes from baseline, descriptive statistics were utilized. To determine statistical significance levels, the mixed model method was employed with a compound symmetry structure (39). This analytical technique was selected due to its ability to handle hierarchical and missing data, as well as repeated measurements from individual patients. A statistical significance level of p=0.05 was established to adjust for both multiple comparisons and to account for the risk of a level I error. Finally, exploratory survival analyses were conducted (based on the median) to evaluate the impact of baseline data on survival.
The Lung PLUS study enrolled 51 patients between June 2017 and December 2020. There was a male predominance (n=37; 73%) and most patients had an Eastern Cooperative Oncology Group (ECOG)/World Health Organisation (WHO) performance status of 1 (n=25; 49%). Furthermore, 35 patients (69%) had cardiovascular co-morbidities and 34 individuals (67%) had pulmonary co-morbidities. The majority of patients presented cT1bN0M0 (n=26; 51%) disease and the most commonly used fractionation schemes were 60 Gy in 3 fractions (n=18; 35%) and 60 Gy in 8 fractions (n=26; 51%). Table 1 provides an overview of patient, tumor and SBRT characteristics. Table 2 provides details on baseline HRQoL.
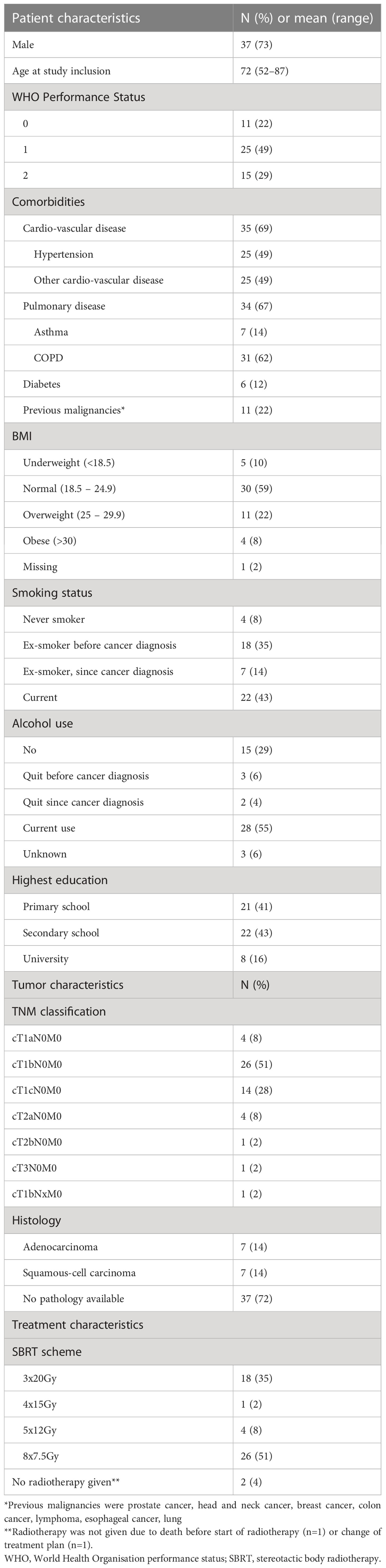
Table 1 Patient, tumor and treatment characteristics.
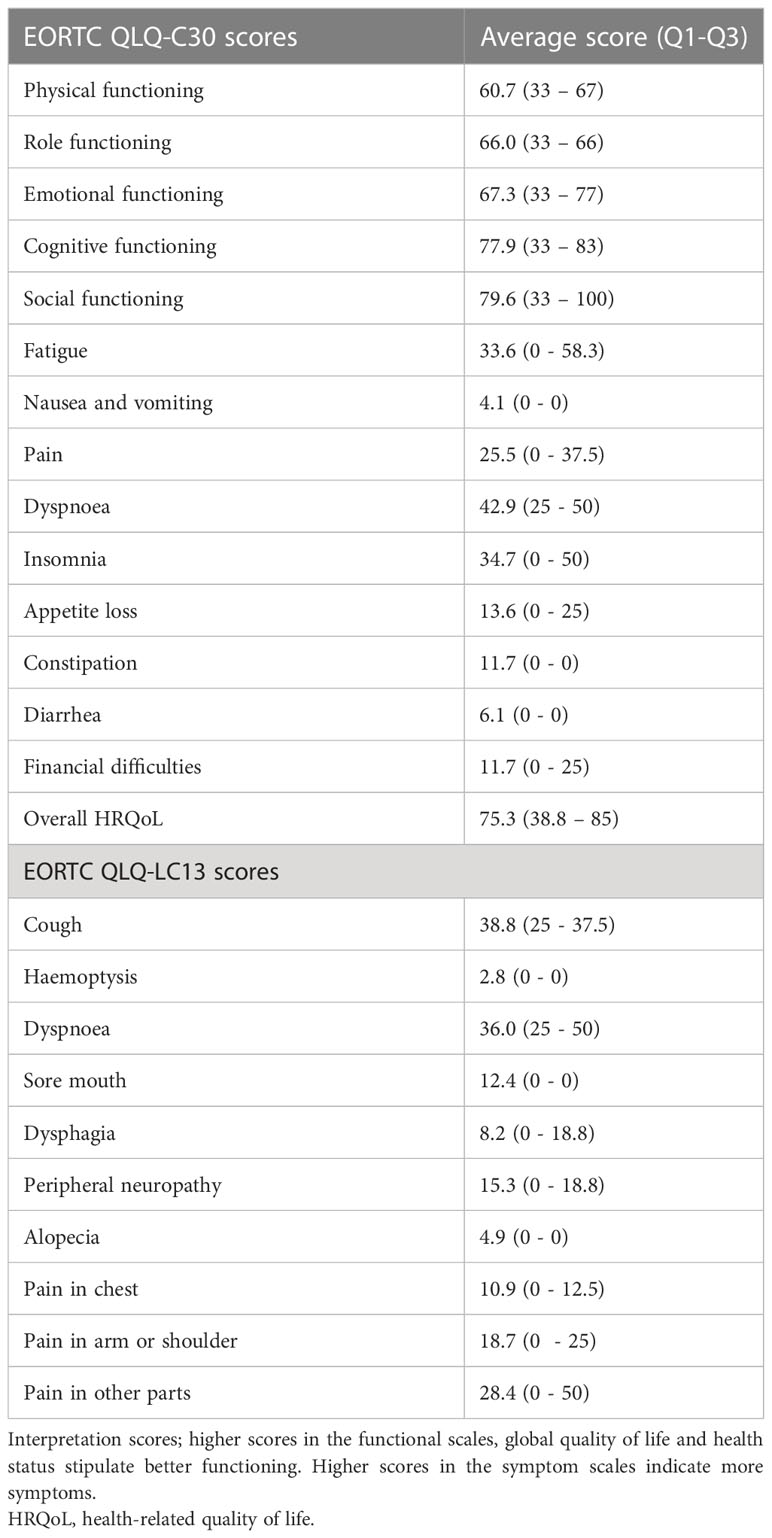
Table 2 Health-related quality of life characteristics.
The overall compliance rate for PROMs was 96% (n=49) at baseline, and 95% (n=42), 89% (n=40) and 67% (n=29) at 1-, 3- and 12-months post-radiotherapy respectively. The compliance rate with the 6MWT was substantially lower, with only 69% (n=35) of patients performing the test at baseline, 66% (n=29) at 3 months and 45% (n=20) at 12 months. The reasons for this lower compliance rate are diverse and are reported in Table 3 which provides a synopsis of the number of data collected and compliances to the study.
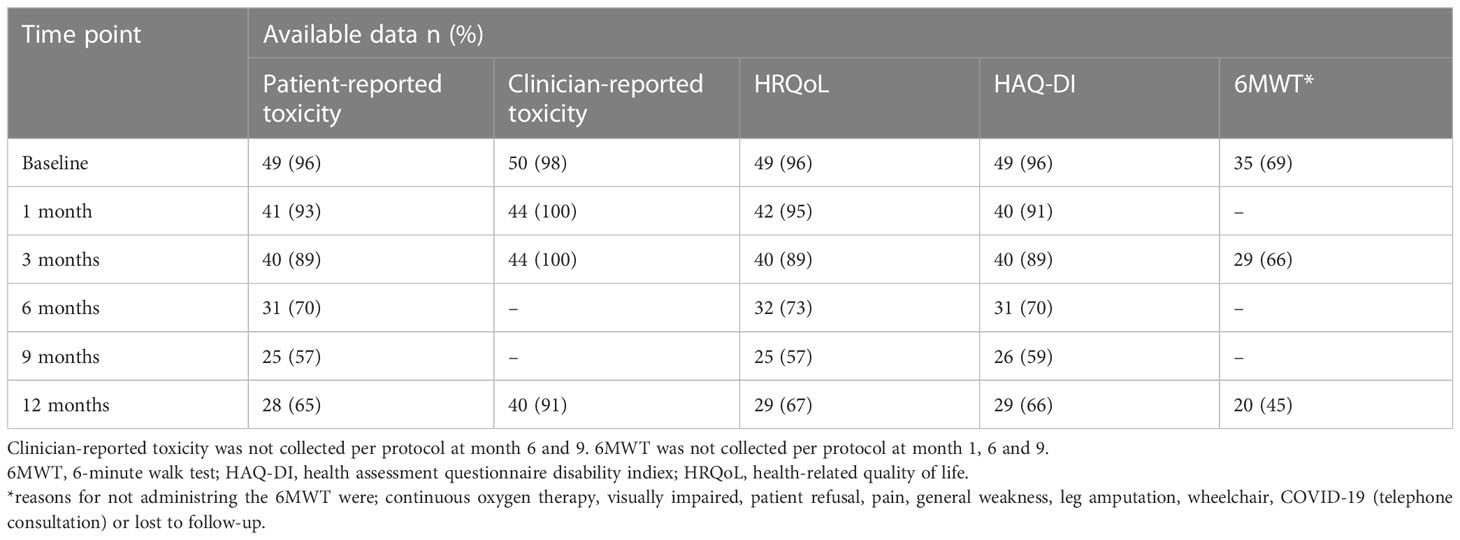
Table 3 Data availability.
At baseline, many patients reported pain (57%), fatigue (79%), cough (75%) and dyspnea (73%) of at least grade one. Baseline dysphagia was the least reported (24%). See Figure 1. for more details. Dyspnea (p=0.041) significantly increased over time, whereas pain (p=0.087), fatigue (p=0.275), cough (p=0.175) and dysphagia (p=0.641) remained stable. In terms of MCIDs, particularly pain, fatigue and cough improved significantly over time. At the 1 month post-treatment mark, dyspnea showed greater deterioration in comparison to other areas of improvement. However, at both the 3 and 12 month post-treatment marks, more improvement than deterioration was observed. Dysphagia, on the other hand, was not frequently reported and generally showed improvement by the 12 month mark.
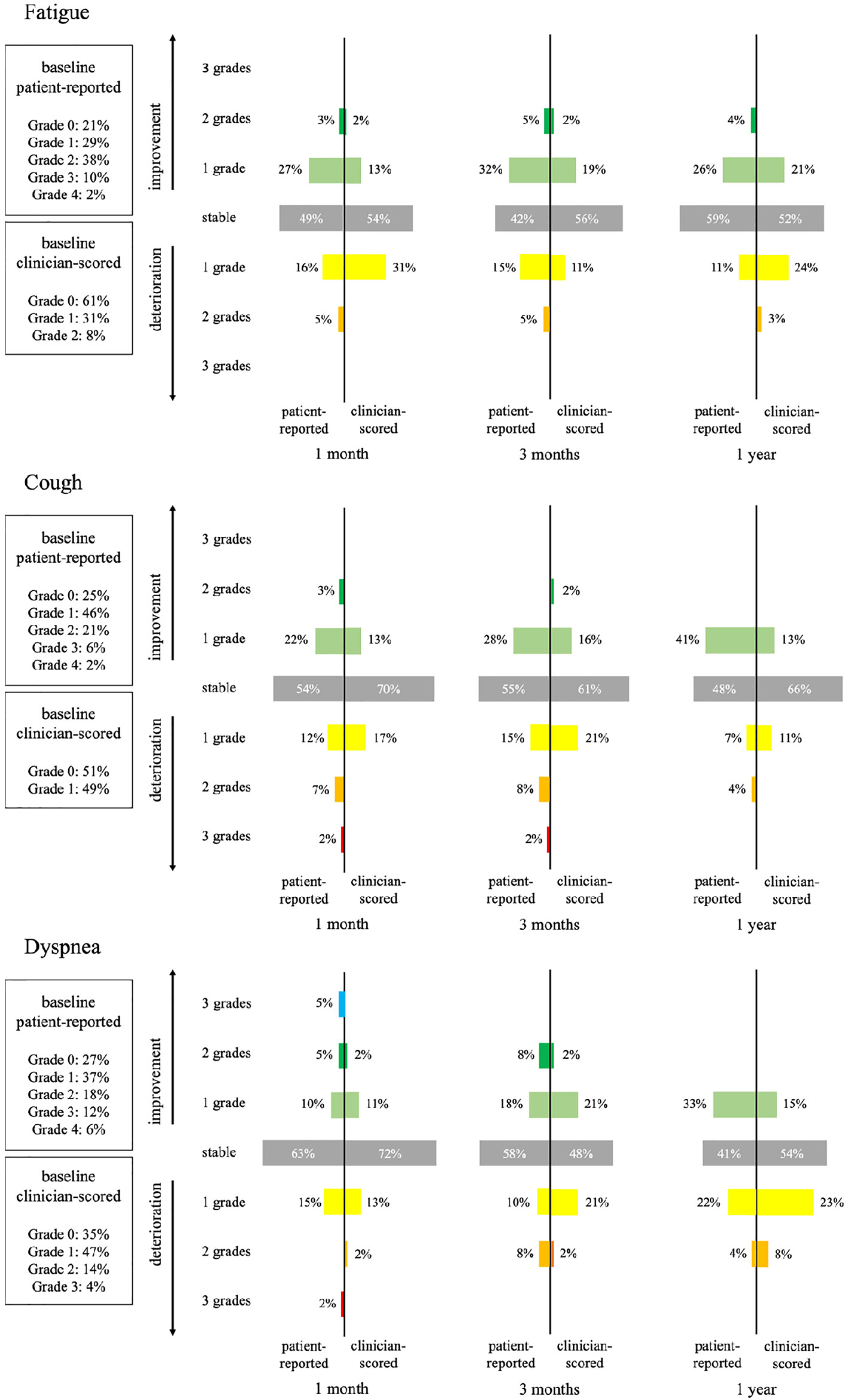
Figure 1 Comparison of patient-reported and clinician-scored toxicity: fatigue, cough and dyspnea.
At baseline, clinicians noted mostly fatigue (63%), cough (49%) and dyspnea (65%). The other symptoms were rarely reported. An overview of the comparison of patient-reported and clinician-scored symptoms and toxicities for fatigue, cough and dyspnea can be found in Figure 1. Clinicians reported fewer symptoms/toxicity than patients.
With regards to clinical significance, fatigue, cough, and dyspnea showed both improvement and deterioration over time. At nearly every time point, more clinicians reported deterioration than improvement in these toxicities. At three months, there were no patients with an increase in dyspnea after SBRT that had progressive disease. At 12 months 15% (2 out of 13) in the patients with an increase of dyspnea after SBRT had progressive disease.
Although chest wall pain and pneumonitis were not commonly reported at baseline, a small percentage of patients experienced these toxicities after receiving radiotherapy. Radiation dermatitis was observed in a relatively small number of patients and occurred particularly at the 1 month post-treatment mark.
At baseline, the average overall score of HRQoL was 75. The poorest score was reported for physical (61) and role (66) functioning. The most severe symptoms were dyspnea (43/36 on the QLQ-C30 and LC13 respectively) and cough (39) and insomnia (35) on the QLQ-LC13 module.
Overall HRQoL (p=0.014), physical (p=0.011) and emotional (p<.001) functioning improved significantly over time, whereas the other domains (role (p=.606), cognitive (p=.076) and social functioning (p=0.570) remained stable. When considering MCID, improvements over time were primarily observed in overall HRQoL and physical functioning, while the deterioration of emotional functioning decreased over time. For an overview of MCID for overall HRQoL and its associated domains, please refer to Figure 2.

Figure 2 Overview of MCID of HRQoL and its domains per time point. A meaningful clinical important difference (MCID) was defined as a score difference of at least 10 points within a patient between 2 different time points.
At baseline, patients had an average walking distance of 359.1 meters (±107, IQR 317-431). The distance remained relatively stable at 3 months (mean 351.1 ± 115 meters, IQR 290-412) and at 12 months (mean 350.9 ± 105 meters, IQR 287-416), with no statistically significant differences observed over time (p=0.862). Figure 3 provides an overview of MCID. No adverse events or medical conditions were observed during the tests. Four patients stopped prematurely or took a break during the test, 2 at the baseline test, one at month 3 and one at month 12.
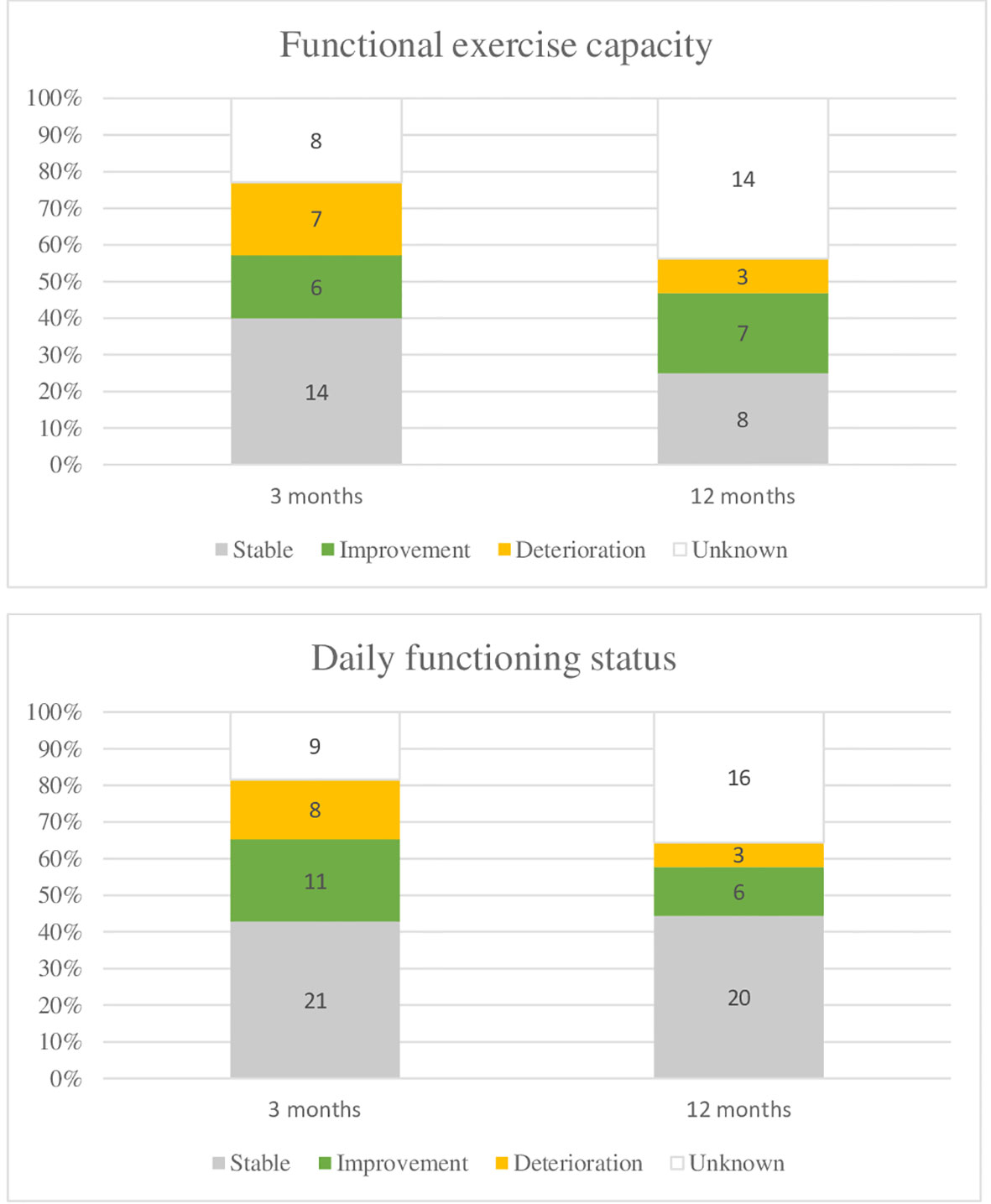
Figure 3 Evolution of functional exercise capacity and daily functioning, at 3 months and 12 months. Functional exercise capacity was measured with the six-minute walk test (6MWT), daily functioning with the health assessment questionnaire disability index (HAQ-DI). At three months, 2 patients died and at 1 year. 5 patients died. In addition, 15 resp. 14 patients were excluded from the 6MWT for a number of reasons. Lost to follow up or administrative failure was reported as unknown. The minimal clinical important difference was determined based on a 9.5% change from baseline for the 6MWT (36); for the daily functioning status, it was determined at 0.22 (38).
At baseline, an average score of daily functioning, measured with the HAQ-ID was 0.813, (IQR 0.062-1.500), while it was 0.812 (IQR 0.125-1.458) and 0.655 (IQR 0-1.312) at 3 and 12 months respectively. No statistically significant difference (p=0.435) was found in daily functioning over time. An overview of MCIDs can be found in Figure 3.
Our exploratory analyses did not show any significant results for baseline overall HRQoL (p=0.068), physical functioning (p=0.079), daily functioning (p=0.261) and exercise capacity (p=0.062). Our findings suggest that patients who reported higher baseline scores for overall HRQoL, physical and daily functioning, as well as exercise capacity, were more likely to have a favorable 1-year survival prognosis. We present exploratory survival plots in Figure 4 to further illustrate these associations.
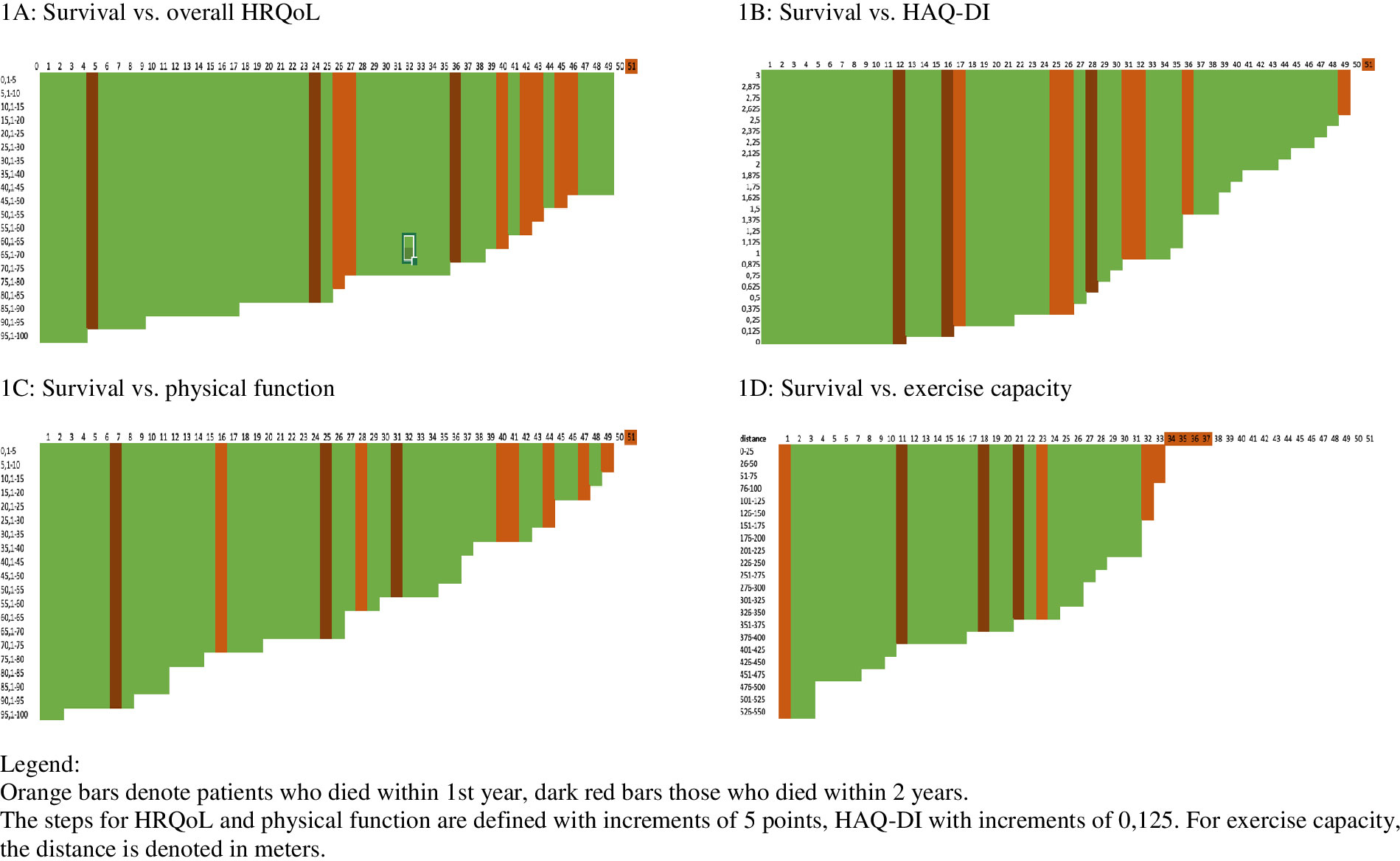
Figure 4 Survival in function of baseline overall HRQoL, physical and daily functioning and exercise capacity. x-as patient ID; y-as PRO scoring or exercise capacity score.
This study aimed to assess the symptom and toxicity scores reported by patients and clinicians, as well as patient-reported HRQoL and its associated domains among ES-NSCLC patients undergoing SBRT. This group of patients is considered vulnerable due to their poor overall and physical health, multiple co-morbidities, and high symptom burden. Thus, it is crucial to comprehend the symptoms associated with the disease, the toxicities induced by radiotherapy, and their influence on decision-making related to HRQoL.
In this study, many patients reported pre-treatment symptoms, particularly fatigue, cough and dyspnea. Fatigue is the most common symptom experienced in patients with cancer, lung and cardio-vascular disease (40, 41). Cancer-related fatigue affects approximately 65% of patients after treatment (41). Cough and dyspnea are typical symptoms of COPD, a condition present in the majority of our patients (n=31; 61%) (42). There was a significant increase in dyspnea over time. Previous studies have also reported a deterioration in dyspnea over time in ES-NSCLC patients who underwent SBRT, which is consistent with our findings (43). Dyspnea correlates with multiple medical factors, co-morbidities, tumor growth. and psychological factors, such as anxiety and depression.
On the other hand, pain, fatigue, and cough that were predominantly present before the treatment showed improvements over time. Our study observed improvements in patient-reported overall HRQoL, physical functioning, and emotional functioning. This is consistent with a previous study (n=39) in a similar patient population, which found a significant improvement in emotional functioning (p=0.002). However, that study reported that overall HRQoL, physical functioning, and respiratory symptoms remained stable. It is possible that the improvement in emotional well-being is linked to decreased anxiety and depression during follow-up (21). In contrast, Schwartz et al. (20) (n=28) found that HRQoL deteriorated after treatment, particularly the physical and mental health. The deterioration in HRQoL in those receiving SBRT was comparable to ES-NSCLC patients receiving surgery. Patients referred to SBRT for ES-NSCLC, as typical of this patient population, had a notably poorer physical and mental functioning before treatment.
Rutkowski and colleagues, using the EORTC QLQ-C30 and lung cancer module (QLQ-LC13), and concluded that physical (p=.032) and emotional functioning (p<.001) wellbeing improved significantly and clinically meaningful at 3 months in those (n=51) receiving SBRT (21). However, most improvements were seen in patients without COPD.
In terms of MCIDs in HRQoL, REQUITE, a large international cohort study, showed different results (9, 10). Whereas in our study, more patients improved in overall HRQoL, its associated domains and all functional domains over time, in the REQUITE study more patients clinically meaningfully deteriorated in overall HRQoL. One possible explanation for this is the variation in the significance placed on different aspects of HRQoL across different patient populations and cross-cultural (44).
The findings indicate that a larger proportion of patients exhibited gradual improvements in overall HRQoL and its related domains compared to deterioration. It should be noted that patients with better baseline health and HRQoL tend to have a more favorable prognosis and are less likely to drop out of the study. Therefore, the results of this study may primarily apply to individuals with higher baseline performance status and overall health.
The results of the 6MWT, which assesses functional exercise capacity, confirm the vulnerability of our patient population. The average walking distance at baseline was 359 meters. Previous research in a similar population (n=306, inoperable NSCLC patients) has also shown comparable results, with an average of 307 meters at baseline (45). However, these results are lower compared to pre-operative lung cancer patients (n=50) who are eligible for surgery (e.g., an average of 477 meters, IQR 417-536) (46) or other tumor groups (an average of 594 meters, as seen in a study of n=50, both curative and palliative breast and colorectal cancer) (47). Previous research has shown the potential predictive value of this simple, safe, and inexpensive 6MWT on survival. They have demonstrated a cut-off distance of 525 meters to distinguish between the group of lung cancer patients eligible for surgery with better long-term survival and those with worse long-term survival (16). In our cohort, only 3 patients had a walking distance above this threshold, which further highlights the vulnerability of our population compared to those suitable for surgery. Additionally, our exploratory survival analyses did not show significant results, but suggest that patients with a low walking distance on the 6MWT or those unable to perform the test may have a worse survival. Therefore, future research should investigate the potential predictive value of the 6MWT and determine the corresponding threshold for specifically ES-NSCLC receiving SBRT.
PROMs were used to collect symptom, toxicity and HRQoL data. The advantages of PROMs are well-known (48, 49). A discrepancy between patient- and clinician-scored symptoms/toxicities has been noted, particularly regarding symptomatic toxicities such as fatigue (12), and PROMs seem to detect potentially serious symptoms earlier than clinician reporting (50). Thus, both patient and clinician-scored, as collected in this study, data are important to provide a more accurate understanding of patient’s underlying health status and functional status.
We noted discrepancies between patient and clinician-reported outcomes with the largest difference in cough (75% vs 49% for patients vs clinicians respectively) at baseline. It is known that clinicians may underreport symptoms, particularly the more subjective symptoms such as fatigue (12).
This study evaluated both statistical significance levels and MCID to determine the changes in HRQoL over time. Statistical significance levels evaluate the reliability of the data and estimate the probability that the differences in the observed size could be because of a sampling error (51). Statistical significance lacks capture of the clinical importance of the data. MCID refers to what patients perceive as beneficial and would mandate a change in patient management. As data can be statistically non-significant due to insufficient power, MCID data can provide the real-world effects of an intervention and whether it is perceived as beneficial by the patient (52).
To distinguish between pre-existing symptoms and treatment-induced toxicity. Regarding toxicity data, changes over time were calculated for toxicity data by subtracting the baseline data from subsequent data. This differentiation is important as certain symptoms related to the tumor and co-morbidities may be alleviated by treatment, whereas other toxicities may emerge due to treatment. As pulmonary symptoms are commonly reported in lung cancer patients, it is crucial to understand the impact of treatment in alleviating symptoms to facilitate informed decision-making in this vulnerable patient population.
Data was collected in a real-world setting. Real-world evidence refers to data routinely collected from daily clinical practice. As randomized-controlled trials apply strict inclusion and exclusion criteria, often excluding patients with poor performance status and multiple co-morbidities, real-world studies provide comprehensive data on a larger patient population. This study aimed to provide data on ES-NSCLC patients, a group that is characterized by poor performance status, overall health, and a multitude of pulmonary and cardiovascular co-morbidities and is therefore often excluded from clinical trials. The aim was to collect data on the standard treatment for ES-NSCLC patients ineligible or unwilling to undergo surgery and to provide evidence applicable to most of this patient population.
Future research should focus on obtaining additional real-world data in this heterogeneous patient population, as this is rather an explorative study due to the small sample size. Prospective real-world data is needed to complement safety and efficacy data from clinical trials. The introduction of new treatments, such as immunotherapy, in this patient cohorts calls for more clinical trial and real-world data. Currently, no HRQoL and patient-reported toxicity data is available in ES-NSCLC patients receiving SBRT and immunotherapy in daily clinical practice. Data collection was difficult, due to the COVID-19 pandemic and to patients’ health deterioration and death. More research is needed to ensure high completion rates in this vulnerable populations and electronic data collection possibilities should be explored.
There are several limitations to this study. Firstly, recruitment was slow due to the introduction of new studies, particularly those involving immunotherapy. Secondly, missing data was a problem. Due to the emergence of COVID-19, consultations were frequently conducted over the phone, which increased the likelihood of missing data since patients were asked to fill out PROMs through the post. Additionally, missing data occurred due to patients’ health deterioration and death.
The results from this study are mostly applicable to those with better pre- and post-treatment health. The small sample size and the data collection from only one hospital may limit the generalizability of the findings.
To summarize, this study found that dyspnea increased over time while certain pre-existing symptoms improved and new toxicities emerged following SBRT. Clinicians mostly reported fatigue, cough, and dyspnea, and reported less toxicity than patients. Patient-reported overall HRQoL, physical, and emotional functioning significantly improved over time, with some patients experiencing meaningful improvements and deteriorations in these domains. Results of the 6MWT remained stable over time but were relatively lower compared to other treatment and tumor groups for those able and willing to conduct the test. ES-NSCLC patients ineligible for surgery are typically older with multiple co-morbidities and poor performance status, so it is important to consider the impact of treatment on symptoms, toxicities, functioning, and HRQoL in making treatment decisions for this vulnerable population. However, this study had limitations, such as slow recruitment and missing data due to COVID-19 and patient deterioration. The data may be more applicable to those with better pre- and post-treatment health, and the small sample size and single hospital data collection further limit generalizability.
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials. Raw data were generated at Ghent University Hospital. The raw data are not publicly available due to privacy and ethics restrictions. Raw data supporting the findings of this study are available from the corresponding author [RB] upon reasonable request.
The studies involving human participants were reviewed and approved by Commissie voor medische ethiek | UZ Gent (2017/0517). The patients/participants provided their written informed consent to participate in this study.
Conceptualization: RB, LW, and YL. Methodology: RB, LW, and YL. Formal analysis: RB and LW. Data curation: RB and LW. Investigation: all authors. Project administration: RB and LW. Resources: RB and LW. Validation: RB, LW, and YL. Visualization: RB, LW, and YL. Writing – original draft preparation: RB, LW, and YL. Writing – review & editing: VH, AV, and ME. Supervision: LY. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clin (2021) 71(3):caac.21660. doi: 10.3322/caac.21660
2. Zheng X, Schipper M, Kidwell K, Lin J, Reddy R, Ren Y, et al. Survival outcome after stereotactic body radiation therapy and surgery for stage i non-small cell lung cancer: A meta-analysis. Int J Radiat Oncol Biol Phys (2014) 90:603–11. doi: 10.1016/j.ijrobp.2014.05.055
3. Postmus PE, Kerr KM, Oudkerk M, Senan S, Waller DA, Vansteenkiste J, et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2017) 28:iv1–iv21. doi: 10.1093/annonc/mdx222
4. Turzer M, Brustugun OT, Waldeland E, Helland Å Stereotactic body radiation therapy is effective and safe in patients with early-stage non-small cell lung cancer with low performance status and severe comorbidity. Case Rep Oncol (2011) 4:25–34 doi: 10.1159/000324113
5. Ball D, Thursfield V, Irving L, Mitchell P, Richardson G, Torn-Broers Y, et al. Evaluation of the Simplified Comorbidity Score (Colinet) as a prognostic indicator for patients with lung cancer: A cancer registry study. Lung Cancer (2013) 82:358–61. doi: 10.1016/j.lungcan.2013.08.011
6. Palma DA, Louie AV, Rodrigues GB. New strategies in stereotactic radiotherapy for oligometastases. Clin Cancer Res (2015) 21:5198–204. doi: 10.1158/1078-0432.CCR-15-0822
7. Thompson M, Rosenzweig KE. The evolving toxicity profile of SBRT for lung cancer. Transl Lung Cancer Res (2018) 8:48–57. doi: 10.21037/tlcr.2018.10.06
8. Van der Weijst L, Aguado-Barrera ME, Azria D, Berkovic P, Boisselier P, Briers E, et al. Overview of health-related quality of life and toxicity of non-small cell lung cancer patients receiving curative-intent radiotherapy in a real-life setting (the REQUITE study). Lung Cancer (2022) 166:228–41. doi: 10.1016/j.lungcan.2022.03.010
9. Ubels RJRJ, Mokhles S, Andrinopoulou ERER, Braat C, van Zyp NC van der V, Aluwini S, et al. Quality of life during 5 years after stereotactic radiotherapy in stage I non-small cell lung cancer. Radiat Oncol (London England) (2015) 10:98. doi: 10.1186/s13014-015-0405-9
10. van der Weijst L, Azria D, Berkovic P, Boisselier P, Briers E, Bultijnck R, et al. The correlation between pre-treatment symptoms, acute and late toxicity and patient-reported health-related quality of life in non-small cell lung cancer patients: results of the REQUITE study. Radiotherapy Oncol (2022) 176:127–37. doi: 10.1016/j.radonc.2022.09.020
11. Seibold P, Webb A, Aguado-barrera ME, Azria D, Bourgier C, Brengues M, et al. REQUITE: a prospective multicentre cohort study of patients undergoing radiotherapy for breast, lung or prostate cancer. Radiat Oncol (2019) 138:59–67. doi: 10.1016/j.radonc.2019.04.034.
12. Basch E, Bennett A, Pietanza MC. Use of patient-reported outcomes to improve the predictive accuracy of clinician-reported adverse events. JNCI J Natl Cancer Institute (2011) 103:1808–10. doi: 10.1093/jnci/djr493
13. Fayers PM, Machin D. Quality of Life Vol. 401. West Sussex, England: John Wiley & Sons Ltd (2000). doi: 10.1002/0470846283
14. Kasymjanova G, Grossman M, Tran T, Jagoe RT, Cohen V, Pepe C, et al. The potential role for acupuncture in treating symptoms in patients with lung cancer: an observational longitudinal study. Curr Oncol (2013) 20:152–7. doi: 10.3747/co.20.1312
15. Rivas-Perez H, Nana-Sinkam P. Integrating pulmonary rehabilitation into the multidisciplinary management of lung cancer: A review. Respir Med (2015) 109:437–42. doi: 10.1016/j.rmed.2015.01.001
16. Marjanski T, Badocha M, Wnuk D, Dziedzic R, Ostrowski M, Sawicka W, et al. Result of the 6-min walk test is an independent prognostic factor of surgically treated non-small-cell lung cancer. Interactive Cardiovasc Thorac Surg (2019) 28:368–74. doi: 10.1093/icvts/ivy258
17. Vogel J, Simone CB. Patient-reported outcomes with stereotactic body radiotherapy and surgery for lung cancer. Clin Lung Cancer (2020) 21:e229–30. doi: 10.1016/j.cllc.2019.12.004
18. Alberts L, Wolff HB, Kastelijn EA, Lagerwaard FJ, Hofman FN, Sharouni SYE, et al. Patient-reported outcomes after the treatment of early stage non–small-cell lung cancer with stereotactic body radiotherapy compared with surgery. Clin Lung Cancer (2019) 20:370–377.e3. doi: 10.1016/j.cllc.2019.04.001
19. van der Voort van Zyp NC, Prévost J-B, van der Holt B, Braat C, van Klaveren RJ, Pattynama PM, et al. Quality of life after stereotactic radiotherapy for stage I non-small-cell lung cancer. Int J Radiat OncologyBiologyPhysics (2010) 77:31–7. doi: 10.1016/j.ijrobp.2009.04.080
20. Schwartz RM, Alpert N, Rosenzweig K, Flores R, Taioli E. Changes in quality of life after surgery or radiotherapy in early-stage lung cancer. J Thorac Dis (2019) 11:154–61. doi: 10.21037/jtd.2018.12.30
21. Rutkowski J, Szymanik M, Blok M, Kozaka J, Zaucha R. Prospective evaluation of anxiety, depression and quality of life in medically inoperable early stage non-small cell lung cancer patients treated with stereotactic ablative radiotherapy. Rep Pract Oncol Radiotherapy (2017) 22:217–22. doi: 10.1016/j.rpor.2017.01.002
22. Adebahr S, Hechtner M, Schräder N, Schimek-Jasch T, Kaier K, Duncker-Rohr V, et al. Early impact of pulmonary fractionated stereotactic body radiotherapy on quality of life:Benefit for patients with low initial scores (STRIPE trial). J Thorac Oncol (2019) 14:408–19. doi: 10.1016/j.jtho.2018.10.170
23. Ferrero C, Badellino S, Filippi AR, Focaraccio L, Giaj Levra M, Levis M, et al. Pulmonary function and quality of life after VMAT-based stereotactic ablative radiotherapy for early stage inoperable NSCLC: a prospective study. Lung Cancer (2015) 89:350–6. doi: 10.1016/j.lungcan.2015.06.019
24. Lagerwaard FJFJ, Aaronson NKNK, Gundy CMCM, Haasbeek CJACJA, Slotman BJBJ, Senan S. Patient-reported quality of life after stereotactic ablative radiotherapy for early-stage lung cancer. J Thorac Oncol (2012) 7:1148–54. doi: 10.1097/JTO.0b013e318252cfef
25. Videtic GMMGMM, Reddy CA, Sorenson L. A prospective study of quality of life including fatigue and pulmonary function after stereotactic body radiotherapy for medically inoperable early-stage lung cancer. Supportive Care Cancer (2013) 21:211–8. doi: 10.1007/s00520-012-1513-9
26. Elting LS, Cooksley C, Bekele BN, Frumovitz M, Avritscher EBC, Sun C, et al. Generalizability of cancer clinical trial results: Prognostic differences between participants and nonparticipants. Cancer (2006) 106:2452–8. doi: 10.1002/cncr.21907
27. Basch E, Reeve BB, Mitchell SA, Clauser SB, Minasian LM, Dueck AC, et al. Development of the national cancer institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Institute (2014) 106:1-11. doi: 10.1093/jnci/dju244
28. Common Terminology Criteria for Adverse Events. (CTCAE), Vol. 147. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES, National Institutes of Health, National Cancer Institute (2017).
29. De Ruysscher D, Dehing C, Yu S, Wanders R, Öllers M, Dingemans AMC, et al. Dyspnea evolution after high-dose radiotherapy in patients with non-small cell lung cancer. Radiotherapy Oncol (2009) 91:353–9. doi: 10.1016/j.radonc.2008.10.006
30. Groenvold M, Klee MC, Sprangers M a. G, Aaronson NK. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol (1997) 50:441–50. doi: 10.1016/S0895-4356(96)00428-3
31. Aaronson N, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organistaion for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Institute (1993) 85:365–76. doi: 10.1093/jnci/85.5.365
32. Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC Core Quality of Life Questionnaire (QLQ-C30) for use in lung cancer clinical trials. EORTC Study Group on Quality of Life. Eur J Cancer (1994) 30A:635–42. doi: 10.1016/j.ejca.2010.08.021
33. Holland AE, Spruit MA, Troosters T, Puhan MA, Pepin V, Saey D, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J (2014) 44:1428–46. doi: 10.1183/09031936.00150314
34. Maska L, Anderson J, Michaud K. Measures of functional status and quality of life in rheumatoid arthritis: Health Assessment Questionnaire Disability Index (HAQ), Modified Health Assessment Questionnaire (MHAQ), Multidimensional Health Assessment Questionnaire (MDHAQ), Health Assessment Questionnaire II (HAQ-II), Improved Health Assessment Questionnaire (Improved HAQ), and Rheumatoid Arthritis Quality of Life (RAQoL). Arthritis Care Res (2011) 63:S4–S13. doi: 10.1002/acr.20620
35. Osoba D. Health-related quality of life and cancer clinical trials. Ther Adv Med Oncol (2011) 3:57–71. doi: 10.1177/1758834010395342
36. Granger CL, Holland AE, Gordon IR, Denehy L. Minimal important difference of the 6-minute walk distance in lung cancer. Chron Respir Dis (2015) 12:146–54. doi: 10.1177/1479972315575715
37. Stanford University School of Medicine Division of Immunology & Rheumatology. THE HEALTH ASSESSMENT QUESTIONNAIRE. Available from https://www.nvr.nl/wp-content/uploads/2018/07/HAQ-Instructions.pdf.
38. Bruce B, Fries JF. The stanford health assessment questionnaire: dimensions and practical applications. Health Qual Life Outcomes (2003) 1. doi: 10.1186/1477-7525-1-20
39. Hamel J-F, Saulnier P, Pe M, Zikos E, Musoro J, Coens C, et al. A systematic review of the quality of statistical methods employed for analysing quality of life data in cancer randomised controlled trials. Eur J Cancer (2017) 83:166–76. doi: 10.1016/j.ejca.2017.06.025
40. Hinz A, Weis J, Brähler E, Härter M, Geue K, Ernst J. Fatigue in cancer patients: comparison with the general population and prognostic factors. Support Care Cancer (2020) 28:4517–26. doi: 10.1007/s00520-019-05260-8
41. Fabi A, Bhargava R, Fatigoni S, Guglielmo M, Horneber M, Roila F, et al. Cancer-related fatigue: ESMO Clinical Practice Guidelines for diagnosis and treatment. Ann Oncol (2020) 31:713–23. doi: 10.1016/j.annonc.2020.02.016
42. Miravitlles M, Ribera A. Understanding the impact of symptoms on the burden of COPD. Respir Res (2017) 18:67. doi: 10.1186/s12931-017-0548-3
43. Widder J, Postmus D, Ubbels JF, Wiegman EM, Langendijk JA. Survival and quality of life after stereotactic or 3D-Conformal radiotherapy for inoperable early-stage lung cancer. Int J Radiat Oncol Biol Phys (2011) 81:E291–7. doi: 10.1016/j.ijrobp.2011.03.052
44. Molzahn AE, Kalfoss M, Schick Makaroff K, Skevington SM. Comparing the importance of different aspects of quality of life to older adults across diverse cultures. Age Ageing (2011) 40:192–9. doi: 10.1093/ageing/afq156
45. Goldsmith I, Chesterfield-Thomas G, Toghill H. Pre-treatment optimization with pulmonary rehabilitation in lung cancer: Making the inoperable patients operable. EClinicalMedicine (2021) 31:100663. doi: 10.1016/j.eclinm.2020.100663
46. Jonsson M, Hurtig-Wennlöf A, Ahlsson A, Vidlund M, Cao Y, Westerdahl E. In-hospital physiotherapy improves physical activity level after lung cancer surgery: a randomized controlled trial. Physiotherapy (2019) 105:434–41. doi: 10.1016/j.physio.2018.11.001
47. Schmidt K, Vogt L, Thiel C, Jäger E, Banzer W. Validity of the six-minute walk test in cancer patients. Int J Sports Med (2013) 34:631–6. doi: 10.1055/s-0032-1323746
48. Weldring T, Smith SMS. Article commentary: patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs). Health Serv Insights (2013) 6:HSI.S11093. doi: 10.4137/HSI.S11093
49. Black N. Patient reported outcome measures could help transform healthcare. BMJ (Online) (2013) 346:1–5. doi: 10.1136/bmj.f167
50. Denis F, Lethrosne C, Pourel N, Molinier O, Pointreau Y, Domont J, et al. Randomized trial comparing a web-mediated follow-up with routine surveillance in lung cancer patients. J Natl Cancer Institute (2017) 109:1–8. doi: 10.1093/jnci/djx029
51. Houle TT, Stump DA. Statistical significance versus clinical significance. Semin Cardiothorac Vasc Anesth (2008) 12:5–6. doi: 10.1177/1089253208316440
Keywords: health-related quality of life, non-small cell lung cancer, patient-reported outcomes, radiotherapy, toxicity
Citation: van der Weijst L, Bultijnck R, Van Damme A, Huybrechts V, van Eijkeren M and Lievens Y (2023) Patient-reported outcomes and functional exercise capacity in a real-life setting in non-small cell lung cancer patients undergoing stereotactic body radiotherapy: the Lung PLUS study. Front. Oncol. 13:1220248. doi: 10.3389/fonc.2023.1220248
Received: 10 May 2023; Accepted: 18 July 2023;
Published: 25 August 2023.
Edited by:
Carlos Gil Ferreira, Instituto Oncoclínicas, BrazilReviewed by:
Signe Friesland, Karolinska University Hospital, SwedenCopyright © 2023 van der Weijst, Bultijnck, Van Damme, Huybrechts, van Eijkeren and Lievens. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Renée Bultijnck, cmVuZWUuYnVsdGlqbmNrQHVnZW50LmJl
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.