 Annalisa Arcari
Annalisa Arcari Federica Cavallo
Federica Cavallo Benedetta Puccini3
Benedetta Puccini3
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol. , 03 July 2023
Sec. Hematologic Malignancies
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1214026
This article is part of the Research Topic Implementation of Novel Drugs and Modern Radiotherapy in the Treatment of Lymphoma Patients View all 7 articles
Most patients with Diffuse Large B-cell Lymphoma (DLBCL) are old (>65 years of age) and this population is expected to increase in the following years. A simplified geriatric assessment based on a careful evaluation of the fitness status and comorbidities is essential to choose the correct intensity of treatment. Fit older patients can benefit from a standard immunochemotherapy, while unfit/frail patients frequently need reduced doses or substitution of particular agents with less toxic ones. This review focuses on new therapies (e.g., polatuzumab vedotin, tafasitamab, bispecific antibodies) that have indicated promising results in relapsed/refractory patients, particularly in cases not eligible to transplant. Some of these new drugs have been tested as single agents or in combinations as first-line treatment, aiming to improve the outcome of the traditional chemotherapy. If preliminary efficacy and safety data are confirmed in future clinical trials, a chemo-free immunotherapic approach could become an alternative option to offer a curative treatment even in frail patients.
Diffuse Large B-cell Lymphoma (DLBCL) is the most frequent lymphoma subtype with a median age at diagnosis of 66 years (1). With the aging of the general population in Western countries, the number of old patients with lymphoma will continually increase, requiring specific considerations (2). Common issues in the treatment of geriatric patients are related to comorbidities and limited organ reserve (e.g., bone marrow, liver, and kidney) with a higher risk of toxicity. Clinicians should also consider issues related to impaired physical and/or cognitive functions that may compromise, especially in the absence of a care giver, the possibility to reach the hospital and to manage therapies at home. Besides factors regarding patients’ fitness status, an unfavorable biology of the disease may also contribute to an inferior outcome. DLBCLs in older patients are characterized by a higher prevalence of activated B-cell (ABC) subtypes and EBV-positive cases (3). The global prognosis of older DLBCL patients has certainly improved in the last few years thanks to immunochemotherapy combinations but is still poorer than in younger patients. Older patients are under-represented in clinical studies, particularly in clinical trials leading to marketing authorization of new cancer therapies (4).
Treating elderly patients with aggressive lymphoma poses the clinical dilemma of balancing a potential cure while minimizing toxicity. Age per se is not a contraindication to a full-dose curative treatment, but comorbid conditions and impaired functional status may often suggest a reduced dose and/or drugs substitution to improve tolerance. Elderly patients present a wide heterogeneity and traditional measures of performance status are not accurate enough to define treatment goals and to tailor treatment intensity. The ESMO guidelines recommend the application of a geriatric assessment to avoid the risk of undertreatment or overtreatment (5). The Fondazione Italiana Linfomi (FIL) has recently validated in a large prospective series of DLBCL patients older than 64 years –the Elderly Project- a simplified geriatric assessment (sGA) based on age (≥ or < 80 years), Cumulative Illness Rating Scale for Geriatrics (CIRS-G), activities of daily living (ADL), and instrumental activities of daily living (IADL) (6). This sGA is an objective, reproducible tool that can be easily managed by onco-hematologists (in less than 10 minutes) and permits to classify older patients as fit (55%), unfit (28%) or frail (18%), with significantly different outcomes.
The aim of the first-line treatment in fit patients up to 80 years old should be curative, with a full dose anthracycline-based regimen. R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) has been the standard initial therapy for more than 20 years (7). Attempts in improving the outcome of R-CHOP by adding new biological agents to immunochemotherapy, especially in non-GCB DLBCL, have failed to show a significant advantage (8). The PHOENIX trial did not demonstrate an improvement of event-free survival adding ibrutinib to R-CHOP in newly diagnosed non-GCB DLBCL; in patients > 60 years ibrutinib plus R CHOP was associated with an increase of toxicity, leading to a compromised R-CHOP administration and worse outcome (9). The ROBUST trial also failed to demonstrate an improvement with the combination of lenalidomide plus R-CHOP in untreated patients with ABC-type DLBCL (10).
The POLARIX study is the only randomised phase III trial in DLBCL which has shown a significant improvement so far of the progression-free survival (PFS) (11). In this trial, polatuzumab vedotin, an antibody-drug-conjugated targeting CD79b, replaced vincristine in the R-CHOP scheme. The new pola-R-CHP regimen showed a 2-year PFS of 76.7% compared to 70.2% of standard R-CHOP in intermediate-risk or high-risk DLBCL patients aged 18-80 years, with similar safety profiles. The overall survival (OS) rate at 2 years did not differ significantly (88.7% in the pola-R-CHP group versus 88.6% in the R-CHOP group). An exploratory subgroup analysis highlighted a stronger benefit in patients > 60 years, non-GCB types, double expressors, and high IPI (3–5). Considering the modest PFS advantage of pola-R-CHP and the equal OS, there are some concerns about a wide application of this regimen. Pola-R-CHP is a good option especially in specific patient subgroups, but probably R-CHOP will remain a standard arm in future clinical trials and a valid backbone for new combinations.
Most patients with high grade B-cell lymphoma (double or triple hit) are currently treated with the dose-adjusted R-EPOCH (rituximab, etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin) regimen. However, this intensive therapy may not be suitable for patients older than 80 years and those < 80 years but with significant comorbidities (12, 13). For double/triple expressors cases there are no advantages using R-DA EPOCH in patients > 65 years (14).
Unfit and frail patients mostly require an adapted therapy. The R-miniCHOP regimen can be considered the standard first-line treatment for DLBCL patients >80 years without severe comorbidities, with a 2-year PFS of 47% and a 2-year OS of 59% (15). The LYSA group has tried to improve the results of R-miniCHOP using ofatumumab instead of rituximab (16). The outcome in terms of 2-year OS (64.7%) was only slightly better than the previous study; nevertheless, this new protocol confirmed the importance of a systematic pre-phase with prednisone and vincristine before immunochemotherapy, which permits an improvement of the performance status and a reduction of treatment-related mortality during the first cycle (17). Based on the encouraging results of the POLARIX study, the Nordic Lymphoma Group is now conducting a randomized phase III trial comparing R-miniCHOP to R-miniCHP plus polatuzumab in patients ≥80 years or ≥75 years and frail (ClinicalTrials.gov Identifier: NCT04332822).
Many older patients have cardiac comorbidity and/or multiple cardiovascular risk factors (such as diabetes, hypertension, chronic renal disease) that are known to be associated with a higher risk of cardiotoxicity from anthracyclines (18, 19). In these cases, replacing conventional doxorubicin by the non-pegylated liposomal form may reduce the risk of cardiac events with a non-inferior efficacy (20–23).
For patients with a full contraindication to anthracyclines, the ESMO guidelines suggest the substitution of doxorubicin by gemcitabine or etoposide (24). The total omission of doxorubicin (such as in the R-CVP regimen) could be an option in older frail patients but the efficacy is generally low, and this option has a palliative aim (25). Tucci et al. recently reported that, within a palliative treatment, the use of rituximab may improve the outcome (2-yr OS with or without rituximab 42% vs. 22%; P=0.008) (26).
The safety and efficacy of rituximab plus bendamustine in indolent lymphoma has prompted its evaluation as first-line treatment in older frail patients with DLBCL. In a phase II trial of 49 DLBCL patients > 70 years with significant comorbidities and/or impaired fitness status, the overall response rate (ORR) was 62% (with 53% of complete remission rate, CRR), but the PFS was disappointing (38% at 2 years) (27). The combination rituximab plus lenalidomide (R2) has been tested in the phase II ReRi study in 68 newly diagnosed DLBCL patients not eligible for conventional cytotoxic therapy. The ORR was 41%, with PFS and OS at 12 months of 55% and 69%, respectively. Although this study did not confirm its initial end point, an activity was observed in a significant proportion of cases, warranting further exploration as backbone of new chemo-free combinations in elderly frail patients (28).
A limited number of elderly patients with relapsed/refractory DLBCL are eligible to the traditional standard approach based on salvage chemotherapy (in most cases with platinum-containing regimens) followed by high-dose therapy and autologous stem cell transplantation (ASCT) in case of chemosensitive disease, ideally in complete remission at PET/CT re-staging. The superior age limit in most studies was 60 or 65 years (29, 30). Only some small retrospective series, subgroup post-hoc analysis and data from international registries have described the outcome of older patients (31–33). In general, ASCT emerges from these studies as a feasible option in selected fit elderly patients up to 75 years of age.
Chimeric antigen receptor (CAR) T-cells have recently revolutionized the treatment landscape of aggressive lymphoma. Axicabtagene ciloleucel (axi-cel), tisagenlecleucel (tisa-cel) and lisocaptagene maraleucel (liso-cel) are currently FDA approved for the treatment of relapsed/refractory DLBCL patients after at least two prior lines of therapy. The pivotal trials ZUMA-1, JULIET and TRANSCEND NHL-001 showed high response rates (ORR 52-82%, CRR 40-54%) and durable complete remissions in about one third of infused patients (34–36). A sub-analysis of older patients enrolled in the ZUMA-1 trial highlighted a similar CAR T-cells in vivo expansion and an apparently higher efficacy in patients ≥65 years compared to patients <65 years (ORR 92% vs 81%, CRR 75% vs 53%, median PFS 13.2 months vs 5.6 months); the rate of grade ≥3 cytokine release syndrome (CRS), cytopenia and infections were similar, but older patients experienced more grade ≥3 neurotoxicity (44% vs 28%) (37). Recent real-world experiences confirmed that the outcome of CAR T-cells therapy is comparable between older and younger patients, indicating that age itself should not preclude CAR T-cells administration; a careful evaluation of comorbidities, a reliable caregiver and a longer rehabilitation therapy may be essential to improve the long-term outcome (38–40). Transplant-ineligible but CAR T-eligible elderly patients could become a real and relevant population in a near future (41).
Based on the favorable results of the ZUMA-7 trial, comparing CAR T-cells to the standard of care (two or three cycles of salvage chemotherapy followed by ASCT), axi-cel has been recently approved as second-line therapy in adult patients with large B-cell lymphoma who are refractory to first-line chemoimmunotherapy or relapsed within 12 months (42). In this trial, patients aged ≥65 years were 51 (28%) in the axi-cel arm and 58 (32%) in the standard arm. In the TRANSFORM trial, liso-cel proved its superiority versus standard of care as second-line therapy in refractory or early relapsed DLBCL patients, while the BELINDA trial did not reach the same end point with tisa-cel (43, 44).
Despite a significant efficacy, many issues can limit the widespread application of CAR T-cells in clinical practice, particularly in older patients: the necessity of specialized centers that may be far from the patient’s residence, the long turnaround time from the leukapheresis to product release, and the cost of the entire treatment.
Elderly patients with relapsed/refractory DLBCL not eligible to transplant have a dismal prognosis with conventional second-line treatments such as rituximab-gemcitabine-oxaliplatin (R-GEMOX), bendamustine-rituximab (BR), pixantrone, and lenalidomide, with an ORR of 35-50% and a median PFS of 4-8.8 months (45–48).
In recent years, novel agents have emerged as potentially more effective therapies in this difficult-to treat setting (Table 1). Polatuzumab vedotin is a new antibody-drug conjugated, that delivers monomethyl auristatin E (MMAE), a microtubule inhibitor, to B-cells, targeting the CD79b antigen (49). A phase II study randomly assigned 80 patients with relapsed/refractory transplant-ineligible DLBCL to the combination polatuzumab-BR versus BR alone (50). The median number of prior lines of therapy was 2 (range 1-7) and most patients (75-85%) were refractory to the last treatment. Polatuzumab-BR showed a significantly higher CR rate (40.0% vs 17.5%), longer PFS (9.5 vs 3.7 months; p < 0.001) and OS (12.4 v 4.7 months; p = 0.002) compared to BR alone. Pola-BR patients had higher rates of hematological toxicities but similar grade 3-4 infections. Peripheral neuropathy, typically associated with MMAE, was grade 1-2 in all cases and resolved in most patients. Updated results from the randomized arms with a median follow up of 48 months and results of an extension cohort of 106 additional patients that received pola-BR confirmed a significant survival benefit; no new safety signals were identified (51).
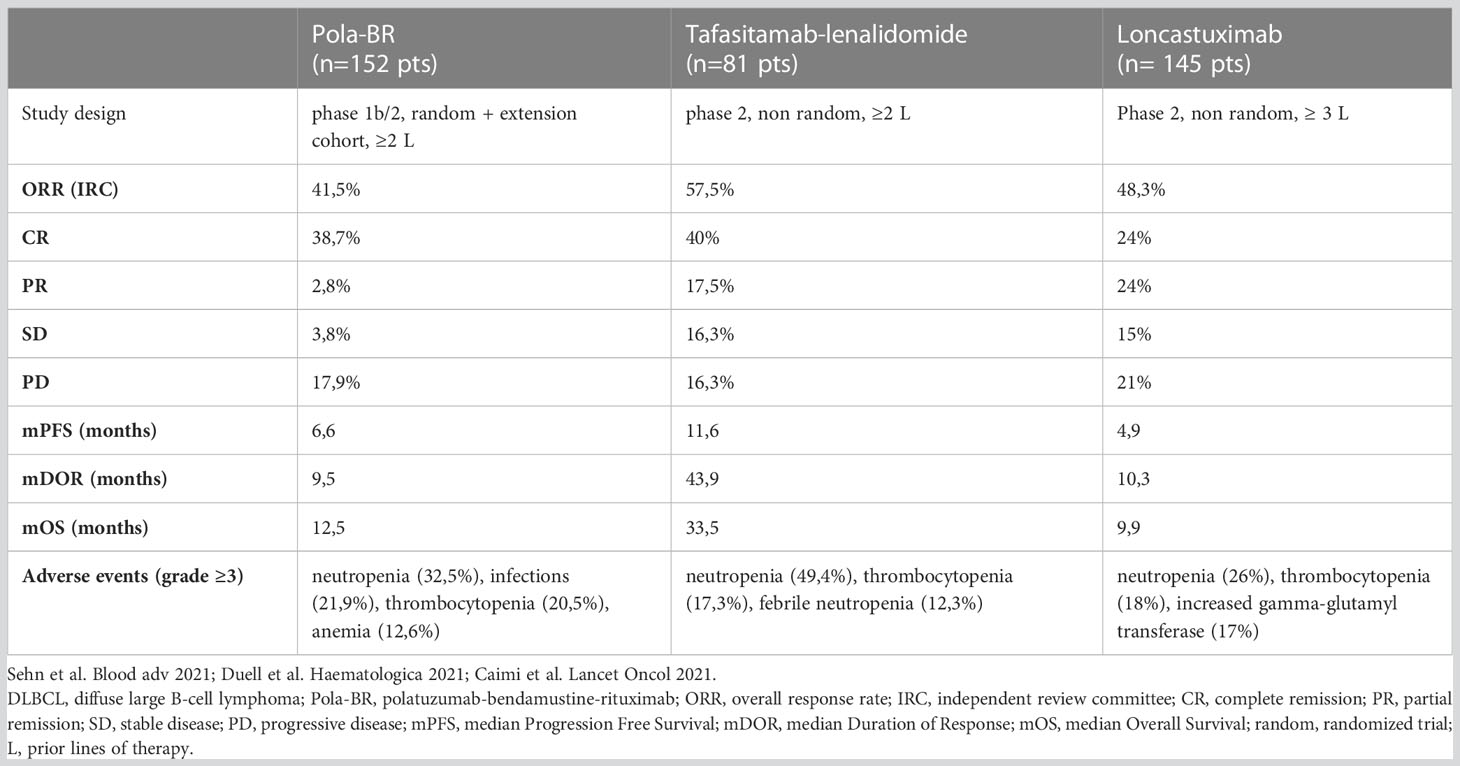
Table 1 Clinical trials in relapsed/refractory DLBCL patients not eligible to transplant.
A second possible salvage option for DLBCL patients not eligible to transplant or CAR-T cells is the combination tafasitamab-lenalidomide. Tafasitamab is a new anti-CD19 antibody with an enhanced Fc-portion. Although tafasitamab and lenalidomide have a limited single-agent activity, in vitro and in vivo studies showed a synergistic effect with limited toxicity (52). The phase II, single-arm, L-MIND study enrolled 81 patients with DLBCL relapsed after 1-3 prior systemic regimens; primary refractory cases were only a minority of the cohort (53). Tafasitamab was administered in combination with lenalidomide for 12 cycles, followed by tafasitamab monotherapy until progression or toxicity. An updated analysis with ≥35 months of follow up showed an ORR of 57.5%, including CR in 40% of cases; the median OS was 33.5 months and the median PFS was 11.6 months. Therefore, tafasitamab-lenalidomide seems to permit a long duration of response with a well-tolerated immuno-modulatory combination (54).
The CD-19 antigen is also the target of loncastuximab tesirine, a new antibody-drug conjugated that delivers pyrrolobenzodiazepine (PBD) dimers after binding to B-cell surface and entering the cell (55). The phase II LOTIS-2 study enrolled 145 DLBCL patients relapsed or refractory after at least 2 prior lines of treatment; 20% of patients were primary refractory, 20% had transformed lymphoma and 10% double/triple hit lymphoma. The ORR in this heavily pre-treated and high-risk cohort was 48.3%, with CR in 24.1% of cases and a median duration of response of 10.3 months. The safety profile was acceptable with neutropenia, thrombocytopenia, increased gamma-glutamyl transferase and pleural effusions as most relevant adverse events (56).
The choice between these different options could be quite difficult in clinical practice. Real-world data described outcomes not as good as that seen in clinical trials, probably due to less selected patients (57, 58). In the absence of randomized trials, a comparison between agents only derives from retrospective, matched cohorts and results should be interpreted with caution. Main factors to be considered for treatment decision are: the aim of therapy (complete remission, duration of response, quality of life), patients’ characteristics (age, fitness, comorbidities), logistic and social aspects (presence of caregiver, distance from the hospital), disease characteristics (prior lines of treatment, refractoriness).
The B-cell lymphoma treatment landscape has recently been broadened by bispecific anti CD20xCD3 antibodies that can engage and redirect patients’ T-cells to eliminate malignant B-cells (59–62; Table 2). The main advantage is an off-the-shelf rapid availability and a toxicity similar but generally inferior to CAR T-cells. Glofitamab, a bispecific antibody characterized by a novel 2:1 CD20-CD3 binding configuration, has shown a high response rate (ORR 52%, CRR 39%) in 154 DLBCL patients (median age 66 years) relapsed or refractory after at least two prior lines of treatment, of which 52 had already received CAR T-cells therapy; complete remissions were ongoing at 12 months in 78% of cases. The most frequent adverse event, common to this class of agents, was CRS (all grades 63% of patients, grade ≥3 4%) (59). Epcoritamab is of particular interest in elderly patients, thanks to its subcutaneous administration. In the dose-expansion cohort of a phase I/II study, 157 DLBCL patients (median age 64 years) were treated, showing an ORR of 63%, a CRR of 39%, and a median duration of response of 12 months with continuous therapy. The CRS was frequent, but of grade 1-2 in most cases (97%) (60).
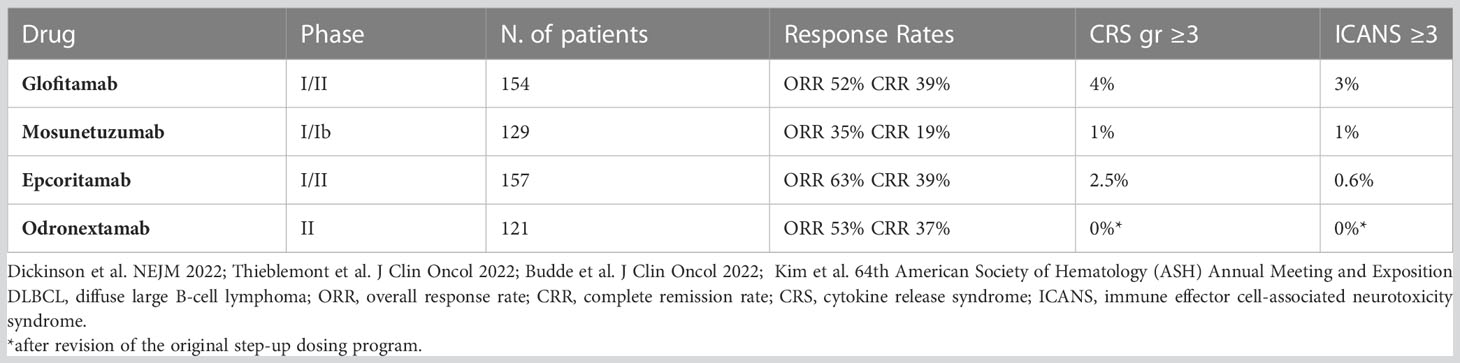
Table 2 Phase I/II trials with bispecific antibodies in relapsed/refractory DLBCL patients.
As mentioned previously, many efforts to improve the standard R-CHOP regimen by adding novel targeted agents (the so-called R-CHOP plus X trials) have failed to demonstrate a better OS. Future trials will attempt to achieve better results combining R-CHOP with novel bruton tyrosin kinase inhibitor characterized by a more favorable profile, such as zanubrutinib (ClinicalTrials.gov Identifier: NCT05189197). The front-MIND phase III trial (ClinicalTrials.gov Identifier: NCT04824092) will compare efficacy and safety of tafasitamab-lenalidomide plus R-CHOP versus R-CHOP alone in newly diagnosed DLBCL patients aged 18-80 years, with high-intermediate or high-risk disease.
A different strategy, proposed by investigators from the MD Anderson Cancer Center, is based on an initial phase with biological agents alone (RLI: rituximab, lenalidomide, and ibrutinib) administered for two cycles to patients with non-GCB DLBCL, followed by the addition of conventional chemotherapy (either R-CHOP or R-EPOCH). With the limits of a small number of patients (60 in total, of which 28% ≥70 years), this “Smart Start study” paths the way for a targeted therapy before chemotherapy, showing an impressive response rate after RLI alone (ORR 86%, CRR 36%). The entire program resulted in an ORR of 100% and a 2-year PFS of 91% (63).
For unfit/frail elderly patients not eligible to standard chemotherapy, an emerging approach is a “chemo-free” treatment, based on new antibodies and small molecules. A phase I/II study explored the use of the bispecific antibody mosunetuzumab as first-line treatment in DLBCL patients >80 years or >60 years but with comorbidities precluding full-dose chemoimmunotherapy. ORR and CRR were 56% and 43%, respectively, in 54 patients with a median age of 83 years; no grade ≥3 CRS and no neurotoxicity were reported (64). An incoming phase II trial will assess epcoritamab alone or in combination with lenalidomide as first-line treatment in elderly DLBCL patients who are considered anthracycline ineligible (ClinicalTrials.gov Identifier: NCT05660967).
The management of elderly patients with aggressive lymphoma continues to be a challenge, but a new era has been opened. Objective parameters that define the fitness status of the patient are fundamental to establish the correct treatment intensity and should be included in future clinical trials. A quality-of-life assessment and patient-reported outcomes should also be considered as crucial end points. New drugs, with immunological mechanisms of action, could help improve the outcome of patients relapsed or refractory after standard chemotherapy or those not eligible to standard chemotherapy because of comorbidities.
AA was responsible for the scientific concept of the review. AA and FC wrote the manuscript. All authors (AA, FC, BP, DV) contributed to the literature review and critical revision of the manuscript, and approved the submitted version.
The authors would like to thank Nadia Miserotti for the English language editing. We are grateful to Angelica Parisotto for the bibliographic research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. National Cancer Institute. Cancer stat facts: NHL-diffuse Large b-cell lymphoma (DLBCL) 2015-2019. Available at: https://seer.cancer.gov/statfacts/html/dlbcl.html (Accessed April 21, 2023).
2. Kanas G, Ge W, Quek RGW, Keeven K, Nersesyan K, Arnason JE. Epidemiology of diffuse large b-cell lymphoma (DLBCL) and follicular lymphoma (FL) in the united states and Western Europe: population-level projections for 2020-2025. Leuk Lymph (2022) 63(1):54–63. doi: 10.1080/10428194.2021.1975188
3. Mareschal S, Lanic H, Ruminy P, Bastard C, Tilly H, Jardin F. The proportion of activated b-cell like subtype among de novo diffuse large b-cell lymphoma increases with age. Haematologica (2011) 96(12):1888–90. doi: 10.3324/haematol.2011.050617
4. Scher KS, Hurria A. Under-representation of older adults in cancer registration trials: known problem, little progress. J Clin Oncol (2012) 30(17):2036–8. doi: 10.1200/JCO.2012.41.6727
5. Buske C, Hutchings M, Ladetto M, Goede V, Mey U, Soubeyran P, et al. ESMO consensus conference on malignant lymphoma: general perspectives and recommendations for the clinical management of the elderly patient with malignant lymphoma. Ann Oncol (2018) 29(3):544–62. doi: 10.1093/annonc/mdx413
6. Merli F, Luminari S, Tucci A, Arcari A, Rigacci L, Hawkes E, et al. Simplified geriatric assessment in older patients with diffuse large b-cell lymphoma: the perspective elderly project of the fondazione italiana linfomi. J Clin Oncol (2021) 39(11):1214–22. doi: 10.1200/JCO.20.02465
7. Coiffier B, Lepage E, Briere R, Herbrecht R, Tilly H, Bouabdallah R, et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-b-cell lymphoma. N Engl J Med (2002) 346(4):235–42. doi: 10.1056/NEJMoa011795
8. Goy A. Succeeding in breaking the r-CHOP ceiling in DLBCL: learning from negative trials. J Clin Oncol (2017) 35(31):3519–22. doi: 10.1200/JCO.2017.74.7360
9. Younes A, Sehn LH, Johnson P, Zinzani PL, Hong X, Zhu J, et al. Randomized phase III trial of ibrutinib and rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone in non-germinal center b-cell diffuse large b-cell lymphoma. J Clin Oncol (2019) 37(15):1285–95. doi: 10.1200/JCO.18.02403
10. Nowakowski GS, Hong F, Scott DW, Macon WR, King RL, Habermann TM, et al. ROBUST: a phase III study of lenalidomide plus r-CHOP versus placebo plus r-CHOP in previously untreated patients with ABC-type diffuse large b-cell lymphoma. J Clin Oncol (2021) 39(12):1317–28. doi: 10.1200/JCO.20.01366
11. Tilly H, Morschhauser F, Sehn LH, Friedberg JW, Trneny M, Sharman JP, et al. Polatuzumab vedotin in previously untreated diffuse large b-cell lymphoma. N Engl J Med (2022) 386(4):351–63. doi: 10.1056/NEJMoa2115304
12. Friedberg JW. How I treat double-hit lymphoma. Blood (2017) 130(5):590–6. doi: 10.1182/blood-2017-04-737320
13. Oki Y, Noorani M, Lin P, Davis RE, Neelapu SS, Ma L, et al. Double hit lymphoma: the MD Anderson cancer center clinical experience. Br J Haematol (2014) 166(6):891–901. doi: 10.1111/bjh.12982
14. Dodero A, Guidetti A, Tucci A, Barretta F, Novo M, Devizzi L, et al. Dose-adjusted EPOCH plus rituximab improves the clinical outcome of young patients affected by double expressor diffuse large b-cell lymphoma. Leukemia (2019) 33(4):1047–51. doi: 10.1038/s41375-018-0320-9
15. Peyrade F, Jardin F, Thieblemont C, Thyss A, Emile J-F, Castaigne S, et al. Attenuated immunochemotherapy regimen (R-miniCHOP) in elderly patients older than 80 years with diffuse large b-cell lymphoma: a multicentre, single-arm, phase 2 trial. Lancet Oncol (2011) 12(5):460–8. doi: 10.1016/S1470-2045(11)70069-9
16. Peyrade F, Bologna S, Delwail V, Emile JF, Pascal L, Fermé C, et al. Combination of ofatumumab and reduced-dose CHOP for diffuse large b-cell lymphomas in patients aged 80 years or older: an open-label, multicentre, single-arm, phase 2 trial from the LYSA group. Lancet Haematol (2017) 4(1):e46–55. doi: 10.1016/S2352-3026(16)30171-5
17. Pfreundschuh M, Trumper L, Kloess M, Schmits R, Feller AC, Rudolph C, et al. Two-weekly or 3-weekly CHOP chemotherapy with or without etoposide for the treatment of elderly patients with aggressive lymphomas: results of the NHL-B2 trial of the DSHNHL. Blood (2004) 104(3):626–33. doi: 10.1182/blood-2003-06-2095
18. Hershman DL, McBride R, Eisenberger A, Tsai WY, Grann VR, Jacobson JS. Doxorubicin, cardiac risk factors, and cardiac toxicity in elderly patients with diffuse b-cell non-hodgkin’s lymphoma. J Clin Oncol (2008) 26:3159–65. doi: 10.1200/JCO.2007.14.1242
19. Lyon AR, Dent S, Stanway S, Earl H, Brezden-Masley C, Cohen-Solal A, et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: a position statement and new risk assessment tools from the cardio-oncology study group of the heart failure association of the European society of cardiology in collaboration with the international cardio-oncology society. Eur J Heart Fail (2020) 22(11):1945–60. doi: 10.1002/ejhf.1920
20. Luminari S, Montanini A, Caballero D, Bologna S, Notter M, Dyer MJS, et al. Nonpegylated liposomal doxorubicin (MyocetTM) combination (R-COMP) chemotherapy in elderly patients with diffuse large b-cell lymphoma (DLBCL): results from the phase II EURO18 trial. Ann Oncol (2010) 21(7):1492–9. doi: 10.1093/annonc/mdp544
21. Sancho JM, Fernandez-Alvarez R, Gual-Capllonch F, Gonzalez-Garcia E, Grande C, Gutierrez N, et al. R-COMP versus r-CHOP as first-line therapy for diffuse large b-cell lymphoma in patients ≥ 60 years: results of a randomized phase 2 study from the Spanish GELTAMO group. Cancer Med (2021) 10(4):1314–26. doi: 10.1002/cam4.3730
22. Rigacci L, Annibali O, Kovalchuk S, Bonifacio E, Pregnolato F, Angrilli F, et al. Nonpegylated liposomal doxorubicin combination regimen (R-COMP) for the treatment of lymphoma patients with advanced age or cardiac comorbidity. Hematol Oncol (2020) 38(4):478–86. doi: 10.1002/hon.2764
23. Visco C, Pregnolato F, Ferrarini I, De Marco B, Bonuomo V, Sbisà E, et al. Efficacy of r-COMP in comparison to r-CHOP in patients with DLBCL: a systematic review and single-arm metanalysis. Crit Rev Oncol Hematol (2021) 163:103377. doi: 10.1016/j.critrevonc.2021.103377
24. Tilly H, Gomes da Silva M, Vitolo U, Jack A, Meignan P, Lopez-Guillermo A, et al. Diffuse large b-cell lymphoma (DLBCL): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2015) 26(Suppl 5):v116–25. doi: 10.1093/annonc/mdv304
25. Laribi K, Denizon N, Bolle D, Truong C, Besancon A, Sandrini J, et al. R-CVP regimen is active in frail elderly patients aged 80 or over with diffuse large b cell lymphoma. Ann Hematol (2016) 95(10):1705–14. doi: 10.1007/s00277-016-2768-x
26. Tucci A, Merli F, Fabbri A, Marcheselli L, Pagani C, Puccini B, et al. Diffuse large b-cell lymphoma in octogenarians aged 85 and older can benefit from treatment with curative intent: a report on 129 patients prospectively registered in the elderly project of the fondazione italiana linfomi (FIL). Haematologica (2023) 108(4):1083–91. doi: 10.3324/haematol.2022.281407
27. Storti S, Spina M, Pesce EA, Salvi F, Merli M, Ruffini A, et al. Rituximab plus bendamustine as front-line treatment in frail elderly (>70 years) patients with diffuse large b-cell non-Hodgkin lymphoma: a phase II multicenter study of the fondazione italiana linfomi. Haematologica (2018) 103(8):1345–50. doi: 10.3324/haematol.2017.186569
28. Gini G, Tani M, Bassan R, Tucci A, Ballerini F, Sampaolo M, et al. Lenalidomide and rituximab (ReRi) as front-line chemo-free therapy for elderly frail patients with diffuse large b-cell lymphoma. a phase II study of the fondazione italiana linfomi, in: 63th ASH Annual Meeting and Exposition, Atlanta. Blood (2021) 138(1):305. doi: 10.1182/blood-2021-148380
29. Philip T, Guglielmi C, Hagenbeek A, Somers R, van der Lelie H, Bron D, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-hodgkin’s lymphoma. N Engl J Med (1995) 333(23):1540–5. doi: 10.1056/NEJM199512073332305
30. Gisselbrecht C, Glass B, Mounier N, Gill DS, Linch DC, Treny M, et al. Salvage regimens with autologous transplantation for relapsed large b-cell lymphoma in the rituximab era. J Clin Oncol (2010) 28(27):4184–90. doi: 10.1200/JCO.2010.28.1618
31. Chihara D, Izutsu K, Kondo E, Sakai R, Mizuta S, Yokoyama K, et al. High-dose chemotherapy with autologous stem cell transplantation for elderly patients with relapsed/refractory diffuse large b cell lymphoma: a nationwide retrospective study. Biol Blood Marrow Transplant (2014) 20(5):684–9. doi: 10.1016/j.bbmt.2014.01.025
32. Davison K, Chen BE, Kukreti V, Couban S, Benger A, Berinstein NL, et al. Treatment outcomes for older patients with relapsed/refractory aggressive lymphoma receiving salvage chemotherapy and autologous stem cell transplantation are similar to younger patients: a subgroup analysis from the phase III CCTG LY. 12 trial. Ann Oncol (2017) 28(3):622–7. doi: 10.1093/annonc/mdw653
33. Munshi PN, Chen Y, Ahn KW, Awan FT, Cashen A, Shouse G, et al. Outcomes of autologous hematopoietic cell transplantation in older patients with diffuse large b-cell lymphoma. Transplant Cell Ther (2022) 28(8):487.e1–7. doi: 10.1016/j.jtct.2022.05.029
34. Neelapu SS, Locke FL, Bartlett NL, Lekakis LJ, Miklos DB, Jacobson CA, et al. Axicabtagene ciloleucel CAR-T cell therapy in refractory large b-cell lymphoma. N Engl J Med (2017) 377(26):2531–44. doi: 10.1056/NEJMoa1707447
35. Schuster SJ, Bishop MR, Tam CS, Waller EK, Borchmann P, McGuirk JP, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large b-cell lymphoma. N Engl J Med (2019) 380(1):45–56. doi: 10.1056/NEJMoa1804980
36. Abramson SJ, Palomba ML, Gordon LI, Lunning MA, Wang M, Arnason J, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large b-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet (2020) 396(10254):839–52. doi: 10.1016/S0140-6736(20)31366-0
37. Neelapu SS, Jacobson CA, Oluwole OO, Munoz J, Deol A, Miklos DB, et al. Outcomes of older patients in ZUMA-1, a pivotal study of axicabtagene ciloleucel in refractory large b-cell lymphoma. Blood (2020) 135(23):2106–9. doi: 10.1182/blood.2019004162
38. Nastoupil L, Jain MD, Feng L, Spiegel JY, Ghobadi A, Lin Y, et al. Standard-of-care axicabtagene ciloleucel for relapsed or refractory large b-cell lymphoma: results from the US lymphoma CAR-T consortium. J Clin Oncol (2020) 38(27):3119–28. doi: 10.1200/JCO.19.02104
39. Jacobson CA, Locke FL, Ma L, Asubonteng J, Hu Z-H, Siddiqi T, et al. Real-world evidence of axicabtagene ciloleucel for the treatment of large b cell lymphoma in the united states. Transplant Cell Ther (2022) 28(9):581.e1–8. doi: 10.1016/j.jtct.2022.05.026
40. Ram R, Grisariu S, Shargian-Alon L, Amit O, Bar-On Y, Stepensky P, et al. Toxicity and efficacy of chimeric antigen receptor T-cell therapy in patients with diffuse large b-cell lymphoma above the age of 70 years compared to younger patients – a matched control multicenter cohort study. Haematologica (2022) 107(5):1111–8. doi: 10.3324/haematol.2021.278288
41. Vic S, Lemoine J, Armand P, Lemonnier F, Houot R. Transplant-ineligible but chimeric antigen receptor T-cell eligible: a real and relevant population. Eur J Cancer (2022) 175:246–53. doi: 10.1016/j.ejca.2022.08.019
42. Locke FL, Miklos DB, Jacobson CA, Perales M-A, Kersten M-J, Oluwole OO, et al. Axicabtagene ciloleucel as second-line therapy for large b-cell lymphoma. N Engl J Med (2022) 386(7):640–54. doi: 10.1056/NEJMoa2116133
43. Abramson JS, Solomon SR, Arnason J, Johnston PB, Glass B, Bachanova V, et al. Lisocabtagene maraleucel as second-line therapy for large b-cell lymphoma: primary analysis of phase 3 TRANSFORM study. Blood (2022) 141(14):1675–84. doi: 10.1182/blood.2022018730
44. Bishop MR, Dickinson M, Purtill D, Barba P, Santoro A, Hamad N, et al. Second-line tisagenlecleucel or standard care in aggressive b-cell lymphoma. N Engl J Med (2022) 386(7):629–39. doi: 10.1056/NEJMoa2116596
45. Mounier N, El Gnaoui T, Tilly H, Canioni D, Sebban C, Casasnovas R-O, et al. Rituximab plus gemcitabine and oxaliplatin in patients with refractory/relapsed diffuse large b-cell lymphoma who are not candidates for high-dose therapy. A phase II Lymhoma Study Assoc trial. Haematol (2013) 98(11):1726–31. doi: 10.3324/haematol.2013.090597
46. Arcari A, Chiappella A, Spina M, Zanlari L, Bernuzzi P, Valenti V, et al. Safety and efficacy of rituximab plus bendamustine in relapsed or refractory diffuse large b-cell lymphoma patients: an Italian retrospective multicenter study. Leuk Lymph (2016) 57(8):1823–30. doi: 10.3109/10428194.2015.1106536
47. Pettengel R, Coiffier B, Narayanan G, Hurtado de Mendoza F, Digumarti R, Gomez H, et al. Pixantrone dimaleate versus other chemotherapeutic agents as a single-agent salvage treatment in patients with relapsed or refractory aggressive non-Hodgkin lymphoma: a phase 3, multicentre, open-label, randomised trial. Lancet Oncol (2012) 13(7):696–706. doi: 10.1016/S1470-2045(12)70212-7
48. Wiernik PH, Lossos IS, Tuscano JM, Justice G, Vose JM, Cole CE, et al. Lenalidomide monotherapy in relapsed or refractory aggressive non-hodgkin’s lymphoma. J Clin Oncol (2008) 26(30):4952–7. doi: 10.1200/JCO.2007.15.3429
49. Deeks ED. Polatuzumab vedotin: first global approval. Drugs (2019) 79(13):1467–75. doi: 10.1007/s40265-019-01175-0
50. Sehn L, Herrera AF, Flowers CR, Kamdar MK, McMillan A, Hertzberg M, et al. Polatuzumab vedotin in relapsed or refractory diffuse large b-cell lymphoma. J Clin Oncol (2020) 38(2):155–65. doi: 10.1200/JCO.19.00172
51. Sehn LH, Hertzberg M, Opat S, Herrera AF, Assouline S, Flowers CR, et al. Polatuzumab vedotin plus bendamustine and rituximab in relapsed/refractory DLBCL: survival update and new extension cohort data. Blood Adv (2022) 6(2):533–43. doi: 10.1182/bloodadvances.2021005794
52. Mougiakakos D, Voelkl S, Bach C, Stoll A, Bitterer K, Beier F, et al. Mechanistic characterization of tafasitamab-mediated antibody-dependent cellular phagocytosis alone or in combination with lenalidomide. Blood (2019) 134(1):4064. doi: 10.1182/blood-2019-124886
53. Salles G, Duell J, Gonzalez-Barca E, Tournilhac O, Jurczak W, Liberati AM, et al. Tafasitamab plus lenalidomide in relapsed or refractory diffuse large b-cell lymphoma (L-MIND): a multicentre, prospective, single-arm, phase 2 study. Lancet Oncol (2020) 21(7):978–88. doi: 10.1016/S1470-2045(20)30225-4
54. Duell J, Maddocks KJ, Gonzalez-Barca E, Jurczak W, Liberati AM, de Vos S, et al. Long-term outcomes from the phase II l-MIND study of tafasitamab (MOR208) plus lenalidomide in patients with relapsed or refractory diffuse large b-cell lymphoma. Haematologica (2021) 106(9):2417–26. doi: 10.3324/haematol.2020.275958
55. Zammarchi F, Corbett S, Adams L, Tyrer PC, Kiakos K, Janghra N, et al. ADCT-402, a PBD dimer-containing antibody drug conjugate targeting CD19-expressing malignancies. Blood (2018) 131(10):1094–105. doi: 10.1182/blood-2017-10-813493
56. Caimi P, Ai W, Alderuccio JP, Ardeshna KM, Hamadani M, Hess B, et al. Loncastuximab tesirine in relapsed or refractory diffuse large b-cell lymphoma (LOTIS-2): a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol (2021) 22(6):790–800. doi: 10.1016/S1470-2045(21)00139-X
57. Northend M, Wilson W, Osborne W, Fox CP, Davies AJ, El-Sharkawi D, et al. Results of a united kingdom real-worl study of polatuzumab vedotin, bendamustine, and rituximab for relapsed/refractory DLBCL. Blood Adv (2022) 6(9):2920–6. doi: 10.1182/bloodadvances.2021005953
58. Qualls D, Buege MJ, Dao P, Caimi PF, Rutherford SC, Wehmeyer G, et al. Tafasitamab and lenalidomide in relapsed/refractory large b cell lymphoma (R/R LBCL): real world outcomes in a multicenter retrospective study, in: 64th ASH Annual Meeting and Exposition, New Orleans. Blood (2022) 140(1):787–9. doi: 10.1182/blood-2022-167620
59. Dickinson MJ, Carlo-Stella C, Morschhauser F, Bachy E, Corradini P, Iacoboni G, et al. Glofitamab for relapsed or refractory diffuse large b-cell lymphoma. N Engl J Med (2022) 387(24):2220–31. doi: 10.1056/NEJMoa2206913
60. Thieblemont C, Phillips T, Ghesquieres H, Cheah CY, Roost Clausen M, Cunningham D, et al. Epcoritamab, a novel, subcutaneous CD3xCD20 bispecific T-cell.engaging antibody, in relapsed or refractory large b-cell lymphoma: dose expansion in a phase I/II trial. J Clin Oncol (2023) 41(12):2238–47. doi: 10.1200/JCO.22.01725
61. Budde LE, Assouline S, Sehn LH, Schuster SJ, Yoon S-S, Yoon DH, et al. Single-agent mosunetuzumab shows durable complete responses in patients with relapsed or refractory b-cell lymphomas: phase I dose-escalation study. J Clin Oncol (2022) 40(5):481–91. doi: 10.1200/JCO.21.00931
62. Kim W-S, Kim TM, Cho S-G, Jarque I, Iskierka-Jazdzewska E, Limei Poon M, et al. Odronextamab in patients with relapsed/refractory (r/r) diffuse large b-cell lymphoma (DLBCL): results from a prespecified analysis of the pivotal phase II study ELM-2, in: 64th ASH Annual Meeting and Exposition, New Orleans. Blood (2022) 140(1):1778–80. doi: 10.1182/blood-2022-158406
63. Westin J, Davis RE, Feng L, Hagemeister F, Steiner R, Lee HJ, et al. Smart start: rituximab, lenalidomide, and ibrutinib in patients with newly diagnosed large b-cell lymphoma. J Clin Oncol (2023) 41(4):745–55. doi: 10.1200/JCO.22.00597
64. Olszewski AJ, Avigdor A, Babu S, Levi I, Eradat H, Abadi U, et al. Mosunetuzumab monotherapy continues to demonstrate promising efficacy and durable complete responses in elderly/unfit patients with previously untreated diffuse large b-cell lymphoma, in: 64th ASH Annual Meeting and Exposition, New Orleans. Blood (2022) 140(1):1070–1. doi: 10.1182/blood-2022-157768
Keywords: elderly, lymphoma, geriatric assessment, chemotherapy, antibody
Citation: Arcari A, Cavallo F, Puccini B and Vallisa D (2023) New treatment options in elderly patients with Diffuse Large B-cell Lymphoma. Front. Oncol. 13:1214026. doi: 10.3389/fonc.2023.1214026
Received: 28 April 2023; Accepted: 18 May 2023;
Published: 03 July 2023.
Edited by:
Annalisa Chiappella, National Cancer Institute Foundation (IRCCS), ItalyReviewed by:
Monica Balzarotti, Humanitas Research Hospital, ItalyCopyright © 2023 Arcari, Cavallo, Puccini and Vallisa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Annalisa Arcari, YS5hcmNhcmlAYXVzbC5wYy5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.