
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 16 June 2023
Sec. Hematologic Malignancies
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1187268
This article is part of the Research Topic Childhood Leukemias in Latin America: Epidemiology, Causality, Novel Predictive Profiles and Therapeutic Strategies View all 22 articles
 Moisés M. Gallardo-Pérez1,2
Moisés M. Gallardo-Pérez1,2 Robert Peter Gale3Oscar A. Reyes-Cisneros1,4Daniela Sánchez-Bonilla1,2José A. Fernández-Gutiérrez1,2Wendy Stock5
Robert Peter Gale3Oscar A. Reyes-Cisneros1,4Daniela Sánchez-Bonilla1,2José A. Fernández-Gutiérrez1,2Wendy Stock5 Iván Murrieta-Álvarez1,2
Iván Murrieta-Álvarez1,2 Juan Carlos Olivares-Gazca1,2Guillermo J. Ruiz-Delgado1,2,6Rafael Fonseca7
Juan Carlos Olivares-Gazca1,2Guillermo J. Ruiz-Delgado1,2,6Rafael Fonseca7 Guillermo J. Ruiz-Argüelles1,2,6*
Guillermo J. Ruiz-Argüelles1,2,6*The therapy of children with acute lymphoblastic leukemia (ALL) in limited resource geospaces is challenging and must balance safety, efficacy, availability, and affordability. We modified the control arm of the St. Jude Total XI protocol for outpatient delivery including once-weekly daunorubicin and vincristine in initial therapy, postponing intrathecal chemotherapy until day 22, prophylactic oral antibiotics/antimycotics, use of generic drugs, and no central nervous system (CNS) radiation. Data were interrogated from 104 consecutive children ≤12 years (median, 6 years [interquartile range (IQR), 3, 9 years]. All therapies were given in an outpatient setting in 72 children. Median follow-up is 56 months (IQR 20, 126 months). A total of 88 children achieved a hematological complete remission. Median event-free survival (EFS) is 87 months [95% confidence interval (CI), 39, 60], 7.6 years in low-risk children (3.4, 8 years) whereas 2.5 years (1, 10 years) in high-risk children. The 5-year cumulative incidence of relapse (CIR) is 28% (18, 35%), 26% (14, 37%) in low-risk children and 35% (14, 52%) in high-risk children. Median survival for all subjects is not reached but must exceed 5 years. A total of 36 children relapsed at a median of 12 months (5, 23 months). Outcomes were comparable to those reported in the control arm of the Total Therapy XI study, but inferior to current treatment protocols in high-income countries. The average cost of the first 2 years of therapy was $28,500 USD compared with an average cost of approximately $150,000 USD in the US, an 80% saving. In conclusion, using an outpatient-based modification of the St. Jude Total XI protocol, we obtained good results with relatively few hospitalizations or adverse events and at a substantial saving. This model can be applied in other resource-poor geospaces.
Long-term survival is achieved in more than 90% of children <10 years old with acute lymphoblastic leukemia (ALL) (1). In resource-poor geospaces, the selection of chemotherapy regimens is challenging and must balance safety, efficacy, availability, and affordability. We modified the control arm of the St. Jude Total XI protocol for outpatient delivery (2–7) and reported outcomes in 104 consecutive children with ALL. We compared our results with those obtained in other geospaces and employing other treatment schedules.
All consecutive children 0–12 years with ALL diagnosed and treated in the Centro de Hematología y Medicina Interna (HMI) de Puebla from September 1983 to 2022 and completed therapy were included. A total of 10 subjects were excluded for not completing therapy because they were lost to follow-up. HMI is a private practice center located in Puebla, México, where people pay for treatment out of pocket or are supported by philanthropies.
Blood and bone marrow smears were stained with May–Grümwald–Giemsa and classified according to the FAB classification (1). The immune phenotype and DNA content were analyzed by flow cytometry (8, 9). Cytogenetics were done by conventional techniques. BCR::ABL1 transcripts (after March 1994) and IKAROS mutations (after July 2014) were assessed by multiplex reverse transcribed polymerase chain reaction (RT-PCR) (10–12).
Subjects received a modified control arm of the St. Jude Total XI regimen, which was chosen because it uses inexpensive generic drugs available in México and, with modifications, can be given in an outpatient setting (5–7): Modifications included initial weekly dosing, postponing intrathecal chemotherapy until day 22 to avoid contamination of the cerebrospinal fluid with blast cells from the peripheral blood, prophylactic oral antibiotics/antimycotics, no CNS radiation, and placement of a central IV catheter. Table 1 shows the main characteristics of modified St. Jude TOTAL XI regimen.
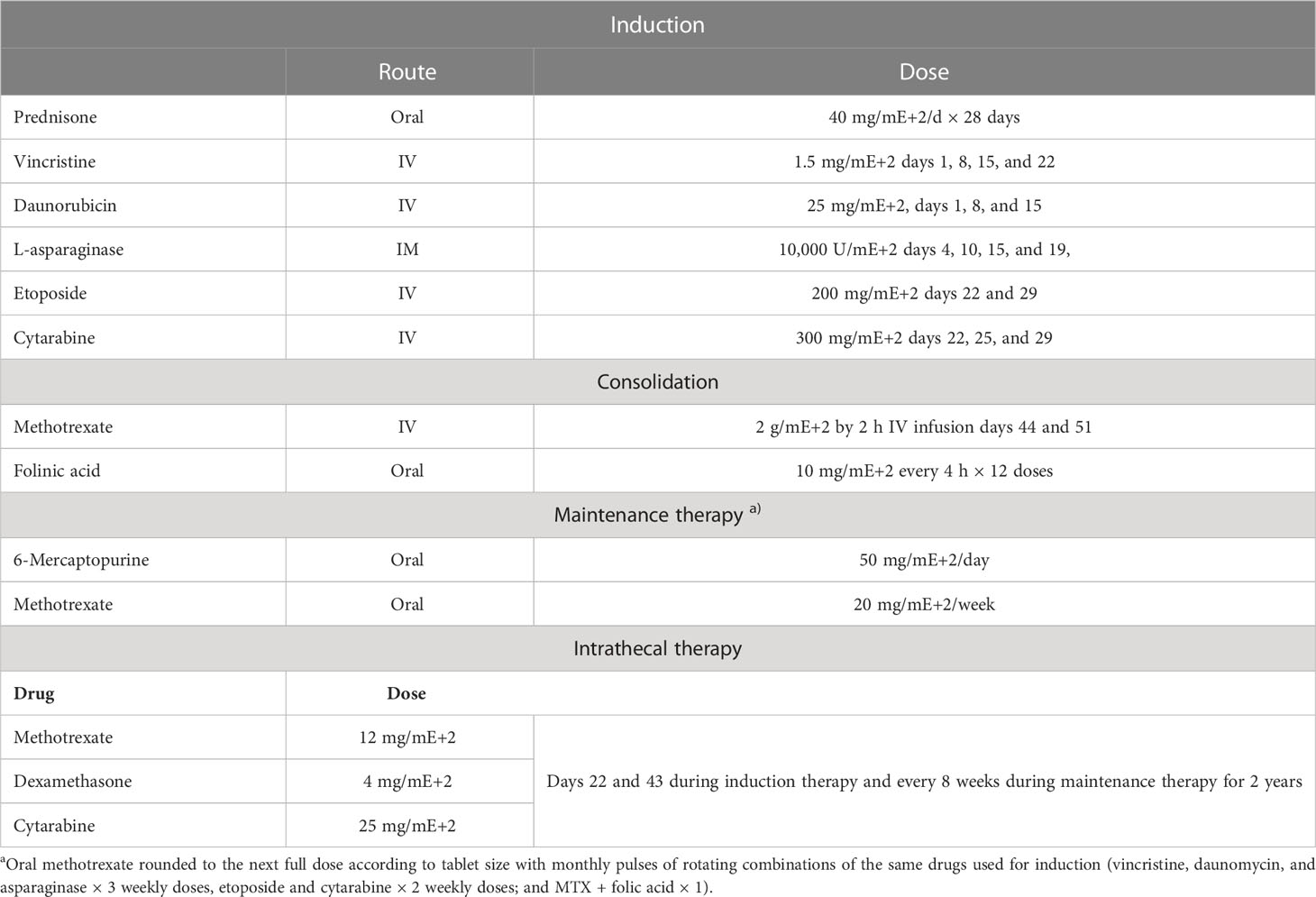
Table 1 Drugs, doses, and schedule used in the modified St. Jude TOTAL XI regimen.
Therapy was given in an outpatient setting. After June 2001, children with BCR::ABL1 received imatinib, 400 mg/day, or dasatinib, 100 mg/day, 7 days after starting therapy and were assessed for hematopoietic cell transplant after achieving a complete remission. The average cost of the first 2 years of therapy was calculated, employing the costs of the drugs and the medical fees for a child with a body surface area of 1 mE+2, treated fully on an outpatient basis. Figure 1 depicts the flow chart of the employed treatment.
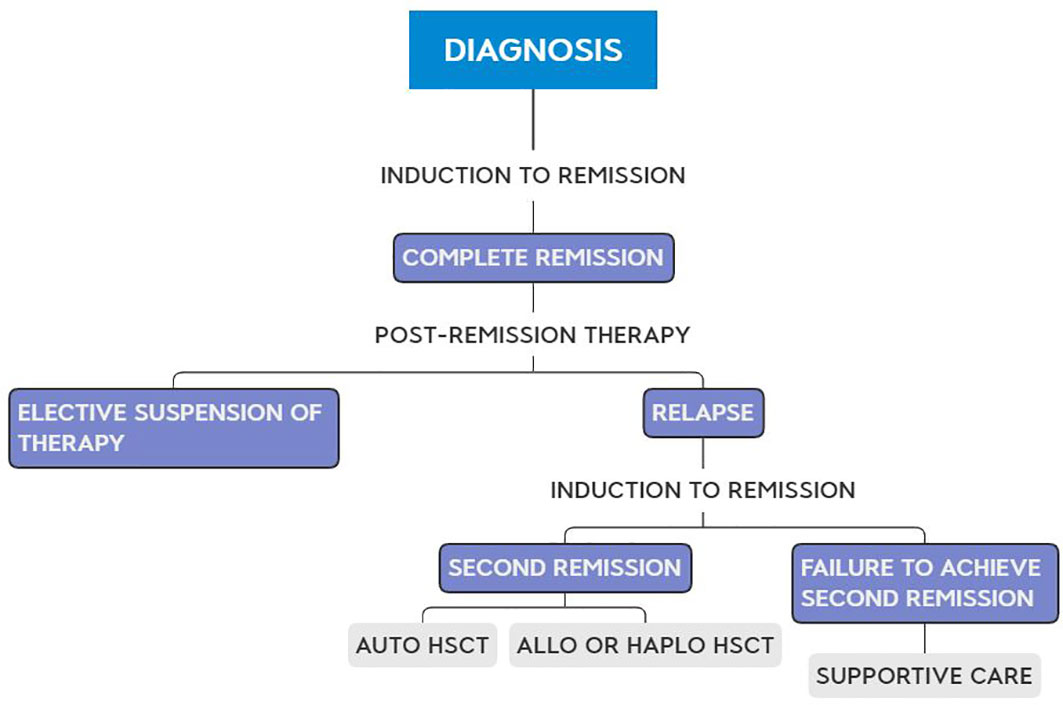
Figure 1 Flow chart of the employed treatment.
Hematological complete remission was defined as no lymphoblasts in blood and cerebrospinal fluid (CSF) and ≤5% in bone marrow for ≥30 days, normal bone marrow histology, no signs or symptoms of leukemia, ECOG performance score of 0–1, and ≥0.5 × 10E+9/L granulocytes and ≥50 × 10E+9/L platelets. Low risk was defined as all of the following: age 1–10 years, white blood cells (WBCs) at diagnosis <50,000 and B phenotype. High risk was defined as one or more of the following: 1) age < 1 or > 10 years; 2) WBC > 50 × 10E+9/L; 3) non-B-cell phenotype; 4) Ph1-chromosome- or BCR::ABL1-positive; 5) IKAROS mutation; and/or 6) t (4, 11). CNS leukemia was diagnosed based on cranial nerve palsies with or without leukemia blasts in the CSF or when mononuclear cells were ≥ 5 × 10E+6/L with leukemia blasts seen on cyto-centrifuged slides. The diagnosis of testes leukemia required biopsy. After 1998, measurable residual disease (MRD) was assayed at the end of induction and consolidation therapies by multi-parameter flow cytometry (MPFC) (12) or PCR (9) and repeated every 3 months whilst receiving therapy. Induction therapy was restarted when the MRD test became positive (>1 × 10E−5 nucleated cells) and a transplant planned after achieving a second complete remission.
The primary endpoint of the analysis was event-free survival (EFS) defined as the interval from starting therapy to relapse or death from any cause. Cumulative incidence of relapse (CIR) was defined as the probability of relapse in children achieving a hematological complete remission. Continuous complete remission (CCR) was defined as the interval from complete remission to relapse. Survival was defined as the interval from starting therapy to death. Transplant recipients were censored at transplant. EFS, CIR, and survival were estimated by Kaplan–Meier plots. Outcomes in the low- and high-risk cohorts were compared using a two-sided log-rank test. Statistical analysis was performed using R Statistical Software (version 3.6.1; R Foundation for Statistical Computing, Vienna, Austria).
A total of 104 consecutive children were analyzed. Median age is 6 years (3–9 years). Of the children, 100 had B-cell lineage, 3 had T-cell lineage, and 1 had null-ALL. At diagnosis, 82 had a WBC concentration <20 × 10E+9/L, 9 had 20–50 × 10E+9/L, and 13 had >50 × 10E+9/L. The DNA content, analyzed in 38 children, was diploid in 22, hyper-diploid in 14, and hypo-diploid in 2. Five of the 56 children tested were BCR : ABL1 positive, and two of the six were IKAROS mutated.
Median follow-up is 56 months (IQR, 20, 12 months). A total of 88 children achieved a hematological complete remission including 57 in the low- and 31 in the high-risk cohorts (p = 0.001). A total of 36 children subsequently relapsed, 18 in the bone marrow only, 13 in the CNS only, 5 in both, and 4 with a synchronous testes relapse. 74 children received chemotherapy only, and 30 children received an autologous (N = 5), allogeneic (N = 23), or auto-allo (N = 2) transplant. Autologous transplants were done in children lacking an HLA-identical sibling. There were 36 children in the low- and 68 in the high-risk cohort. Median time to relapse was 17 months (95% CI, 5, 33 months). Median EFS is 87 months (39, 60 months). Median EFS in the low-risk cohort is 92 versus 35 months (13, 129 months) in the high-risk cohort (p = 0.55; Figure 2). CIR at 5 years is 28% (18, 35%), 26% (14, 37%) in the low- and 35% (14, 52%) in the high-risk cohorts (p = 0.74). Median survival has not been achieved, being >5 years (Figure 3). In the low-risk cohort, 20-year survival probability is 66% (55, 80%) versus 61% (45, 86%; p = 0.64) in the high-risk cohort (Figure 4).
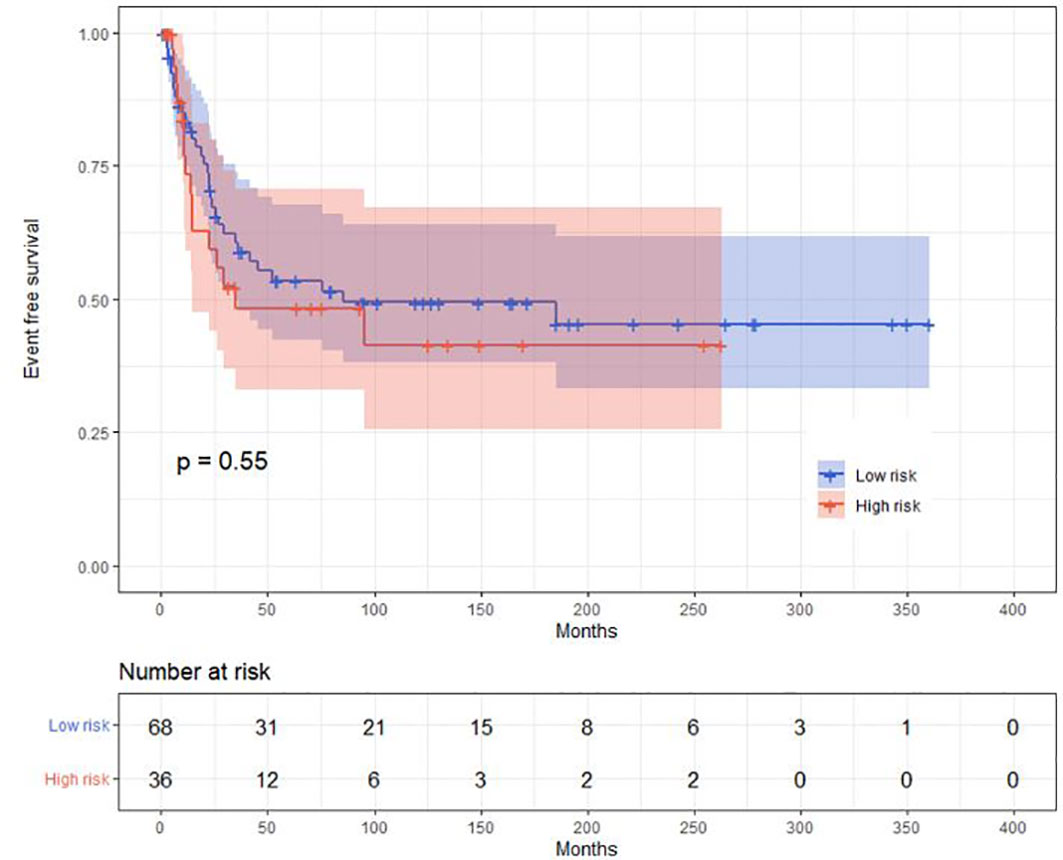
Figure 2 Event-free survival curve in the low- and high-risk cohorts.
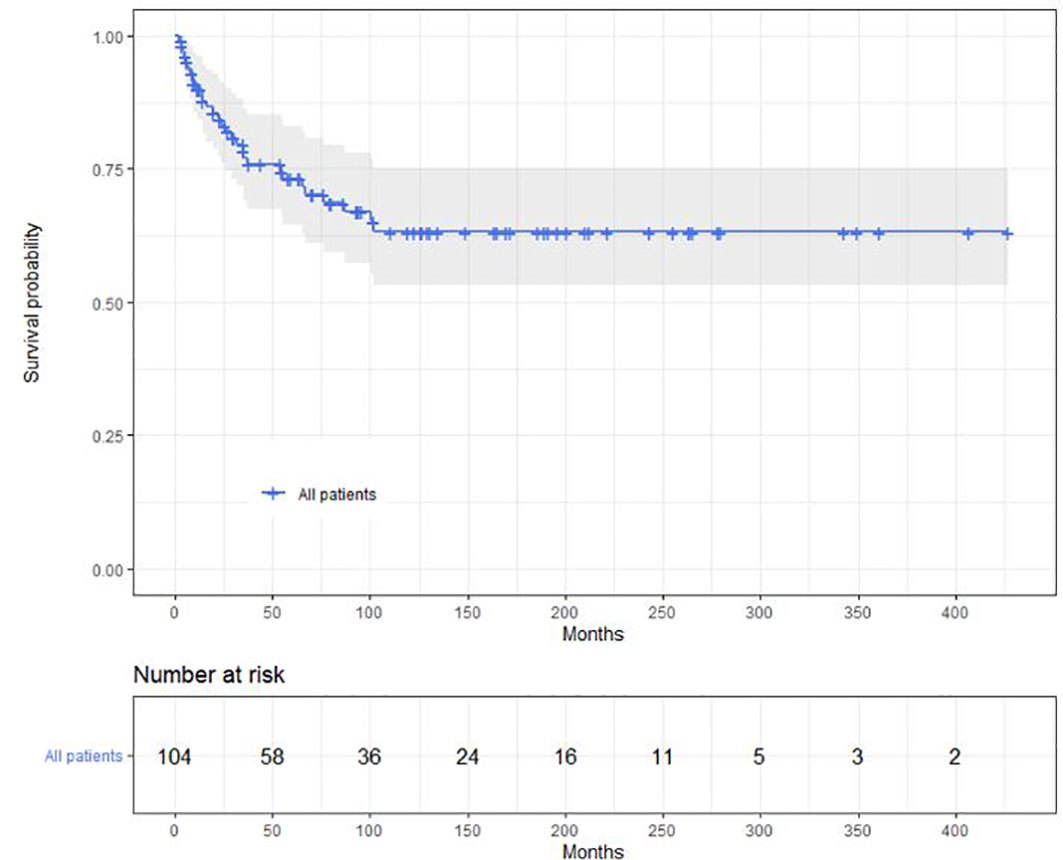
Figure 3 Overall survival of the 104 children.
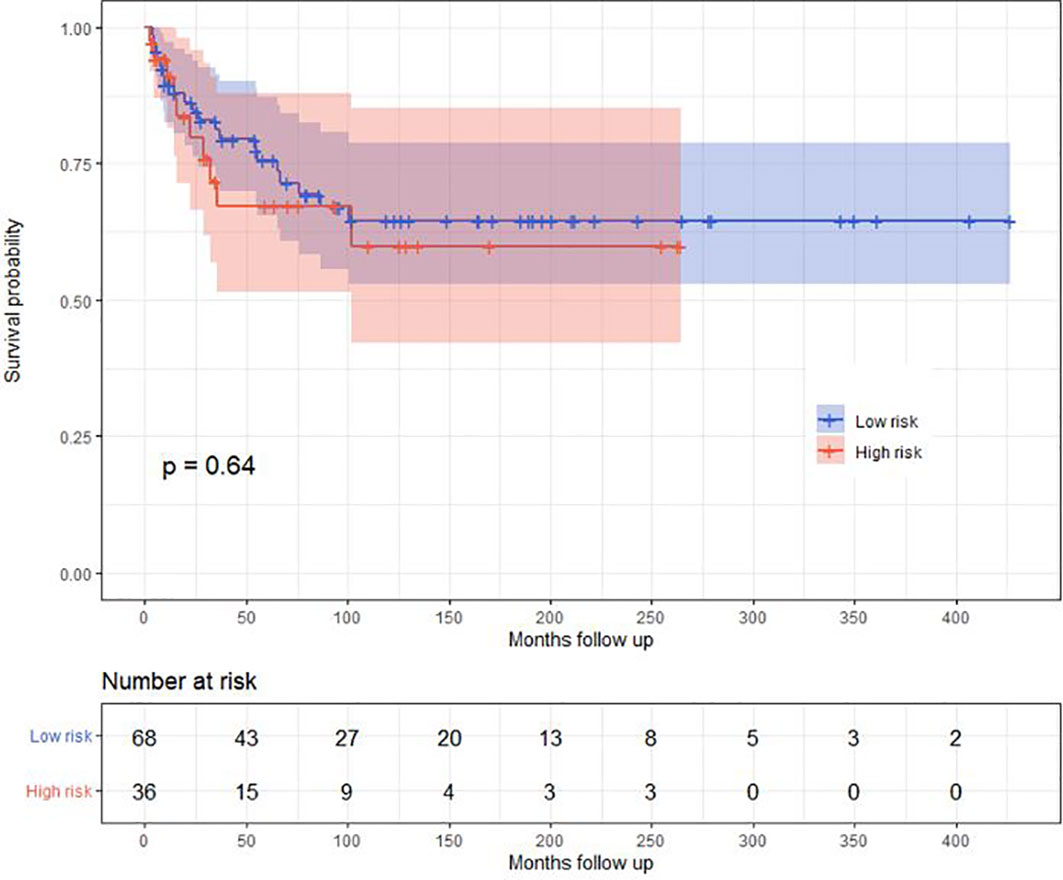
Figure 4 Overall survival of the low- and high-risk cohorts.
Chemotherapy was started in an outpatient setting in all subjects. Four were hospitalized in the first 7 weeks for mucositis, granulocytopenia, meningitis (two patients), and 27 were hospitalized thereafter at a median of 10 days (8–13) after starting therapy. The leading causes of hospitalization were meningitis, mucositis, and pneumonia. A total of 72 children had all their therapy as outpatients.
Data from our study indicate success in treating children with ALL in a resource-poor geospace by modifying the St. Jude Total Therapy XI study for a predominantly outpatient setting, using inexpensive generic drugs and adjusted doses. Of the children, 70% were never hospitalized. Outcomes were like those reported for the control arm of the Total Therapy XI study (6, 7, 14) but inferior to current treatment protocols in high-income countries. The average cost of the first 2 years of therapy of a child with a body surface area of 1 mE+2 and treated fully as outpatient and without complications was $28,500 USD compared with an average cost of $150,000 USD in the US, an 80% saving (14). This cost does not include non-medical cost not incurred at the clinic, such as transportation and accommodation out of the clinic and tutor or parent time off from employment. It is also important to consider that the cost of the drugs varies and that if the costs were more effectively controlled, more children might receive treatment. The need of data management programs for careful documentation of medical costs should also be considered.
In adolescents and young adults, we have previously shown that our TOTAL-XI-based chemotherapy schedule is more effective and less toxic than the Hyper-CVAD regimen, which is commonly employed in North America and requires inpatient chemotherapy administration (4, 5). The 5-year OS in children with ALL treated in different regions of the world ranges from 8% in Eastern Africa to 83% in North America, Latin America being approximately 50% (14–23) (see Supplementary Table S1). Thus, our results over a 30-year period suggest slightly better outcomes than those previously reported in Latin America studies and similar to those obtained in other middle income countries.
Our study has several limitations. First, it was done over 39 years, over which time technologies such as BCR::ABL1-testing, diagnostics, supportive care, financial conditions, and therapies such as TKIs have evolved. Second, we lacked cytogenetic and mutation analyses for some children. Third, substantial numbers of children were lost to follow-up, a common problem in resource-poor geospaces (17, 18). Fourth, the value of currency has changed in our country during the study.
In conclusion, using an outpatient-based modification of the St. Jude Total XI protocol, we obtained good results with relatively few hospitalizations or adverse events and at a substantial saving. This model can be applied in other resource-poor geospaces, with difficulties to admit patients to the hospital.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human/animal participants were reviewed and approved by Comité de Ética en Investigación del Centro de Hematología y Medicina Interna, Clínica Ruiz. The patients/participants provided their written informed consent to participate in this study.
Conception and design: GR-A and GR-D. Collection and assembly of data: OR-C, DS-B, JF-G, IM-Á, and JO. Data analysis and interpretation: WS, RF, RG, MG-P, and GR-A. Manuscript writings: All authors. The work reported in the paper has been performed by the authors, unless clearly specified in the text. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1187268/full#supplementary-material
ALL, acute lymphoblastic leukemia; CI, confidence interval; CCR, continuous complete remission; CIR, cumulative incidence of relapse; CNS, central nervous system; CSF, cerebrospinal fluid; EFS, event-free survival; IQR, interquartile range; MRD, measurable residual disease.
1. Ruiz-Argüelles GJ, Ruiz-Delgado GJ. Leucemias agudas. In: Ruiz-Argüelles GJ, Ruiz-Delgado GJ, editors. Fundamentos de hematología, 6th edition. México City: Editorial Médica Panamericana (2021). p. 135–48. AMEH.
2. Ruiz-Argüelles GJ. En el tratamiento de leucemia aguda en méxico se obtienen resultados tan buenos como en los países desarrollados; sin embargo. Rev Invest Clin Méx (1990) 42:161–3.
3. Gómez-Almaguer D, Ruiz-Argüelles GJ, Ponce-de-León S. Nutritional status and socioeconomic conditions as prognostic factors in the outcome of therapy in acute lymphoblastic leukemia. Int J Cancer (1998) Suppl 11:52–5. doi: 10.1002/(SICI)1097-0215(1998)78:11+<52::AID-IJC15>3.0.CO;2-3
4. García-Villaseñor E, Cortés JE, Reyes-Cisneros OA, Fernández-Gutiérrez JA, Sánchez-Bonilla D, Bojalil-Álvarez L, et al. Long-term results of the treatment of adolescents and adults with acute lymphoblastic leukemia with a pediatric-inspired regimen delivered on an outpatient basis: a single institution experience. Leuk Res (2022) 121:106935. doi: 10.1016/j.leukres.2022.106935
5. Ruiz-Delgado GJ, Macías-Gallardo J, Lutz-Presno JA, Montes-Montiel M, Ruiz-Argüelles GJ. Outcome of adults with acute lymphoblastic leukemia treated with a pediatric-inspired therapy: a single institution experience. Leuk Lymph (2011) 52:314–6. doi: 10.3109/10428194.2010.529202
6. Rivera GK, Raimondi SC, Hancock ML, Behm FG, Pui CH, Abromovitch M, et al. Improved outcome in acute lymphoblastic leukaemia with reinforced early treatment and rotational combination chemotherapy. Lancet (1991) 337:61–6. doi: 10.1016/0140-6736(91)90733-6
7. Pui CH, Pei D, Sandlund JT, Ribeiro RC, Raimondi SC, Onciu M, et al. Long-term results of St Jude total therapy studies 11, 12, 13A, 13B, and 14 for childhood acute lymphoblastic leukemia. Leukemia (2010) 24:371–82. doi: 10.1038/leu.2009.252
8. Ruiz-Argüelles A. Flow cytometry in the clinical laboratory. principles, applications and problems. Ann Biol Clin (1992) 50:735–43.
9. San-Miguel JF, Duque R. Utilidad del inmunofenotipo en el diagnóstico y clasificación de las leucemias agudas. In: Ruiz-Argüelles GJ, San-Miguel JF, editors. Actualización en leucemias. Mexico City: Editorial Médica Panamericana (1996). p. 25–34.
10. Ruiz-Argüelles GJ, López-Martínez B, Ramírez-Cabrera JM, Reyes-Nuñez V, Rodríguez-Cedeño H, Garcés-Eisele J. Molecular monitoring of the treatment of patients with BCR/ABL (+) chronic myelogenous leukemia. Rev Invest Clín Méx (2001) 53:235–9.
11. Ruiz-Argüelles GJ, Garcés-Eisele J, Reyes-Núñez V, Pérez-Romano B, Ruiz-Argüelles A, Ramírez-Cisneros F, et al. Assessment of residual disease in acute leukemia by means of polymerase chain reaction: a prospective study in a single institution. Rev Invest Clin Méx (2000) 52:118–24.
12. Ruiz-Delgado GJ, Cantero-Fortiz Y, León-Peña AA, León-González M, Nuñez-Cortés AK, Ruiz-Argüelles GJ. IKAROS gene deleted b-cell acute lymphoblastic leukemia in Mexican mestizos: observations in seven patients and a short review of the literature. Rev Invest Clin (2016) 68:210–4.
13. Malczewska M, Kośmider K, Bednarz K, Ostapińska K, Lejman M, Zawitkowska J. Recent advances in treatment options for childhood acute lymphoblastic leukemia. Cancers (Basel) (2022) 16:14. doi: 10.3390/cancers14082021
14. Evans WE, Relling MV, Rodman JH, Crom WR, Boyett JM, Pui CH. Conventional compared with individualized chemotherapy for childhood acute lymphoblastic leukemia. N Engl J Med (1998) 338:499–505. doi: 10.1056/NEJM199802193380803
15. Wang YR, Jin RM, Xu JW, Zhang ZQ. A report about treatment refusal and abandonment in children with acute lymphoblastic leukemia in China, 1997–2007. Leuk Res (2011) 35:1628–31. doi: 10.1016/j.leukres.2011.07.004
16. Atun R, Bhakta N, Denburg A, Frazier AL, Friedrich P, Gupta S, et al. (44 authors).: sustainable care for children with cancer: a lancet oncology commission. Lancet Oncol (2020) 21:e185–224. doi: 10.1016/S1470-2045(20)30022-X
17. Barr RD, Antillon-Klussmann F. Cancer and nutrition among children and adolescents in low- and middle-income countries. Hematology (2022) 27(1):987–93. doi: 10.1080/16078454.2022.2115437
18. Omar AA, Basiouny L, Elnoby AS, Zaki A, Abouzid M. St. Jude total therapy studies from I to XVII for childhood acute lymphoblastic leukemia: a brief review. J Egypt Natl Canc Inst (2022) 34(1):25. doi: 10.1186/s43046-022-00126-3
19. Olbara G, van der Wijk T, Njuguna F, Langat S, Mwangi H, Skiles J, et al. Childhood acute lymphoblastic leukemia treatment in an academic hospital in Kenya: treatment outcomes and healthcare providers’ perspectives. Pediatr Blood Cancer (2021) 68:e29366. doi: 10.1002/pbc.29366
20. Oyesakin AB, Nwatah VE, Ukpai NU, David EI, Wakama TT, Oniyangi O. Pattern of childhood acute leukemia presentation at a tertiary hospital in nigeria: a five-year review. Int J Contemp Pediatr (2018) 5:2123–8. doi: 10.18203/2349-3291.ijcp20184202
21. Yang W, Cai J, Shen S, Gao J, Yu J, Hu S, et al. Pulse therapy with vincristine and dexamethasone for childhood acute lymphoblastic leukaemia (CCCG-ALL-2015): an open-label, multicentre, randomised, phase 3, non-inferiority trial. Lancet Oncol (2021) 22(9):1322–32. doi: 10.1016/S1470-2045(21)00328-4
22. Rivera GK, Ribeiro RC. Improving treatment of children with acute lymphoblastic leukemia in developing countries through technology sharing, collaboration and partnerships. Expert Rev Hematol (2014) 7(5):649–57. doi: 10.1586/17474086.2014.949233
Keywords: acute lymphoblastic leukaemia, resource poor countries, Total XI St. Jude protocol, outpatient, children
Citation: Gallardo-Pérez MM, Gale RP, Reyes-Cisneros OA, Sánchez-Bonilla D, Fernández-Gutiérrez JA, Stock W, Murrieta-Álvarez I, Olivares-Gazca JC, Ruiz-Delgado GJ, Fonseca R and Ruiz-Argüelles GJ (2023) Therapy of childhood acute lymphoblastic leukemia in resource-poor geospaces. Front. Oncol. 13:1187268. doi: 10.3389/fonc.2023.1187268
Received: 15 March 2023; Accepted: 05 June 2023;
Published: 16 June 2023.
Edited by:
Juan Carlos Núñez-Enríquez, Instituto Mexicano del Seguro Social, MexicoReviewed by:
Vilma Carolina Bekker Mendez, La Raza National Medical Center, MexicoCopyright © 2023 Gallardo-Pérez, Gale, Reyes-Cisneros, Sánchez-Bonilla, Fernández-Gutiérrez, Stock, Murrieta-Álvarez, Olivares-Gazca, Ruiz-Delgado, Fonseca and Ruiz-Argüelles. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guillermo J. Ruiz-Argüelles, Z3J1aXoxQGNsaW5pY2FydWl6LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.