 Antonin Schmitt
Antonin Schmitt Bernard Royer3
Bernard Royer3 Romain Boidot
Romain Boidot François Ghiringhelli
François Ghiringhelli
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol. , 20 June 2023
Sec. Gastrointestinal Cancers: Gastric and Esophageal Cancers
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1187052
Esophageal cancer is a cancer with poor prognosis and the standard 1st line treatment for metastatic or recurrent EC is systemic chemotherapy with doublet chemotherapy based on platinum and 5-fluorouracil (5-FU). However, 5-FU could be a source of severe treatment-related toxicities due to deficiency of dihydropyrimidine dehydrogenase (DPD). In this case report, a 74-year-old man with metastatic esophageal cancer was found to have partial DPD deficiency based on uracilemia measurements (about 90 ng/mL). Despite this, 5-FU was safely administered thanks to therapeutic drug monitoring (TDM). The case report highlights the importance of TDM in administering 5-FU to patients with partial DPD deficiency, as it allows individualized dosing and prevents severe toxicity.
Esophageal cancer (EC) is the seventh most common cancer, accounting for 3.1% of all cancers, and the sixth leading cause of cancer deaths worldwide, accounting for 5.5% of all cases (1). EC is a cancer with a poor prognosis, detected symptomatically in advance stages. Systemic chemotherapy, a doublet chemotherapy based on platinum and 5-fluorouracil (5-FU), is the standard 1st line treatment for patients with metastatic or recurrent EC who have no curative options, despite limited efficacy (2). Moreover, 5-FU could be the source of severe treatment-related toxicities requiring hospitalization and leading to death in 0.5% to 2% of cases (3–5).
The most well-known biochemical cause of intolerance to fluoropyrimidines is deficiency of dihydropyrimidine dehydrogenase (DPD) (6, 7). DPD is defined as the first and rate-limiting enzyme in the catabolic pathway of 5-FU, responsible for more than 80% of 5-FU elimination (8, 9). Partial or complete deficiency in the DPD enzyme has been observed in 3-5% and 0.1% of the general population, respectively (10–12). DPD-deficient patients experience excessive and severe toxicity in the form of neutropenia, diarrhea, mucositis and hand and foot syndrome. DPD deficiency may be investigated by genotyping DPYD gene or by phenotyping by means of uracilemia (U) or dihydrouracilemia/U ratio (UH2/U).
In France, to date, uracilemia is mandatory before prescription of fluoropyrimidine (uracilemia is not yet mandatory in most countries outside European Union) (13). National institute of cancer in France (INCa) propose that if U < 16 ng/mL patient should be considered with functional DPD, if 16 ≤ U < 150 ng/mL a partial deficiency is suspected and in case of U ≥ 150 ng/mL a total deficiency is suspected. The French recommendations propose to decrease the initial 5-FU dose in case of partial deficiency and to contra-indicate it in case of total deficiency. However, no clear information is given on the extent of dose adaptation in the 1st situation. With regards to UH2/U ratio, no consensus exists with regards to the cut-off value for which a patient would be characterized as deficient because of an important heterogeneity in ratio measurements and a poor prognostic value (14–16).
In our center, we routinely monitor 5-FU concentration to adapt doses based on clinical evidence, but also on individual exposure. Recent French recommendations state that exposure after 5-FU infusion of 46h, by mean of Area Under the Curve of the concentrations time course of 5-FU (AUC), should be within 20-30 mg.h/L (17). We report here a case of a metastatic esophageal cancer patient with a partial DPD deficiency (U ≈ 90 ng/mL) for which 5-FU could be administered thanks to Therapeutic Drug Monitoring (TDM).
A 74-year-old man was diagnosed in April 2022 with an esophageal adenocarcinoma with bone, liver, lung, and lymph node metastases. As 5-FU is the chemotherapy’s backbone of esophageal cancer, DPD activity had to be tested in this patient. A first uracilemia measurement return a value of 85.3 ng/mL, leading to a partial DPD deficiency. UH2/U ratio was equal to 3.9 (UH2 being equal to 332.7). Glomerular filtration rate according to CDK-EPI was 91.5 mL/min/1.73m², total bilirubinemia was 6 mg/L, GGT and ASAT 2N, and ALAT were normal. Because there were some doubts about potential pre-analytical issues potentially leading to hyperuracilemia (e.g., centrifugation done too late as compared to recommendations…), one week later, U and UH2 were controlled at, respectively, 82.6 ng/mL and 348 ng/mL (UH2/U = 4.2). Hepatic and renal biological parameters re-evaluated meanwhile were consistent with the previous values. To confirm the previous values, a third test was performed one week later, with U and UH2 equal to, respectively, 99.6 ng/mL and 217.1 ng/mL. The UH2/U ratio was, thus, a little bit lower, at 2.2. All these uracilemias were unusually high, as these values were above the 99 percentiles of the uracilemia and leaded to characterize the patient as partially deficient. Based on genotyping routinely performed in the hospital, there were no mutations known to be associated with DPD deficiency (detection of DPYD*2A, D949V, *6, *13 and HapB3 by allelic discrimination with a QuantStudio® 5 Real-Time PCR system). A complete exome analysis was conducted as described previously and did not reveal any rare mutation on DPYD gene (18).
Because the patient was presenting a disseminated intravascular coagulation (DIC), a chemotherapy had to be rapidly started. Prothrombin time was at 44%, fibrinogen at 1.1 g/L, platelets at 131 000/L, and normal Factor V. Clinically there was spontaneous hematoma, particularly on the posterior surface of the right thigh and on the upper limb. Bleeding in the central venous line was observed. The patient did not present any thrombotic phenomenon. Thus, mid-April 2022, a chemotherapy by docetaxel 50 mg/m² and oxaliplatin 85 mg/m² was initiated.
After the first cycle, the patient’s general condition gradually improved. He started oral feeding (since then, he was fed by nasogastric tube). No recurrence of bleeding, neither diarrhea was evidenced at home. The tolerance of chemotherapy was excellent without adverse events reported by the patient. Thus, 5-FU infusion (without bolus) was initiated at the second cycle at 20% of the recommended dose (i.e., 800 mg over 46h). A blood sample was drawn 13h54 after the beginning of 5-FU to measure the exposure. The AUC was equal to 4 mg.h/L (N: [20-30 mg.h/L]).
5-FU dose was thus increase up to 2500 mg over 46h (Figure 1). In addition to asthenia, the only side effect was grade 1 diarrhea, leading to an interruption in the dose rising. After cycle 5, the patient was then switched to tipiracil/trifluridin, but died one week later due to intracerebral hemorrhage, independent of his pathology.
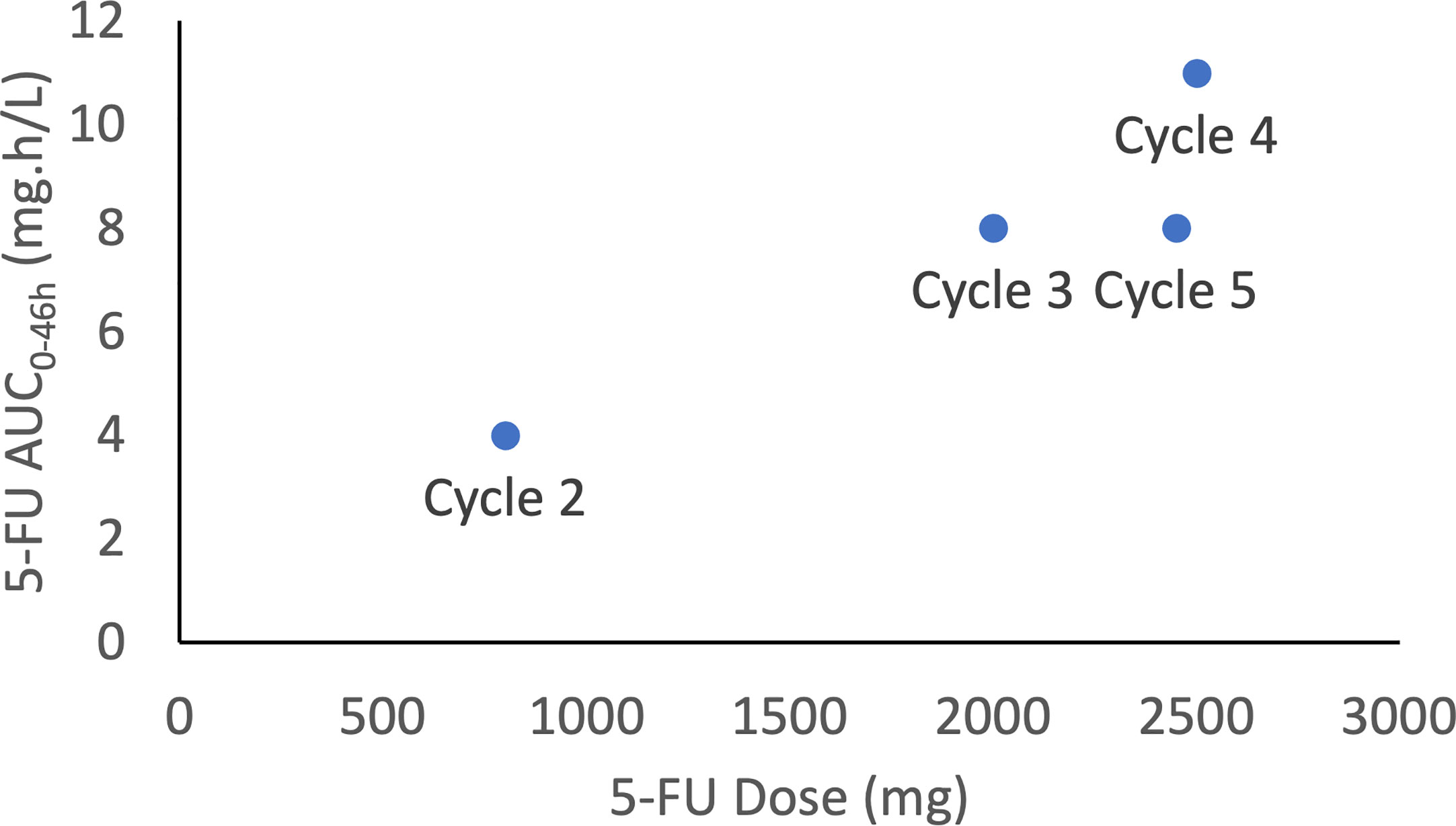
Figure 1 5-FU exposure (AUC0-46h) vs. 5-FU dose for the 4 cycles where 5-FU was dosed.
Thus, in this specific situation, without Therapeutic Drug Monitoring (TDM), our patient would never have received 5-FU because of the risk of over-exposure linked to its DPD deficiency.
To the best of our knowledge, this is the first case report where 5-FU is safely dosed in a patient with a known relatively important partial deficiency.
Our first problematic was to ensure that this deficiency was a real one. Indeed, recent papers have shown that uracilemia may be artificially increased due to non-controlled pre-analytical conditions, renal or hepatic impairment (19–22). However, no prior organ dysfunction was evidenced in our patient. Moreover, despite doubts on the pre-analytical handling of the 1st uracilemia measurement, the two other samples were closely monitored and confirmed the deficiency. Thus, even in the absence of any mutation on DPYD gene (by RT-PCR and exome analyses), the DPD deficiency harbored by the patient was a real deficiency.
The second problematic was then to evaluate the dose of 5-FU that could be given. None of the key recommendations on DPD deficiency handling suggest a refined 5-FU dosing strategy based solely on uracilemia values. Additionally, Dolat et al. has shown the absence of correlation between uracilemia and 5-FU clearance for uracilemia up to 30 ng/mL (23). However, in the French guidelines, TDM is proposed as an option to dose-adapt 5-FU in case of deficiency (13). As 5-FU TDM is routinely conducted in our institution, and because of the need to quickly start an effective chemotherapy in our patient, we have decided to start with a very low dose of 5-FU, estimate the exposure by TDM approach and increase doses accordingly. This strategy allowed to increase doses up to 50% of the nominal dose, with only limited toxicity. Unfortunately, at the highest tested dose, the patient remained under-exposed, which could have led to a potential lack of efficacy. This important point highlight one of the limitations of adapting 5-FU dose solely on uracilemia: deficient patients are at high risk of underexposure and the lack of efficacy may be life-threatening.
5-FU TDM should be done during the 1st 5-FU controlled flow infusion (not during bolus and avoid gravity diffusers). The 1st dose must be adapted to DPD phenotype or DPYD genotype. A single 3 mL blood sample collected in heparinized tube, without separator gel, at least 4 h after the start of the perfusion, in the morning between 8 and 10 a.m., is enough. Centrifugation should be done maximally 30 min after sampling, or a stabilizer reagent (gimeracil) must be added to the blood sample just after sampling (maximal delay before centrifugation: 24 h). AUC is calculated by multiplying the 5-FU concentration by the infusion duration and compared to an algorithm (24).
This strategy could, consequently, be adapted to other patients with known DPD deficiency, in particular in case of discrepancy between genotype and phenotype, such as for our patient. As DPD phenotyping might leads to eventual underexposure (25), we think that TDM associated to 5-FU tolerance during previous cycles may help to recover an optimal 5-FU dose. However, 5-FU introduction should be conducted by experts with the support of a multidisciplinary team and only if no therapeutic alternative is available.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
FG participated in the treatment of this case. AS drafted the manuscript. BR and JB participated in measurement of uracilemia and 5-fluorouracil concentrations. RB was responsible of the pharmacogenetic analysis. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Lordick F, Mariette C, Haustermans K, Obermannová R, Arnold D. ESMO guidelines committee. oesophageal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol (2016) 27(suppl 5):v50–7. doi: 10.1093/annonc/mdw329
3. Meulendijks D, Henricks LM, Sonke GS, Deenen MJ, Froehlich TK, Amstutz U, et al. Clinical relevance of DPYD variants c.1679T>G, c.1236G>A/HapB3, and c.1601G>A as predictors of severe fluoropyrimidine-associated toxicity: a systematic review and meta-analysis of individual patient data. Lancet Oncol (2015) 16(16):1639–50. doi: 10.1016/S1470-2045(15)00286-7
4. Meta-Analysis Group In Cancer, Lévy E, Piedbois P, Buyse M, Pignon JP, Rougier P, et al. Toxicity of fluorouracil in patients with advanced colorectal cancer: effect of administration schedule and prognostic factors. J Clin Oncol Off J Am Soc Clin Oncol (1998) 16(11):3537–41. doi: 10.1200/JCO.1998.16.11.3537
5. Tsalic M, Bar-Sela G, Beny A, Visel B, Haim N. Severe toxicity related to the 5-fluorouracil/leucovorin combination (the Mayo clinic regimen): a prospective study in colorectal cancer patients. Am J Clin Oncol (2003) 26(1):103–6. doi: 10.1097/01.COC.0000017526.55135.6D
6. van Kuilenburg ABP. Dihydropyrimidine dehydrogenase and the efficacy and toxicity of 5-fluorouracil. Eur J Cancer (2004) 40(7):939–50. doi: 10.1016/j.ejca.2003.12.004
7. Liu XQ, Zhuang M, Wang Z, Huber RM. Correlation between dihydropyrimidine dehydrogenase and efficacy and toxicity of fluoropyrimidine drugs. Eur Rev Med Pharmacol Sci (2014) 18(18):2772–6.
8. Matsusaka S, Lenz HJ. Pharmacogenomics of fluorouracil-based chemotherapy toxicity. Expert Opin Drug Metab Toxicol (2015) 11(5):811–21. doi: 10.1517/17425255.2015.1027684
9. Amstutz U, Froehlich TK, Largiadèr CR. Dihydropyrimidine dehydrogenase gene as a major predictor of severe 5-fluorouracil toxicity. Pharmacogenomics (2011) 12(9):1321–36. doi: 10.2217/pgs.11.72
10. Boisdron-Celle M, Remaud G, Traore S, Poirier AL, Gamelin L, Morel A, et al. 5-fluorouracil-related severe toxicity: a comparison of different methods for the pretherapeutic detection of dihydropyrimidine dehydrogenase deficiency. Cancer Lett (2007) 249(2):271–82. doi: 10.1016/j.canlet.2006.09.006
11. Bocci G, Barbara C, Vannozzi F, Di Paolo A, Melosi A, Barsanti G, et al. A pharmacokinetic-based test to prevent severe 5-fluorouracil toxicity. Clin Pharmacol Ther (2006) 80(4):384–95. doi: 10.1016/j.clpt.2006.06.007
12. Saif MW, Ezzeldin H, Vance K, Sellers S, Diasio RB. DPYD*2A mutation: the most common mutation associated with DPD deficiency. Cancer Chemother Pharmacol (2007) 60(4):503–7. doi: 10.1007/s00280-006-0392-5
13. Des recommandations pour prévenir certaines toxicités sévères des chimiothérapies par fluoropyrimidines. Paris: Haute Autorité de Santé (2018). Available at: https://www.has-sante.fr/jcms/c_2892234/fr/des-recommandations-pour-prevenir-certaines-toxicites-severes-des-chimiotherapies-par-fluoropyrimidines.
14. Meulendijks D, Henricks LM, Jacobs BAW, Aliev A, Deenen MJ, de Vries N, et al. Pretreatment serum uracil concentration as a predictor of severe and fatal fluoropyrimidine-associated toxicity. Br J Cancer (2017) 116(11):1415–24. doi: 10.1038/bjc.2017.94
15. van Kuilenburg ABP, Meijer J, Tanck MWT, Dobritzsch D, Zoetekouw L, Dekkers LL, et al. Phenotypic and clinical implications of variants in the dihydropyrimidine dehydrogenase gene. Biochim Biophys Acta (2016) 1862(4):754–62. doi: 10.1016/j.bbadis.2016.01.009
16. Sistonen J, Büchel B, Froehlich TK, Kummer D, Fontana S, Joerger M, et al. Predicting 5-fluorouracil toxicity: DPD genotype and 5,6-dihydrouracil: uracil ratio. Pharmacogenomics (2014) 15(13):1653–66. doi: 10.2217/pgs.14.126
17. Lemaitre F, Goirand F, Launay M, Chatelut E, Boyer JC, Evrard A, et al. [5-fluorouracil therapeutic drug monitoring: update and recommendations of the STP-PT group of the SFPT and the GPCO-unicancer]. Bull Cancer (Paris) (2018) 105(9):790–803. doi: 10.1016/j.bulcan.2018.06.008
18. Réda M, Richard C, Bertaut A, Niogret J, Collot T, Fumet JD, et al. Implementation and use of whole exome sequencing for metastatic solid cancer. EBioMedicine (2020) 51:102624. doi: 10.1016/j.ebiom.2019.102624
19. Callon S, Brugel M, Botsen D, Royer B, Slimano F, Feliu C, et al. Renal impairment and abnormal liver function tests in pre-therapeutic phenotype-based DPD deficiency screening using uracilemia: a comprehensive population-based study in 1138 patients. Ther Adv Med Oncol (2023) 15:17588359221148536. doi: 10.1177/17588359221148536
20. Thomas F, Maillard M, Launay M, Tron C, Etienne-Grimaldi MC, Gautier-Veyret E, et al. Artificial increase of uracilemia during fluoropyrimidine treatment can lead to DPD deficiency misinterpretation. Ann Oncol Off J Eur Soc Med Oncol (2021) 32(6):810–1. doi: 10.1016/j.annonc.2021.02.020
21. Thomas F, Launay M, Guitton J, Loriot MA, Boyer JC, Haufroid V, et al. Plasma uracil as a DPD phenotyping test: pre-analytical handling matters! Clin Pharmacol Ther (2023) 113(3):471–2. doi: 10.1002/cpt.2772
22. Maillard M, Launay M, Royer B, Guitton J, Gautier-Veyret E, Broutin S, et al. Quantitative impact of pre-analytical process on plasma uracil when testing for dihydropyrimidine dehydrogenase deficiency. Br J Clin Pharmacol (2022) 89(2):762–72. doi: 10.1111/bcp.15536
23. Dolat M, Macaire P, Goirand F, Vincent J, Hennequin A, Palmier R, et al. Association of 5-FU therapeutic drug monitoring to DPD phenotype assessment may reduce 5-FU under-exposure. Pharm Basel Switz (2020) 13(11):416. doi: 10.3390/ph13110416
24. Goirand F, Lemaitre F, Launay M, Tron C, Chatelut E, Boyer JC, et al. How can we best monitor 5-FU administration to maximize benefit to risk ratio? Expert Opin Drug Metab Toxicol (2018) 14(12):1303–13. doi: 10.1080/17425255.2018.1550484
25. Hodroj K, Barthelemy D, Lega JC, Grenet G, Gagnieu MC, Walter T, et al. Issues and limitations of available biomarkers for fluoropyrimidine-based chemotherapy toxicity, a narrative review of the literature. In: ESMO open. (Elsevier), vol. 6. (2021). Available at: https://www.esmoopen.com/article/S2059-7029(21)00084-3/fulltext.
Keywords: uracilemia, DPD deficiency, 5-Fu (5-Fluorouracil), esophageal cancer, therapeutic drug monitoring
Citation: Schmitt A, Royer B, Boidot R, Berthier J and Ghiringhelli F (2023) Case report: 5-Fluorouracil treatment in patient with an important partial DPD deficiency. Front. Oncol. 13:1187052. doi: 10.3389/fonc.2023.1187052
Received: 15 March 2023; Accepted: 30 May 2023;
Published: 20 June 2023.
Edited by:
Ji-Feng Feng, University of Chinese Academy of Sciences, ChinaCopyright © 2023 Schmitt, Royer, Boidot, Berthier and Ghiringhelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonin Schmitt, YXNjaG1pdHRAY2dmbC5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.