 Esmeralda García-Torralba1,2,3Esther Navarro Manzano2,3
Esmeralda García-Torralba1,2,3Esther Navarro Manzano2,3 Gines Luengo-Gil1,2,3Pilar De la Morena Barrio1,2,3Asunción Chaves Benito4Miguel Pérez-Ramos4Beatriz Álvarez-Abril1,2,3Alejandra Ivars Rubio1,2,3Elisa García-Garre1,2,3
Gines Luengo-Gil1,2,3Pilar De la Morena Barrio1,2,3Asunción Chaves Benito4Miguel Pérez-Ramos4Beatriz Álvarez-Abril1,2,3Alejandra Ivars Rubio1,2,3Elisa García-Garre1,2,3 Francisco Ayala de la Peña1,2,3*†
Francisco Ayala de la Peña1,2,3*† Elena García-Martínez1,2,3,5
Elena García-Martínez1,2,3,5- 1Department of Haematology and Medical Oncology, University Hospital Morales Meseguer, Murcia, Spain
- 2Department of Medicine, Medical School, University of Murcia, Murcia, Spain
- 3Instituto Murciano de Investigación Biosanitaria (IMIB), Murcia, Spain
- 4Department of Pathology, University Hospital Morales Meseguer, Murcia, Spain
- 5Medical School, Catholic University of Murcia, Murcia, Spain
Background: Up to 30% of breast cancer (BC) patients treated with neoadjuvant chemotherapy (NCT) will relapse. Our objective was to analyze the predictive capacity of several markers associated with immune response and cell proliferation combined with clinical parameters.
Methods: This was a single-center, retrospective cohort study of BC patients treated with NCT (2001-2010), in whom pretreatment biomarkers were analyzed: neutrophil-to-lymphocyte ratio (NLR) in peripheral blood, CD3+ tumor-infiltrating lymphocytes (TILs), and gene expression of AURKA, MYBL2 and MKI67 using qRT-PCR.
Results: A total of 121 patients were included. Median followup was 12 years. In a univariate analysis, NLR, TILs, AURKA, and MYBL2 showed prognostic value for overall survival. In multivariate analyses, including hormone receptor, HER2 status, and response to NCT, NLR (HR 1.23, 95% CI 1.01-1.75), TILs (HR 0.84, 95% CI 0.73-0.93), AURKA (HR 1.05, 95% CI 1.00-1.11) and MYBL2 (HR 1.19, 95% CI 1.05-1.35) remained as independent predictor variables.
Conclusion: Consecutive addition of these biomarkers to a regression model progressively increased its discriminatory capacity for survival. Should independent cohort studies validate these findings, management of early BC patients may well be changed.
1 Introduction
Neoadjuvant chemotherapy (NCT) is the first treatment option for locally advanced and inflammatory breast cancer (BC). It is also a standard treatment in HER2-positive (HER2+) and triple-negative (TNBC) early BC (1). NCT increases the rate of conservative surgery, enables treatment response monitoring and the selection of adjuvant treatment according to risk, and provides unique opportunities for developing novel and individualized therapeutic strategies (1, 2).
Risk stratification is critical in BC patients receiving NCT, as residual pathological disease can affect postoperative decision-making (3). Pathological complete response (pCR) has been classically considered a robust predictor of recurrence, disease-free survival (DFS), and overall survival (OS), especially in the context of the most aggressive subtypes, i. e., HER2+BC and TNBC (2, 4, 5). Despite curative intent, up to 30%-40% of these cases, including some who achieved pCR, will relapse in the first 5 years of follow-up (6). It is crucial that we identify other prognostic factors that can help distinguish individuals who will relapse despite having achieved pCR after NCT.
The adaptive and the innate immune response play a pivotal role in tumor immunosurveillance and can limit tumor development and growth, and determine response to new therapeutic approaches, such as immunotherapy. The role of the immune response in BC has not been fully elucidated. Nevertheless, there is growing evidence that the tumor immune microenvironment plays a key role in the response to different cancer treatments and in prognosis (7).
Several immunological parameters are being investigated or developed as intermediate biomarkers of cancer regression, progression, or recurrence. The most extensively studied marker to date is probably tumor lymphocytic infiltration (8). Tumor-infiltrating lymphocytes (TILs) have been proposed as a predictor of response and prognosis in HER2+ BC and TNBC subtypes, but their involvement in luminal BC is less clear (7). The characterization of the immune cell population in BC and its activation status is mandatory to improve prognosis and to predict treatment response (9).
The chronic inflammatory response is also closely linked to the development and prognosis of certain cancers (10). There is mounting evidence that the total leukocyte count and, most notably, the neutrophil-to-lymphocyte ratio (NLR) prior to embarking on anticancer treatment predict an adverse clinical outcome in several solid tumor (11, 12). This marker is particularly interesting since it integrates the subject’s immune response capacity with their inflammatory status, which tends to correlate with tumor progression and poor prognosis (13). In BC patients, an elevated NLR has been implicated in decreased survival, above all in localized stages (14–16).
The expression of proliferation-related genes in BC is linked to more aggressive subtypes (luminal B and non-luminal subtypes) and forms the foundation for the recent inclusion of clinical KI67 determinations as a predictive and prognostic immunohistochemical (IHC) marker (17). Furthermore, proliferation gene expression is key to understanding biological diversity in luminal BC (18). In fact, gene testing to determine the risk of recurrence includes this information (18–20).
The aurora A kinase (AURKA) gene codifies a serine/threonine kinase with a key role in mitosis regulation that works as an oncogene promoting tumorigenesis (21, 22). Several signaling pathways have been related with AURKA, including PI3K-Akt, Wnt, Hippo, p53 and FOXO (21). Additionally, AURKA is a proliferation marker and its overexpression has also been linked to unfavorable prognosis in BC (23, 24). AURKA has been proposed as a possible biomarker and therapeutic target in chemotherapy and hormonotherapy resistance (25–31).
MYBL2 overexpression has been described as a robust marker of replicative instability (RIN) that can occur in multiple tumor and is a driver in progressive disease and treatment resistance (32). In BC patients, a high MYBL2 proto-oncogene level may also be a biomarker of adverse prognosis (33, 34) and could promote tumor invasion by the induction of epithelial–mesenchymal transition (EMT) and modulation of immune microenvironment (35, 36). In vitro studies have demonstrated its role in tamoxifen resistance (37). Interestingly, Guarneri et al. in the ShortHER phase III trial found that HER2-enriched BC tumor with mutated PIK3CA had an upregulated expression of MKI67, MYBL2, ESR1, PDCD1 and other genes, but only MYBL2 and PDCD1 were related with a better DFS (38).
A single perfect biomarker is unlikely to exist. Recent publications suggest that combined biomarker determination can potentially yield more complete and relevant information (39). Importantly, the predictive value of proliferative signatures and immune signatures are apparently independent, at least in TNBC (40). Combining two proliferation markers such as AURKA and MYBL2, with different biological meaning and with diverse impact on therapeutic resistance, might also improve prognostic stratification. Hence, given the need to enhance currently available prognostic systems and to optimize therapeutic strategies, we have analyzed the prognostic contribution of several immune response-related markers, both in the tumor microenvironment and systemically, in combination with tumor proliferation and clinical-pathological features, in BC patients treated with NCT.
2 Materials and methods
2.1 Study cohort and clinical management
A series of patients consecutively diagnosed with stage II or III BC who received NCT in the Hematology and Medical Oncology Department of a single tertiary hospital (University Hospital Morales Meseguer, Murcia, Spain) between July 2001 and October 2010 was retrospectively analyzed. Clinical evaluation at diagnosis was conducted as per clinical practice criteria, including breast MRI and axillary ultrasound in all cases. Pre-NCT lymph node status was determined by ultrasound-guided fine needle aspiration or sentinel node biopsy. Treatment followed local protocols, in accordance with international recommendations applicable at the time of diagnosis (41). NCT included taxanes and anthracyclines, as well as trastuzumab in patients with HER2+ tumor. After surgery, hormone therapy was prescribed to all patients with hormone receptor (HR)-positive tumor and adjuvant trastuzumab in HER2+ tumor. Adjuvant radiotherapy was administered to all patients treated with conservative surgery, and to patients undergoing mastectomy with a high risk of relapse.
Written informed consent was obtained from all patients included in the study. The study was approved by the Clinical Research and Trials Committee of the University Hospital Morales Meseguer (Internal code: EST07/15) and was conducted in accordance with the ethical principles of the Declaration of Helsinki.
2.2 Clinical and laboratory variables and neutrophil-to-lymphocyte ratio estimation
Demographic and clinical-pathological variables and treatment and response data were obtained from participants’ clinical records. Primary outcome variables included DFS, measured from the date of diagnosis to last follow-up or disease relapse, and OS, quantified as the date of diagnosis to the date of last follow-up or demise.
Routine laboratory parameters were collected from laboratory databases, using the closest blood count prior to the date NCT was initiated (maximum time: four weeks). Pretreatment NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count.
2.3 Histopathological evaluation of the tumor
Estrogen receptor (ER) and progesterone receptor (PR) status were assessed by IHC. Cases were considered negative when the percentage of immunoreactive tumor cells was <1%; the remaining cases (≥1% of stained tumor cells) were classified as positive. A validated IHC method (Herceptest, Dako North America, CA, USA) or fluorescent in situ hybridization (FISH) was used to determine HER2 status. Cases were positive if the Herceptest result was 3+ and/or FISH exhibited a HER2/CEP17 ratio ≥ 2; all others were coded as negative. pCR was defined as the absence of invasive carcinoma in the breast and axilla, regardless of the presence of carcinoma in situ (ypT0/Tis ypN0).
2.4 Tumor-infiltrating lymphocyte counts
CD3-positive TILs (TIL-CD3+) were quantified using IHC, as previously reported (9). In brief, after a pathologist (ACB) had selected tumor-predominant areas, a tissue microarray was constructed from 2 mm biopsies prior to initiating NCT treatment. Appropriate controls were included in each array. Sections measuring 4 μm were cut from the tissue microarray, deparaffinized, rehydrated, and processed by standard methods using an automated stainer (Autostainer Link 48, Dako, CA, USA). Secondary antibodies and visualization were performed using standard Dako Envision systems. All slides were simultaneously stained to avoid intersection variability. Positivity for human CD3 was tested using the polyclonal antibody IS503 (Dako, CA, USA).
After two independent observers had verified that staining was correct, each slide was scanned and digitized using an automated scanning system (Leica SCN400F). Digital images of pre-NCT samples were obtained for each tissue core and, after area quantification, adjusted morphometric analysis of the tumor area was performed with ImageJ software (National Institutes of Health, NIH, USA), including both stromal and intratumoral CD3+ cells. The results are expressed as TIL count/mm2.
2.5 RNA purification and tumor gene expression assay
Total RNA from formalin-fixed paraffin-embedded (FFPE) biopsies was extracted using a RNeasy FFPE kit (QIAGEN, MD, USA) following the supplier’s instructions. Total RNA from cells was extracted using RNAzol reagent (MRC Inc, OH, USA) and a Direct-zol RNA MiniPrep kit (ZYMO Research, CA, USA).
mRNA (with preamplification) was retrotranscribed and amplified using TaqMan® Gene Expression Assays (Applied Biosystems, CA, USA) on a LightCycler® 480 real-time PCR (qRT-PCR) system (Roche Diagnostics, Switzerland). Relative expression levels of each gene were calculated and quantified by 2-ΔΔCt using ACTB as the endogenous control.
2.6 Statistical analysis
Descriptive analyses of qualitative variables included proportions. Shapiro-Wilk tests were used to test continuous variables for normality. Continuous variables with normal distribution were presented as means ± standard deviations (SD), whereas non-normally distributed variables were reported as median and interquartile ranges (IQR). Pearson’s χ2 test was used to compare proportions or ordinal variables. Differences in means were studied with the Student’s t-test (parametric) or the Mann-Whitney U test (non-parametric).
Survival analyses of DFS and OS outcome variables were calculated using the Kaplan-Meier method and log-rank tests. The predictive impact of the different clinical, biological, and genomic variables on the outcome variables was ascertained by uni- and multivariate Cox proportional hazards regression analyses. To overcome the possibility of collinearity, variables with strong (|r| ≥ 0.5) or significant (p < 0.05) correlations were excluded. The predictive capacity of the regression models was appraised using the Akaike Information Criterion (AIC) index and Likelihood Ratio Test (LLRT). Biological and genomic variables were analyzed as continuous quantitative variables, although logarithmic or square root transformations of the TILs, AURKA, MYBL2, and MKI67 variables were performed so that the data would comply more closely with the assumptions of the statistical procedures to be applied or to enhance interpretability. Assessment of mean calibration at 10 years was calculated for each model as observed/expected (O/E) survival ratio.
Statistical analyses were performed with STATA v.16 (StataCorp LLC, TX, USA); R version 4.2.3 and RStudio (version 2023.03.0) was also used for model assessment.
3 Results
3.1 Patients
A total of 121 NCT-treated BC patients were analyzed. Patients’ baseline characteristics are shown in Table 1. Median age was 56 years and most tumors were diagnosed at stage IIB or IIIA-C. Infiltrating ductal carcinoma was the most common histological type and more than half of the tumors were poorly differentiated. ICH subtype distribution revealed 63.6% HR+ (13.2% HER2+), 10.7% HER2+/HR- tumors, and 21.5% TNBC.
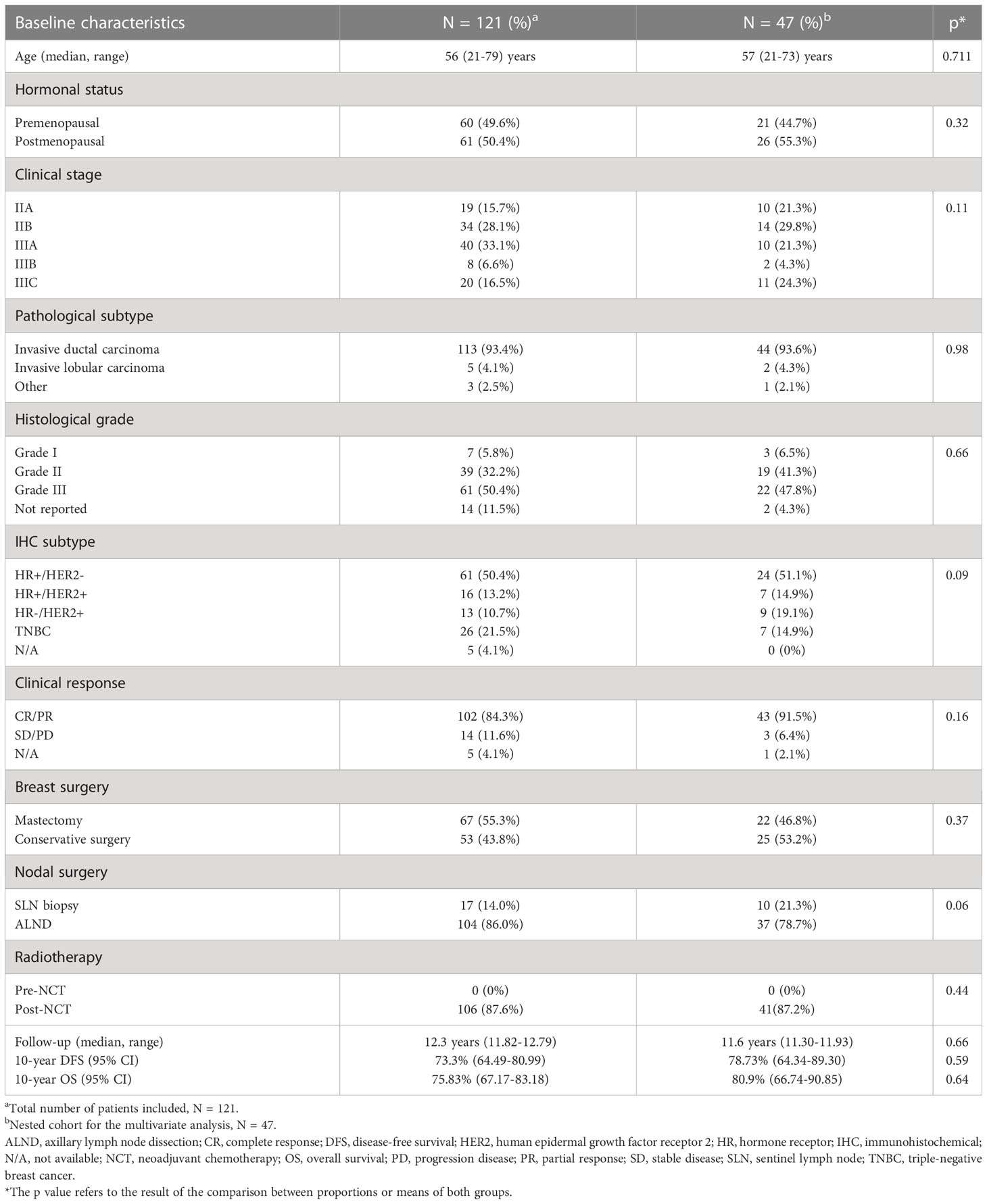
Table 1 Patients’ baseline characteristics.
Neoadjuvant treatment consisted primarily of sequential Adriamycin-cyclophosphamide for four cycles, followed by docetaxel for four cycles (NSABP-B27 scheme, 80.2%). The pCR rate was 17% (primary tumor pCR: 20.7%; axillary pCR: 36.4%). Median follow-up was 12.3 years, the 10-year DFS rate was 73.33%, and 10-year OS was 75.83%.
Of the total 121 participants, the full analysis of clinical variables (HR/HER2 status, response to NCT), immunological variables (NLR, TILs), and genomic markers (AURKA, MYBL2, and MKI67) were available for multivariate analysis in 47 patients (Supplementary Figure 1). Since the clinical and pathological characteristics of both groups were comparable and no statistically significant differences were found, this subgroup was representative of the total sample (Table 1).
3.2 Prognostic significance of clinical, biological, and genomic factors
We evaluated the prognostic significance of the clinical factors and the various biomarkers selected by Cox regression. NLR, TILs, and genomic markers were analyzed as continuous quantitative variables. Correlation analysis demonstrated association between genomic markers MKI67, and MYBL2 (Supplementary Table 1). Notably, there was no correlation between pretreatment NLR and TILs in the pretreatment biopsy (|r|= 0.087, p = 0.503).
In a univariate analysis (Figure 1), pCR (N = 119) was a protective factor for DFS (HR 0.13, 95% CI 0.02-0.94) and OS (HR 0.30, 95% CI 0.07-1.27), albeit falling short of statistical significance. Results were similar for patients with HR+ and HER2+, in terms of DFS (HR 0.91, 95% CI 0.46-1.78 and HR 1.15, 95% CI 0.56-2.38, respectively) and OS (HR 0.97, 95% CI 0.46-2.06 and HR 0.76, 95% CI 0.31-1.85, respectively).
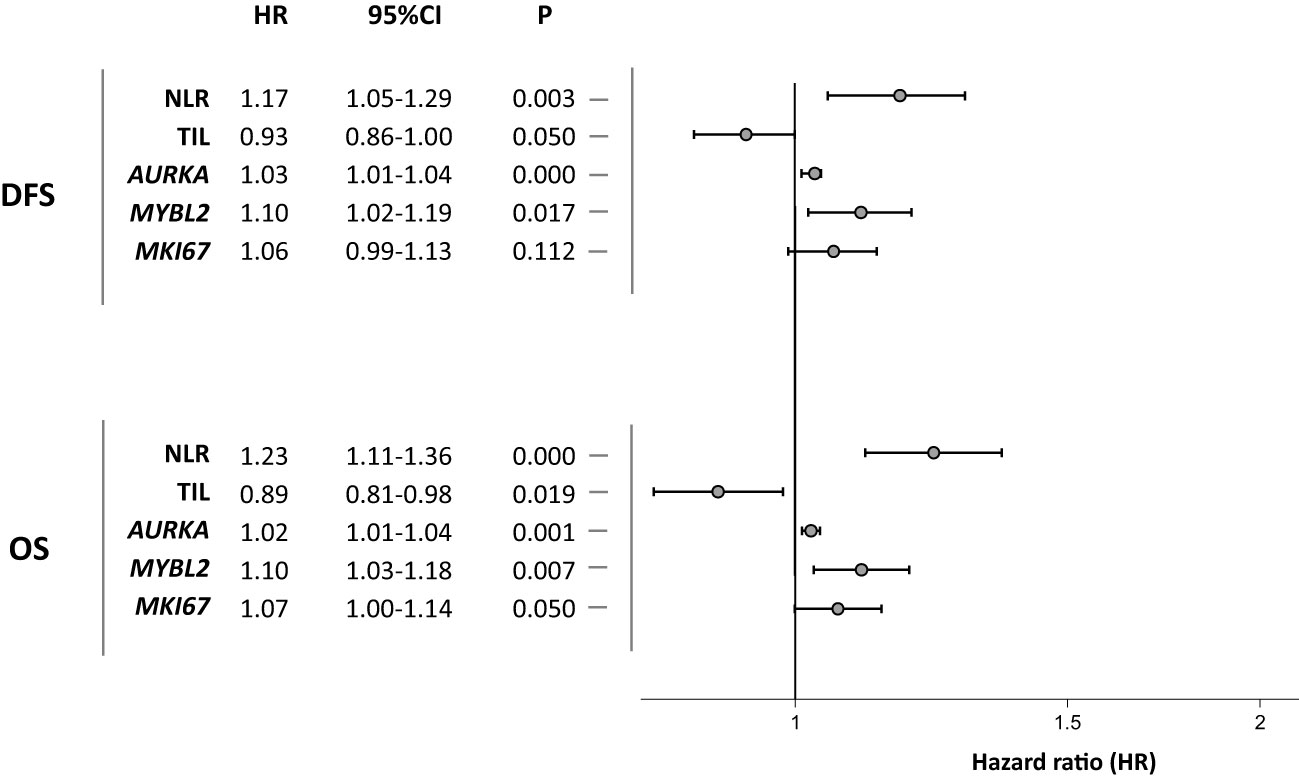
Figure 1 Univariate associations between immune response-related and proliferation markers and disease-free survival and overall survival.
The NLR biomarker in peripheral blood (N = 101) was found to have prognostic implications. Increased NLR was associated with lower DFS (HR 1.17, 95% CI 1.05-1.29) and OS (HR 1.23, 95% CI 1.11-1.36). At the tumor level, the immunological marker TIL (N = 71) exhibited a statistically significant association in the opposite direction from NLR. Patients with higher tumor lymphocytic infiltration had a better prognosis in terms of DFS (HR 0.93, 95% CI 0.86-1.00) and OS (HR 0.89, 95% CI 0.81-0.98).
Genomic markers for tumor proliferation assessed were AURKA, MYBL2, and MKI67. AURKA (N = 79) demonstrated a significant prognostic impact on DFS (HR 1.03, 95% CI 1.01-1.04) and OS (HR 1.02, 95% CI 1.01-1.04). MYBL2 expression (N = 79) also correlated with lower DFS (HR 1.10, 95% CI 1.02-1.19) and OS (HR 1.10, 95% CI 1.03-1.18). The proliferation marker MKI67 (N = 79) only exhibited prognostic significance for OS (HR 1.07, 95% CI 1.00-1.14).
Clinically relevant variables and biomarkers that had previously exhibited prognostic significance were included to generate multivariate Cox models. MKI67, that showed significant correlation with MYBL2, was excluded to prevent collinearity (Supplementary Table 1). Thus, together with HR/HER2 status and response to NCT, the NLR, TILs, and AURKA and MYBL2 expression remained as independent prognostic variables for both DFS and OS (Table 2).
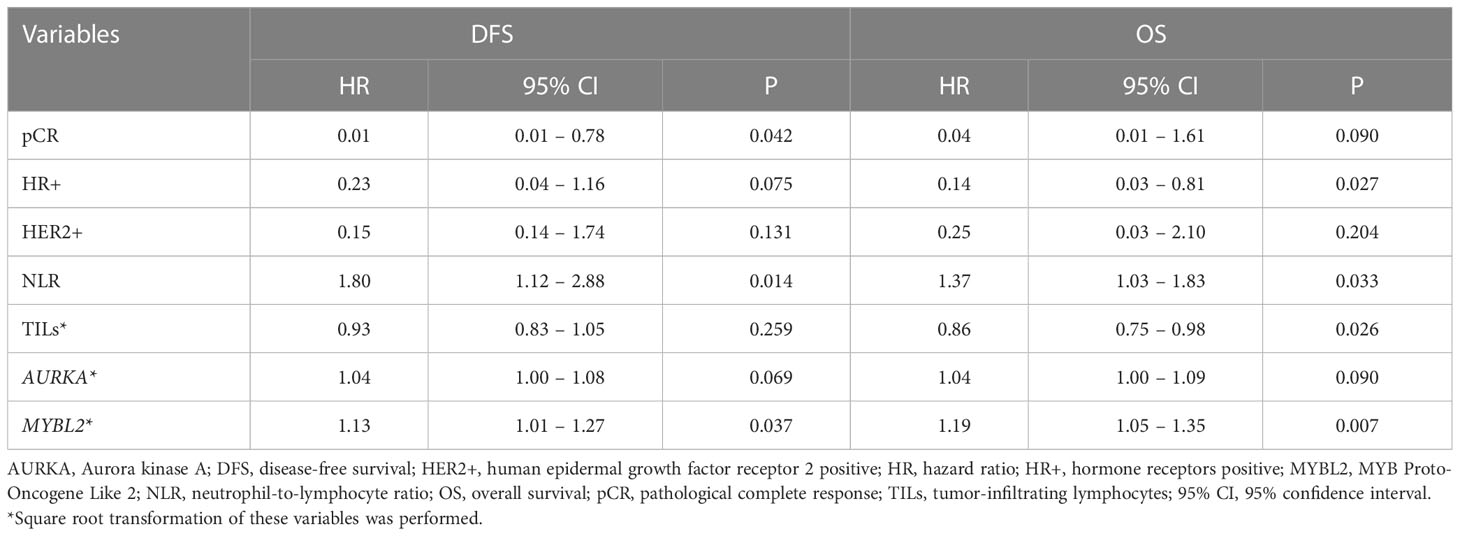
Table 2 Multivariate analysis of immune response-related and proliferation markers for disease- free survival and overall survival.
3.3 Analysis of the prognostic capacity of the different models
We assessed the predictive performance of the biomarkers included in the multivariate Cox proportional hazards models using AIC and LLRT. We consecutively added the immune response biomarkers, NLR and TILs (model 2), and genomic markers, AURKA and MYBL2 (model 3), to HR/HER2 status and NCT response (model 1). For both DFS and OS, we established that the consecutive addition of biomarkers generated a progressive increase in the models’ predictive capacity (Table 3). This was reflected in a gradual decrease in AIC for both DFS (AIC model 3: 64 vs AIC model 1: 79) and OS (AIC model 3: 58 vs AIC model 1: 70), in addition to differences in LLRT for the different models that were statistically significant compared to the isolated clinical parameter (DFS: p < 0.001; OS: p = 0.005). A side-by-side comparison between this combinatorial model versus prediction using individual markers, is provided as Supplementary Table 2. Additionally, the 10 years mean calibration of the OS model also improved with the addition of proliferation and immune markers, while it remained virtually unchanged for the DFS models (Figure 2 and Supplementary Table 3).
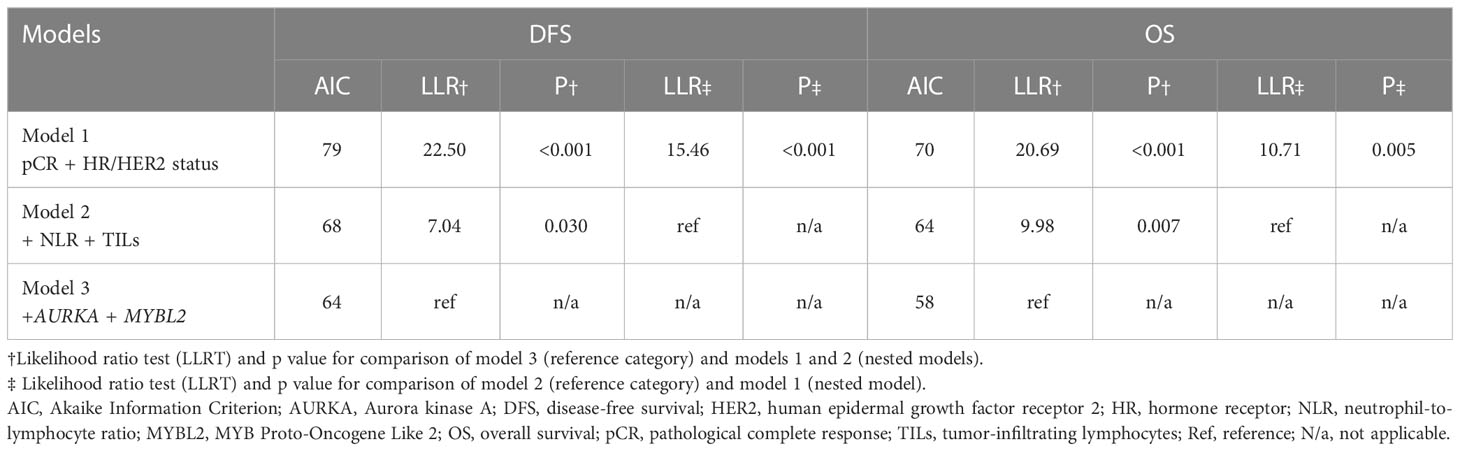
Table 3 Predictive capacity following the consecutive addition of biomarkers to clinical variables.
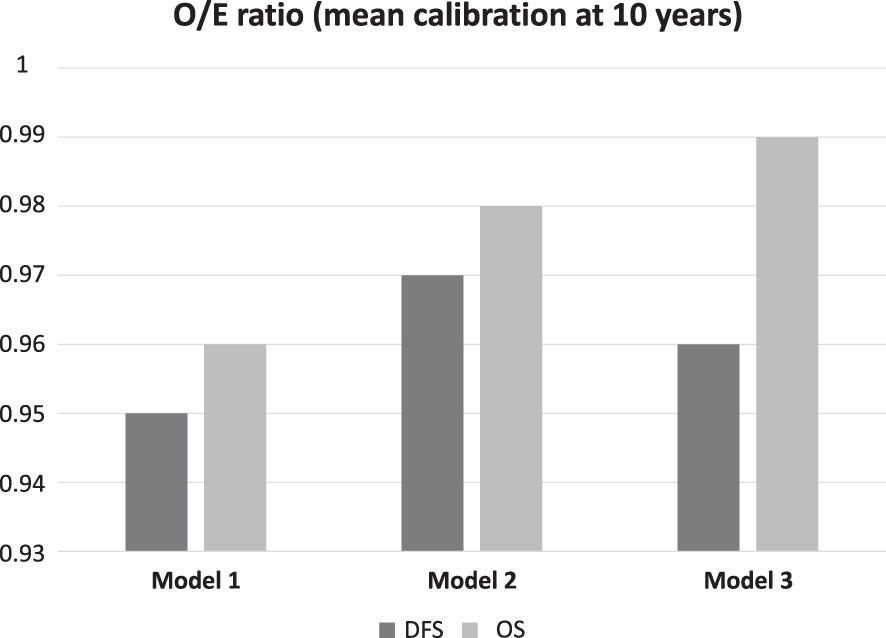
Figure 2 Mean calibration at 10 years. O/E (observed/expected) ratios for each model are shown, both for OS and DFS.
The predictive value added by the biomarkers was also gauged by plotting cohort survival as a function of the predictions obtained with each model. Figure 3 depicts the Kaplan-Meier curves for DFS and OS obtained with the predictions of pCR and model 3 (pCR, HR and HER2 status, NLR, TILs, AURKA, and MYBL2), the latter divided into tertiles. This exploratory analysis showed that the incorporation of the immunological and proliferation parameters with the clinical variable (pCR) in model 3 allowed a better stratification of the risk of events in the cohort analyzed than model 1. In fact, while the log-rank test indicated no statistically significant differences for model 1, such differences were statistically significant for model 3, both for DFS (p = 0.0014) and OS (p = 0.0054).
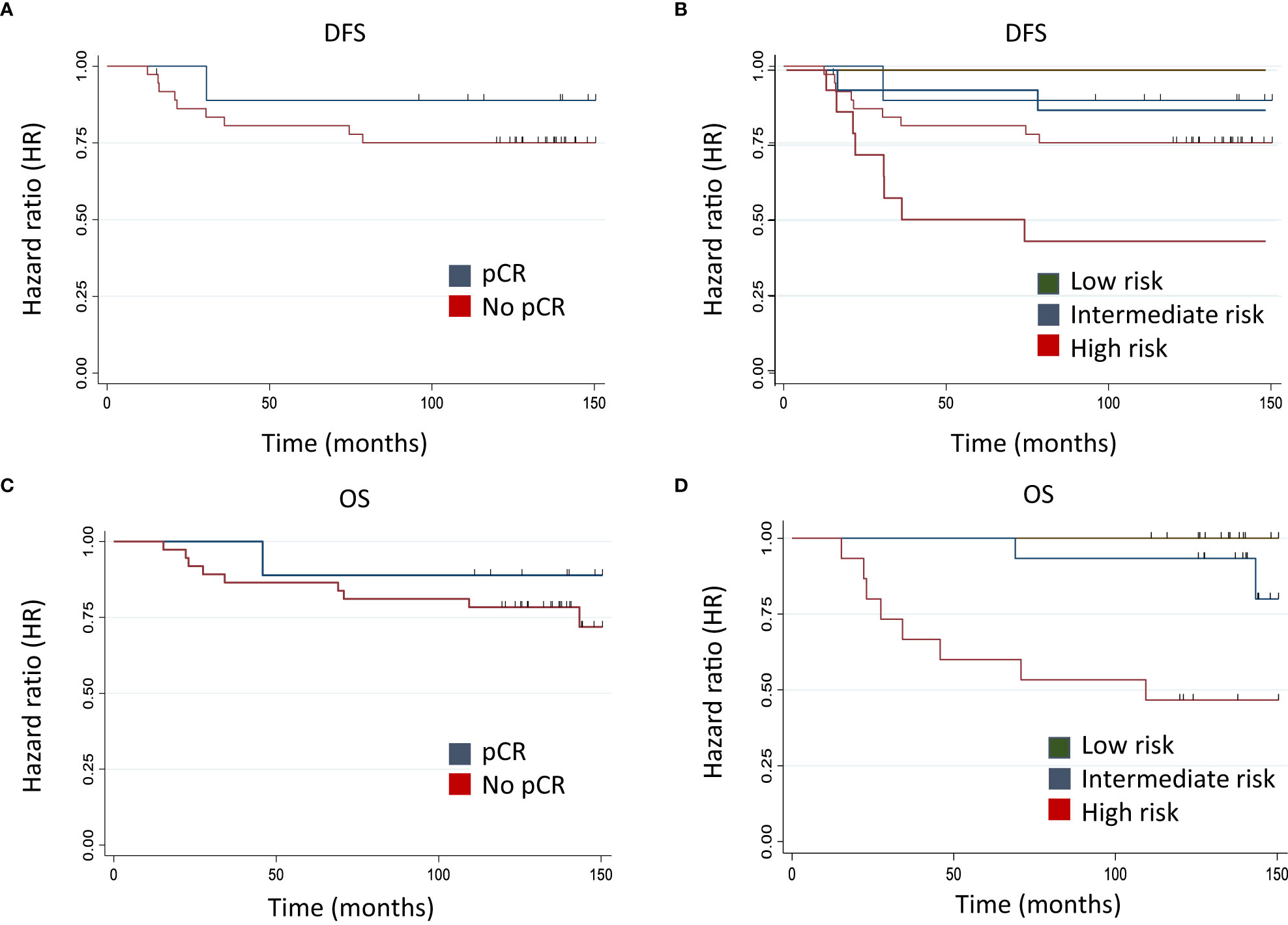
Figure 3 Model prediction with Kaplan-Meier curves for DFS and OS. Kaplan-Meier curves for DFS and OS obtained with predictions from clinical variable (pCR) (A, C) and model 3 (pCR, NLR, TILs AURKA, and MYBL2) (B, D), the latter divided into tertiles. Model 1: PLR DFS: 0.34 - PLR OS: 0.41. Model 3: PLR DFS: 0.0014 - PLR OS: 0.0054.
4 Discussion
The expanding body of knowledge of the immune response to BC and the differences between the systemic and microenvironment response provides opportunities for identifying predictive and prognostic biomarkers (10, 42). In the challenging context of neoadjuvant BC treatment, it is likely that several biomarkers will need to be combined to improve prognostic stratification (39, 43). Although pCR has been considered a surrogate marker of survival in early BC patients treated with NCT, in the luminal subtype we should probably consider additional markers to achieve better survival prediction. Moreover, the selection of patients who may gain real benefit from chemotherapy and those who may not is a pressing issue in the investigation of new therapeutic strategies and the avoidance of unnecessary chemotherapy side effects.
To explore new combination prognostic biomarkers, we conducted this study in a cohort of NCT-treated BC patients and investigated the prognostic implications for both DFS and OS of immune biomarkers in peripheral blood, such as NLR, and at the tumor level (TILs), together with genomic proliferation markers (AURKA, MYBL2, and MKI67) and conventional parameters, and response to NCT. Integrating all of these factors in a prognostic model consisting of NLR, TIL, AURKA and MYBL2, as a complement to HR/HER2 status and response to NCT, displayed a remarkable capacity to predict relapse and death.
Individually, NLR and TILs reflect systemic and local immune status, respectively. Specifically, for NLR, the results we obtained in our cohort were consistent with most of the literature reported to date. Zhoe et al. confirmed in a recent meta-analysis with 5504 BC patients treated with NCT that an NLR < 2.3 was predictive of pCR independently of tumor stage or grade and KI67 expression level (44). They also identified NLR as a prognostic biomarker, with patients with higher NLR levels having worse DFS (44). A previous meta-analysis of 8563 patients reached similar conclusions, with a large NLR cut-off range (1.9 – 5) and a median of 3 (14). In our study, we evaluated NLR as a continuous quantitative variable, thus avoiding the selection of an arbitrary or data-driven cut-off point. To better understand the significance of the NLR, we should probably investigate the dynamic change of NLR associated with chemotherapy. It has been reported that a lower NLR after chemotherapy predicts better pCR (45), while another study demonstrated that this change could be a predictor of pCR beyond the third NCT cycle (46). This is consistent with previous data generated by our group, that evaluated the prognostic value of peripheral blood lymphocytes and changes associated with NCT in BC patients (47).
The prognostic implications of TILs were also in line with earlier works (7, 48). The 12-year follow-up of our series of BC patients who received NCT is one of the longest published. It is relevant that in this 12-year study, TILs predict the same good prognosis as we reported in our 5-year study (9). One strength of this analysis is that, since there is no valid cut-off point and the evidence available is extremely heterogeneous, we have evaluated TILs as a continuous quantitative variable, which is the recommended approach in these cases (49). The positive response and outcome of women with greater lymphocyte infiltration could be, at least in part, due to the activation of the antitumor immune response during NCT, induced after DNA damage and cell death (50). A meta-analysis of 18170 BC patients confirmed high TILs as a predictive and prognostic biomarker in HER2+ and TNBC. In luminal subtypes, high TILs were correlated with poor prognosis (51). Unfortunately, our series is small for BC subtype analyses. Luminal BC is characterized by low TIL infiltration with low HLA expression, so other immune cells such as tumor associated macrophages (TAM) could be more relevant than T cells (52) or even NK cells whose role has not yet been studied in depth in BC. In this line, it is essential to determine the infiltrating lymphocyte subtypes in BC (9, 53). The significance of defining the immune-infiltrating cell type has been studied by an immune risk score analyses using TGCA and other database genes. A low prognostic immune risk score with five cell subtypes (B cells, endothelial cells, macrophages, NK cells, other cells) has been correlated with better survival in BC (54).
The correlation between NLR and TILs and their combined predictive capacity for adverse events has yet to be fully elucidated. Our study confirms the lack of correlation between both variables, suggesting that systemic and local immunities respond to different regulatory mechanisms (55); therefore, combined predictive models can offer a more comprehensive vision (39).This lack of correlation is consistent with previously published findings in TNBC and luminal BC (55–58). In our cohort, not only did both remain as independent prognostic variables in the multivariate analysis, but the combination of NLR and TILs improved the prognostic accuracy over pCR to NCT alone.
Genomics has improved our understanding of BC biology and revealed four intrinsic molecular subtypes with significant immunological differences, as previously mentioned (43). Immune-activated gene subsets, higher expression of proimmune factors and/or TILs have been associated with chemosensitivity, but also proliferation has been identified as a key factor in BC (59). Particularly, in the context of BC patients treated with NCT, proliferation markers correlate with oncologic progression and prognosis for the different IHC subtypes (60, 61). Therefore, the information they provide might complement what we learn from immunological biomarkers (61, 62). The choice of the optimal combination of proliferation markers was a difficult decision to make. Wirapati et al. published a meta-analysis of gene expression profiles with three gene modules (proliferation, ER signaling and ERBB2 amplification) in 2833 breast tumor to better understand cancer subtyping and prognosis signatures (63). AURKA was chosen as a proliferation gene based on this study and others already discussed in the introduction (23, 24, 64). As we mentioned previously, MYBL2 is one of the proliferation genes included in Oncotype, PAM50 and MammaPrint tests (19). Finally, MKI67 was chosen since Ki67 is used in the clinical setting to identify luminal B cases and the correlation between Ki67 and MKI67 has been previously established (65). One interesting finding is the statistically significant association observed between genomic markers MKI67 and MYBL2. Previous reports have shown that the expression of MKI67 can be regulated by MYBL2, and this regulation is not specific to BC (66, 67). In our cohort, we did not observe a significant correlation between the proliferation markers AURKA and MYBL2, although previous work have noted a shared transcription between them (68).
Our study has demonstrated the independent prognostic value of the combination of systemic and microenvironmental immune biomarkers (NLR and TILs) with genomic proliferation markers (AURKA and MYBL2) and classical clinical factors (HR/HER status, pCR). Compellingly, the addition of proliferation biomarkers markedly increased the discriminatory capacity of the model. The model combining all variables (HR/HER status, pCR, NLR, TILs, AURKA, and MYBL2) exhibited the greatest predictive ability for DFS and OS, both in terms of AIC and statistically significance (LLRT). To date, the factors associated with response to NCT have been obtained from clinical, pathological and molecular analyses. However, the majority of these studies include a limited sample size, combine data from patients with different therapeutic strategies and use profiles with isolated variables that fail to capture the complexity of the tumor ecosystem. As a result, empirical clinical risk stratification continues to be used for selecting patients who are candidates for neoadjuvant treatment (69).
Several studies have explored the combination of local immune biomarkers associated with classical clinical factors such as response to neoadjuvant treatment (39). In particular, TILs, PD-L1 and genomic signatures and their combinations have been extensively studied (39, 69). Prat et al. compared the three-gene model (SCMGENE) with ESR1, ERBB2 and AURKA with that of the PAM50 test. They concluded that while both models were able to anticipate patient outcomes, PAM50 was the superior model and the only one with predictive value. This was because PAM50 reveals biological diversity better than the three-gene model (70). Interestingly, our results are consistent with the results obtained using the three-gene model.
In this context, it is important to remark the potential benefit of a model that combines multiple biomarkers, in which all variable contribute to provide comprehensive patient information. Such a novel approach can provide an integrated immuno-genetic-oncological biomarker for selecting the most accurate therapy strategy. Furthermore, the available evidence suggest the potential value of the systematic implementation of combined biomarkers to improve patient selection and safety (39). To identify the most appropriate combined model, it is necessary to start exploring some of the most extensively studied biomarkers, as we have done in our original research.
Our study has some limitations. First, the method used to quantify TILs was based on IHC for CD3, which includes both stromal and intra-tumor lymphocytic infiltration and differs from the currently accepted method (49). However, our group has previously shown good correlation for TILs measured by IHC for CD3 with HE-based assessment of lymphocyte infiltration (9). Second, the use of genomic markers of proliferation differs from the more recent routine use of KI67 (71), although genomic signatures of proliferation are the strongest factor for prognostic stratification in most predictive genomic tests in early luminal BC (60, 72) and also comprise a key prognostic marker in non-luminal subtypes (73, 74). Finally, this is a small, single-center, retrospective cohort, in which it was not possible to perform subgroup analyses according to tumor subtype with sufficient statistical power to draw conclusions.
Nonetheless, our series does have a number of strengths that make it compelling. Besides having one of the longest follow-up published in literature, it is highly homogeneous with respect to clinical management, including diagnosis, NCT, and response determination, which are key to obtain and interpret data within the context of early BC. NCT, surgery and radiation therapy were performed according to usual clinical procedures and following current clinical practice guidelines, which makes treatment bias unlikely for the final prognostic model. Furthermore, the inclusion in our model of clinical classical factors, local immunological factors, such as TILs, systemic immune status, such as NLR, and two of the most relevant proliferation markers, is a novel approach in the study of breast cancer prognosis. These results warrant prospective, multi-centre validation studies with a larger sample size.
5 Conclusions
In conclusion, our study reveals that combining systemic immune and proliferation biomarkers with clinical-pathological markers improved the predictive capacity for DFS and OS compared to treatment response alone in a cohort of BC patients treated with NCT. The real benefit and clinical usefulness of these biomarker-based models should be confirmed in broader series. The validation of these findings in independent cohorts could provide a new tool for improving prognostic stratification and therapeutic management in these patients.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statement
The studies involving human participants were reviewed and approved by Clinical Research and Trials Comittee of the University Hospital Morales Meseguer. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Concept, EG-T, EM, FP and EG-M. Data curation, EG-T, EM, EG-G, FP and EG-M. Formal analysis, EG-T, EM, FP and EG-M. Funding acquisition, FP. and EG-M. Investigation, EG-T, EM, GL-G, PB, MP-R, FP, and EG-M. Methodology, EG-T, EM, GL-G, MP-R, FP, and EG-M. Project administration, EG-T, EM, GL-G, FP and EG-M. Supervision, FP and EG-M. Writing—original draft, EG-T, FP and EG-M. Writing—review and editing, EG-T. EM, GL-G, PB., AB, MP-R, BA-A, AR, EG-G, FP, and EG-M. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Ana Balil-GEICAM grant (Spanish Breast Cancer Research Group); the funding institution has not participated in collecting, analyzing, or interpreting the data, nor did it participate in drafting this manuscript. This work was also supported by Instituto de Salud Carlos III (PI12/02877), including FEDER funding by the European Union. ENM was funded by the Ministerio de Educación, Cultura y Deporte [Ministry of Education, Culture, and Sports] (Spain) [FPU16/06537]. This work was also partially funded by two research-funding initiatives: “Calasparra se mueve”, inspired by women from Calasparra (Murcia), Spain, and “Pulseras solidarias”, Cieza (Murcia), Spain. The sponsors have in no way been involved in the study design, data collection, and analysis, decision to publish, or preparation of the manuscript. BIOBANC-MUR is supported by the Instituto de Salud Carlos III (project PT20/00109), by the Instituto Murciano de Investigación Biosanitaria, IMIB and by the Consejeria de Salud de la Comunidad Autónoma de la Región de Murcia [the regional healthcare authority for the Autonomous Community of Murcia].
Acknowledgments
The authors thank Dr Carlos Bravo-Pérez (Department of Haematology and Medical Oncology) for his contributions and critical review of the statistical analyses and writing style. We are particularly grateful for the generous contribution of the patients and the collaboration of the Biobank Network of the Region of Murcia, BIOBANC-MUR, registered with the National Registry of Biobanks with registration number B.0000859.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1182725/full#supplementary-material
References
1. Untch M, Konecny GE, Paepke S, von Minckwitz G. Current and future role of neoadjuvant therapy for breast cancer. Breast (2014) 23:526–37. doi: 10.1016/j.breast.2014.06.004
2. van Nes JGH, Putter H, Julien J-P, Tubiana-Hulin M, van de Vijver M, Bogaerts J, et al. Preoperative chemotherapy is safe in early breast cancer, even after 10 years of follow-up; clinical and translational results from the EORTC trial 10902. Breast Cancer Res Treat (2009) 115:101–13. doi: 10.1007/s10549-008-0050-1
3. Haque W, Verma V, Hatch S, Suzanne Klimberg V, Brian Butler E, Teh BS. Response rates and pathologic complete response by breast cancer molecular subtype following neoadjuvant chemotherapy. Breast Cancer Res Treat (2018) 170:559–67. doi: 10.1007/s10549-018-4801-3
4. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet (2014) 384:164–72. doi: 10.1016/S0140-6736(13)62422-8
5. Mamounas EP, Anderson SJ, Dignam JJ, Bear HD, Julian TB, Geyer CEJ, et al. Predictors of locoregional recurrence after neoadjuvant chemotherapy: results from combined analysis of national surgical adjuvant breast and bowel project b-18 and b-27. J Clin Oncol (2012) 30:3960–6. doi: 10.1200/JCO.2011.40.8369
6. LeVasseur N, Sun J, Gondara L, Diocee R, Speers C, Lohrisch C, et al. Impact of pathologic complete response on survival after neoadjuvant chemotherapy in early-stage breast cancer: a population-based analysis. J Cancer Res Clin Oncol (2020) 146:529–36. doi: 10.1007/s00432-019-03083-y
7. Denkert C, von Minckwitz G, Darb-Esfahani S, Lederer B, Heppner BI, Weber KE, et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol (2018) 19:40–50. doi: 10.1016/S1470-2045(17)30904-X
8. Dieci MV, Radosevic-Robin N, Fineberg S, van den Eynden G, Ternes N, Penault-Llorca F, et al. Update on tumor-infiltrating lymphocytes (TILs) in breast cancer, including recommendations to assess TILs in residual disease after neoadjuvant therapy and in carcinoma in situ: a report of the international immuno-oncology biomarker working group on breast cancer. Semin Cancer Biol (2018) 52:16–25. doi: 10.1016/j.semcancer.2017.10.003
9. García-Martínez E, Gil GL, Benito AC, González-Billalabeitia E, Conesa MAV, García García T, et al. Tumor-infiltrating immune cell profiles and their change after neoadjuvant chemotherapy predict response and prognosis of breast cancer. Breast Cancer Res (2014) 16:488. doi: 10.1186/s13058-014-0488-5
10. Hiam-Galvez KJ, Allen BM, Spitzer MH. Systemic immunity in cancer. Nat Rev Cancer (2021) 21:345–59. doi: 10.1038/s41568-021-00347-z
11. Templeton AJ, McNamara MG, Šeruga B, Vera-Badillo FE, Aneja P, Ocaña A, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst (2014) 106:dju124. doi: 10.1093/jnci/dju124
12. Cupp MA, Cariolou M, Tzoulaki I, Aune D, Evangelou E, Berlanga-Taylor AJ. Neutrophil to lymphocyte ratio and cancer prognosis: an umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med (2020) 18:360. doi: 10.1186/s12916-020-01817-1
13. McAndrew NP, Bottalico L, Mesaros C, Blair IA, Tsao PY, Rosado JM, et al. Effects of systemic inflammation on relapse in early breast cancer. NPJ Breast Cancer (2021) 7:7. doi: 10.1038/s41523-020-00212-6
14. Ethier J-L, Desautels D, Templeton A, Shah PS, Amir E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: a systematic review and meta-analysis. Breast Cancer Res (2017) 19:2. doi: 10.1186/s13058-016-0794-1
15. Ivars Rubio A, Yufera JC, de la Morena P, Fernández Sánchez A, Navarro Manzano E, García Garre E, et al. Neutrophil-lymphocyte ratio in metastatic breast cancer is not an independent predictor of survival, but depends on other variables. Sci Rep (2019) 9:16979. doi: 10.1038/s41598-019-53606-3
16. Cullinane C, Creavin B, O’Leary DP, O’Sullivan MJ, Kelly L, Redmond HP, et al. Can the neutrophil to lymphocyte ratio predict complete pathologic response to neoadjuvant breast cancer treatment? a systematic review and meta-analysis. Clin Breast Cancer (2020) 20:e675–81. doi: 10.1016/j.clbc.2020.05.008
17. Yerushalmi R, Woods R, Ravdin PM, Hayes MM, Gelmon KA. Ki67 in breast cancer: prognostic and predictive potential. Lancet Oncol (2010) 11:174–83. doi: 10.1016/S1470-2045(09)70262-1
18. Paik S, Shak S, Tang G, Kim C, Baker J, Cronin M, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med (2004) 351:2817–26. doi: 10.1056/NEJMoa041588
19. Beňačka R, Szabóová D, Guľašová Z, Hertelyová Z, Radoňák J. Classic and new markers in diagnostics and classification of breast cancer. Cancers (Basel) (2022) 14(21):5444–5466. doi: 10.3390/cancers14215444
20. Kalinsky K, Barlow WE, Gralow JR, Meric-Bernstam F, Albain KS, Hayes DF, et al. 21-gene assay to inform chemotherapy benefit in node-positive breast cancer. N Engl J Med (2021) 385:2336–47. doi: 10.1056/NEJMoa2108873
21. Du R, Huang C, Liu K, Li X, Dong Z. Targeting AURKA in cancer: molecular mechanisms and opportunities for cancer therapy. Mol Cancer (2021) 20:15. doi: 10.1186/s12943-020-01305-3
22. Whately KM, Voronkova MA, Maskey A, Gandhi J, Loskutov J, Choi H, et al. Nuclear aurora-a kinase-induced hypoxia signaling drives early dissemination and metastasis in breast cancer: implications for detection of metastatic tumors. Oncogene (2021) 40:5651–64. doi: 10.1038/s41388-021-01969-1
23. Xu J, Wu X, Zhou W, Liu A, Wu J, Deng J, et al. Aurora-a identifies early recurrence and poor prognosis and promises a potential therapeutic target in triple negative breast cancer. PLoS One (2013) 8:e56919. doi: 10.1371/journal.pone.0056919
24. Siggelkow W, Boehm D, Gebhard S, Battista M, Sicking I, Lebrecht A, et al. Expression of aurora kinase a is associated with metastasis-free survival in node-negative breast cancer patients. BMC Cancer (2012) 12:562. doi: 10.1186/1471-2407-12-562
25. Jalalirad M, Haddad TC, Salisbury JL, Radisky D, Zhang M, Schroeder M, et al. Aurora-a kinase oncogenic signaling mediates TGF-β-induced triple-negative breast cancer plasticity and chemoresistance. Oncogene (2021) 40:2509–23. doi: 10.1038/s41388-021-01711-x
26. Zhang Y, Wang Y, Xue J. Paclitaxel inhibits breast cancer metastasis via suppression of aurora kinase-mediated cofilin-1 activity. Exp Ther Med (2018) 15:1269–76. doi: 10.3892/etm.2017.5588
27. Zhou T, Zhang A, Kuang G, Gong X, Jiang R, Lin D, et al. Baicalin inhibits the metastasis of highly aggressive breast cancer cells by reversing epithelial-to-mesenchymal transition by targeting β-catenin signaling. Oncol Rep (2017) 38:3599–607. doi: 10.3892/or.2017.6011
28. Hole S, Pedersen AM, Lykkesfeldt AE, Yde CW. Aurora kinase a and b as new treatment targets in aromatase inhibitor-resistant breast cancer cells. Breast Cancer Res Treat (2015) 149:715–26. doi: 10.1007/s10549-015-3284-8
29. Lykkesfeldt AE, Iversen BR, Jensen M-B, Ejlertsen B, Giobbie-Hurder A, Reiter BE, et al. Aurora kinase a as a possible marker for endocrine resistance in early estrogen receptor positive breast cancer. Acta Oncol (2018) 57:67–73. doi: 10.1080/0284186X.2017.1404126
30. Donnella HJ, Webber JT, Levin RS, Camarda R, Momcilovic O, Bayani N, et al. Kinome rewiring reveals AURKA limits PI3K-pathway inhibitor efficacy in breast cancer. Nat Chem Biol (2018) 14:768–77. doi: 10.1038/s41589-018-0081-9
31. Wander SA, Cohen O, Gong X, Johnson GN, Buendia-Buendia JE, Lloyd MR, et al. The genomic landscape of intrinsic and acquired resistance to cyclin-dependent kinase 4/6 inhibitors in patients with hormone receptor-positive metastatic breast cancer. Cancer Discovery (2020) 10:1174–93. doi: 10.1158/2159-8290.CD-19-1390
32. Morris BB, Smith JP, Zhang Q, Jiang Z, Hampton OA, Churchman ML, et al. Replicative instability drives cancer progression. Biomolecules (2022) 12(11):1570–1592. doi: 10.3390/biom12111570
33. Shi H, Bevier M, Johansson R, Enquist-Olsson K, Henriksson R, Hemminki K, et al. Prognostic impact of polymorphisms in the MYBL2 interacting genes in breast cancer. Breast Cancer Res Treat (2012) 131:1039–47. doi: 10.1007/s10549-011-1826-2
34. Bayley R, Ward C, Garcia P. MYBL2 amplification in breast cancer: molecular mechanisms and therapeutic potential. Biochim Biophys Acta Rev Cancer (2020) 1874:188407. doi: 10.1016/j.bbcan.2020.188407
35. Tao D, Pan Y, Jiang G, Lu H, Zheng S, Lin H, et al. B-myb regulates snail expression to promote epithelial-to-mesenchymal transition and invasion of breast cancer cell. Med Oncol (2015) 32:412. doi: 10.1007/s12032-014-0412-y
36. Chen X, Lu Y, Yu H, Du K, Zhang Y, Nan Y, et al. Pan-cancer analysis indicates that MYBL2 is associated with the prognosis and immunotherapy of multiple cancers as an oncogene. Cell Cycle (2021) 20:2291–308. doi: 10.1080/15384101.2021.1982494
37. Li X, Zhang X, Wu C-C, Li P-P, Fu Y-M, Xie L-H, et al. The role of MYB proto-oncogene like 2 in tamoxifen resistance in breast cancer. J Mol Histol (2021) 52:21–30. doi: 10.1007/s10735-020-09920-6
38. Guarneri V, Dieci MV, Bisagni G, Brandes AA, Frassoldati A, Cavanna L, et al. PIK3CA mutation in the ShortHER randomized adjuvant trial for patients with early HER2(+) breast cancer: association with prognosis and integration with PAM50 subtype. Clin Cancer Res (2020) 26:5843–51. doi: 10.1158/1078-0432.CCR-20-1731
39. Gonzalez-Ericsson PI, Stovgaard ES, Sua LF, Reisenbichler E, Kos Z, Carter JM, et al. The path to a better biomarker: application of a risk management framework for the implementation of PD-L1 and TILs as immuno-oncology biomarkers in breast cancer clinical trials and daily practice. J Pathol (2020) 250:667–84. doi: 10.1002/path.5406
40. Filho OM, Stover DG, Asad S, Ansell PJ, Watson M, Loibl S, et al. Association of immunophenotype with pathologic complete response to neoadjuvant chemotherapy for triple-negative breast cancer: a secondary analysis of the BrighTNess phase 3 randomized clinical trial. JAMA Oncol (2021) 7:603–8. doi: 10.1001/jamaoncol.2020.7310
41. Carlson RW, Anderson BO, Burstein HJ, Carter WB, Edge SB, Farrar WB, et al. Invasive breast cancer. J Natl Compr Canc Netw (2007) 5:246–312. doi: 10.6004/jnccn.2007.0025
42. Dieci MV, Miglietta F, Guarneri V. Immune infiltrates in breast cancer: recent updates and clinical implications. Cells (2021) 10(2):223–250. doi: 10.3390/cells10020223
43. Hammerl D, Smid M, Timmermans AM, Sleijfer S, Martens JWM, Debets R. Breast cancer genomics and immuno-oncological markers to guide immune therapies. Semin Cancer Biol (2018) 52:178–88. doi: 10.1016/j.semcancer.2017.11.003
44. Zhou Q, Dong J, Sun Q, Lu N, Pan Y, Han X. Role of neutrophil-to-lymphocyte ratio as a prognostic biomarker in patients with breast cancer receiving neoadjuvant chemotherapy: a meta-analysis. BMJ Open (2021) 11:e047957. doi: 10.1136/bmjopen-2020-047957
45. Dan J, Tan J, Huang J, Zhang X, Guo Y, Huang Y, et al. The dynamic change of neutrophil to lymphocyte ratio is predictive of pathological complete response after neoadjuvant chemotherapy in breast cancer patients. Breast Cancer (2020) 27:982–8. doi: 10.1007/s12282-020-01096-x
46. Choi H, Noh H, Cho I-J, Lim S-T, Han A. Changes in neutrophil to lymphocyte ratio (NLR) during neoadjuvant treatment correlated with patients’ survival. Breast Cancer (2020) 27:871–9. doi: 10.1007/s12282-020-01083-2
47. Vicente Conesa MA, Garcia-Martinez E, Gonzalez Billalabeitia E, Chaves Benito A, Garcia Garcia T, Vicente Garcia V, et al. Predictive value of peripheral blood lymphocyte count in breast cancer patients treated with primary chemotherapy. Breast (2012) 21:468–74. doi: 10.1016/j.breast.2011.11.002
48. Denkert C, Loibl S, Noske A, Roller M, Müller BM, Komor M, et al. Tumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancer. J Clin Oncol (2010) 28:105–13. doi: 10.1200/JCO.2009.23.7370
49. Salgado R, Denkert C, Demaria S, Sirtaine N, Klauschen F, Pruneri G, et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an international TILs working group 2014. Ann Oncol (2015) 26:259–71. doi: 10.1093/annonc/mdu450
50. Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity (2013) 39:1–10. doi: 10.1016/j.immuni.2013.07.012
51. Gao Z-H, Li C-X, Liu M, Jiang J-Y. Predictive and prognostic role of tumour-infiltrating lymphocytes in breast cancer patients with different molecular subtypes: a meta-analysis. BMC Cancer (2020) 20:1150. doi: 10.1186/s12885-020-07654-y
52. Goldberg J, Pastorello RG, Vallius T, Davis J, Cui YX, Agudo J, et al. The immunology of hormone receptor positive breast cancer. Front Immunol (2021) 12:674192. doi: 10.3389/fimmu.2021.674192
53. Mao P, Cohen O, Kowalski KJ, Kusiel JG, Buendia-Buendia JE, Cuoco MS, et al. Acquired FGFR and FGF alterations confer resistance to estrogen receptor (ER) targeted therapy in ER(+) metastatic breast cancer. Clin Cancer Res (2020) 26:5974–89. doi: 10.1158/1078-0432.CCR-19-3958
54. Sun Y, Zhang C. The types of tumor infiltrating lymphocytes are valuable for the diagnosis and prognosis of breast cancer. Front Genet (2022) 13:1019062. doi: 10.3389/fgene.2022.1019062
55. Pang J, Zhou H, Dong X, Wang S, Xiao Z. Relationship between the neutrophil to lymphocyte ratio, stromal tumor-infiltrating lymphocytes, and the prognosis and response to neoadjuvant chemotherapy in triple-negative breast cancer. Clin Breast Cancer (2021) 21:e681–7. doi: 10.1016/j.clbc.2021.04.004
56. Dong X, Liu C, Yuan J, Wang S, Ding N, Li Y, et al. Prognostic roles of neutrophil-to-Lymphocyte ratio and stromal tumor-infiltrating lymphocytes and their relationship in locally advanced triple-negative breast cancer treated with neoadjuvant chemotherapy. Breast Care (Basel) (2021) 16:328–34. doi: 10.1159/000509498
57. Lee J, Kim D-M, Lee A. Prognostic role and clinical association of tumor-infiltrating lymphocyte, programmed death ligand-1 expression with neutrophil-lymphocyte ratio in locally advanced triple-negative breast cancer. Cancer Res Treat (2019) 51:649–63. doi: 10.4143/crt.2018.270
58. Bun A, Fujimoto Y, Higuchi T, Sata A, Fukui R, Ozawa H, et al. Prognostic significance of neutrophil-to-lymphocyte ratio in luminal breast cancers with low levels of tumour-infiltrating lymphocytes. Anticancer Res (2020) 40:2871–80. doi: 10.21873/anticanres.14263
59. Denkert C, Loibl S, Müller BM, Eidtmann H, Schmitt WD, Eiermann W, et al. Ki67 levels as predictive and prognostic parameters in pretherapeutic breast cancer core biopsies: a translational investigation in the neoadjuvant GeparTrio trial. Ann Oncol (2013) 24:2786–93. doi: 10.1093/annonc/mdt350
60. Torrisi R, Marrazzo E, Agostinetto E, De Sanctis R, Losurdo A, Masci G, et al. Neoadjuvant chemotherapy in hormone receptor-positive/HER2-negative early breast cancer: when, why and what? Crit Rev Oncol Hematol (2021) 160:103280. doi: 10.1016/j.critrevonc.2021.103280
61. Sinn BV, Loibl S, Hanusch CA, Zahm D-M, Sinn H-P, Untch M, et al. Immune-related gene expression predicts response to neoadjuvant chemotherapy but not additional benefit from PD-L1 inhibition in women with early triple-negative breast cancer. Clin Cancer Res (2021) 27:2584–91. doi: 10.1158/1078-0432.CCR-20-3113
62. Wang K, Li H-L, Xiong Y-F, Shi Y, Li Z-Y, Li J, et al. Development and validation of nomograms integrating immune-related genomic signatures with clinicopathologic features to improve prognosis and predictive value of triple-negative breast cancer: a gene expression-based retrospective study. Cancer Med (2019) 8:686–700. doi: 10.1002/cam4.1880
63. Wirapati P, Sotiriou C, Kunkel S, Farmer P, Pradervand S, Haibe-Kains B, et al. Meta-analysis of gene expression profiles in breast cancer: toward a unified understanding of breast cancer subtyping and prognosis signatures. Breast Cancer Res (2008) 10:R65. doi: 10.1186/bcr2124
64. Fadaka AO, Sibuyi NRS, Madiehe AM, Meyer M. MicroRNA-based regulation of aurora a kinase in breast cancer. Oncotarget (2020) 11:4306–24. doi: 10.18632/oncotarget.27811
65. Chen L, Chen Y, Xie Z, Luo J, Wang Y, Zhou J, et al. Comparison of immunohistochemistry and RT-qPCR for assessing ER, PR, HER2, and Ki67 and evaluating subtypes in patients with breast cancer. Breast Cancer Res Treat (2022) 194:517–29. doi: 10.1007/s10549-022-06649-6
66. Qin H, Li Y, Zhang H, Wang F, He H, Bai X, et al. Prognostic implications and oncogenic roles of MYBL2 protein expression in esophageal squamous-cell carcinoma. Onco Targets Ther (2019) 12:1917–27. doi: 10.2147/OTT.S190145
67. Luengo-Gil G, García-Martínez E, Chaves-Benito A, Conesa-Zamora P, Navarro-Manzano E, González-Billalabeitia E, et al. Clinical and biological impact of miR-18a expression in breast cancer after neoadjuvant chemotherapy. Cell Oncol (Dordr) (2019) 42:627–44. doi: 10.1007/s13402-019-00450-2
68. Musa J, Aynaud M-M, Mirabeau O, Delattre O, Grünewald TG. MYBL2 (B-myb): a central regulator of cell proliferation, cell survival and differentiation involved in tumorigenesis. Cell Death Dis (2017) 8:e2895. doi: 10.1038/cddis.2017.244
69. Sammut S-J, Crispin-Ortuzar M, Chin S-F, Provenzano E, Bardwell HA, Ma W, et al. Multi-omic machine learning predictor of breast cancer therapy response. Nature (2022) 601:623–9. doi: 10.1038/s41586-021-04278-5
70. Prat A, Parker JS, Fan C, Perou CM. PAM50 assay and the three-gene model for identifying the major and clinically relevant molecular subtypes of breast cancer. Breast Cancer Res Treat (2012) 135:301–6. doi: 10.1007/s10549-012-2143-0
71. Nielsen TO, Leung SCY, Rimm DL, Dodson A, Acs B, Badve S, et al. Assessment of Ki67 in breast cancer: updated recommendations from the international Ki67 in breast cancer working group. J Natl Cancer Inst (2021) 113:808–19. doi: 10.1093/jnci/djaa201
72. Buus R, Sestak I, Kronenwett R, Ferree S, Schnabel CA, Baehner FL, et al. Molecular drivers of oncotype DX, prosigna, EndoPredict, and the breast cancer index: a TransATAC study. J Clin Oncol (2021) 39:126–35. doi: 10.1200/JCO.20.00853
73. Stover DG, Coloff JL, Barry WT, Brugge JS, Winer EP, Selfors LM. The role of proliferation in determining response to neoadjuvant chemotherapy in breast cancer: a gene expression-based meta-analysis. Clin Cancer Res (2016) 22:6039–50. doi: 10.1158/1078-0432.CCR-16-0471
Keywords: Breast cancer, neoadjuvant chemotherapy, neutrophil-to-lymphocyte ratio, tumor-infiltrating lymphocytes, proliferation markers
Citation: García-Torralba E, Navarro Manzano E, Luengo-Gil G, De la Morena Barrio P, Chaves Benito A, Pérez-Ramos M, Álvarez-Abril B, Ivars Rubio A, García-Garre E, Ayala de la Peña F and García-Martínez E (2023) A new prognostic model including immune biomarkers, genomic proliferation tumor markers (AURKA and MYBL2) and clinical-pathological features optimizes prognosis in neoadjuvant breast cancer patients. Front. Oncol. 13:1182725. doi: 10.3389/fonc.2023.1182725
Received: 09 March 2023; Accepted: 17 May 2023;
Published: 29 May 2023.
Edited by:
Chao Liu, Shandong Cancer Hospital, ChinaReviewed by:
Jingyi Xie, University of Washington, United StatesXin Li, Houston Methodist Research Institute, United States
Copyright © 2023 García-Torralba, Navarro Manzano, Luengo-Gil, De la Morena Barrio, Chaves Benito, Pérez-Ramos, Álvarez-Abril, Ivars Rubio, García-Garre, Ayala de la Peña and García-Martínez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisco Ayala de la Peña, ZnJheWFsYUB1bS5lcw==
†ORCID: Francisco Ayala de la Peña, orcid.org/0000-0001-6311-920X