 Liang-Kang Huang1
Liang-Kang Huang1 Yu-Ching Lin2Hai-Hua Chuang3Cheng-Keng Chuang1See-Tong Pang1Chun-Te Wu1Ying-Hsu Chang4Kai-Jie Yu1
Yu-Ching Lin2Hai-Hua Chuang3Cheng-Keng Chuang1See-Tong Pang1Chun-Te Wu1Ying-Hsu Chang4Kai-Jie Yu1 Po-Hung Lin1Hung-Cheng Kan1Yuan-Cheng Chu1Wei-Kang Hung5Ming-Li Hsieh1I-Hung Shao1*
Po-Hung Lin1Hung-Cheng Kan1Yuan-Cheng Chu1Wei-Kang Hung5Ming-Li Hsieh1I-Hung Shao1*- 1Division of Urology, Department of Surgery, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
- 2Department of Medical Imaging and Intervention, Chang Gung Memorial Hospital, Keelung and Chang Gung University, Taoyuan, Taiwan
- 3Department of Family Medicine, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan
- 4Department of Urology, New Taipei Municipal TuCheng Hospital, Chang Gung Memorial Hospital and Chang Gung University, New Taipei, Taiwan
- 5College of Medicine, Chang Gung University, Taoyuan, Taiwan
Introduction: Body status, categorized as sarcopenia or obesity and assessed using body mass index and body composition, affects the outcome of bladder cancer patients. However, studies comparing disease progression, recurrence, or overall survival in patients with non-muscle-invasive bladder cancer (NMIBC) with different body compositions are lacking. Therefore, we conducted a retrospective study to identify the impact of body composition, sarcopenia, and obesity on the oncological prognosis of patients with NMIBC who underwent transurethral resection of bladder tumor (TURBT) with Bacillus Calmette-Guerin (BCG) intravesical instillation (IVI).
Methods: Patients with NMIBC who had undergone TURBT with adjuvant IVI with BCG from March 2005 to April 2021 were included. Body composition parameters were evaluated using computed tomography images of the third lumbar vertebrae and further categorized by sarcopenia and obesity. Oncological outcomes including recurrence-free survival (RFS), progression-free survival, and overall survival (OS) after treatment were analyzed.
Results: A total of 269 patients were enrolled. Subcutaneous adipose tissue (SAT) density was a significant predictor of RFS, whereas psoas muscle density was a significant predictor of OS in the multivariate analysis. Patients with sarcopenia but without obesity tolerated significantly fewer BCG IVIs than patients without sarcopenia or obesity. Patients with sarcopenia had poorer RFS and OS than those without sarcopenia. In contrast, patients with obesity had better OS than those without obesity.
Discussion: Body composition parameters, including SAT density and psoas muscle density, emerged as significant predictors of OS and RFS, respectively. Hence, our findings indicate that body composition is a helpful measurement to assess the oncological outcomes of patients with NMIBC.
1 Introduction
Bladder cancer (BC) is the 10th most common cancer worldwide. BC is divided into two categories: non-muscle-invasive bladder cancer (NMIBC) and muscle-invasive bladder cancer (MIBC). The majority of the patients are initially diagnosed with NMIBC, and the 5-year survival rate of NMIBC is 90–98%, whereas only a 35–40% survival rate is reported for those with MIBC. Standard treatment of NMIBC includes transurethral resection of bladder tumor (TURBT) and intravesical instillation (IVI) with chemotherapy or immunotherapy (1). In contrast to MIBC, the most distinct treatment goal of NMIBC is to both spare the bladder and achieve oncological control. However, the strategy of sparing the bladder to maintain the quality of life could lead to a high risk of local recurrence. Thus, high 5-year recurrence (28.3–51.7%) and progression rates (4.6–19.8%) have been reported in the NMIBC patient population (2). Despite receiving IVI, a notable proportion of patients with NMIBC may still experience disease recurrence or progression to MIBC, which could lead to poor survival outcomes. Various studies have identified the risk factors for the recurrence of NMIBC after treatment, namely multifocal tumors larger than 3 cm, high tumor grade, or carcinoma in situ (3).
Among various risk factors, high body mass index (BMI) is also an independent risk factor for BC (4). BMI is simple, easy to measure, and is currently the most commonly used index to evaluate nutritional or metabolic status. It is simply expressed as the ratio of weight to height but does not distinguish between muscle and fat tissue (5). Meanwhile, body composition, which compensates for the limitations of BMI, is used to describe the percentage of fat, bone, and muscle in a human body.
Based on BMI and body composition, body status can be further categorized as sarcopenia and obesity, which has been reported to have a marked impact on the outcome of patients with BC. A meta-analysis conducted by Guo et al., which included patients who had undergone surgery for urological cancers, showed that sarcopenia had a worse impact on both overall and disease-specific survival (6). Furthermore, several authors have reported negative survival outcomes in patients with BC with sarcopenia after neoadjuvant chemotherapy and radical cystectomy (RC) (7, 8).
Obesity represents a type of body composition and may increase the risk of BC. Adiposity is connected with alterations in sex hormone metabolism, adipokine pathways, and inflammatory processes (9, 10). Although obesity is associated with increased incidence and poor prognosis in some cancers, including BC, a positive impact has been observed when patients with high BMI receive systemic immunotherapy with checkpoint inhibitors, resulting in improved outcomes (11). The phenomenon is sometimes known as the “obesity paradox” (12). There are conflicting opinions regarding the influence of obesity on BC prognosis.
Many studies have been conducted to determine the impact of sarcopenia or obesity on patients with MIBC. To the best of our knowledge, no study has compared disease progression, recurrence, or overall survival in patients with NMIBC with different body compositions. This study aimed to assess the impact of body composition, sarcopenia, and obesity on the oncological prognosis of patients with NMIBC.
2 Materials and methods
2.1 Patients
We retrospectively included patients with NMIBC who underwent TURBT with adjuvant Bacillus Calmette-Guerin (BCG) IVI from March 2005 to April 2021. All patients fulfilled the criteria of intermediate- or high-risk group classification, and all patients were newly diagnosed with NMIBC and were treatment naïve, with no recurrence. The medical charts and computed tomography (CT) images of all the patients were collected from a single tertiary medical center. Patients with incomplete data or images were excluded. This study was approved by the Institutional Review Board of the Chang Gung Medical Foundation (IRB no. 202100259B0) and followed the ethical principles outlined in the Declaration of Helsinki. The requirement for informed consent was waived owing to the retrospective study design.
2.2 Data collection
According to the American Joint Committee on Cancer, NMIBC is defined as carcinoma in situ (Tis), tumors confined to the mucosa (Ta), or tumors invading the lamina propria (T1). All preoperative patient information, including height, weight, underlying diseases, and Eastern Cooperative Oncology Group performance status, were recorded. Information on tumor-related parameters, such as tumor histologic type, primary tumor numbers, and whether the patient had any cancer other than BC or upper tract urothelial carcinoma, were also collected. Recurrence-free survival (RFS), progression-free survival (PFS), and overall survival (OS) were documented as endpoints. Survival status was documented according to the patient’s chart or condition at the last follow-up. RFS was measured from disease-free time to the time of recurrence in the bladder, detected using cystoscopy or follow-up imaging. Progression was defined as Tis, Ta, or T1 to a higher stage of T2 to T4, any N or any M. PFS was defined as disease-free time to the time of progression according to the imaging or pathology report during follow-up. OS was assessed from the first TURBT until death or the last follow-up.
2.3 Image analyses
For the assessment of body composition, we obtained CT images of patients before surgery as the benchmark and selected four images at the level of the third lumbar vertebra (L3) for subsequent analyses. We then assessed body composition based on CT images. CT images were analyzed, and five indices were derived from the image, including subcutaneous adipose tissue (SAT), visceral adipose tissue (VAT), all skeletal muscles (MUSCLE), paraspinal muscle (PARA), and psoas muscle (PSOAS). All indices were calculated with the area in square centimeters (cm2) and radiation attenuation in the Hounsfield unit (HU).
Body composition area is a measurement of the axial slice close to the inferior aspect of the vertebral body. The height adjustment area was computed as the body composition area divided by the square of height, which normalized the area of adipose tissue or muscle for height. Radiation attenuation is a measurement of the fat content of adipose tissue or muscle and is correlated with physical function. Radiation attenuation was calculated as the mean HU value of all pixels within the intended area of adipose tissue or muscle (13).
2.4 Sarcopenia and obesity
According to the European Working Group on Sarcopenia in Older Adults, the cutoff value of sarcopenia is set at two standard deviations below the mean of the healthy young adult population (14). According to Derstine et al., the cutoff values of skeletal muscle area and radiation attenuation at the L3 level of sarcopenia were 34.4 cm2/m2 and 34.3 HU, respectively, in women and 45.4 cm2/m2 and 38.5 HU, respectively, in men (13). In this study, we also considered adipose tissue and muscle, and patients with both indices below the cutoff values were included in the sarcopenia group.
BMI is a widely recognized surrogate marker for adiposity for patients of any age, calculated as weight divided by the square of height (kg/m2). Obesity is defined as BMI greater than 30 kg/m2. However, in Taiwan, the Ministry of Health and Welfare defines obesity as a BMI greater than 27 kg/m2. Therefore, in this study, patients with a BMI greater than 27 kg/m2 were included in the obese group (15).
2.5 Statistical analyses
Pearson’s correlation test was used to analyze the association between sarcopenia and obesity in patients with NMIBC according to age at diagnosis, number of BCG IVIs, and cancer stage. The correlation between the prognostic factors and endpoints was assessed using Cox proportional hazards models and logistic regression test. Finally, Kaplan–Meier survival test was used to determine the correlation between sarcopenia/obesity and survival benefits. All tests were two-sided, and p-values <0.05 were statistically significant. All statistical analyses were performed using IBM SPSS Statistics for Mac, version 25 (IBM Corp, Armonk, NY, USA).
3 Results
We initially restrospectively collected 2779 bladder cancer patients. In total, 269 patients were enrolled in this study. The flowchart was showed in Figure 1. Among them, 208 (77.3%) were men and 61 (22.7%) were women. The mean age of the patients at diagnosis was 66.41 years. All patients were diagnosed with NMIBC, and most had Ta or T1 disease, accounting for 44.6% and 50.9%, respectively. According to the CT images and BMI data obtained at the time of the initial diagnosis of NMIBC, 80 patients had sarcopenia, whereas 53 had obesity, accounting for 29.7% and 19.7%, respectively. A total of 111 patients (41.3%) experienced recurrence, whereas 68 (25.3%) experienced progression. The other general characteristics and tumor-related parameters are presented in Table 1.
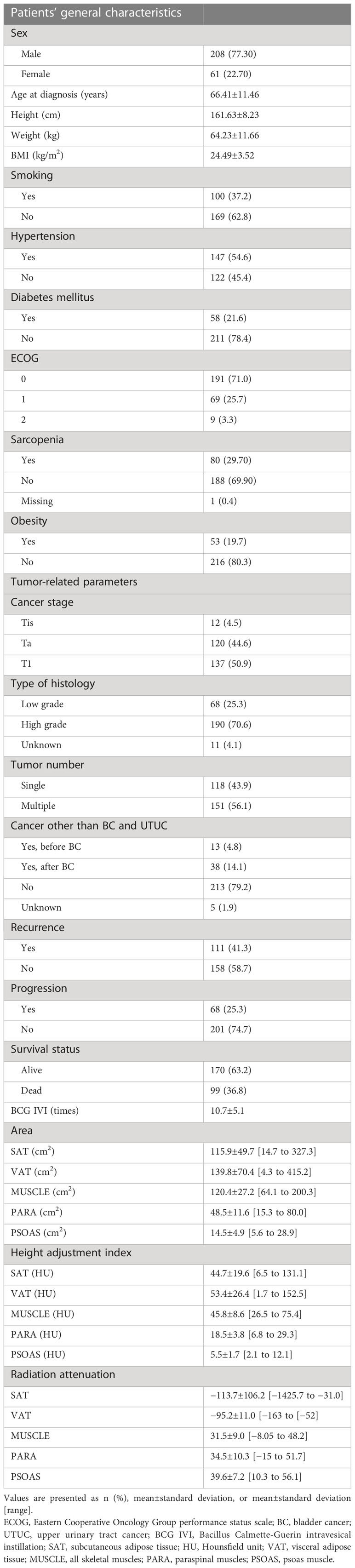
Table 1 Patients’ general characteristics and body composition indices (n = 269).
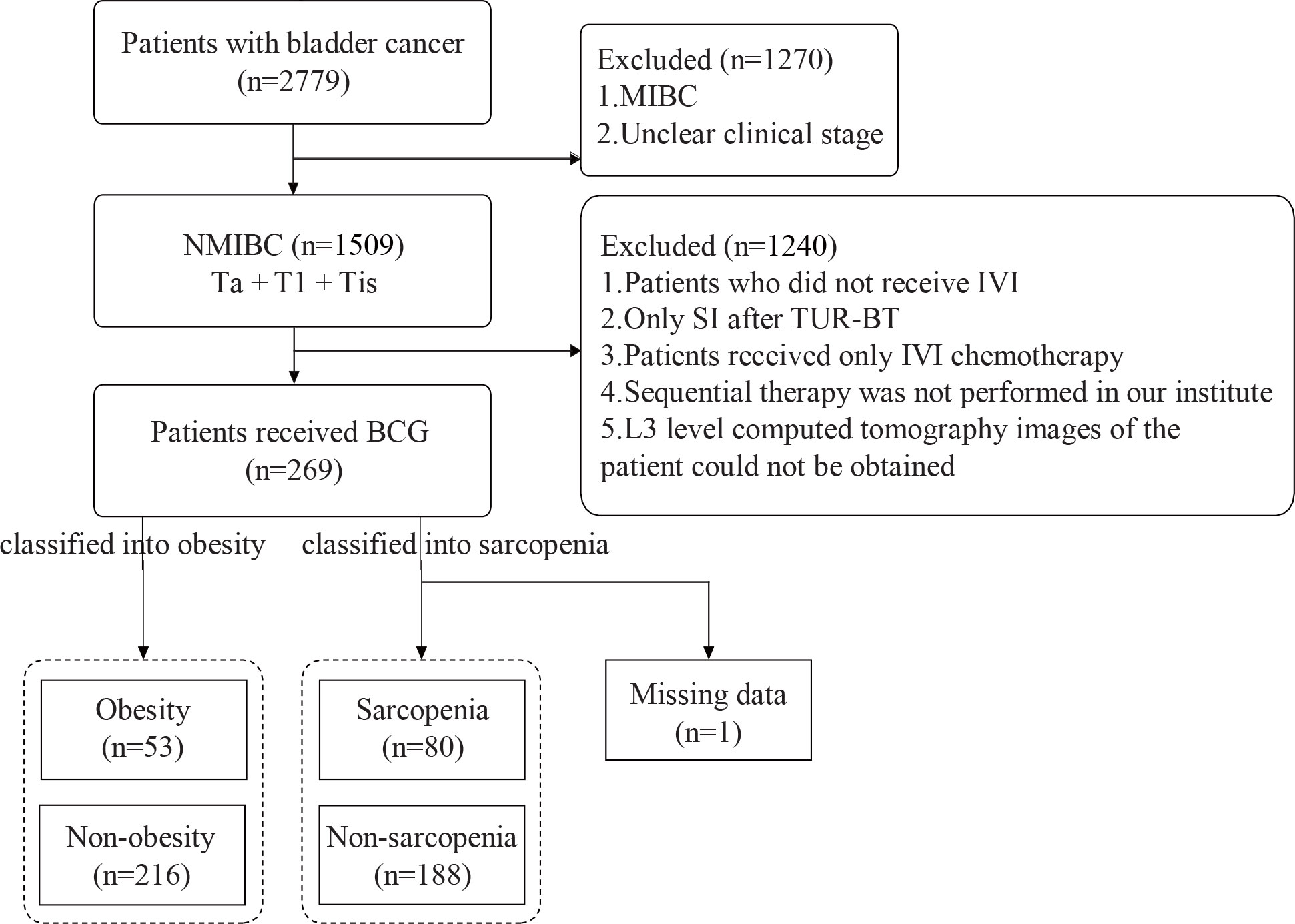
Figure 1 Flowchart of patient selection. MIBC, muscle-invasive bladder cancer; NMIBC, non-muscle-invasive bladder cancer; Tis, carcinoma in situ; Ta, tumors confined to the mucosa; Tl, tumors invading the lamina propria; IVI, intravesical instillation; TURBT, transurethral resection of bladder tumor; CT, computed tomography.
Based on the CT images for staging, the body composition areas of the five parameters of the SAT, VAT, MUSCLE, PARA, and PSOAS were 115.9, 139.8, 120.4, 48.9, and 14.5 cm2, respectively. The height adjustment areas for the five parameters were 44.7, 53.4, 45.8, 18.5, and 5.5 cm2/m2. The radiation attenuation values of each part were −113.7, −95.2, 31.5, 34.5, and 39.6 HU, respectively. Details of the remaining body composition analyses are presented in Table 1.
After analyzing univariate and multivariate Cox proportional hazards models, we found that age at diagnosis and BMI were correlated with OS (p < 0.001 and p = 0.018, respectively). The RFS and PFS differed significantly according to cancer stage (p < 0.001 and p = 0.001, respectively). In addition, we demonstrated a significant effect of the number of times patients received BCG IVI on the RFS, PFS, and OS of patients (p < 0.001, p < 0.001, and p = 0.025, respectively).
As for the impact of body composition parameters on the RFS, PFS, and OS, we found that radiation attenuation by SAT had a statistically significant impact on the RFS (hazards ratio [HR] = 0.998, 95% confidence interval [CI] = 0.99–1.00, p = 0.011), whereas radiation attenuation by PSOAS had no effect on the RFS (HR = 0.978, 95% CI = 0.96–1.00, p = 0.053) and a significant impact on the OS (HR = 0.948, 95% CI = 0.90–1.00, p = 0.044). Radiation attenuation by MUSCLE and PARA also had notable effects on the OS. In contrast, the height adjustment areas of SAT, MUSCLE, and PSOAS had a significant impact on the OS (p = 0.03, p = 0.03, and p = 0.04, respectively). However, we were unable to identify a single parameter as a prognostic factor for patients with NMIBC in this study. Age, cancer stage, the number of times BCG IVI was received, radiation attenuation, and height adjustment area had an effect on the RFS, PFS, and OS. The rest of the Cox proportional hazards model results are presented in Table 2.
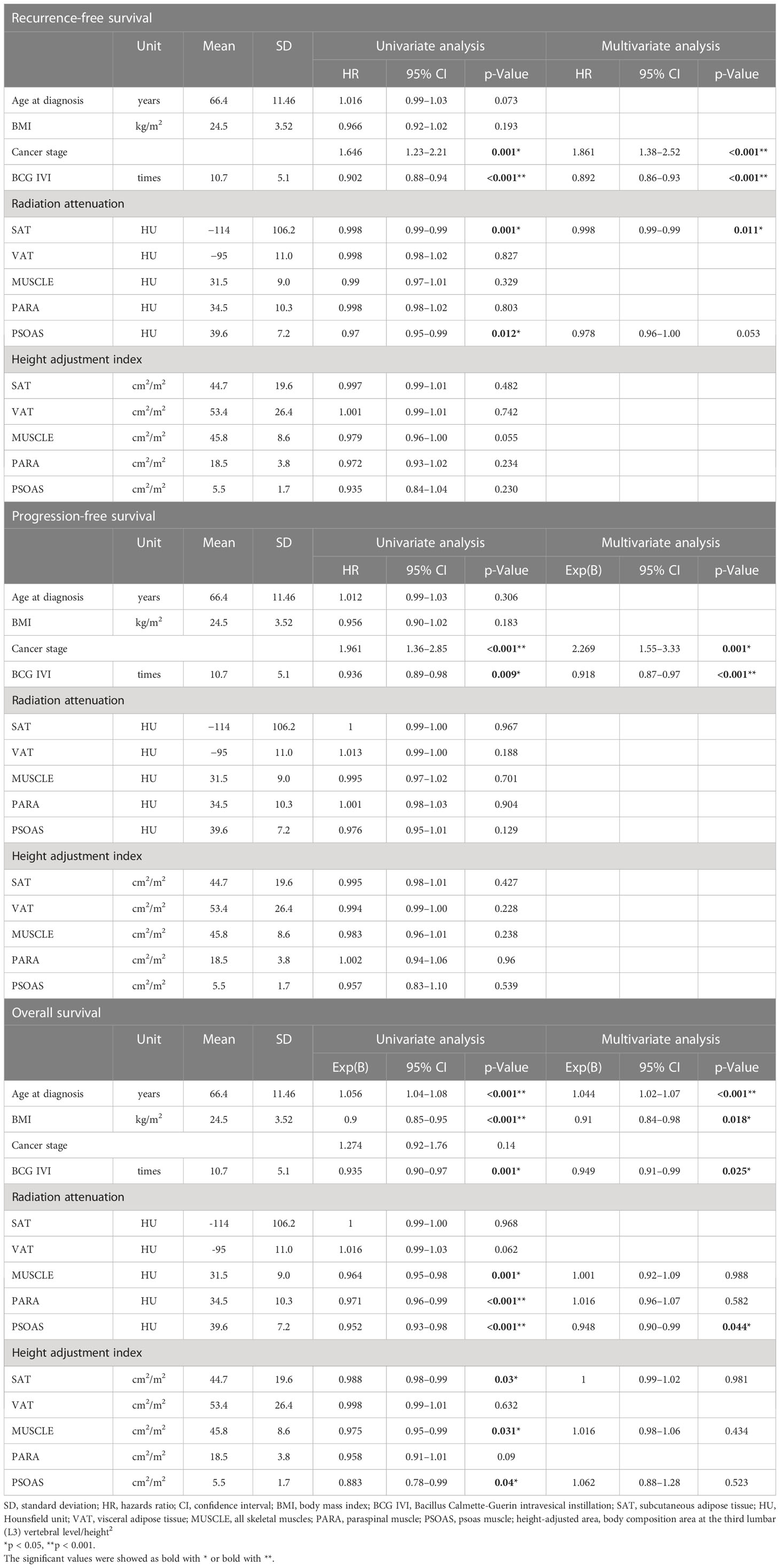
Table 2 Summary of the univariate and multivariate Cox regression analyses.
In Pearson’s correlation analysis test, we found statistically significant correlations among sarcopenia or obesity, age at diagnosis, and the number of BCG IVIs. Patients with sarcopenia were diagnosed at an older age (r = 0.263, p < 0.001), whereas patients with obesity were diagnosed at a younger age (r = −0.155, p = 0.011; Table 3). In addition, patients with sarcopenia were found to receive fewer BCG IVIs (r = −0.178, p = 0.003) than patients without sarcopenia, whereas patients with obesity received more BCG IVIs than those without obesity (r = 0.126, p = 0.039; Table 3).
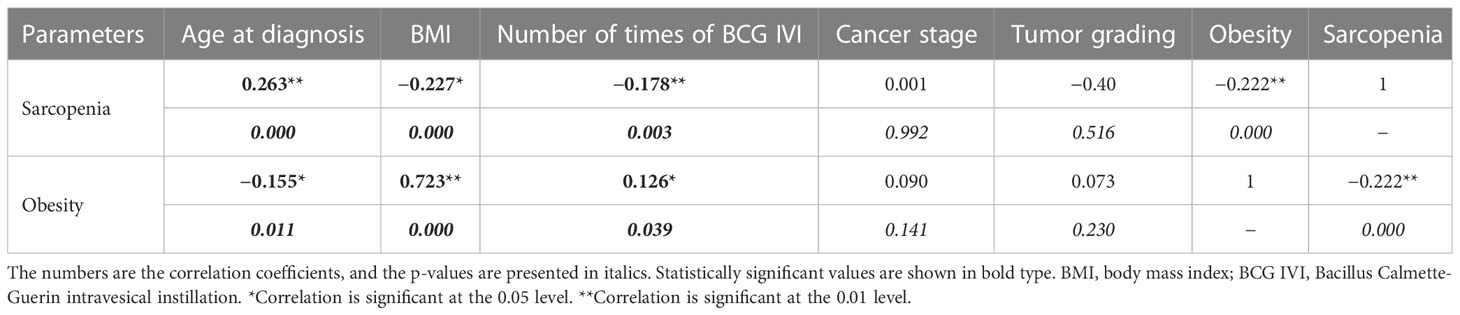
Table 3 Correlation matrix between sarcopenia/obesity and significant factors.
In all, 147 patients discontinued BCG IVIs during treatment: 52 patients discontinued owing to adverse events, three discontinued owing to BCG shortage, and the status was not documented in 92 patients. As per chi-square analysis, patients with sarcopenia had a higher risk of discontinuation of BCG IVIs owing to adverse events (p = 0.012).
Finally, using the Kaplan–Meier survival test, we found that patients with sarcopenia had poorer RFS and OS (p = 0.030 and p = 0.033, respectively). In contrast, patients with obesity had better OS (p = 0.008). However, with regards to PFS, there was no significant difference between patients with sarcopenia and obesity (p = 0.390 and p = 0.638, respectively; Figure 2).
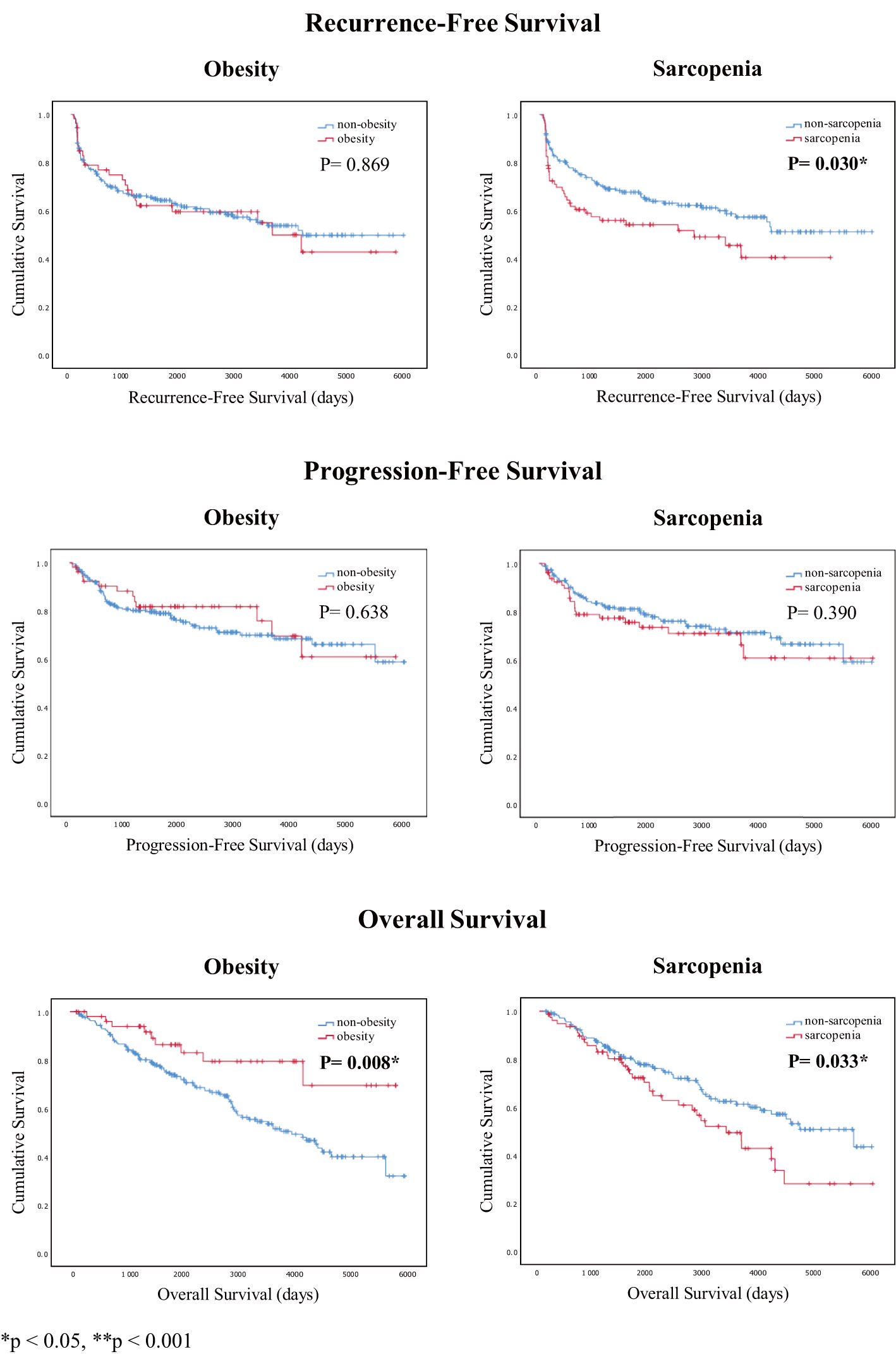
Figure 2 Kaplan–Meier survival curves of recurrence-free, progression-free, and overall survival analyses for patients with obesity and sarcopenia.
4 Discussion
This is the first study to demonstrate the impact of body composition on the oncological prognosis of patients with NMIBC treated with TURBT and BCG instillation. Body composition parameters, such as SAT density and psoas muscle density, were significant predictors of RFS and OS, respectively. Sarcopenia and obesity are simple indicators of lean and adipose tissue mass. Therefore, we classified sarcopenia according to the skeletal muscle index, using CT measurements (16) and also considered the results of Derstine et al. (13) and adipose tissue and muscle into account; patients with both indices below the cutoff values were included in the sarcopenia group. Approximately 30% of the patients were diagnosed with sarcopenia. The incidence was similar to that previously reported in patients with advanced BC (17).
Psutka et al. were the first to report that patients with sarcopenia and BC undergoing RC had poorer cancer-specific survival and OS than those without sarcopenia (18). In addition, Ornaghi et al. showed that patients with sarcopenia and BC had worse 5-year cancer-specific survival and OS than those without sarcopenia (19). Moreover, Mayr et al. showed an independent correlation between sarcopenia and increasing cancer-specific mortality (CSM) and all-cause mortality among patients receiving RC (20). Meanwhile, Hu et al. showed sarcopenia to be correlated with diminished cancer-specific survival and OS in patients with urothelial cancer (21). Lyon et al. also found that lower skeletal muscle mass after treatment with neoadjuvant chemotherapy, but before RC, had a markedly negative impact on CSM after surgery (22).
The exact underlying cause for fewer BCG IVIs received by patients with sarcopenia remains unknown. Loosen et al. demonstrated that sarcopenia negatively influences immune checkpoint therapy for cancer treatment. They linked sarcopenia to the activation of the immune system and systemic inflammation. This association resulted in impaired anti-cancer effects of immunotherapy (23).
However, as mentioned previously, BCG IVI is the recommended standard treatment for the prevention of recurrence and progression after TURBT in high-risk patients with NMIBC (1). Nonetheless, most patients with NMIBC treated with BCG IVI experience BCG toxicity, such as flu-like symptoms and cystitis, and some patients develop systemic tuberculosis infections (24, 25). In a previous study, nearly 2.9% of the patients with NMIBC discontinued immunotherapy owing to systemic or urinary BCG-related infection or intolerability (26). Meanwhile, different BCG strains such as TICE and RIVM may also impact the oncological outcomes of patients with BC (27). However, whether a different strain would result in a different type of toxicity remains unknown.
In our study, we noted that patients with sarcopenia were older and required fewer BCG IVIs than those who were not. Older patients usually have sarcopenia; moreover, their muscle mass decreases owing to poor nutrition, hormonal status, and lack of sports activities. Patients with sarcopenia usually have poor general health, and skeletal muscle deficiency may be correlated with the activation of the immune response (28). Thus, we hypothesized that patients with sarcopenia might have poorer tolerance to BCG IVI. As a result, treatment with few BCG IVIs in patients with sarcopenia will be less beneficial to them, further negatively influencing the OS and RFS.
Nevertheless, correlations between BMI and the risk of developing NMIBC or MIBC remain controversial. A 10% increase in the risk of BC development in patients with a high BMI was reported in three meta-analyses (9, 29, 30). In a discussion of prognosis among patients with NMIBC, recent meta-analyses showed that compared with patients who were not overweight or obese, patients who were overweight or obese had a markedly increased risk of cancer recurrence (31, 32). In another study, Kluth et al. found a negative correlation between recurrence and progression while comparing patients with and without obesity with high-grade T1 BC (33). High BMI was associated with a high risk of BC recurrence in a previous article (34). In addition to BMI and obesity, diet factors were also possibly related to the occurrence of BC. Multiple studies have illustrated the relationship between diet and risk of BC, including the cooking method, amount of meat intake, type of meat consumed, and temperature applied (35). Although many studies have mentioned that obesity is a negative risk factor for BC, these conclusions remain controversial.
Our study showed contradictory results to the studies above. Patients with obesity had better OS outcomes than those without obesity. This was echoed in the research conducted by Brooks et al. (36). They showed that elevated BMI was correlated with superior outcomes in patients with NMIBC who were treated with intravesical BCG immunotherapy. Arthuso et al. found that patients with advanced BC who were overweight or obese had a better prognosis within the first 5 years after RC (37). Obesity may be correlated with poorer outcomes in patients with NMIBC treated without BCG but is related to improved prognosis for those treated with intravesical immunotherapy (38, 39).
This can be explained by a few well-known mechanisms, namely increased activation of mitogenic pathways and increased levels of circulating inflammatory cytokines related to obesity (40). These factors may change the tumor microenvironment or systemic priming of BC, although BCG acts locally. This, in turn, may improve the oncological outcomes of BC (36). However, BCG IVI remains the gold standard treatment in terms of prevention of recurrence and progression in patients with NMIBC (1). The fact that patients with obesity received more BCG IVIs than those without obesity may have improved the OS of the patients with BC.
To our knowledge, previous studies aimed to determine the correlations among sarcopenia, cachexia, and nutritional status in patients with MIBC, regardless of whether the patients were receiving RC, neoadjuvant chemotherapy, or adjuvant chemotherapy. However, in our study, we aimed to determine the differences in the effect of sarcopenia and obesity on patients with BC. As shown in our results, patients with obesity had better OS than those without obesity, and patients with sarcopenia had worse OS and RFS than those without sarcopenia.
Our study had some limitations. First, we retrospectively collected data from approximately 300 patients. Second, the side effects and toxicity of BCG IVI were not analyzed in our study. More comprehensive data might help clarify the definite reasons for the discontinuation of BCG IVI. Third, we only calculated the results from some of the prognostic factors, such as the number of BCG IVIs, radiation attenuation, and height adjustment index. Nutritional and immune statuses, such as albumin level or neutrophil-to-lymphocyte ratio, were not assessed. Fourth, we showed significant differences in OS and RFS of patients with sarcopenia and OS of patients with obesity. We anticipate expanding our case numbers to determine if there is a correlation between body composition and PFS, which may better represent the independent role of sarcopenia in BC treatment. Fifth, all patients were recruited from a single center. Multicenter data collection is required for a thorough statistical analysis, and further prospective and larger series are needed to confirm our current findings. Sixth, OS was not an optimal oncological outcome for patients with NMIBC because NMIBC would progress to disseminated disease, thus impacting OS. However, OS was influenced by patient’s general condition, which may be correlated with sarcopenia or obesity. Thus, OS was still assessed as an endpoint in this study. Finally, there is currently no consensus regarding the definition of sarcopenia. Therefore, definitions differed across studies, and this may have led to a difference in the results between papers.
To our knowledge, this study is the first to demonstrate the impact of body composition on the oncological prognosis of NMIBC treated with TURBT and BCG instillation. Certain body composition parameters were found to be significant predictors of RFS and OS. Patients without sarcopenia and obesity can significantly tolerate more BCG IVIs, and this may result in favorable oncological outcomes. Among patients with NMIBC, the obese group had better OS than the non-obese group. Patients with sarcopenia had worse OS and RFS than those without sarcopenia. Further prospective research is required to validate the correlation between body composition and oncological outcomes in patients with NMIBC.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
All medical charts and computed tomography (CT) images of patients were reviewed and collected from a single tertiary medical center. Patients with incomplete data or images were excluded. This study was approved by the Institutional Review Board of the Chang Gung Medical Foundation. (IRB Number: 202100259B0), and followed the ethical principles outlined in the Declaration of Helsinki. The requirement for informed consent was waived owing to the retrospective study design.
Author contributions
Conceptualization: L-KH and I-HS. Methodology: Y-CL. Software: W-KH. Validation: L-KH. Formal analysis: L-KH and I-HS. Investigation: L-KH. Resources: C-KC, S-TP, C-TW, Y-HC, K-JY, P-HL, I-HS, H-CK, Y-CC, L-KH and M-LH. Data curation: L-KH and I-HS: writing—original draft preparation: L-KH and W-KH. Writing—review and editing: H-HC and I-HS. Visualization: Y-CL. Supervision: C-TW and I-HS. Project administration: L-KH. All authors have read and agreed to the published version of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AI, artificial intelligence; BC, bladder cancer; BCG, Bacillus Calmette-Guerin; BMI, body mass index; CSM, cancer-specific mortality; CT, computed tomography; HR, hazards ratio; HU, Hounsfield unit; IVI, intravesical instillation; IVI, intravesical instillation; MIBC, muscle-invasive bladder cancer; MUSCLE, all skeletal muscles; NMIBC, non-muscle-invasive bladder cancer; OS, overall survival; PARA, paraspinal muscle; PFS, progression-free survival; PSOAS, and psoas muscle; RC, radical cystectomy; RFS, recurrence-free survival; SAT, subcutaneous adipose tissue; TURBT, transurethral resection of bladder tumor; VAT, visceral adipose tissue.
References
1. Sanchez A, Kissel S, Coletta A, Scott J, Furberg H. Impact of body size and body composition on bladder cancer outcomes: risk stratification and opportunity for novel interventions. Urol Oncol (2020) 38:713–8. doi: 10.1016/j.urolonc.2020.03.017
2. Cambier S, Sylvester RJ, Collette L, Gontero P, Brausi MA, van Andel G, et al. EORTC nomograms and risk groups for predicting recurrence, progression, and disease-specific and overall survival in non-muscle-invasive stage Ta-T1 urothelial bladder cancer patients treated with 1–3 years of maintenance Bacillus Calmette-Guerin. Eur Urol (2016) 69:60–9. doi: 10.1016/j.eururo.2015.06.045
3. Sylvester RJ, van der Meijden AP, Oosterlinck W, Witjes JA, Bouffioux C, Denis L, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol (2006) 49:466–5; discussion 475. doi: 10.1016/j.eururo.2005.12.031
4. Choi JB, Lee EJ, Han KD, Hong SH, Ha US. Estimating the impact of body mass index on bladder cancer risk: stratification by smoking status. Sci Rep (2018) 8:947. doi: 10.1038/s41598-018-19531-7
5. Bandera EV, Qin B, Lin Y, Zeinomar N, Xu B, Chanumolu D, et al. Association of body mass index, central obesity, and body composition with mortality among black breast cancer survivors. JAMA Oncol (2021) 7:1–10. doi: 10.1001/jamaoncol.2021.1499
6. Guo Z, Gu C, Gan S, Li Y, Xiang S, Gong L, et al. Sarcopenia as a predictor of postoperative outcomes after urologic oncology surgery: a systematic review and meta-analysis. Urol Oncol (2020) 38:560–73. doi: 10.1016/j.urolonc.2020.02.014
7. Chappidi MR, Kates M, Patel HD, Tosoian JJ, Kaye DR, Sopko NA, et al. Frailty as a marker of adverse outcomes in patients with bladder cancer undergoing radical cystectomy. Urol Oncol (2016) 34:256.e1–6. doi: 10.1016/j.urolonc.2015.12.010
8. Stangl-Kremser, Mari A, D’Andrea D, Kimura S, Resch I, Shariat SF, et al. Sarcopenia as a predictive factor for response to upfront cisplatin-based chemotherapy in patients with muscle-invasive urothelial bladder cancer. Urol Int (2018) 101:197–200. doi: 10.1159/000489013
9. Sun JW, Zhao LG, Yang Y, Ma X, Wang YY, Xiang YB. Obesity and risk of bladder cancer: a dose–response meta-analysis of 15 cohort studies. PloS One (2015) 10:e0119313. doi: 10.1371/journal.pone.0119313
10. Avgerinos KI, Spyrou N, Mantzoros CS, Dalamaga M. Obesity and cancer risk: emerging biological mechanisms and perspectives. Metabolism (2019) 92:121–35. doi: 10.1016/j.metabol.2018.11.001
11. Murphy WJ, Longo DL. The surprisingly positive association between obesity and cancer immunotherapy efficacy. JAMA (2019) 321:1247–8. doi: 10.1001/jama.2019.0463
12. Lennon H, Sperrin M, Badrick E, Renehan AG. The obesity paradox in cancer: a review. Curr Oncol Rep (2016) 18:56. doi: 10.1007/s11912-016-0539-4
13. Derstine BA, Holcombe SA, Ross BE, Wang NC, Su GL, Wang SC. Skeletal muscle cutoff values for sarcopenia diagnosis using T10 to L5 measurements in a healthy US population. Sci Rep (2018) 8:11369. doi: 10.1038/s41598-018-29825-5
14. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing (2010) 39:412–23. doi: 10.1093/ageing/afq034
15. Chu NF. Prevalence of obesity in Taiwan. Obes Rev (2005) 6:271–4. doi: 10.1111/j.1467-789X.2005.00175.x
16. Hirasawa Y, Nakashima J, Yunaiyama D, Sugihara T, Gondo T, Nakagami Y, et al. Sarcopenia as a novel preoperative prognostic predictor for survival in patients with bladder cancer undergoing radical cystectomy. Ann Surg Oncol (2016) 23(Suppl 5):1048–54. doi: 10.1245/s10434-016-5606-4
17. Stangl-Kremser J, Ahmadi H, Derstine B, Wang SC, Englesbe MJ, Daignault-Newton S, et al. Psoas muscle mass can predict postsurgical outcomes in patients who undergo radical cystectomy and urinary diversion reconstruction. Urology (2021) 158:142–9. doi: 10.1016/j.urology.2021.08.013
18. Psutka SP, Carrasco A, Schmit GD, Moynagh MR, Boorjian SA, Frank I, et al. Sarcopenia in patients with bladder cancer undergoing radical cystectomy: impact on cancer-specific and all-cause mortality. Cancer (2014) 120:2910–8. doi: 10.1002/cncr.28798
19. Ornaghi PI, Afferi L, Antonelli A, Cerruto MA, Odorizzi K, Gozzo A, et al. The impact of preoperative nutritional status on post-surgical complication and mortality rates in patients undergoing radical cystectomy for bladder cancer: a systematic review of the literature. World J Urol (2021) 39:1045–81. doi: 10.1007/s00345-020-03291-z
20. Mayr R, Gierth M, Zeman F, Reiffen M, Seeger P, Wezel F, et al. Sarcopenia as a comorbidity-independent predictor of survival following radical cystectomy for bladder cancer. J Cachexia Sarcopenia Muscle (2018) 9:505–13. doi: 10.002/jcsm.12279
21. Hu X, Dou WC, Shao YX, Liu JB, Xiong SC, Yang WX, et al. The prognostic value of sarcopenia in patients with surgically treated urothelial carcinoma: a systematic review and meta-analysis. Eur J Surg Oncol (2019) 45:747–54. doi: 10.1016/j.ejso.2019.03.003
22. Lyon TD, Frank I, Takahashi N, Boorjian SA, Moynagh MR, Shah PH, et al. Sarcopenia and response to neoadjuvant chemotherapy for muscle-invasive bladder cancer. Clin Genitourin Cancer (2019) 17:216–222.e5. doi: 10.1016/j.clgc.2019.03.007
23. Loosen SH, van den Bosch V, Gorgulho J, Schulze-Hagen M, Kandler J, Jördens MS, et al. Progressive sarcopenia correlates with poor response and outcome to immune checkpoint inhibitor therapy. J Clin Med (2021) 10:1361. doi: 10.3390/jcm10071361
24. Larsen ES, Joensen UN, Poulsen AM, Goletti D, Johansen IS. Bacillus Calmette-Guerin immunotherapy for bladder cancer: a review of immunological aspects, clinical effects and BCG infections. APMIS (2020) 128:92–103. doi: 10.1111/apm.13011
25. Pérez-Jacoiste Asín MA, Fernández-Ruiz M, López-Medrano F, Lumbreras C, Tejido Á, San Juan R, et al. Bacillus Calmette-Guerin (BCG) infection following intravesical BCG administration as adjunctive therapy for bladder cancer: incidence, risk factors, and outcome in a single-institution series and review of the literature. Medicine (2014) 93:236–54. doi: 10.1097/MD.0000000000000119
26. Nummi A, Järvinen R, Sairanen J, Huotari K. A retrospective study on tolerability and complications of bacillus Calmette-Guérin (BCG) instillations for non-muscle-invasive bladder cancer. Scand J Urol (2019) 53:116–22. doi: 10.1080/21681805.2019.1609080
27. Del Giudice F, Flammia RS, Chung BI, Moschini M, Pradere B, Mari A, et al. Compared efficacy of adjuvant intravesical BCG-TICE vs. BCG-RIVM for high-risk non-muscle invasive bladder cancer (NMIBC): a propensity score matched analysis. Cancers (2022) 14:887. doi: 10.3390/cancers14040887
28. Afzali AM, Müntefering T, Wiendl H, Meuth SG, Ruck T. Skeletal muscle cells actively shape (auto)immune responses. Autoimmun Rev (2018) 17:518–29. doi: 10.1016/j.autrev.2017.12.005
29. Zhao L, Tian X, Duan X, Ye Y, Sun M, Huang J. Association of body mass index with bladder cancer risk: a dose–response meta-analysis of prospective cohort studies. Oncotarget (2017) 8:33990–4000. doi: 10.18632/oncotarget.16722
30. Qin Q, Xu X, Wang X, Zheng XY. Obesity and risk of bladder cancer: a meta-analysis of cohort studies. Asian Pac J Cancer Prev (2013) 14:3117–21. doi: 10.7314/apjcp.2013.14.5.3117
31. Westhoff E, Witjes JA, Fleshner NE, Lerner SP, Shariat SF, Steineck G, et al. Body mass index, diet-related factors, and bladder cancer prognosis: a systematic review and meta-analysis. Bladder Cancer (2018) 4:91–112. doi: 10.3233/BLC-170147
32. Ferro M, Vartolomei MD, Russo GI, Cantiello F, Farhan ARA, Terracciano D, et al. An increased body mass index is associated with a worse prognosis in patients administered BCG immunotherapy for T1 bladder cancer. World J Urol (2019) 37:507–14. doi: 10.1007/s00345-018-2397-1
33. Kluth LA, Xylinas E, Crivelli JJ, Passoni N, Comploj E, Pycha A, et al. Obesity is associated with worse outcomes in patients with T1 high grade urothelial carcinoma of the bladder. J Urol (2013) 190:480–6. doi: 10.1016/j.juro.2013.01.089
34. Wyszynski A, Tanyos SA, Rees JR, Marsit CJ, Kelsey KT, Schned AR, et al. Body mass and smoking are modifiable risk factors for recurrent bladder cancer. Cancer (2014) 120:408–14. doi: 10.1002/cncr.28394
35. Aveta A, Cacciapuoti C, Barone B, Di Zazzo E, Del Giudice F, Maggi M, et al. The impact of meat intake on bladder cancer incidence: is it really a relevant risk? Cancers (2022) 14:4775. doi: 10.3390/cancers14194775
36. Brooks NA, Kokorovic A, Xiao L, Matulay JT, Li R, Ranasinghe WKB, et al. The obesity paradox: defining the impact of body mass index and diabetes mellitus for patients with non-muscle-invasive bladder cancer treated with bacillus Calmette–Guérin. BJU Int (2021) 128:65–71. doi: 10.1111/bju.15296
37. Arthuso FZ, Fairey AS, Boulé NG, Courneya KS. Associations between body mass index and bladder cancer survival: is the obesity paradox short-lived? Can Urol Assoc J (2022) 16:E261–7. doi: 10.5489/cuaj.7546
38. Evers J, Grotenhuis AJ, Aben KKH, Kiemeney LALM, Vrieling A. No clear associations of adult BMI and diabetes mellitus with non-muscle invasive bladder cancer recurrence and progression. PloS One (2020) 15:e0229384. doi: 10.1371/journal.pone.0229384
39. Xu T, Zhu Z, Wang X, Xia L, Zhang X, Zhong S, et al. Impact of body mass on recurrence and progression in Chinese patients with Ta, T1 urothelial bladder cancer. Int Urol Nephrol (2015) 47:1135–41. doi: 10.1007/s11255-015-1013-1
Keywords: bladder cancer, non-muscle-invasive bladder cancer, sarcopenia, obesity, body composition, transurethral resection, intravesical instillation
Citation: Huang L-K, Lin Y-C, Chuang H-H, Chuang C-K, Pang S-T, Wu C-T, Chang Y-H, Yu K-J, Lin P-H, Kan H-C, Chu Y-C, Hung W-K, Hsieh M-L and Shao I-H (2023) Body composition as a predictor of oncological outcome in patients with non-muscle-invasive bladder cancer receiving intravesical instillation after transurethral resection of bladder tumor. Front. Oncol. 13:1180888. doi: 10.3389/fonc.2023.1180888
Received: 06 March 2023; Accepted: 07 July 2023;
Published: 10 August 2023.
Edited by:
Hong Weng, Wuhan University, ChinaReviewed by:
Savio Domenico Pandolfo, Federico II University Hospital, ItalyMurat Akand, University Hospitals Leuven, Belgium
Copyright © 2023 Huang, Lin, Chuang, Chuang, Pang, Wu, Chang, Yu, Lin, Kan, Chu, Hung, Hsieh and Shao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: I-Hung Shao, Yjg5MDIwNjhAY2dtaC5vcmcudHc=