
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 09 June 2023
Sec. Head and Neck Cancer
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1173578
 Francesco Trevisani1*
Francesco Trevisani1* Federico Di Marco1Giulia Quattrini1Nicola Lepori2
Federico Di Marco1Giulia Quattrini1Nicola Lepori2 Matteo Floris2Davide Valsecchi3Leone Giordano4Italo Dell’Oca5
Matteo Floris2Davide Valsecchi3Leone Giordano4Italo Dell’Oca5 Sara Cardellini6Alessandra Cinque7
Sara Cardellini6Alessandra Cinque7 Aurora Mirabile8
Aurora Mirabile8Background: In locally advanced head and neck squamous cell carcinoma (LA-SCCHN) at least 200mg/m2 (standard dose 300 mg/m2) of cisplatin concomitant with radiotherapy represents the standard of care, both in postoperative and conservative settings. Nevertheless, high dose administration every 3 weeks is often replaced with low dose weekly cisplatin to avoid toxicities like kidney injury, though often failing to reach the therapeutic dose. Our aim was to investigate the incidence of renal impairment in the real-life setting, integrating high dose cisplatin with adequate supportive therapy, and to explore both Acute Kidney Injury (AKI) and Acute Kidney Disease (AKD), a recently described clinical renal syndrome that encompasses functional alterations of the kidney lasting fewer than 3 months.
Methods: One hundred and nine consecutive patients affected by LA-SCCHN and treated with at least a cumulative dosage of 200 mg/m2 of cisplatin concomitant with radiotherapy were enrolled in this prospective observational study.
Results: AKI was reported in 12.8% of patients, 50% of whom were stage 1 (KDIGO criteria), while 25.7% of the cohort developed AKD. Patients with baseline estimated Glomerular Filtration Rate (eGFR) < 90 ml/min showed a higher incidence of AKD (36.2% vs 17.7%). Hypertension, baseline eGFR, and therapy with Renin-angiotensin-aldosterone system inhibitors proved to be significant factors associated with both AKI and AKD.
Conclusion: AKI and AKD are not rare complications of high-dose cisplatin, but an appropriate prevention strategy and accurate monitoring of patients during treatment could lead to a reduction of the burden of these conditions.
Head and neck cancer represents the sixth most common neoplasm worldwide, accounting for 800,000 new cases and 400,000 deaths globally every year (1). Among head and neck cancers, squamous cell carcinoma is the most prominent and aggressive histology, being responsible for more than 90% of cases (2). The overall 5-year survival rate for people with locally advanced head and neck squamous cell carcinoma (LA-SCCHN) ranges from 33% to 68% depending on risk factors and primary site (3).
Due to the anatomically complex structure of the head and neck district, which is responsible for nourishment, language and breathing, a multidisciplinary clinical approach is always mandatory in order to keep the functional aspects intact. Therefore, the combination of surgery, chemotherapy and radiation are of paramount importance to maximize the efficacy of the therapy and minimize the rate of side effects (4).
Cisplatin is especially interesting since it has shown anticancer activity in a variety of tumors, including head and neck. In the 1960s it was found to have cytotoxic properties, and by the end of the 1970s it had earned a place as the key component in the systemic treatment of germ cell cancers. Among the many chemotherapy drugs that are widely used for cancer treatment, Cisplatin is one of the most compelling, and in 1978 it was the first FDA-approved platinum compound for treating cancer (5).
In day-to-day clinical practice, a schedule including at least two cycles of thrice-weekly high-dose administrations of cisplatin (100 mg/m2) given concomitantly with radiotherapy represents the standard of care for LA-SCCHN with a curative intent, both in postoperative and conservative settings.
However, due to the awareness of platinum-based, compound-related, renal toxicity, thrice-weekly high-dose cisplatin is often replaced with a lower-dose weekly schedule to avoid toxicities like kidney dysfunction (6).
Nevertheless, often this approach fails to reach the therapeutic cumulative dose of 200mg/m2, and since there is a paucity of prospective randomized studies, and the optimal dosing of weekly cisplatin is still a contentious issue, low dose weekly cisplatin should be prospectively studied in a phase III trial (7).
Moreover, several articles in the literature underline that the nephrotoxic effect of platin is cumulative and dose-dependent (8) (9). In fact, cisplatin accumulation in the kidneys increases the amount of tumor necrosis factor alpha and reactive oxygen species, resulting in inflammation, oxidative stress, vascular injury, and renal vasoconstriction (10). From a clinical point of view, all these biological processes promote the development of acute tubular necrosis and apoptotic cascade in the proximal tubules, inexorably leading to the onset of acute kidney injury (AKI). In addition, recurrent AKI events make a non-negligible percentage of patients susceptible to developing chronic renal impairment over time, thus resulting in chronic kidney disease (CKD) (11, 12).
However, despite all these nephrological considerations, from an oncological perspective, there is no level 1 evidence of comparable efficacy to cisplatin once every 3 weeks (13). Recently, a new clinical entity named Acute Kidney Disease (AKD), was proposed in order to consider all functional and structural kidney alterations lasting less than three months (14). The evaluation of AKD is of particular interest in LA-SCCHN patients to be able to explore the whole acute spectrum of renal damage after cumulative cisplatin exposure. Aim of this study was to investigate real-life acute nephrotoxicity in LA-SCCHN patients during and after treatment with high-dose cisplatin-based chemoradiotherapy (CRT), with particular focus on AKI and AKD onset.
A total of 109 patients were included in this study. The mean age was 60 years (SD: 10) and 70.6% of patients were male. Mean estimated glomerular filtration rate (eGFR) at baseline was 90.8 ml/min/1.73m2: 57% of patients presented baseline eGFR ≥ 90 mL/min, while 43% showed < 90 mL/min (only 5 patients had eGFR < 60 mL/min). Median body mass index (BMI) was 24.8. Diabetic patients made up 9.2% of the total, while 36.7% had arterial hypertension. When patients with baseline eGFR ≥ 90 ml/min were compared to patients with eGFR < 90 ml/min, a statistically significant difference was found in both BMI (23.6 vs 25.3, p 0.003) and prevalence of arterial hypertension (22.6% vs 55.3%, p < 0.001) (Table 1).
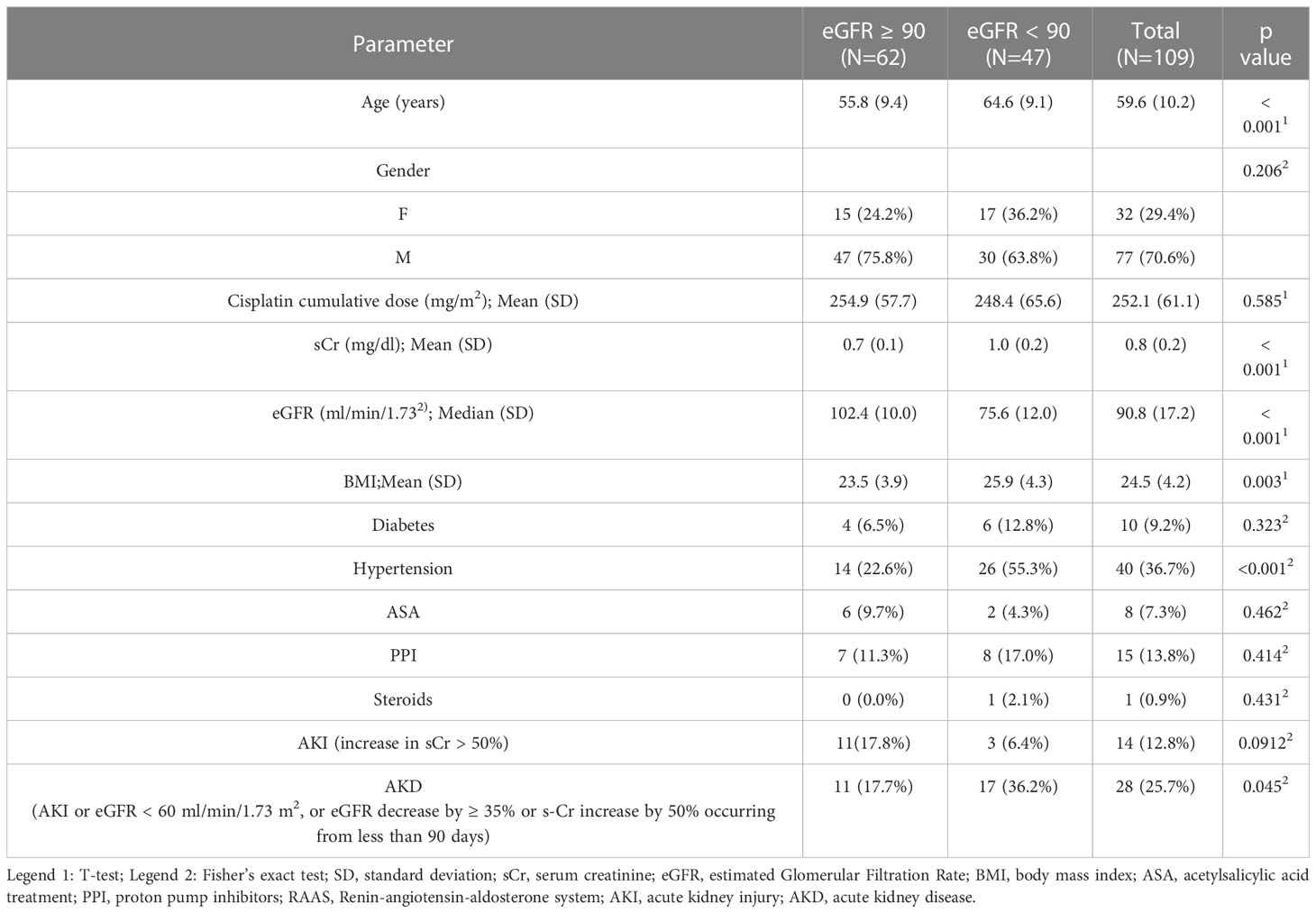
Table 1 Descriptive statistics.
Forty patients (38.8%) were on anti-hypertensive medication: no differences were found between patients with baseline eGFR ≥ 90 ml/min and those with eGFR < 90 ml/min (Table 2).
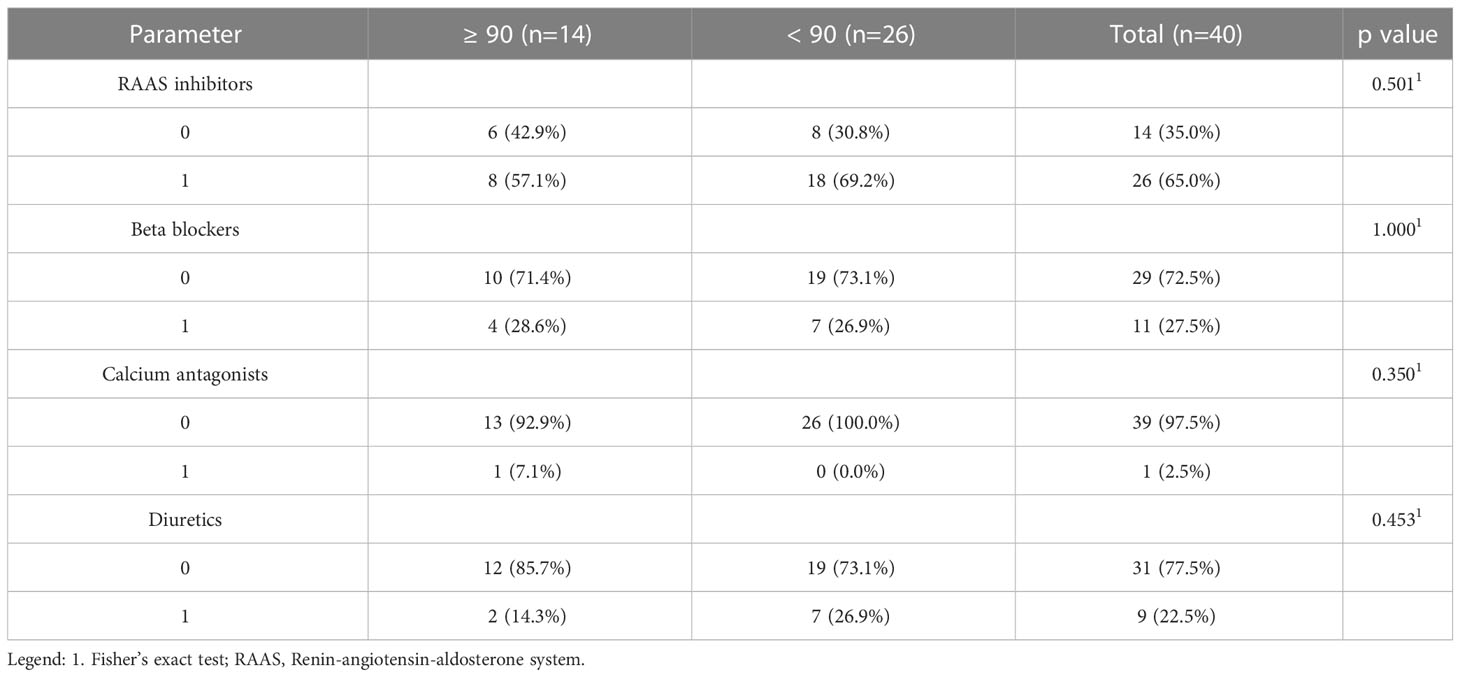
Table 2 Anti-hypertensive drug use by the study cohort.
Acute Kidney Injury was reported in 14 patients (12.8%): the majority of AKI episodes (50%) were stage 1 according to KDIGO criteria, 43% were AKI stage 2 and only 1 patient had AKI stage 3. Patients with baseline eGFR ≥ 90 ml/min/1.73m2 showed a higher incidence of AKI (17.8% vs 6.4%) when AKI was defined as an increase in serum creatinine (sCr) >50% of baseline, although the difference was not statistically significant (p=0.091). Median cumulative cisplatin dose was 300 mg/m2 (interquartile interval 200-300): 99 patients (90.8%) reached a cisplatin-cumulative dose >200 mg/m2.
Acute Kidney Disease occurred in 28 patients (25.7%). Patients with baseline eGFR ≥ 90 ml/min/1.73m2 showed a statistically significant lower incidence of AKD (17.7% vs 36.2%; p=0.045).
Median cumulative cisplatin dose was 300 mg/m2 (interquartile interval 200-300): 99 patients (90.8%) reached a cisplatin-cumulative dose >200 mg/m2. Five patients discontinued planned cisplatin-based chemotherapy due to sepsis (1 patient), AKI (1 patient), cytopenia (2 patients), hypoacusis (1 patient) and death due to other causes (1 patient).
In order to better define which aspect might be most involved in eGFR decline as a predictive risk factor during therapy, we decided to use a multivariable linear regression model for eGFR percentage decay, including comorbidities, baseline eGFR, cycle treatment and number of days from last cycle. The analysis showed the presence of hypertension (beta = 3%, CI=0.2%-6%, p=0.03), baseline eGFR (beta = 0.1%, CI = 0.05%-0.2%, p=0.001) and the number of chemotherapy cycles (beta = 3%, CI = 2%-4%, p < 0.001) to be predictive factors (Supplementary Data Table 1).
In order to evaluate which clinical and demographic factors were related to the risk of developing AKI during cisplatin treatment, a multivariable logistic analysis was performed. Results showed a significant correlation for baseline eGFR (OR = 1.03, CI=1;1.1, p=0.04), hypertension (OR=3.26, CI=1.4;7.6, p=0.005), number of chemotherapy cycles (OR=1.82, CI=1.2;2.9, p=0.007) and number of days after the last cycle (OR=1.15, CI=1.1;1.3, p < 0.001). The same analysis was performed in order to evaluate the factors linked to AKD development. Despite AKI results, an inverse correlation between baseline eGFR and AKD was found (OR = 0.95, CI=0.92;0.97, p=0.04). A significant correlation was also found with hypertension (OR=4.95, CI= 1.8;14, p=0.002), and the number of days after the last cycle (OR=1.09, CI=1;1.2, 0.02) (Table 3).
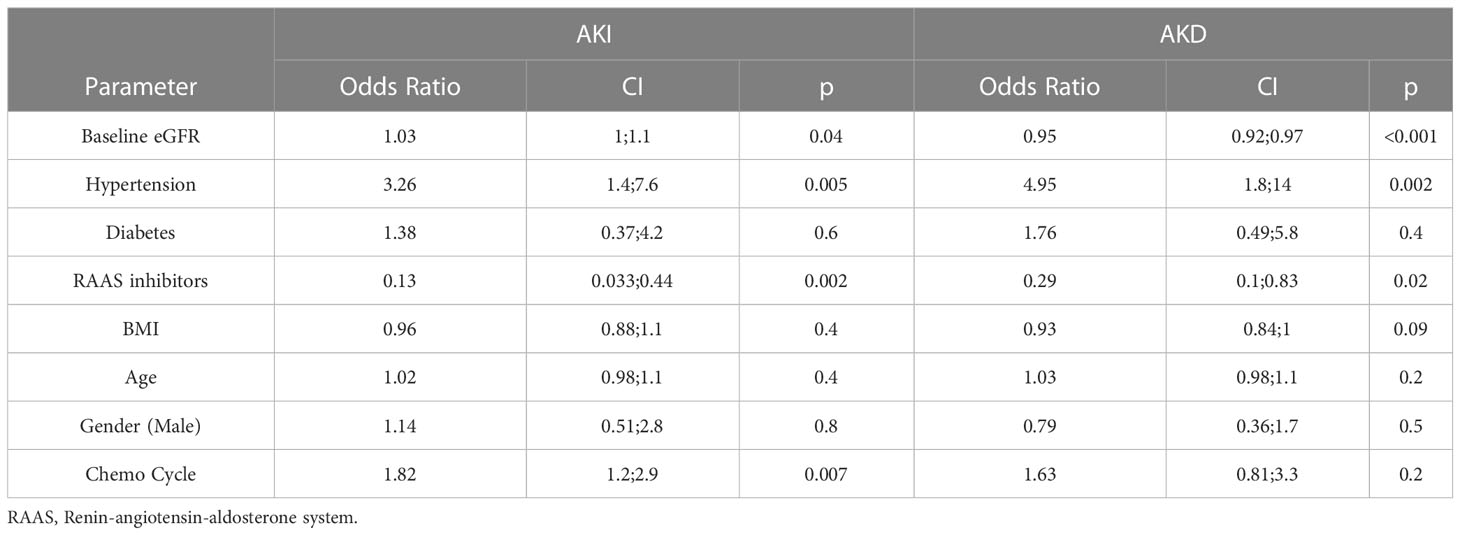
Table 3 Multivariable logistic regression model: AKI onset.
Cisplatin-based chemotherapy is widely used in the management of locally advanced squamous cell carcinoma of the head and neck to enhance the tumoricidal activity of irradiation, adding to radiotherapy alone a survival benefit estimated at 6.5% at 5 years. AKI is a common adverse effect associated with cisplatin CRT and represents a possible limitation to the delivery of the planned cisplatin dose. Moreover, AKI is a well-known risk factor for the development of CKD.
The present cohort study shows that 12.8% of 109 patients with head and neck cancer treated with high-dose cisplatin developed AKI according to the KDIGO definition and staging criteria. The majority of AKI episodes (50%) were stage 1, 43% were AKI stage 2 and only 1 patient had AKI stage 3. Interestingly, only 1 patient among those who experienced AKI (AKI stage 3) discontinued cisplatin-based treatment. Among the several potential risk factors studied (use of potentially nephrotoxic drugs, use of angiotensin converting enzyme inhibitors [ACEi], hypertension, diabetes, number of CT cycles, baseline eGFR), predictive risk factors for cisplatin-induced AKI included hypertension, and number of chemotherapy cycles. Previous studies in patients affected by LA-SCCHN showed broad variability in AKI incidence during cisplatin-based CRT, ranging from 4% to 69% (Table 4).
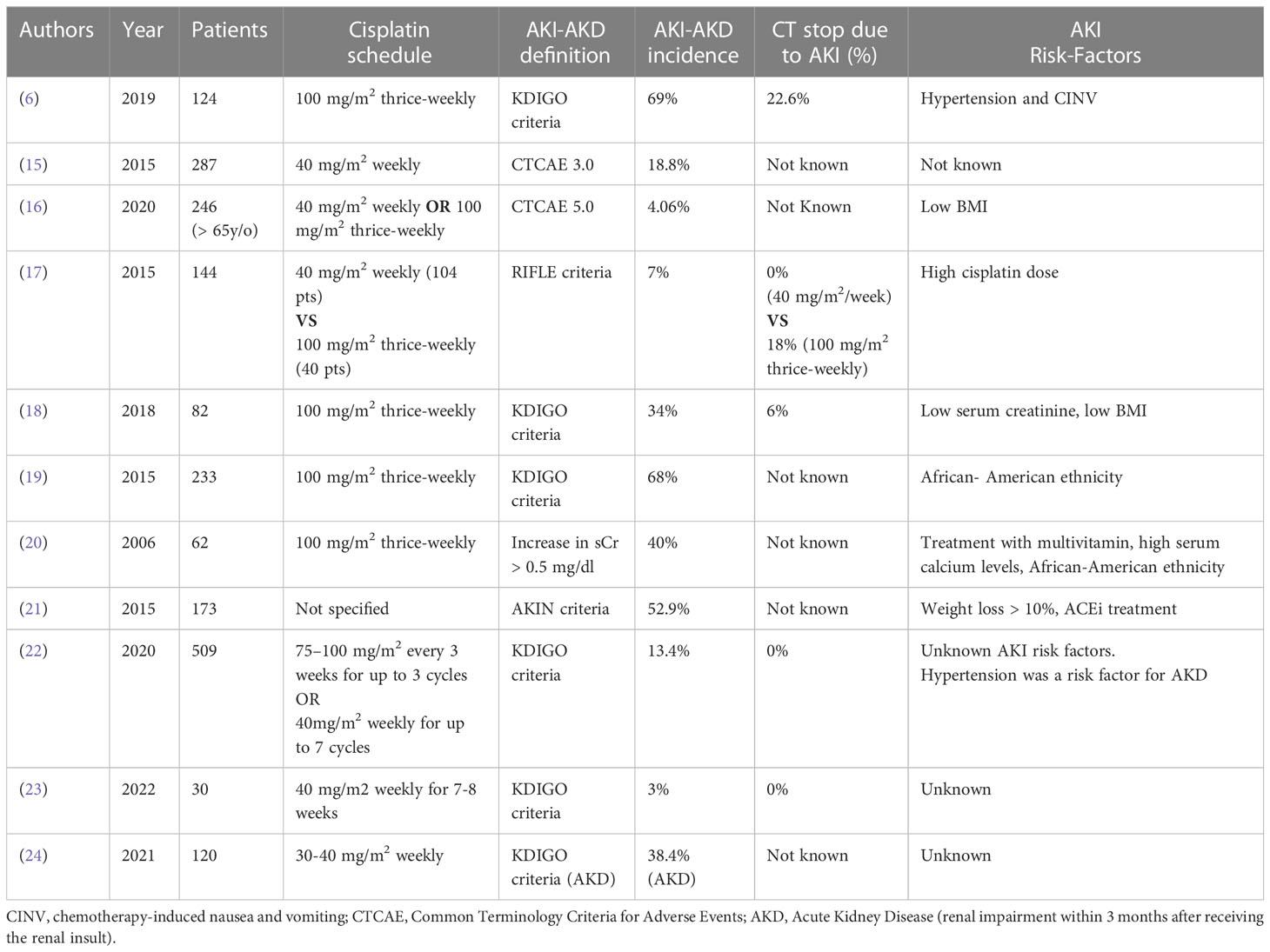
Table 4 Main studies on AKI and AKD incidence in head and neck cancer patients treated with cisplatin-based chemotherapy.
The explanations for this broad difference in AKI incidence reside mainly in the use of different definitions of AKI in different studies (Table 5). Studies which used different versions of the Common Terminology Criteria for Adverse Events system (CTCAE), i.e., CTCAE 3.0, CTCAE v5.0, showed the lowest incidence of AKI (15, 16). The 3.0 version of the CTCAE system defines AKI as an increase in sCr to a level higher than the upper limit of normal for the specific laboratory, while with regard to the CTCAE 4.0 version, an increase in sCr >0.3 mg/dl has been introduced as an AKI diagnostic criterion, following the KDIGO definition of AKI (6). However, in contrast to KDIGO criteria, there is no provision of a time course in CTCAE versions 4.0 and 5.0. Consequently, the higher AKI incidence observed in those studies which used KDIGO criteria or AKIN criteria (6) is likely due to a more frequent diagnosis of early stages of AKI. Interestingly, a correlation between cisplatin doses used in cisplatin-based CRT and incidence of AKI has been reported in several studies. Driessen and colleagues showed that 7% of patients who underwent intermediate-dose cisplatin-based CRT (40 mg/m2 weekly) developed AKI (all stage 1 according RIFLE criteria), while a much higher incidence of AKI (70%) was described in the high-dose group (100 mg/m2 thrice-weekly) (17). These results are coherent with a retrospective study published by Rades in 2011 which found a significant difference in grade 3 nephrotoxicity (using the CTCAE 2.0 version) between patients treated with cisplatin 100 mg/m2 on days 1, 22, and 43 and cisplatin 20 mg/m2 on days 1 to 5 and 29 to 33 of 8% versus 1% (29).
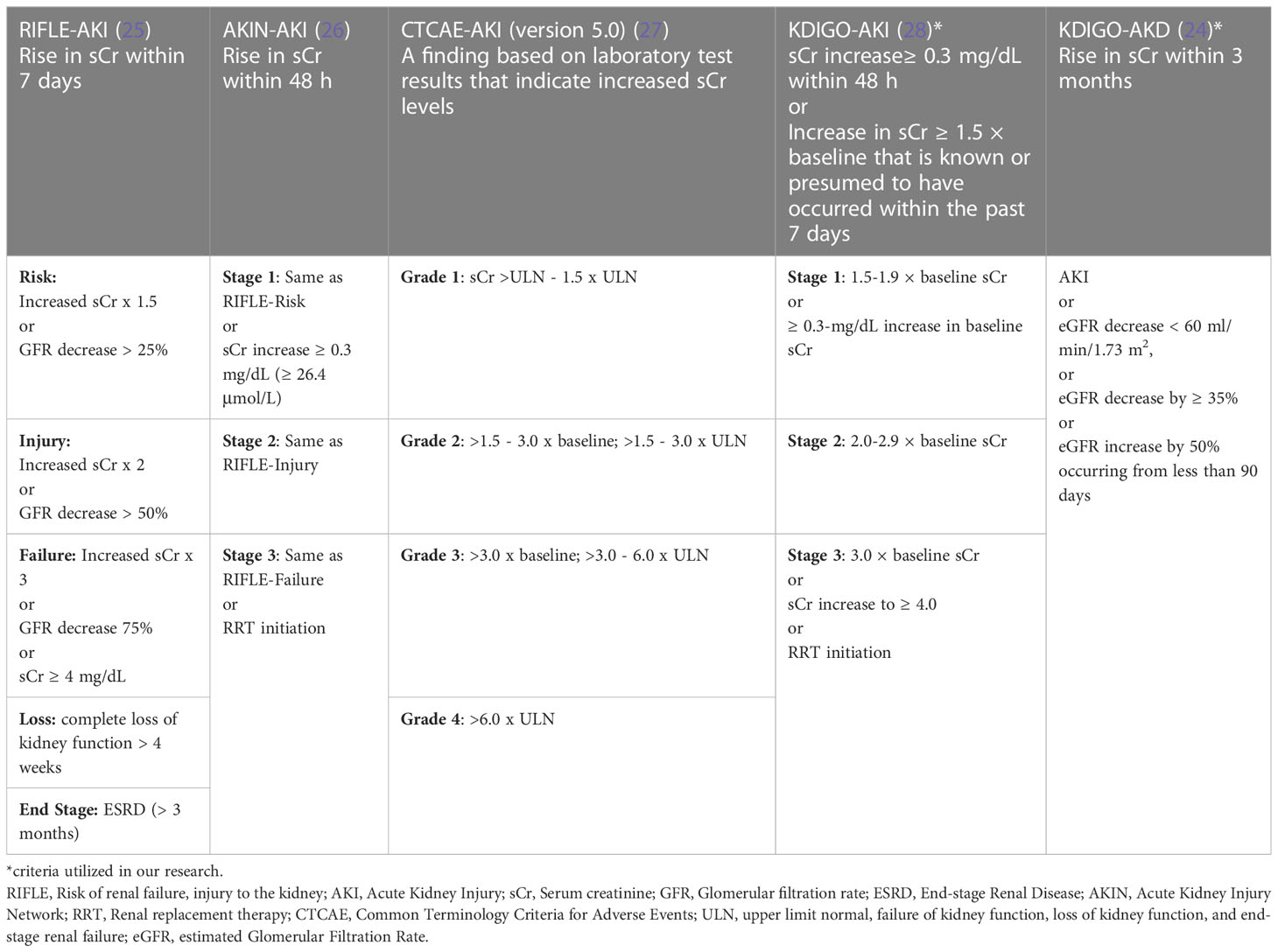
Table 5 Functional criteria utilized for acute kidney injury and acute kidney disease definition in head and neck cancer patients.
Although low-dose, once-a-week cisplatin could be considered a promising strategy to attempt to avoid AKI, often this approach fails to reach the therapeutic cumulative dose of 200 mg/m2 and, since there is a lack of prospective randomized studies, the optimal dosing of weekly cisplatin is still a contentious issue (7). Reported predictors of cisplatin-induced AKI included older age and hypertension, female sex, smoking, black ethnicity, hypokalemia, and hypoalbuminemia (30). Data from LA-SCCHN patients showed several risk factors for cisplatin-induced AKI: hypertension (6), low BMI (16, 18), low sCr (18), African-American ethnicity (19), treatment with ACEi (21). In our study, consistently with data present in the literature, hypertension was the most important factor associated with increased risk of cisplatin-induced AKI. Hypertension is a well-known risk factor for AKI in cisplatin-based chemotherapy, as described by several authors (31, 32). The most likely explanation for the correlation between hypertension and increased risk of cisplatin-nephrotoxicity is the presence of subclinical kidney damage due to hypertension, which could constitute a predisposing ground for cisplatin nephrotoxicity (31). In fact, hypertension can cause ischemic glomerulosclerosis, which further stimulates interstitial fibrosis and atrophy of tubular cells, the main target of cisplatin nephrotoxicity (33).
Acute Kidney Disease is a term that was introduced in 2017 to define all renal function alterations not fulfilling AKI and CKD criteria: the current definition includes AKI or eGFR < 60 ml/min/1.73 m2, or eGFR decrease by ≥ 35% or sCr increase by 50% occurring from less than 90 days (14). Few studies have evaluated the incidence of AKD in the setting of high-dose cisplatin chemotherapy in LA-SCCHN. In 2021, Patimarattananan et al. published a retrospective study analyzing data from 509 patients. Reported incidence of AKI and AKD were respectively 13.4 and 27.9%. On multivariate analysis, hypertension was found to be related to long term follow-up of these patients: patients who were diagnosed with AKD showed a more significant decline in eGFR at 3 months (-39.4% from baseline) without complete recovery of pre-CRT renal function at 12 months (-29.1% from baseline) (22). A higher incidence of AKD (38%) was demonstrated by an Indonesian group that analyzed data from a cohort of 120 patients with local advanced nasopharyngeal cancer treated with cisplatin-based CRT (24). Our data showed an incidence of AKD of 25.7% (similar to Patimarattanan et al, but lower than data provided by Rachman and colleagues), clearly demonstrating 2 risk factors for AKD: hypertension and baseline eGFR < 90 ml/min.
In this scenario, our study shows a lower incidence of AKI compared to previously published studies which used KDIGO or RIFLE criteria to define AKI, in which AKI incidence ranged from 34% to 69% (6, 19). The reasons for this finding are not completely clear. Although a role of the different composition of the studied populations cannot be excluded, it seems unlikely, since baseline features of our cohort do not differ significantly from those of cohorts described in other studies (Table 6). Moreover, mean age, prevalence of female sex and prevalence of diabetes are higher in our cohort than in the populations described in other studies.
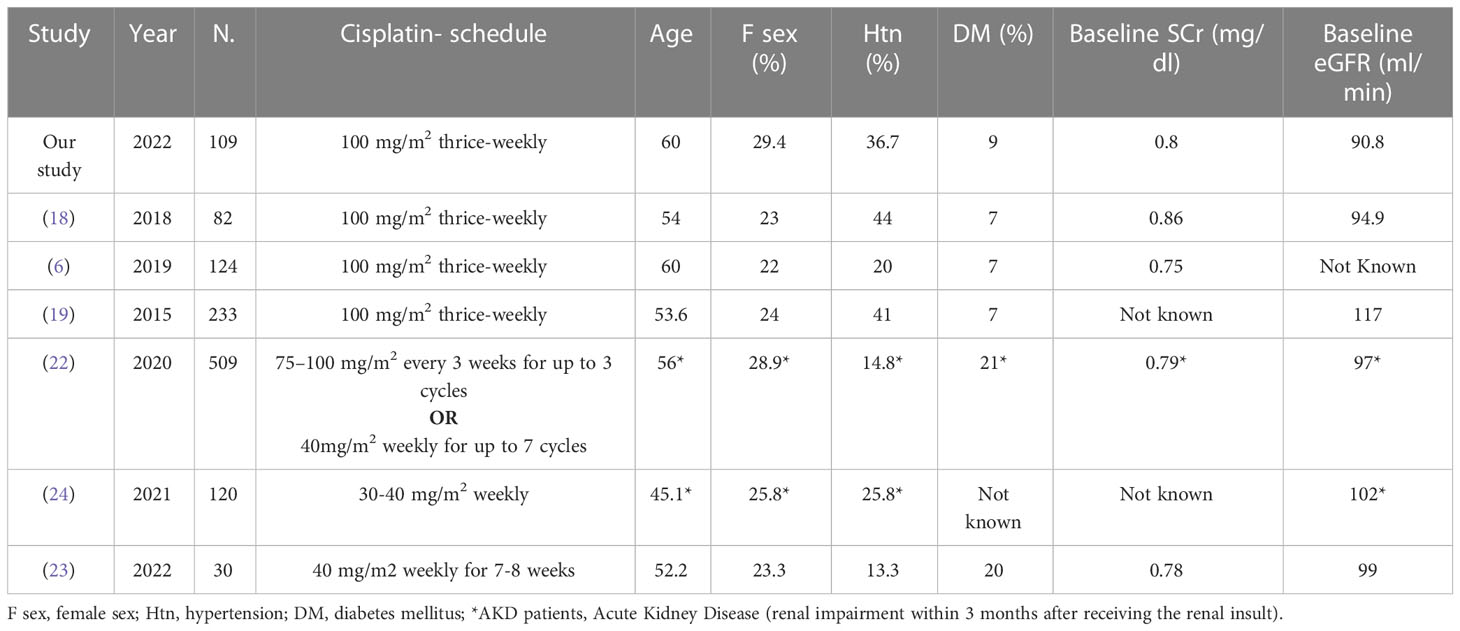
Table 6 Comparison among studies which used KDIGO criteria to define AKI or AKD in the setting of head and neck cancer patients treated with cisplatin-based CRT.
Therefore, a possible cause of the low incidence of AKI in our cohort could be the rigorous protocol used in our study to prevent cisplatin-induced nephrotoxicity. All patients received intravenous hydration with 0.9% saline 750 ml + 16mEq of magnesium sulfate before and after cisplatin administration (a total of 1500 ml at day 0 and again at day 1). Mannitol 10% (375 ml) was administered if diuresis after hydration was less than 100 ml/hour; meanwhile antiemetic prophylaxis (to prevent chemotherapy-induced nausea and vomiting which could lead to hypovolemia and an increased risk of AKI) with dexamethasone 12 mg IV as chemo premedication at day 0 and 8 mg PO at days 1 to 3 was administered. Evidence from previous studies is not strong enough to support the superiority of a specific hydration regimen for preventing nephrotoxicity associated with cisplatin administration.
Hypomagnesemia can upregulate OCT-2, leading to increased cisplatin transport to the kidneys, thus resulting in nephrotoxicity (34). Several systematic reviews suggest that magnesium supplementation may limit cisplatin-induced nephrotoxicity (35). A recent study by Kimura et al, analyzed the nephroprotective role of magnesium supplementation in patients receiving cisplatin for head and neck cancer: in multivariate analysis the use of magnesium-supplemented hydration was the only factor associated with a reduction in AKI-incidence (OR 0.157) (36). The use of mannitol to promote diuresis (and consequent cisplatin clearance) could raise concerns regarding over-diuresis and possible pre-renal AKI due to dehydration. Data from different studies are conflicting. A retrospective study conducted among head and neck tumor patients highlighted that patients who did not receive mannitol were more likely to develop nephrotoxicity (37), while Leu and colleagues showed a higher incidence of AKI in patients who did receive mannitol (38). In order to prevent potential over-diuresis, in our protocol mannitol was used only in patients who did not reach adequate diuresis after hydration.
A result of non-univocal interpretation regards the role of ACEi/angiotensin receptor blocker (ARB) treatment. Previous studies showed an increased risk of AKI in patients receiving ACEi therapy. Our study does not show this correlation: the risk of AKD appears lower in patients treated with ACEi/ARBs. The meaning of this result is not clear: a possible explanation could be that the hydration protocol and the active management of ACEi/ARBs (discontinuation of ACEi/ARBs in the most frail patients) may have reduced the incidence of AKD in this subset of patients. The lack of correlation between the increased risk of AKD and the use of ACEi/ARBs represents a relevant clinical finding, supporting the hypothesis that in our cohort, the main determinants of the development of AKD were renal function at the time of chemotherapy initiation, hypertension and the chemotherapy treatment itself.
An important result of our study is the extremely low incidence of stage 3 AKI and AKD (1 case). Similar data have been previously described by several authors. Van der Vorst reported stage 3 only in 5% of AKI cases, while in the study published by Faig in 2015, among 88 patients only 4 cases of stage 3 AKI were reported (6, 18). The low incidence of severe AKI in our cohort is confirmed by the evidence that only 1 patient out of 109 discontinued cisplatin-based chemotherapy because of nephrotoxicity.
The concept of AKD is relatively new in nephrology literature, and data on the incidence of AKD in cancer patients are still scarce (22, 24, 34). The evidence that this pathological entity is significantly correlated with renal prognosis in the mid to long term (progression to chronic kidney disease, end-stage renal disease and death), makes the possibility of using it to evaluate the impact of chemotherapy treatment on renal function very attractive. The higher incidence of AKD compared to AKI in our cohort (data also confirmed by previously published studies) could be an expression of repeated exposure to chemotherapy treatment leading to a progressive worsening of renal damage (not always of such a degree as to allow us to identify a picture of AKI). In our opinion, the use of the AKD concept is very promising as it allows the clinician to intercept those conditions of renal damage that do not fall within the AKI criteria. The prevalence of AKD we have demonstrated makes it clear that a non-negligible percentage of patients undergoing chemotherapy with cisplatin develop renal impairment that would not be recognized using the classic criteria for AKI. These patients represent a population of cancer patients worthy of long-term nephrological follow-up considering the risk of progression to CKD and end-stage renal disease.
A second significant clinical message from these results is that although cisplatin-induced AKI and AKD are not rare events (12.8% and 25.7% of patients in our cohort), severe AKI and AKD are rare, and in the vast majority of cases the development of AKI or AKD does not affect the achievement of the planned cisplatin dose.
Our study presents some limitations but also several strengths. The main strengths of this study are the size and the careful characterization of the study cohort, as well as the homogeneity of treatment, prophylactic measures and clinical management of patients. Another strength of our study is the identification of several risk factors for cisplatin-induced AKI and AKD. The main limitation is the absence of long-term follow-up, which does not allow to evaluate the clinical meaning of the AKI and AKD episode as it relates to renal function and patient survival. Moreover, data regarding urinary output (which is part of the AKI definition according to KDIGO criteria), markers of tubular injury (urinary b-2 microglobulin, urinary bicarbonates, urinary ph), and proteinuria levels are not available. Other weaknesses include; the relatively small percentage of patients receiving ACEi and ARB treatment, which could lead to underestimation of the role of these medications in increasing the risk of renal damage, the single-center nature of the study, the absence of evaluation of quality of life in our patients.
All 109 consecutive adult patients treated with cisplatin-based CRT for LA-SCCHN between January 2017 and December 2021 were enrolled in a prospective, single-center study in a tertiary care university hospital. Inclusion criteria were: age above 18 years, complete availability of clinical and laboratory data at the time of CRT start, informed consent. Exclusion criteria were: absence of complete clinical and laboratory data, age below 18 years, refusal to sign informed consent, a diagnosis of end-stage renal disease. The follow-up period was in line with the duration of the treatment (3 cycles), and continued until discontinuation due to adverse events requiring treatment schedule modification and/or discontinuation, or death.
All patients received adequate supportive care including 750 ml of saline solution + 16mEq of intravenous magnesium sulphate infused at the rate of 200 ml/h before and after cisplatin administration (a total of 1500 ml at day 0 and again at day 1). In patients with diuresis less than 100 ml/hour after hydration, 375 ml of 10% mannitol was administered. Lastly, dexamethasone at a dose of 12 mg was administered intravenously to all patients as chemo premedication on day 0, and orally at a dose of 8 mg on days 1 to 3 as antiemetic prophylaxis, followed by six days of progressive tapering. The present study was performed in accordance with the Declaration of Helsinki (6th revision, 2008), and the study protocol was reviewed and approved by the local Ethics committee.
Demographic data, medical history, and clinical, laboratory, and histological data at presentation were retrieved from the medical records. For this study we considered the following data: age, gender, BMI, TNM staging, comorbidities (hypertension, diabetes, cardiovascular disease, thyroid disease), platinum dose, and medical therapy (ACEi, ARBs), calcium antagonists, beta blockers and diuretics). Use of concomitant medications that have been reported to cause acute interstitial nephritis, such as non-steroidal anti-inflammatory drugs, allopurinol, proton pump inhibitors and antibiotics, as well as contrast agents for CT-scan or MRI, were reported before treatment and during follow up. Patients were evaluated at the time of the clinical visit in order to identify known causes of renal damage other than cisplatin exposure; these patients were excluded from the analysis. Serum creatinine values (Kinetic Picrate standardized (COBAS C 800) for IDMS) were recorded at baseline and after each cycle of treatment, respectively, at day 1 and day 7. The eGFR was calculated using the creatinine-based eGFR formula, CKD-EPI 2012.
Chronic Kidney Disease classes were created according to the KDIGO guidelines for G categories with the following thresholds: over 90 mL/min/1.73m2 (G1), 89-60 mL/min/1.73m2 (G2), 59-45 mL/min/1.73m2 (G3a), 44-30 mL/min/1.73m2 (G3b) and below 30 mL/min/1.73m2 (G4-5) (39). Acute kidney injury onset was diagnosed according to KDIGO 2012 criteria, based on the sCr increase, i.e., a sCr increase greater than 1.5 times the baseline value was classified as stage 1, greater than 2 times as stage 2, and greater than 3 times as stage 3 (28). Urinary output data were not collected for AKI evaluation. In 2017, the Acute Disease Quality Initiative (ADQI) and KDIGO consensus conferences introduced the term ‘Acute Kidney Disease’ in an effort to define all renal function alterations not fulfilling AKI and CKD criteria. Although the original definition encompassed all renal function abnormalities occurring from 7 to 90 days following a possible insult (40), the current definition includes AKI or eGFR < 60 ml/min/1.73 m2, or eGFR decrease by ≥ 35%, or sCr increase by 50% occurring less than 90 days after the possible insult (24). In our manuscript, all episodes of a sCr increase of more than 50% within 7 days after cisplatin exposure have been defined as AKI, while the AKD term was reserved for renal function abnormalities occurring up to 90 days after cisplatin exposure.
Comparisons between numerical variables were performed using multivariable linear regressions to evaluate clinical factors associated with eGFR decline; for between-group differences, the t-test for numerical variables was used, while Fisher’s exact test was used for categorical variables. Multivariable logistic regression was used to evaluate clinical factors related to AKI onset. Data analysis was performed using programming language R and RSTUDIO integrated development environment.
In literature, AKI and AKD are frequent and frightening complications of high-dose cisplatin-based CRT in patients with LA-SCCHN, thus limiting the use of this type of chemotherapy in the general population and especially in CKD patients.
Our study highlights a lower incidence of platinum-induced AKI than previously reported, with the presence of hypertension and normal baseline eGFR ≥ 90 ml/min/1.73 m2 as possible risk factors for both AKI and AKD development. Moreover, hydration and magnesium support represent the cornerstone of AKI prevention in our cisplatin-based CRT, suggesting that both patients with normal and mildly reduced renal function could undergo high dosage cisplatin therapy for LA-SCCHN as long as monitoring with an accurate multidisciplinary strategy is carried out. Further studies are needed to confirm our results.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by San Raffaele Ethics Committee (65/INT/2022). Informed consent was obtained from all subjects involved in the study.
Conceptualization: FT, AM, MF, and NL; Methodology: FT, FM, MF, NL, and AM; Investigation: GQ, DV, LG, ID’O, and SC; Visualization: FT, and MF; Supervision: FT, MF, AM, and NL; Project administration: FT, AC, and AM; Software: FM; Formal analysis: FM; Data curation: FM, NL, and GQ; Writing – original draft: FT, AM, NL, and MF; Writing – review and editing: FT, NL, MF, and AM. All authors contributed to the article and approved the submitted version.
Author AC was employed by the company Biorek srl.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1173578/full#supplementary-material
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2018) 68:394–424. doi: 10.3322/CAAC.21492
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA: A Cancer J Clin (2020) 70:7–30. doi: 10.3322/CAAC.21590
3. Cancer.Net editorial board | Cancer.Net . Available at: https://www.cancer.net/about-us/cancernet-editorial-board (Accessed 11 March 2022).
4. Mehanna HM, Rattay T, Smith J, McConkey CC. Treatment and follow-up of oral dysplasia - a systematic review and meta-analysis. Head Neck (2009) 31:1600–9. doi: 10.1002/HED.21131
5. Kelland L. The resurgence of platinum-based cancer chemotherapy. Nat Rev Cancer (2007) 7:573–84. doi: 10.1038/NRC2167
6. van der Vorst MJDL, Neefjes ECW, Toffoli EC, Oosterling-Jansen JEW, Vergeer MR, Leemans CR, et al. Incidence and risk factors for acute kidney injury in head and neck cancer patients treated with concurrent chemoradiation with high-dose cisplatin. BMC Cancer (2019) 19. doi: 10.1186/S12885-019-6233-9
7. Akmar L, Cunnell M, Kelly C, Kovarik J, Iqbal MS. Concomitant weekly cisplatin-based chemoradiotherapy in head and neck cancer: the value of a second measured glomerular filtration rate during treatment. Br J Radiol (2021) 94. doi: 10.1259/BJR.20200717
8. Miller RP, Tadagavadi RK, Ramesh G, Reeves WB. Mechanisms of cisplatin nephrotoxicity. Toxins (Basel) (2010) 2:2490–518. doi: 10.3390/TOXINS2112490
9. Pabla N, Dong Z. Cisplatin nephrotoxicity: mechanisms and renoprotective strategies. Kidney Int (2008) 73:994–1007. doi: 10.1038/SJ.KI.5002786
10. Sahu BD, Kuncha M, Sindhura GJ, Sistla R. Hesperidin attenuates cisplatin-induced acute renal injury by decreasing oxidative stress, inflammation and DNA damage. Phytomedicine (2013) 20:453–60. doi: 10.1016/J.PHYMED.2012.12.001
11. Perazella MA, Wilson FP. Preventing acute kidney injury through nephrotoxin management. Nat Rev Nephrol 2016 12:9 (2016) 12:511–2. doi: 10.1038/nrneph.2016.95
12. Bouglé A, Duranteau J. Pathophysiology of sepsis-induced acute kidney injury: the role of global renal blood flow and renal vascular resistance. Contrib Nephrol (2011) 174:89–97. doi: 10.1159/000329243
14. Lameire NH, Levin A, Kellum JA, Cheung M, Jadoul M, Winkelmayer WC, et al. Harmonizing acute and chronic kidney disease definition and classification: report of a kidney disease: improving global outcomes (KDIGO) consensus conference. Kidney Int (2021) 100(3):516–26. doi: 10.1016/j.kint.2021.06.028
15. Ghosh S, Rao PB, Kumar PR, Manam S. Concurrent chemoradiation with weekly cisplatin for the treatment of head and neck cancers: an institutional study on acute toxicity and response to treatment. Asian Pac J Cancer Prev (2015) 16:7331–5. doi: 10.7314/APJCP.2015.16.16.7331
16. Rühle A, Haehl E, David H, Kalckreuth T, Sprave T, Stoian R, et al. The value of laboratory parameters for anemia, renal function, systemic inflammation and nutritional status as predictors for outcome in elderly patients with head-and-Neck cancers. Cancers (Basel) (2020) 12:1–19. doi: 10.3390/CANCERS12061698
17. Driessen CML, Uijen MJM, van der Graaf WTA, van Opstal CCM, Kaanders JHAM, Nijenhuis T, et al. Degree of nephrotoxicity after intermediate- or high-dose cisplatin-based chemoradiotherapy in patients with locally advanced head and neck cancer. Head Neck (2016) 38 Suppl 1:E1575–81. doi: 10.1002/HED.24281
18. Faig J, Haughton M, Taylor RC, D’Agostino RB, Whelen MJ, Porosnicu Rodriguez KA, et al. Retrospective analysis of cisplatin nephrotoxicity in patients with head and neck cancer receiving outpatient treatment with concurrent high-dose cisplatin and radiotherapy. Am J Clin Oncol (2018) 41:432–40. doi: 10.1097/COC.0000000000000301
19. Bhat ZY, Cadnapaphornchai P, Ginsburg K, Sivagnanam M, Chopra S, Treadway CK, et al. Understanding the risk factors and long-term consequences of cisplatin-associated acute kidney injury: an observational cohort study. PloS One (2015) 10(11):e0142225. doi: 10.1371/JOURNAL.PONE.0142225
20. Shord SS, Thompson DM, Krempl GA, Hanigan MH. Effect of concurrent medications on cisplatin-induced nephrotoxicity in patients with head and neck cancer. Anticancer Drugs (2006) 17(2):207–15. doi: 10.1097/00001813-200602000-00013
21. Spiotto MT, Cao H, Mell L, Toback FG. Angiotensin-converting enzyme inhibitors predict acute kidney injury during chemoradiation for head and neck cancer. Anticancer Drugs (2015) 26:343–9. doi: 10.1097/CAD.0000000000000191
22. Patimarattananan T, Nongnuch A, Pattaranutaporn P, Unwanatham N, Jiarpinitnun C, Ngamphaiboon N. Risk and impact of delayed renal impairment in patients with locally advanced head and neck squamous cell carcinoma receiving chemoradiotherapy with cisplatin. Support Care Cancer. (2021) 29(2):877–87. doi: 10.1007/s00520-020-05566-y
23. Suppadungsuk S, Phitakwatchara W, Reungwetwattana T, Pathumarak A, Phakdeekitcharoen B, Kitiyakara C, et al. Preloading magnesium attenuates cisplatin-associated nephrotoxicity: pilot randomized controlled trial (PRAGMATIC study). ESMO Open (2022) 7(1):100351. doi: 10.1016/j.esmoop.2021.100351
24. Rachman A, Shatri H. Correlation between higher cumulative dose of cisplatin for concurrent chemoradiation and acute kidney disease incidence among nasopharyngeal carcinoma patients: a comparative study. Int J Gen Med (2021) 14:10527–39. doi: 10.2147/IJGM.S343644
25. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, Acute Dialysis Quality Initiative workgroup Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the second international consensus conference of the acute dialysis quality initiative (ADQI) group. Crit Care (2004) 8(4):R204–12. doi: 10.1186/cc2872
26. Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, et al. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care (2007) 11(2):R31. doi: 10.1186/cc5713
27. US DEPARTMENT OF HEALTH AND HUMAN SERVICES, et al. Common terminology criteria for adverse events. (2020). Available at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_50.
28. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl (2012) 2(1):1–138. doi: 10.1038/kisup.2012.1
29. Rades D, Kronemann S, Meyners T, Bohlen G, Tribius S, Kazic N, et al. Comparison of four cisplatin-based radiochemotherapy regimens for nonmetastatic stage III/IV squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Phys (2011) 80:1037–44. doi: 10.1016/J.IJROBP.2010.03.033
30. de Jongh FE, van Veen RN, Veltman SJ, de Wit R, van der Burg MEL, van den Bent MJ, et al. Weekly high-dose cisplatin is a feasible treatment option: analysis on prognostic factors for toxicity in 400 patients. Br J Cancer (2003) 88:1199–206. doi: 10.1038/SJ.BJC.6600884
31. Galfetti E, Cerutti A, Ghielmini M, Zucca E, Wannesson L. Risk factors for renal toxicity after inpatient cisplatin administration. BMC Pharmacol Toxicol (2020) 21. doi: 10.1186/S40360-020-0398-3
32. Motwani SS, McMahon GM, Humphreys BD, Partridge AH, Waikar SS, Curhan GC. Development and validation of a risk prediction model for acute kidney injury after the first course of cisplatin. J Clin Oncol (2018) 36:682–8. doi: 10.1200/JCO.2017.75.7161
33. Prasaja Y, Sutandyo N, Andrajati R. Incidence of cisplatin-induced nephrotoxicity and associated factors among cancer patients in Indonesia. Asian Pac J Cancer Prev (2015) 16:1117–22. doi: 10.7314/APJCP.2015.16.3.1117
34. Yokoo K, Murakami R, Matsuzaki T, Yoshitom K, Hamada A, Saito H. Enhanced renal accumulation of cisplatin via renal organic cation transporter deteriorates acute kidney injury in hypomagnesemic rats. Clin Exp Nephrol (2009) 13:578–84. doi: 10.1007/S10157-009-0215-1
35. Crona DJ, Faso A, Nishijima TF, McGraw KA, Galsky MD, Milowsky MI. A systematic review of strategies to prevent cisplatin-induced nephrotoxicity. Oncologist (2017) 22:609–19. doi: 10.1634/THEONCOLOGIST.2016-0319
36. Kimura T, Ozawa T, Hanai N, Hirakawa H, Suzuki H, Hosoi H, et al. Renal protective effect of a hydration supplemented with magnesium in patients receiving cisplatin for head and neck cancer. J otolaryngol head. Neck Surg (2018) 47. doi: 10.1186/S40463-018-0261-3
37. Morgan KP, Snavely AC, Wind LS, Buie LW, Grilley-Olson J, Walko CM, et al. Rates of renal toxicity in cancer patients receiving cisplatin with and without mannitol. Ann Pharmacother (2014) 48:863–9. doi: 10.1177/1060028014533303
38. Leu L, Baribeault DA. Comparison of the rates of cisplatin (CDDP)–induced nephrotoxicity associated with sodium loading or sodium loading with forced diuresis as a preventative measure. J Oncol Pharm Pract (2010) 16:167–71. doi: 10.1177/1078155209346071
39. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. (2013) 3:1–150. doi: 10.1038/kisup.2012.63
Keywords: AKI, acute kidney injury, cancer, cisplatin, head and neck, AKD, acute kidney disease
Citation: Trevisani F, Di Marco F, Quattrini G, Lepori N, Floris M, Valsecchi D, Giordano L, Dell’Oca I, Cardellini S, Cinque A and Mirabile A (2023) Acute kidney injury and acute kidney disease in high-dose cisplatin-treated head and neck cancer. Front. Oncol. 13:1173578. doi: 10.3389/fonc.2023.1173578
Received: 24 February 2023; Accepted: 10 May 2023;
Published: 09 June 2023.
Edited by:
Michele Ghidini, IRCCS Ca ‘Granda Foundation Maggiore Policlinico Hospital, ItalyReviewed by:
Nerina Denaro, IRCCS Ca ‘Granda Foundation Maggiore Policlinico Hospital, ItalyCopyright © 2023 Trevisani, Di Marco, Quattrini, Lepori, Floris, Valsecchi, Giordano, Dell’Oca, Cardellini, Cinque and Mirabile. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Trevisani, dHJldmlzYW5pLmZyYW5jZXNjb0Boc3IuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.