
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 19 April 2023
Sec. Surgical Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1166327
This article is part of the Research TopicBody Composition and Malnutrition in Transplant Oncology and in Hepato-Pancreato-Biliary Cancers: Potentially Modifiable Risk-Factors with Major Clinical ImpactView all 7 articles
 Shilei Bai1†
Shilei Bai1† Pinghua Yang2†
Pinghua Yang2† Yanping Wei3,4†Jie Wang1Caixia Lu1
Yanping Wei3,4†Jie Wang1Caixia Lu1 Yong Xia5Anfeng Si6Baohua Zhang2
Yong Xia5Anfeng Si6Baohua Zhang2 Feng Shen3
Feng Shen3 Yexiong Tan3,4*
Yexiong Tan3,4* Kui Wang1*
Kui Wang1*Background and Aim: The prediction models of postoperative survival for hepatitis B virus-related hepatocellular carcinoma (HBV-HCC) with microvascular invasion (MVI) have not been well established. The study objective was the development of nomograms to predict disease recurrence and overall survival (OS) in these patients.
Methods: Data were obtained from 1046 HBV-related MVI-positive HCC patients who had undergone curative resection from January 2014 to December 2017. The study was approved by the Eastern Hepatobiliary Surgery Hospital and Jinling Hospital ethics committee, and patients provided informed consent for the use of their data. Nomograms for recurrence and OS were created by Cox regression model in the training cohort (n=530). The modes were verified in an internal validation cohort (n= 265) and an external validation cohort (n= 251).
Results: The nomograms of recurrence and OS based on preoperative serological indicators (HBV-DNA, neutrophil-lymphocyte ratio, a-fetoprotein), tumor clinicopathologic features (diameter, number), surgical margin and postoperative adjuvant TACE achieved high C-indexes of 0.722 (95% confidence interval [CI], 0.711-0.732) and 0.759 (95% CI, 0.747-0.771) in the training cohort, respectively, which were significantly higher than conventional HCC staging systems (BCLC, CNLC, HKLC).The nomograms were validated in the internal validation cohort (0.747 for recurrence, 0.758 for OS) and external validation cohort(0.719 for recurrence, 0.714 for OS) had well-fitted calibration curves. Our nomograms accurately stratified patients with HBV-HCC with MVI into low-, intermediate- and high-risk groups of postsurgical recurrence and mortality. Prediction models for recurrence-free survival (https://baishileiehbh.shinyapps.io/HBV-MVI-HCC-RFS/) and OS (https://baishileiehbh.shinyapps.io/HBV-MVI-HCC-OS/) were constructed.
Conclusions: The two nomograms showed good predictive performance and accurately distinguished different recurrence and OS by the nomograms scores for HBV-HCC patients with MVI after resection.
Hepatocellular carcinoma (HCC) is a prevalent and deadly tumor (1). In East Asia, between 70% and 90% of HCC is related to infection with hepatitis B virus (HBV) (2). The first-line treatment is usually liver resection (LR); however, the long-term outcome after LR remains unsatisfactory due to the high rate of early recurrence (2).
The presence of microvascular invasion (MVI) may significantly influence HCC outcomes following either LR or liver transplantation (LT), increasing the risk of early tumor recurrence (3–6). There appears to be an association between microscopic metastases within the liver related to MVI that is not apparent in other forms of HCC (7–9). It has been suggested that HBV infection promotes angiogenesis by increasing levels of metastasis-associated protein 1 (MTA1) or by suppressing the immune response to migrating tumor cells, resulting in invasion of the vasculature (10, 11).
Several factors have been found to influence outcome in HBV-related MVI-positive HCC following LR. Viral status, tumor clinicopathologic features, the patient’s overall condition (including immune and liver function, and systemic inflammation), surgical factors, and the availability of postoperative adjuvant therapy may potentially contribute to progression and recurrence of the cancer. There is no specific prognostic tool for predicting outcome in HBV-related MVI-positive HCC patients following LR and, although there are several traditional staging systems, such as The American Joint Committee on Cancer (AJCC), Barcelona Clinic Liver Cancer (BCLC), Hong-Kong Liver Cancer staging system (HKLC) and the China Liver Cancer (CNLC) systems, that are used for HCC classification and outcome prediction, there is no single uniformly accepted system (12, 13). Moreover, these criteria vary widely and cannot accurately predict individualized outcomes after surgery in this patient population.
The nomogram, which integrates multiple prognostic factors, is considered reliable for risk quantification and has been used in many cancer varieties (14–18). Nomograms have been developed for the prediction of outcomes of HCC after LR and have greater accuracy than the traditional staging systems (19–21). Nevertheless, there is no specific model for prognosis prediction in HBV-related MVI-positive HCC. Therefore, we used a retrospective analysis of 795 HBV-related MVI-positive HCC patients to develop nomograms for assessing the likelihood of postoperative recurrence and overall survival (OS) to guide clinical decision-making in these patients.
795 consecutive HBV-related HCC patients were included. The patients had undergone radical LR and had been pathologically confirmed as MVI-positive between January 2014 and December 2017 at Shanghai Eastern Hepatobiliary Surgery Hospital (EHBH). Inclusion criteria were: (I). postoperative pathologically confirmed HCC with positive MVI; (II). patients with Child score of grade A or B; (III). no preoperative antitumor therapy; (IV). the surgical approach was radical LR (R0 resection); (V). no large vessel invasion. Exclusion criteria were: (I). incomplete clinical data; (II). tumor recurrence within 1 month or patient death within 3 months after surgery; (III). patient combined with other tumor history; (IV). bile duct tumor thrombosis. The R function “create Data Partition” was used to divide the 795 patients into training(n=530) and internal validation cohorts(n=265) with a ratio of 2:1 to guarantee random distribution of outcomes between the groups. The training cohort was used for filtering variables and model construction, which were then verified in the validation cohort. A total of 251 patients between January 2014 and December 2017 from Jinling Hospital of Nanjing Medical University served as an external validation cohort. The study was approved by the hospital ethics committee, and patients provided informed consent for the use of their data.
Routine preoperative tests included measurement of liver function, hepatitis B and C antigens/antibodies, alpha-fetoprotein (AFP), abdominal ultrasound, abdominal contrast-enhanced magnetic resonance imaging (MRI) or computed tomography (CT), and chest X-ray. Serum HBV deoxyribonucleic acid (HBV-DNA) levels were quantified by polymerase chain reaction (ABI7300 Real-Time PCR System). HCC was diagnosed preoperatively using the criteria of the American Association for the Study of Liver Diseases (AASLD) (22).
All procedures were conventional open surgery with routine use of intraoperative ultrasound, and the extent of resection was determined by the tumor size and location, as well as the general condition of the patient. The shortest distance between the tumor margin and the plane of resection ≥1 cm, depending on the postoperative pathology, was used to define the wide margin (23, 24). The presence of microscopic tumor metastases within the portal or hepatic veins in tissue surrounding the tumor was used to define MVI (25). Tumor differentiation was evaluated using the Edmondson-Steiner system (26). Transcatheter arterial chemoembolization (TACE) was performed on the whole residual liver or the corresponding half of the liver approximately 1 month after LR.
Follow-up assessments were undertaken every two months in the six-month period following LR and thereafter at three-monthly intervals for 18 months and at six-monthly intervals thereafter. Assessments included testing for the tumor marker AFP in peripheral blood and ultrasound, as well as in enhanced abdominal CT or MRI. Patients on preoperative antiviral treatment (AVT) were advised to continue AVT postoperatively. CT, MRI, or bone scan were conducted if there was suspicion of distant metastases or recurrence. Recurrence was defined as a newly present tumor nodule, either within or outside the liver. Decisions for the management of recurrent tumors were based on recurrence pattern, liver functioning, and the overall condition. The options were re-resection, local ablation, TACE, radiotherapy, systemic therapy or best supportive care, either individually or combined.
The primary endpoint was OS, calculated as the time between the dates of diagnosis and all-cause death, respectively, or last follow-up visit at December 2021. Time to recurrence (TTR) was determined as the time between the dates of surgery and tumor recurrence, respectively.
Continuous variables were compared using t-tests or Mann-Whitney U tests, while categorical variables were compared using χ2 or Fisher exact tests. Survival curves were calculated and compared using the Kaplan-Meier method. Cox regression analyses were used for analysis of prognostic factors.
The nomograms were developed using multivariate analysis of the data of patients in the training. Variables for inclusion were selected using stepwise regression based on the minimum of the Akaike information criterion. Recurrence and OS rates at 1/3/5 years were assessed using nomograms. The concordance index (C-index) calculated by bootstrapping and the area under the time-dependent receiver operating characteristic curve (time-dependent AUC) were used to assess discriminatory capability. Calibration capability was assessed using calibration curves. The C-index and AUC values ranged from 0.5 to 1.0, where 0.5 represents perfectly random and 1.0 represents a perfect fit. Values over 0.7 for both these parameters are considered to have superior predictive power. X-tile was used to select cutoff points for risk stratification (27).
P-values were two-tailed with values < 0.05 considered significant. Data were analyzed in R (http://www.r-project.org/)
The baseline profiles in the training and validation cohorts are shown in Table 1. A total of 1046 HBV-related MVI-positive HCC patients were enrolled, including 530 patients in the training cohort,265 patients in the internal validation cohort and 251 patients in the external validation cohort, respectively. The exclusion criteria are provided in Supplementary Figure 1. Of all patients, 932 patients (89.1%) were male, 1024 (97.9%) were Child A grade, while 458 (43.8%) had AFP>400 ng/ml, 325 (31.1%) were HBeAg-positive, and 394 (37.7%) had HBV-DNA>2000 IU/ml. The mean tumor diameter of the patients was 6.7 cm, 144 (13.8%) patients had multiple HCC, 577 (55.2%) patients had a postoperative pathological diagnosis of cirrhosis, and 523 (50.0%) patients underwent postoperative TACE therapy. There were no significant differences in baseline characteristics among the 3 cohorts except that patients in the external validation cohort had a lower ALBI grade II (P=0.011), smaller tumor diameter (P=0.026) and more postoperative TACE rates (P <0.001) when compared with the data of the training and internal validation cohorts.
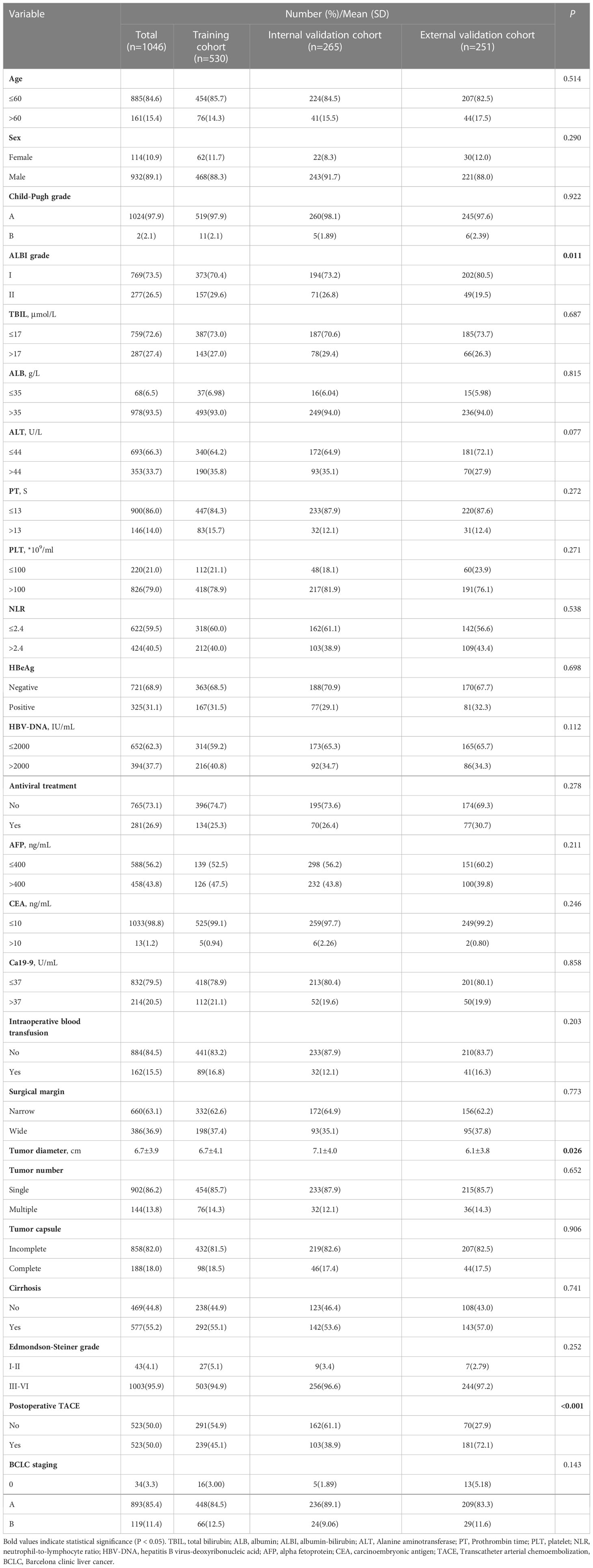
Table 1 Baseline characteristics of patients between training and validation cohort.
The postoperative survival curves of the training and validation cohorts are shown in the Supplementary Figure 2. The recurrence and OS rates at 1-, 3-, and 5- years were 45.5%, 59.1%, 71.0% vs. 45.7%, 66.8%, 77.2%, and 77.4%, 56.9%, 42.7% vs. 78.0%, 54.4%, 39.3% for the training cohort and internal validation cohort, respectively,. The median TTR was 18.1 months and 16.9 months in the two groups, respectively. For the external validation cohort, the 1-, 3- and 5-year recurrence rates were 37.7%, 62.9% and 68.8%, respectively, and the 1-, 3- and 5-year OS rates were 84.3%, 59.1% and 44.4%, respectively. The median TTR was 19.4 months. Moreover, there was no significant difference in the 1-, 3- and 5-year recurrence and OS among these 3 cohorts.
Univariate Cox regression showed 15 variables associated with recurrence and 17 associated with survival (Tables 2, 3). After inclusion of these variables in the multivariate analysis, it was found that the neutrophil-lymphocyte ratio (NLR)>2.4, HBV-DNA>2000 IU/ml, AFP>400 ng/ml, narrow surgical margins, tumor diameter, multiple tumors, and the absence of postoperative TACE independently predicted both recurrence and OS (Tables 2, 3). Nomograms were then developed using these results for the prediction of recurrence (Figure 1A) and OS rates (Figure 1B) at one, three, and five years in HBV-related MVI-positive HCC patients. The nomogram predicted the probabilities by summation of the scores of the individual variables and their location on a scale of the total score.
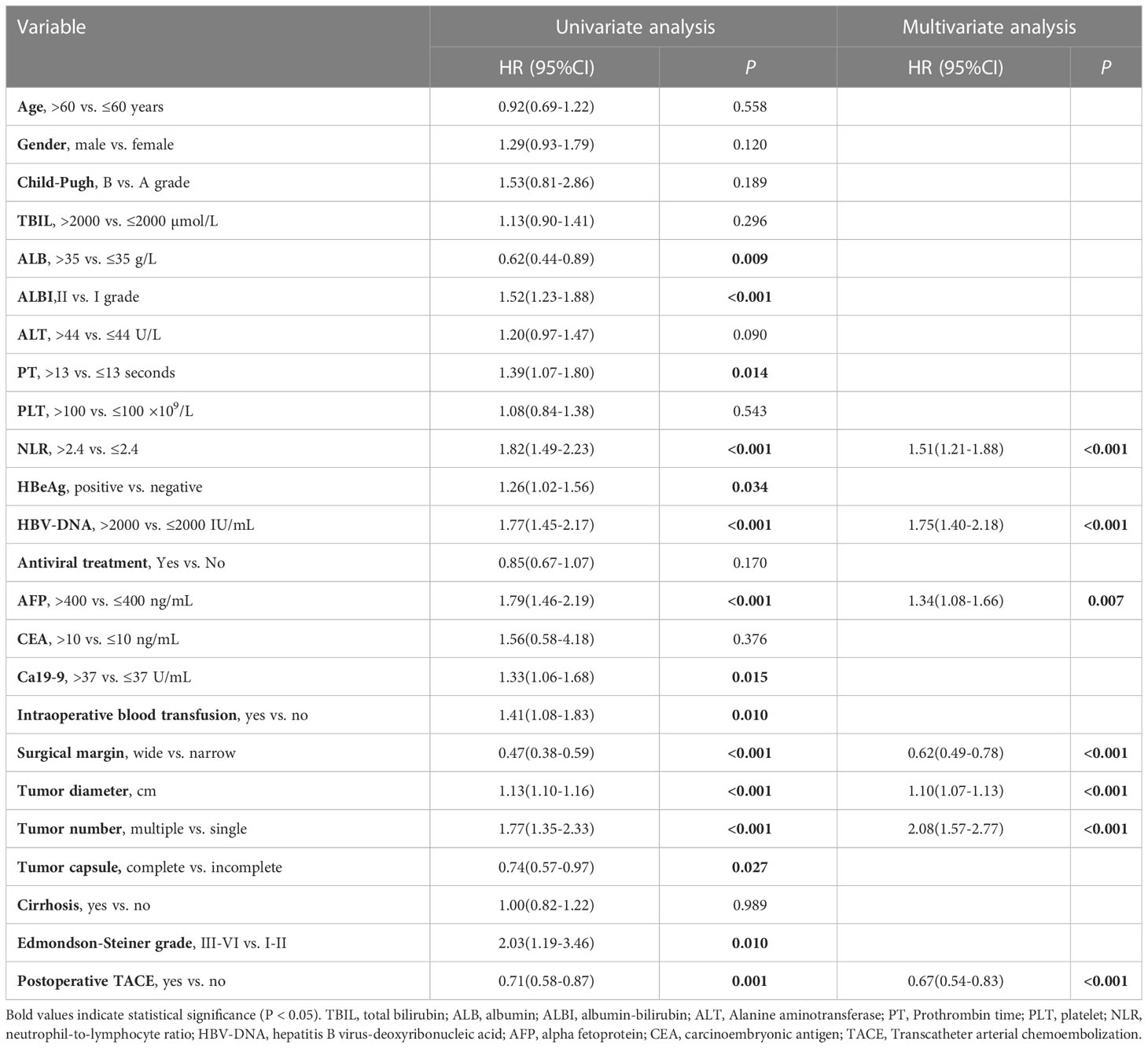
Table 2 Univariate and multivariate cox regression analysis of recurrence in the training cohort.
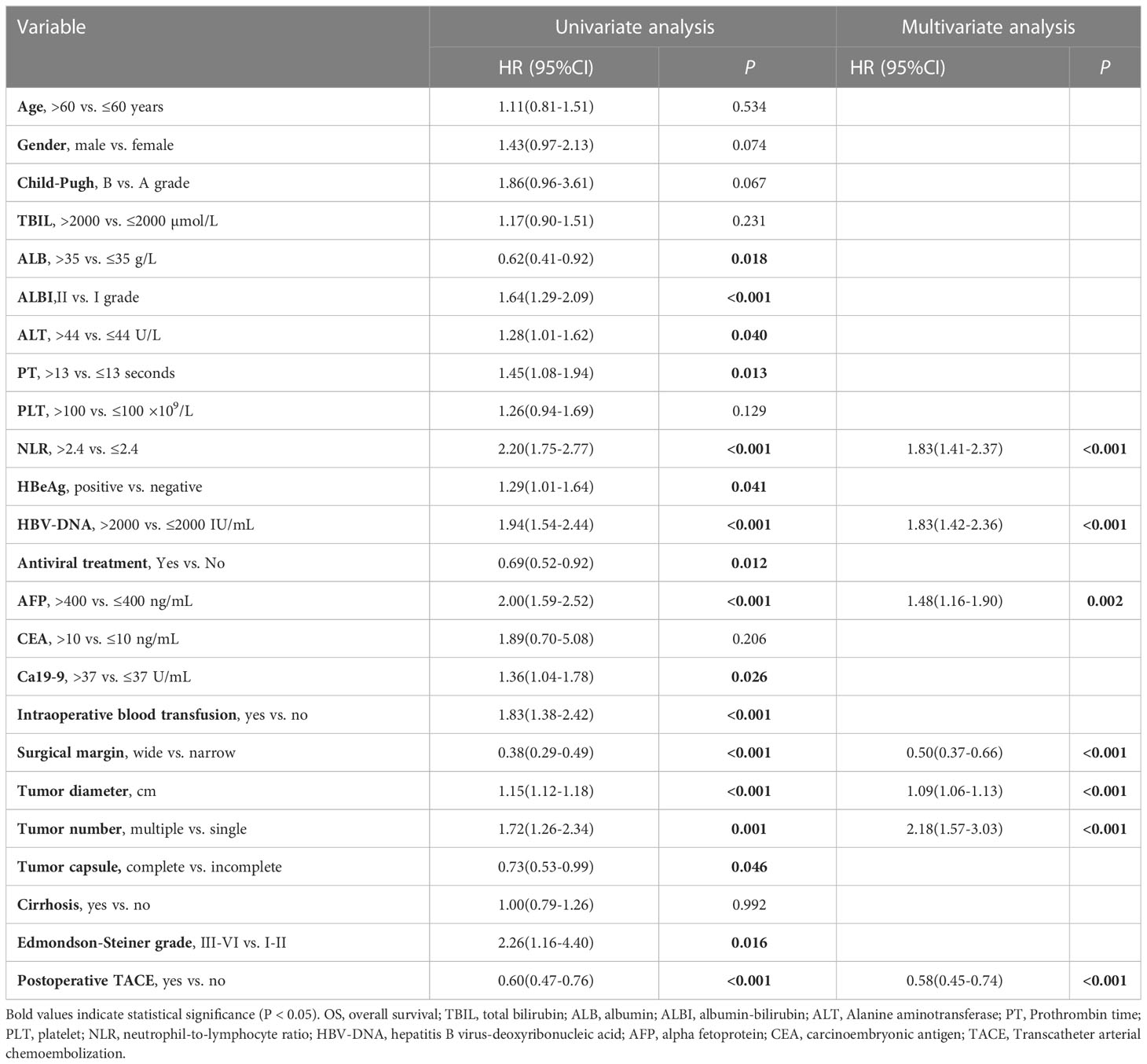
Table 3 Univariate and multivariate cox regression analysis of OS in the training cohort.
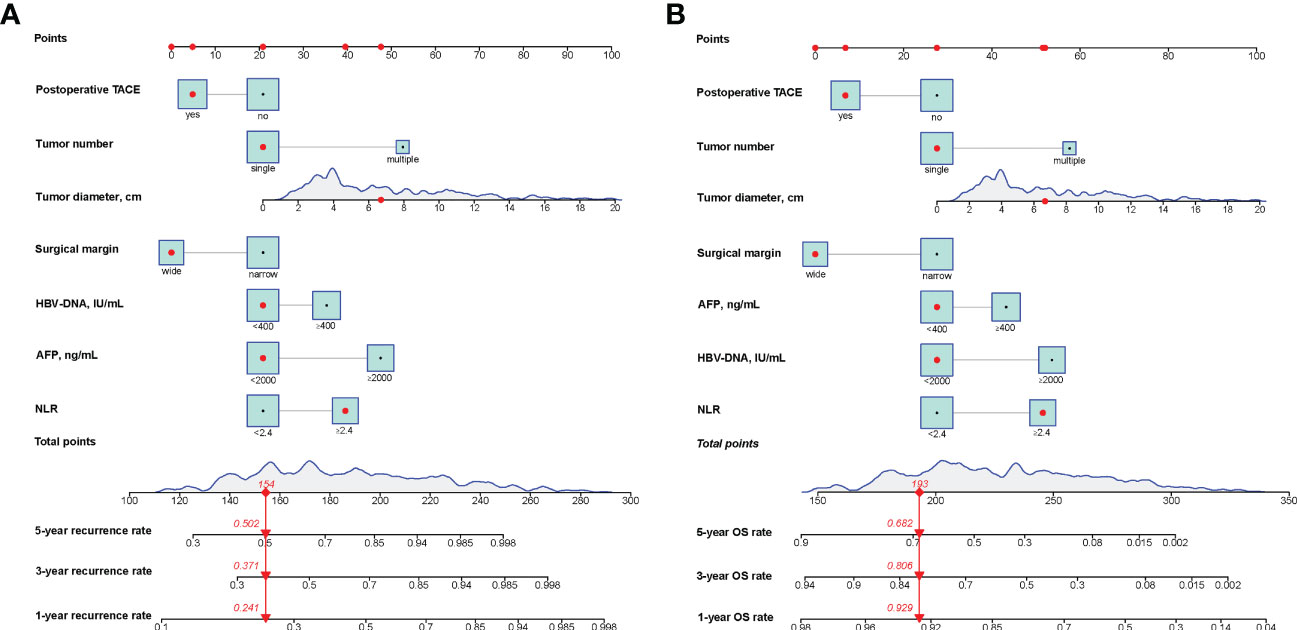
Figure 1 Nomograms for predicting the 1-, 3- and 5-year recurrence (A) and OS (B) rates in patients with HBV-HCC with MVI. OS, overall survival; HCC, hepatocellular carcinoma; NLR, neutrophilto-lymphocyte ratio; TACE, transcatheter arterial chemoembolisation; AFP, alpha-fetoprotein; HBV-DNA, HBV deoxyribonucleic acid.
For the prediction of recurrence, the Harrell’s C-indices in the training and validation cohorts were 0.722 (95% CI, 0.711-0.732) and 0.747 (0.733-0.760), respectively, while the C-indices for OS were 0.759 (95% CI, 0.747-0.771) and 0.758 (0.741-0.776), respectively. In the external validation cohort, Harrell’s C-indices for recurrence and OS prediction were 0.719 (95% CI, 0.701-0.738) and 0.714(95% CI, 0.694-0.734), respectively. The C-index for predicting recurrence for the staging system CNLC, BCLC and HKLC were 0.639 (95% CI, 0.627-0.651),0.552 (95% CI, 0.542-0.562) and 0.617(95% CI, 0.604-0.629), respectively; the corresponding C-index values for predicted OS were 0.653 (95% CI,0.639-0.666),0.558 (95% CI,0.546-0.569) and 0.636(95% CI, 0.622-0.650) respectively. The time-dependent AUCs were >0.7 for predicting recurrence and OS within five years in three groups (Figure 2). Furthermore, the calibration curves for recurrence and OS at 1-, 3-, and 5- years indicated consistency between the nomogram predictions and actual data (Figure 3).
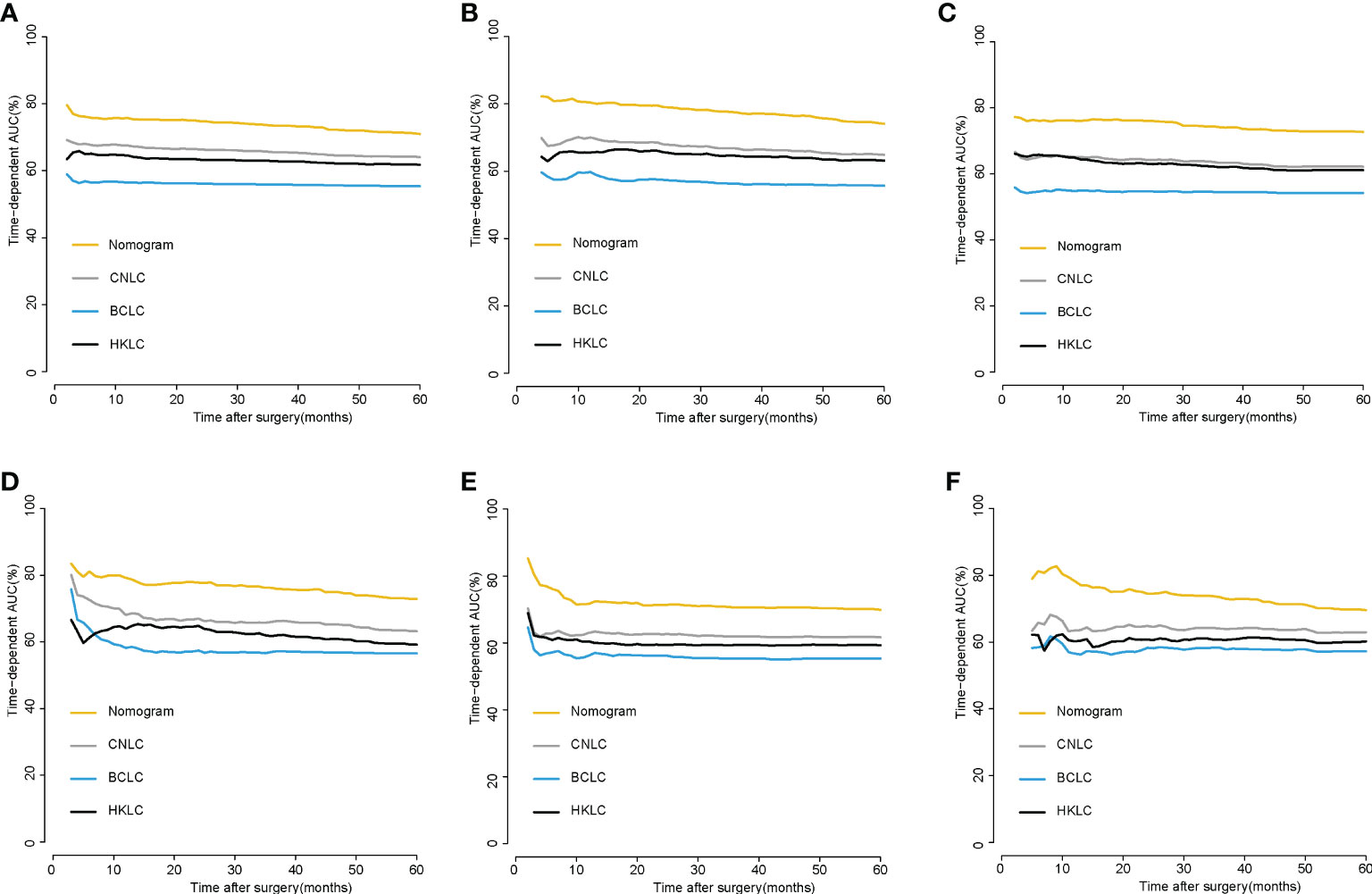
Figure 2 Time-dependent AUC of using the nomogram to predict recurrence and OS probability within 5 years in the training cohort (A, B),internalvalidation cohorts (C, D) and external validation cohorts (E, F).
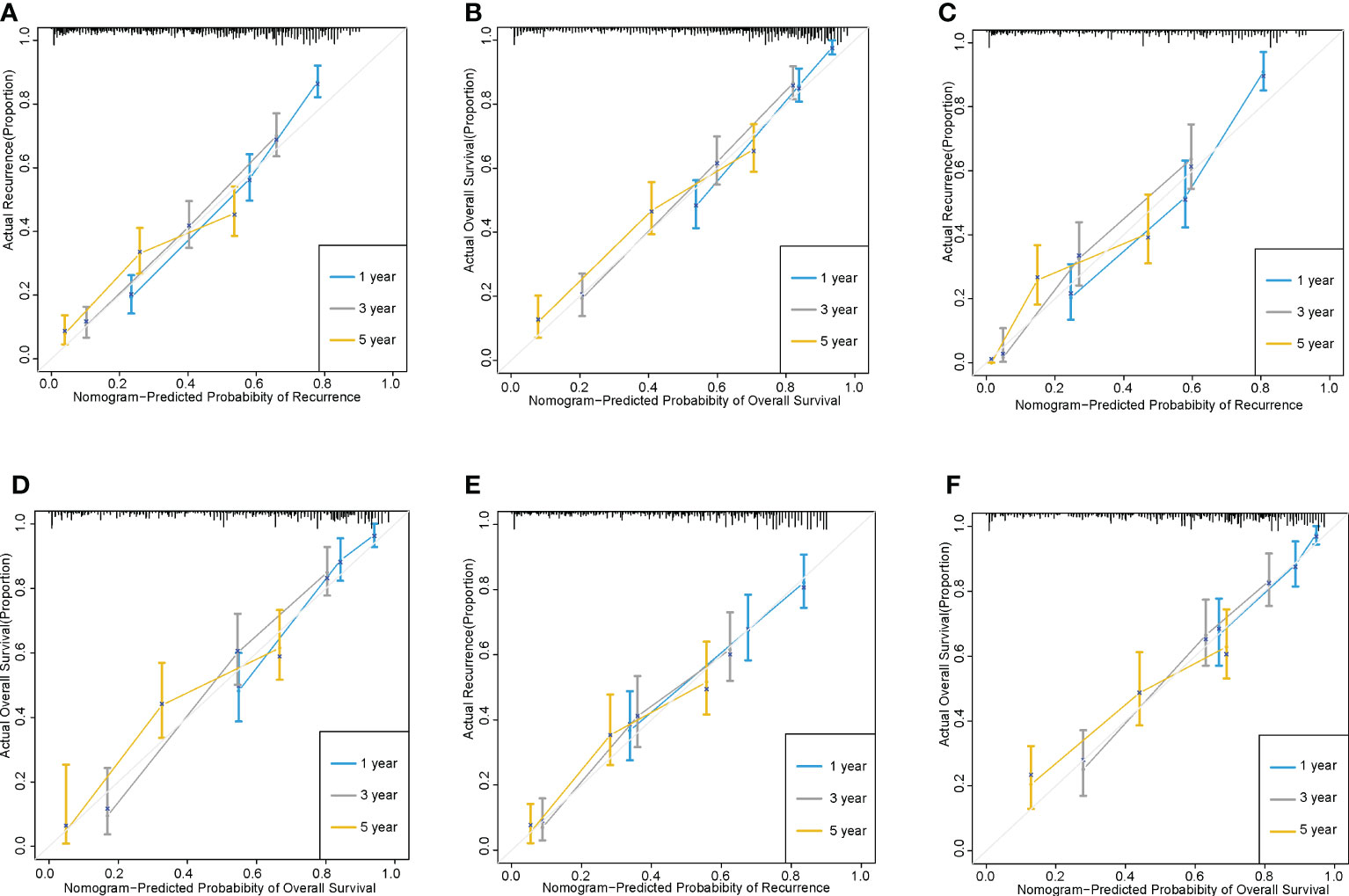
Figure 3 The calibration curves of recurrence and OS based on nomogram prediction and actual observation. 1-, 3- and 5-year recurrence and overall survival in the training cohorts (A, B); 1-, 3- and 5-year recurrence and overall survival in the internal validation cohorts (C, D);1-, 3- and 5-year recurrence and overall survival in the external validation cohorts (E, F).
X-tile software was applied for the determination of the optimum cut off values of the cumulative scores of the nomograms. In the recurrence nomogram in the training cohort, patients were graded as low (≤ 172 points), intermediate (172-203 points), and high (>203 points) risk, with three-year recurrence rates of 32.1%, 59.1%, and 89.1%, respectively (P<0.001) (Figure 4A). In the OS nomogram, patients were graded as low (≤ 214 points), intermediate (214-246 points), and high (> 246 points) risk, with three-year OS rates of 84.8%, 59.1%, and 21.7%, respectively (P<0.001) (Figure 4B). The findings for the internal validation cohort and external validation cohort were consistent (Figures 4C–F).
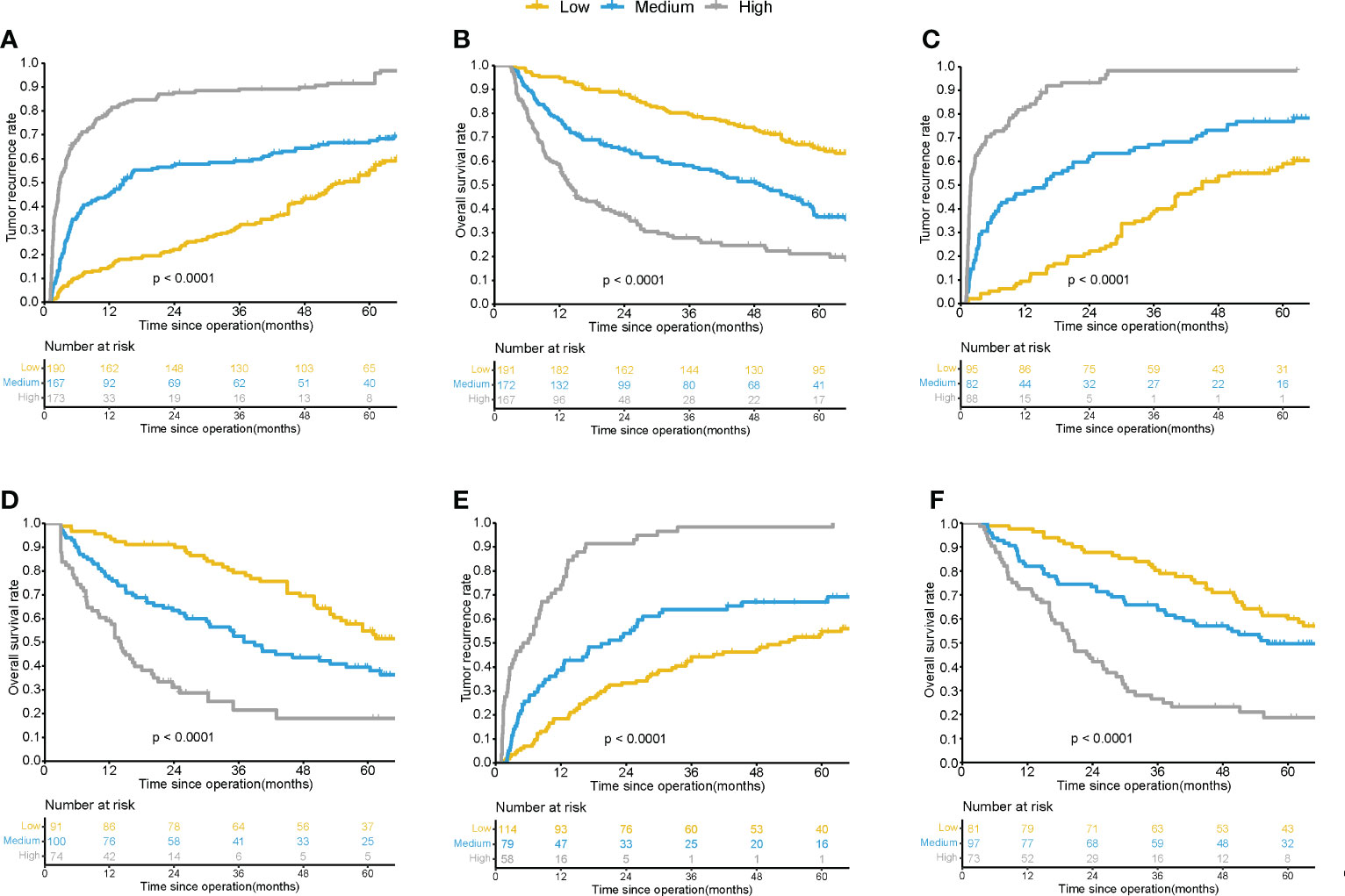
Figure 4 Kaplan-Meier survival curves for patients with different risk of postsurgical recurrence and OS by the nomogram score in training cohorts (A, B), internalvalidation cohorts (C, D) and external validation cohorts (E, F).
To make the nomograms more accessible, we have established a webserver allowing researchers and clinicians to predict recurrence and OS in HBV-associated MVI-positive HCC patients. This is available at https://baishileiehbh.shinyapps.io/HBV-MVI-HCC-RFS/ and https://baishileiehbh.shinyapps.io/HBV-MVI-HCC-OS/.
In East Asia, 70%-90% of HCC is caused by HBV infection, and the presence of MVI can be detected in 15.0%-57.1% of pathological specimens of HCC patients undergoing LR or LT (2, 6). There are various factors affecting the long-term prognosis of HBV-associated MVI-positive HCC patients, but previous staging guidelines often fail to take into account all relevant parameters to make individualized prognosis predictions for this type of HCC patients (6, 28, 29). In this paper, nomograms incorporate seven variables related to recurrence and OS in HBV-related MVI-positive HCC patients, encompassing tumor characteristics (tumor diameter, tumor number), inflammatory indicators (NLR), viral status (HBV-DNA), AFP, surgical status (surgical margins) and postoperative adjuvant therapy (postoperative adjuvant TACE). We established the first nomograms based on large sample data to predict recurrence and OS after LR in HBV-associated MVI-positive HCC patients. The C-indices of nomograms for predicting recurrence and OS were 0.722 and 0.759, respectively, for the training cohort with good predictive ability and better predictive ability than BCLC staging and CNLC staging.
Several preoperative high-risk indicators such as HBV-DNA and NLR have been found to be linked with reduced survival after LR (29–31). Li et al. observed that preoperative HBV-DNA > 2000 IU/ml was linked with a higher MVI incidence and a greater likelihood of early recurrence in HCC patients (28). Elevated NLR has also been shown to reduce the OS after LR in HCC patients (30). AFP, tumor diameter, and tumor number are well-known indicators affecting outcomes after LR for HCC and were included in several clinical guidelines (2, 22). Here, we also fully considered the effects of these factors.
Surgical margins are known to influence the prognosis of HCC after LR (23, 29, 32, 33). Portal vein infiltration and small metastatic nodules are usually seen within a 10-mm distance of the primary tumor and rarely at distances over 20 mm (34–36). Thus, a minimum resection margin of 10 mm is recommended. However, for tumors adjoining large blood vessels or in the presence of poor liver function, narrow resection may be a more appropriate surgical approach because it preserves more liver tissue and avoids damage to major blood vessels, but it also leads to a greater likelihood of recurrence and reduced survival. Yang et al. analyzed 929 patients with HBV-related MVI-positive HCC patients, including 545 patients with narrow margins and 545 patients with wide margins, the 5-year recurrence and OS rates were 71.1% vs. 85.9% and 44.9% vs. 25.0% for wide and narrow margin patients, respectively (both P<0.001) (29). In this article, it was also demonstrated that for HBV-related MVI-positive HCC patients, a wide margin surgical approach improves patient prognosis compared to a narrow margin.
There is no consensus on the use or type of adjuvant therapy for MVI-positive HCC. TACE involves the injection of embolic and chemotherapeutic drugs into arteries to decrease the tumor blood supply and induce ischemic necrosis. Recent studies have also shown that postoperative adjuvant TACE prolongs both recurrence-free survival (RFS) and OS in patients with HCC, especially in MVI-positive patients (37–39). The randomized clinical trial by Wei et al. included 250 patients with MVI-positive HCC, including 125 each with and without postoperative adjuvant TACE, respectively, observing that the postoperative TACE markedly increased both RFS and OS in MVI-positive patients (39). In this paper, 342 of 795 patients were treated with postoperative adjuvant TACE, and the multivariate analysis also indicated that postoperative adjuvant TACE treatment was a protective factor for recurrence and OS, confirming the previous study.
There are several limitations to this study. First, the study was conducted at a single institution and needs confirmation by multicenter results. Second, the nomograms are specific for HBV-infected HCC patients and are not applicable to patients with HCC due to other etiologies. Third, we did not exclude patients with HBV who also had other etiologies such as alcoholism or fatty liver, etc., this may have a certain impact on the research results. Lastly, the study is retrospective, leading to inevitable issues in selection bias and bias from incomplete adherence to the post-operative follow-up protocol.
In summary, we developed and validated nomograms for predicting one-, three-, and five-year recurrence and OS in HBV-associated MVI-positive HCC. The nomograms were found to have good predictive ability and could accurately differentiate between patients differing in recurrence and survival risk. It is recommended that close monitoring together with adjuvant therapy be used for patients at risk of tumor recurrence following surgery.
The data that support the findings of this study are available from the corresponding author upon reasonable request. Requests to access these datasets should be directed to Shilei Bai, NTA0NzM5NDI2QHFxLmNvbQ==.
The studies involving human participants were reviewed and approved by Eastern Hepatobiliary Surgery Hospital ethics committee. The patients/participants provided their written informed consent to participate in this study.
Study concept and design: SB, PY, YW, YT and KW. Acquisition, analysis, or interpretation of data: SB, AS, PY and FS. Statistical analysis: SB, JW, CL, YX. Critical revision of the manuscript for important intellectual content: YT and KW. All authors contributed to the article and approved the submitted version.
The Clinical Research Plan for SHDC (SHDC2020CR2038B); The Explorer Program of Shanghai Scientific and Technological Committee (21TS1400500). Star Cultivation Project of Science and Technology Innovation Action Plan in Shanghai 2022(Yangfan: 22YF1459000); Youth Cultivation Program of Chinese National Natural Science Foundation(2021GZR002). Fund of Science and Technology Commission of Shanghai Municipality (20JC1419400).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1166327/full#supplementary-material
Supplementary Figure 1 | Flow Chart of patient’s inclusion.
Supplementary Figure 2 | Postoperative recurrence (A) and OS (B) in the training and validation cohorts.
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin (2015) 65:87–108. doi: 10.3322/caac.21262
2. EASL Clinical Practice Guidelines. Management of hepatocellular carcinoma. J Hepatol (2018) 69:182–236. doi: 10.1016/j.jhep.2018.03.019
3. Lim KC, Chow PK, Allen JC, Chia GS, Lim M, Cheow PC, et al. Microvascular invasion is a better predictor of tumor recurrence and overall survival following surgical resection for hepatocellular carcinoma compared to the Milan criteria. Ann Surg (2011) 254:108–13. doi: 10.1097/SLA.0b013e31821ad884
4. Erstad DJ, Tanabe KK. Prognostic and therapeutic implications of microvascular invasion in hepatocellular carcinoma. Ann Surg Oncol (2019) 26:1474–93. doi: 10.1245/s10434-019-07227-9
5. Zhang X, Li J, Shen F, Lau WY. Significance of presence of microvascular invasion in specimens obtained after surgical treatment of hepatocellular carcinoma. J Gastroenterol Hepatol (2018) 33:347–54. doi: 10.1111/jgh.13843
6. Rodríguez-Perálvarez M, Luong TV, Andreana L, Meyer T, Dhillon AP, Burroughs AK. A systematic review of microvascular invasion in hepatocellular carcinoma: Diagnostic and prognostic variability. Ann Surg Oncol (2013) 20:325–39. doi: 10.1245/s10434-012-2513-1
7. Yang T, Lu JH, Zhai J, Lin C, Yang GS, Zhao RH, et al. High viral load is associated with poor overall and recurrence-free survival of hepatitis b virus-related hepatocellular carcinoma after curative resection: a prospective cohort study. Eur J Surg Oncol (2012) 38:683–91. doi: 10.1016/j.ejso.2012.04.010
8. Utsunomiya T, Shimada M, Kudo M, Ichida T, Matsui O, Izumi N, et al. A comparison of the surgical outcomes among patients with HBV-positive, HCV-positive, and non-b non-c hepatocellular carcinoma: a nationwide study of 11,950 patients. Ann Surg (2015) 261:513–20. doi: 10.1097/SLA.0000000000000821
9. Takeishi K, Maeda T, Shirabe K, Tsujita E, Yamashita Y, Harimoto N, et al. Clinicopathologic features and outcomes of non-b, non-c hepatocellular carcinoma after hepatectomy. Ann Surg Oncol (2015) 22 Suppl 3:S1116–24. doi: 10.1245/s10434-015-4728-4
10. Ryu SH, Chung YH, Lee H, Kim JA, Shin HD, Min HJ, et al. Metastatic tumor antigen 1 is closely associated with frequent postoperative recurrence and poor survival in patients with hepatocellular carcinoma. Hepatology (2008) 47:929–36. doi: 10.1002/hep.22124
11. Bui-Nguyen TM, Pakala SB, Sirigiri RD, Xia W, Hung MC, Sarin SK, et al. NF-kappaB signaling mediates the induction of MTA1 by hepatitis b virus transactivator protein HBx. Oncogene (2010) 29:1179–89. doi: 10.1038/onc.2009.404
12. Faria SC, Szklaruk J, Kaseb AO, Hassabo HM, Elsayes KM. TNM/Okuda/Barcelona/UNOS/CLIP international multidisciplinary classification of hepatocellular carcinoma: concepts, perspectives, and radiologic implications. Abdom Imaging (2014) 39:1070–87. doi: 10.1007/s00261-014-0130-0
13. Xie DY, Ren ZG, Zhou J, Fan J, Gao Q. 2019 Chinese Clinical guidelines for the management of hepatocellular carcinoma: updates and insights. Hepatobiliary Surg Nutr (2020) 9:452–63. doi: 10.21037/hbsn-20-480
14. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol (2015) 16:e173–80. doi: 10.1016/S1470-2045(14)71116-7
15. Wu J, Zhang H, Li L, Hu M, Chen L, Xu B, et al. A nomogram for predicting overall survival in patients with low-grade endometrial stromal sarcoma: a population-based analysis. Cancer Commun (Lond) (2020) 40:301–12. doi: 10.1002/cac2.12067
16. Choi SY, Kim JH, Lim S, Lee JE, Park HJ, Lee B, et al. CT-based nomogram for predicting survival after R0 resection in patients with gallbladder cancer: a retrospective multicenter analysis. Eur Radiol (2021) 31:3336–46. doi: 10.1007/s00330-020-07402-7
17. Chen D, Liu Z, Liu W, Fu M, Jiang W, Xu S, et al. Predicting postoperative peritoneal metastasis in gastric cancer with serosal invasion using a collagen nomogram. Nat Commun (2021) 12:179. doi: 10.1038/s41467-020-20429-0
18. Hiremath A, Shiradkar R, Fu P, Mahran A, Rastinehad AR, Tewari A, et al. An integrated nomogram combining deep learning, prostate imaging-reporting and data system (PI-RADS) scoring, and clinical variables for identification of clinically significant prostate cancer on biparametric MRI: a retrospective multicentre study. Lancet Digit Health (2021) 3:e445–e54. doi: 10.1016/S2589-7500(21)00082-0
19. Lei Z, Li J, Wu D, Xia Y, Wang Q, Si A, et al. Nomogram for preoperative estimation of microvascular invasion risk in hepatitis b virus-related hepatocellular carcinoma within the Milan criteria. JAMA Surg (2016) 151:356–63. doi: 10.1001/jamasurg.2015.4257
20. Long J, Wang A, Bai Y, Lin J, Yang X, Wang D, et al. Development and validation of a TP53-associated immune prognostic model for hepatocellular carcinoma. EBioMed (2019) 42:363–74. doi: 10.1016/j.ebiom.2019.03.022
21. Huo TI, Liu PH, Hsu CY. Nomogram to predict surgical hepatocellular carcinoma with child-pugh b: feasibility and overlooked predictors. J Hepatol (2020) 72:1032–3. doi: 10.1016/j.jhep.2019.12.024
22. Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatol (2005) 42:1208–36. doi: 10.1002/hep.20933
23. Shi M, Guo RP, Lin XJ, Zhang YQ, Chen MS, Zhang CQ, et al. Partial hepatectomy with wide versus narrow resection margin for solitary hepatocellular carcinoma: a prospective randomized trial. Ann Surg (2007) 245:36–43. doi: 10.1097/01.sla.0000231758.07868.71
24. Poon RT, Fan ST, Ng IO, Wong J. Significance of resection margin in hepatectomy for hepatocellular carcinoma: a critical reappraisal. Ann Surg (2000) 231:544–51. doi: 10.1097/00000658-200004000-00014
25. Roayaie S, Blume IN, Thung SN, Guido M, Fiel MI, Hiotis S, et al. A system of classifying microvascular invasion to predict outcome after resection in patients with hepatocellular carcinoma. Gastroenterology (2009) 137:850–5. doi: 10.1053/j.gastro.2009.06.003
26. Zhou L, Rui JA, Ye DX, Wang SB, Chen SG, Qu Q. Edmondson-Steiner grading increases the predictive efficiency of TNM staging for long-term survival of patients with hepatocellular carcinoma after curative resection. World J Surg (2008) 32:1748–56. doi: 10.1007/s00268-008-9615-8
27. Camp RL, Dolled-Filhart M, Rimm DL. X-Tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res (2004) 10:7252–9. doi: 10.1158/1078-0432.CCR-04-0713
28. Li Z, Lei Z, Xia Y, Li J, Wang K, Zhang H, et al. Association of preoperative antiviral treatment with incidences of microvascular invasion and early tumor recurrence in hepatitis b virus-related hepatocellular carcinoma. JAMA Surg (2018) 153:e182721. doi: 10.1001/jamasurg.2018.2721
29. Yang P, Si A, Yang J, Cheng Z, Wang K, Li J, et al. A wide-margin liver resection improves long-term outcomes for patients with HBV-related hepatocellular carcinoma with microvascular invasion. Surg (2019) 165:721–30. doi: 10.1016/j.surg.2018.09.016
30. Johnson PJ, Dhanaraj S, Berhane S, Bonnett L, Ma YT. The prognostic and diagnostic significance of the neutrophil-to-lymphocyte ratio in hepatocellular carcinoma: a prospective controlled study. Br J Cancer (2021) 125:714–6. doi: 10.1038/s41416-021-01445-3
31. EASL. 2017 clinical practice guidelines on the management of hepatitis b virus infection. J Hepatol (2017) 67:370–98. doi: 10.1016/j.jhep.2017.03.021
32. Shi C, Zhao Q, Liao B, Dong Z, Wang C, Yang J, et al. Anatomic resection and wide resection margin play an important role in hepatectomy for hepatocellular carcinoma with peritumoural micrometastasis. ANZ J Surg (2019) 89:E482–e6. doi: 10.1111/ans.15396
33. Zhang EL, Cheng Q, Huang ZY, Dong W. Revisiting surgical strategies for hepatocellular carcinoma with microvascular invasion. Front Oncol (2021) 11:691354. doi: 10.3389/fonc.2021.691354
34. Nakashima Y, Nakashima O, Tanaka M, Okuda K, Nakashima M, Kojiro M. Portal vein invasion and intrahepatic micrometastasis in small hepatocellular carcinoma by gross type. Hepatol Res (2003) 26:142–7. doi: 10.1016/S1386-6346(03)00007-X
35. Shi M, Zhang CQ, Zhang YQ, Liang XM, Li J-Q, et al. Micrometastases of solitary hepatocellular carcinoma and appropriate resection margin. World J Surg (2004) 28:376–81. doi: 10.1007/s00268-003-7308-x
36. Sasaki A, Kai S, Iwashita Y, Liang XM, Li JQ. Microsatellite distribution and indication for locoregional therapy in small hepatocellular carcinoma. Cancer (2005) 103:299–306. doi: 10.1002/cncr.20798
37. Wang Z, Ren Z, Chen Y, Hu J, Yang G, Yu L, et al. Adjuvant transarterial chemoembolization for HBV-related hepatocellular carcinoma after resection: a randomized controlled study. Clin Cancer Res (2018) 24:2074–81. doi: 10.1158/1078-0432.CCR-17-2899
38. Liang L, Li C, Wang MD, Wang H, Zhou YH, Zeng YY, et al. Development and validation of a novel online calculator for estimating survival benefit of adjuvant transcatheter arterial chemoembolization in patients undergoing surgery for hepatocellular carcinoma. J Hematol Oncol (2021) 14:165. doi: 10.1186/s13045-021-01180-5
39. Wei W, Jian PE, Li SH, Guo ZX, Zhang YF, Ling YH, et al. Adjuvant transcatheter arterial chemoembolization after curative resection for hepatocellular carcinoma patients with solitary tumor and microvascular invasion: a randomized clinical trial of efficacy and safety. Cancer Commun (Lond) (2018) 38:61. doi: 10.1186/s40880-018-0331-y
Keywords: microvascular invasion, nomogram, hepatocellular carcinoma, prognosis, hepatitis B virus
Citation: Bai S, Yang P, Wei Y, Wang J, Lu C, Xia Y, Si A, Zhang B, Shen F, Tan Y and Wang K (2023) Development and validation of prognostic dynamic nomograms for hepatitis B Virus-related hepatocellular carcinoma with microvascular invasion after curative resection. Front. Oncol. 13:1166327. doi: 10.3389/fonc.2023.1166327
Received: 15 February 2023; Accepted: 05 April 2023;
Published: 19 April 2023.
Edited by:
Quirino Lai, Sapienza University of Rome, ItalyReviewed by:
Coskun Ozer Demirtas, Marmara University, TürkiyeCopyright © 2023 Bai, Yang, Wei, Wang, Lu, Xia, Si, Zhang, Shen, Tan and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kui Wang, d2FuZ2t1aXlrbEAxNjMuY29t; Yexiong Tan, eXh0YW4xMjE0QDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.