
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 05 May 2023
Sec. Pediatric Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1164949
This article is part of the Research Topic Safety consideration in the development of anti-tumor monoclonal antibodies during drug development View all 7 articles
 Amalia Varo1
Amalia Varo1 Alicia Castañeda1Saray Chamorro1Juan Pablo Muñoz1
Alicia Castañeda1Saray Chamorro1Juan Pablo Muñoz1 Maite Gorostegui1Mónica S. Celma2Sandra Lopez1
Maite Gorostegui1Mónica S. Celma2Sandra Lopez1 Margarida Simao1
Margarida Simao1 Sara Perez-Jaume1
Sara Perez-Jaume1 Jaume Mora1*
Jaume Mora1*Introduction: Anti-disialoganglioside 2 (anti-GD2) monoclonal antibodies (mAbs) are associated with Grade ≥3 (≥G3) adverse events (AEs) such as severe pain, hypotension, and bronchospasm. We developed a novel method of administering the GD2-binding mAb naxitamab, termed “Step-Up” infusion (STU), to reduce the risk of AEs of severe pain, hypotension, and bronchospasm.
Methods: Forty-two patients with GD2-positive tumors received naxitamab under “compassionate use” protocols and administered via either the standard infusion regimen (SIR) or the STU regimen. The SIR comprises a 60-min infusion of 3 mg/kg/day on Day 1 of cycle 1 and a 30- to 60-min infusion on Day 3 and Day 5, as tolerated. The STU regimen uses a 2-h infusion on Day 1, initiated at a rate of 0.06 mg/kg/h during 15 min (0.015 mg/kg) and which increases gradually to a cumulative dose of 3 mg/kg; on Days 3 and 5, the 3-mg/kg dose is initiated at 0.24 mg/kg/h (0.06 mg/kg) and delivered in 90 min according to the same gradual-increase strategy. AEs were graded according to Common Terminology Criteria for Adverse Events version 4.0.
Results: The frequency of infusions with an associated G3 AE was reduced from 8.1% (23/284 infusions) with SIR to 2.5% (5/202 infusions) with STU. The odds of an infusion being associated with a G3 AE reduced by 70.3% with STU vs. SIR (odds ratio: 0.297; p = 0.037). Mean serum naxitamab levels pre- and post-STU (11.46 µg/ml pre-infusion; 100.95 µg/ml post-infusion) were within the range reported for SIR.
Discussion: The comparable pharmacokinetics of naxitamab during SIR and STU may indicate that switching to STU reduces G3 AEs without impact on efficacy.
Anti-disialoganglioside 2 (anti-GD2) monoclonal antibodies (mAbs) are an important treatment modality for patients with high-risk neuroblastoma (HR-NB), both in the frontline setting and for those with refractory or relapsed (R/R) disease (1–5). Naxitamab (hu3F8) is a humanized mAb approved for use in combination with granulocyte-macrophage colony-stimulating factor (GM-CSF) in pediatric (age >1 year) and adult patients with R/R HR-NB in the bone and/or bone marrow (BM) and who have demonstrated a partial response (PR), minor response (MR), or stable disease (SD) following prior therapy (6). Accelerated approval was granted in November 2020 by the United States Food and Drug Administration. Naxitamab is administered without the need for overnight hospital stay (for the infusion) as a 30- to 60-min infusion (standard infusion regimen; SIR) on Days 1, 3, and 5 of each cycle (7, 8). This contrasts with treatment protocols for other approved anti-GD2 mAbs for HR-NB (dinutuximab and dinutuximab beta), which require longer infusion times: dinutuximab is administered over 10–20 h for four consecutive days; dinutuximab beta is administered over 8 h for 5 days, or via continuous infusion with a portable pump for 10 days (9, 10). Naxitamab is similar to other approved anti-GD2 mAbs in terms of type of associated adverse events (AEs), which primarily occur during the treatment infusion and include pain, hypotension, hypertension, and bronchospasm (9–14). Most patients treated with naxitamab experience mild-to-moderate AEs, which are defined as Common Terminology Criteria for Adverse Events (CTCAE) Grade 1 or 2 (G1, G2); however, many patients also experience severe AEs (mostly CTCAE Grade 3; G3).
During naxitamab SIR (used during Trial 201; NCT03363373), G3 pain was experienced by 54% of patients, G3 hypotension by 59% of patients, and G3 bronchospasm by 18% of patients (see Supplementary Table 1) (8). G3 AEs such as hypotension and bronchospasm are medically significant events that may complicate treatment or result in hospitalization. While G3 pain may not pose the same clinical risks, it is nonetheless challenging for clinicians to manage and distressing for patients and caregivers.
Naxitamab infusion-related severe hypotension and bronchospasm are usually manageable with the use of normal saline bolus and a β2 receptor agonist, respectively; however, infusion-rate reductions or pauses may also be helpful (11). Pre-hydration with normal saline is recommended in the Trial 201 protocol to mitigate the risk of severe hypotension. In addition, premedication with a corticosteroid on Cycle 1, Day 1 is recommended to reduce the risk of severe bronchospasm and other potential infusion-related reactions. Based on the observation that the intensity of anti-GD2 mAbs-induced reactions diminishes over subsequent infusions (tachyphylaxis), we developed a novel infusion regimen for naxitamab, termed the “Step-up” infusion (STU) regimen, established on a pharmacodynamically adaptive sigmoid curve administration of the drug. This regimen aims to reduce the likelihood of a G3 AE (such as severe hypotension or bronchospasm) occurring during infusion, while maintaining efficacy. STU, which is designed to deliver a cumulative dose (3 mg/kg/day) via a stepwise approach and using a slower initial infusion rate, aims to modulate the pharmacodynamics of naxitamab. Herein, we report on safety outcomes from patients treated with SIR and STU regimens at HSJD.
Patients with GD2-positive tumors (HR-NB, retinoblastoma, and osteosarcoma) were included in the analysis. Patients were either in complete remission (CR), or had HR-NB with residual disease in the bone and/or BM compartment following multimodal or salvage therapy (i.e., refractory or relapsed disease) and were ineligible for Trial 201 (Table 1). Patients received naxitamab and GM-CSF under compassionate use between 7 December 2020 and 28 December 2021. Patients were deemed eligible for immunotherapy with naxitamab if major organ toxicity was of CTCAE ≤G2. Informed written consent for treatments and tests were obtained according to HSJD institutional review board rules. Treatment was planned to be administered without the need for overnight hospital stay during the infusion.
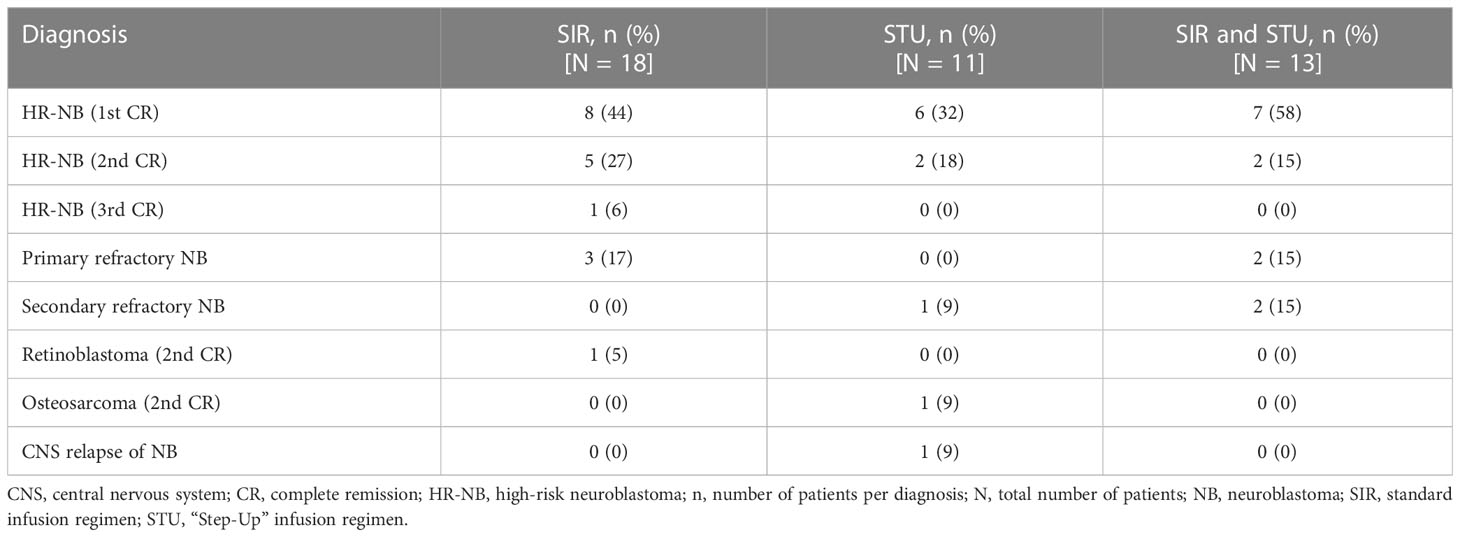
Table 1 Distribution of diagnoses per infusion administration cohort.
All patients were managed by the same team of nurses and physicians regardless of the infusion type. During the first half of the year 2021, infusions were administered following the SIR. While the STU was being developed, patients experiencing G3 AEs on the SIR were progressively moved to the STU and intrapatient comparisons were made for those having received both types of infusion. Over the course of the second half of the year, and given the improvements observed with the STU, patients’ infusions were progressively moved to the STU. As previously described (5), the infusion team consisted of three nurses: two to prepare the infusion suite before the patient arrived and to receive patients and families upon arrival, while the third nurse verified all the medications and doses, prepared the medications for each infusion, and ensured that the medications were available in the infusion suite. Throughout the infusions, two of the nurses were present at the patient’s bedside together with an infusion medical doctor. One nurse was responsible for the medication while the other nurse monitored vital signs and completed any registration paperwork. The third nurse remained outside the infusion suite and was responsible for post-naxitamab infusion patient monitoring/follow-up and for providing premedication to patients awaiting naxitamab infusion.
Per SIR protocols (as used in Trial 201), naxitamab was administered on Days 1, 3, and 5 of each treatment cycle at a dose of 3 mg/kg/day. The first infusion of naxitamab (Cycle 1, Day 1) was administered intravenously (i.v.) over 60 min; subsequent infusions were administered over 30–60 min, as tolerated.
Infusions following STU protocols were initiated at a rate of 0.06 mg/kg/h for 15 min (0.015 mg/kg) naxitamab on Day 1. The rate was then doubled every 15 min, delivering a total dose of 3 mg/kg over 120 min (Table 2). On Days 3 and 5 of naxitamab administration, STU was initiated at a higher rate (0.24 mg/kg/h [0.06 mg/kg]), before the rate was doubled every 15 min up to a maximum rate of 6 mg/kg/h, delivering a total dose of 3 mg/kg in 90 min (Table 2).
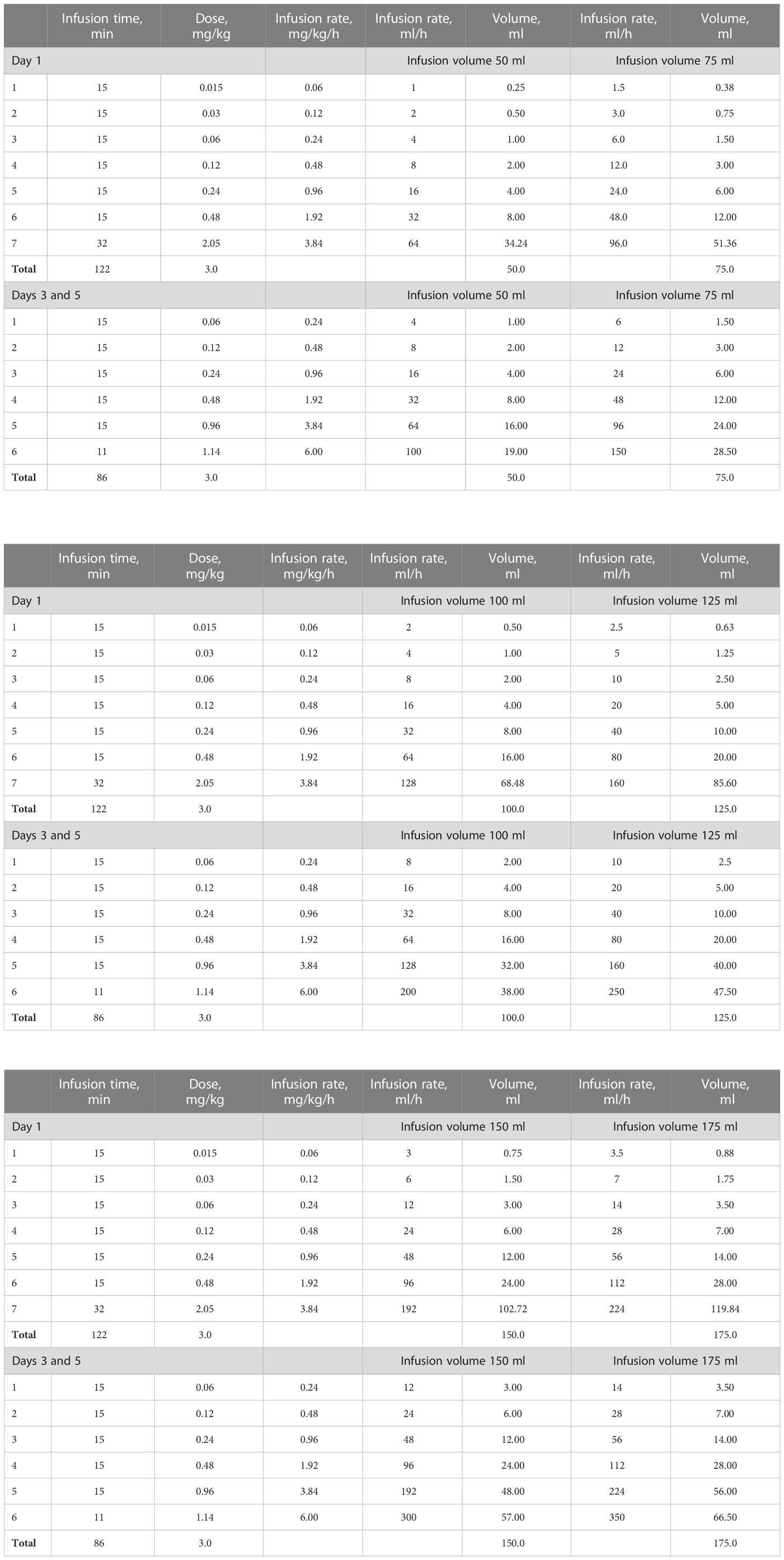
Table 2 “Step-Up” infusion regimen by infusion volume (50 ml, 75 ml, 100 ml, 125 ml, 150 ml, and 175 ml).
Naxitamab cycles started with subcutaneous (s.c.) GM-CSF for 5 days at 250 μg/m2/day before the first dose of naxitamab (Days −4 to 0); GM-CSF at 500 μg/m2/day s.c. was then administered on Days 1–5, with GM-CSF administered at least an hour before naxitamab on infusion days. GM-CSF was not given if the absolute neutrophil count was >20×109/L and/or white blood cell count was >50×109/L. Treatment cycles of 9 mg/kg total naxitamab dose were repeated every 4 weeks for up to 7 cycles.
Pharmacokinetics were studied by quantifying serum naxitamab concentrations by enzyme-linked immunosorbent assay (ELISA) as previously reported for the SIR (15). Naxitamab serum levels were measured immediately before and 5 min after the end of STU over multiple cycles. Comparison of reported SIR and newly acquired STU naxitamab serum levels using the same methodology was performed. Infusion-related AEs were graded according to CTCAE version 4 (16) and managed as reported (5, 11).
All patients, regardless of the infusion protocol, received the same premedication with paracetamol (15 mg/kg oral, 1,000 mg max), cetirizine (<20 kg body weight: 2.5 mg oral; ≥20 kg body weight: 5 mg oral; age >12 years and >30 kg body weight: 10 mg oral), ranitidine (i.v. 1 mg/kg, 50 mg max), which was later changed to famotidine (0.5 mg/kg oral, 40 mg max) due to availability issues, and ondansetron (i.v. 0.15 mg/kg, 8 mg max) 30 min prior to the start the infusion. All patients on Cycle 1, Day 1 received methylprednisolone (i.v. 2 mg/kg; 80 mg max) per the standard Trial 201 protocol. For each infusion, patients followed pain management according to either regimen 1 (opioids only) or regimen 2 (ketamine-based) as described below:
Opioids only. Both SIR and STU: morphine chloride (i.v. 50 µg/kg, 4 mg max) 5 min before infusion and during infusion, if needed, for breakthrough pain.
Ketamine only. Approach differed slightly for SIR vs. STU. Initial combination for both was ketamine (i.v. 0.5–1 mg/kg) in combination with midazolam (i.v. 0.05 mg/kg, 2 mg max), atropine (i.v. 0.005 mg/kg, 0.6 mg max), and lidocaine (i.v. 2 mg/kg)—for SIR, this was given as premedication 3–5 min before the infusion, whereas for STU, it was given as supportive therapy when the first signs of pain appeared. For SIR, a second bolus of ketamine (dose as before) and lidocaine (1 mg/kg) was administered 15 min into the infusion. In both regimens, additional doses of ketamine (same dose, up to a total of 4 mg/kg) were administered as needed for breakthrough pain; in the STU group, this was supplemented by lidocaine (1 mg/kg, >15 min after the last dose) or midazolam (i.v. 0.05 mg/kg; total max of 4 mg), as required.
In this study, most patients began naxitamab treatment with STU, or switched to STU, after the ketamine-based regimen was established as the preferred pain management strategy for naxitamab infusions at HSJD. Therefore, most patients following STU protocols were given ketamine during infusions. All patients, regardless of pain-management regimen or infusion protocol, received dexketoprofen (1 mg/kg oral, 50 mg max) or metamizole (i.v. 20–30 mg/kg, 2,000 mg max) at the end of naxitamab infusion, if needed.
A logistic mixed model (estimated using maximum likelihood) was fit using the R (17) and lme4 (18) software packages to analyze the relationship between the type of infusion (SIR vs. STU) and the occurrence of G3 AEs. The model included individual and cycle number as random effects, and type of infusion (SIR vs. STU) as a fixed effect; odds ratios were derived from this model. The Wald approximation was used to compute 95% confidence intervals (CIs) and p-values (p-values <0.05 were considered statistically significant).
Forty-two patients with GD2-positive tumors (HR-NB: n = 40; retinoblastoma: n = 1; osteosarcoma: n = 1) were treated with naxitamab (Table 1); 24 patients completed planned 5 cycles, 2 patients completed 7 cycles, and 16 patients received less than 5 cycles. Of these 42 patients, 18 followed SIR infusion protocols exclusively, 11 followed STU protocols exclusively, and 13 followed a mixture of both SIR and STU protocols. For patients who followed both SIR and STU protocols, most began naxitamab treatment with SIR and switched to STU for subsequent cycles as a strategy for mitigating severe AEs. However, seven patients were required to switch from STU to SIR for logistical reasons (not enough space for long infusions in the day hospital area).
A total of 486 naxitamab infusions were completed, 284 (58%) following SIR protocols and 202 (42%) following STU protocols. SIR was used for 73 infusions in Cycle 1 (25%), 71 in Cycle 2 (24%), 50 in Cycle 3 (18%), 45 in Cycle 4 (15%), 39 in Cycle 5 (13%), 3 in Cycle 6 (1%), and 3 in Cycle 7 (1%). STU was used for 47 (23%) infusions in Cycle 1, 40 (20%) in Cycle 2, 43 (21%) in Cycle 3, 33 (16%) in Cycle 4, 33 (16%) in Cycle 5, 3 (1.5%) in Cycle 6, and 3 (1.5%) in Cycle 7. Opioids were administered during 196 (69%) infusions that followed SIR protocols and 21 (10%) that followed STU protocols. Ketamine was administered during 88 (31%) infusions that followed SIR protocols and 181 (90%) that followed STU protocols.
All patients experienced at least one G1 or G2 AE during naxitamab infusion; 19 (45%) patients experienced at least one G3 AE. Of those patients who experienced at least one G3 AE, eight (42%) were following SIR protocols exclusively, two (11%) were following STU protocols exclusively, and nine (47%) were following both SIR and STU protocols. Of the nine patients following both protocols and who experienced at least one G3 AE, six (67%) experienced the G3 AE(s) during SIR, one (11%) experienced the G3 AE(s) during STU, and two (22%) experienced the G3 AE(s) during both SIR and STU.
A total of 23 episodes of G3 AEs occurred during SIR infusions, whereas a total of 5 episodes of G3 AEs occurred during STU infusions; G3 AEs were hypotension, hypertension, laryngospasm, bronchospasm, apnea, pain, and anaphylaxis (Table 3). Some patients experienced several G3 episodes during each cycle (three infusions/cycle) given either as SIR or STU. Seven patients experienced G3 hypotension episodes during SIR (37%) vs. two during STU (11%), and six patients experienced G3 hypertension episodes during SIR (32%) vs. two during STU (11%); no patients experienced both hypotension and hypertension at the same episode. Severe upper-airway compromise in the form of laryngospasm or bronchospasm episodes occurred in four patients each (21%; during SIR only), whereas apnea occurred in two patients (11%; one during SIR and one during STU), pain occurred in one patient (5%; during STU), and anaphylaxis occurred in one patient (5%; during SIR). None of the G3 AEs were life threatening or required hospitalization, irrespective of infusion regimen.
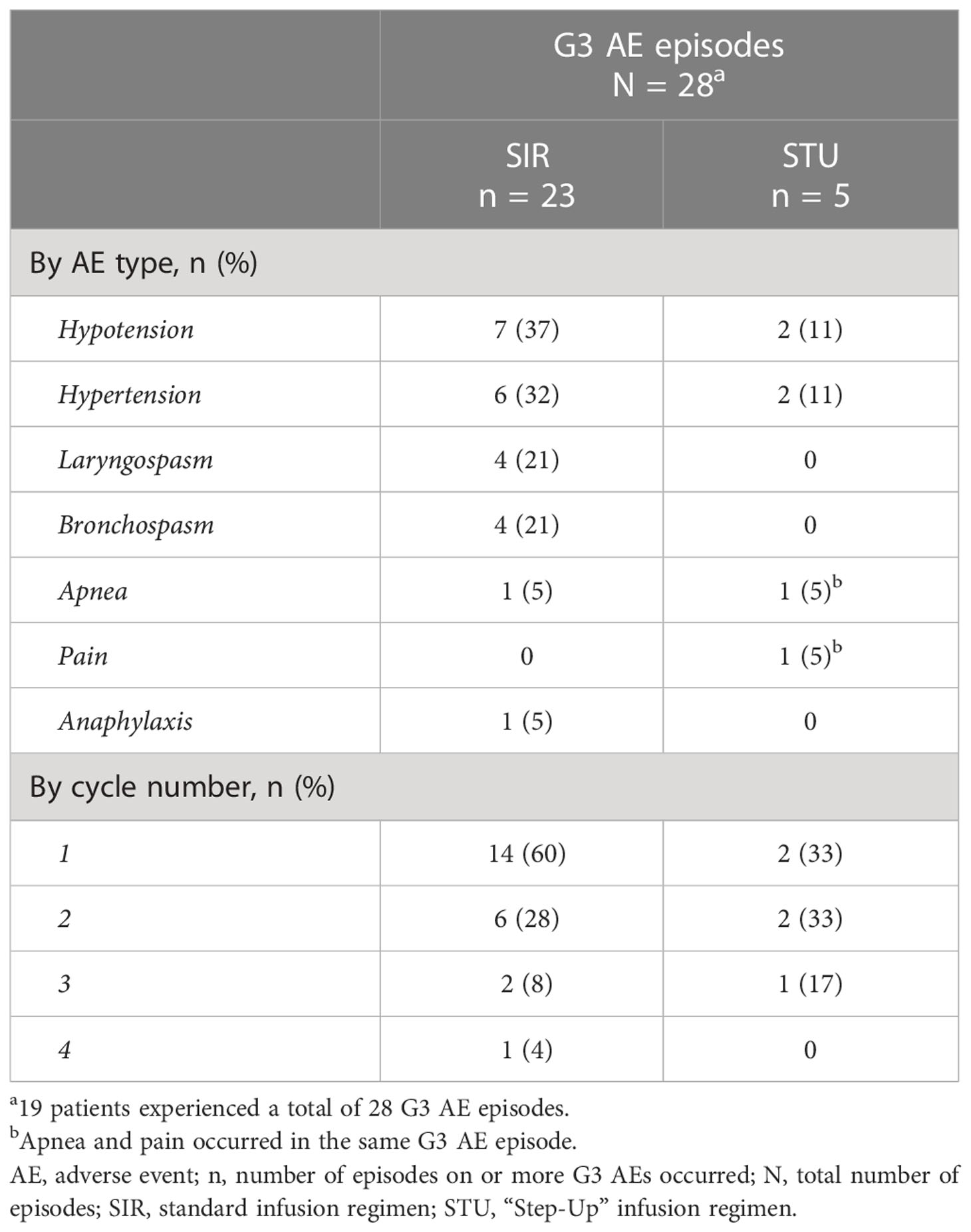
Table 3 Number of G3 AEs occurring during SIR and STU infusions by AE type and by cycle number.
Thirty-one G3 AEs were reported across both infusion protocols from the total of 486 infusions; these AEs occurred during 28 infusions, giving an overall G3 AE frequency of ~6%. When naxitamab infusion was administered per SIR protocols, 25 G3 AEs occurred during 23 of 284 infusions, giving a G3 AE frequency of 8.1% for SIR. A lower frequency was observed for STU protocols, with a G3 AE reported in 5 of 202 infusions (giving a frequency of 2.5%; 1 infusion had two G3 AEs recorded at the same time, pain and apnea). The association of the type of infusion with the occurrence of a G3 adverse event was statistically significant (p = 0.037); the odds ratio for STU vs. SIR infusion was 0.297 (95% CI 0.095–0.929), representing a 70.3% reduction in the likelihood of a G3 AE with STU vs. SIR.
When considering AEs by infusion cycle, the majority of G3 AEs occurred during Cycle 1, with a decrease over subsequent cycles. For SIR protocols: 14 G3 AEs (60% of the total) occurred during Cycle 1, 6 (28%) occurred during Cycle 2, 2 (8%) occurred during Cycle 3, and 1 (4%) occurred during Cycle 4; there were no G3 AEs in subsequent cycles. However, for STU, the occurrence of G3 AEs during infusion did not appear to decrease over subsequent cycles: two (33%) G3 AEs occurred during Cycle 1, two (33%) occurred during Cycle 2, and one (17%) occurred during Cycle 3.
Naxitamab pharmacokinetics have been well described following SIR protocols (15). In order to investigate whether the STU regimen may interfere with drug distribution, we systematically collected serum to determine naxitamab levels pre- and post-infusion for all STU infusions. Examples from samples obtained from 12 patients over multiple cycles of STU pre- and post-infusion serum levels are shown in Figure 1. Overall, the average pre- and post-infusion serum naxitamab levels were 11.46 µg/ml and 100.95 µg/ml, respectively. No correlation with patient body weight was found. Post-infusion levels are within the same range (88–114 μg/ml) as those reported in the phase 1 Trial 12-230 study (NCT01757626; SIR only; 87.99 µg/ml at a total dose of 3.0 mg/kg) (15).

Figure 1 Pharmacokinetics of naxitamab on the “Step-Up” infusion protocol.
A reduction in the occurrence of G3 AEs when naxitamab was administered per STU protocols permitted a decrease in the intensity of patient monitoring required. As previously reported, with the SIR protocol, two nurses were required at the patient’s bedside together with the infusion physician (5). With the decrease in severity of the infusion-related reactions seen with STU protocols, only one bedside nurse was required, and a physician was no longer required to stay at the bedside. Pain management was still required during STU.
The data presented in this analysis is based on patients treated with naxitamab under compassionate use at HSJD managed and assessed by the same team accustomed to evaluating naxitamab-related AEs. In the current study, STU (vs. SIR) protocols reduced the odds of G3 AEs occurring during infusion by 70.3% in patients with anti-GD2 positive tumors and who were in CR, and in patients with HR-NB with residual disease limited to the bone and/or BM following multimodal or salvage therapy (i.e., refractory or relapsed disease).
A similar approach to the STU regimen has been developed for bispecific antibodies like blinatumomab to prevent severe toxicities like the Cytokine Release Syndrome. The severe toxicity induced by blinatumomab has been mitigated by the administration of a stepwise dosing approach (19). By exposing the patient to a lower dose of naxitamab at the start of the infusion, STU has the potential to modify the pharmacodynamics of naxitamab, which may reduce associated toxicity. However, pain remains to be a notable AE and requires pre-medication and AE management during naxitamab infusion. Previous phase 1 studies (15, 20) have demonstrated a strong correlation between the peak serum concentration and area under the serum concentration time curve, which are measures of drug exposure over time and a critical determinant of mAb antitumor effect. Peak serum concentration of naxitamab is reached for an average of 5 min post-infusion (15). As naxitamab serum levels post-infusion for STU were similar to those previously reported during phase 1 studies using SIR protocols (15), drug exposure and antitumor effects should not be negatively affected by STU administration. This suggests that STU administration can reduce toxicity during naxitamab infusions without compromising efficacy.
As opioids can exacerbate hypotension, the type and timing of medication administered to manage pain (opioids only or a ketamine-based regimen) should be considered. Opioids are recommended for managing pain associated with naxitamab infusion (6) and are given to most patients treated using SIR protocols. The potential hypotensive effects of opioids may have contributed to the increased number of hypotension events seen in patients following SIR protocols vs. STU (seven for SIR vs. two for STU). Therefore, patients may have a lower risk of G3 hypotension when following STU protocols, partially due to following a ketamine-based regimen for pain management. However, it is also possible that the onset of hypotension may be slower with STU vs. SIR, allowing staff to prevent G1 or G2 hypotension from progressing to G3.
A physician and two nurses are normally required at the bedside for SIR, whereas only one nurse is required for STU. STU provides a clinically meaningful impact by reducing staffing needs vs. SIR. Furthermore, like SIR, STU has a short infusion time (1.5–2 h), allowing for treatment without the need for overnight hospital stay, providing convenience for patients and families.
In conclusion, STU naxitamab administration represents a novel way to deliver naxitamab treatment that may have the potential to reduce the likelihood of G3 AEs occurring during infusion. As the current analysis is retrospective, a prospective study is needed to establish whether STU protocols can deliver an improved AE profile for naxitamab vs. SIR. Establishing STU as the preferred method for naxitamab administration could optimize patient care and reduce both the care load for clinicians and staffing requirements for institutions.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Hospital Sant Joan de Deu. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Conceptualization: JM. Data curation: AV and SP-J. Formal analysis: SP-J and JM. Funding acquisition: JM. Methodology: SC, JPM, AC, MG, MC, SL, and MS. Project administration: JM. Resources: JM. Software: SP-J. Supervision: JM. Validation: all authors. Writing—original draft: JM. Writing—review and editing: all authors. All authors contributed to the article and approved the submitted version.
We want to acknowledge Dr. Nai-Kong Cheung of Memorial Sloan Kettering Cancer Center who suggested the concept of step-up dosing based on his insights into the kinetics of pain from anti-GD2 antibodies. We also want to thank Dr. Irene Cheung for the measurement of serum naxitamab levels. We acknowledge the Neuroblastoma Immunotherapy Team of nurses and supportive personnel at PCCB. We are grateful to the Band of Parents at Hospital Sant Joan de Déu for supporting the overall research activities of the developmental tumor laboratory, PCCB.
The authors declare that this study received funding from Ymabs therapeutics. The funder had the following involvement in the study: editorial and writing.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1164949/full#supplementary-material
1. Cheung NK, Lazarus H, Miraldi FD, Abramowsky CR, Kallick S, Saarinen UM, et al. Ganglioside GD2 specific monoclonal antibody 3F8: a phase I study in patients with neuroblastoma and malignant melanoma. J Clin Oncol (1987) 5(9):1430–40. doi: 10.1200/JCO.1987.5.9.1430
2. Modak S, Cheung NKV. Disialoganglioside directed immunotherapy of neuroblastoma. Cancer Invest (2007) 25:67–77. doi: 10.1080/07357900601130763
3. Yu AL, Gilman AL, Ozkaynak MF, London WB, Kreissman SG, Chen HX, et al. Anti-GD2 antibody with GM-CSF, interleukin-2 and isotretinoin for neuroblastoma. N Engl J Med (2010) 363(14):1324–34. doi: 10.1056/NEJMoa0911123
4. Mody R, Naranjo A, Van Ryn C, Yu AL, London WB, Shulkin BL, et al. Irinotecan–temozolomide with temsirolimus or dinutuximab in children with refractory or relapsed neuroblastoma (COG ANBL1221): an open-label, randomised, phase 2 trial. Lancet Oncol (2017) 18:946–57. doi: 10.1016/s1470-2045(17)30355-8
5. Castañeda A, Gorostegui M, Miralles SL, Chamizo A, Patiño SC, Flores MA, et al. How we approach the treatment of patients with high-risk neuroblastoma with naxitamab: experience from the hospital sant Joan de déu in Barcelona, Spain. ESMO Open (2022) 7(2):100462. doi: 10.1016/j.esmoop.2022.100462
6. Danyelza (naxitamab-gqgk) injection, for intravenous use prescribing information (2020). Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/761171lbl.pdf.
7. Morgenstern DA, Mora J, Chan GC, Nysom K, Bear M, Worsaae Dalby L, et al. 74P – pivotal trial 201 data on outpatient administration of naxitamab (Hu3F8), a humanized GD2 targeted immunotherapy for the treatment of refractory/relapsed (R/R) high-risk (HR) neuroblastoma (NB). Ann Oncol (2020) 31(Suppl 7):S1448. doi: 10.1016/j.annonc.2020.10.562
8. Mora J, Chan GC, Morgenstern DA, Amoroso L, Nysom K, Faber J, et al. 891P – naxitamab treatment for relapsed or refractory high-risk neuroblastoma: outcomes from the first prespecified analyses of the pivotal 201 trial. Ann Oncol (2022) 33(suppl 7):S956. doi: 10.1016/j.annonc.2022.07.1017
9. Unituxin (dinutuximab) injection, for intravenous use prescribing information (2020). Available at: https://unituxin.com/full-prescribing-information.pdf.
10. Qarziba (dinutuximab beta) summary of product characteristics (2020). Available at: https://www.ema.europa.eu/en/documents/product-information/qarziba-epar-product-information_en.pdf.
11. Mora J, Chan GC, Morgenstern DA, Bear MK, Tornøe K, Kushner BH. Outpatient administration of naxitamab in combination with granulocyte-macrophage colony-stimulating factor in patients with refractory and/or relapsed high-risk neuroblastoma: management of adverse events. Cancer Rep (Hoboken) (2022) 6:e1627. doi: 10.1002/cnr2.1627
12. Kushner BH, Cheung IY, Modak S, Basu EM, Roberts SS, Cheung NK. Humanized 3F8 anti-GD2 monoclonal antibody dosing with granulocyte-macrophage colony-stimulating factor in patients with resistant neuroblastoma: a phase 1 clinical trial. JAMA Oncol (2018) 4:1729–35. doi: 10.1001/jamaoncol.2018.4005
13. Ladenstein RL, Pötschger U, Valteau-Couanet D, Luksch R, Castel V, Yaniv I, et al. Interleukin 2 with anti-GD2 antibody ch14.18/CHO (dinutuximab beta) in patients with high-risk neuroblastoma (HR-NBL1/SIOPEN): a multicentre, randomised, phase 3 trial. Lancet Oncol (2018) 19:1617–29. doi: 10.1016/S1470-2045(18)30578–3
14. Barone G, Barry A, Bautista F, Brichard B, Defachelles A-S, Herd F, et al. Managing adverse events associated with dinutuximab beta treatment in patients with high-risk neuroblastoma: practical guidance. Paediatr Drugs (2021) 23:537–48.
15. Cheung IY, Kushner BH, Modak S, Basu EM, Roberts SS, Cheung NV. Phase I trial of anti-GD2 monoclonal antibody hu3F8 plus GM-CSF: impact of body weight, immunogenicity and anti-GD2 response on pharmacokinetics and survival. Oncoimmunology (2017) 6(11):e1358331. doi: 10.1080/2162402X.2017.1358331
16. National Cancer Institute. Common terminology criteria for adverse events (CTCAE), version 5.0 (2017). Available at: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf.
17. R Core Team. R: a language and environment for statistical computing (2022). Vienna, Austria: R Foundation for Statistical Computing. Available at: https://www.R-project.org/ (Accessed Feb, 2023).
18. Bates D, Maechler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Soft (2015) 67(1):1–48. doi: 10.18637/jss.v067.i01
19. Baumeister SHC, Mohan GS, Elhaddad A, Lehmann L. Cytokine release syndrome and associated acute toxicities in pediatric patients undergoing immune effector cell therapy or hematopoietic cell transplantation. Front Oncol (2022) 12:841117. doi: 10.3389/fonc.2022.841117
Keywords: neuroblastoma, immunotherapy, adverse events, GD2 monoclonal antibody, naxitamab, pharmacokinetics, pharmacodynamics
Citation: Varo A, Castañeda A, Chamorro S, Muñoz JP, Gorostegui M, Celma MS, Lopez S, Simao M, Perez-Jaume S and Mora J (2023) Novel infusion strategy reduces severe adverse events caused by the anti-GD2 monoclonal antibody naxitamab. Front. Oncol. 13:1164949. doi: 10.3389/fonc.2023.1164949
Received: 13 February 2023; Accepted: 12 April 2023;
Published: 05 May 2023.
Edited by:
Sergi Aranda, Center for Genomic Regulation (CRG), SpainReviewed by:
Shinya Suzuki, National Cancer Center Hospital East, JapanCopyright © 2023 Varo, Castañeda, Chamorro, Muñoz, Gorostegui, Celma, Lopez, Simao, Perez-Jaume and Mora. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jaume Mora, amF1bWUubW9yYUBzamQuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.