 Víctor Albarrán*
Víctor Albarrán* Jesús Chamorro
Jesús Chamorro Javier Pozas
Javier Pozas María San Román
María San Román Diana Isabel Rosero
Diana Isabel Rosero Cristina SaavedraMaría Gion
Cristina SaavedraMaría Gion Alfonso CortésElena EscaleraEva GuerraElena López Miranda
Alfonso CortésElena EscaleraEva GuerraElena López Miranda María Fernández Abad
María Fernández Abad Noelia Martínez Jañez
Noelia Martínez Jañez- Medical Oncology Department, Ramon y Cajal University Hospital, Madrid, Spain
PARP inhibitors are progressively becoming a part of our therapeutic arsenal against BRCA-defective tumors, because of their capacity to induce synthetic lethality in cells with a deficiency in the homologous recombination repair system. Olaparib and talazoparib have been approved for metastatic breast cancer in carriers of germline BRCA mutations, which are found in approximately 6% of patients with breast cancer. We report the case of a patient with metastatic breast cancer, carrier of a germline mutation in BRCA2, with a complete response to first-line treatment with talazoparib, maintained after 6 years. To the best of our knowledge, this is the longest response reported with a PARP inhibitor in a BRCA-mutated tumor. We have made a review of literature, regarding the rationale for PARP inhibitors in carriers of BRCA mutations and their clinical relevance in the management of advanced breast cancer, as well as their emerging role in early stage disease, alone and in combination with other systemic therapies.
1 Introduction
Breast cancer (BC) accounts for approximately 30% of malignancies in women worldwide (1), with an incidence ranging from 27 in 100000 (Africa and East Asia) to 97 in 100000 (North America and Western Europe), reflecting its association with lifestyle and social factors (2). Metastatic BC remains a virtually incurable disease and is still the leading cause of cancer-related death in women globally (3), though the prognosis of this condition has been improved by the incorporation of novel therapies beyond conventional chemotherapy (CT).
Around 10% of malignant breast tumors are associated with a genetic predisposition (3). Although several breast cancer susceptibility genes have been identified, the most common germline mutations that lead to a family history of BC affect BRCA1 and BRCA2. Pathogenic variants in these genes are associated with an increased risk of several tumors, being the strongest hereditary risk factors for breast and ovarian cancers. A contemporary prospective cohort study with 9856 carriers of pathogenic BRCA variants, reported a cumulative BC risk to 80 years of 72% in BRCA1 mutation carriers (95% confidence interval [CI] 65-79%) and 69% in BRCA2 mutation carriers (95% CI 61-77%) (4). Germline BRCA2 mutation is more present in the ER+/HER2- population compared to BRCA1 (5).
The biological functions of BRCA1 and BRCA2 are related to the repair of DNA double-strand breaks (DSBs) by homologous recombination (HR), whereas PARP is an enzyme involved in base excision repair, which is key to repair of DNA single-strand breaks (SSBs). The blockade of PARP function causes an increase in SSBs, which are converted during cell replication to DSBs -usually repaired by HR-. In BRCA1/2 defective cells, the inhibition of PARP leads to the accumulation of DSBs that cannot be repaired due to a deficiency in the HR system, causing cell death, a phenomenon known as synthetic lethality. This is the biological rationale for the use of PARP inhibitors (PARPi) in BRCA-defective tumors.
BRCA1/2 mutations are classified as ESCAT I/OncoKb I actionable alterations. PARPi have been approved by the FDA for the treatment of four BRCA-associated tumors. In ovarian cancer, several drugs (olaparib, niraparib, rucaparib) have demonstrated clinical benefit both in recurrent tumors and as maintenance treatment after first-line CT in platinum-sensitive disease (6–12). In pancreatic and castrate-resistant prostate cancers, olaparib has been approved for patients with mutations in BRCA and other HR-related genes (13, 14).
In breast cancer, both olaparib and talazoparib have received FDA approval for carriers of BRCA mutations (pathogenic or likely pathogenic variants) with metastatic Her2-negative disease, based on the results from the OlympiAD (15) and EMBRACA (16) trials, respectively. In the phase III trial BROCADE-3 (17), addition of PARPi (veliparib) to an active platinum doublet (carboplatin/paclitaxel) resulted in significant improvement in progression-free survival (PFS) in patients with metastatic BC and germline BRCA mutations.
2 Case report
Our patient was a 38-year-old female, with no relevant previous medical history -except for mild bronchial asthma and chronic treatment with low-dose steroids, due to primary adrenal insufficiency-. Regarding family history, her mother had been diagnosed with breast cancer at 42 years of age, her father had been diagnosed with prostate cancer at 78 years, and her maternal aunt had been diagnosed with breast and ovarian cancer at 46 years.
In September 2014, the patient consulted for a palpable lesion, approximately 3 cm in size, in the inner upper quadrant of her right breast. Physical examination confirmed the lesion and did not reveal skin retraction, ulceration, tangible lymph nodes, or any other pathological findings. Mammogram, breast echography and breast magnetic resonance imaging (MRI) revealed the presence of a highly suspicious mass with irregular margins, with a maximum diameter of 32 mm, together with two satellite nodules approximately 8 mm in size. No pathological lymph nodes were identified.
A core needle biopsy was performed, which confirmed the diagnosis of multifocal infiltrating ductal carcinoma, with histologic grade 3 and a Ki67 proliferation index of 90%. Estrogen and progesterone receptor expression was detected in 70% and 15% of the cells, respectively. Immunohistochemical analysis revealed intense expression of E-cadherin and cytokeratin 19, with no Her2 overexpression (score 0+). Considering her family history and her age at diagnosis, the patient was referred to the hereditary cancer unit. She and her mother underwent a genetic study that revealed a pathogenic germline mutation in BRCA2.
In October 2014, she started neoadjuvant treatment with 5-fluorouracil, epirubicin and cyclophosphamide for 4 cycles (FEC scheme), followed by 8 cycles of weekly paclitaxel. In April 2015, she underwent bilateral mastectomy, with no relevant surgical complications. Histological examination of the surgical piece demonstrated pathological complete response [grade 5 of the Miller and Payne system (18)]. She started adjuvant hormone therapy with tamoxifen in May 2015 and began usual post-treatment surveillance. In January 2016, the patient underwent prophylactic bilateral oophorectomy after detailed genetic counseling.
In October 2016, she consulted with a rapidly growing lump on the right side of her head. A core needle biopsy was performed, demonstrating bone relapse of breast carcinoma, with positive expression of estrogen and progesterone receptors. The score for the immunohistochemical determination of Her2 was 2+, but gene amplification was discarded by fluorescence in situ hybridization (FISH).
Whole-body positron emission tomography with 18F-fluorodeoxyglucose (FDG-PET) revealed pathological deposits of radiotracer, with high metabolic activity, in the right frontal bone, corresponding with the biopsied lesion, the right acetabulum and the tenth right rib, all of which were suggestive of tumor viability (Figure 1), as well as two non-specific liver nodular lesions. Bone scintigraphy confirmed the bone metastases, and MRI confirmed the metastatic nature of the liver nodules. These findings led to a diagnosis of stage IV hormone-receptor (HR)+ breast cancer with bone and liver infiltration.
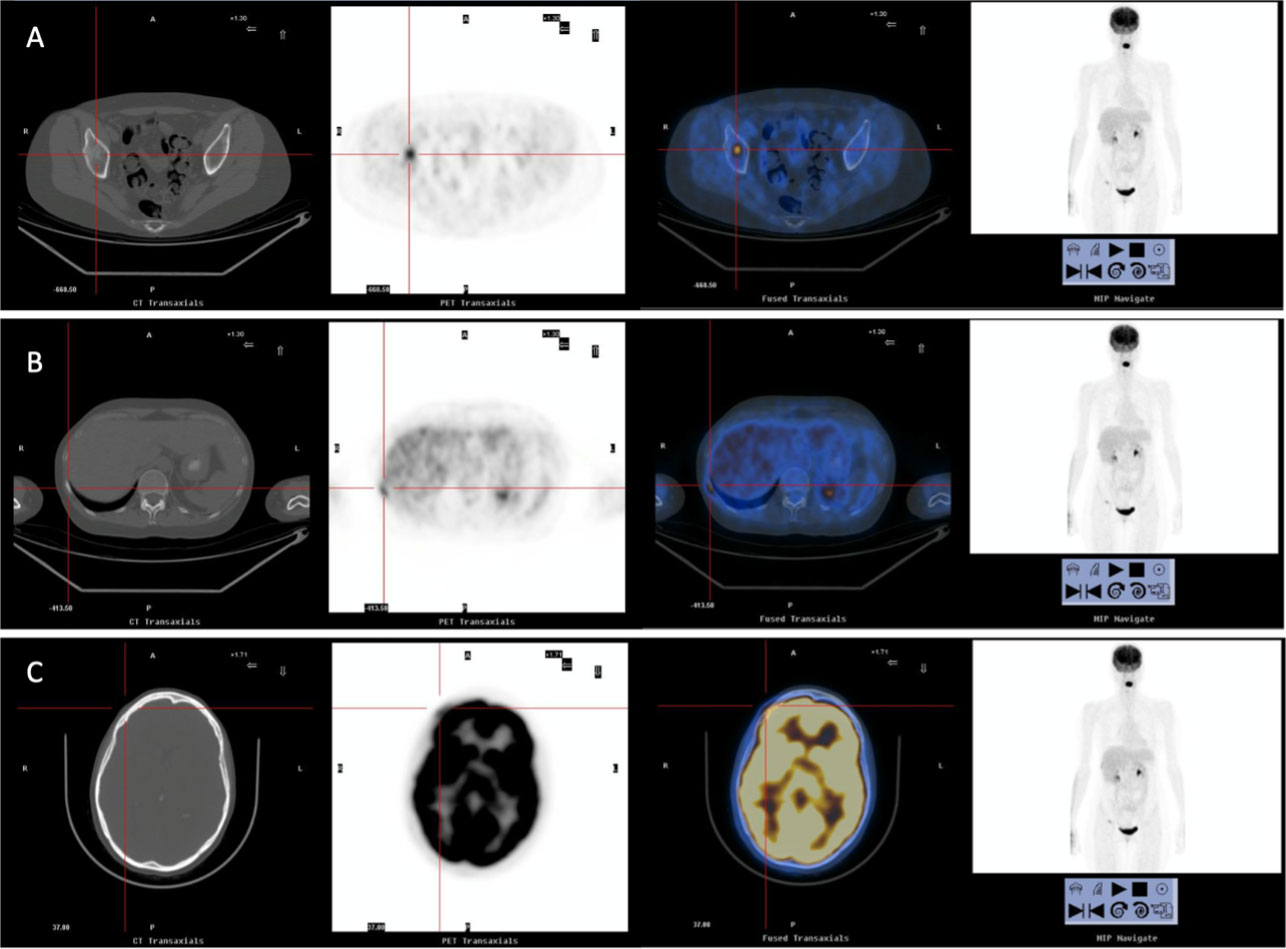
Figure 1 Images from computerized tomography (CT), FDG-PET and bone scintigraphy, showing bone relapse in right acetabulum (A), tenth right rib (B) and right frontal bone (C).
Due to the early relapse of the disease while on adjuvant treatment with tamoxifen, the patient declined hormone therapy, alone or in combination with a cyclin-dependent kinase inhibitor (CDKi). After being informed about the non-curative intent and potential adverse effects of conventional CT, the patient discarded this option, and asked about additional therapeutic options. Preliminary data regarding the promising results of PARP inhibitors in untreated BRCA mutation carriers with BC (19–21), were discussed with the patient, and talazoparib was solicited as a compassionate drug.
She started treatment with talazoparib 1 mg/24 h in February 2017, achieving a complete clinical and metabolic response after two cycles. In April 2017, bone scintigraphy and liver MRI showed no evidence of disease (Figure 2). She has completed 90 cycles of treatment to date, with good tolerance, except for mild hematologic toxicity (grade 1 anemia). The disease remains in complete response on the last FDG-PET scan, performed in November 2022. A timeline of the case is presented in Figure 3.
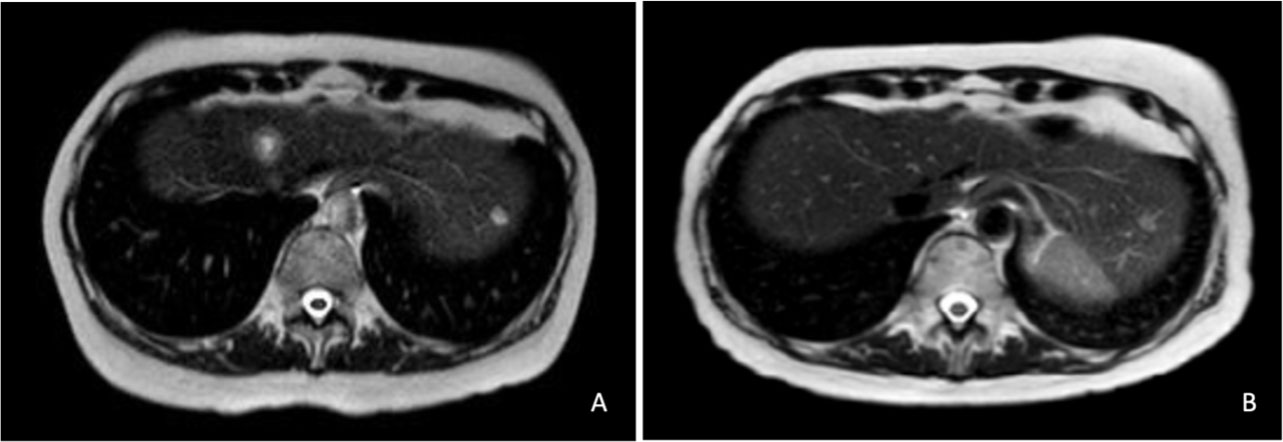
Figure 2 MRI study showing two liver metastases in January 2017 (A). Complete response of liver lesions after 2 cycles of talazoparib in April 2017 (B).

Figure 3 Timeline of the case.
3 Discussion
3.1 PARPi in metastatic BC
The OlympiAD (15) was a phase 3 clinical trial that compared olaparib (300 mg twice daily) with standard non-platinum single-agent CT (eribulin, capecitabine or vinorelbine) in 205 patients who were carriers of gBRCAm with metastatic Her2-negative BC (randomization 2 to 1). Among the patients in the experimental group, 57.1% had mutations in BRCA1, 41.0% had mutations in BRCA2 and 2.0% had mutations in BRCA1 and BRCA2 simultaneously. The patients had received no more than two previous lines of CT (12.7% had new metastatic BC and 71.2% had been previously treated with CT in the olaparib group). In the olaparib group, 77.6% of patients had two or more metastatic sites. Among the patients who received olaparib, 50.2% had HR+ tumors and 41.0% had triple-negative tumors. The median PFS, set as primary endpoint, was significantly longer in the olaparib group (7.0 months vs 4.2 months; HR 0.58, p <0.001). Patients in the olaparib arm achieved a median overall survival (OS) of 19.3 months, versus 17.1 months in the control arm (p = 0.51). The objective response rate (ORR) was 59.9% in the olaparib group (28.8% in the control group). The experimental group also appeared to have a favorable rate of grade 3-4 adverse events and treatment discontinuation. An analysis of OlympiAD patients treated in the first-line setting demonstrated a survival benefit with olaparib, suggesting a higher benefit with the earlier use of PARPi (22).
In the phase 3 trial EMBRACA (16), 431 patients with advanced BC and gBRCAm were randomly assigned (2:1) to receive talazoparib (1 mg once daily) or standard single-agent CT (eribulin, capecitabine, vinorelbine, or gemcitabine). Of the patients treated with talazoparib, 42.9% harbored mutations in BRCA1, and 51.2% of them had mutations in BRCA2. The patients had received no more than three previous lines of CT (38.7% had new metastatic BC, 37.3% had been treated with 1 prior regime of CT, and 24% had received 2 or 3 previous lines of CT). In the talazoparib group, 45.3% were triple-negative and 54.7% HR+ tumors based on the most recent biopsy. The experimental group obtained a higher median PFS (8.6 months vs 5.6 months; HR 0.54; p < 0.001), a higher median OS (22.3 months vs 19.5 months; HR 0.76; p = 0.11) and a higher ORR (62.6% vs 27.2%) -complete response in 5.5% and partial response in 57.1% of patients-. Hematologic grade 3-4 adverse events were more frequent with talazoparib (55% vs. 38%), although globally tolerance, quality-of-life reports, and time to clinical deterioration favored the experimental group.
The use of a PARP inhibitor in the first-line setting, due to the unwillingness of our patient to receive hormone therapy or conventional CT, was an unusual situation out of the context of a clinical trial. The combination of hormone therapy and CDKi is currently the standard first-line therapy for HR+ BC. Pivotal phase III clinical trials with CDKi reported median PFS rates of 24.8 months for letrozole + palbociclib [PALOMA-2 (23)], 20.5 months for letrozole + ribociclib [MONALEESA-2 (24)] and 28.2 months for letrozole + abemaciclib [MONARCH-3 (25)].
Information regarding the effectiveness of CDKi in gBRCAm BC is limited. A real-world study published by Collins et al. (26) shows that the outcomes with CDKi may be worse in patients with gBRCAm, with a shorter time-to-first subsequent therapy or death and a shorter median OS, suggesting biological differences between gBRCAm and gBRCA wild-type BC. Frenel et al. (27) demonstrated that patients with HR+/Her2- metastatic BC from PADA-1 trial, who were carriers of BRCA and PALB2 germline mutations, seemed to have a poorer benefit from palbociclib plus hormone therapy than non-mutated patients (mPFS 14 months vs. 26.7 months), presumably because of frequent emergence of ESR1 resistance mutation in this subgroup.
On the other hand, there is also scarce evidence about the efficacy of PARP inhibitors in the first-line setting of HR+ BC, since both OlympiAD and EMBRACA studies mainly included pretreated patients. Rugo et al. (28) published a subanalysis of outcomes in the prespecified patient subgroups from the EMBRACA study, reporting a median PFS of 9.8 months with talazoparib (95% CI 8.5-13.3) in patients that had not received any previous CT, compared to 8.7 months with physician choice CT (95% CI 5.5-18.0). However, it is presumable that a significant proportion of these patients had triple-negative BC, and among those with HR+ tumors, many had previously received hormone therapy. Well-designed studies are required to properly compare the outcomes of CDKi and PARPi as first-line therapy in advanced gBRCAm BC.
Although the prognosis of metastatic BC is worse in cases of endocrine-refractory tumors and visceral involvement (29), the oligometastatic presentation of the disease might have played a role in the favorable outcomes observed in our patient.
3.2 PARPi in early-stage BC
PARPi have also shown efficacy in early stage disease. In the OlympiA trial (30), 1 year adjuvant olaparib was compared with placebo in gBRCAm carriers with Her2-negative BC and a high risk of recurrence. The olaparib arm was superior, with better invasive disease-free survival (iDFS) (HR 0.58, p < 0.0001), distant disease-free survival (dDFS) (HR 0.57, p < 0.0001), and OS (HR 0.68, p = 0.009). According to these results, not only metastatic patients, but also newly diagnosed patients with localized high-risk disease, should undergo germline testing if a PARP inhibitor may be used for treatment.
The OlympiA eligibility criteria included patients with TNBC and high-burden HR+ BC with residual disease after neoadjuvant CT, as well as patients directly undergoing surgery who had an HR+ tumor with at least four involved axillary nodes, TNBC > 2 cm, or with any axillary involvement. Our patient, who suffered an early relapse of HR+ BC during adjuvant hormone therapy, would not have met the inclusion criteria of the OlympiA study, whose patients with HR+ tumors comprised a particularly high-risk cohort -with a 3-year iDFS of 77% in the placebo arm (15)-. It is inevitable to question whether adjuvant PARPi may have prevented or delayed relapse in our case. Further research is necessary to assess whether a larger population of gBRCAm carriers with HR+ BC, with lower-volume tumors or fewer involved axillary nodes than the OlympiA RH+ population, could also benefit from adjuvant PARPi.
Another question relates to the possible role of PARPi in the neoadjuvant setting, which may allow de-escalation or even omission of CT in some gBRCAm carriers, especially those with lower-risk BC. Comparable pCR rates were observed with paclitaxel/carboplatin and paclitaxel/olaparib in the GeparOLA trial (31). The use of PARPi alone as neoadjuvant treatment has also been explored, with a 48% pCR rate with talazoparib in gBRCAm carriers with TNBC in the NeoTALA trial (32).
Several studies have demonstrated that patients with BRCA1/2 mutations are more sensitive to cytotoxic drugs that induce DSBs, mainly platinum analogs, because of the deficiency of the HR system. The TNT trial (33) showed that BRCAm patients had an increased ORR with carboplatin compared to docetaxel (68% vs. 33%). In both the Geparsixto (34) and CALGB40603 (35) trials, the addition of neoadjuvant carboplatin in TNBC achieved a higher pathologic complete response (pCR). Available data support the efficacy of combining PARPi and platinum in BRCAm metastatic BC (36), though phase III trials are warranted to approve its clinical use.
However, there is growing evidence regarding the association between previous platinum exposure and lower response rates to PARPi. In the Olympia trial (30), the improvement in invasive disease-free survival was significantly lower among patients who had previously received platinum-based chemotherapy (HR 0.52) than in platinum-naïve patients (HR 0.77). Desnoyers et al. (37) published a meta-regression analysis of 43 studies, confirming that previous platinum-based treatment was also associated with a lower ORR (p = 0.02) in patients with metastatic BC.
3.3 The future of PARPi in BC
Several questions remain unanswered regarding the optimal use of PARPi, both in metastatic and (neo)adjuvant scenarios. Further research is required to explore the possible role of PARPi in combination with other systemic therapies, such as CDKi in HR+ tumors and immune checkpoint inhibitors (ICIs) in TNBC. In advanced BC, the combination of PARPi with ICIs -in gBRCAm carriers- has shown promising results, for both olaparib plus anti-PDL1 durvalumab [MEDIOLA trial (38)] and niraparib plus anti-PD1 pembrolizumab [TOPACIO/Keynote162 trial (39)]. In the adjuvant setting, up to 12.5% of TNBC patients from the OlympiA study still had distant recurrence even after an accurate treatment with olaparib and intense CT, leaving a wide room for improvement in results, which may be achieved by the addition of ICIs to PARPi. This combination may seem reasonable in TNBC with a large tumor size, nodal involvement, or residual disease after neoadjuvant CT (40), although prospective data are required to validate this hypothesis.
Some preclinical studies have even brought up the concept of ‘chemopreventive’ PARPi, suggesting their potential benefit in healthy gBRCAm carriers to reduce the risk of BRCA-related cancers, maybe avoiding early prophylactic surgeries (41). Clinical evaluation of the prophylactic effect of PARPi is challenging, because of the limitations in generating prospective evidence, and the difficulty in assessing the risk of contralateral BC in patients treated with PARPi, since most of gBRCAm carriers with BC undergo bilateral mastectomy.
The exponential expansion of PARPi from a restricted group of metastatic patients to a much wider population. regarding their use in early stage disease and even their potential prophylactic role in healthy gBRCAm carriers, should be accompanied by careful evaluation of their long-term safety. A recent meta-analysis of 31 randomized controlled trials, including 5693 patients treated with PARPi and 3406 in control groups, demonstrated a significant increase in the risk of myelodysplastic syndrome and acute myeloid leukemia (HR 2.63, p = 0.026), although the absolute risk remained low (0.73% vs. 0.47%) (42) and PARPi are generally well-tolerated drugs.
In our patient, with no adverse effects, except for mild hematologic toxicity, interruption of talazoparib has not been considered. However, in long-responding patients with worse treatment tolerance and a negative impact on quality of life, one might consider the use of lower-dose schedules, an intermittent exposure to the drug, or even a temporary interruption of PARPi. Prospective studies are needed to explore whether these are feasible strategies, and their impact on clinical outcomes.
To our knowledge, our patient has the longest response to a PARP inhibitor reported to date, as well as the first reported long-term response to talazoparib. Wang et al. (43) have recently published the case of a patient with advanced TNBC and a germline deletion of exon 2 in BRCA1, with a complete response to olaparib since September 2017. Exman et al. (44) have reported a partial response to olaparib in a gBRCA2m carrier with metastatic BC and leptomeningeal carcinomatosis. Little is known about the biological features of BC or possible predictive factors related to these long-term responses, and further studies are needed to identify this subgroup of patients.
Although somatic BRCA mutations (classified as ESCAT IIA) have not the same value as germline alterations (ESCAT I), the potential benefit of PARPi in this subgroup of patients is also a matter of research. In the RUBY trial, rucaparib monotherapy was evaluated in 41 patients with HRR deficiency, including 4 patients with somatic BRCA mutations, reporting 1 partial response and 1 stable disease (45). The TBCRC048 trial evaluated olaparib in 54 patients with metastatic BC and germline mutations in various non-BRCA DNA damage repair genes (cohort 1) and somatic mutations in several genes, including BRCA (cohort 2), with ORR of 33% and 31% respectively (46).
Kuemmel et al. (47) reported a partial response to olaparib in a patient with metastatic HR+ BC harboring a germline sequence variant affecting PALB2, supporting the possible benefit of PARPi not only in patients with alterations in BRCA, but also in other genes implicated in the HR repair system. Further research is needed to explore whether the benefits of PARPi can be extended to patients harboring germline alterations in other HR-related genes, such as BARD1 and RAD51D mutations or BRCA promoter methylation (48).
4 Conclusion
Germline mutations in BRCA1 and BRCA2 are the most relevant causes of a genetic predisposition to breast cancer. Dysfunction of the homologous recombination repair system makes BRCA-deficient cells sensitive to PARP inhibitors, because of the phenomenon of synthetic lethality. In carriers of germline BRCA mutations with metastatic BC, olaparib and talazoparib achieved better median PFS than conventional CT, according to the results of the phase III trials OlympiAD and EMBRACA. Olaparib has also shown efficacy as an adjuvant therapy for triple-negative and high-risk HR+ tumors. Neoadjuvant olaparib may be useful to increase the rate of pCR and allow de-escalation or omission of conventional CT in some gBRCAm carriers.
Further research is required to answer open questions regarding the use of PARPi, such as their benefit as adjuvant treatment for lower-risk HR+ BC, their possible combination with other systemic therapies, their potential role as prophylactic agents for healthy gBRCAm carriers, biological predictive markers of long-term responses, feasibility of de-escalation strategies in long responders, and efficacy in patients with other alterations involving the HR repair system beyond germline BRCA mutations.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Author contributions
VA - conception of the work, writing and review of literature JC, JP, MS, DR – contribution to writing and review of literature CS, MG, AC, EE, EG, EL, MF – treating oncologists and provision of study material NM – treating oncologist, provision of study material and supervision of the work. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin (2021) 71(1):7–33. doi: 10.3322/caac.21654
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
3. Loibl S, Poortmans P, Morrow M, Denkert C, Curigliano G. Breast cancer. Lancet (2021) 397(10286):1750–69. doi: 10.1016/S0140-6736(20)32381-3
4. Kuchenbaecker KB, Hopper JL, Barnes DR, Phillips K-A, Mooij TM, Roos-Blom M-J, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA (2017) 317(23):2402–16. doi: 10.1001/jama.2017.7112
5. Mulligan AM, Couch FJ, Barrowdale D, Domchek SM, Eccles D, Nevanlinna H, et al. Common breast cancer susceptibility alleles are associated with tumour subtypes in BRCA1 and BRCA2 mutation carriers: results from the consortium of investigators of modifiers of BRCA1/2. Breast Cancer Res BCR (2011) 13(6):R110. doi: 10.1186/bcr3052
6. Moore K, Colombo N, Scambia G, Kim B-G, Oaknin A, Friedlander M, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med (2018) 379(26):2495–505. doi: 10.1056/NEJMoa1810858
7. Pujade-Lauraine E, Ledermann JA, Selle F, Gebski V, Penson RT, Oza AM, et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol (2017) 18(9):1274–84. doi: 10.1016/S1470-2045(17)30469-2
8. Ray-Coquard I, Pérol D, Pujade-Lauraine E. PARP inhibitors in ovarian cancer. Reply N Engl J Med (2020) 382(16):1574–5. doi: 10.1056/NEJMc2000644
9. Ledermann J, Harter P, Gourley C, Friedlander M, Vergote I, Rustin G, et al. Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer. N Engl J Med (2012) 366(15):1382–92. doi: 10.1056/NEJMoa1105535
10. Coleman RL, Oza AM, Lorusso D, Aghajanian C, Oaknin A, Dean A, et al. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Lond Engl (2017) 390(10106):1949–61. doi: 10.1016/S0140-6736(17)32440-6
11. Del Campo JM, Matulonis UA, Malander S, Provencher D, Mahner S, Follana P, et al. Niraparib maintenance therapy in patients with recurrent ovarian cancer after a partial response to the last platinum-based chemotherapy in the ENGOT-OV16/NOVA trial. J Clin Oncol Off J Am Soc Clin Oncol (2019) 37(32):2968–73. doi: 10.1200/JCO.18.02238
12. González-Martín A, Pothuri B, Vergote I, DePont Christensen R, Graybill W, Mirza MR, et al. Niraparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med (2019) 381(25):2391–402. doi: 10.1056/NEJMoa1910962
13. de Bono J, Mateo J, Fizazi K, Saad F, Shore N, Sandhu S, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med (2020) 382(22):2091–102. doi: 10.1056/NEJMoa1911440
14. Golan T, Hammel P, Reni M, Van Cutsem E, Macarulla T, Hall MJ, et al. Maintenance olaparib for germline BRCA-mutated metastatic pancreatic cancer. N Engl J Med (2019) 381(4):317–27. doi: 10.1056/NEJMoa1903387
15. Robson M, Im S-A, Senkus E, Xu B, Domchek SM, Masuda N, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N Engl J Med (2017) 377(6):523–33. doi: 10.1056/NEJMoa1706450
16. Litton JK, Rugo HS, Ettl J, Hurvitz SA, Gonçalves A, Lee K-H, et al. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. N Engl J Med (2018) 379(8):753–63. doi: 10.1056/NEJMoa1802905
17. Diéras V, Han HS, Kaufman B, Wildiers H, Friedlander M, Ayoub J-P, et al. Veliparib with carboplatin and paclitaxel in BRCA-mutated advanced breast cancer (BROCADE3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol (2020) 21(10):1269–82. doi: 10.1016/S1470-2045(20)30447-2
18. Corben AD, Abi-Raad R, Popa I, Teo CHY, Macklin EA, Koerner FC, et al. Pathologic response and long-term follow-up in breast cancer patients treated with neoadjuvant chemotherapy: a comparison between classifications and their practical application. Arch Pathol Lab Med (2013) 137(8):1074–82. doi: 10.5858/arpa.2012-0290-OA
19. Litton JK, Scoggins M, Ramirez DL, Murthy RK, Whitman GJ, Hess KR, et al. A pilot study of neoadjuvant talazoparib for early-stage breast cancer patients with a BRCA mutation. Ann Oncol (2016) 27:vi46. doi: 10.1093/annonc/mdw364.10
20. Schouten PC, Dackus GMHE, Marchetti S, van Tinteren H, Sonke GS, Schellens JHM, et al. A phase I followed by a randomized phase II trial of two cycles carboplatin-olaparib followed by olaparib monotherapy versus capecitabine in BRCA1- or BRCA2-mutated HER2-negative advanced breast cancer as first line treatment (REVIVAL): study protocol for a randomized controlled trial. Trials (2016) 17(1):293. doi: 10.1186/s13063-016-1423-0
21. Dent RA, Lindeman GJ, Clemons M, Wildiers H, Chan A, McCarthy NJ, et al. Phase I trial of the oral PARP inhibitor olaparib in combination with paclitaxel for first- or second-line treatment of patients with metastatic triple-negative breast cancer. Breast Cancer Res BCR (2013) 15(5):R88. doi: 10.1186/bcr3484
22. Robson ME, Tung N, Conte P, Im S-A, Senkus E, Xu B, et al. OlympiAD final overall survival and tolerability results: olaparib versus chemotherapy treatment of physician’s choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Ann Oncol Off J Eur Soc Med Oncol (2019) 30(4):558–66. doi: 10.1093/annonc/mdz012
23. Finn RS, Martin M, Rugo HS, Jones S, Im S-A, Gelmon K, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med (2016) 375(20):1925–36. doi: 10.1056/NEJMoa1607303
24. Hortobagyi GN, Stemmer SM, Burris HA, Yap YS, Sonke GS, Paluch-Shimon S, et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann Oncol Off J Eur Soc Med Oncol (2018) 29(7):1541–7. doi: 10.1093/annonc/mdy155
25. Goetz MP, Toi M, Campone M, Sohn J, Paluch-Shimon S, Huober J, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J Clin Oncol Off J Am Soc Clin Oncol (2017) 35(32):3638–46. doi: 10.1200/JCO.2017.75.6155
26. Collins JM, Nordstrom BL, McLaurin KK, Dalvi TB, McCutcheon SC, Bennett JC, et al. A real-world evidence study of CDK4/6 inhibitor treatment patterns and outcomes in metastatic breast cancer by germline BRCA mutation status. Oncol Ther (2021) 9(2):575–89. doi: 10.1007/s40487-021-00162-4
27. Frenel J-S, Dalenc F, Pistilli B, de La Motte Rouge T, Levy C, Mouret-Reynier M-A, et al. 304P ESR1 mutations and outcomes in BRCA1/2 or PALB2 germline mutation carriers receiving first line aromatase inhibitor + palbociclib (AI+P) for metastatic breast cancer (MBC) in the PADA-1 trial. Ann Oncol (2020) 31:S364. doi: 10.1016/j.annonc.2020.08.406
28. Rugo HS, Ettl J, Hurvitz SA, Gonçalves A, Lee K-H, Fehrenbacher L, et al. Outcomes in clinically relevant patient subgroups from the EMBRACA study: talazoparib vs physician’s choice standard-of-Care chemotherapy. JNCI Cancer Spectr (2020) 4(1):pkz085. doi: 10.1093/jncics/pkz085
29. Deluche E, Antoine A, Bachelot T, Lardy-Cleaud A, Dieras V, Brain E, et al. Contemporary outcomes of metastatic breast cancer among 22,000 women from the multicentre ESME cohort 2008–2016. Eur J Cancer (2020) 129:60–70. doi: 10.1016/j.ejca.2020.01.016
30. Tutt ANJ, Garber JE, Kaufman B, Viale G, Fumagalli D, Rastogi P, et al. Adjuvant olaparib for patients with BRCA1- or BRCA2-mutated breast cancer. N Engl J Med (2021) 384(25):2394–405. doi: 10.1056/NEJMoa2105215
31. Fasching PA, Link T, Hauke J, Seither F, Jackisch C, Klare P, et al. Neoadjuvant paclitaxel/olaparib in comparison to paclitaxel/carboplatinum in patients with HER2-negative breast cancer and homologous recombination deficiency (GeparOLA study). Ann Oncol Off J Eur Soc Med Oncol (2021) 32(1):49–57. doi: 10.1016/j.annonc.2020.10.471
32. Litton JK, Scoggins ME, Hess KR, Adrada BE, Murthy RK, Damodaran S, et al. Neoadjuvant talazoparib for patients with operable breast cancer with a germline BRCA pathogenic variant. J Clin Oncol Off J Am Soc Clin Oncol (2020) 38(5):388–94. doi: 10.1200/JCO.19.01304
33. Tutt A, Tovey H, Cheang MCU, Kernaghan S, Kilburn L, Gazinska P, et al. Carboplatin in BRCA1/2-mutated and triple-negative breast cancer BRCAness subgroups: the TNT trial. Nat Med (2018) 24(5):628–37. doi: 10.1038/s41591-018-0009-7
34. von Minckwitz G, Schneeweiss A, Loibl S, Salat C, Denkert C, Rezai M, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trial. Lancet Oncol (2014) 15(7):747–56. doi: 10.1016/S1470-2045(14)70160-3
35. Sikov WM, Berry DA, Perou CM, Singh B, Cirrincione CT, Tolaney SM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol Off J Am Soc Clin Oncol (2015) 33(1):13–21. doi: 10.1200/JCO.2014.57.0572
36. Wang X, Shi Y, Huang D, Guan X. Emerging therapeutic modalities of PARP inhibitors in breast cancer. Cancer Treat Rev (2018) 68:62–8. doi: 10.1016/j.ctrv.2018.05.014
37. Desnoyers A, Nadler M, Wilson BE, Stajer S, Amir E. Associations with response to Poly(ADP-ribose) polymerase (PARP) inhibitors in patients with metastatic breast cancer. NPJ Breast Cancer (2022) 8(1):43. doi: 10.1038/s41523-022-00405-1
38. Domchek SM, Postel-Vinay S, Im S-A, Park YH, Delord J-P, Italiano A, et al. Olaparib and durvalumab in patients with germline BRCA-mutated metastatic breast cancer (MEDIOLA): an open-label, multicentre, phase 1/2, basket study. Lancet Oncol (2020) 21(9):1155–64. doi: 10.1016/S1470-2045(20)30324-7
39. Konstantinopoulos PA, Waggoner S, Vidal GA, Mita M, Moroney JW, Holloway R, et al. Single-arm phases 1 and 2 trial of niraparib in combination with pembrolizumab in patients with recurrent platinum-resistant ovarian carcinoma. JAMA Oncol (2019) 5(8):1141–9. doi: 10.1001/jamaoncol.2019.1048
40. Tung N, Garber JE. PARP inhibition in breast cancer: progress made and future hopes. NPJ Breast Cancer (2022) 8(1):47. doi: 10.1038/s41523-022-00411-3
41. To C, Kim E-H, Royce DB, Williams CR, Collins RM, Risingsong R, et al. The PARP inhibitors, veliparib and olaparib, are effective chemopreventive agents for delaying mammary tumor development in BRCA1-deficient mice. Cancer Prev Res (Phila Pa) (2014) 7(7):698–707. doi: 10.1158/1940-6207.CAPR-14-0047
42. Morice P-M, Leary A, Dolladille C, Chrétien B, Poulain L, González-Martín A, et al. Myelodysplastic syndrome and acute myeloid leukaemia in patients treated with PARP inhibitors: a safety meta-analysis of randomised controlled trials and a retrospective study of the WHO pharmacovigilance database. Lancet Haematol (2021) 8(2):e122–34. doi: 10.1016/S2352-3026(20)30360-4
43. Wang X, Hu N, Cui L, Si Y, Yue J, Zheng F, et al. Durable disease-free survival in a patient with metastatic triple-negativeBreast cancer treated with olaparib monotherapy. Curr Cancer Drug Targets (2022) 22(6):530–6. doi: 10.2174/1568009622666220214092207
44. Exman P, Mallery RM, Lin NU, Parsons HA. Response to olaparib in a patient with germline BRCA2 mutation and breast cancer leptomeningeal carcinomatosis. NPJ Breast Cancer (2019) 5(1):46. doi: 10.1038/s41523-019-0139-1
45. Patsouris A, Tredan O, Nenciu D, Tran-Dien A, Campion L, Goncalves A, et al. RUBY: a phase II study testing rucaparib in germline (g) BRCA wild-type patients presenting metastatic breast cancer (mBC) with homologous recombination deficiency (HRD). J Clin Oncol (2019) 37(15_suppl):1092–2. doi: 10.1200/JCO.2019.37.15_suppl.1092
46. Tung NM, Robson ME, Ventz S, Santa-Maria CA, Nanda R, Marcom PK, et al. TBCRC 048: phase II study of olaparib for metastatic breast cancer and mutations in homologous recombination-related genes. J Clin Oncol Off J Am Soc Clin Oncol (2020) 38(36):4274–82. doi: 10.1200/JCO.20.02151
47. Kuemmel S, Harrach H, Schmutzler RK, Kostara A, Ziegler-Löhr K, Dyson MH, et al. Olaparib for metastatic breast cancer in a patient with a germline PALB2 variant. NPJ Breast Cancer (2020) 6(1):31. doi: 10.1038/s41523-020-00174-9
Keywords: breast cancer, BRCA, germline, PARP inhibitors, olaparib, talazoparib
Citation: Albarrán V, Chamorro J, Pozas J, San Román M, Rosero DI, Saavedra C, Gion M, Cortés A, Escalera E, Guerra E, López Miranda E, Fernández Abad M and Martínez Jañez N (2023) Maintained complete response to talazoparib in a BRCA-2 mutated metastatic luminal breast cancer: case report and review of literature. Front. Oncol. 13:1158981. doi: 10.3389/fonc.2023.1158981
Received: 04 February 2023; Accepted: 20 April 2023;
Published: 05 May 2023.
Edited by:
Nan Wang, First Affiliated Hospital of Zhengzhou University, ChinaReviewed by:
Gregory Vidal, West Cancer Center, United StatesIda Paris, Fondazione Policlinico Agostino Gemelli IRCSS, Italy
Copyright © 2023 Albarrán, Chamorro, Pozas, San Román, Rosero, Saavedra, Gion, Cortés, Escalera, Guerra, López Miranda, Fernández Abad and Martínez Jañez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Víctor Albarrán, dmljYWxiYXJyYW5mZXJuYW5kZXpAZ21haWwuY29t