 Binhao Shi1,2
Binhao Shi1,2 Junli Chang1,2Xingyuan Sun1,2Xiaoping Ma1,2
Junli Chang1,2Xingyuan Sun1,2Xiaoping Ma1,2 Peng Zhao1,2Chujie Zhou1,2Yongjun Wang1,2*
Peng Zhao1,2Chujie Zhou1,2Yongjun Wang1,2* Yanping Yang1,2*
Yanping Yang1,2*- 1Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, China
- 2Key Laboratory of Theory and Therapy of Muscles and Bones, Ministry of Education, Shanghai, China
Backgrounds: PD-1 inhibitors and TKIs have been used to treat advanced osteosarcoma, but there is still a lack of intuitive data for the comparison of their efficacy. We conducted a meta-analysis to evaluate their therapeutic benefits.
Methods: A systematic methodological search of five primary electronic databases was performed. Studies with a randomized design of any type about PD-1 inhibitors or TKIs for the treatment of advanced osteosarcoma were included. The primary outcomes mainly included CBR, PFS, OS and ORR, The CR, PR, SD and AEs were the secondary outcomes. The survival period (months) of patients was taken as the main analysis data. Random-effects models were used for meta-analysis.
Results: Eight immunocheckpoint inhibitors in 327 patients from 10 clinical trials were finally evaluated. For OS, TKIs [11.67 months (95% CI, 9.32-14.01)] show more obvious advantages than PD-1 inhibitors [6.37 months (95% CI, 3.96-8.78)]. For PFS, TKIs [4.79 months (95% CI, 3.33-6.24)] are longer than PD-1 inhibitors [1.46 months (95% CI, 1.23-1.69)]. Although there was no fatal event, attention should still be paid, especially during the combined application of PD-1 inhibitors with TKIs since their obvious AEs.
Conclusions: The findings of this study suggest that patients with advanced osteosarcoma, TKIs may be more beneficial than PD-1 inhibitors. TKIs combined with PD-1 inhibitors has a bright future in the treatment of advanced osteosarcoma, but we should always pay attention to the strong side effects.
Introduction
Osteosarcoma is a malignant bone tumor that often occurs in the metaphysis of growing long tubular bones and usually arises in children, adolescents and young adults (1, 2), which is easy to invade the lungs and other bones. Modern imaging techniques identify that about 25% of newly diagnosed patients showing metastatic lesions (3). Local surgery and chemotherapy are still currently the dominant treatment strategy for the osteosarcoma patients, with the combination of high dose methotrexate, adriamycin and cisplatin (MAP) as the international standard regimen in perioperative period (4). This greatly contribute to the 5-year overall survival (OS) rate and the 5-year event-free survival rate of patients after successful surgery and chemotherapy reaching about 60% (1). However, patients with initially metastatic disease, those who relapse after achieving remission, or those who fail to respond to the MAP regimens have an extremely poor 5-year survival rate of less than 30% (5). Furthermore, approximately one third of osteosarcoma patients will eventually develop disease recurrence or metastasis (6). Moreover, the efficacy of chemotherapy combination in the treatment of advanced osteosarcoma is limited, with an effective rate of only 3% to 29% and a median PFS of less than 4 months (7–9).
Immunotherapy is a method to improve the immune clearance of cancer cells via complementation or stimulation of the immune system with a plethora of compounds, which includes the three main forms of cancer vaccines, cytokine therapies and passive cancer immunotherapy (10). As an important form of tumor immunotherapy, immune checkpoint inhibitors bring hopes to patients with refractory tumors and have improved the prognosis of many patients with advanced tumors (11, 12), which belongs to the passive cancer immunotherapy. Programmed cell death protein (PD-1) is a member of the immunoglobulin gene superfamily, and exerts the immunosuppressive effect on active T cells. Interaction between PD-1 with programmed death-ligand 1 (PD-L1) results in tumor-specific T cell exhaustion and apoptosis, which enables tumor cells to evade the T cell based immune surveillance. Theoretically, inhibition of PD-1 relieves the immunosuppressive microenvironment of activated T cells, B cells, monocytes, dendritic cells (DCs), regulatory T cells (Tregs) and natural killer T cells (NKTs), thus to improve the killing effect on tumor cells and inhibit the tumor growth (13). For example, nivolumab and pembrolizumab showed anti-tumor activity in the treatment of advanced osteosarcoma. However, the current clinical benefits have not met people’s expectations (14, 15).
As a major member of the protein kinase family, protein tyrosine kinases play vital roles in the growth, regulation, differentiation, migration, and apoptosis of tumor cells. Excessive tyrosine kinase activity induces the initiation and progression of malignancy (16). Therefore, ideally, the malignant tumor related tyrosine kinase can be used as an inhibitory target to control the continuous development of the malignant tumors. Multiple potent and well-tolerated tyrosine kinase inhibitor (TKI)-targets, including EGFR (epidermal growth factor receptor), ALK (anaplastic lymphocyte kinase), ROS1 (ROS proto-oncogene 1), HER2 (human epidermal growth factor receptor 2), TRK (tropomyosin receptor kinase), VEGFR (vascular endothelial growth factor receptor), RET (rearranged during transfection), MET (mesenchymal-epithelial transition factor), MEK (mitogen-activated protein kinase pathway), FGF (fibroblast growth factor), PDGF (Platelet-derived growth factor), and KIT (proto-oncogene c-KIT), have emerged and contributed to the significant improvement in cancer treatment (17). Tyrosine kinase inhibitors (TKIs) have objective responsiveness in the treatment of osteosarcoma, such as retinofenib and cabozantinib (18). In addition, the positive expression of VEGFR-2 and PD-L1 is significantly correlated with the grading and distant metastasis of osteosarcoma. VEGF/VEGFR inhibitors can play a synergistic role with PD-1 inhibitors in the treatment of osteosarcoma (15).
PD-1 inhibitors and TKIs have been used in patients with inoperable or recurrent osteosarcoma. However, there is no systematic evaluation of the difference between PD-1 inhibitors and TKIs in inhibiting disease progression and improving the survival of patients with advanced osteosarcoma. Our current work attempts to compare the efficacies of PD-1 inhibitors and TKIs in advanced osteosarcoma through a comprehensive meta-analysis.
Search methods and study selection
To identify the therapeutic effects of PD-1 inhibitors or TKIs on osteosarcoma, a comprehensive literature search for the published clinical trials was performed from December 2, 2021, through final search for updates on May 30, 2022, in PubMed, Web of Science, Embase, Science Direct, Scopus and Cochrane library using the terms of osteosarcoma, bone sarcoma, osteogenic sarcoma, PD-1 inhibitor, PD-L1 inhibitor, anti-PD-1, anti-PD-L1, TKIs, and tyrosine kinase inhibitor.
The included studies met all the following criteria: (1) clinical trial of osteosarcoma treatment, (2) participants were treated with a single drug PD-1 inhibitor or TKI, (3) reported the treatment-related data, and (4) published in English. Exclusion criteria: (1) Literature review; (2) Non clinical trial literature; (3) Non English literature. Literature search, study selection and data extraction were conducted by two independent researchers, and discrepancies were reviewed by another researcher in the team and resolved by consensus. Using the MINORS scale or JADAD scale to evaluate the quality of included literatures. The review was registered with PROSPERO (CRD42022297820). This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guideline.
Data extraction
The first author, the year of publication, the country, the trial name, the phase, the name of medicine, the number of patients, the staging, the efficacy estimation indices (CBR, ORR, PFS, OS). Grade 3 or higher (severity) adverse event (AE) data were both extracted.
Statistical analysis
The number of events and the total number of participants in the clinical trials were obtained. The relative risk and 95% CI were calculated using Stata 14 software. Heterogeneity of studies supporting each pairwise comparison was also evaluated quantitatively using chi-square test for heterogeneity and the inconsistency statistic (I2). If P > 0.1, I2<50%, it means that there is no statistical heterogeneity among the research results, and the fixed effect model is used for combined analysis. If P ≤ 0.1, I2≥50%, it indicates that there is statistical heterogeneity among the research results, and the random effect model is used for combined analysis.
Results
Eligible studies and characteristics
A total of 1401 publications were identified after literature search and browsing. Ten clinical trials involving 327 patients were finally included in this meta-analysis after the screening and qualification evaluation (Figure 1; Table 1). PD-1 and PD-L1 inhibitors for treatment included Pembrolizumab and Camrelizumab. TKIs for treatment included Regorafenib, Lenvatinib, Apatinib, Regorafenib, Cabozantinib, and TAS-115.
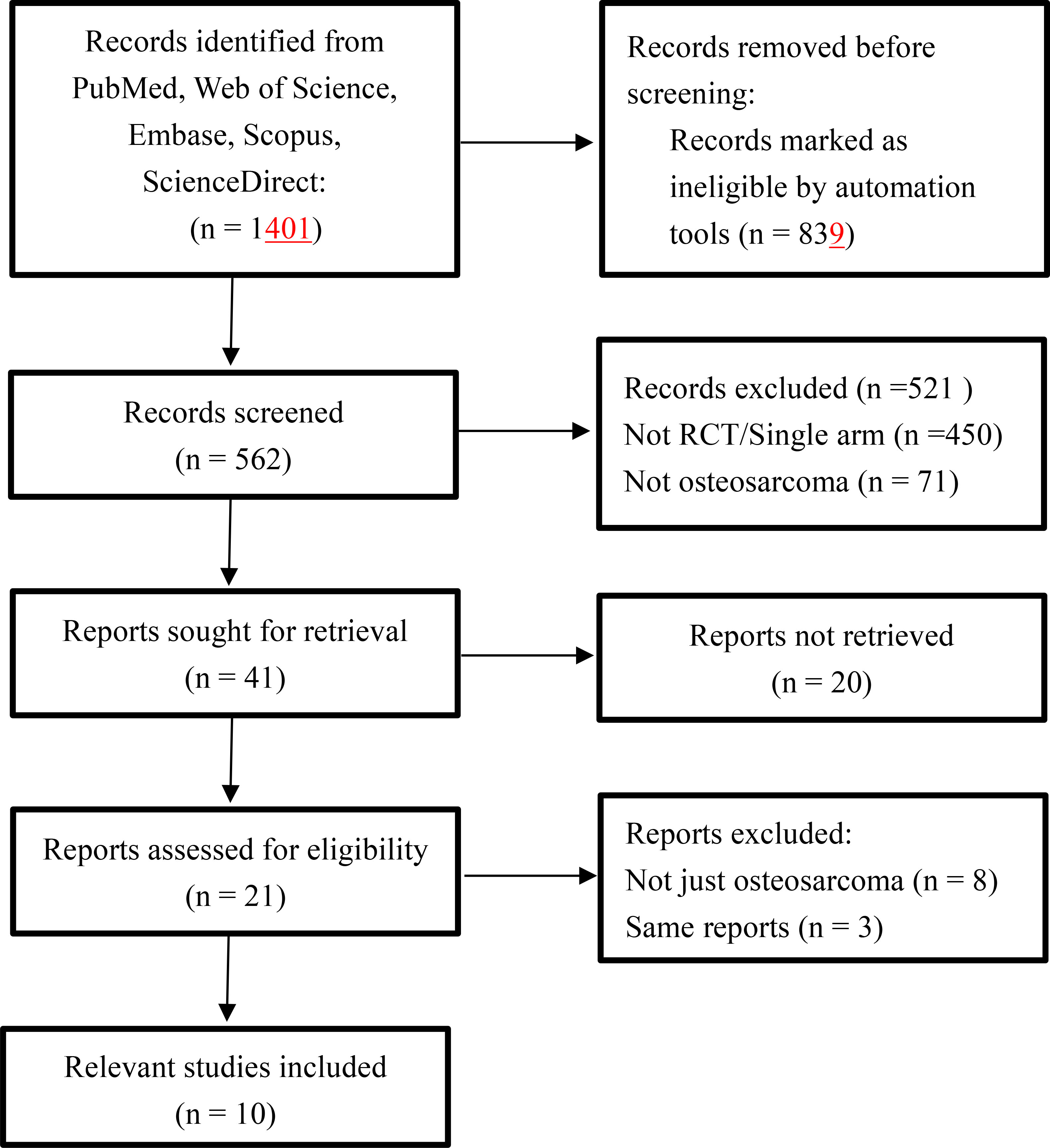
Figure 1 Flow diagram for the meta-analysis.
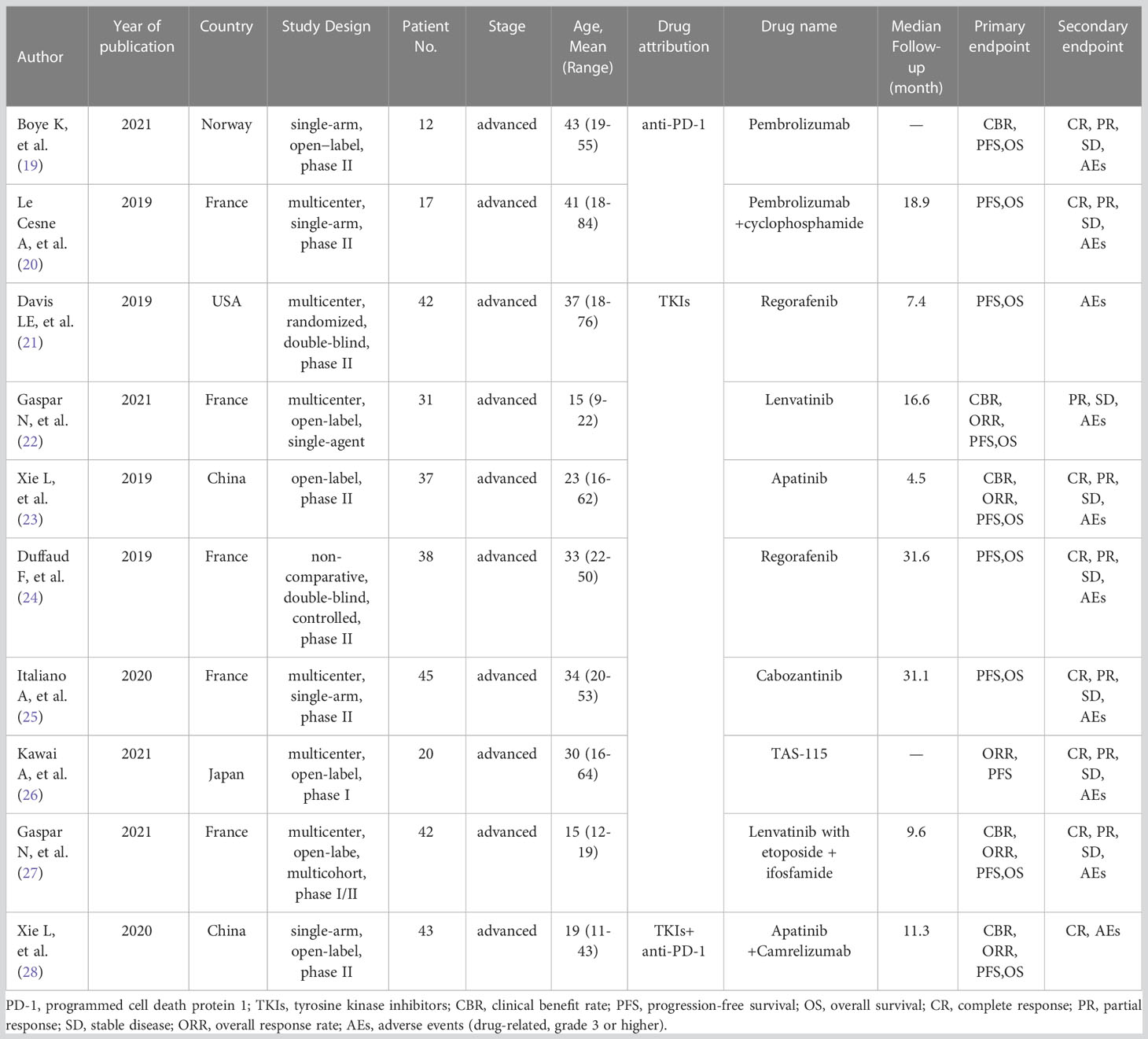
Table 1 Characteristics of the trials.
Among the 10 clinical trials included, two were randomized controlled double-blind trials, and the rest were single arm trials. There were two literatures on the treatment of osteosarcoma with PD-1 inhibitors, seven literatures on the treatment of osteosarcoma with TKIs, and one literature on the treatment of osteosarcoma with PD-1 inhibitors combined with TKIs. The quality of all 10 articles meets the inclusion requirements (Table 2). Among the 327 patients included, 132 were females and 195 were males, involving Europeans and Americans (Norway, France and the United States) and Asians (China, Japan). All the patients were in advanced stage of osteosarcoma. The efficacy evaluation indexes mainly included CBR (clinical benefit rate), PFS (progression free survival), OS (overall survival), CR (complete response), PR (partial response), SD (stable disease), ORR (overall response rate), AEs (adverse events). In view of the quality of literature data, we only performed statistical analysis on OS and PFS (Table 3). Next, we conducted the sensitivity analysis to evaluate the selected literatures. The results showed that OS related literatures (I2 = 61.7%, P = 0.007) and PFS related literatures (I2 = 93.7%, P = 0.000). Subgroup analysis by drug grouping was then conducted to objectively evaluate the difference between the two immune checkpoint inhibitors.
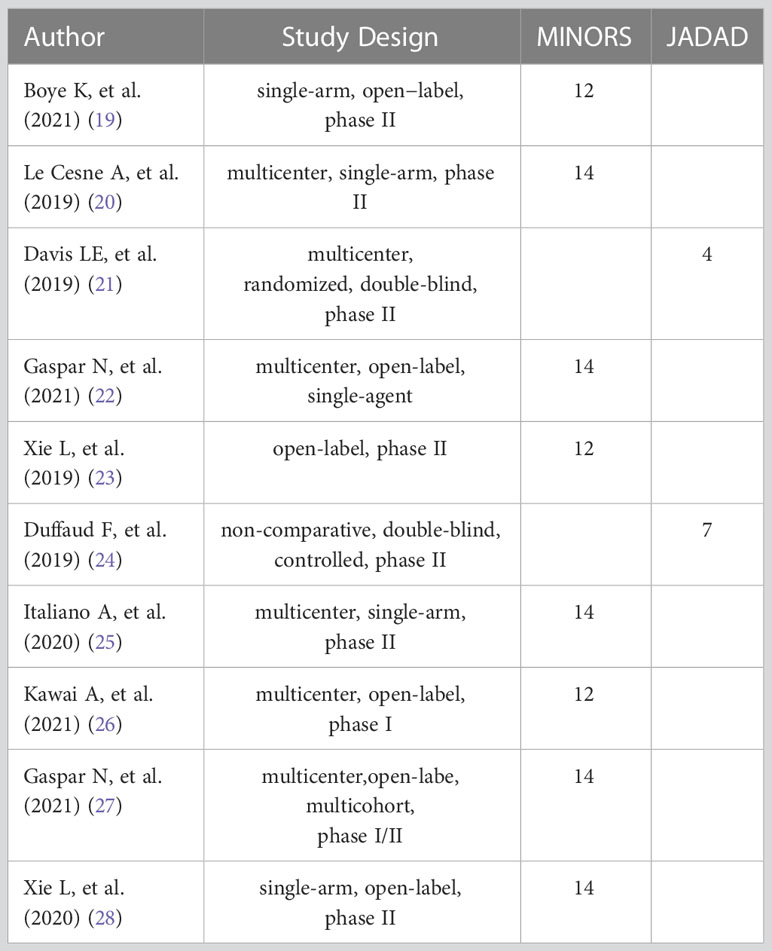
Table 2 Literature quality evaluation assessment.
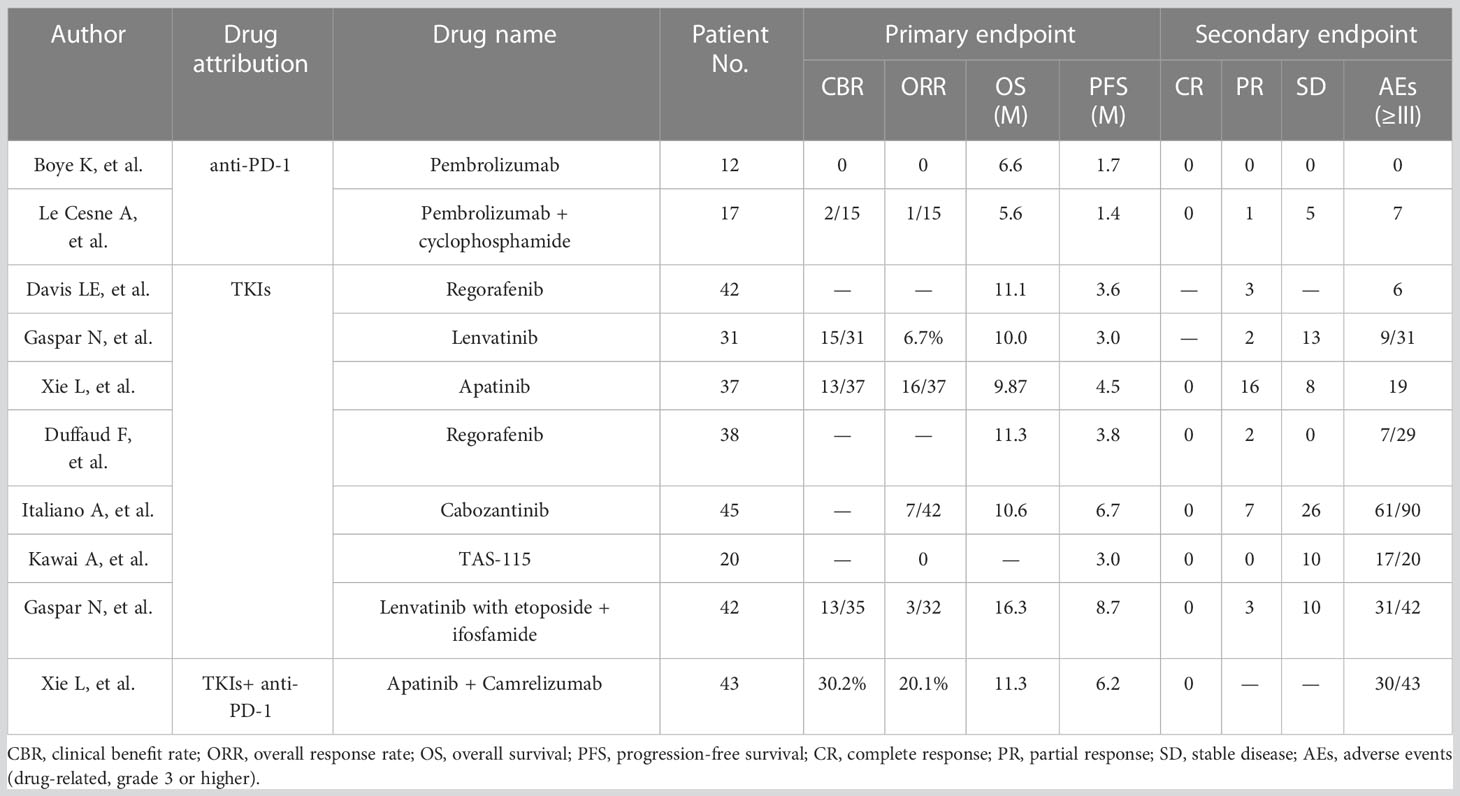
Table 3 Characteristics of the endpoints.
The OS in osteosarcoma patient treatment with PD-1 inhibitors or TKIs
The OS data were available from 9 (of 10) studies including 307 patients. The statistical analysis of all literatures suggested that the total OS was 10.22 months (95% CI, 7.99-12.45). Two clinical trials of PD-1 inhibitors (I2 = 0.0%, P = 0.731) showed that the combined OS of PD-1 inhibitors in the treatment of advanced osteosarcoma was 6.37 months (95% CI, 3.96-8.78) (Figure 2), which was similar to their respective median OS [6.60 months (95% CI, 3.80-9.30) or 5.60 months (95% CI, 2.10-12.10)]. The PD-1 inhibitors used in both studies were pembrolizumab. Six trials on TKIs (I2 = 37.9%, P = 0.153) showed that the OS of TKIs in the treatment of advanced osteosarcoma was 11.67 months (95% CI, 9.32-14.01). The TKIs used in these clinical trials included Lenvatinib, Cabozantinib, Regorafenib and Apatinib. The OS of each clinical trial was 11.1 months (95% CI, 4.7-26.70), 10.00 months (95% CI, 4.7-26.70), 9.87 months (95% CI, 7.97-18.93), 11.3 months (95% CI, 5.90-23.9), 10.60 months (95% CI, 7.40-12.50), or 16.30 months (95% CI, 12.60-20.00). Only one clinical trial applied the PD-1 inhibitor combined with TKI in the treatment of advanced osteosarcoma, which showed that the OS was 11.30 months (95% CI, 7.95-14.65). From the statistical results of drug classification, compared with PD-1 inhibitors, it seems that the survival period of advanced osteosarcoma patients treated with TKIs have been prolonged.
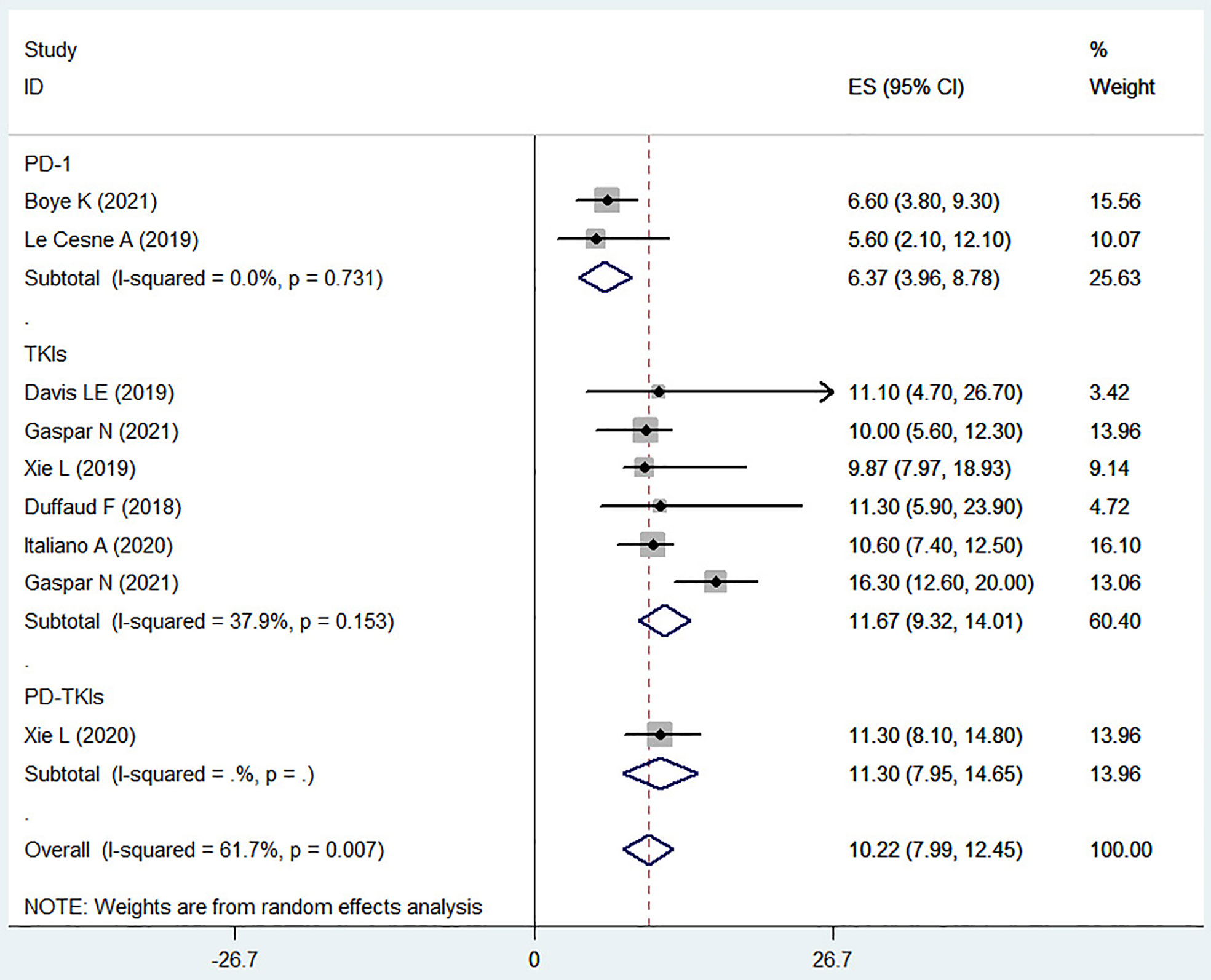
Figure 2 The OS of osteosarcoma patients treated with PD-1 inhibitors or TKIs.
The PFS in osteosarcoma patient treatment with PD-1 inhibitors or TKIs
PFS was systematically described in the ten included clinical trials. A total of 327 patients with advanced osteosarcoma were included for the final statistical analysis, which evidenced that the PFS in the advanced osteosarcoma patient treatment was 1.46 months (95% CI, 1.23-1.69) for the PD-1 inhibitors, 4.79 months (95% CI, 3.33-6.24) for the TKIs, and 6.20 months (95% CI, 4.75-7.65) for the PD-1 inhibitors combined with TKIs.
The included clinical trials with TKIs as the test drug showed a significant heterogeneity (I2 = 67.6%, P = 0.005), indicating that different test drugs may have different impact on the PFS, and the overall median PFS improved by PD-1 inhibitors combined with TKIs was more meaningful (Figure 3).
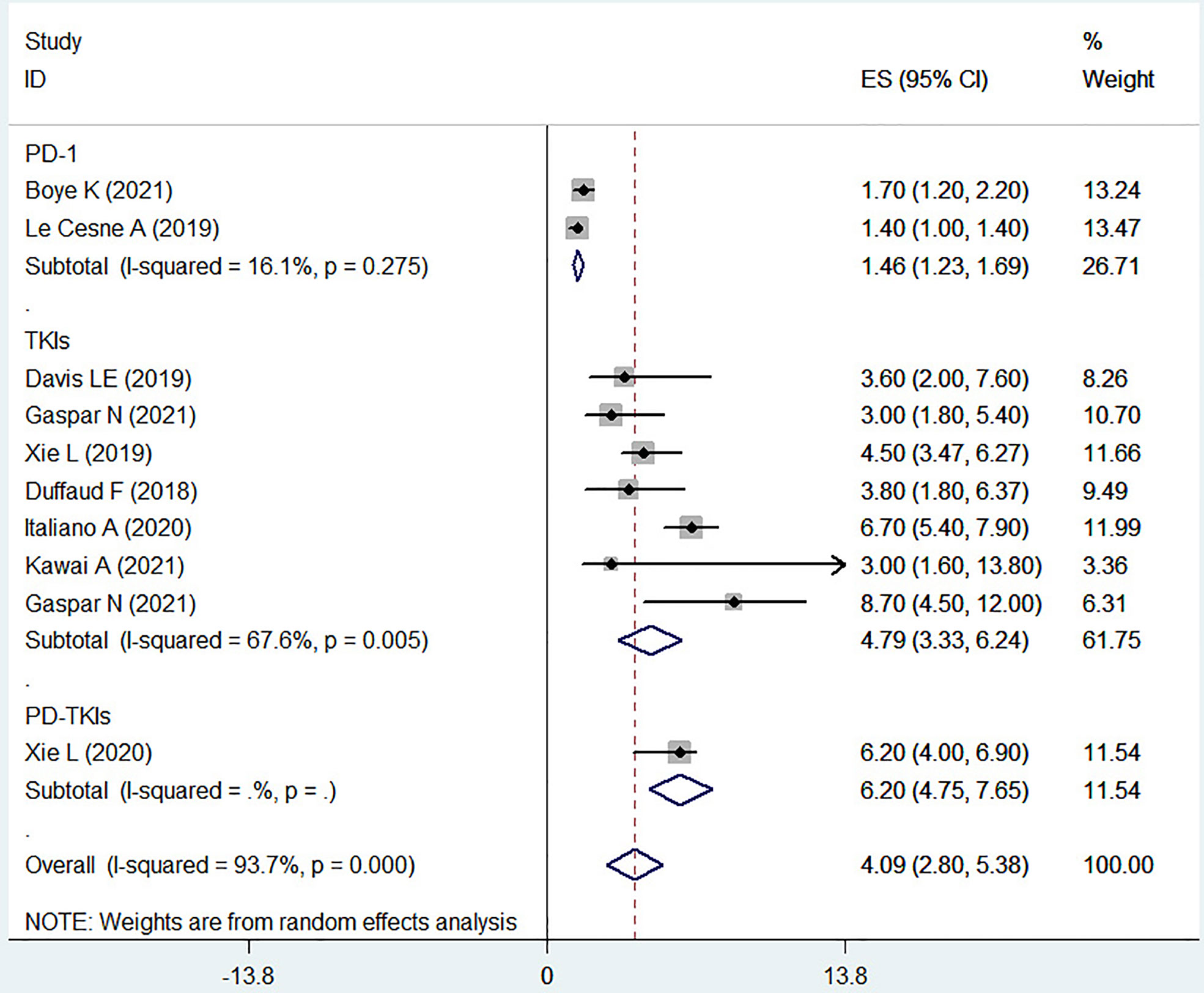
Figure 3 The PFS of osteosarcoma treated with PD-1 or TKIs.
The AEs in osteosarcoma patient treatment with PD-1 inhibitors or TKIs
The immune related adverse events (irAEs) refer to the immune activation and inflammatory response against the healthy tissues of the hosts, which are the common concomitant phenomena of immunotherapies. The drug-related adverse reactions over grade III in the included literatures were sorted out to evaluate the AEs(Table 4). Pembrolizumab may cause drug-related AEs such as anemia, fatigue, leuopenia, acute renal failure, dyspnea, lymphoenia (13). Camrelizumab may lead to hypothyroidism, thrombocytopenia, anorexia and diarrhea (25). The severity of the treatment-related AEs in the Regorafenib was at least grade III, such as hypertension, hypophosphataemia, hand-foot skin reaction, increased transaminases, increased lipase, increased blood alkaline phosphatase, epilepsy, haemothorax and fatigue (14, 21). Lenvatinib may cause hypertension, pneumothorax, colonic perforation, anemia, thrombocytopenia, febrile neutropenia and neutropenia (19, 24). Grade III or above AEs during the treatment of osteosarcoma patients with Apatinib included hypertriglyceridemia, increased blood bilirubin, increased transaminases, increased blood LDH, weight loss, leukopenia, decreased platelet count, pneumothorax, wound dehiscence, diarrhea, anorexia, hand-foot syndrome, pain in extremity, rash, mucositis oral, hypertension, abdominal pain, toothache, non-cardiac chest pain, proteinuria, cough, nausea, vomiting, hemorrhoidal hemorrhage, fatigue, peripheral neuroinflammation, abdominal cramps, pleural infection, bladder perforation, anemia, hypokalemia, palpitations, back pain, anorectal infection and cholecystitis (20, 25). The increased transaminases, increased lipase, hypertension, thrombocytopenia, hypophosphatemia, neutropenia, hypomagnesaemia, leucopenia, fatigue, diarrhea, oral mucositis, palmar-plantar syndrome, anemia, pneumothorax, and other AEs may occur during the application of Cabozantinib (22). Finally, TAS-115 may cause increased aspartate aminotransferase, increased alanine aminotransferase, increased blood creatine phosphokinase, increased amylase, decreased neutrophil count, decreased platelet count, decreased white blood cell count, hypophosphatemia, anemia, rash, and fever (23). The drug-related serious AEs of different TKIs in the treatment of osteosarcoma patients were basically similar. However, the AEs of PD-1 inhibitors in the treatment of osteosarcoma patients still need to be clarified.
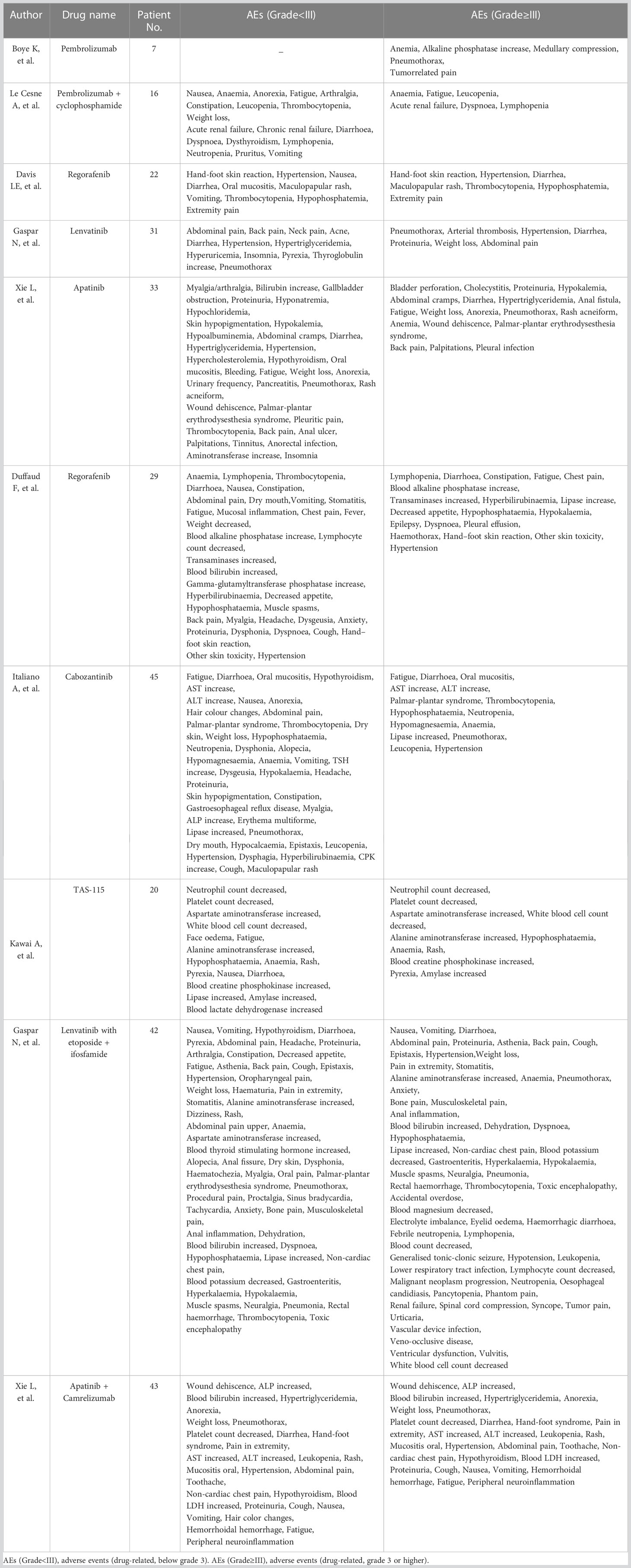
Table 4 Treatment-related adverse events.
Discussion
Osteosarcoma is a commonly diagnosed malignant bone cancer with unclear pathogenesis. The growth factors may play important roles in the oncogenesis of this disease. Patients with refractory or relapsed osteosarcoma have a very poor prognosis. The PD-1 inhibitors and TKIs offer the few available alternatives when the surgical resection and chemoradiotherapy are not suitable.
PD-1 inhibitors are known to prevent the interaction between T-cell/PD-1 and tumor cell/PD-L1, leading to restoration of the T-cell mediated anti-tumor immunity (29). Pembrolizumab is a humanized monoclonal IgG4 kappa anti-PD-1 antibody, which has been applied in many types of malignant tumors or is undergoing clinical trials, including bladder, breast, colorectal, esophagus, gastric, head and neck, hematology, lung, melanoma, ovarian, pediatric, and other solid malignant tumors (30). Studies have shown that pembrolizumab responds better to lung metastases than other site metastases, with a 1-year survival rate of 89% for lung metastases, while the median OS of patients with recurrence and other site metastases is 6-8 months or less (31, 32). The included clinical trials reported that the median OS of advanced osteosarcoma patients treated with pembrolizumab only was 6.60 months(95% CI, 3.80-9.30) (19), while treated with pembrolizumab and low-dose chemotherapy drugs was 5.60 months (95% CI, 2.10-12.10) (20), suggesting that these patients treated with pembrolizumab did not benefit from the combination of low-dose chemotherapy drugs. Chemotherapy drugs can facilitate anti-tumor responses, such as cyclophosphamide, can increase tumor cell immunogenicity by activating CD8+ T cells and other immune cells (33). A multi-center phase II study on the treatment of advanced osteosarcomas with pembrolizumab combined with metronomic cyclophosphamide was conducted, and the results showed some benefits for patients (20). But, considering the similar demographic characteristics, drug dosage, patient’s condition and Adverse events of grade 3 or higher in these two trials, At present, the superiority of combined chemotherapy cannot be determined, and it is still necessary to refine the drug selection, dosage, and timing of application for combined chemotherapy.
Changes in tyrosine kinase receptor pathways (including VEGF, FGF and PDGF) are related to the growth, invasion and metastasis of osteosarcoma (34). VEGF expression is associated with poor long-term prognosis in osteosarcoma. FGF and FGF receptor signaling pathway promotes the resistance of osteosarcoma to radiotherapy, chemotherapy and molecular targeted therapy (35, 36). Therefore, TKIs suppress the tumor angiogenesis and induce the tumor cell apoptosis, thus to inhibit the growth and metastasis of tumor cells by inhibiting the abnormal activity of tyrosine kinase through single or multiple targets via the four signaling pathways (JAK/STAT, RAS/RAF/MEK/ERK, PI3K/AKT/mTOR, and PLC/PIP2/DAG/PLK) (14). Five TKIs including Regorafenib, Lenvatinib, Apatinib, Cabozantinib and TAS-115 were evaluated in this study.
Regorafenib is a TKI affecting the vasculature and tumor microenvironment by targeting the specific kinase proteins (VEGFR1,2,3, PDGFR, FGFR, KIT, BRAF, and RET), which is a category 1 option recommended by the NCCN guidelines for the treatment of patients with recurrent/refractory or metastatic osteosarcoma. Regorafenib showed high activity in osteosarcoma and soft tissue sarcoma and prolonged the PFS (37–39). Regorafenib was used as the test drug to treat osteosarcoma in two separated double-blind control trials by Davis (21) and Duffaud (24), which showed a similar OS. However, the study by Davis showed that the OS was 11.10 months (95% CI, 4.7-26.7) and the PFS was 3.6 months (95% CI, 2.0-7.6) in the test group; the OS was 13.4 months (95% CI, 8.5-38.1) and the PFS was 1.7 months (95% CI, 1.2-1.8) in the placebo control group; the study by Duffaud (25) showed that the OS was 11.3 months (95% CI, 5.9-23.9) and the PFS was 3.8 months (95% CI, 1.8-6.37) in the test group; the OS was 5.9 months (95% CI, 1.3-16.4) and the PFS was 1 month (95% CI, 0.7-1.33) in the placebo control group. These two studies showed that regorafenib did prolong the PFS, but the effect on prolonging OS was contradictory.
Lenvatinib is a novel antiangiogenic and orally acting multikinase inhibitor that targets VEGFR 1-3, FGFR 1-4, PDGFR-α, RET and KIT products (40). Lenvatinib treatment significantly improved the clinical outcomes (PFS and ORR) of patients with unresectable HCC compared with Sorafenib (41). In the two included articles on Lenvatinib, the children and adolescent populations were involved. From the experimental results, it can be seen that the effect of using Lenvatinib alone to treat osteosarcoma on OS and PFS is similar to the results of other trials using TKIs, which may further suggest that TKIs have little difference in treatment for different ages (as other included literature on TKIs also involves the adolescent population). But when Lenvatinib combined chemotherapy appears to be relatively beneficial for prolonging OS and PFS (Table 1; Figures 2, 3), TKIs combined chemotherapy for osteosarcoma may be a promising option, but may also face more side effects (Table 3). Apatinib inhibits VEGFR-2, thereby potently reducing tumor angiogenesis and decreasing microvessel density in tumors. Apatinib showed positive results in the treatment of gastric cancer, breast cancer, lung cancer, esophageal cancer and other tumors (42). The median PFS and median OS were 5.0 months (95% CI, 3.6-6.4) and 16 months (95% CI, 14.6-17.4) in a multicenter, single-arm, prospective phase II study of Apatinib for the treatment of recurrent nasopharyngeal carcinoma (43), however, the median PFS and OS of Apatinib in osteosarcoma treatment were 4.5 months (95% CI, 3.47-6.27) and 9.87 months (95% CI, 7.97-18.93), respectively (23). Differences between the results of these two studies may be related to the age and tumor type of patients. In this study, we found that Apatinib combined with PD-1 inhibitor (Camrelizumab) seemed to have more advantages in prolonging PFS of osteosarcoma patients, this may be related to the VEGFR inhibitors improved immunotherapeutic activity of PD-1/PD-L1 antibodies by enhancing the tumor infiltration of immune cells and reducing the immunosuppressive effects of myeloid-derived suppressor cells (17), however, the risk of serious AEs is also increasing. In another trial of Apatinib combined with camrelizumab for the treatment of triple negative breast cancer (44), the PFS of continuous dosing cohort was 3.7 months (95% CI 2.0-6.4), while that of intermittent dosing cohort was 1.9 months (95% CI 1.8-3.7), which was similar to the results of the trial included in this study. However, there is currently a lack of reliable evidence to support the priority choice of TKIs combined with PD-1 inhibitors for the treatment of advanced osteosarcoma. Cabozantinib, a TKI targeting VEGFR2 and MET (a transmembrane tyrosine kinase receptor), decreased the proliferation and migration of osteosarcoma cells, and the production of RANK ligands via inhibition of the ERK and AKT signaling pathways (45). Cabozantinib improved the OS rate and prolonged the PFS of patients with advanced renal cell carcinoma or differentiated thyroid carcinoma (46, 47). Application of Cabozantinib showed that the 4-month progression-free survival was 71% (95% CI 55-83) (25). The 21 of 41 patients had tumor shrinkage and 7 patients had objective response. The tumor shrinkage rate of the targeted therapy for osteosarcoma was the highest until now. TAS-115 is an oral multikinase inhibitor targeting the MET proto-oncogene, VEGFR, and colony-stimulating factor 1 receptor, which helps to inhibit the tumor growth and the osteoclast differentiation. TAS-115 showed an anti-tumor activity (bone scan index, BSI) in a clinical trial of prostate cancer bone metastasis, which alleviated the bone pain by reducing osteoclast activity and contributed to the improvement of quality of life (48). TAS-115 also reduced the BSI and improved the progression free rates in patients with advanced osteosarcoma (26).
Both PD-1 inhibitors and TKIs show AEs, which are within the controllable range through drug withdrawal or dose adjustment. Fatigue, blood cell abnormalities and enzyme abnormalities are the most common, but none of them have drug-related lethal reactions. However, we should always pay close attention to the AEs of immune checkpoint inhibitors.
Since the most reliable efficacy information about the test drugs is provided by the randomized controlled clinical trials, limitation of this study is existed because several non-randomized clinical trials were included. Therefore, PD-1 inhibitors and TKIs in the treatment of advanced osteosarcoma still need to be further investigated by high-quality randomized controlled clinical studies.
Conclusion
Compared with PD-1 inhibitors, TKIs showed a comparative advantage in improving the OS and are more beneficial in prolonging the PFS of patients with advanced osteosarcoma. Moreover, PD-1 inhibitors combined with TKIs is more prospective then PD-1 inhibitors or TKIs only in the treatment of advanced osteosarcoma patients, but more serious AEs may occur. We should always pay attention to the adverse drug reactions. It is still a long way to go to develop and explore new drugs with high efficiency and low toxicity.
Compared with PD-1 inhibitors, TKIs seem to have a relative advantage in improving OS and prolonging PFS, but there is currently no evidence to suggest that TKIs are superior to PD-1 inhibitors in treating advanced osteosarcoma. In addition, PD-1 inhibitors combined with TKIs or TKIs combined with chemotherapy in the treatment of advanced osteosarcoma are worth further exploration and have potential applications, but more serious AEs may occur. We should always pay attention to the adverse drug reactions. There is still a long way to go to develop and explore new drugs or combination formulations with high efficiency and low toxicity.
Author contributions
Research: BS, XS. Article writing: BS. Interpretation of data: BS, JC, PZ. Software application: XM, CZ. Article guidance and control: YW, YY. All authors contributed to the article and approved the submitted version.
Funding
Our current work is supported by grants from (1) Shanghai Top Priority Research Center construction project (No. 2022ZZ01009 for YW), (2) National Key R&D Program of China (2020YFE0201600), (3) National Nature Science Foundation (81973877 and 82174408), (4) Research Projects within Budget of Shanghai University of Traditional Chinese Medicine (2021LK047).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Smeland S, Bielack SS, Whelan J, Bernstein M, Hogendoorn P, Krailo MD, et al. Survival and prognosis with osteosarcoma: outcomes in more than 2000 patients in the EURAMOS-1 (European and American osteosarcoma study) cohort. Eur J Cancer (2019) 109:36–50. doi: 10.1016/j.ejca.2018.11.027
2. Klein MJ, Siegal GP. Osteosarcoma: anatomic and histologic variants. Am J Clin Pathol (2006) 125(4):555–81. doi: 10.1309/UC6KQHLD9LV2KENN
3. Prudowsky ZD, Yustein JT. Recent insights into therapy resistance in osteosarcoma. Cancers (Basel) (2020) 13(1):83. doi: 10.3390/cancers13010083
4. Benjamin RS. Adjuvant and neoadjuvant chemotherapy for osteosarcoma: a historical perspective. Adv Exp Med Biol (2020) 1257:1–10. doi: 10.1007/978-3-030-43032-0_1
5. Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence and survival rates from 1973 to 2004 data from the surveillance, epidemiology, and end results program. Cancer (2009) 115(7):1531–43. doi: 10.1002/cncr.24121
6. Marko TA, Diessner BJ, Spector LG. Prevalence of metastasis at diagnosis of osteosarcoma: an international comparison. Pediatr Blood Cancer (2016) 63(6):1006–11. doi: 10.1002/pbc.25963
7. Duffaud F, Egerer G, Ferrari S, Rassam H, Boecker U, Bui-Nguyen B. A phase II trial of second-line pemetrexed in adults with advanced/metastatic osteosarcoma. Eur J Cancer (2012) 48(4):564–70. doi: 10.1016/j.ejca.2011.12.015
8. Massimo B, Giovanni G, Stefano F, Biasin E, Brach del Preve A, Aliberti S, et al. Phase 2 trial of two courses of cyclophos-phamide and etoposide for relapsed high-risk osteosarcoma patients. Cancer (2009) 115(13):2980–7. doi: 10.1002/cncr.24368
9. Song BS, Seo J, Kim DH, Lim JS, Yoo JY, Lee JA. Gemcitabine and docetaxel for the treatment of children and adolescents with recurrent or refractory osteosarcoma: Korea cancer center hospital experience. Pediatr Blood Cancer (2014) 61(8):1376–81. doi: 10.1002/pbc.25035
10. Schuster M, Nechansky A, Kircheis R. Cancer immunotherapy. Biotechnol J (2006) 1(2):138–47. doi: 10.1002/biot.200500044
11. Bellmunt J, de Wit R, Vaughn DJ, Fradet Y, Lee JL, Fong L, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med (2017) 376(11):1015–26. doi: 10.1056/NEJMoa1613683
12. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab versus docetaxel in advanced nonsquamous non–Small-Cell lung cancer. N Engl J Med (2015) 373(17):1627–39. doi: 10.1056/NEJMoa1507643
13. Jiang Y, Chen M, Nie H, Yuan Y. PD-1 and PD-L1 in cancer immunotherapy: clinical implications and future considerations. Hum Vaccin Immunother (2019) 15(5):1111–22. doi: 10.1080/21645515.2019.1571892
14. Chen C, Xie L, Ren T, Huang Y, Xu J, Guo W. Immunotherapy for osteosarcoma: fundamental mechanism, rationale, and recent breakthroughs. Cancer Lett (2021) 500:1–10. doi: 10.1016/j.canlet.2020.12.024
15. Wen Y, Tang F, Tu C, Hornicek F, Duan Z, Min L. Immune checkpoints in osteosarcoma: recent advances and therapeutic potential. Cancer Lett (2022) 547:215887. doi: 10.1016/j.canlet.2022.215887
16. Xu W, Ye C, Qing X, Liu S, Lv X, Wang W, et al. Multi-target tyrosine kinase inhibitor nanoparticle delivery systems for cancer therapy. Mater Today Bio (2022) 16:100358. doi: 10.1016/j.mtbio.2022.100358
17. Huang L, Jiang S, Shi Y. Tyrosine kinase inhibitors for solid tumors in the past 20 years (2001-2020). J Hematol Oncol (2020) 13(1):143. doi: 10.1186/s13045-020-00977-0
18. Albarrán V, Villamayor ML, Chamorro J, Rosero DI, Pozas J, San Román M, et al. Receptor tyrosine kinase inhibitors for the treatment of recurrent and unresectable bone sarcomas. Int J Mol Sci (2022) 23(22):13784. doi: 10.3390/ijms232213784
19. Boye K, Longhi A, Guren T, Lorenz S, Næss S, Pierini M, et al. Pembrolizumab in advanced osteosarcoma: results of a single-arm, open-label, phase 2 trial. Cancer Immunol Immunother (2021) 70(9):2617–24. doi: 10.1007/s00262-021-02876-w
20. Le Cesne A, Marec-Berard P, Blay JY, Gaspar N, Bertucci F, Penel N, et al. Programmed cell death 1 (PD-1) targeting in patients with advanced osteosarcomas: results from the PEMBROSARC study. Eur J Cancer (2019) 119:151–7. doi: 10.1016/j.ejca.2019.07.018
21. Davis LE, Bolejack V, Ryan CW, Ganjoo KN, Loggers ET, Chawla S, et al. Randomized double-blind phase II study of regorafenib in patients with metastatic osteosarcoma. J Clin Oncol (2019) 37(16):1424–31. doi: 10.1200/JCO.18.02374
22. Gaspar N, Campbell-Hewson Q, Gallego Melcon S, Locatelli F, Venkatramani R, Hecker-Nolting S, et al. Phase I/II study of single-agent lenvatinib in children and adolescents with refractory or relapsed solid malignancies and young adults with osteosarcoma (ITCC-050). ESMO Open (2021) 6(5):100250. doi: 10.1016/j.esmoop.2021.100250
23. Xie L, Xu J, Sun X, Tang X, Yan T, Yang R, et al. Apatinib for advanced osteosarcoma after failure of standard multimodal therapy: an open label phase II clinical trial. Oncologist (2019) 24(7):e542–50. doi: 10.1634/theoncologist.2018-0542
24. Duffaud F, Mir O, Boudou-Rouquette P, Piperno-Neumann S, Penel N, Bompas S, et al. Efficacy and safety of regorafenib in adult patients with metastatic osteosarcoma: a non-comparative, randomised, double-blind, placebo-controlled, phase 2 study. Lancet Oncol (2019) 20(1):120–33. doi: 10.1016/S1470-2045(18)30742-3
25. Italiano A, Mir O, Mathoulin-Pelissier S, Penel N, Piperno-Neumann S, Bompas E, et al. Cabozantinib in patients with advanced Ewing sarcoma or osteosarcoma (CABONE): a multicentre, single-arm, phase 2 trial. Lancet Oncol (2020) 21(3):446–55. doi: 10.1016/S1470-2045(19)30825-3
26. Kawai A, Naka N, Shimomura A, Takahashi S, Kitano S, Imura Y, et al. Efficacy and safety of TAS-115, a novel oral multi-kinase inhibitor, in osteosarcoma: an expansion cohort of a phase I study. Invest New Drugs (2021) 39(6):1559–67. doi: 10.1007/s10637-021-01107-4
27. Gaspar N, Venkatramani R, Hecker-Nolting S, Melcon SG, Locatelli F, Bautista F, et al. Lenvatinib with etoposide plus ifosfamide in patients with refractory or relapsed osteosarcoma (ITCC-050): a multicentre, open-label, multicohort, phase 1/2 study. Lancet Oncol (2021) 22(9):1312–21. doi: 10.1016/S1470-2045(21)00387-9
28. Xie L, Xu J, Sun X, Guo W, Gu J, Liu K, et al. Apatinib plus camrelizumab (anti-PD1 therapy, SHR-1210) for advanced osteosarcoma (APFAO) progressing after chemotherapy: a single-arm, openlabel, phase 2 trial. J Immunother Cancer (2020) 8(1):e000798. doi: 10.1136/jitc-2020-000798
29. Dong H, Strome SE, Salomao DR, Tamura H, Hirano F, Flies DB, et al. Tumor-associated B7-H1 promotes T-cell apoptosis: a potential mechanism of immune evasion. Nat Med (2002) 8(8):793–800. doi: 10.1038/nm730
30. Kwok G, Yau TC, Chiu JW, Tse E, Kwong YL. Pembrolizumab (Keytruda). Hum Vaccin Immunother (2016) 12(11):2777–89. doi: 10.1080/21645515.2016.1199310
31. Joseph RW, Elassaiss-Schaap J, Kefford R, Hwu WJ, Wolchok JD, Joshua AM, et al. Baseline tumor size is an independent prognostic factor for overall survival in patients with melanoma treated with pembrolizumab. Clin Cancer Res (2018) 24(20):4960–7. doi: 10.1158/1078-0432.CCR-17-2386
32. Pelster MS, Mott F, Lewin J. Pembrolizumab-induced mucositis in a patient with recurrent hypopharynx squamous cell cancer. Laryngoscope (2020) 130(4):E140–3. doi: 10.1002/lary.28038
33. Wu J, Waxman DJ. Immunogenic chemotherapy: dose and schedule dependence and combination with immunotherapy. Cancer Lett (2018) 419:210–21. doi: 10.1016/j.canlet.2018.01.050
34. Xie L, Ji T, Guo W. Anti-angiogenesis target therapy for advanced osteosarcoma (Review). Oncol Rep (2017) 38(2):625–36. doi: 10.3892/or.2017.5735
35. Kaya M, Wada T, Akatsuka T, Kawaguchi S, Nagoya S, Shindoh M, et al. Vascular endothelial growth factor expression in untreated osteosarcoma is predictive of pulmonary metastasis and poor prognosis. Clin Cancer Res (2000) 6(2):572–7.
36. Zhou Y, Wu C, Lu G, Hu Z, Chen Q, Du X. FGF/FGFR signaling pathway involved resistance in various cancer types. J Cancer (2020) 11(8):2000–7. doi: 10.7150/jca.40531
37. Mross K, Frost A, Steinbild S, Hedbom S, Büchert M, Fasol U, et al. A phase I dose–escalation study of regorafenib (BAY 73–4506), an inhibitor of oncogenic, angiogenic, and stromal kinases, in patients with advanced solid tumors. Clin Cancer Res (2012) 18(9):2658–67. doi: 10.1158/1078-0432.CCR-11-1900
38. Mir O, Brodowicz T, Italiano A, Wallet J, Blay JY, Bertucci F, et al. Safety and efficacy of regorafenib in patients with advanced soft tissue sarcoma (REGOSARC): a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol (2016) 17(12):1732–42. doi: 10.1016/S1470-2045(16)30507-1
39. Niu XH. Interpretation of 2020 NCCN clinical practice guidelines in oncology-bone cancer. Zhonghua Wai Ke Za Zhi (2020) 58(6):430–4. doi: 10.3760/cma.j.cn112139-20200204-00061
40. Matsui J, Funahashi Y, Uenaka T, Watanabe T, Tsuruoka A, Asada M. Multi-kinase inhibitor E7080 suppresses lymph node and lung metastases of human mammary breast tumor MDA-MB-231 via inhibition of vascular endothelial growth factor-receptor (VEGF-r) 2 and VEGF-R3 kinase. Clin Cancer Res (2008) 14(17):5459–65. doi: 10.1158/1078-0432.CCR-07-5270
41. Yamashita T, Kudo M, Ikeda K, Izumi N, Tateishi R, Ikeda M, et al. REFLECT-a phase 3 trial comparing efficacy and safety of lenvatinib to sorafenib for the treatment of unresectable hepatocellular carcinoma: an analysis of Japanese subset. J Gastroenterol (2020) 55(1):113–22. doi: 10.1007/s00535-019-01642-1
42. Zhao D, Hou H, Zhang X. Progress in the treatment of solid tumors with apatinib: a systematic review. Onco Targets Ther (2018) 11:4137–47. doi: 10.2147/OTT.S172305
43. Ruan X, Liang JH, Pan Y, Cai R, Zhang RJ, He Z, et al. Apatinib for the treatment of metastatic or locoregionally recurrent nasopharyngeal carcinoma after failure of chemotherapy: a multicenter, single-arm, prospective phase 2 study. Cancer (2021) 127(17):3163–71. doi: 10.1002/cncr.33626
44. Liu J, Liu Q, Li Y, Li Q, Su F, Yao H, et al. Efficacy and safety of camrelizumab combined with apatinib in advanced triple-negative breast cancer: an open-label phase II trial. J Immunother Cancer (2020) 8(1):e000696. doi: 10.1136/jitc-2020-000696
45. Assi T, Watson S, Samra B, Rassy E, Le Cesne A, Italiano A, et al. Targeting the VEGF pathway in osteosarcoma. Cells (2021) 10(5):1240. doi: 10.3390/cells10051240
46. Choueiri TK, Escudier B, Powles T, Tannir NM, Mainwaring PN, Rini B, et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): final results from a randomised, open-label, phase 3 trial. Lancet Oncol (2016) 17(7):917–27. doi: 10.1016/S1470-2045(16)30107-3
47. Brose MS, Robinson B, Sherman SI, Krajewska J, Lin CC, Vaisman F, et al. Cabozantinib for radioiodine-refractory differentiated thyroid cancer (COSMIC-311): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol (2021) 22(8):1126–38. doi: 10.1016/S1470-2045(21)00332-6
Keywords: immunotherapy, PD-1 inhibitors, protein tyrosinase inhibitors, advanced osteosarcoma, meta-analysis
Citation: Shi B, Chang J, Sun X, Ma X, Zhao P, Zhou C, Wang Y and Yang Y (2023) A meta-analysis: the clinical value of PD-1 inhibitor or protein tyrosine kinase inhibitors in the treatment of advanced osteosarcoma. Front. Oncol. 13:1148735. doi: 10.3389/fonc.2023.1148735
Received: 23 January 2023; Accepted: 26 May 2023;
Published: 12 June 2023.
Edited by:
Matiullah Khan, AIMST University, MalaysiaReviewed by:
Lei Guo, Texas A and M University, United StatesMarcus Breese, University of California, San Francisco, United States
Copyright © 2023 Shi, Chang, Sun, Ma, Zhao, Zhou, Wang and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yanping Yang, eWFucGluZ3lhbmdrc0AxNjMuY29t; Yongjun Wang, d2FuZ3lvbmdqdW4xMDE0QDE2My5jb20=