 Fang Cheng
Fang Cheng Qiang Li1,2†
Qiang Li1,2† Weiming Li
Weiming Li Yu Zhang
Yu Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 05 April 2023
Sec. Hematologic Malignancies
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1146108
This article is part of the Research Topic Reviews in Hematologic Malignancies: 2023 View all 15 articles
With the advent of tyrosine kinase inhibitors (TKIs), the treatment prospects of chronic myeloid leukemia (CML) have changed markedly. This innovation can lengthen the long-term survival of patients suffering from CML. However, long-term exposure to TKIs is accompanied by various adverse events (AEs). The latter affect the quality of life and compliance of patients with CML, and may lead to serious disease progression (and even death). Recently, increasing numbers of patients with CML have begun to pursue a dose optimization strategy. Dose optimization may be considered at all stages of the entire treatment, which includes dose reduction and discontinuation of TKIs therapy. In general, reduction of the TKI dose is considered to be an important measure to reduce AEs and improve quality of life on the premise of maintaining molecular responses. Furthermore, discontinuation of TKIs therapy has been demonstrated to be feasible and safe for about half of patients with a stable optimal response and a longer duration of TKI treatment. This review focuses mainly on the latest research of dose optimization of imatinib, dasatinib, and nilotinib in CML clinical trials and real-life settings. We consider dose reduction in newly diagnosed patients, or in optimal response, or for improving AEs, either as a prelude to treatment-free remission (TFR) or as maintenance therapy in those patients unable to discontinue TKIs therapy. In addition, we also focus on discontinuation of TKIs therapy and second attempts to achieve TFR.
Chronic myeloid leukemia (CML) is a myeloproliferative tumor formed by clonal adult cases of leukemia (1). With the advent of tyrosine kinase inhibitors (TKIs) targeting BCR::ABL1, the therapeutic prospect of CML has changed markedly (2). The long-term survival of patients with CML in the chronic phase (CP) has become close to normal life expectancy (3). Imatinib, dasatinib and nilotinib are the most commonly used TKIs for CML patients in clinical practice in China.
Long-term treatment with TKIs is accompanied with various adverse events (AEs) that significantly affect the quality of life and compliance of patients with CML, and have the potential to cause significant disease progression and mortality. Severe AEs associated with second-generation TKIs have also been reported. These include pleural effusion (PE) and pulmonary hypertension induced by dasatinib (4, 5) as well as nilotinib-related dyslipidemia and arterial thrombosis (6, 7).
Recently, increasing numbers of patients with CML have begun to pursue a dose optimization strategy, which included dose reduction and discontinuation of TKIs therapy. Dose reduction of TKIs has been suggested to be safe and feasible, and to elicit an optimal response, in patients with CML. Also, the prevention and management of AEs must also be considered to improve patient compliance and reduce the risk of treatment interruption (8, 9). Fassoni and colleagues developed a patient data-based mathematical model which suggested that a reduction ≥50% of the full dose of a TKI did not exacerbate outcomes from long-term treatment (10). Importantly, the dose reduction of TKIs should be considered as early as possible, but the clinical benefit of this approach is controversial if chronic toxicity occurs, especially in some specific settings (11). Furthermore, some patients with a sustained deep molecular response (DMR, BCR::ABL1IS ≤ 0.01%) can achieve relatively long-lasting safe discontinuation of TKIs therapy [i.e., treatment-free response (TFR)].
In recent years, several clinical trials and real-life practices have indicated that treatment discontinuation has become a new therapeutic goal for patients with CML who are stable and have a DMR (12, 13). However, about half of patients have molecular recurrence and need re-introduction of TKIs therapy. Imatinib was first applied to the treatment of CML two decades ago, and only 5%–10% of patients can maintain TFR (14). Eighty percent of patients continue to need long-term therapy with a TKI to achieve long-term survival (though 20% of them meet the conditions for treatment discontinuation) (15). Therefore, this review focuses mainly on the latest research on the dose optimization of the TKIs imatinib, dasatinib, and nilotinib in patients with CML. This information includes dose reduction (Table 1) and TFR (Table 2). In this way, we aim to provide important references for the formulation of individualized therapeutic regimen for patients with CML.
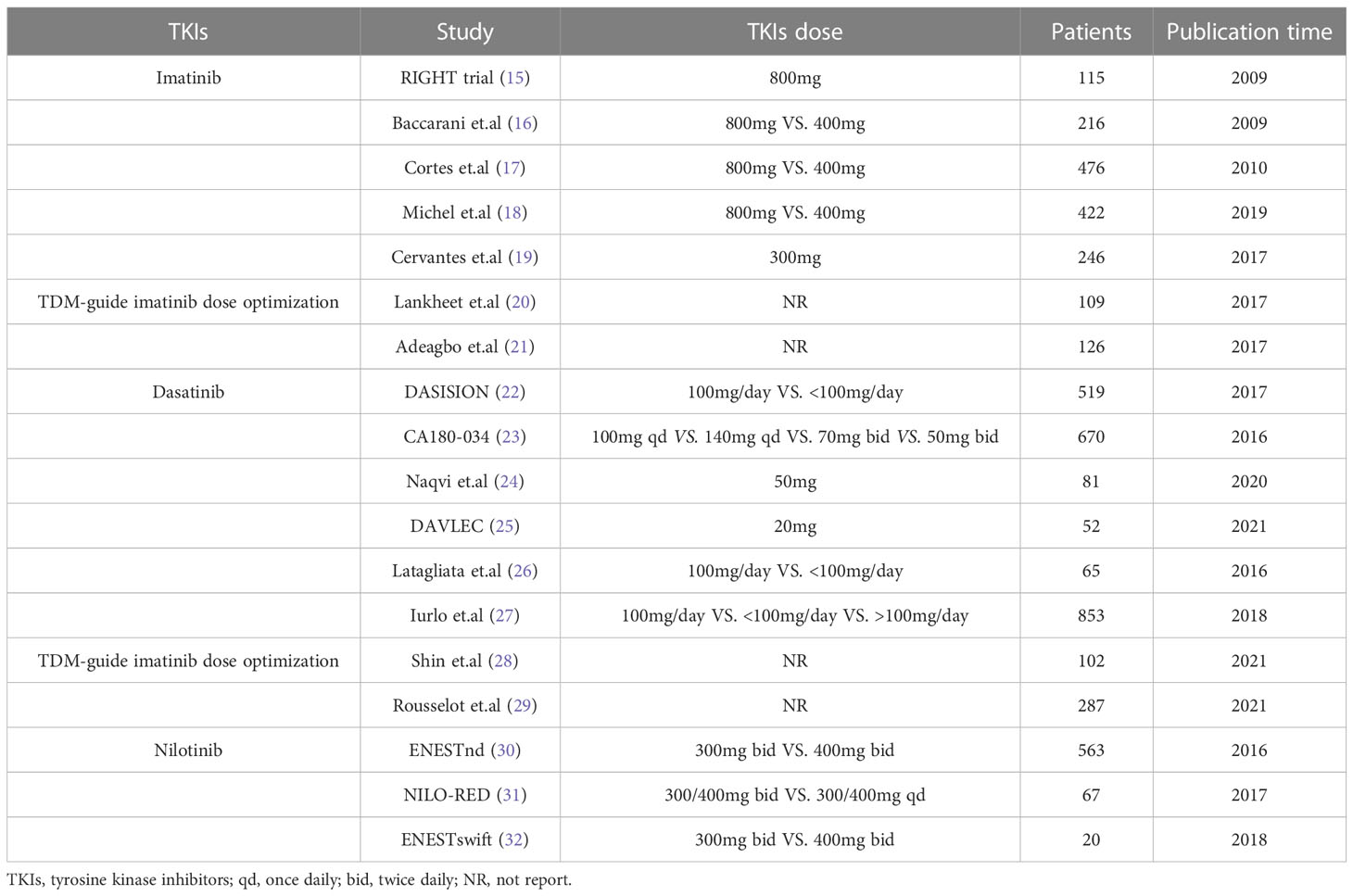
Table 1 Clinical trials evaluating different imatinib, dasatinib and nilotinib doses.
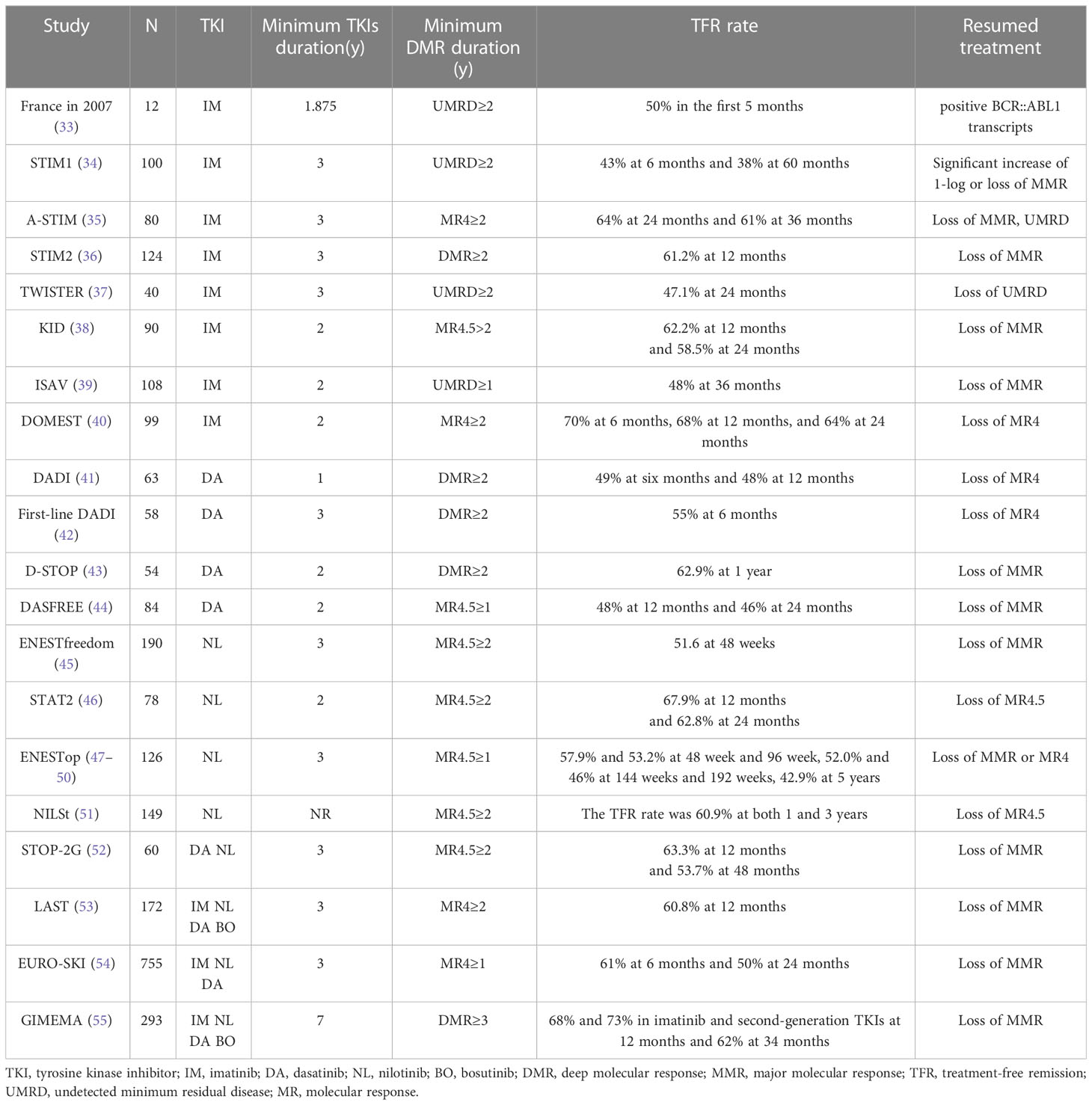
Table 2 Characteristics of TKIs discontinuation trials.
Several clinical trials have explored the efficacy of high-dose imatinib (800 mg/day) treatment compared with standard-dose therapy (16–19). High-dose imatinib appeared to elicit a faster major molecular response (MMR, BCR::ABL1IS ≤ 0.1%), but the prevalence of MMR was similar at 1 years or 2 years between the two groups being assessed. However, an increased prevalence of severe AEs and worse compliance by patients was reported in the high-dose-imatinib arm. As a result, patients received imatinib at 800 mg/day initially which was later reduced to 400 mg/day. In addition, dose reduction was accompanied by a reduction in the prevalence of AEs and medical costs, and could improve patient compliance. Claudiani and coworkers (8) conducted a retrospective study of 246 patients with CML receiving treatment with a lower dose of a TKI (imatinib, n = 90; dasatinib, n = 88; nilotinib, n = 81; bosutinib, n = 39) after achievement of MMR because of intolerable AEs. A “lower dose” of a TKI (mg/day) was defined as 200 or 300 for imatinib, 70, 50, 40 or ≤20 for dasatinib; 400, 300, or ≤200 for nilotinib; 300, 200, or <200 for bosutinib. Their findings suggested that dose reduction should not be recommended as routine clinical practice, but could be an acceptable and safe option for patients who cannot tolerate a standard dose of a TKI. Cervantes and collaborators (56) found that a reduction to 300 mg/day in 43 patients with CML who received imatinib (400 mg/day) initially as first-line treatment with a sustained DMR improved tolerability significantly and maintained a DMR continuously.
Therapeutic drug monitoring (TDM) is gradually becoming a practical tool to achieve individualized medicine for patients receiving targeted drugs (57). Peng and colleagues showed that fixed-dose imatinib showed high inter-patient variability to plasma exposure in patients with CML (58). An imatinib concentration in plasma >1000 ng/mL in patients with CML can lead to a beneficial clinical outcome (59, 60). Therefore, a TDM-based dose-adjustment strategy could improve the efficacy, and reduce the toxicity and medical cost, of imatinib therapy (20). In daily practice, Lankheet and colleagues (21) monitored the proportion of patients who reached the target trough concentration (Cmin) of a TKI (imatinib, sunitinib, or pazopanib) after a TDM-based dose-adjustment strategy. The proportion of patients with the target Cmin increased from 38% to 64%, which suggested that a TDM-based dose-adjustment strategy may be an effective strategy to enable patients who received a TKI to achieve the target Cmin. The population pharmacokinetics of imatinib in patients with CML in Nigeria (61) showed that treatment with a standard dose of imatinib may not elicit the desired effect in most patients, and that exposure to low concentrations continuously might lead to drug resistance. They suggested the need for a TDM-guided dose- adjustment strategy of imatinib in this population. In summary, those data indicated that dose reduction could be a feasible and safe option for patients with a stable optimal response but who cannot tolerate a standard dose of imatinib (22). If possible, the imatinib concentration in plasma could be monitored to provide an important reference for the dose adjustment of imatinib.
Several studies have explored the efficacy and safety of standard-dose dasatinib (100 mg/day) compared with low-dose therapy (<100 mg/day) in clinical trials and real-life settings. A retrospective analysis of the DASISION trial (23) revealed that dose reduction of dasatinib could maintain a superior prevalence of MMR while reducing the risk of dasatinib-related AEs. Of 65 patients with CML (age >65 years) receiving first-line treatment with dasatinib (100 mg/day VS. <100 mg/day),10 patients who required permanent drug withdrawal due to toxicity all received an initial dose of 100 mg/day (24). Iurlo and colleagues (25) retrospectively evaluated 853 CML patients who received dasatinib as first-line and second-line therapy (100 mg/day VS. <100 mg/day). A total of 196 episodes of PE (23.0%) were identified, and 70.4% of PE events were observed in patients who received 100 mg/day.
The CA180-034 study (26) enrolled patients with CML who were resistant and intolerant to imatinib and who were switched to dasatinib. The result of 7-year follow-up indicated that the clinical response at 100 mg/day was similar to that of 70-mg twice daily or 140 mg/day, and was more beneficial in terms of toxicity. Initial half-dose dasatinib therapy (50 mg/day) was suggested to be a safe option for newly diagnosed CP-CML patients. The clinical response and toxicity profile of initial treatment with half-dose dasatinib were more favorable compared with those documented in the DASISION trial (27). The DAVLEC study (28) suggested that low-dose dasatinib (20 mg/day) as the initial dose for older patients with newly diagnosed CP-CML was worthy of consideration.
Dasatinib exposure may be related to the clinical response and toxicity profile. The dose-limiting toxicities (DLTs) and clinical response of dasatinib were analyzed in patients with CP-CML at 17 hospitals in South Korea (62). Those results suggested that the initial dasatinib dose could be reduced to 80 mg/day according to dose adjusted for bodyweight (dose/BW) in South Korean CML patients, especially for those with lower BW. Mizuta and coworkers found that Patients experienced a higher risk of altered treatment with a higher Cmin/D/W (dasatinib concentration adjusted by dose (g), and bodyweight (kg)) (63). Therefore, TDM-guided dose-adjustment strategy may have potential benefits for dasatinib treatment (29). Rousselot and co-workers evaluated whether TDM could reduce the prevalence of dasatinib-induced AEs at 12 months (30). All eligible patients received an initial dose of 100 mg/day of dasatinib, followed by assessment of the Cmin of dasatinib. Patients were assigned randomly to a dose-reduction strategy (TDM) group and standard-dose strategy (control) group according to Cmin ≥3 nmol/L. The cumulative prevalence of PE was reduced significantly in the TDM group (15% vs. 4%, 35% vs. 11%, and 39% vs.12% at 1, 2 and 3 years, respectively, p = 0.0094), whereas the prevalence of MMR was similar. A TDM-guided dose-adjustment strategy for dasatinib was feasible and resulted in a significant reduction in the incidence of PE events without impairing the MMR rate upon long-term treatment.
The ENESTnd study (64) reported that nilotinib (400 mg, twice daily (bid) VS. 300 mg, bid) had equivalent efficacy, but high-dose therapy led to longer 5-year overall survival compared with imatinib. However, a higher prevalence of cardiovascular events was observed in the high-dose arm. Furthermore, the ENESTswift trial (31) suggested crossover with nilotinib (300 mg, bid) to be efficacious and well tolerated in most patients treated with nilotinib as second-line therapy. In the NILO-RED study (32), patients were recommended to receive dose adjustments to a lower-dose once-daily (qd) regimen after achieving a MMR with standard-dose nilotinib bid schedule (first-line 300 mg, bid; and second-line 400 mg, bid) solely in case of severe toxicity. Switching to a nilotinib qd regimen as maintenance therapy after achievement of MMR on standard-dose schedule is feasible and safe in CP-CML patients regardless of prior treatment history.
In recent years, the experience of discontinuation of TKIs therapy in patients with CML has been reported worldwide. A research team in France reported the first key study in 2007 (33). They suggested that a certain proportion of patients with molecular diseases not detected for ≥2 years could discontinue TKIs treatment and maintain molecular remission. One-hundred patients with CP-CML with undetectable molecular disease for ≥2 years were involved in the STIM1 trial (34). Molecular relapse was defined as a significant increase of 1-log reduction or loss of MMR in two consecutive samples. The prevalence of molecular recurrence-free survival was 43% at 6 months and 38% at 60 months, respectively. The cumulative prevalence of molecular recurrence was estimated to be ~60%. Furthermore, 55 patients who suffered molecular relapse achieved a faster DMR after resumption of TKIs treatment, and no patient had disease progression or mutations of the ABL1 kinase domain. Eighty patients with CML who received imatinib treatment were involved in the A-STIM study (35). Molecular relapse was defined as loss of MMR. The TFR prevalence was 64% at 24 months and 61% at 26 months, respectively. In the STIM2 study, 50% of patients continued to have TFR at 24 months (36). Forty patients with CP-CML enrolled in the TWISTER study in Australia (37) received imatinib treatment for >3 years and achieved 4.5-log reduction (MR4.5) for ≥2 years. Molecular relapse was defined as loss of MMR. At 2-year follow-up, the TFR prevalence was 47.1%, and most molecular relapses occurred in the first 4 months after treatment discontinuation. No patient had disease progression or mutations of the ABL1 kinase domain, and imatinib therapy was restarted successfully in all patients who suffered molecular relapse. The Korean Imatinib Discontinuation (KID) study (38) aimed to identify the predictors for safe and successful discontinuation of imatinib therapy, and 90 patients with CML were enrolled. The probability of achieving a sustained MMR at 12 months and 24 months was 62.2% and 58.5%, respectively. The ISAV study in Italy (39) enrolled CML patients with 112 who received imatinib treatment and who had undergone interferon-α treatment previously. If patients maintained MR4.5 for ≥2 years, then imatinib treatment was stopped. In that study, 50.9% of patients lost their MMR. The DOMEST trial (40) was a multicenter phase-II trial conducted in Japan to assess the clinical efficacy and safety of discontinuing imatinib therapy in patients with CML. Patients with sustained MR4.0 for ≥2 years were included. Molecular relapse was defined as the loss of MR4.0, and resumed dasatinib or other TKIs therapy. The prevalence of molecular recurrence-free survival was 69.6%, 68.6%, and 64.3% at 6, 12, and 24 months, respectively.
Lee and collaborators (65) aimed to identify the predictors for successful discontinuation of imatinib therapy, and 48 patients with CP-CML were enrolled. Patients were eligible for therapy cessation after receiving imatinib treatment for ≥3 years, and to maintain undetectable minimal residual disease (MRD) for ≥2 years. That study also included 20 patients who suffered a post-transplant relapse. Molecular relapse was defined as loss of UMRD or MMR. After a median follow-up of 15.8 months, nine patients lost UMRD and MMR in the non-transplant group, whereas all patients in the post-transplantation group maintained UMRD. Previous transplantation, imatinib duration, and UMRD duration were significantly associated with sustained molecular responses. Campiotti and coworkers (66) conducted a systematic review to assess the long-term safety of discontinuation of imatinib therapy in patients with CML. Approximately 50% of patients had TFR, and no death occurred 2 years after discontinuation of imatinib therapy. Those results indicated that discontinuation of imatinib therapy was feasible and safe for patients with CP-CML who had a sustained DMR.
STOP-2G (52) was the first multicenter observational study to investigate the feasibility of discontinuation of second-generation TKIs therapy. The discontinuation criteria were patients with ≥3 years for first-line or subsequent lines of dasatinib or nilotinib therapy with sustained MR4.5 for >2 years. Molecular relapse was defined as loss of MMR. Sixty patients were enrolled and the follow-up was 12 months: 43.3% of patients suffered a relapse at a median of 4 months. The TFR prevalence at 1 year and 2 years was 63.3% and 53.6%, respectively. The DADI trial (41) in Japan included 63 patients with CML with a sustained DMR for >1 year. Molecular relapse was considered to be the loss of DMR at any time point. They found that 52.4% of patients experienced a relapse at a median follow-up of 20 months, and all patients regained DMR 6 months after resumption of dasatinib therapy. The first-line DADI trial (42) was a multicenter phase-II trial in 23 Japanese hospitals, and aimed to assess molecular relapse-free survival at 6 months after discontinuation therapy. Fifty-eight patients with CML received dasatinib as first-line treatment and had a sustained DMR for >1 year. Thirty-two patients maintained TFR at 6 months and TFR prevalence at 6 months was 55.2%. The D-STOP trial (43) explored the long-term outcome of 54 patients with CML who stopped dasatinib treatment after achieving a sustained DMR for ≥2 years. At a median follow-up of 16.2 months, 12 patients suffered molecular relapse. The TFR prevalence at 12 months and 36 months was 62.9% and 44.4%, respectively. The DASFREE study (44) enrolled 74 patients with CML who received dasatinib treatment for >2 years and maintained MR4.5 for ≥1 year. At 2-year follow-up, 51% of patients in the first-line-treatment arm and 42% in the second-line-treatment arm continued to have TFR. The prevalence of TFR was 44% for patients who were resistant or intolerant to first-line dasatinib treatment.
A meta-analysis was conducted in patients with CML under a stable DMR to assess the prevalence of TFR and the long-term safety of discontinuation of second-generation TKIs therapy (67). Five single-armed, prospective cohort studies were included, and 517 patients were enrolled. The overall estimated TFR prevalence at a follow-up of 12 months and 24 months was 57% and 53%, respectively. Molecular recurrence occurred mainly in first 12 months after discontinuation therapy. Investigators discovered that 96.5% of patients who resumed TKIs treatment after molecular relapse could achieve MMR rapidly. During 2-year follow-up, four patients died (including two non-CML-related deaths: one died from arterial hemorrhage during the consolidation phase, and the other death was due to heart failure).
The phase-II ENESTFreedom trial (45) was the first to evaluate discontinuation of nilotinib therapy. It enrolled 215 patients who received first-line nilotinib treatment and had stable MR4.5 for ≥2 years. All patients continued to receive 1 year of consolidated nilotinib treatment after enrollment, and 190 patients underwent discontinuation of nilotinib treatment. 48.9% of patients maintained TFR at 96-week follow-up. Furthermore, TFR prevalence was closely associated with the Sokal score at the diagnosis (low risk: 61.3%; intermediate risk: 50.0%; high risk: 28.6%). At 5-year follow-up, 81 patients (42.6%) continued to have TFR, and 76 (40.0%) had MR4.5. Patients who suffered a relapse regained MMR (98.9%) and 92.3% had a DMR (68). The STAT2 trial (46) evaluated the efficacy of 2-year consolidated nilotinib (300 mg, bid) therapy for achieving TFR in CML patients with sustained DMR. Molecular relapse was defined as loss of DMR. Fifty-three patients continued to have TFR in the first 12 months among the 78 patients who were eligible to discontinue nilotinib therapy. The TFR prevalence at 3 years was estimated to be 62.8%. Of the 29 patients who suffered a relapse, 25 patients regained DMR after treatment resumption. The ENESTop study evaluated the TFR prevalence in patients with CP-CML treated with TKIs for >3 years and who achieved a sustained DMR after replacing imatinib with nilotinib. The TFR prevalence was 57.9% and 53.2% at 48 weeks and 96 weeks, respectively (47). Treatment-free survival was 52.0% and 46% at 144 weeks (48) and 192 weeks (49). At 5-year follow-up (50), 42.9% (54/126) of patients continued to have TFR. Of the 59 patients who lost the MMR or DMR and were re-introduced to nilotinib treatment, 98.3% regained the MMR, 94.9% regained MR4, and 93.2% regained MR4.5. Overall, AE rates decreased over the 5 years of TFR, and no patients suffered disease progression or CML-related death. The NILSt study (51) enrolled patients with DMR who received nilotinib consolidation therapy for ≤24 months, and who maintained MR4.5 proceeded to discontinuation of nilotinib treatment. Molecular relapse was defined as loss of MR4.5. Eighty-seven patients (58.4%) underwent discontinuation of nilotinib therapy. The TFR prevalence was 60.9% at 1 year and 3 years, respectively. The phase-II study GIMEMA CML 0307 (69) found that 24 (32.9%) patients with a stable DMR discontinued nilotinib treatment at 10-year follow-up, and the TFR prevalence at 2 years was 72.6%. The overall TFR prevalence was estimated to be 24.7%.
LAST (53) was a prospective clinical trial that included 172 patients with CML from 14 academic medical centers in the USA, which aimed to evaluate molecular relapse and patient-reported outcomes after discontinuation of TKIs treatment. Molecular relapse was defined as loss of the MMR. At a median follow-up of 41.6 months, 112 (65.5%) continued to maintained MMR, and 104 (60.8%) achieved TFR. A total of 755 patients were enrolled across Europe in the EURO-SKI trial (54): 94% of patients discontinued imatinib therapy, and 2% and 4% discontinued dasatinib therapy and nilotinib therapy, respectively. Patients received TKIs treatment for ≥3 years and had sustained MR4 for ≥1 year. Relapse-free survival was 61% at 6 months and 50% at 24 months. Disease progression was not observed. The optimal duration of sustained MR4 before treatment discontinuation was 3.1 years calculated by a prognostic model, with 61% probability of retaining MMR. The cutoff for imatinib therapy was 5.8 years, and the molecular relapse-free survival was 63%. Also, 86% of patients regained the MMR after restarting TKIs treatment. The GIMEMA trial enrolled 293 Italian patients with CP-CML who discontinued TKIs therapy (55). 72% patients received imatinib treatment, and the remainder of patients received second-generation TKIs before treatment discontinuation. At 12 months, the TFR prevalence was 68% in the imatinib arm and 73% in the second-generation-TKIs arm. At a median follow-up of 34 months, the overall estimated TFR prevalence was 62%, and disease progression did not occur.
Recently, several retrospective studies have assessed the safety of discontinuation of TKIs therapy outside of clinical trials. One research team (70) enrolled 236 patients with CML from 33 Spanish centers to evaluate the safety of discontinuation of TKIs treatment in a real-life setting. Overall, the TFR prevalence was 64% at 4 years, and no patients suffered disease progression. Most patients who experienced molecular relapse regained the DMR after resuming TKIs therapy for 3–5 months. Iino and coworkers (71) assessed the outcome of 21 patients with CML who discontinued TKIs treatment. The TFR prevalence at 2 years was 66.7%, and no patients experienced disease progression or died. A retrospective study demonstrated that discontinuation of TKIs therapy was safe (especially for patients with a stable DMR with a longer duration of TKI treatment) (72): the prevalence of molecular relapse was 25% in patients with a stable DMR and 85% in those with an unstable DMR. Overall, discontinuation of dasatinib or nilotinib therapy was feasible and safe for patients with a sustained DMR and a longer duration of TKI treatment in clinical trials and real-world settings.
The DESTINY study (73) aimed to evaluate the outcome of gradual dose reduction before TKIs discontinuation as well as the safety of TFR for patients with less deep (but stable) remission. In detail, patients from 20 UK hospitals were assigned to a MR4 group and MMR group. TKIs treatment was reduced to half of the standard dose (imatinib = 200 mg/day; dasatinib = 50 mg/day; nilotinib = 200 mg, bid) for 12 months, then discontinued for a further 24 months. Molecular relapse was defined as loss of MMR that necessitated resumption of TKIs treatment at the full dose. The primary endpoint was the proportion of patients who could first experience half-dose therapy for 1 year, and then stop treatment completely for a further 2 years, without losing the MMR. Of the 174 patients, 148, 10, and 16 were treated with imatinib, dasatinib, and nilotinib, respectively. Forty-nine patients were assigned to the MMR group and 125 to the MR4 group. Three patients in the DMR group and nine patients in the MMR group suffered molecular relapse during dose reduction. Eighty-four (67%) patients achieved the primary endpoint and recurrence-free survival was 72% in the DMR group. Sixteen (33%) patients achieved the primary endpoint and recurrence-free survival was 36% in the MMR group. No patients suffered disease progression and two patients died due to unrelated causes. All patients who relapsed regained the MMR within 5 months of resumption of TKIs therapy.
In a retrospective analysis in 2020 (74), 26 patients with CML received a low-dose TKI before discontinuation, and the TFR prevalence at 5 years was 47.5% in the full-dose group and 58.8% in the low-dose group. That study suggested that low-dose TKI regimens before discontinuation of TKI therapy did not impair the chance of achieving TFR in patients with CML. An investigation on the attitude of hematologists practicing in Italy towards a low-dose TKI regimen and its impact on TFR was undertaken (75). Results showed that 64.4% of hematologists believed that TFR should not be affected by low-dose TKIs. Furthermore, this strategy was applied to 194 patients with CML. Except for three patients, all patients reached a DMR with a median treatment duration of 61.0 months at the time of TFR. At a median follow-up of 29.2 months, 138 (71.1%) patients continued to have TFR, and the TFR prevalence was improved significantly after dose reduction due to AEs. However, outside of clinical trials, one-third of Italian hematologists continued to harbor doubts about the safety of TFR after patients received a low dose of TKIs. Interestingly, only 28.9% of patients suffered molecular relapse, which was lower than that reported in the standard dose therapy. That survey suggested that TFR may be an effective and safe option, even in patients who receive treatment with low-dose TKIs. Those findings suggest that low-dose TKIs do not impair the opportunity to achieve TFR. However, more prospective and multicenter clinical trials must be undertaken to explore the efficacy and safety for patients receiving low-dose TKIs before discontinuation of TKI therapy.
A second attempt to achieve TFR may be considered for some patients. The details of trials focusing on a second opportunity to achieve TFR are shown in Table 3. Ross and collaborators (76) conducted a study on a second discontinuation for 12 patients who regained MR4.5 with restarted treatment after a first molecular relapse. At a median of 8.6 years follow-up, the TFR prevalence was 50%. Patients who relapsed after the first discontinuation of TKIs therapy and who regained a DMR were enrolled in the RE-STIM trial (77). The TFR prevalence after a second attempt at therapy discontinuation was 44.3% at 24 months, 38.5% at 36 months, and 33.2% at 48 months in 70 patients. In the TRAD trial (78), patients who suffered a relapse (loss of MR4 or MMR) after discontinuation of imatinib therapy were resumed on dasatinib therapy (100 mg/day). Patients who regained MR4 that was sustained for >1 year had a second attempt at achieving TFR. The TFR prevalence after a successful attempt at therapy discontinuation was 21.5% at 6 months. In the 2020 A-STIM study (79), 32 (49.2%) patients underwent a second attempt to achieve TFR. The TFR prevalence at the second attempt at treatment discontinuation was 35.8%. Although the TFR prevalence of the second therapy discontinuation was lower than that of the first treatment discontinuation (46.8%), the failure of the first treatment discontinuation did not preclude the success of the second treatment discontinuation. However, patients who lost the MMR rapidly after the first treatment discontinuation had a negligible chance of achieving TFR on a second occasion using TKIs therapy alone.

Table 3 Characteristics of secondary TFR trials.
Switching TKIs are required if there are intolerable toxicities, failure to achieve treatment milestones, or a BCR::ABL1 mutation that leads to resistance to specific TKI, (80, 81). The change is mandatory and should be accompanied by BCR::ABL1 KD-mutations tests in cases of failure/resistance. In the absence of BCR::ABL1 KD-mutations, there are no definitive recommendation for any particular TKIs. The criteria for selection of the second-line TKIs are almost entirely patient-related and dependent upon comorbidities, age, and the toxicity of the first TKI. If there is a mutation for a specific TKI, further TKI selection should be select accordingly. In case of warning response, the change is optional, and dependent upon the patients’ long-term treatment goals and personal factors (e.g., age, complications, tolerance and economic situation). In the case of treatment-related complications and intolerance, the decision to switch TKIs is in part subjective, dependent upon the patient, physician, supportive care, and also upon the clinical response levels. The choice of dose of converted TKIs must take into account the clinical response and tolerance of the patient, as well as the standard- or reduced-dose regimens.
In addition to imatinib, dasatinib and nilotinib were approved recently for pediatric CML treatment, which has expanded the therapeutic options. Moreover, allogeneic stem cell transplantation suggest to be third-line treatment for most pediatric cases (82). However, children are actively growing during TKIs treatment, so they develop unique AEs, such as growth disturbance (83). Currently, there are lacking of sufficient data on efficacy and safety to pediatric patients, TKI selection mostly to be reliant on the clinical effects observed in adults.
Some research teams based in European groups recommend a lower starting dose of imatinib in children with CP-CML (260–300 mg/m2/day) (84). However, Children’s Oncology Group CML Working Group suggested a higher dose of imatinib was also well tolerated (85), and the initial recommended dose is 340 mg/m2/day (maximum to 600 mg). The initial dose of dasatinib is 400-100 mg/m2 qd (maximum to 100 mg) in children with CP-CML (86), and 230 mg/m2/dose bid for nilotinib (maximum single dose of 400 mg) (87). The dose should be recalculated every 3 months based on changes in body-weight or more frequently if required, and could be adjust on the basis of clinical response and tolerability, but the maximum dose should not be exceeded.
Limited evidence regarding discontinuation of TKIs therapy is available for pediatric CML, mostly in small studies and case series. The Japanese Pediatric Leukemia/Lymphoma Study Group (88) reported the first prospective pediatric discontinuation of TKIs trial in 22 patients with CP-CML who had been taking TKIs for >3 years and had sustained MMR (MR4.0) for >2 years. TFR at 12 months was 50%. Of seven pediatric patients who discontinued imatinib, two patients achieved TFR (85). The STOP IMAPED study enrolled 14 pediatric patients who were treated with imatinib for ≥3 years and sustained DMR for ≥2 years to discontinued imatinib, the TFR rate at 6 months was 28.6% (89). Millot and colleagues (90) reported a TFR rate of 56% at 36 months after discontinuation of imatinib in 18 pediatric patients with sustained DMR for ≥23.9 months. Shima and coworkers (91) evaluated the feasibility of discontinuation of TKIs in pediatric CML patients. Twenty-two patients were eligible to discontinue TKIs if they treated with TKIs for ≥3 years, and sustained MR4.0 for ≥2 years. Their results showed the TFR rate to be 50.0% at 12 months, and that all patients regained MR4.0 after resumption of TKIs therapy. Therefore, discontinuation of TKIs therapy in pediatric CML is not recommended outside of clinical trials, and more prospective studies in pediatric CML are needed.
Recently, increasing numbers of patients with CML have begun to pursue a dose optimization strategy, which included dose reduction and discontinuation of TKIs therapy. In the real-life settings, we will comprehensively consider the dose optimization strategy base on the treatment goal, clinical response, tolerance, and economic situation of patients. A dose-reduction regimen could allow for broader clinical use of TKIs (even in patients with comorbidities). For example, if the elderly patient with multiple comorbidities or is previously intolerant to other TKIs, we may suggest a half-dose of dasatinib treatment (50 mg/day). If conditions permit, the dose can also be adjusted according to blood concentration monitoring. For patients with sustained optimal clinical response (MMR or DMR), reducing TKIs dose can reduce AE and improve treatment compliance. The proposal of TFR as a possible final treatment endpoint should be discussed with patients (especially younger patients) at the diagnosis to achieve a DMR rapidly and improve long-term compliance. For patients with stable DMR and long duration of TKIs treatment, it is feasible and safe to stop TKI treatment. Patients who discontinued TKIs should follow the discontinuation standards recommended in ELN or NCCN guidelines. For patients with stable DMR who want to stop TKIs treatment but are afraid of relapse, we recommend to reduce TKIs dose before discontinuation of TKIs therapy. For patients who cannot achieve TFR, the TKIs dose must be reduced without affecting the clinical response. Importantly, patients who underwent dose optimization should be advised for more intensive molecular monitoring, especially during the first 6 months. Once the patients lose the optimal response, physicians should take measures immediately, such as resuming to standard-dose therapy, reintroducing TKIs treatment, or switching to other TKIs, etc. However, evidence for dose optimization in pediatrics CML is limited. Hence, evidence from novel, prospective clinical trials and real-life clinical practice are required to explore dose-optimization strategies, which may provide more promising options for CML treatment.
FC: Writing (original draft) and data curation. QL: Validation, data curation, and writing (original draft). ZC: Data curation. MH: Revision of the original draft. WL: Conceptualization, visualization, and data curation. YZ: Project administration and funding acquisition. All authors contributed to the article and approved the submitted version.
This work was supported by Open fund of Hubei Key Laboratory of Biological Targeted Therapy (No. 2022swbx001).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet (2021) 398(10314):1914–26. doi: 10.1016/s0140-6736(21)01204-6
2. Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring. Am J Hematol (2020) 95(6):691–709. doi: 10.1002/ajh.25792
3. Rosti G, Castagnetti F, Gugliotta G, Baccarani M. Tyrosine kinase inhibitors in chronic myeloid leukaemia: Which, when, for whom? Nat Rev Clin Oncol (2017) 14(3):141–54. doi: 10.1038/nrclinonc.2016.139
4. Nekoukar Z, Moghimi M, Salehifar E. A narrative review on adverse effects of dasatinib with a focus on pharmacotherapy of dasatinib-induced pulmonary toxicities. Blood Res (2021) 56(4):229–42. doi: 10.5045/br.2021.2021117
5. Weatherald J, Bondeelle L, Chaumais MC, Guignabert C, Savale L, Jaïs X, et al. Pulmonary complications of bcr-abl tyrosine kinase inhibitors. Eur Respir J (2020) 56(4):2000279. doi: 10.1183/13993003.00279-2020
6. Wang Z, Jiang L, Yan H, Xu Z, Luo P. Adverse events associated with nilotinib in chronic myeloid leukemia: Mechanisms and management strategies. Expert Rev Clin Pharmacol (2021) 14(4):445–56. doi: 10.1080/17512433.2021.1894129
7. Cirmi S, El Abd A, Letinier L, Navarra M, Salvo F. Cardiovascular toxicity of tyrosine kinase inhibitors used in chronic myeloid leukemia: An analysis of the FDA adverse event reporting system database (FAERS). Cancers (Basel) (2020) 12(4):826. doi: 10.3390/cancers12040826
8. Claudiani S, Apperley JF, Szydlo R, Khan A, Nesr G, Hayden C, et al. TKI dose reduction can effectively maintain major molecular remission in patients with chronic myeloid leukaemia. Br J Haematol (2021) 193(2):346–55. doi: 10.1111/bjh.17286
9. Iurlo A, Cattaneo D, Bucelli C, Breccia M. Dose optimization of tyrosine kinase inhibitors in chronic myeloid leukemia: A new therapeutic challenge. J Clin Med (2021) 10(3):515. doi: 10.3390/jcm10030515
10. Fassoni AC, Baldow C, Roeder I, Glauche I. Reduced tyrosine kinase inhibitor dose is predicted to be as effective as standard dose in chronic myeloid leukemia: A simulation study based on phase III trial data. Haematologica (2018) 103(11):1825–1834. doi: 56710.3324/haematol.2018.194522
11. Okamoto S, Ureshino H, Kawaguchi A, Miyazono M, Ikeda Y, Kimura S. Assessment of estimated glomerular filtration rate in patients with chronic myeloid leukemia following discontinuation of tyrosine kinase inhibitors. Int J Hematol (2020) 112(1):41–5. doi: 10.1007/s12185-020-02880-3
12. Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep (2021) 16(5):433–9. doi: 10.1007/s11899-021-00653-1
13. Breccia M, Scalzulli E, Pepe S, Colafigli G, Bisegna ML, Capriata M, et al. Emerging concepts for assessing and predicting treatment-free remission in chronic myeloid leukemia patients. Expert Rev Hematol (2022) 15(1):25–32. doi: 10.1080/17474086.2022.2018296
14. Cortes J, Rea D, Lipton JH. Treatment-free remission with first- and second-generation tyrosine kinase inhibitors. Am J Hematol (2019) 94(3):346–57. doi: 10.1002/ajh.25342
15. Saglio G, Gale RP. Prospects for achieving treatment-free remission in chronic myeloid leukaemia. Br J Haematol (2020) 190(3):318–27. doi: 10.1111/bjh.16506
16. Cortes JE, Kantarjian HM, Goldberg SL, Powell BL, Giles FJ, Wetzler M, et al. High-dose imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: high rates of rapid cytogenetic and molecular responses. J Clin Oncol (2009) 27(28):4754–9. doi: 10.1200/jco.2008.20.3869
17. Baccarani M, Rosti G, Castagnetti F, Haznedaroglu I, Porkka K, Abruzzese E, et al. Comparison of imatinib 400 mg and 800 mg daily in the front-line treatment of high-risk, Philadelphia-positive chronic myeloid leukemia: a European LeukemiaNet study. Blood (2009) 113(19):4497–504. doi: 10.1182/blood-2008-12-191254
18. Cortes JE, Baccarani M, Guilhot F, Druker BJ, Branford S, Kim DW, et al. Randomized, open-label study of daily imatinib mesylate 400 mg versus 800 mg in patients with newly diagnosed, previously untreated chronic myeloid leukemia in chronic phase using molecular end points: Tyrosine kinase inhibitor optimization and selectivity study. J Clin Oncol (2010) 28(3):424–30. doi: 10.1200/jco.2009.25.3724
19. Michel C, Burchert A, Hochhaus A, Saussele S, Neubauer A, Lauseker M, et al. Imatinib dose reduction in major molecular response of chronic myeloid leukemia: Results from the German chronic myeloid leukemia-study IV. Haematologica (2019) 104(5):955–62. doi: 10.3324/haematol.2018.206797
20. Clarke WA, Chatelut E, Fotoohi AK, Larson RA, Martin JH, Mathijssen RHJ, et al. Therapeutic drug monitoring in oncology: International association of therapeutic drug monitoring and clinical toxicology consensus guidelines for imatinib therapy. Eur J Cancer (2021) 157:428–40. doi: 10.1016/j.ejca.2021.08.033
21. Lankheet NAG, Desar IME, Mulder SF, Burger DM, Kweekel DM, van Herpen CML, et al. Optimizing the dose in cancer patients treated with imatinib, sunitinib and pazopanib. Br J Clin Pharmacol (2017) 83(10):2195–204. doi: 10.1111/bcp.13327
22. Westerdijk K, Desar IME, Steeghs N, van der Graaf WTA, van Erp NP. Imatinib, sunitinib and pazopanib: From flat-fixed dosing towards a pharmacokinetically guided personalized dose. Br J Clin Pharmacol (2020) 86(2):258–73. doi: 10.1111/bcp.14185
23. Cortes JE, Hochhaus A, Kantarjian HM, Guilhot F, Kota VK, Hughes TP, et al. Impact of dose reductions on 5-year efficacy in newly diagnosed patients with chronic myeloid leukemia in chronic phase (CML-CP) from DASISION. J Clin Oncol (2017) 35(15_suppl):7051–. doi: 10.1200/JCO.2017.35.15_suppl.7051
24. Latagliata R, Stagno F, Annunziata M, Abruzzese E, Iurlo A, Guarini A, et al. Frontline dasatinib treatment in a "Real-life" cohort of patients older than 65 years with chronic myeloid leukemia. Neoplasia (2016) 18(9):536–40. doi: 10.1016/j.neo.2016.07.005
25. Iurlo A, Galimberti S, Abruzzese E, Annunziata M, Bonifacio M, Latagliata R, et al. Pleural effusion and molecular response in dasatinib-treated chronic myeloid leukemia patients in a real-life Italian multicenter series. Ann Hematol (2018) 97(1):95–100. doi: 10.1007/s00277-017-3144-1
26. Shah NP, Rousselot P, Schiffer C, Rea D, Cortes JE, Milone J, et al. Dasatinib in imatinib-resistant or -intolerant chronic-phase, chronic myeloid leukemia patients: 7-year follow-up of study CA180-034. Am J Hematol (2016) 91(9):869–74. doi: 10.1002/ajh.24423
27. Naqvi K, Jabbour E, Skinner J, Anderson K, Dellasala S, Yilmaz M, et al. Long-term follow-up of lower dose dasatinib (50 mg daily) as frontline therapy in newly diagnosed chronic-phase chronic myeloid leukemia. Cancer (2020) 126(1):67–75. doi: 10.1002/cncr.32504
28. Murai K, Ureshino H, Kumagai T, Tanaka H, Nishiwaki K, Wakita S, et al. Low-dose dasatinib in older patients with chronic myeloid leukaemia in chronic phase (DAVLEC): A single-arm, multicentre, phase 2 trial. Lancet Haematol (2021) 8(12):e902–e11. doi: 10.1016/s2352-3026(21)00333-1
29. He S, Bian J, Shao Q, Zhang Y, Hao X, Luo X, et al. Therapeutic drug monitoring and individualized medicine of dasatinib: Focus on clinical pharmacokinetics and pharmacodynamics. Front Pharmacol (2021) 12:797881. doi: 10.3389/fphar.2021.797881
30. Rousselot P, Mollica L, Guilhot J, Guerci A, Nicolini FE, Etienne G, et al. Dasatinib dose optimisation based on therapeutic drug monitoring reduces pleural effusion rates in chronic myeloid leukaemia patients. Br J Haematol (2021) 194(2):393–402. doi: 10.1111/bjh.17654
31. Hiwase D, Tan P, D'Rozario J, Taper J, Powell A, Irving I, et al. Efficacy and safety of nilotinib 300mg twice daily in patients with chronic myeloid leukemia in chronic phase who are intolerant to prior tyrosine kinase inhibitors: Results from the phase IIIb ENESTswift study. Leuk Res (2018) 67:109–15. doi: 10.1016/j.leukres.2018.02.013
32. Rea D, Cayuela J-M, Dulucq S, Etienne G. Molecular responses after switching from a standard-dose twice-daily nilotinib regimen to a reduced-dose once-daily schedule in patients with chronic myeloid leukemia: A real life observational study (NILO-RED). Blood (2017) 130:318. doi: 10.1182/blood.V130.Suppl_1.318.318
33. Rousselot P, Huguet F, Rea D, Legros L, Cayuela JM, Maarek O, et al. Imatinib mesylate discontinuation in patients with chronic myelogenous leukemia in complete molecular remission for more than 2 years. Blood (2007) 109(1):58–60. doi: 10.1182/blood-2006-03-011239
34. Etienne G, Guilhot J, Rea D, Rigal-Huguet F, Nicolini F, Charbonnier A, et al. Long-term follow-up of the French stop imatinib (STIM1) study in patients with chronic myeloid leukemia. J Clin Oncol (2017) 35(3):298–305. doi: 10.1200/jco.2016.68.2914
35. Rousselot P, Charbonnier A, Cony-Makhoul P, Agape P, Nicolini FE, Varet B, et al. Loss of major molecular response as a trigger for restarting tyrosine kinase inhibitor therapy in patients with chronic-phase chronic myelogenous leukemia who have stopped imatinib after durable undetectable disease. J Clin Oncol (2014) 32(5):424–30. doi: 10.1200/jco.2012.48.5797
36. Nicolini FE, Dulucq S, Boureau L, Cony-Makhoul P, Charbonnier A, Escoffre-Barbe M, et al. Evaluation of residual disease and TKI duration are critical predictive factors for molecular recurrence after stopping imatinib first-line in chronic phase CML patients. Clin Cancer Res (2019) 25(22):6606–13. doi: 10.1158/1078-0432.Ccr-18-3373
37. Ross DM, Branford S, Seymour JF, Schwarer AP, Arthur C, Yeung DT, et al. Safety and efficacy of imatinib cessation for CML patients with stable undetectable minimal residual disease: results from the TWISTER study. Blood (2013) 122(4):515–22. doi: 10.1182/blood-2013-02-483750
38. Lee SE, Choi SY, Song HY, Kim SH, Choi MY, Park JS, et al. Imatinib withdrawal syndrome and longer duration of imatinib have a close association with a lower molecular relapse after treatment discontinuation: the KID study. Haematologica (2016) 101(6):717–23. doi: 10.3324/haematol.2015.139899
39. Mori S, Vagge E, le Coutre P, Abruzzese E, Martino B, Pungolino E, et al. Age and dPCR can predict relapse in CML patients who discontinued imatinib: the ISAV study. Am J Hematol (2015) 90(10):910–4. doi: 10.1002/ajh.24120
40. Fujisawa S, Ueda Y, Usuki K, Kobayashi H, Kondo E, Doki N, et al. Feasibility of the imatinib stop study in the Japanese clinical setting: delightedly overcome CML expert stop TKI trial (DOMEST trial). Int J Clin Oncol (2019) 24(4):445–53. doi: 10.1007/s10147-018-1368-2
41. Imagawa J, Tanaka H, Okada M, Nakamae H, Hino M, Murai K, et al. Discontinuation of dasatinib in patients with chronic myeloid leukaemia who have maintained deep molecular response for longer than 1 year (DADI trial): A multicentre phase 2 trial. Lancet Haematol (2015) 2(12):e528–35. doi: 10.1016/s2352-3026(15)00196-9
42. Kimura S, Imagawa J, Murai K, Hino M, Kitawaki T, Okada M, et al. Treatment-free remission after first-line dasatinib discontinuation in patients with chronic myeloid leukaemia (first-line DADI trial): A single-arm, multicentre, phase 2 trial. Lancet Haematol (2020) 7(3):e218–e25. doi: 10.1016/s2352-3026(19)30235-2
43. Kumagai T, Nakaseko C, Nishiwaki K, Yoshida C, Ohashi K, Takezako N, et al. Discontinuation of dasatinib after deep molecular response for over 2 years in patients with chronic myelogenous leukemia and the unique profiles of lymphocyte subsets for successful discontinuation: A prospective, multicenter Japanese trial (D-STOP trial). Blood (2016) 128(22):791. doi: 10.1182/blood.V128.22.791.791
44. Shah NP, García-Gutiérrez V, Jiménez-Velasco A, Larson S, Saussele S, Rea D, et al. Dasatinib discontinuation in patients with chronic-phase chronic myeloid leukemia and stable deep molecular response: the DASFREE study. Leuk Lymphoma (2020) 61(3):650–9. doi: 10.1080/10428194.2019.1675879
45. Ross DM, Masszi T, Gómez Casares MT, Hellmann A, Stentoft J, Conneally E, et al. Durable treatment-free remission in patients with chronic myeloid leukemia in chronic phase following frontline nilotinib: 96-week update of the ENESTfreedom study. J Cancer Res Clin Oncol (2018) 144(5):945–54. doi: 10.1007/s00432-018-2604-x
46. Takahashi N, Nishiwaki K, Nakaseko C, Aotsuka N, Sano K, Ohwada C, et al. Treatment-free remission after two-year consolidation therapy with nilotinib in patients with chronic myeloid leukemia: STAT2 trial in Japan. Haematologica (2018) 103(11):1835–42. doi: 10.3324/haematol.2018.194894
47. Radich J, Mahon F-X, Hochhaus A, Hughes T, Ailawadhi S, Lipton J, et al. ENESTfreedom and ENESTop update: Durable treatment-free remission (TFR) at 96 weeks after nilotinib treatment cessation in patients with chronic myeloid leukemia in chronic phase (CML-CP). Clin Lymphoma Myeloma Leukemia (2017) 17:S314–S5. doi: 10.1016/j.clml.2017.07.115
48. Hughes TP, Boquimpani C, Takahashi N, Benyamini N, Clementino NCD, Shuvaev V, et al. ENESTop 144-week update: Long-term treatment-free remission (TFR) in patients with chronic myeloid leukemia in chronic phase (CML-CP) after stopping second-line nilotinib. Clin Lymphoma Myeloma Leukemia (2018) 18:S222. doi: 10.1016/j.clml.2018.07.092
49. Mahon F-X, Boquimpani C, Takahashi N, Benyamini N, Clementino NCD, Shuvaev V, et al. ENESTop 192-weeks results: Treatment-free remission (TFR) in patients with chronic myeloid leukemia in chronic phase (CML-CP) after stopping second-line nilotinib. Clin Lymphoma Myeloma Leukemia (2019) 19:S288–S9. doi: 10.1016/j.clml.2019.07.233
50. Hughes TP, Clementino NCD, Fominykh M, Lipton JH, Turkina AG, Moiraghi EB, et al. Long-term treatment-free remission in patients with chronic myeloid leukemia after second-line nilotinib: ENESTop 5-year update. Leukemia (2021) 35(6):1631–42. doi: 10.1038/s41375-021-01260-y
51. Nagafuji K, Matsumura I, Shimose T, Kawaguchi T, Kuroda J, Nakamae H, et al. Cessation of nilotinib in patients with chronic myelogenous leukemia who have maintained deep molecular responses for 2 years: A multicenter phase 2 trial, stop nilotinib (NILSt). Int J Hematol (2019) 110(6):675–82. doi: 10.1007/s12185-019-02736-5
52. Rea D, Nicolini FE, Tulliez M, Guilhot F, Guilhot J, Guerci-Bresler A, et al. Discontinuation of dasatinib or nilotinib in chronic myeloid leukemia: Interim analysis of the STOP 2G-TKI study. Blood (2017) 129(7):846–54. doi: 10.1182/blood-2016-09-742205
53. Atallah E, Schiffer CA, Radich JP, Weinfurt KP, Zhang MJ, Pinilla-Ibarz J, et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: A nonrandomized clinical trial. JAMA Oncol (2021) 7(1):42–50. doi: 10.1001/jamaoncol.2020.5774
54. Saussele S, Richter J, Guilhot J, Gruber FX, Hjorth-Hansen H, Almeida A, et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukaemia (EURO-SKI): A prespecified interim analysis of a prospective, multicentre, non-randomised, trial. Lancet Oncol (2018) 19(6):747–57. doi: 10.1016/s1470-2045(18)30192-x
55. Fava C, Rege-Cambrin G, Dogliotti I, Cerrano M, Berchialla P, Dragani M, et al. Observational study of chronic myeloid leukemia Italian patients who discontinued tyrosine kinase inhibitors in clinical practice. Haematologica (2019) 104(8):1589–96. doi: 10.3324/haematol.2018.205054
56. Cervantes F, Correa JG, Pérez I, García-Gutiérrez V, Redondo S, Colomer D, et al. Imatinib dose reduction in patients with chronic myeloid leukemia in sustained deep molecular response. Ann Hematol (2017) 96(1):81–5. doi: 10.1007/s00277-016-2839-z
57. Mueller-Schoell A, Groenland SL, Scherf-Clavel O, van Dyk M, Huisinga W, Michelet R, et al. Therapeutic drug monitoring of oral targeted antineoplastic drugs. Eur J Clin Pharmacol (2021) 77(4):441–64. doi: 10.1007/s00228-020-03014-8
58. Peng B, Lloyd P, Schran H. Clinical pharmacokinetics of imatinib. Clin Pharmacokinet (2005) 44(9):879–94. doi: 10.2165/00003088-200544090-00001
59. De Francia S, DʼAvolio A, Ariaudo A, Pirro E, Piccione F, Simiele M, et al. Plasma and intracellular imatinib concentrations in patients with chronic myeloid leukemia. Ther Drug Monit (2014) 36(3):410–2. doi: 10.1097/ftd.0000000000000013
60. Cortes JE, Egorin MJ, Guilhot F, Molimard M, Mahon FX. Pharmacokinetic/pharmacodynamic correlation and blood-level testing in imatinib therapy for chronic myeloid leukemia. Leukemia (2009) 23(9):1537–44. doi: 10.1038/leu.2009.88
61. Adeagbo BA, Olugbade TA, Durosinmi MA, Bolarinwa RA, Ogungbenro K, Bolaji OO. Population pharmacokinetics of imatinib in nigerians with chronic myeloid leukemia: Clinical implications for dosing and resistance. J Clin Pharmacol (2017) 57(12):1554–63. doi: 10.1002/jcph.953
62. Shin H, Ha JE, Zang DY, Kim SH, Do YR, Lee WS, et al. Appropriate starting dose of dasatinib based on analyses of dose-limiting toxicities and molecular responses in Asian patients with chronic myeloid leukemia. Clin Lymphoma Myeloma Leuk (2021) 21(6):e521–e9. doi: 10.1016/j.clml.2021.01.020
63. Mizuta S, Sawa M, Tsurumi H, Matsumoto K, Miyao K, Hara T, et al. Plasma concentrations of dasatinib have a clinical impact on the frequency of dasatinib dose reduction and interruption in chronic myeloid leukemia: an analysis of the DARIA 01 study. Int J Clin Oncol (2018) 23(5):980–8. doi: 10.1007/s10147-018-1300-9
64. Hochhaus A, Saglio G, Hughes TP, Larson RA, Kim DW, Issaragrisil S, et al. Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia (2016) 30(5):1044–54. doi: 10.1038/leu.2016.5
65. Lee SE, Choi SY, Bang JH, Kim SH, Jang EJ, Byeun JY, et al. Predictive factors for successful imatinib cessation in chronic myeloid leukemia patients treated with imatinib. Am J Hematol (2013) 88(6):449–54. doi: 10.1002/ajh.23427
66. Campiotti L, Suter MB, Guasti L, Piazza R, Gambacorti-Passerini C, Grandi AM, et al. Imatinib discontinuation in chronic myeloid leukaemia patients with undetectable BCR-ABL transcript level: A systematic review and a meta-analysis. Eur J Cancer (2017) 77:48–56. doi: 10.1016/j.ejca.2017.02.028
67. Di Q, Deng H, Zhao Y, Li BY, Qin L. Second-generation tyrosine kinase inhibitor discontinuation in chronic myeloid leukemia patients with stable deep molecular response: A systematic review and a meta-analysis. Comput Math Methods Med (2021) 2021:3110622. doi: 10.1155/2021/3110622
68. Radich JP, Hochhaus A, Masszi T, Hellmann A, Stentoft J, Casares MTG, et al. Treatment-free remission following frontline nilotinib in patients with chronic phase chronic myeloid leukemia: 5-year update of the ENESTfreedom trial. Leukemia (2021) 35(5):1344–55. doi: 10.1038/s41375-021-01205-5
69. Gugliotta G, Castagnetti F, Breccia M, Levato L, Intermesoli T, D'Adda M, et al. Treatment-free remission in chronic myeloid leukemia patients treated front-line with nilotinib: 10-year follow-up of the GIMEMA CML 0307 study. Haematologica (2022) 107(10):2356–64. doi: 10.3324/haematol.2021.280175
70. Hernández-Boluda JC, Pereira A, Pastor-Galán I, Alvarez-Larrán A, Savchuk A, Puerta JM, et al. Feasibility of treatment discontinuation in chronic myeloid leukemia in clinical practice: Results from a nationwide series of 236 patients. Blood Cancer J (2018) 8(10):91. doi: 10.1038/s41408-018-0125-0
71. Iino M, Yamamoto T, Sakamoto Y. Outcomes of unplanned tyrosine kinase inhibitor discontinuation in patients with chronic myeloid leukemia: Retrospective analysis of real-world experience in a single institution. Hematology (2019) 24(1):355–61. doi: 10.1080/16078454.2019.1590964
72. Cerveira N, Loureiro B, Bizarro S, Correia C, Torres L, Lisboa S, et al. Discontinuation of tyrosine kinase inhibitors in CML patients in real-world clinical practice at a single institution. BMC Cancer (2018) 18(1):1245. doi: 10.1186/s12885-018-5167-y
73. Clark RE, Polydoros F, Apperley JF, Milojkovic D, Rothwell K, Pocock C, et al. De-escalation of tyrosine kinase inhibitor therapy before complete treatment discontinuation in patients with chronic myeloid leukaemia (DESTINY): A non-randomised, phase 2 trial. Lancet Haematol (2019) 6(7):e375–e83. doi: 10.1016/s2352-3026(19)30094-8
74. Cayssials E, Torregrosa-Diaz J, Gallego-Hernanz P, Tartarin F, Systchenko T, Maillard N, et al. Low-dose tyrosine kinase inhibitors before treatment discontinuation do not impair treatment-free remission in chronic myeloid leukemia patients: Results of a retrospective study. Cancer (2020) 126(15):3438–47. doi: 10.1002/cncr.32940
75. Iurlo A, Cattaneo D, Artuso S, Consonni D, Abruzzese E, Binotto G, et al. Treatment-free remission in chronic myeloid leukemia patients treated with low-dose TKIs: A feasible option also in the real-life. A Campus CML Study Front Oncol (2022) 12:839915. doi: 10.3389/fonc.2022.839915
76. Ross DM, Pagani IS, Shanmuganathan N, Kok CH, Seymour JF, Mills AK, et al. Long-term treatment-free remission of chronic myeloid leukemia with falling levels of residual leukemic cells. Leukemia (2018) 32(12):2572–9. doi: 10.1038/s41375-018-0264-0
77. Legros L, Nicolini FE, Etienne G, Rousselot P, Rea D, Giraudier S, et al. The TKI-free duration after a first discontinuation attempt that failed in CP CML patients is a predictive factor of TKI-free remission after a second attempt. Blood (2019) 134:28. doi: 10.1182/blood-2019-123719
78. Kim DDH, Busque L, Forrest DL, Savoie L, Bence-Bruckler I, Couban S, et al. Second attempt of TKI discontinuation with dasatinib for treatment-free remission after failing first attempt with imatinib: Treatment-free remission accomplished by dasatinib (TRAD) trial. Blood (2018) 132:787. doi: 10.1182/blood-2018-99-114656
79. Rousselot P, Loiseau C, Delord M, Cayuela JM, Spentchian M. Late molecular recurrences in patients with chronic myeloid leukemia experiencing treatment-free remission. Blood Adv (2020) 4(13):3034–40. doi: 10.1182/bloodadvances.2020001772
80. Hochhaus A, Baccarani M, Silver RT, Schiffer C, Apperley JF, Cervantes F, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia (2020) 34(4):966–84. doi: 10.1038/s41375-020-0776-2
81. Deininger MW, Shah NP, Altman JK, Berman E, Bhatia R, Bhatnagar B, et al. Chronic myeloid leukemia, version 2. 2021 NCCN Clin Pract Guidelines Oncol J Natl Compr Canc Netw (2020) 18(10):1385–415. doi: 10.6004/jnccn.2020.0047
82. Hijiya N, Suttorp M. How I treat chronic myeloid leukemia in children and adolescents. Blood (2019) 133(22):2374–84. doi: 10.1182/blood.2018882233
83. Samis J, Lee P, Zimmerman D, Suttorp M, Hijiya N. The complexity of growth failure in children receiving tyrosine kinase inhibitor therapy for chronic myelogenous leukemia. Pediatr Blood Cancer (2017) 64(12). doi: 10.1002/pbc.26703
84. Hijiya N, Millot F, Suttorp M. Chronic myeloid leukemia in children: Clinical findings, management, and unanswered questions. Pediatr Clin North Am (2015) 62(1):107–19. doi: 10.1016/j.pcl.2014.09.008
85. Suttorp M, Schulze P, Glauche I, Göhring G, von Neuhoff N, Metzler M, et al. Front-line imatinib treatment in children and adolescents with chronic myeloid leukemia: Results from a phase III trial. Leukemia (2018) 32(7):1657–69. doi: 10.1038/s41375-018-0179-9
86. McCafferty EH, Dhillon S, Deeks ED. Dasatinib: A review in pediatric chronic myeloid leukemia. Paediatr Drugs (2018) 20(6):593–600. doi: 10.1007/s40272-018-0319-8
87. Hijiya N, Zwaan CM, Rizzari C, Foà R, Abbink F, Lancaster D, et al. Pharmacokinetics of nilotinib in pediatric patients with Philadelphia chromosome-positive chronic myeloid leukemia or acute lymphoblastic leukemia. Clin Cancer Res (2020) 26(4):812–20. doi: 10.1158/1078-0432.Ccr-19-0090
88. Kurosawa H, Tanizawa A, Tono C, Watanabe A, Shima H, Ito M, et al. Leukostasis in children and adolescents with chronic myeloid leukemia: Japanese pediatric Leukemia/Lymphoma study group. Pediatr Blood Cancer (2016) 63(3):406–11. doi: 10.1002/pbc.25803
89. de Bruijn CMA, Millot F, Suttorp M, Borisevich M, Brons P, Lausen B, et al. Discontinuation of imatinib in children with chronic myeloid leukaemia in sustained deep molecular remission: Results of the STOP IMAPED study. Br J Haematol (2019) 185(4):718–24. doi: 10.1111/bjh.15826
90. Millot F, Suttorp M, Ragot S, Leverger G, Dalle JH, Thomas C, et al. Discontinuation of imatinib in children with chronic myeloid leukemia: A study from the international registry of childhood CML. Cancers (Basel) (2021) 13(16):4102. doi: 10.3390/cancers13164102
Keywords: tyrosine kinase inhibitors, dose optimization, chronic myeloid leukemia, dose reduction, treatment-free remission
Citation: Cheng F, Li Q, Cui Z, Hong M, Li W and Zhang Y (2023) Dose optimization strategy of the tyrosine kinase inhibitors imatinib, dasatinib, and nilotinib for chronic myeloid leukemia: From clinical trials to real-life settings. Front. Oncol. 13:1146108. doi: 10.3389/fonc.2023.1146108
Received: 04 February 2023; Accepted: 23 March 2023;
Published: 05 April 2023.
Edited by:
Massimo Breccia, Sapienza University of Rome, ItalyReviewed by:
Elisabetta Abruzzese, University of Rome Tor Vergata, ItalyCopyright © 2023 Cheng, Li, Cui, Hong, Li and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu Zhang, emhhbmd3a3BAMTYzLmNvbQ==; Weiming Li, bGVlOTM3QDEyNi5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.