
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 08 May 2023
Sec. Hematologic Malignancies
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1135160
This article is part of the Research TopicReviews in Hematologic Malignancies: 2023View all 15 articles
 Momen Nassani1
Momen Nassani1 Riad El Fakih1*
Riad El Fakih1* Jakob Passweg2
Jakob Passweg2 Simone Cesaro3Hazzaa Alzahrani1
Simone Cesaro3Hazzaa Alzahrani1 Ali Alahmari1Carmem Bonfim4
Ali Alahmari1Carmem Bonfim4 Raheel Iftikhar5Amal Albeihany1
Raheel Iftikhar5Amal Albeihany1 Constantijn Halkes6Syed Osman Ahmed1
Constantijn Halkes6Syed Osman Ahmed1 Carlo Dufour7Mahmoud Aljurf1
Carlo Dufour7Mahmoud Aljurf1Bone marrow failure syndromes are a heterogeneous group of diseases. With the major advancements in diagnostic tools and sequencing techniques, these diseases may be better classified and therapies may be further tailored. Androgens, a historic group of drugs, were found to stimulate hematopoiesis by enhancing the responsiveness of progenitors. These agents have been used for decades to treat different forms of bone marrow failure. With the availability of more effective pathways to treat BMF, androgens are less used currently. Nevertheless, this group of drugs may serve BMF patients where standard therapy is contraindicated or not available. In this article, we review the published literature addressing the use of androgens in BMF patients and we make recommendations on how to best use this class of drugs within the current therapeutic landscape.
Aplastic anemia (AA) is a term used to describe a group of heterogeneous syndromes that affect hematopoiesis and result in bone marrow failure (1). It can be inherited, acquired or a result of exposure to certain toxins. This syndrome was first described by the German physician Paul Ehrlich in 1885 (1). Back then, it used to be a fatal condition due to uncontrolled bleeding or overwhelming infections. The advancement in allogeneic stem cell transplantation and immunosuppressive treatment in the 20th century changed the outcome of the disease dramatically (2, 3). The long term overall survival of bone marrow failure (BMF) syndromes have remarkably improved in the modern era and can exceed 90% (4). Trials comparing transplant to conventional therapies (including androgens) showed clear survival benefit of transplant compared to conventional therapies (5, 6). Nevertheless, limitations and challenges in the management of aplastic anemia and BMF still exist. Allogeneic stem cell transplant may not be feasible for all patients for a number of reasons, especially in countries with limited resources. Alternatives to transplantation include immunosuppressive therapy, growth factors, thrombopoietin agonists and androgen therapy. The objective of this article is to provide a comprehensive and systemic evaluation of the published literature regarding the use of androgens in acquired and to a lesser extent inherited bone marrow failure syndromes.
In the early days, the management of AA patients consisted of supportive transfusions in addition to other interventions with questionable efficacy (steroids, splenectomy, vitamins, etc.) (7). The first indications about the possible efficacy of androgens in bone marrow failure, were the spontaneous remission in two boys upon pubescence and the development of myeloid metaplasia in a patient taking testosterone for breast cancer (7). A small report followed, where five AA patients who failed steroids and transfusion were given testosterone and four of them achieved remarkable responses in hemoglobin levels and transfusion independence along with variable response in neutrophils and platelets (7). A number of publications were reported thereafter supporting the role of testosterone and anabolic steroids in aplastic anemia (8–11). Overall, around 70% of patients on these studies achieved a hemoglobin above 12 g/dl along with improvement in the platelet and neutrophil numbers. Another multicenter trial recruited 45 patients with hypoproliferative or aregenerative anemia treated with oxymetholone for a minimum of 3 months. Patients with hypocellular marrow had the best response (12). In 1976, a prospective randomized clinical trial showed superiority of allogeneic bone marrow transplantation compared to standard of care, which included androgen therapy (5). A clear reduction in mortality was reported in the transplanted group compared to the non-transplant group. Currently, with the consistent encouraging results of transplant over the last decades, HSCT is considered the standard of care for young, fit SAA patients with available donors. Other trials compared different compounds of anabolic steroids. One of these trials, showed better outcome with methandrostenolone compared to other types of anabolic steroids, while methanolone was associated with the worst response and survival rates in this study (13). In another study, where 125 patients with AA were randomized to receive four different androgens (norethandrolone 1 mg/kg/day, fluoxymesterone 1 mg/kg/day, stanozolol 1mg/kg/day and testosterone undecanoate 1.7 mg/kg/day) fluoxymesterone treated group had the best overall survival. The worst survival rate was in patients on stanozolol (14).
The body building action of androgens and their euphoric action on the brain led to widespread illicit use of AAS. Hence, all AAS were designated as class III controlled substances. Nevertheless, these agents have shown significant benefits in a number of disorders. Testosterone was first discovered in 1935 and found to have effects on both reproductive (androgenic) and non-reproductive tissues (anabolic). It has been used in different catabolic states due to its anabolic effects through nitrogen fixation and as such protein synthesis (15). Virilization, on the other hand, is one of the unwanted side effects. Numerous derivatives have been developed aiming to prolong its biological activity, increase its anabolic effects and decrease the androgenic side effects. These derivatives are commonly known as anabolic androgenic steroids (AAS) (15). More than a hundred synthetic products have been developed by different reactions (17 α-alkylation, 17 β-esterification, etc.) to overcome the rapid biotransformation of testosterone and synthesize orally active longer acting compounds (9, 15). Oxandrolone, oxymetholone and nandrolone are commonly used AAS, whereas danazol (2,3-isoxazol-17α-ethynyltestosterone) is a synthetic steroid with antiestrogenic, antigonadotropic, and androgenic activities (15). Hepatotoxicity is a potential side effect of anabolic steroids traditionally observed with the 17 α-alkylated compounds (methyltestosterone, oxymetholone, oxandrolone, norethandrolone, etc.) (16). Around a quarter of patients may experience elevation in liver function tests while on therapy and liver tumors are not uncommon (9). Early studies reported fatality cases from liver disease and jaundice; however, it is unclear if these were due to the anabolic steroids or other potential complications observed in patients with BMF like viral hepatitis, iron overload. The optimal recommended dose of androgens is not well defined; however, it is well known that patients who do not respond to a certain dose may achieve remission using a higher dose of the same product. The recommended doses of the commonly used products are: 2.5 mg/kg/d for oxymetholone and methanolone and 1 mg/kg/d for methandrostenolone and Norethandrolone (9, 13). Given the biological effects of AAS, serious adverse events can happen (masculinization, aggression, liver dysfunction and adenomas among others). Close medical supervision and dose adjustment to the minimal effective dose is recommended. Androgens should be avoided in pregnant women, cancer patients (prostate, breast, etc.), patients with nephrotic syndrome or liver dysfunction and patients with hypercalcemia of malignancy. The androgen side effects (flushing, acne, hirsutism, change in voice, others) usually disappear quickly after discontinuation (17). Table 1 is a summary of side effects and authors’ recommendations on how to mitigate these.
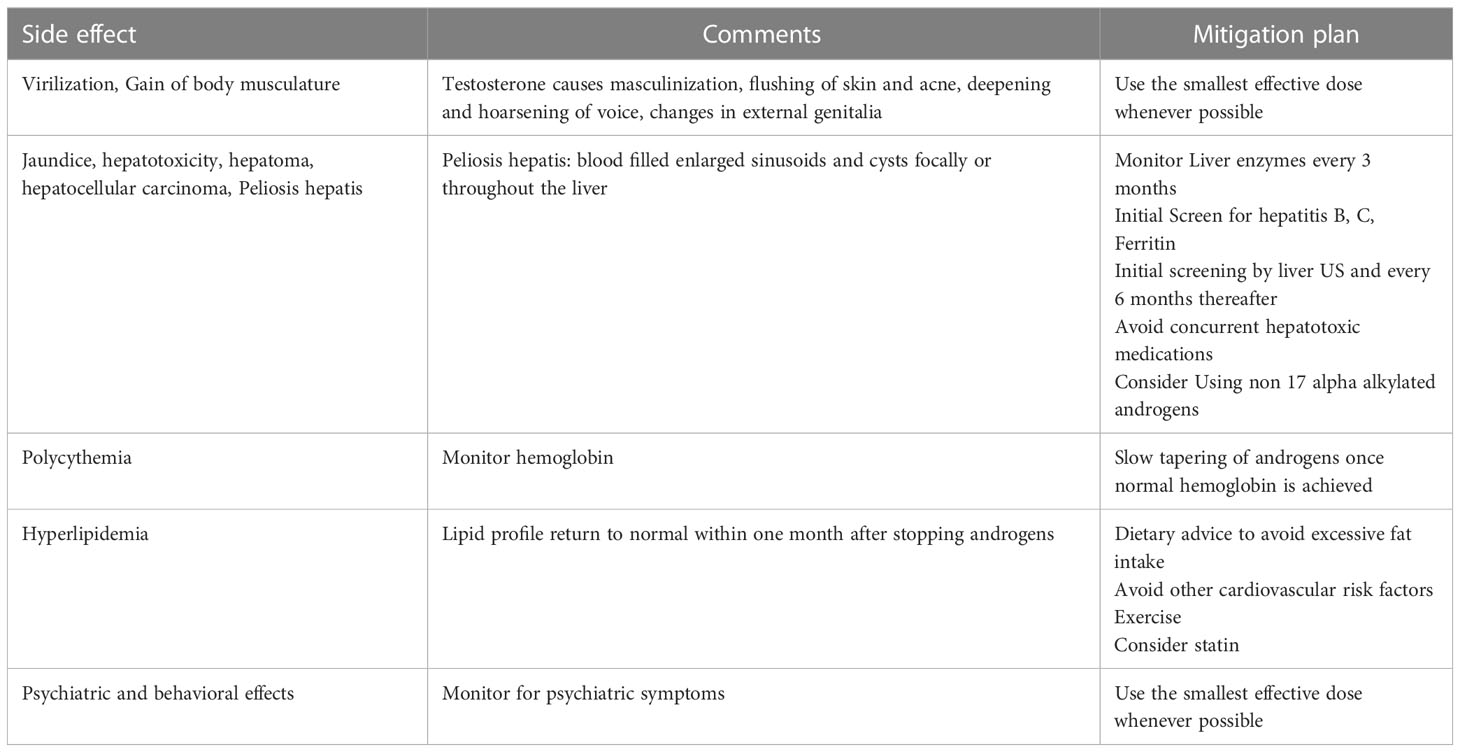
Table 1 Potential side effects of androgens and authors’ recommendations on how to mitigate these.
A randomized trial compared anti-lymphocyte globulin (ALG) (with androgens and haploidentical HSCT vs. Androgens alone) showed 76% vs. 31% survival respectively at two years (p <0.002) (18). Another trial randomized 121 patients to receive anti-thymocyte globulin (ATG) alone or ATG with androgens showed similar response (44% vs 42% respectively) and survival rates (19). In a subsequent trial, 15 patients received ATG and methanolone and 15 patients received ATG alone (20). The response rate was 73% in the combination group with eight complete responses compared to 33% in the ATG alone group with two complete responses (P = 0.01). The difference in survival (87% in the combination arm vs 43%) was not statistically significant. Shahidi et al. treated 23 AA patients with oxymetholone and cyclosporine combination. Thirteen of these patients had already received ATG and did not respond and the remaining 10 did not receive ATG. The response rate was 38% and 70% respectively (21). Further, a randomized controlled trial showed significant difference in responses among males and females to androgens, where females with low neutrophil counts had significant benefit from ATG combined with androgens compared with ATG alone (22). Bacigalupo et al. randomized 134 patients to ALG and methylprednisolone with or without oxymetholone. At 4 months, the response rate with significantly higher in patients who received oxymetholone (56% vs 40%; P < 0.04) (22). In a relatively recent report, Jaime-Pérez et al. reported the outcomes of fifty AA patients (23). Thirteen patients were transplanted and 37 patients were not eligible to transplant, had no access to IST, and as such were treated with danazol (median dose 400 mg) and supportive measures. The five-year OS was in favor of the transplant group (92% vs 41%, p = 0.001). The ORR in the danazol group was 46% with a median time to respond of 3 months. Although, transplant and IST are highly efficacious in AA, androgens continue to be an option, even in the frontline, for transplant ineligible patients with no access to modern IST.
Congenital bone marrow failure syndromes are a heterogeneous group of cytopenias associated with various congenital defects and cancer predisposition. HSCT is the only curative treatment for the hematological complications related to these diseases, but many patients are ineligible and androgens are considered the main non-transplant modality to treat these patients. Early studies of using androgens in these patients showed favorable responses (8). Oxymetholone and danazol are frequently used for Fanconi anemia (FA) and dyskeratosis congenita (DC) patients with responses reaching up to 80% (24–26). Diamond-Blackfan anemia patients are usually treated with steroids but many of them fail steroids (tolerance, side effects, relapse) and eventually receive androgens (24). Oxymetholone is the androgen of choice for congenital anemias with a starting dose of 0.5-2 mg/kg/day. Expectedly, response starts within 4-8 weeks and once a hemoglobin concentration of 12 g/dl is reached the dose is reduced gradually to the minimum effective dose to maintain hemoglobin between 10-12 g/dl (25). In paroxysmal nocturnal hemoglobinuria (PNH), a rare acquired clonal stem cell disorder, androgens were efficacious to treat the anemia part of the disease especially in patients with hypoplasia (27–29). However, androgens have no effect on hemolysis and their impact on thrombogenesis need to be watched closely in these patients.
Fanconi anemia is the prototype of inherited bone marrow failure syndromes characterized by a number of mutations leading to genetic instability and multiple cancer susceptibility with frequent incidence of marrow failure and myelodysplasia (30–32). Clinically, FA patients are characterized by diverse congenital malformations (small stature, skeletal malformations, hyperpigmentation, urogenital abnormalities, etc.) (32). In a small cohort of FA patients, seven out of eight patients responded to danazol 5 mg/kg/day and had stable counts up to 3 years (33). In another cohort, seven out nine patients treated with oxandrolone had a hematologic response with major side effects being elevated liver function tests and virilzation (34). A retrospective trial analyzed 70 patients who received androgens for FA. Out of 70 patients, 37 were evaluable. Oxymetholone was the most frequently used androgen. Hematologic response was seen in 25 out 37 evaluable patients (68%) with a median of 6.5 g/dl improvement in hemoglobin (median time to respond of 14 weeks), a median of 70000 platelet count increase (median time to respond of 11.5 weeks) and a median of 1350/ml improvement in neutrophils (median time to respond of 12 weeks) (35). Virilization, liver toxicity, liver adenomas and clonal evolution were the most frequently reported adverse events. In the largest retrospective trial addressing androgen use in FA patients, 66 patients were reported; 49 received oxymetholone and 17 received danazol (36). Danazol was started at a dose of 2-4 mg/kg/day and oxymetholone was started at as dose of 0.5-1 mg/kg/day. After a median duration of therapy of 18 months, 52 patients (78%) achieved hematologic response and 30 patients (45%) had trilineage response. There was no difference in response rates between danazol and oxymetholone. Seven patients (11%) developed grade 3 liver toxicity that was noticed more in patients on oxymetholone. Peliosis hepatis developed in one patient on oxymetholone. The majority of patients developed virilzation signs. These reports included patients from different age groups (age range: 3 – 22 years).
Telomeres are essential for genomic stability but their length decreases with each cellular division. Dyskeratosis congenita (DC) is the prototype of telomeropathies. Androgens improve blood counts and reduce transfusion frequency in telomeropathies. Some studies have shown improvement in telomere length as well (37–41), although other reports did not confirm this finding (42). Apparently, the improvement in telomere length depends on the underlying mutational profile (41). In a phase 1/2 study, danazol (800 mg/day) was administered to patients with telomeropathies. In 12 evaluable patients, telomere elongation was achieved in all. Hematologic response was seen in 19 of 24 evaluable patients (79%) after 3 months of therapy. Liver toxicity (41%) and muscle cramps (33%) were the most frequently reported side effects (37). In another study, 26 DC patients were followed prospectively. Ten patients received androgens and 16 were not treated. There was no statistical difference in telomere length in the two groups (42). Seven out of the 10 treated patients had a consistent RBC and platelets response to androgens. In a more recent report, seven patients were treated with androgens (danazol, oxymetholone). All patients had hematological response as well as significant increase in telomere length (41). An ongoing trial (clinicaltrials.gov NCT02055456) is evaluating nandrolone decanoate (parenteral androgen with no first hepatic pass) in patients with telomeropathies. These reports included patients from different age groups (age range: 3 – 66 years). Table 2 is a summary of androgen studies in AA and BMF syndromes.
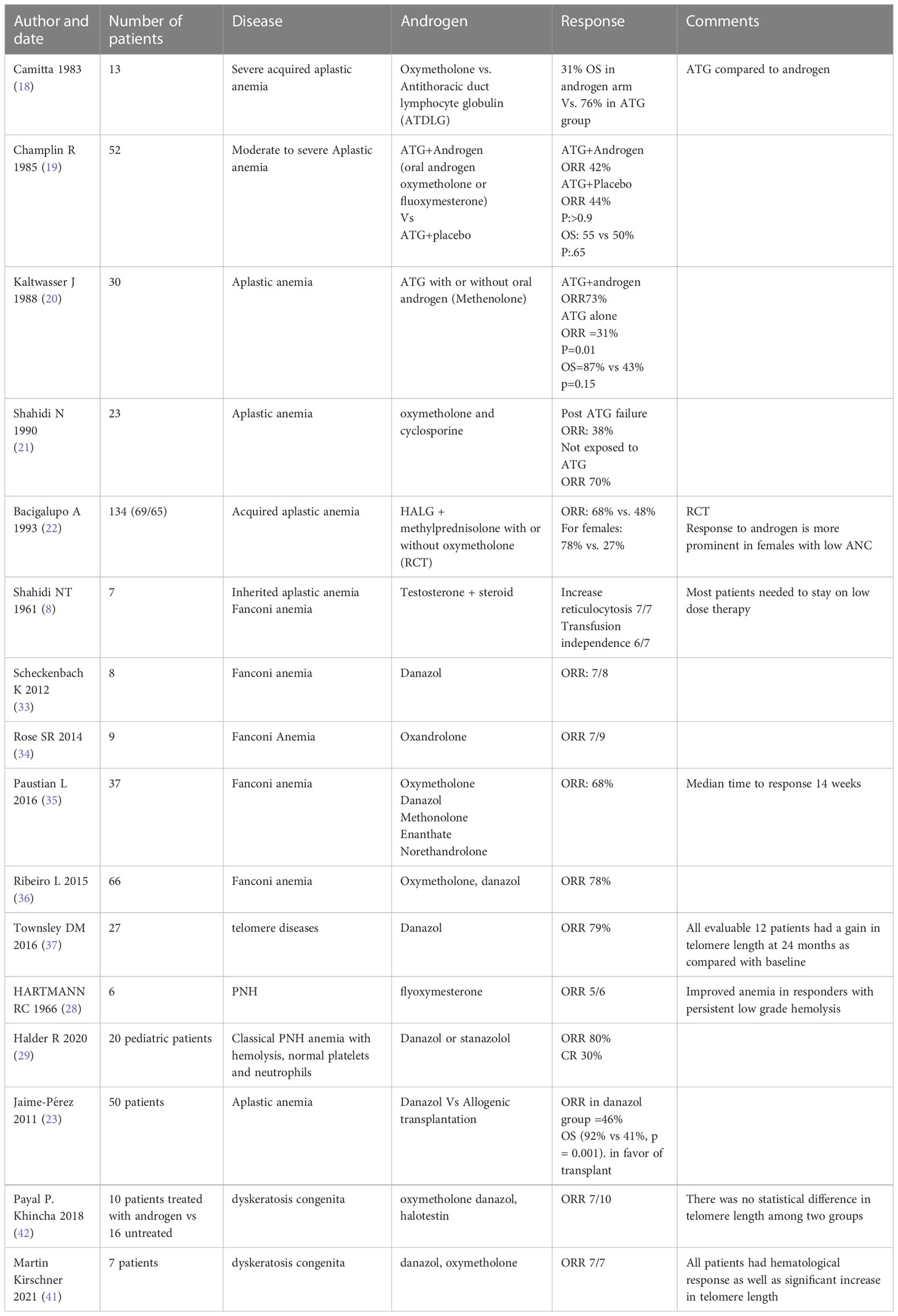
Table 2 Important studies about androgens in BMF patients.
The exact mechanism of action of androgens in stimulating hematopoiesis remains unknown, however it seems that the use of supra-physiological doses of androgens cause erythropoiesis expansion. This is in contrast to hematinic supplements (iron, folate) where excess supply will not cause excessive response in hematopoiesis. Earlier studies showed that androgens enhance the responsiveness of erythroid progenitors to erythropoietin and possibly enhance the growth of pluripotent and committed granulocyte/macrophage progenitors (19). Some of the anabolic steroids have unique properties, for example, danazol inhibits interleukin-1 and TNF-α production (a property of corticosteroids) and has myelosuppressive effects (43). More recent studies showed that androgens stimulate erythropoietin production and release, activation of the erythropoietin receptor on progenitor cells and increase iron incorporation into the red cells (44, 45). Additionally, androgens increase telomerase activity in hematopoietic cells (39). Lately, a study showed that the chronic use of oxymetholone improves hematological parameters by diminution of quiescence and promotion of proliferation of hematopoietic progenitors and stem cells. Oxymetholone down regulated the transcription of osteopontin, a cytokine that up-regulates the expression of certain interferons and interleukins, which inhibits cellular proliferation. Hence, it was proposed that oxymetholone suppression of osteopontin transcription induces hematopoietic stem cell cycling (46). The earliest phase of erythroid response is characterized by erythrocytosis that happens shortly after initiating androgen therapy followed by delayed improvement in hemoglobin. This delay is probably related to an initial increase in erythrocyte destruction while patients are still transfusion dependent. Usually, the improvement of hemoglobin may be observed as early as 3 months or as late as 6 months after starting androgen therapy (13). The increase in neutrophils usually mirrors the response of hemoglobin. The response rate of neutrophils was found to be 35.8% in one case series (8, 13). Platelets are the latest to improve and usually show less prominent improvement (13). The response rate of platelets is observed in about one-third of cases. In one study, normal platelets were achieved in 18 out of 67 patients (8, 13). Of note that despite the minimal improvement in the numbers of neutrophils and platelets, the clinical benefit, in terms of less bleeding and infections is disproportionately higher (9). Responding patients can achieve a normal hemoglobin level and a protective platelets and neutrophils levels (8). The bone marrow examination of patients receiving androgens show groups of growing stromal cells, reduction of fat cells and the appearance of erythroid hyperplasia foci. These changes are usually seen within 3 months of treatment initiation (7). In summary, response to androgens starts 3 to 6 months after treatment initiation and responding patients may enjoy durable response in around 50% of cases while the other 50% will relapse with relapse being higher in rapidly tapered patients (< 3 months) (9, 17). A second remission can be achieved with re-treatment but these patients will need continuous androgen therapy thereafter (17). Upon withdrawal of androgens, the reticulocytes and hemoglobin drop within the first month, and then stabilize during the second month with similar effects in the neutrophils and platelets.
The diagnostic armamentarium is expanding with the use of new and more comprehensive sequencing and molecular techniques. These new diagnostic tools help to better delineate these syndromes and to identify more patients with cryptic alterations who may not benefit from immunosuppression. A number of innovative ideas and approaches (gene therapy, leucine, quercetin, etc.) to address the unmet needs of these patients are in ongoing trials. Bone marrow failure patients who are not candidates for transplant (elderly, comorbidities, no donors, etc.) and patients with the non-severe forms are usually defaulted to non-transplant medical interventions. In affluent countries, a number of non-transplant options are available for this group of patients. However, in restricted resources countries these novel options are not readily available. Androgens are considered a classic old group of medications that can stimulate hematopoiesis and as such used for this group of disorders when modern resources are not available or have failed already. Androgens result in hematologic responses (transient in some patients however) in most patients with FA and telomeropathies but does not alter nor affect the risk of clonal evolution. A number of pros and cons have to be considered when a decision is made to treat a BMF patient with non-transplant modalities including the use of androgens. Factors linked to a potential better response to androgens include higher residual cellularity, mild to moderate cytopenia, toxin induced BMF, women with lower absolute neutrophil count, the use of higher dose of androgens and rapid improvement of counts after androgen initiation (9, 13, 14). The presence of a number of these factors in a patient may sway the managing team to consider androgens, while the presence of contraindications may push the team to consider alternatives. Below are selected scenarios in which the authors’ believe androgen therapy should be considered.
- As a bridge to transplant in patients with symptomatic FA and telomeropathies
- Older SAA patients, not candidate for HSCT and failed standard immunosuppression therapy (IST) and thrombopoietin mimetic (TPO) or TPO inaccessible
- Patients with renal failure precluding the use of calcineurin inhibitors and failed TPO mimetic or TPO inaccessible
- Multiply relapsed patients after failing standard lines of therapy
- PNH patients with no access to complement inhibitors and parallel existing AA (AA/PNH overlap)
Currently, there are no published trials looking into the safety, efficacy and different dosages of various AAS formulations to guide the clinicians’ choice when treating BMF patients. New trials looking into these issues are warranted.
MA, RE, and MN designed and performed the research. MN wrote the first draft. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
2. El Fakih R, Alfraih F, Alhayli S, Ahmed SO, Shaheen M, Chaudhri N, et al. Frontline-matched sibling donor transplant of aplastic anemia patients using primed versus steady-state bone marrow grafts. Ann Hematol (2022) 101(2):421–8. doi: 10.1007/s00277-021-04708-4
3. Bacigalupo A, Hows J, Gluckman E, Nissen C, Marsh J, Van Lint M, et al. Bone marrow transplantation (BMT) versus immunosuppression for the treatment of severe aplastic anaemia (SAA): a report of the EBMT* SAA working party. Br J haematol (1988) 70(2):177–82. doi: 10.1111/j.1365-2141.1988.tb02460.x
4. Scheinberg P. Aplastic anemia: therapeutic updates in immunosuppression and transplantation. Hematol 2010 Am Soc Hematol Educ Program Book. (2012) 2012(1):292–300. doi: 10.1182/asheducation.V2012.1.292.3798310
5. Camitta BM, Thomas ED, Nathan DG, Santos G, Gordon-Smith E, Gale RP, et al. Severe aplastic anemia: a prospective study of the effect of early marrow transplantation on acute mortality. Blood. (1976) 48:63–70. doi: 10.1182/blood.V48.1.63.bloodjournal48163
6. Camitta BM, Thomas ED, Group IAAS. Severe aplastic anaemia: a prospective study of the effect of androgens or transplantation on haematological recovery and survival. Clinics haematol (1978) 7(3):587–95. doi: 10.1016/S0308-2261(21)00051-5
7. Shahidi NT, Diamond LK. Testosterone-induced remission in aplastic anemia. AMA J Dis Children (1959) 98(3):293–302. doi: 10.1001/archpedi.1959.02070020295002
8. Shahidi NT, Diamond LK. Testosterone-induced remission in aplastic anemia of both acquired and congenital types. Further observations 24 cases N Engl J Med (1961) 264:953–67. doi: 10.1056/NEJM196105112641901
9. Sanchez-Medal L, Gomez-Leal A, Duarte L, Rico MG. Anabolic androgenic steroids in the treatment of acquired aplastic anemia. Blood. (1969) 34(3):283–300. doi: 10.1182/blood.V34.3.283.283
10. Daiber A, Herveé L, Con I, Donoso A. Treatment of aplastic anemia with nandrolone decanoate. Blood. (1970) 36(6):748–53. doi: 10.1182/blood.V36.6.748.748
11. Allen DM, Fine MH, Necheles TF, Dameshek W. Oxymetholone therapy in aplastic anemia. Blood. (1968) 32(1):83–9. doi: 10.1182/blood.V32.1.83.83
12. Skarberg K, Engstedt L, Jameson S, Killander A, Lundh B, Pers B, et al. OXYMETHOLONE TREATMENT IN HYPOPROLIFERATIVE ANEMIA. 1. FREQUENCY OF RESPONSE. Acta Haematologica (1973) 49(6):321–30. doi: 10.1159/000208422
13. Najean Y, Pecking A, Danvic ML, CGftSo A, Secretaries RA. Androgen therapy of aplastic anaemia-a prospective study of 352 cases. Scandinavian J Haematol (1979) 22(4):343–56. doi: 10.1111/j.1600-0609.1979.tb00430.x
14. Najean Y. Aplastic fcgftso, anaemias r. androgen therapy in aplastic anaemia: a comparative study of high and low-doses and of 4 different androgens. Scandinavian J Haematol (1986) 36(4):346–52.
15. Shahidi NT. A review of the chemistry, biological action, and clinical applications of anabolic-androgenic steroids. Clin Ther (2001) 23(9):1355–90. doi: 10.1016/S0149-2918(01)80114-4
16. Al-Sharefi A, Mohammed A, Abdalaziz A, Jayasena CN. Androgens and anemia: current trends and future prospects. Front Endocrinol (2019) 10:754. doi: 10.3389/fendo.2019.00754
17. Najean Y. Long-term follow-up in patients with aplastic anemia: a study of 137 androgen-treated patients surviving more than two years. Am J Med (1981) 71(4):543–51. doi: 10.1016/0002-9343(81)90204-7
18. Camitta B, O'Reilly RJ, Sensenbrenner L, Rappeport J, Champlin R, Doney K, et al. Antithoracic duct lymphocyte globulin therapy of severe aplastic anemia. Blood. (1983) 62:883–8. doi: 10.1182/blood.V62.4.883.bloodjournal624883
19. Champlin R, Ho W, Feig S, Winston D, Lenarsky C, Gale R. Do androgens enhance the response to antithymocyte globulin in patients with aplastic anemia? a prospective randomized trial. Blood. (1985) 66(1):184–8. doi: 10.1182/blood.V66.1.184.184
20. Kaltwasser J, Dix U, Schalk K, Vogt H. Effect of androgens on the response to antithymocyte globulin in patients with aplastic anaemia. Eur J haematol (1988) 40(2):111–8. doi: 10.1111/j.1600-0609.1988.tb00806.x
21. Shahidi N, Wang W, Shurin S, Finlay J, Sondel P, Dinndorf P. Treatment of acquired aplastic anemia with cyclosporine and androgens. In: Shahidi NT ed. Aplastic anemia and other bone marrow failure syndromes. Springer-Verlag New York Berlin Heidelberg London Paris Tokyo (1990). p. 155–65.
22. Bacigalupo A, Chaple M, Hows J, Van Lint M, McCann S, Milligan D, et al. Treatment of aplastic anaemia (AA) with antilymphocyte globulin (ALG) and methylprednisolone (MPred) with or without androgens: a randomized trial from the EBMT SAA working party. Br J haematol (1993) 83(1):145–51. doi: 10.1111/j.1365-2141.1993.tb04645.x
23. Jaime-Pérez JC, Colunga-Pedraza PR, Gómez-Ramírez CD, Gutiérrez-Aguirre CH, Cantú-Rodríguez OG, Tarín-Arzaga LC, et al. Danazol as first-line therapy for aplastic anemia. Ann Hematol (2011) 90(5):523–7. doi: 10.1007/s00277-011-1163-x
24. Calado RT, Clé DV. Treatment of inherited bone marrow failure syndromes beyond transplantation. Hematol 2014 Am Soc Hematol Educ Program Book. (2017) 2017(1):96–101. doi: 10.1182/asheducation-2017.1.96
25. Glader BE, Guinan E, Lipton JM, Boxer L. Congenital bone marrow failure syndromes: diagnosis and therapeutic strategies. Am Soc Hematol Educ Program Book Washington DC: Am Soc Hematol (1998) 1998:384–403.
26. Khincha PP, Wentzensen IM, Giri N, Alter BP, Savage SA. Response to androgen therapy in patients with dyskeratosis congenita. Br J Haematol (2014) 165(3):349–57. doi: 10.1111/bjh.12748
27. Rosse WF. Treatment of paroxysmal nocturnal hemoglobinuria. Blood. (1982) 60(1):20–3. doi: 10.1182/blood.V60.1.20.20
28. Hartmann Rc, Jenkins De Jr, Mckee Lc, Heyssel Rm. Paroxysmal nocturnal hemoglobinuria: clinical and laboratory studies relating to iron metabolism and therapy with androgen and iron. Medicine (1966) 45(5):331–63. doi: 10.1097/00005792-196609000-00001
29. Halder R, Mishra P, Aggarwal M, Mannivanan P, Dhawan R, Seth T, et al. Outcomes of paroxysmal nocturnal hemoglobinuria in the pediatric age group in a resource-constrained setting. Pediatr Blood Cancer. (2020) 67(4):e27712. doi: 10.1002/pbc.27712
30. Antoniou AC, Casadei S, Heikkinen T, Barrowdale D, Pylkäs K, Roberts J, et al. Breast-cancer risk in families with mutations in PALB2. New Engl J Med (2014) 371(6):497–506. doi: 10.1056/NEJMoa1400382
31. D'Andrea AD. Susceptibility pathways in fanconi's anemia and breast cancer. New Engl J Med (2010) 362(20):1909–19. doi: 10.1056/NEJMra0809889
32. Auerbach AD. Fanconi anemia and its diagnosis. Mutat Research/Fundamental Mol Mech Mutagenesis (2009) 668(1-2):4–10. doi: 10.1016/j.mrfmmm.2009.01.013
33. Scheckenbach K, Morgan M, Filger-Brillinger J, Sandmann M, Strimling B, Scheurlen W, et al. Treatment of the bone marrow failure in fanconi anemia patients with danazol. Blood Cells Molecules Diseases (2012) 48(2):128–31. doi: 10.1016/j.bcmd.2011.11.006
34. Rose SR, Kim MO, Korbee L, Wilson KA, Douglas Ris M, Eyal O, et al. Oxandrolone for the treatment of bone marrow failure in fanconi anemia. Pediatr Blood Cancer. (2014) 61(1):11–9. doi: 10.1002/pbc.24617
35. Paustian L, Chao MM, Hanenberg H, Schindler D, Neitzel H, Kratz CP, et al. Androgen therapy in fanconi anemia: a retrospective analysis of 30 years in Germany. Pediatr Hematol Oncol (2016) 33(1):5–12. doi: 10.3109/08880018.2015.1129567
36. Ribeiro L, Pilonetto D, Bitencourt M. Treatment of bone marrow failure in 49 fanconi anemia patients with oxymetholone. Rev Bras Hematol Hemoter (2015) 37(suppl 1):220.
37. Townsley DM, Dumitriu B, Liu D, Biancotto A, Weinstein B, Chen C, et al. Danazol treatment for telomere diseases. New Engl J Med (2016) 374(20):1922–31. doi: 10.1056/NEJMoa1515319
38. Ziegler P, Schrezenmeier H, Akkad J, Brassat U, Vankann L, Panse J, et al. Telomere elongation and clinical response to androgen treatment in a patient with aplastic anemia and a heterozygous hTERT gene mutation. Ann hematol (2012) 91:1115–20. doi: 10.1007/s00277-012-1454-x
39. Calado RT, Yewdell WT, Wilkerson KL, Regal JA, Kajigaya S, Stratakis CA, et al. Sex hormones, acting on the TERT gene, increase telomerase activity in human primary hematopoietic cells. Blood J Am Soc Hematol (2009) 114(11):2236–43. doi: 10.1182/blood-2008-09-178871
40. Bär C, Huber N, Beier F, Blasco MA. Therapeutic effect of androgen therapy in a mouse model of aplastic anemia produced by short telomeres. Haematologica. (2015) 100(10):1267. doi: 10.3324/haematol.2015.129239
41. Kirschner M, Vieri M, Kricheldorf K, Ferreira MSV, Wlodarski MW, Schwarz M, et al. Androgen derivatives improve blood counts and elongate telomere length in adult cryptic dyskeratosis congenita. Br J Haematol (2021) 193(3):669–73. doi: 10.1111/bjh.16997
42. Khincha PP, Bertuch AA, Gadalla SM, Giri N, Alter BP, Savage SA. Similar telomere attrition rates in androgen-treated and untreated patients with dyskeratosis congenita. Blood advances (2018) 2(11):1243–9. doi: 10.1182/bloodadvances.2018016964
43. Chuhjo T, Yamazaki H, Omine M, Nakao S. Danazol therapy for aplastic anemia refractory to immunosuppressive therapy. Am J hematol (2008) 83(5):387–9. doi: 10.1002/ajh.21118
44. Shahani S, Braga-Basaria M, Maggio M, Basaria S. Androgens and erythropoiesis: past and present. J endocrinological Invest (2009) 32(8):704–16. doi: 10.1007/BF03345745
45. Maggio M, Snyder P, Ceda G, Milaneschi Y, Luci M, Cattabiani C, et al. Is the haematopoietic effect of testosterone mediated by erythropoietin? the results of a clinical trial in older men. Andrology. (2013) 1(1):24–8. doi: 10.1111/j.2047-2927.2012.00009.x
Keywords: androgen, aplastic anemia (AA), bone marrow failure (BMF), hematopoiesis, anabolic steroid
Citation: Nassani M, Fakih RE, Passweg J, Cesaro S, Alzahrani H, Alahmari A, Bonfim C, Iftikhar R, Albeihany A, Halkes C, Ahmed SO, Dufour C and Aljurf M (2023) The role of androgen therapy in acquired aplastic anemia and other bone marrow failure syndromes. Front. Oncol. 13:1135160. doi: 10.3389/fonc.2023.1135160
Received: 31 December 2022; Accepted: 06 April 2023;
Published: 08 May 2023.
Edited by:
Jean El Cheikh, American University of Beirut Medical Center, LebanonReviewed by:
Fabian Beier, University Hospital RWTH Aachen, GermanyCopyright © 2023 Nassani, Fakih, Passweg, Cesaro, Alzahrani, Alahmari, Bonfim, Iftikhar, Albeihany, Halkes, Ahmed, Dufour and Aljurf. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Riad El Fakih, cmlhZGZha2loQGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.