 Bobo Zheng
Bobo Zheng Quan Wang
Quan Wang Mingtian Wei
Mingtian Wei Yumin Yue1
Yumin Yue1 Xiaojun Li
Xiaojun Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol. , 15 February 2023
Sec. Surgical Oncology
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1116502
This article is part of the Research Topic Recent Advances and New Challenges in Minimally Invasive Surgery and Chemotherapy for Colorectal Cancer View all 7 articles
Background: There is controversy about the outcomes of prophylactic ileostomy via the specimen extraction site (SES) after laparoscopic rectal cancer surgery (LRCS). We, therefore, performed a meta-analysis to determine the efficacy and safety of stoma through the SES versus new site (NS).
Methods: All relevant studies from 1997 to 2022 were searched in the PubMed, EMBASE, Cochrane Library, CNKI, VIP databases. This meta-analysis was performed using RevMan software 5.3 for statistical analysis.
Results: 7 studies with 1736 patients were included. The present meta-analysis noted that prophylactic ileostomy via SES was associated with a higher risk of overall stoma-related complications, especially parastomal hernia (OR, 2.39, 95% CI 1.43-4.00; p=0.0008). No statistical difference was found in terms of wound infection, ileus, stoma edema, stoma prolapse, stoma necrosis, stoma infection, stoma bleeding, stoma stenosis, skin inflammation around the stoma, stoma retraction and postoperative pain score on postoperative day 1 and 3 between SES group and NS group. However, prophylactic ileostomy via SES was associated with lesser blood loss (MD = -0.38, 95% CI: -0.62 - -0.13; p=0.003), shorter operation time(MD = -0.43, 95% CI: -0.54 - -0.32 min; p<0.00001), shorter post-operative hospital stay (MD = -0.26, 95% CI: -0.43 - -0.08; p=0.004), shorter time to first flatus(MD = -0.23, 95% CI: -0.39 - -0.08; p=0.003) and lower postoperative pain score on postoperative day 2.
Conclusion: Prophylactic ileostomy via SES after LRCS reduces new incision, decreases operative time, promotes postoperative recovery, and improves cosmetic outcomes, but may increase the incidence of parastomal hernias. The vast majority of parastomal hernias can be repaired by closing the ileostomy, therefore SES remain an option for temporary ileostomy after LRCS.
Colorectal cancer (CRC) remains the third most common cancer in the world (1). Surgery is still the main treatment option. With the development of laparoscopic technology, laparoscopic rectal cancer surgery (LRCS) has been widely carried out, and achieve better treatment results (2). Laparoscopic surgery was able to achieve similar disease-free survival and longer overall survival compared to open surgery (3). Laparoscopic surgery has replaced open surgery as the mainstream treatment for rectal cancer.
Anastomotic leak (AL) is a serious complication of rectal cancer surgery, associating with high local recurrence rates and poor survival (4). The incidence of anastomotic leakage after anterior resection remains disturbingly high, ranging from 3.5% - 17.0% (5–8). When performing laparoscopic low anterior resection, prophylactic ileostomy is considered to prevent AL in patients with low anastomosis levels, receiving neoadjuvant concurrent radiotherapy or at high risk of anastomotic leak due to vascular incompetence (9–11).
With the widespread use of Natural orifice specimen extraction surgery (NOSES) in laparoscopic colorectal cancer surgery(LCRCS) in recent years, it is gradually becoming recognized by more surgeons. Several studies have shown that NOSES can significantly accelerate postoperative recovery and achieve cosmetic results compared to conventional laparoscopic colorectal cancer surgery, while there is no statistical difference in 3-year overall survival time and disease-free survival time between NOSES and conventional LCRCS (12–15). For patients with rectal cancer requiring prophylactic ileostomy, an new incision in the abdomen is unavoidable, so theoretically it would be more in line with the minimally invasive concept to perform prophylactic ileostomy through specimen extraction site (SES).
Conventional LRCS requires an abdominal incision (approximately 4-8 cm) to remove the specimen, which increases the incision-related complications, including incision site infection, incisional steatosis and incisional hernia (14, 16, 17). However, there is controversy about the outcomes of prophylactic ileostomy via SES. Yoo SB reported that no statistical differences were found for prophylactic ileostomy through SES or new site (NS) after LRCS (18), however, several studies in recent years reported stoma through the SES was be superior than NS (19–21). We, therefore, performed a meta-analysis to determine the efficacy and safety of stoma through the SES versus NS.
The present meta-analysis follows Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) reporting guidelines (22).
All relevant studies from 1997 to 2022 were searched in the PubMed, EMBASE, Cochrane Library, CNKI (China National Knowledge Infrastructure Whole Article Database), VIP (http://vip.hbsti.ac.cn/) databases. The following search terms were used:
“Laparoscopic”, “rectal cancer surgery”, “low anterior resection”, “ileostomy”, “stoma”, “the specimen extraction site” and “new site”. The latest search date for this study was October 22, 2022. The search strategy was not restricted to languages.
The inclusion criteria were as follows (1): Case-control studies, including randomized controlled trials, prospective studies and retrospective studies (2), The patient underwent laparoscopic surgery for rectal cancer and had a prophylactic ileostomy (3), Study comparing the safety and efficacy of ileostomy via SES with NS;
The exclusion criteria were as follows (1): The studies were case reports, reviews, or comments (2), Study did not compare prophylactic ileostomy via SES with NS after LRCS (3). The meeting abstract did not provide detailed data.
The primary outcomes of interest were stoma-related complications (including parastomal hernia, stoma edema, stoma prolapse, stoma necrosis, stoma infection, stoma bleeding, stoma stenosis, skin inflammation around the stoma, stoma retraction).
The secondary outcomes were blood loss, operation time, post-operative hospital stay, time to first flatus, ileus, wound infection and postoperative pain score.
Postoperative pain score was performed by the nurse in charge using the numerical rating system (NRS).
The following data was extracted from each included study: country, year, No. of patients, age, sex, body mass index (BMI), neoadjuvant chemoradiation, pTNM, stoma site, the specimen extraction site and outcomes. The data was extracted by two authors separately, and a third author was added to discuss the decision in case of disagreement.
The methodological quality of the included literature was evaluated using the Newcastle-Ottawa Quality Assessment Scale (NOS) (23).
We used Revman Statistical Software (Ver. 5.3 Copenhagen, Denmark) for statistical analysis. For binary data, the pooled outcomes were expressed as odds ratios (ORs) and 95% confidence intervals (95% CI). For continuous data, the pooled outcomes were reported as mean differences and 95% CI. If the article provided only the median and range, the formula described by Hozo SP was used to calculate the mean and standard deviation (24). Heterogeneity was evaluated using the i-squared statistic, and when i-squared > 50%, it was considered to have considerable heterogeneity, which was then analyzed statistically using a random-effects model, otherwise a fixed-effects model was used. A p value < 0.05 was considered statistically significant.
A total of 670 studies were obtained by the literature search strategy described above (Figure 1). After removal of duplicates, 430 literature abstracts were reviewed and assessed according to the inclusion and exclusion criteria. 43 studies were downloaded in full for screening. Seven studies were finally included for quantitative analysis. The total number of participants in the 7 included studies (18–21, 25–27) was 1736. Overall, 704 patients underwent prophylactic ileostomy via the SES, while 1032 patients underwent prophylactic ileostomy via the NS after LRCS.
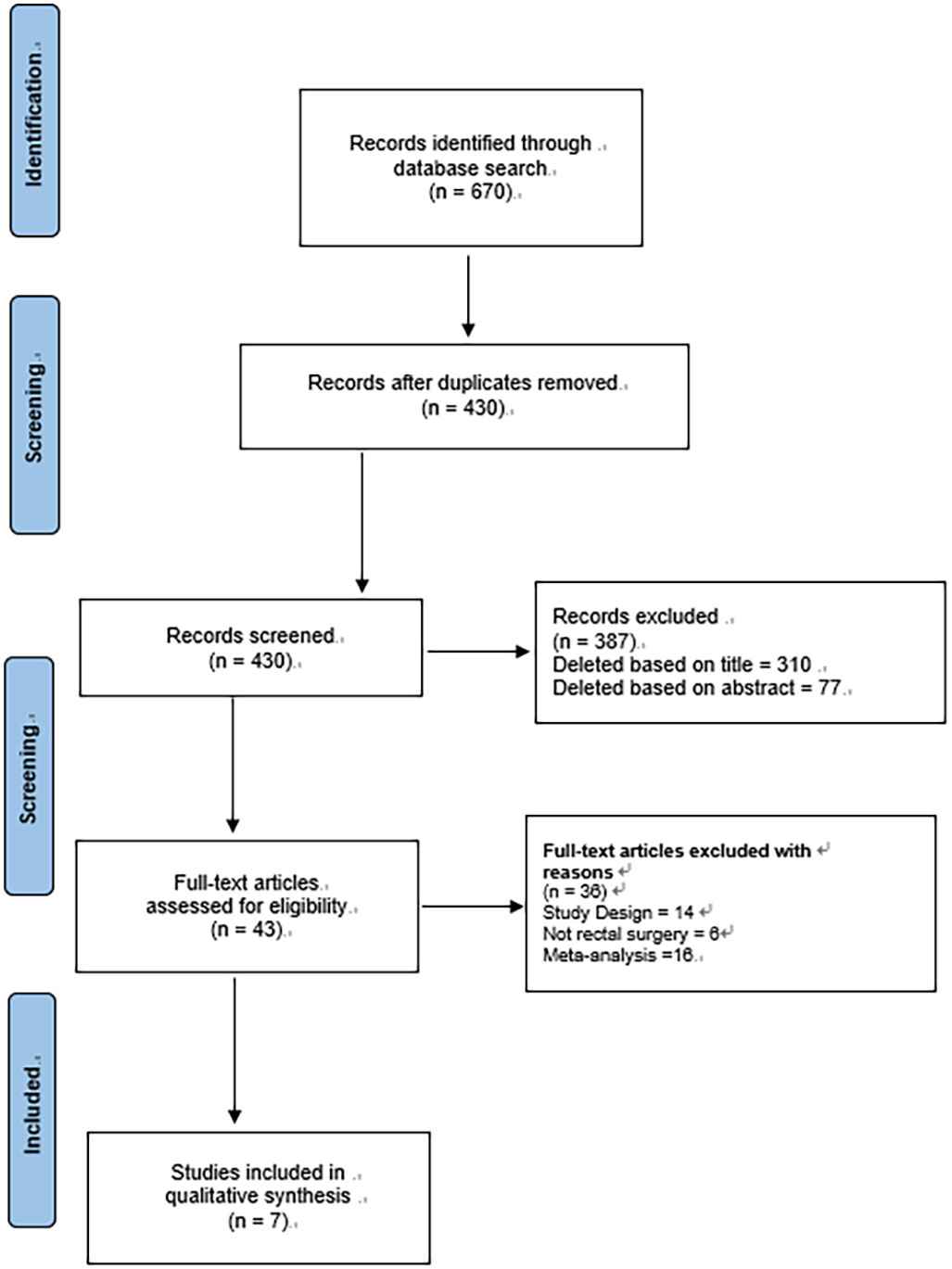
Figure 1 Flowchart of the screening process for included studies.
Table 1 showed characteristics of the included studies. Four studies were completed in China (19, 21, 25, 27), two studies (18, 20) in Korea and one study (26) in Turkey. Three studies (21, 25, 26) performed prophylactic ileostomy at the right lower abdominal SES, two studies (18, 19) performed ileostomy at the left lower abdominal SES, one study (27) performed ileostomy at the median lower abdominal SES, and one study (20) performed ileostomy at either the left lower abdominal or right lower abdominal SES. All included studies were retrospective in design (Table 2). One study (27) had an NOS score of 7 and the remaining 6 studies had an NOS score of 8.
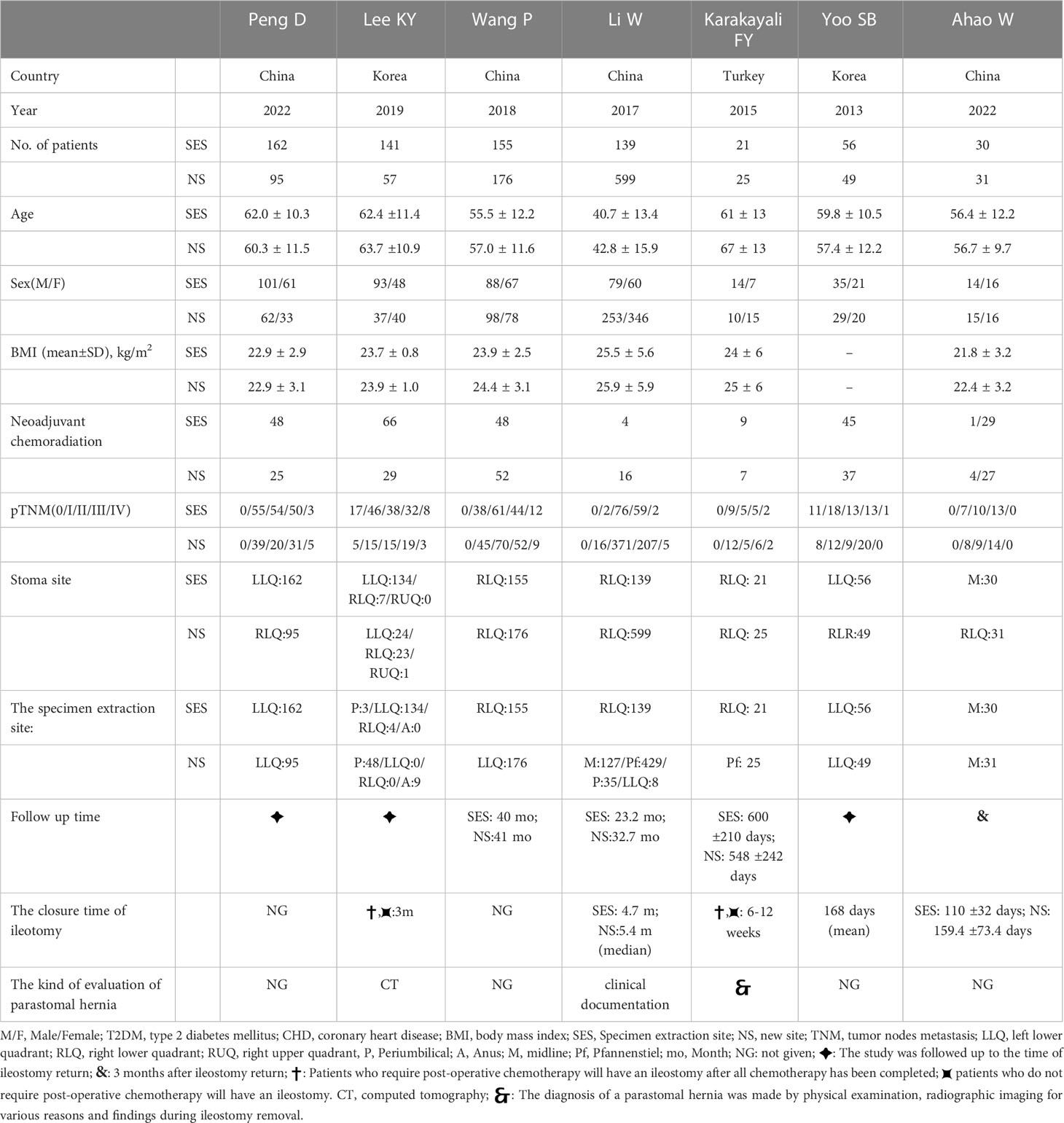
Table 1 Characteristics of the included studies.
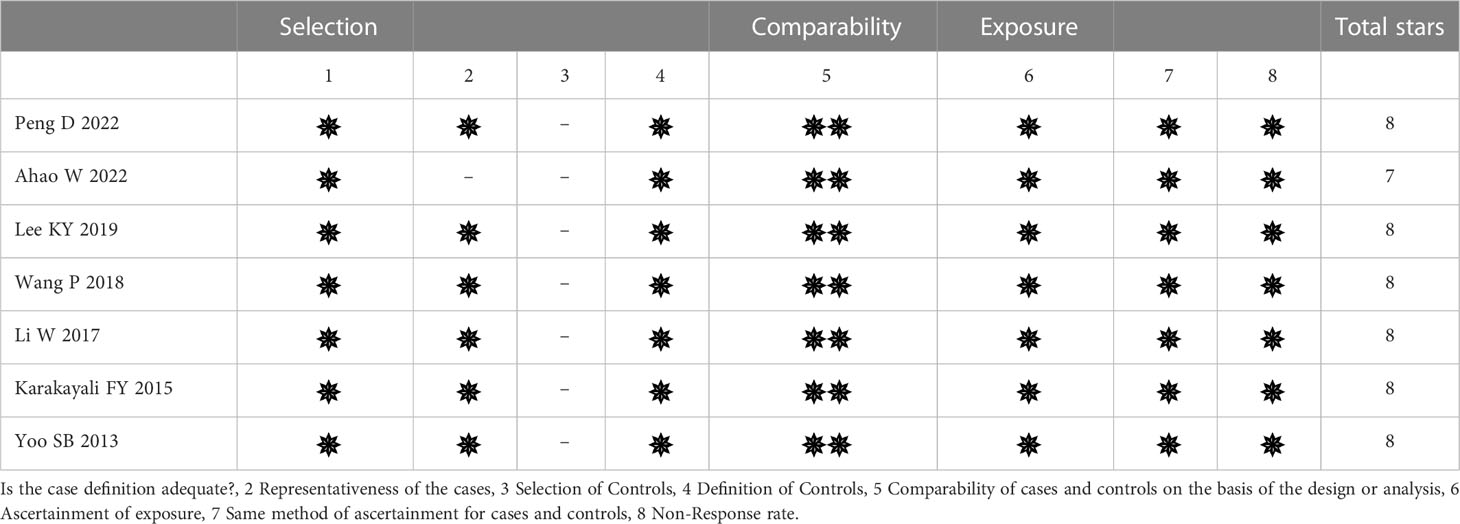
Table 2 Methodological quality of the included studies.
All seven studies reported parastomal hernia rates; 6.4% (45/704) in the SES group compared to 3.3% (34/1032) in the NS group. The pooled risk of parastomal hernia was higher in those with prophylactic ileostomy via the SES compared with NS (OR, 2.39, 95% CI 1.43-4.00; p=0.0008). No heterogeneity was found (I2 = 0%) (Figure 2).
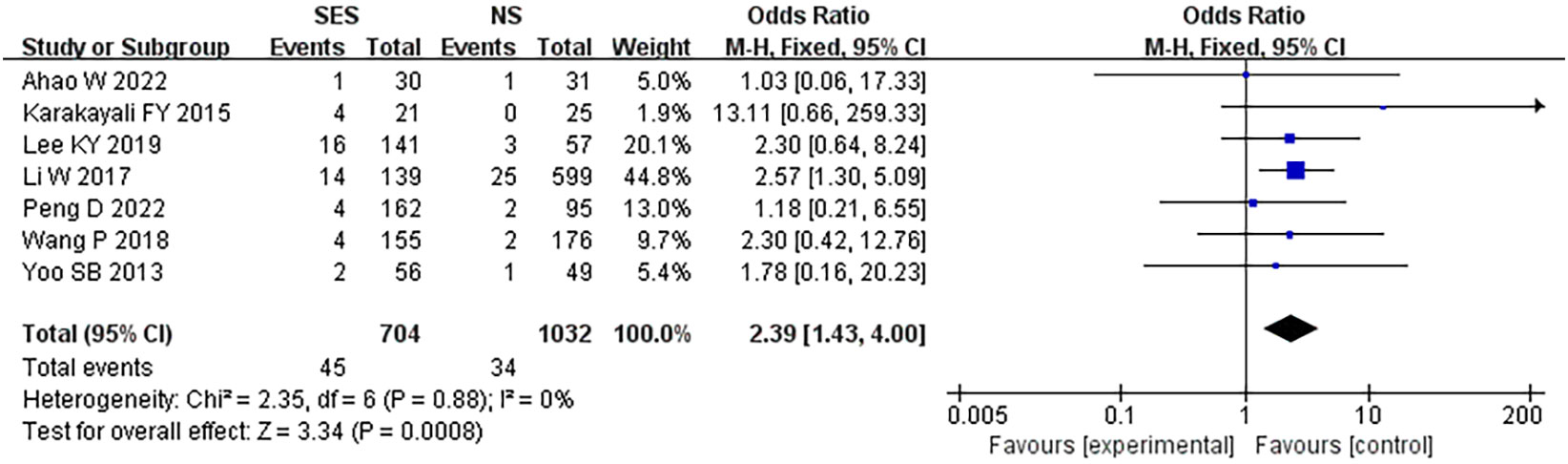
Figure 2 Parastomal hernia. NS: new site.
Table 3 presents the results of the pooled analysis of overall stoma-related complications. The SES group was significantly higher than the NS group in terms of total stoma-related complications (OR, 2.11, 95% CI 1.37-3.26; p=0.0007; I2 = 18%). There was no statistical difference between the SES and NS groups in terms of stoma edema (OR, 0.8, 95% CI 0.4-1.59; p=0.52; I2 = 43%), stoma prolapse(OR, 1.93, 95% CI 0.71-5.23; p=0.20; I2 = 0%), stoma necrosis(OR, 0.17, 95% CI 0.02-1.54; p=0.12; I2 = 0%), stoma infection(OR, 3.39, 95% CI 0.83-13.78; p=0.09; I2 = 0%), stoma bleeding(OR, 1.16, 95% CI 0.26-5.23; p=0.85; I2 = 21%), stoma stenosis(OR, 1.69, 95% CI 0.45-6.35; p=0.44; I2 = 45%), skin inflammation around the stoma(OR, 1.28, 95% CI 0.76-2.15; p=0.35; I2 = 0%) and stoma retraction(OR, 4.09, 95% CI 0.83-20.08; p=0.08; I2 = 0%).
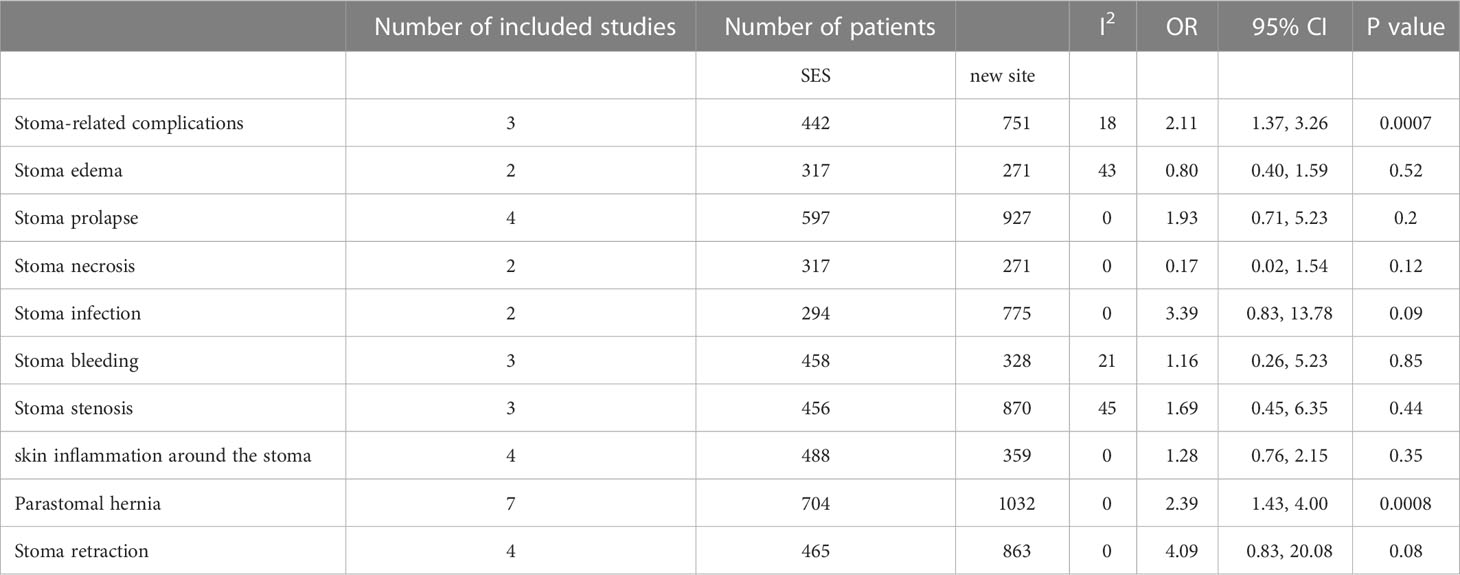
Table 3 The results of the pooled analysis of stoma-related complications.
Six studies (19–21, 25–27) reported operation time. The time of operation in the prophylactic ileostomy via the SES was shorter than that in the prophylactic ileostomy via NS after LRCS (MD = -0.43, 95% CI: -0.54 - -0.32 min; p<0.00001). No heterogeneity was found (I2 = 0%) (Figure 3).
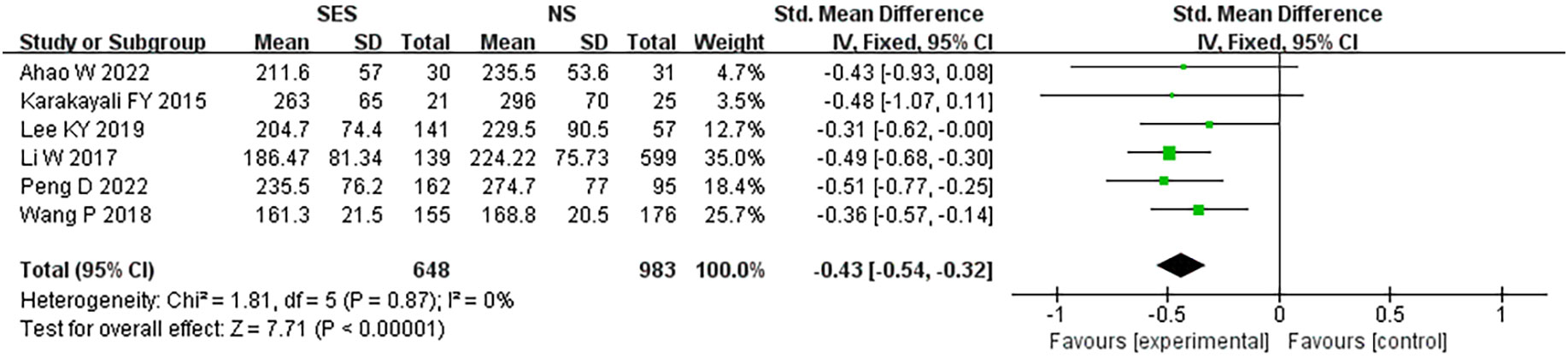
Figure 3 Operation time. NS: new site.
Five studies (19–21, 25, 27) reported blood loss. A pooled analysis performed using the fixed-effects model revealed a significantly reduced blood loss in the SES group compared with the NS group (MD = -0.38, 95% CI: -0.62 - -0.13; p=0.003). High heterogeneity was detected (I2 = 76%) (Figure 4).
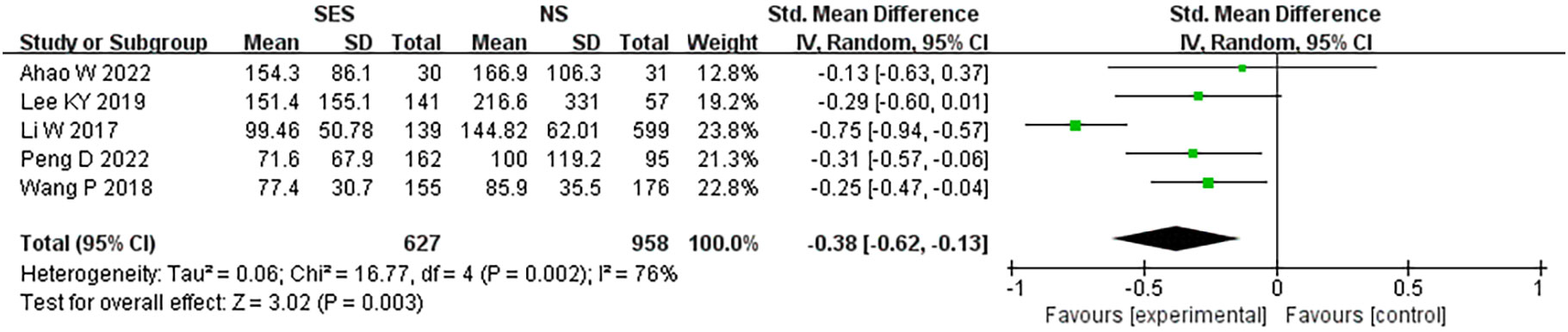
Figure 4 Blood loss. NS: new site.
All seven studies reported post-operative hospital stay. This pooled analysis using a random effects model showed that the SES group had a significantly lower postoperative hospital stay than the NS group (MD = -0.26, 95% CI: -0.43 - -0.08; p=0.004). High heterogeneity was detected (I2 = 57%) (Figure 5).
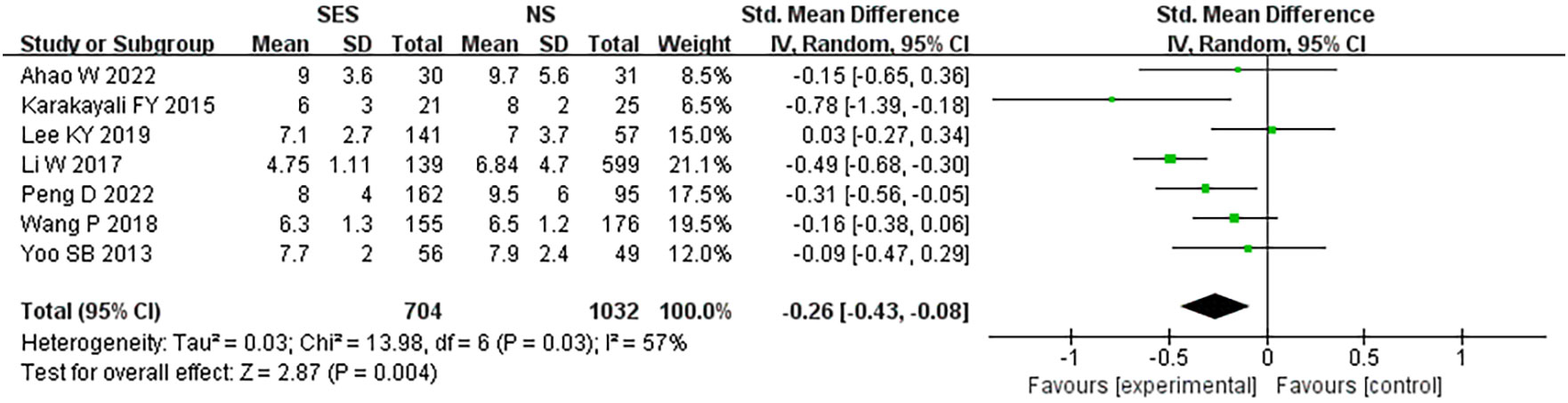
Figure 5 Postoperative hospital stay. NS: new site.
Three studies (19, 21, 27) reported time to first flatus. This pooled analysis using a fixed effects model showed that the SES group had a significantly shorter time to first flatus than the NS group (MD = -0.23, 95% CI: -0.39 - -0.08; p=0.003). No heterogeneity was found (I2 = 0%) (Figure 6).

Figure 6 Time to first flatus. NS: new site.
Five studies (18, 19, 21, 25, 26) reported ileus rate. This pooled analysis using a fixed effects model showed that there was no significantly difference between the SES group and the NS group. (OR, 0.82, 95% CI 0.53-1.27; p=0.37). No heterogeneity was found (I2 = 0%) (Figure 7).
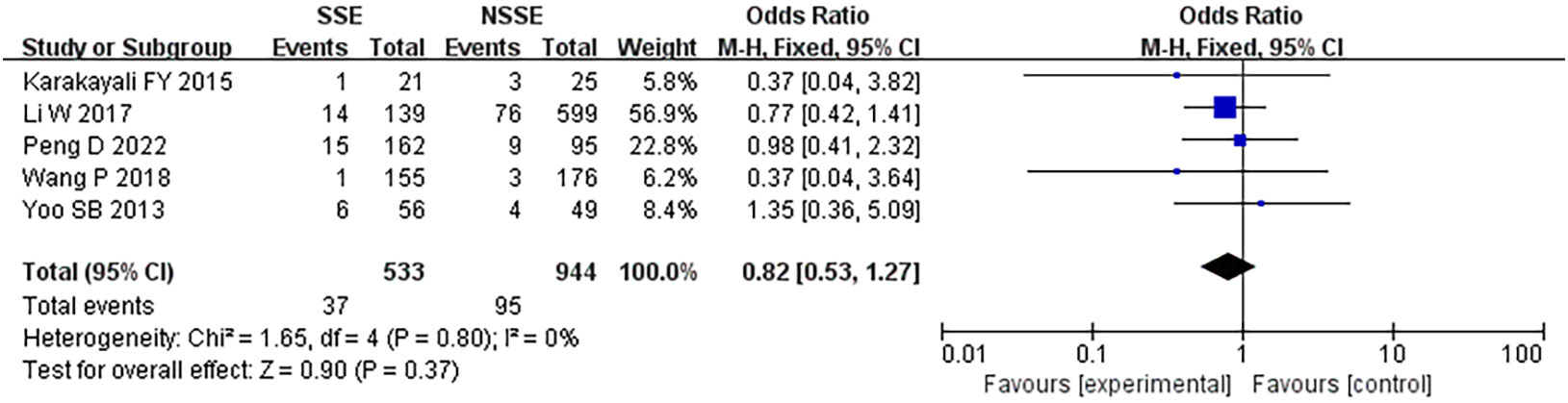
Figure 7 Ileus.
Three studies (21, 25, 26) reported wound infection; 1.4% (4/315) in the SES group compared to 3.5% in the NS group. A pooled analysis using the fixed-effects model revealed no significant difference in wound infection rates between the two groups (OR, 0.47, 95% CI 0.18–1.19; p=0.11). Moderate heterogeneity was found (I2 = 31%) (Figure 8).
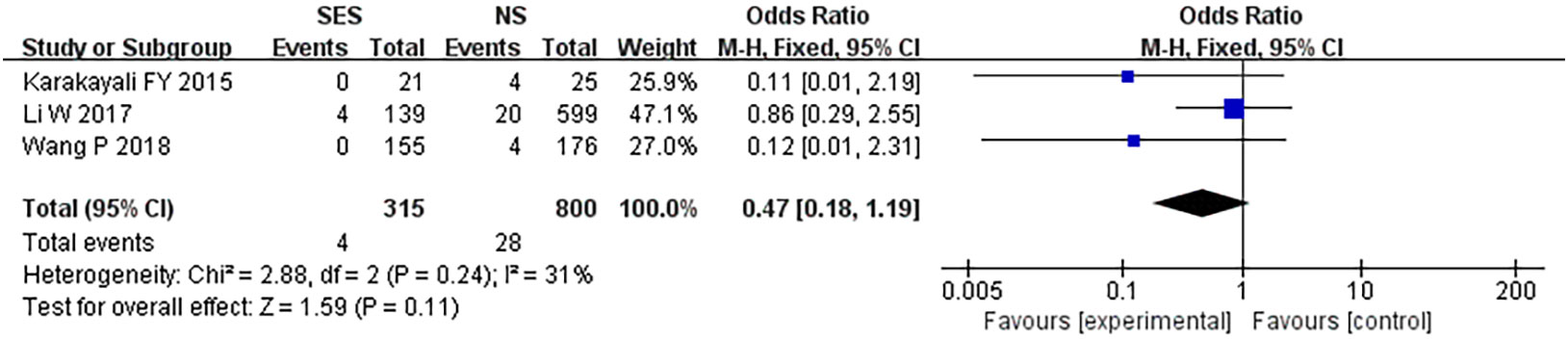
Figure 8 Wound infection. NS: new site.
Three studies (20, 21, 27) reported postoperative pain score. This pooled analysis using a random effects model showed that there was no statistical difference in postoperative pain score between the SES and NS group on postoperative day 1(MD = -0.20, 95% CI: -0.62 -0.23; p=0.36) and postoperative day 3(MD = 0.00, 95% CI: -0.17 – 0.17; p=1.00), while on postoperative day 2, postoperative pain score was significantly lower in the SES group than in the NS group(MD = -0.28, 95% CI: -0.46 – 0.10; p=0.002). High heterogeneity was detected on postoperative day 1 (I2 = 80%) (Figure 9).
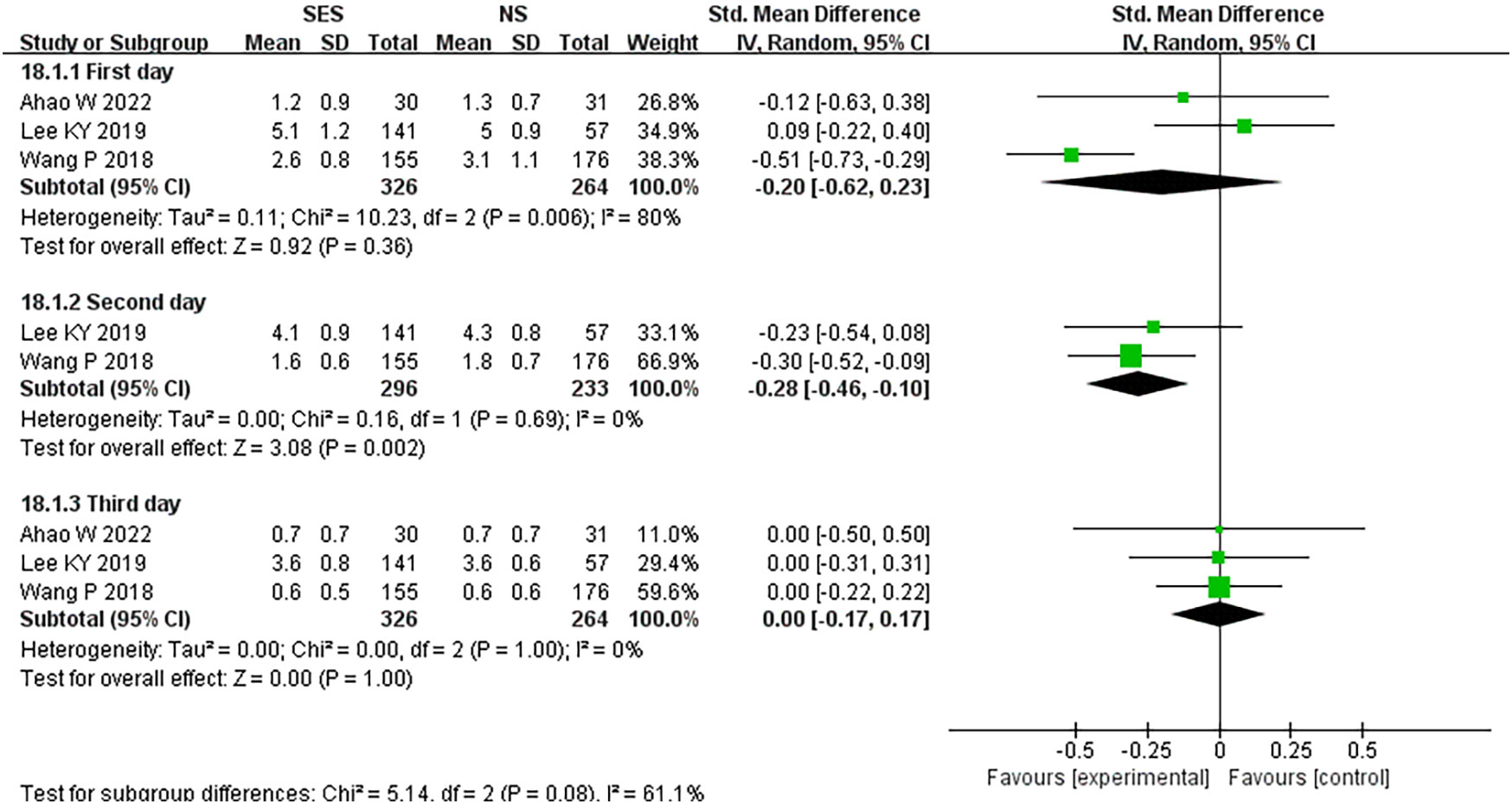
Figure 9 Postoperative pain. NS: new site.
To our knowledge, this was the first meta-analysis comparing prophylactic ileostomy through SES with NS after LRCS. The present meta-analysis noted that prophylactic ileostomy via SES was associated with a higher risk of overall stoma-related complications, especially parastomal hernia. We observed no statistical difference in terms of wound infection, ileus, stoma edema, stoma prolapse, stoma necrosis, stoma infection, stoma bleeding, stoma stenosis, skin inflammation around the stoma, stoma retraction and postoperative pain score on postoperative day 1 and 3 between SES group and NS group. However, prophylactic ileostomy via SES was associated with lesser blood loss, shorter operation time, shorter post-operative hospital stay, shorter time to first flatus and lower postoperative pain score on postoperative day 2.
Anastomotic leak (AL) is the most dreaded postoperative complication of colorectal cancer, with an incidence ranging from 1% to 21%, and it has a serious negative impact on the patient’s postoperative recovery, quality of life and survival (28–31). There are many risk factors for AL, such as longer operation time, use of more than 3 staples, ultra-low anastomosis, male, neoadjuvant radiotherapy (32–35). Prophylactic ileostomy has been proven and accepted by colorectal surgeons to prevent postoperative AL in rectal cancer and to reduce the adverse consequences of anastomosis (36–38). Conventional laparoscopic rectal cancer surgery is followed by prophylactic ileostomy through a new incision other than the one from which the specimen was taken. Theoretically, if prophylactic ileostomy is performed through the specimen retrieval incision, it will reduce the number of abdominal wall incisions and thus be more in line with the minimally invasive concept.
There is still no consensus on the definition of a parastomal hernia, which has caused the incidence of parastomal hernia to fluctuate from 1% to 50% as reported in the literature (39). One study reported that parastomal hernias were detected by clinical examination, imaging or during ileostomy reversal (26), while recent literature has reported that parastomal hernias were diagnosed by CT scan (20). The present meta-analysis reported a 6.4% incidence of parastomal hernia in the SES group compared to a 3.3% incidence of parastomal hernia in the NS group. Although the incidence of parastomal hernias was significantly higher in the SES group than in the NS group, all parastomal hernias could be resolved by ileostomy reversal surgery, and parastomal hernias had a minor impact on clinical prognosis (25).
The present study reported a significantly shorter operative time in the SES group compared with the NS group; This may be due to the fact that a temporary ileostomy through the specimen retrieval site reduces the number of surgical steps required to close the new incision; and results in a shorter operative time.
Our study also has limitations: first, all the studies included in the current meta-analysis were retrospective studies, which may have some influence on the results to some extent. Second, only short-term outcomes were included in this study, and long-term indicators such as survival were not analyzed; this is because the original studies reported very few long-term survival data. Third, due to the inconsistency in the definition of parastomal hernia, this may have had some impact on the results. Fourth, there was some variation in the location of the stoma and the method of stoma between studies, thus potentially affecting outcomes. However, the greatest strength of this meta-analysis is that it is the first study to examine the effectiveness and safety of prophylactic ileostomy after laparoscopic rectal cancer through SES.
Prophylactic ileostomy via SES after LRCS reduces new incision, decreases operative time, promotes postoperative recovery, and improves cosmetic outcomes, but may increase the incidence of parastomal hernias. The vast majority of parastomal hernias can be repaired by closing the ileostomy, therefore SES remain an option for temporary ileostomy after LRCS.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
BZ and XL contributed to the conception and design of the work. BZ, QW and MW conducted the literature search and extracted the data. YY was involved in the resolution of all the arguments. BZ and QW conducted the data analysis and wrote the manuscript. BZ and XL performed critical revision for this manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA: Cancer J Clin (2022) 72(1):7–33. doi: 10.3322/caac.21708
2. van der Pas MH, Haglind E, Cuesta MA, Fürst A, Lacy AM, Hop WC, et al. Laparoscopic versus open surgery for rectal cancer (COLOR II): Short-term outcomes of a randomised, phase 3 trial. Lancet Oncol (2013) 14(3):210–8. doi: 10.1016/s1470-2045(13)70016-0
3. Kong M, Chen H, Shan K, Sheng H, Li L. Comparison of survival among adults with rectal cancer who have undergone laparoscopic vs open surgery: A meta-analysis. JAMA net. Open (2022) 5(5):e2210861. doi: 10.1001/jamanetworkopen.2022.10861
4. Wang S, Liu J, Wang S, Zhao H, Ge S, Wang W. Adverse effects of anastomotic leakage on local recurrence and survival after curative anterior resection for rectal cancer: A systematic review and meta-analysis. World J surgery. (2017) 41(1):277–84. doi: 10.1007/s00268-016-3761-1
5. Rutegård M, Hemmingsson O, Matthiessen P, Rutegård J. High tie in anterior resection for rectal cancer confers no increased risk of anastomotic leakage. Br J surgery. (2012) 99(1):127–32. doi: 10.1002/bjs.7712
6. Boström P, Haapamäki MM, Rutegård J, Matthiessen P, Rutegård M. Population-based cohort study of the impact on postoperative mortality of anastomotic leakage after anterior resection for rectal cancer. BJS Open (2019) 3(1):106–11. doi: 10.1002/bjs5.50106
7. Koyama M, Murata A, Sakamoto Y, Morohashi H, Hasebe T, Saito T, et al. Risk factors for anastomotic leakage after intersphincteric resection without a protective defunctioning stoma for lower rectal cancer. Ann Surg Oncol (2016) 23 Suppl 2:S249–56. doi: 10.1245/s10434-015-4461-z
8. Smith JD, Paty PB, Guillem JG, Temple LK, Weiser MR, Nash GM. Anastomotic leak is not associated with oncologic outcome in patients undergoing low anterior resection for rectal cancer. Ann surgery. (2012) 256(6):1034–8. doi: 10.1097/SLA.0b013e318257d2c1
9. Gu WL, Wu SW. Meta-analysis of defunctioning stoma in low anterior resection with total mesorectal excision for rectal cancer: evidence based on thirteen studies. World J Surg Oncol (2015) 13:9. doi: 10.1186/s12957-014-0417-1
10. Matthiessen P, Hallböök O, Rutegård J, Simert G, Sjödahl R. Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer: A randomized multicenter trial. Ann surgery. (2007) 246(2):207–14. doi: 10.1097/SLA.0b013e3180603024
11. Tan WS, Tang CL, Shi L, Eu KW. Meta-analysis of defunctioning stomas in low anterior resection for rectal cancer. Br J surgery. (2009) 96(5):462–72. doi: 10.1002/bjs.6594
12. Chang SC, Chen HC, Chen YC, Ke TW, Tsai YY, Wang HM, et al. Long-term oncologic outcomes of laparoscopic anterior resections for cancer with natural orifice versus conventional specimen extraction: A case-control study. Dis colon rectum. (2020) 63(8):1071–9. doi: 10.1097/dcr.0000000000001622
13. Liu G, Shi L, Wu Z. Is natural orifice specimen extraction surgery really safe in radical surgery for colorectal cancer? Front Endocrinol (2022) 13:837902. doi: 10.3389/fendo.2022.837902
14. Wang S, Tang J, Sun W, Yao H, Li Z. The natural orifice specimen extraction surgery compared with conventional laparoscopy for colorectal cancer: A meta-analysis of efficacy and long-term oncological outcomes. Int J Surg (London England). (2022) 97:106196. doi: 10.1016/j.ijsu.2021.106196
15. Zhu Z, Wang KJ, Orangio GR, Han JY, Lu B, Zhou ZQ, et al. Clinical efficacy and quality of life after transrectal natural orifice specimen extraction for the treatment of middle and upper rectal cancer. J gastrointestinal Oncol (2020) 11(2):260–8. doi: 10.21037/jgo.2020.03.05
16. Ihnát P, Tulinský L, Jonszta T, Koscielnik P, Ihnát Rudinská L, Penka I. Parastomal and incisional hernia following laparoscopic/open abdominoperineal resection: is there a real difference? Surg endoscopy (2019) 33(6):1789–94. doi: 10.1007/s00464-018-6453-0
17. Chida K, Watanabe J, Suwa Y, Suwa H, Momiyama M, Ishibe A, et al. Risk factors for incisional surgical site infection after elective laparoscopic colorectal surgery. Ann gastroenterol. surgery. (2019) 3(2):202–8. doi: 10.1002/ags3.12229
18. Yoo SB, Jeong SY, Lim SB, Park JW, Choi HS, Oh JH. Left-sided ileostomy at specimen extraction site in laparoscopic-assisted low anterior resection for rectal cancer. J laparoendoscop. advanced Surg techniques Part A. (2013) 23(1):22–5. doi: 10.1089/lap.2012.0105
19. Peng D, Yu DL, Liu XY, Tao W, Kang B, Zhang H, et al. Does temporary ileostomy via specimen extraction site affect the short outcomes and complications after laparoscopic low anterior resection in rectal cancer patients? a propensity score matching analysis. BMC surgery. (2022) 22(1):263. doi: 10.1186/s12893-022-01715-8
20. Lee KY, Park JW, Lee KY, Cho S, Kwon YH, Kim MJ, et al. Safety of temporary ileostomy via specimen extraction site in rectal cancer patients who underwent laparoscopic low anterior resection. Sci Rep (2019) 9(1):2316. doi: 10.1038/s41598-019-38790-6
21. Wang P, Liang JW, Zhou HT, Wang Z, Zhou ZX. Surgical specimen extraction via a prophylactic ileostomy procedure: A minimally invasive technique for laparoscopic rectal cancer surgery. World J gastroenterol. (2018) 24(1):104–11. doi: 10.3748/wjg.v24.i1.104
22. PRISMA. Transparent reporting of systematic reviews and meta-analyses. Available at: http://www.prisma-statement.org/.
23. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol (2010) 25(9):603–5. doi: 10.1007/s10654-010-9491-z
24. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res methodol. (2005) 5:13. doi: 10.1186/1471-2288-5-13
25. Li W, Benlice C, Stocchi L, Kessler H, Gorgun E, Costedio M. Does stoma site specimen extraction increase postoperative ileostomy complication rates? Surg endoscopy (2017) 31(9):3552–8. doi: 10.1007/s00464-016-5384-x
26. Karakayali FY, Tezcaner T, Moray G. Specimen extraction from the defunctioning ileostomy site or pfannenstiel incision during total laparoscopic low anterior resection for rectal cancer. J laparoendoscop. advanced Surg techniques Part A. (2015) 25(5):380–5. doi: 10.1089/lap.2014.0545
27. Ahao W XS, Yi C. Median specimen extraction incision vs the traditional right lower abdominal incision for prophylactic ileostomy in radical resection of rectal cancer: A comparative perspective. J Pract Med (2022) 38(8):985–9.
28. Gastinger I, Marusch F, Steinert R, Wolff S, Koeckerling F, Lippert H. Protective defunctioning stoma in low anterior resection for rectal carcinoma. Br J surgery. (2005) 92(9):1137–42. doi: 10.1002/bjs.5045
29. Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: Systematic review and meta-analysis. Ann surgery. (2011) 253(5):890–9. doi: 10.1097/SLA.0b013e3182128929
30. Rondelli F, Balzarotti R, Bugiantella W, Mariani L, Pugliese R, Mariani E. Temporary percutaneous ileostomy versus conventional loop ileostomy in mechanical extraperitoneal colorectal anastomosis: A retrospective study. Eur J Surg Oncol (2012) 38(11):1065–70. doi: 10.1016/j.ejso.2012.07.110
31. Rondelli F, Avenia S, De Rosa M, Rozzi A, Rozzi S, Chillitupa CIZ, et al. Efficacy of a transanal drainage tube versus diverting stoma in protecting colorectal anastomosis: A systematic review and meta-analysis. Surg Today (2022). doi: 10.1007/s00595-021-02423-1
32. Ashburn JH, Stocchi L, Kiran RP, Dietz DW, Remzi FH. Consequences of anastomotic leak after restorative proctectomy for cancer: effect on long-term function and quality of life. Dis colon rectum. (2013) 56(3):275–80. doi: 10.1097/DCR.0b013e318277e8a5
33. Lim SB, Yu CS, Kim CW, Yoon YS, Park IJ, Kim JC. Late anastomotic leakage after low anterior resection in rectal cancer patients: clinical characteristics and predisposing factors. Colorectal Dis (2016) 18(4):O135–40. doi: 10.1111/codi.13300
34. Ji WB, Kwak JM, Kim J, Um JW, Kim SH. Risk factors causing structural sequelae after anastomotic leakage in mid to low rectal cancer. World J gastroenterol. (2015) 21(19):5910–7. doi: 10.3748/wjg.v21.i19.5910
35. Boyce SA, Harris C, Stevenson A, Lumley J, Clark D. Management of low colorectal anastomotic leakage in the laparoscopic era: More than a decade of experience. Dis colon rectum. (2017) 60(8):807–14. doi: 10.1097/dcr.0000000000000822
36. hiomi A, Ito M, Saito N, Hirai T, Ohue M, Kubo Y, et al. The indications for a diverting stoma in low anterior resection for rectal cancer: A prospective multicentre study of 222 patients from Japanese cancer centers. Colorectal Dis (2011) 13(12):1384–9. doi: 10.1111/j.1463-1318.2010.02481.x
37. Güenaga KF, Lustosa SA, Saad SS, Saconato H, Matos D. Ileostomy or colostomy for temporary decompression of colorectal anastomosis. Systemat. Rev meta-anal. Acta cirurgica brasileira. (2008) 23(3):294–303. doi: 10.1590/s0102-86502008000300014
38. Miyo M, Takemasa I, Hata T, Mizushima T, Doki Y, Mori M. Safety and feasibility of umbilical diverting loop ileostomy for patients with rectal tumor. World J surgery. (2017) 41(12):3205–11. doi: 10.1007/s00268-017-4128-y
Keywords: prophylactic ileostomy, the specimen extraction site, new site, laparoscopic rectal cancer surgery, parastomal hernias
Citation: Zheng B, Wang Q, Wei M, Yue Y and Li X (2023) Which site is better for prophylactic ileostomy after laparoscopic rectal cancer surgery? By the specimen extraction site or new site: A systematic review and meta-analysis. Front. Oncol. 13:1116502. doi: 10.3389/fonc.2023.1116502
Received: 05 December 2022; Accepted: 16 January 2023;
Published: 15 February 2023.
Edited by:
Nobu Oshima, Kyoto University, JapanReviewed by:
Mikhail Danilov, A. S. Loginov Moscow Clinical Scientific Centre, RussiaCopyright © 2023 Zheng, Wang, Wei, Yue and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaojun Li, bGl4aWFvanVuMjAwNDA5MTJAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.