 Ke Chai1,2
Ke Chai1,2 Rong Xiao
Rong Xiao
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol., 27 January 2023
Sec. Skin Cancer
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1086963
Lip verrucous carcinoma is a rare low-grade neoplasm, with an unsightly appearance and locally aggressive nature. Treatment of verrucous carcinoma is as yet challenging, no well-defined guidelines for effective and safe management of this disease are available. A case of a patient with a huge verrucous carcinoma of the lower lip successfully treated by surgical excision and double Abbe flap reconstruction technique is presented, and striking features of lip locations of this tumor as well as their management are discussed.
Verrucous carcinoma (VC) is a rare, well-differentiated variant of squamous cell carcinoma that can be separated into four subtypes according to the region of occurrence: oral type, plantar type, anogenital type, and other mucocutaneous sites (1, 2). Oral verrucous carcinoma (OVC) represents approximately 2–12% of all oral carcinomas (1, 3). As an uncommon disease, lip verrucous carcinoma typically presents as a verrucous, thick plaque on the lips resembling a cauliflower. The tumor grows slowly, it may cause tissue destruction but does not metastasize. The etiologies are not precisely known, which probably include smoking, betel nut chewing, and chronic inflammation (4, 5). The available results do not support a causal role of human papillomavirus (HPV) infection in the development of verrucous carcinoma (6–8). Treatment needs to be chosen with caution as the lesions are located on the face. We report a patient with a huge verrucous carcinoma of the lower lip, successfully treated by surgical excision and double Abbe flap reconstruction technique after failed non-surgical treatments.
A 67-year-old man presented with an enlarging verrucous tumor at his lower lip for 5 years. The patient smoked 10 cigarettes per day for 50 years and he was a heavy betel nut chewer. He noticed recurrent ulcers on his lower lip five years ago and applied topical application of spoiled egg white (a folk prescription) to the lesions on his own. After that, a hyperplastic warty mass gradually developed on the lower lip. The lesion was not accompanied by itching, pain or bleeding. Over the past 5 years, the lip lesion had been excised by cryosurgery or laser ablation on ten occasions. However, the disease recurred repeatedly. The patient recently visited our department with an exophytic verrucous yellowish-to-whitish tumor occupying almost all the lower lip of approximately 5cm × 3cm2 (Figure 1A). No analogous lesions were identified elsewhere in the body, and a clinical diagnosis of verrucous carcinoma was verified by the deep biopsy (Figure 2). Polymerase chain reaction (PCR) failed to support a relationship with HPV infection. Serology: hepatitis B was positive but inactive; syphilis, HIV, and hepatitis A were negative. Physical examination and further imaging did not give rise to the dissemination of the peripheral lymph nodes. Subsequently, the patient was referred to the department of maxillofacial surgery for further treatment. A wide local excision followed by the double Abbe flap reconstruction technique was performed by maxillofacial surgeons. Two symmetrical flaps with full-layer incisions were made on the external sides of the philtrum column apart for rotation and inset, with the vascular connection reserved at the distal end (Figure 3). The tumor was completely excised, and the histopathological result showed negative margins. After two weeks of evaluation, the double Abbe flap survived, and then the patient underwent the secondary procedure to separate the vascular pedicles. No relapse was observed more than 30 months after surgery, with a superior cosmetic result and nearly no limitation of mouth opening (Figures 1B, C).
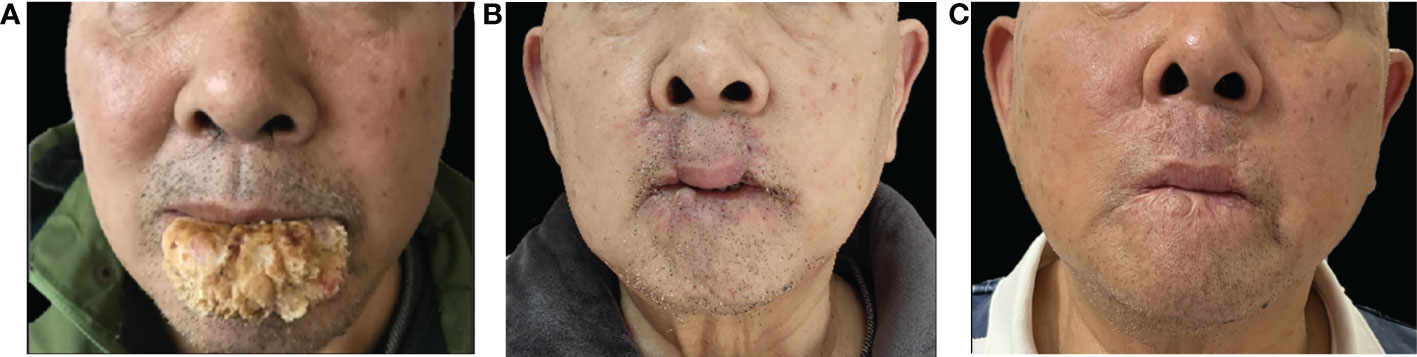
Figure 1 Clinical pictures: (A) Pre-operation image, an exophytic verrucous yellowish-to-whitish tumor occupying almost all the lower lip of approximately 5cm × 3cm2, resembling a cauliflower. (B) 30 days after surgical excision and double Abbe flap reconstruction, all skin lesions disappeared. (C) 30 months after surgery with a cosmetic appearance.
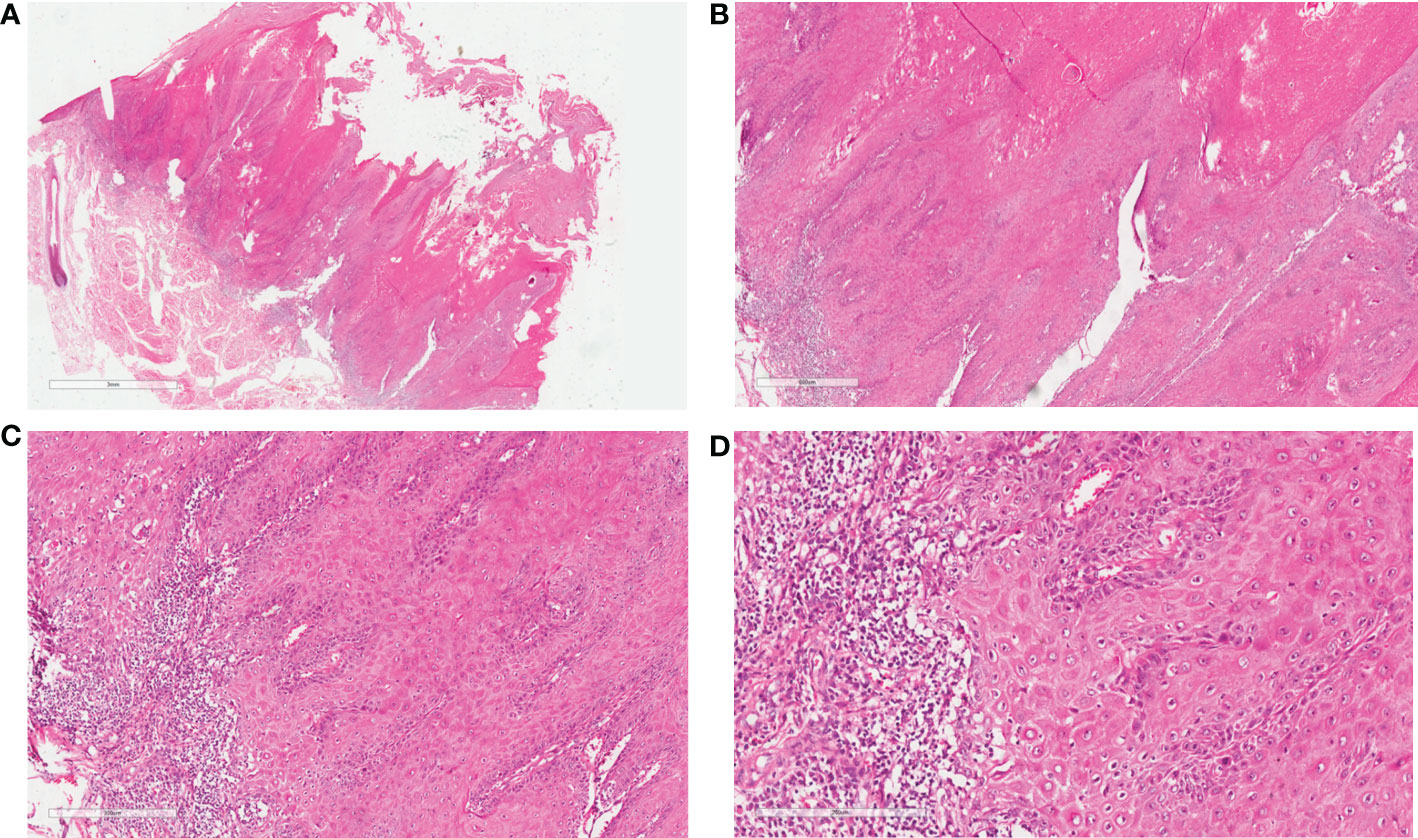
Figure 2 Pathological pictures: (A, B) Epithelial proliferation with verrucous appearance and significant keratosis, enlarged and fused endophytic epithelial ends with inflammatory infiltrate at the epithelial-stromal interface (H&E, ×10, ×40). (C) Endophytic papillae ending at different levels which forms pushing margins (H&E, ×100). (D) At high magnification, the basal cells are actively proliferating, and the spinous cells are enlarged in size with keratosis and red staining cytoplasm (H&E, ×100).
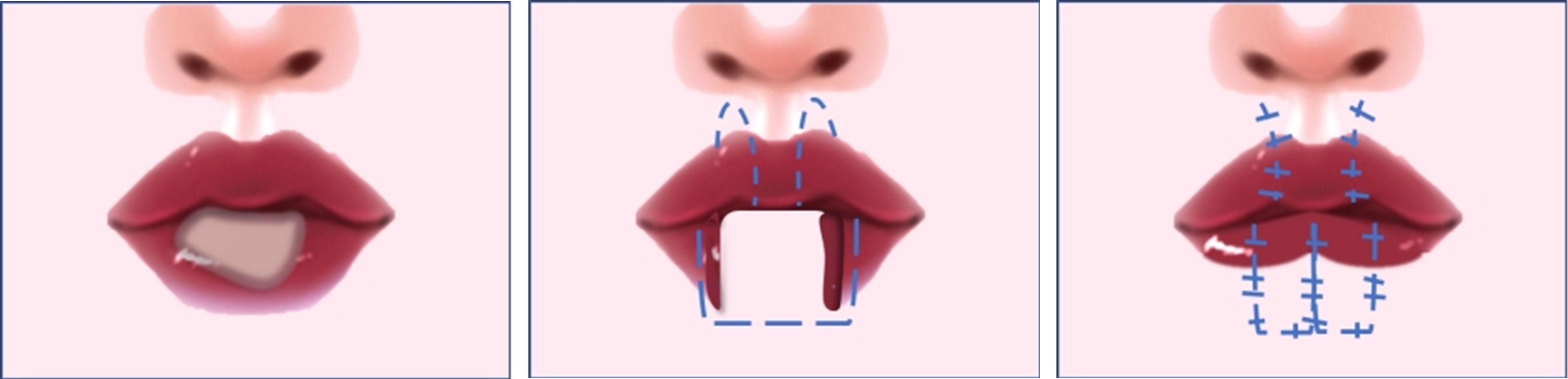
Figure 3 Reconstruction procedures: Rotating and insetting the double Abbe flap in the defect and suturing the distal edges of the two flaps to complete the repair of the defect.
Bad oral habits, including cigarette smoking and betel nut chewing, persistent lip ulcers, and the irritation of deteriorated foods may have contributed to the development of verrucous carcinoma of the lip in our case (1, 9). This disease is typically characterized by locally destructive behavior, with an unlikely tendency to metastasize, and appears as exophytic cauliflower-like, thick plaques on the lips (2). The most typical pathological features of VC are broad-based, well differentiated exophytic and endophytic epithelial proliferations with marked surface keratinization, without cellular atypia, invading the stroma with pushing borders (1). VC is comparable to many diseases in clinical and pathological conditions and deserves cautious differentiation, such as verrucous hyperplasia, squamous papilloma, and conventional squamous cell carcinoma (1, 10). Among them, squamous cell carcinoma, with varying degrees of cell atypia, has a potential proclivity to metastasize and carries a relatively dismal prognosis (10, 11). Although the prognosis of lip verrucous carcinoma is much better than other types of life-threatening malignancies, as a facially disfiguring disease, the particular location and the freakish appearance of lesions seriously affect patients’ mental health and quality of life. The choice of treatment modality is therefore crucial and clinicians strive to completely remove the tumor with normal tissue margins and to maximize preservation or restoration of lip function and appearance.
There are some treatment modalities reported to be applied, including surgery, cryosurgery, laser ablation, photodynamic therapy (PDT), radiation, chemotherapy, and immune response modifiers. Surgical excision is perceived as the primary treatment mode for verrucous carcinoma not exceeding 30% of the upper or lower lip. The radical treatment can simultaneously reduce the recurrence rate and avoid excessive lip defects (1, 12). Flap transplantation techniques are useful for repairing defects exceeding 30% of the lip length. However, inappropriate flaps may cause permanent deformity and limited function of the graft site (13, 14). Cryosurgery is commonly applied to minor or superficial lesions with a certain recurrence rate and associated side effects. Complaints about repetitive cryosurgery accompanied by pain or edema at the healing region are general (15). The laser ablation affords accurate resection, limited blood loss, as well as minimal contraction and scarring (16). But laser therapy also needs to be repeatedly operated, and a more extensive case series need to be explored (17, 18). Since the procedure of PDT is excruciating for regions with abundant nerve endings, there may be poor patient compliance in the application of lip disorders (19). Radiotherapy is debatable because of the potential for anaplastic transformation after irradiation (20, 21). Intra-arterial infusion chemotherapy facilitates the delivery of a high concentration of cancer medicine to the target region, inducing rapid tumor shrinkage and realizing local palliation within a relatively short duration (22). However, long-term chemotherapy may attract tumor resistance. In the meantime, it has been shown that immune response modifiers may be effective, such as imiquimod, which exhibits antiviral and antitumor effects in vivo (2). Even though multiple treatment modalities have been used for the treatment of verrucous carcinoma, surgical excision with adequate margins with or without reconstruction still remains the standard and widely adopted treatment.
Actually, no well-defined standards for safe and effective management of lip verrucous carcinoma are currently available. We present the related reports about lip verrucous carcinoma (Table 1) and summarize the advantages and disadvantages of various treatment modalities (Table 2). Our patient had undergone ten previous unsatisfactory non-surgical regimens, including cryosurgery and laser ablation, which could be partly attributed to incomplete lesion eradication. After a comprehensive evaluation by the dermatologist and maxillofacial surgeons, considering that the recurrence predicts a poor prognosis, the decision was made to conduct a surgical intervention. Restoring wide defects caused by lip carcinoma resection (commissure was not involved) was a challenge for surgeons. However, the use of conventional flaps, which are used for defects of two-thirds or even more of the lip length may result in the formation of deformity. For example, a smile deformity or a “fish-mouth” may accompany with the use of Bernard and Paramaniac flaps, especially in edentulous patients (39). Maxillofacial surgeons designed two Abbe flaps symmetrically on the upper lip to restitute the lower lip defect, named as the double Abbe flap. The double Abbe flap can better maintain the lip shape with the bilateral symmetrical design and a small auxiliary incision. Combined with two flaps, the novel reconstruction technique is suitable for large-area lip defects, which avoids some major trauma or postoperative complications caused by other single larger adjuvant incisions (14, 39). Overall, this reconstruction technique has less influence on the lip shape and provides adequate mouth opening without dysfunction in our case.

Table 1 Summary of the 22 patients with verrucous carcinoma of the lip.
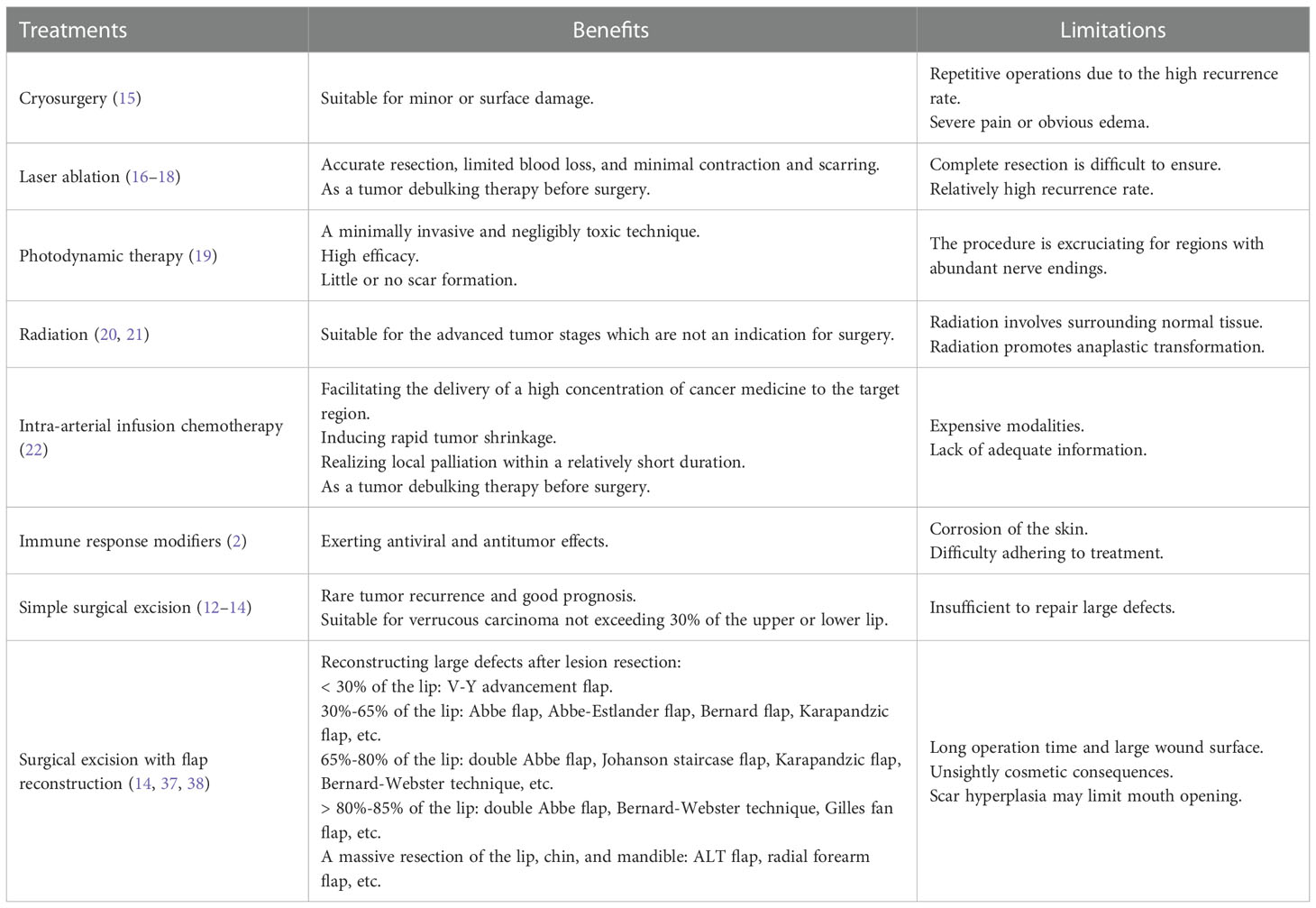
Table 2 Summary of benefits and limitations of treatments used in Lip Verrucous Carcinoma.
It seems that the curative effect of this therapy is excellent at present, as the patient remains asymptomatic 30 months after surgery. There is currently no report regarding the use of double Abbe flap reconstruction techniques for lip verrucous carcinoma defects as we know. The authors report a case of a rare tumor with a relatively large size and bizarre appearance. The interest of this case is to gather previous reports to present the striking features of lip verrucous carcinoma: epidemiology, cosmetic features, peripheral dissemination, pathophysiological determinants such as human papillomavirus infection, treatment modalities, and follow-up results. Furthermore, the reporters summarized various treatment modalities and their advantages and disadvantages to supply additional clues during clinical assessment and optimize the clinical benefits for patients. In addition, it is worth emphasizing that the double Abbe flap may be a useful and promising approach in the reconstruction of the lower lip following large-area verrucous carcinoma resection, as it helps to completely remove the tumor while maximizing the preservation or restoration of lip function and cosmesis.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
KC drafted the manuscript, drew the figures, and summarized the table. JL, RX, and GZ discussed and revised the manuscript. YZ designed the study, reviewed and edited the paper. All authors contributed to the article and approved the submitted version.
This work was supported by the National Natural Science Foundation of China (No.82003363, No.81773333, No.82073449, No.82001738), the Hunan Provincial Natural Science Foundation of China (2021JJ40820), and the Changsha Municipal Natural Science Foundation(kq2007059).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Peng Q, Wang Y, Quan H, Li Y, Tang Z. Oral verrucous carcinoma: From multifactorial etiology to diverse treatment regimens (Review). Int J Oncol (2016) 49(1):59–73. doi: 10.3892/ijo.2016.3501
2. Kwon HB, Choi YS, Lee JH, Jin SY, Kim BJ, Lee SH, et al. Treatment of verrucous carcinoma of the lower lip with topical imiquimod (Aldara®) and debulking therapy. Ann Dermatol (2011) 23 Suppl 1:S68–71. doi: 10.5021/ad.2011.23.S1.S68
3. Ulrich M, von Braunmuehl T, Kurzen H, Dirschka T, Kellner C, Sattler E, et al. The sensitivity and specificity of optical coherence tomography for the assisted diagnosis of nonpigmented basal cell carcinoma: An observational study. Br J Dermatol (2015) 173(2):428–35. doi: 10.1111/bjd.13853
4. Alkan A, Bulut E, Gunhan O, Ozden B. Oral verrucous carcinoma: A study of 12 cases. Eur J Dent (2010) 4(2):202–7. doi: 10.1055/s-0039-1697831
5. Mitsuishi T, Ohara K, Kawashima M, Kobayashi S, Kawana S. Prevalence of human papillomavirus DNA sequences in verrucous carcinoma of the lip: Genomic and therapeutic approaches. Cancer Lett (2005) 222(2):139–43. doi: 10.1016/j.canlet.2004.09.019
6. del Pino M, Bleeker MCG, Quint WG, Snijders PJF, Meijer CJLM, Steenbergen RDM. Comprehensive analysis of human papillomavirus prevalence and the potential role of low-risk types in verrucous carcinoma. Mod Pathol (2012) 25(10):1354–63. doi: 10.1038/modpathol.2012.91
7. Patel KR, Chernock RD, Zhang TR, Wang X, El-Mofty SK, Lewis JS. Verrucous carcinomas of the head and neck, including those with associated squamous cell carcinoma, lack transcriptionally active high-risk human papillomavirus. Hum Pathol (2013) 44(11):2385–92. doi: 10.1016/j.humpath.2013.07.011
8. Odar K, Kocjan BJ, Hošnjak L, Gale N, Poljak M, Zidar N. Verrucous carcinoma of the head and neck - not a human papillomavirus-related tumour? J Cell Mol Med (2014) 18(4):635–45. doi: 10.1111/jcmm.12211
9. Schütze M, Boeing H, Pischon T, Rehm J, Kehoe T, Gmel G, et al. Alcohol attributable burden of incidence of cancer in eight European countries based on results from prospective cohort study. BMJ (2011) 342:d1584. doi: 10.1136/bmj.d1584
10. Ye Q, Hu L, Jia M, Deng L-J, Fang S. Cutaneous verrucous carcinoma: A clinicopathological study of 21 cases with long-term clinical follow-up. Front Oncol (2022) 12:953932. doi: 10.3389/fonc.2022.953932
11. Chauhan K, Jassal V, Sara GK, Bansal V, Hatwal V. Histopathological study of verrucous lesions and its mimics. J Microsc Ultrastruct (2021) 9(2):86–97. doi: 10.4103/JMAU.JMAU_47_19
12. Koch BB, Trask DK, Hoffman HT, Karnell LH, Robinson RA, Zhen W, et al. National survey of head and neck verrucous carcinoma: Patterns of presentation, care, and outcome. Cancer (2001) 92(1):110–20. doi: 10.1002/1097-0142(20010701)92:1<110::aid-cncr1298>3.0.co;2-k
13. Marks R, Gebauer K, Shumack S, Amies M, Bryden J, Fox TL, et al. Imiquimod 5% cream in the treatment of superficial basal cell carcinoma: Results of a multicenter 6-week dose-response trial. J Am Acad Dermatol (2001) 44(5):807–13. doi: 10.1067/mjd.2001.113689
14. Langstein HN, Robb GL. Lip and perioral reconstruction. Clin Plast Surg (2005) 32(3):431–45. doi: 10.1016/j.cps.2005.02.007
15. Yu C-H, Lin H-P, Cheng S-J, Sun A, Chen H-M. Cryotherapy for oral precancers and cancers. J Formos Med Assoc (2014) 113(5):272–7. doi: 10.1016/j.jfma.2014.01.014
16. Hsu CK, Lee JYY, Yu CH, Hsu MML, Wong TW. Lip verrucous carcinoma in a pregnant woman successfully treated with carbon dioxide laser surgery. Br J Dermatol (2007) 157(4):813–5. doi: 10.1111/j.1365-2133.2007.08078.x
17. Lee C-N, Huang C-C, Lin IC, Lee JY-Y, Ou C-Y, Wong T-W. Recalcitrant lip verrucous carcinoma successfully treated with acitretin after carbon dioxide laser ablation. JAAD Case Rep (2018) 4(6):576–8. doi: 10.1016/j.jdcr.2018.02.002
18. Antonio AM, Barreiros H, Goulão J, Barbosa N, Bártolo E. Verrucous carcinoma of the upper lip: An exuberant presentation in a patient with other synchronous lesions. Indian J Dermatol Venereol Leprol (2020) 86(2):230. doi: 10.4103/ijdvl.IJDVL_529_17
19. Wong TW, Sheu HM, Lee JY, Fletcher RJ. Photodynamic therapy for bowen's disease (Squamous cell carcinoma in situ) of the digit. Dermatol Surg (2001) 27(5):452–6. doi: 10.1046/j.1524-4725.2001.00187.x
20. Tharp ME, Shidnia H. Radiotherapy in the treatment of verrucous carcinoma of the head and neck. Laryngoscope (1995) 105(4 Pt 1):391–6. doi: 10.1288/00005537-199504000-00011
21. Perez CA, Kraus FT, Evans JC, Powers WE. Anaplastic transformation in verrucous carcinoma of the oral cavity after radiation therapy. Radiology (1966) 86(1):108–15. doi: 10.1148/86.1.108
22. Sheen MC, Sheu HM, Lai FJ, Lin SD, Wu CF, Wang YW, et al. A huge verrucous carcinoma of the lower lip treated with intra-arterial infusion of methotrexate. Br J Dermatol (2004) 151(3):727–9. doi: 10.1111/j.1365-2133.2004.06139.x
23. Chen H-M, Chen C-T, Yang H, Lee M-I, Kuo MY-P, Kuo Y-S, et al. Successful treatment of an extensive verrucous carcinoma with topical 5-aminolevulinic acid-mediated photodynamic therapy. J Oral Pathol Med (2005) 34(4):253–6. doi: 10.1111/j.1600-0714.2004.00267.x
24. Tsuji T. Bleomycin iontophoretic therapy for verrucous carcinoma. Arch Dermatol (1991) 127(7):973–5. doi: 10.1001/archderm.1991.01680060047004
25. Florin EH, Kolbusz RV, Goldberg LH. Verrucous carcinoma of the lip originating on the vermilion border. Int J Dermatol (1994) 33(9):637. doi: 10.1111/j.1365-4362.1994.tb02923.x
26. De Socio GV, Bidovanets O, Tomassini GM, Fanelli L, Simonetti S. Human papilloma virus-associated lips verrucous carcinoma in hiv-infected Male. J Int Assoc Provid AIDS Care (2017) 16(4):324–6. doi: 10.1177/2325957417711255
27. Phulari RG, Rathore R, Talegaon TP, Shah A. Cutaneous horn: A mask to underlying malignancy. J Oral Maxillofac Pathol (2018) 22(Suppl 1):S87–90. doi: 10.4103/jomfp.JOMFP_156_17
28. Nagao Y, Sata M. Oral verrucous carcinoma arising from lichen planus and esophageal squamous cell carcinoma in a patient with hepatitis c virus-related liver cirrhosis-hyperinsulinemia and malignant transformation: A case report. BioMed Rep (2013) 1(1):53–6. doi: 10.3892/br.2012.14
29. Suda T, Yotsuyanagi T, Ezoe K, Saito T, Ikeda K, Yamauchi M, et al. Reconstruction of a red lip that has a defect in one half, using the remaining red lip. J Plast Reconstr Aesthet Surg (2009) 62(12):e570–e3. doi: 10.1016/j.bjps.2008.11.047
30. Koike T, Kanno T, Karino M, Sekine J. A patient with lower lip verrucous carcinoma treated with a tongue flap for functional and esthetic reconstruction. Gan To Kagaku Ryoho (2017) 44(12):1936–8.
31. Cannon CR, Hayne ST. Concurrent verrucous carcinomas of the lip and buccal mucosa. South Med J (1993) 86(6):691–3. doi: 10.1097/00007611-199306000-00022
32. Lu XG, Cai ZG, Zhang Y, Sun YG. One-stage operation for noma-induced bilateral ankylosis accompanied with mouth verrucous carcinoma - a case report and review of literature. Chin J Dent Res (2010) 13(1):67–9.
33. Hakeem AH, Hakeem IH, Wani FJ. Single-stage reconstruction of Large defect of oral commissure and lips by submental artery island flap. Natl J Maxillofac Surg (2018) 9(2):222–4. doi: 10.4103/njms.NJMS_61_16
34. Yadav PS, Ahmad QG, Shankhdhar VK, Lakshmi VS, Nambi GI. Verrucous carcinoma of the lip: An unusual kissing type. Dermatol Surg (2011) 37(7):1023–5. doi: 10.1111/j.1524-4725.2011.02066.x
35. Lai C-L, Ou K-W, Chiu W-K, Chen S-G, Chen T-M, Li H-P, et al. Reconstruction of the complete loss of upper and lower lips with a chimeric anterolateral thigh flap: A case report. Microsurgery (2012) 32(1):60–3. doi: 10.1002/micr.20943
36. El Ghelbazouri N, Afifi Y, Benameur H, Bella A, Elhallaoui Y, Kettani F, et al. Oral verrucous carcinoma and human papillomavirus infection. Ann Dermatol Venereol (2007) 134(8-9):659–62. doi: 10.1016/S0151-9638(07)91828-1
37. Ebrahimi A, Kalantar Motamedi MH, Ebrahimi A, Kazemi M, Shams A, Hashemzadeh H. Lip reconstruction after tumor ablation. World J Plast Surg (2016) 5(1):15–25.
38. Kornevs E, Skagers A, Tars J, Bigestans A, Lauskis G, Libermanis O. 5 year experience with lower lip cancer. Stomatologija (2005) 7(3):95–8.
Keywords: lip verrucous carcinoma, double Abbe flap reconstruction, differential diagnosis, decision optimization, case report
Citation: Chai K, Liu J, Xiao R, Zhang G and Zhan Y (2023) A huge verrucous carcinoma of the lower lip reconstructed by double Abbe flap: A case report and literature review. Front. Oncol. 13:1086963. doi: 10.3389/fonc.2023.1086963
Received: 01 November 2022; Accepted: 16 January 2023;
Published: 27 January 2023.
Edited by:
Nina Zidar, University of Ljubljana, SloveniaReviewed by:
Shilpi Sharma, Aarvy Healthcare Superspeciality Hospital, IndiaCopyright © 2023 Chai, Liu, Xiao, Zhang and Zhan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi Zhan, bWlzc2V2ZW42OUBjc3UuZWR1LmNu
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.