
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol. , 16 June 2023
Sec. Breast Cancer
Volume 13 - 2023 | https://doi.org/10.3389/fonc.2023.1046003
 Yan-Fang Sui1†Lang-Qian Tong2†Xia-Fei Lin1Hai-Xia Wu1Jing-Qin Shi1Shan-Shan Wang1Bu-He Tang3*
Yan-Fang Sui1†Lang-Qian Tong2†Xia-Fei Lin1Hai-Xia Wu1Jing-Qin Shi1Shan-Shan Wang1Bu-He Tang3* Zhen-Hua Song1*
Zhen-Hua Song1*Objective: To underscore the paramount significance of incorporating comprehensive rehabilitation therapy as a crucial aspect of managing lymphedema caused by breast cancer surgery, and to illuminate our first-hand experience and insights gained in utilizing this approach.
Methods: We present a case report of a breast cancer survivor who had been suffering from persistent left upper-limb edema for over 15 years, who was effectively treated with a combination of conventional rehabilitation (seven-step decongestion therapy) and a comprehensive rehabilitation program (seven-step decongestion therapy, along with core and respiratory function training, as well as functional brace wearing). The efficacy of the rehabilitation therapy was evaluated through a comprehensive assessment
Results: Although the patient underwent the conventional rehabilitation program for one month, only limited improvement was observed. However, after an additional month of comprehensive rehabilitation treatment, the patient exhibited significant improvement in both lymphedema and the overall function of the left upper limb. The patient’s progress was quantified by measuring the reduction in arm circumference, which demonstrated a notable decrease. Furthermore, improvements in joint range of motion were observed, with forward flexion of the shoulder enhancing by 10°, forward flexion improving by 15°, and elbow flexion increasing by 10°. In addition, manual muscular strength tests revealed an increase in strength from Grade 4 to Grade 5. The patient’s quality of life was also significantly improved, as evidenced by the increase in the Activities of Daily Living score from 95 to 100 points, the increase in the the Functional Assessment of Cancer Therapy: Breast score from 53 to 79 points, and the decrease in the Kessler Psychological Distress Scale score from 24 to 17 points.
Conclusion: While seven-step decongestion therapy has been shown to be effective in reducing upper-limb lymphedema caused by breast cancer surgery, it has limitations in treating more chronic cases of the condition. However, when combined with core and respiratory function training and functional brace wearing, seven-step decongestion therapy has been shown to be even more effective in reducing lymphedema and improving limb function, ultimately leading to significant improvements in quality of life.
Breast cancer is the most frequently diagnosed cancer in women worldwide and continues to be a major global health concern (1). Breast cancer incidence rates have been rapidly increasing in China, making it one of the countries with the fastest-growing rates of breast cancer globally (2–4). The primary components of breast cancer surgery typically involve lumpectomy and/or axillary lymph node dissection (2). Lymphedema can result from a variety of causes including surgery, chemotherapy, radiotherapy, trauma, infection, obesity, and other personal factors (4, 5).
Breast cancer-related lymphedema (BCRL) affects about 25% of women following breast cancer surgery (1, 6). This condition can have a significant impact on a patient’s quality of life and physical function (5–7).The typical treatments for breast cancer-related lymphedema (BCRL) involve lymphatic drainage, elastic bandaging, exercise therapy, and other rehabilitation therapies. However, there is limited research on comprehensive rehabilitation therapy for this condition (8–13).Therefore, a case is presented to underscore the significance of comprehensive rehabilitation and share the practical knowledge gained from it. The presented case involves a patient who experienced left upper-limb swelling for over 15 years following breast cancer surgery. Although conventional therapy yielded limited improvements, the patient’s lymphedema and function markedly improved after undergoing one month of comprehensive rehabilitation.
A 51-year-old female patient who had undergone modified radical resection of her left breast and had been experiencing left upper limb swelling and limited mobility for 15 years was admitted to the Affiliated Haikou Hospital of Xiangya Medical College. The patient underwent modified radical resection of the left breast on April 19, 2006, following preoperative chemotherapy, due to a mass found on the left breast. The specific details regarding the intraoperative lymph node dissection are unknown. However, intraoperative pathology confirmed the mass as Grade 3 invasive ductal cancer, and the patient received postoperative concurrent chemotherapy and radiation. The patient experienced redness, swelling, pain, and increased skin temperature in the left upper limb six months after the surgery. This was diagnosed as cellulitis of the left upper limb caused by Staphylococcus aureus infection. The patient received appropriate treatments that provided some relief from the pain, but these treatments were irregular. Nonetheless, the left upper limb remained swollen. As the patient was left-handed, the swelling of her left hand had a serious impact on the quality of life. Consequently, she sought rehabilitation treatment at our hospital.
During the post-admission examination, it was noted that the left upper limb and left hand were significantly swollen in comparison with the contralateral side. However, there was no elevation in the skin temperature and palpation revealed that the skin was rigid, tensed, and had reduced elasticity. The left upper extremity displayed hypoesthesia and was found to have positive pitting and Stemmer indications. (Figure 1) Ultrasound examination of the axilla indicated that neither the deep nor superficial veins of the left upper limb were thrombosed. Figure 2 illustrates the specific measurement method used. Initially, the patient underwent a conventional rehabilitation program with seven-step decongestion therapy (14) for a duration of one month, and Table 1 showed an improvement in patient’s left upper lymphedema. But the rehabilitation progress was sluggish and unsatisfactory. To enhance the progress of rehabilitation and identify any additional factors that might be hindering the recovery, a comprehensive rehabilitation therapy was adopted, including the conventional seven-step decongestion therapy, the posture and respiratory assessment combined with their corresponding training and bracing wearing (details can be seen in the Supplement). According to the assessment, the patient exhibited abnormal posture, weakened strength in the respiratory and core muscles, and was incapable of sustaining a functional position of the left upper limb for prolonged periods. The substantial edema in the patient’s left upper limb caused an imbalance in the strength between the left and right sides of the body, leading to an unnatural posture. Based on the reassessment findings, there was implementation of core and respiratory function training as well as utilization of a functional brace (i.e., upper arm-waist fixing brace) (Figure 3). A brace was designed and utilized to stabilize the lumbar spine, prevent lateral trunk flexion, and support upper arm abduction during upper-limb activities. The brace also reduced weight bearing of the edematous upper limb and allowed for extended functional activity time. A low-temp. thermoplastic sheet brace was selected due to its good shaping properties, and lightweight, breathability, high strength, and waterproof nature. Appropriate sheets were chosen and limb part sizes were measured. Low-temp. thermoplastic sheets of 3 different specifications and models were selected based on hardness and breathability needed for different fixations. Sheets were put in 65-70°C water and heated for 1-3 min. Softened materials were removed, dried, and shaped. Hook-and-loop fasteners and screws were used to fix, with padding for protection. Elastic sleeves should be worn on affected limb before wearing. To wear, first fix trunk part and Velcro, then upper arm part and Velcro, and adjust to prevent skin compression. Release Velcro every 2 hrs to relieve local pressure. Tables 2, 3 shows the changes before and after the comprehensive rehabilitation therapy. Figure 4 shows the edema of the patient’s left upper limb after treatment. The treatment flow chart outlined the whole intervention process (Figure 5).

Figure 1 Left Upper Limb Lymphedema. (A: Palmar Side of Forearm, B: Dorsal Side of Forearm).

Figure 2 Measurement Method for Left Upper Limb Lymphedema.
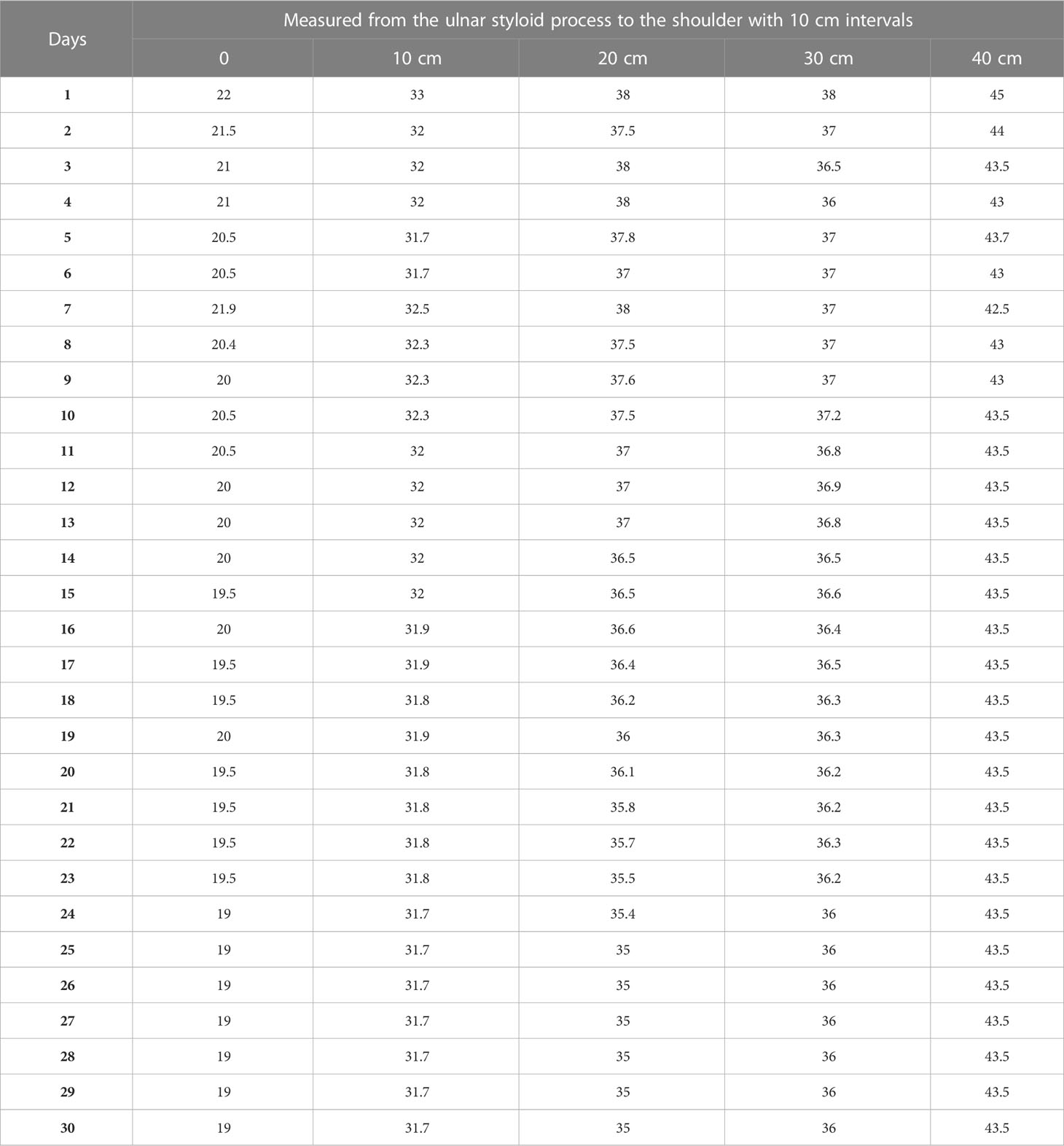
Table 1 The changes of arm circumference within the first month.

Figure 3 Functional Brace Wearing.
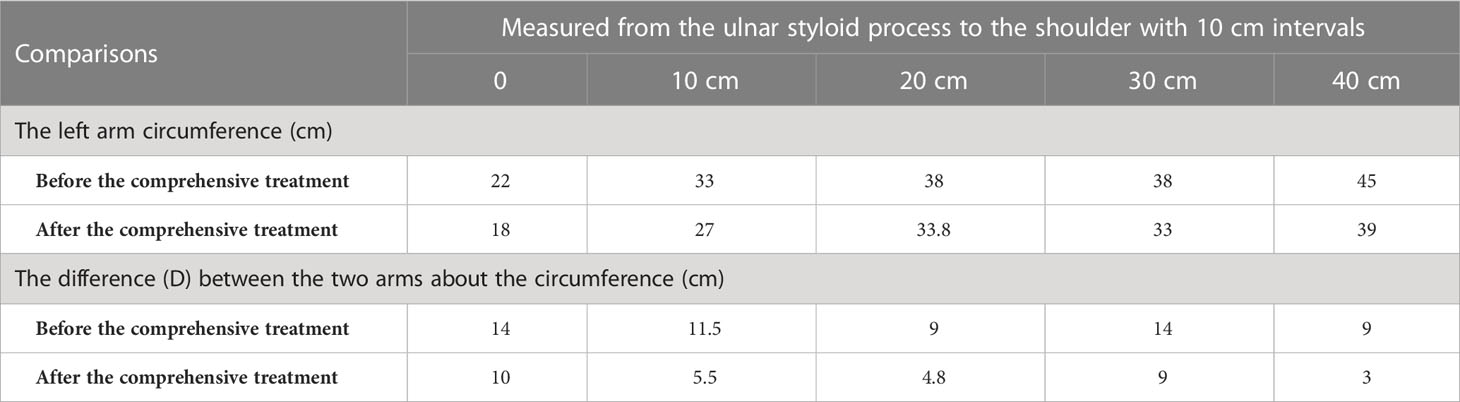
Table 2 The changes of arm circumference.
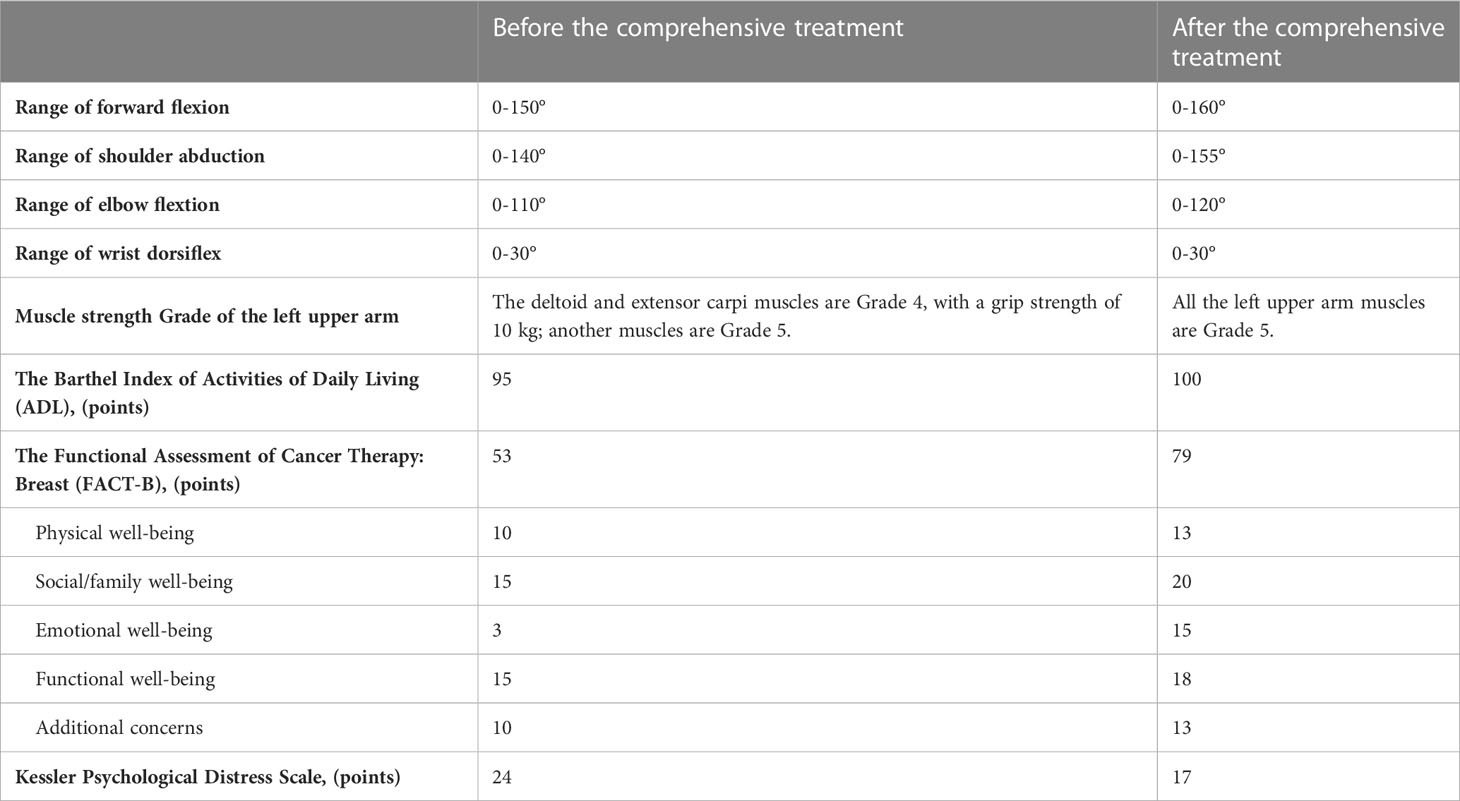
Table 3 Changes before and after the comprehensive treatment.

Figure 4 Left Upper Limb Lymphedema After Treatment.
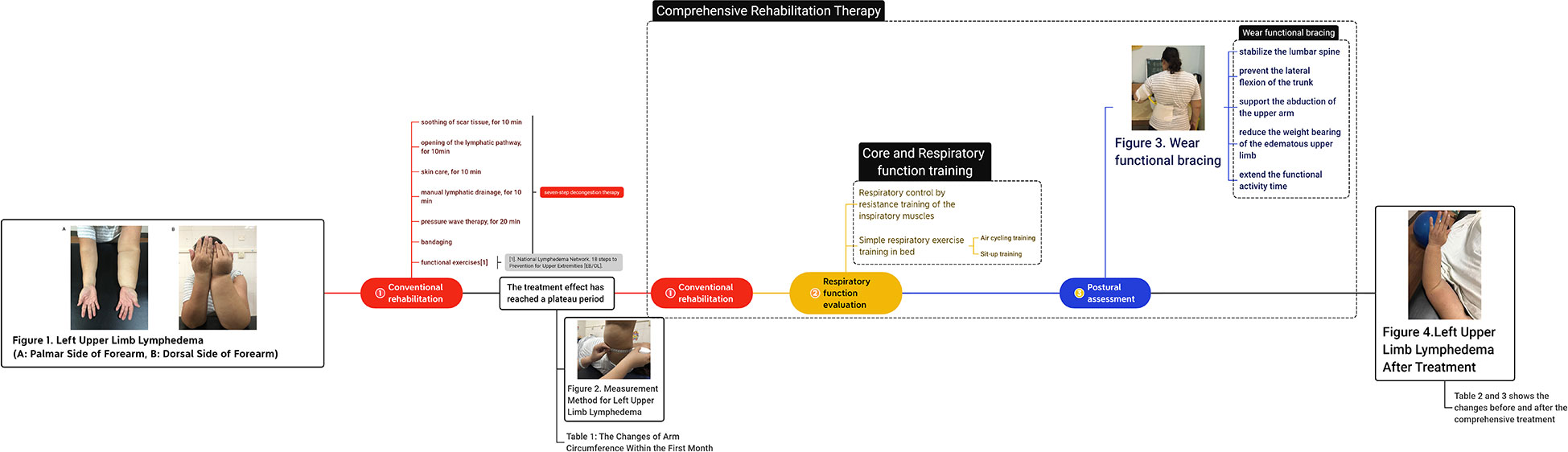
Figure 5 The flow chart of treatment.
The Ethics Committee of the Affiliated Haikou Hospital of Xiangya Medical College has approved this case report, and the informed consent of the patient has been obtained.
The prevailing view in most studies is that lymphatic obstruction is the underlying cause of upper-limb lymphedema following breast cancer surgery, although the exact mechanism remains unclear (7–10). Treatments such as surgery, radiotherapy, chemotherapy, and others can obstruct or disrupt the lymphatic return pathway in the upper limb. This can result in the retention of lymphatic fluid containing protein in the interstitial spaces, which in turn increases colloid osmotic pressure, and reduces the difference between inside and outside the blood vessels. Consequently, a large amount of fluid from capillaries can enter these spaces. Proteins present in the lymphatic fluid can stimulate the multiplication and release of collagen by fibroblasts. This can lead to fibrosis of subcutaneous tissue and inhibit lymphatic return. As a result of lymphatic vessel dilation and edema, the walls of the vessels thicken and harden and fibrinogen emboli may appear in the lumen. This obstructs lymphatic return and sets off a vicious cycle (1).
According to Stanton et al. (15) long-term work overload can lead to lymphatic pump failure and decompensation, which can eventually cause lymphedema. Bates (16) proposed the concept of interstitial space pressure dysregulation as the potential mechanics for this process. In addition, postoperative radiation can lead to fibrosis and further damage to lymphatic vessels regions such as the proximal limb, axillary, thoracic, and cervical regions where lymphatic fluid stagnation already exist. This can negatively impact, lymphatic return and worsen limb edema.
The standard treatment for lymphedema is complex decongestion therapy (CDT) (17). This therapy typically includes skin care, lymphatic drainage, elastic bandage compression, and functional exercise of the affected limb as part of the international CDT protocol (18). Seven-step CDT is a technique that aims to open the lymphatic route, soothe scar tissue, and utilize CDT-based pressure wave therapy. Shockwave therapy has shown potential benefits on BCRL according to previous research. One possible mechanism is that stretching the skin creates tension on the anchoring filaments, which pulls the Lymphatic Endothelial Cell (LEC) and allows junctions between LEC to open. This leads to fluid accumulation entering the lymphatic lumen and being collected. Additionally, it has been found to reduce skin fibrosis and impact the molecular aspects of lymphangiogenesis. However, there are limitations to its use, including mode (focused or radial), treatment area, treatment frequency, and dosage. When used in combination with CDT, it can significantly improve the volume of lymphedema, skin thickness, and shoulder ROM compared to CDT used alone. However, the current evidence for these benefits is of low methodological quality (19). Previous studies have demonstrated that seven-step CDT following breast cancer surgery can be effective in improving upper-limb lymphedema (14). Liposuction is also a potential treatment option for reducing lymphedema volume, but in this case, the patient declined this treatment option.
In the present study, one month after undergoing seven-step decongestion therapy, the patient’s left upper-limb lymphedema was alleviated. However, further reduction in the lymphedema was not observed after reaching a certain extent, possibly due to subcutaneous tissue fibrosis from prolonged lymphedema after breast cancer surgery (1). It may also have been caused by CDT limitations (1, 18, 19). Thereafter, through the combination of respiratory and core muscle training and the correction of abnormal posture, the patient’s left upper-limb lymphedema was significantly reduced.
Lymphatic fluid circulation relies on various factors such as lymphatic vessel pumping, arterial pulsation, muscle contraction, and thoracic negative pressure. The radical mastectomy of breast cancer destroyed lymph nodes, lymphatic pumping, and surrounding muscle tissue, reducing lymphatic return. In the present study, the patient’s strength, endurance, and coordination of respiratory muscles were improved, abnormal posture was adjusted, thoracic mobility was improved, thoracic breathing ability was strengthened, and thoracic negative pressure was increased, which boosted lymphatic return (20). Additionally, active rehabilitation has been shown to promote lymphatic vessel regeneration and restore vessel continuity by establishing extensive connections between normal tissues containing lymph nodes and those with lymphatic obstruction, thereby draining excessive lymphatic fluid from edematous areas (11).
We studied the effects of comprehensive rehabilitation therapy on lymphedema following breast cancer surgery. The patient in this case had persistent lymphedema and subcutaneous tissue fibrosis as a result of the surgery, and the efficacy of seven-step CDT alone was limited in the sequelae stage of breast cancer surgery. Moreover, by conducting a targeted assessment of the patient’s dysfunction, we were able to identify the underlying cause and provide specific training. Additionally, a custom auxiliary brace was used to correct the malfunction.
Seven-step decongestion therapy is a useful treatment option for managing upper-limb lymphedema in the aftermath of breast cancer surgery. However, this therapy may have limitations for patients with chronic and prolonged conditions. To address these challenges, a comprehensive rehabilitation approach can be employed, which combines seven-step decongestion therapy with core and respiratory function training, and functional brace wearing. This combined approach has been shown to significantly improve lymphedema symptoms, enhance limb function, and ultimately lead to an improved quality of life for patients with long-standing lymphedema.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of Affiliated Haikou Hospital of Xiangya Medical College. The patients/participants provided their written informed consent to participate in this study.
Conception and design of the research: Y-FS, JQ-S. Acquisition of data: S-SW Analysis and interpretation of the data: X-FL, H-XW. Statistical analysis: L-QT. Obtaining financing: Z-HS. Writing of the manuscript: Y-FS, L-QT. Critical revision of the manuscript for intellectual content: Z-HS, B-HT. All authors contributed to the article and approved the submitted version.
Project supported by Hainan Province Clinical Medical Center, NO:0202067. Supported by Hainan Provincial Natural Science Foundation of China, NO:822QN497.
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1046003/full#supplementary-material
1. Martin ML, Hernandez MA, Avendano C, Rodriguez F, Martinez H. Manual lymphatic drainage therapy in patients with breast cancer related lymphoedema. BMC Cancer (2011) 11:94. doi: 10.1186/1471-2407-11-94
2. Zhou Y, Zhang S. Research progress on postoperative rehabilitation of patients with breast cancer. Chin Gen Pract (2014) 18):2051–5. doi: 10.3969/j.issn.1007-9572.2014.18.001
3. Chen WQ, Zheng RS, Zhang SW, Li N, Zhao P, Li GL, et al. Report of incidence and mortality in china cancer registries, 2008. Chin J Cancer Res (2012) 24(3):171–80. doi: 10.1007/s11670-012-0171-2
4. Yesil H, Eyigor S, Inbat M, Bulut F. The effects of complex decongestive therapy on kinesthetic sense of hands, upper extremity function, and quality of life in patients with breast cancer-related lymphedema. Turk J Phys Med Rehabil (2021) 67(2):211–7. doi: 10.5606/tftrd.2021.5191
5. He L, Qu H, Wu Q, et al. Lymphedema in survivors of breast cancer. Oncol Lett (2020) 19(3):2085–96. doi: 10.3892/ol.2020.11307
6. Jia J. To standardize the diagnosis and treatment process of upper limb lymphedema after breast cancer surgery. Chin J Rehabil Med (2018) 33(04):375–8. doi: 10.3969/j.issn.1001-1242.2018.04.001
7. McLaughlin SA, Brunelle CL, Taghian A. Breast cancer-related lymphedema: risk factors, screening, management, and the impact of locoregional treatment. J Clin Oncol (2020) 38(20):2341–50. doi: 10.1200/JCO.19.02896
8. Gillespie TC, Sayegh HE, Brunelle CL, Daniell KM, Taghian AG. Breast cancer-related lymphedema: risk factors, precautionary measures, and treatments. Gland Surg (2018) 7(4):379–403. doi: 10.21037/gs.2017.11.04
9. Nguyen TT, Hoskin TL, Habermann EB, Cheville AL, Boughey JC. Breast cancer-related lymphedema risk is related to multidisciplinary treatment and not surgery alone: results from a Large cohort study. Ann Surg Oncol (2017) 24(10):2972–80. doi: 10.1245/s10434-017-5960-x
10. Paskett ED, Dean JA, Oliveri JM, Harrop JP. Cancer-related lymphedema risk factors, diagnosis, treatment, and impact: a review. J Clin Oncol (2012) 30(30):3726–33. doi: 10.1200/JCO.2012.41.8574
11. Panchik D, Masco S, Zinnikas P, Hillriegel B, Lauder T, Suttmann E, et al. Effect of exercise on breast cancer-related lymphedema: what the lymphatic surgeon needs to know. J Reconstr Microsurg (2019) 35(1):37–45. doi: 10.1055/s-0038-1660832
12. Gutierrez-Espinoza H, Araya-Quintanilla F, Olguin-Huerta C, Valenzuela-Fuenzalida J, Gutierrez-Monclus R, Moncada-Ramirez V. Effectiveness of manual therapy in patients with distal radius fracture: a systematic review and meta-analysis. J Man Manip Ther (2022) 30(1):33–45. doi: 10.1080/10669817.2021.1992090
13. Huang TW, Tseng SH, Lin CC, Bai CH, Chen CS, Hung CS, et al. Effects of manual lymphatic drainage on breast cancer-related lymphedema: a systematic review and meta-analysis of randomized controlled trials. World J Surg Oncol (2013) 11:15. doi: 10.1186/1477-7819-11-15
14. Zhang H, Zhong Q, Zhang H, Liu L, Liu L, Zhang L, et al. Effects of seven-step complex decongestion therapy on upper limb lymphedema after operation for breast cancer. Chin J Rehabil Theory Pract (2017) 23(9):1015–20. doi: 10.3969/j.issn.1006-9771.2017.09.006
15. Stanton AW, Modi S, Bennett BT, Purushotham AD, Peters AM, Levick JR, et al. Lymphatic drainage in the muscle and subcutis of the arm after breast cancer treatment. Breast Cancer Res Treat (2009) 117(3):549–57. doi: 10.1007/s10549-008-0259-z
16. Bates DO. An interstitical by pothesis for breast cancer related lymphedema. Pathophysiology (2010) 17(4):289–94. doi: 10.1016/j.pathophys.2009.10.006
17. Leal NF, Carrara HH, Vieira KF, Ferreira CH. Physiotherapy treatments for breast cancer-related lymphedema: a literature review. Rev Lat Am Enfermagem (2009) 17(5):730–6. doi: 10.1590/S0104-11692009000500021
18. Koo JH, Song SH, Oh HS, Oh SH. Comparison of the short-term effects of hyperbaric oxygen therapy and complex decongestive therapy on breast cancer-related lymphedema: a pilot study. Med (Baltimore) (2020) 99(11):19564. doi: 10.1097/MD.0000000000019564
19. Tsai YL, TJ I, Chuang YC, Cheng YY, Lee YC. Extracorporeal shock wave therapy combined with complex decongestive therapy in patients with breast cancer-related lymphedema: a systemic review and meta-analysis. J Clin Med (2021) 10(24):5970. doi: 10.3390/jcm10245970
Keywords: breast cancer, comprehensive rehabilitation, functional brace, lymphedema, seven-step decongestion therapy
Citation: Sui Y-F, Tong L-Q, Lin X-F, Wu H-X, Shi J-Q, Wang S-S, Tang B-H and Song Z-H (2023) Revitalizing quality of life: a case report on the beneficial impact of comprehensive rehabilitation therapy in treating upper-limb lymphedema following breast cancer surgery. Front. Oncol. 13:1046003. doi: 10.3389/fonc.2023.1046003
Received: 16 September 2022; Accepted: 23 May 2023;
Published: 16 June 2023.
Edited by:
Areerat Suputtitada, Chulalongkorn University, ThailandCopyright © 2023 Sui, Tong, Lin, Wu, Shi, Wang, Tang and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhen-Hua Song, c29uZ3poZW5odWFzemg5QDEyNi5jb20=; Bu-He Tang, dGFuZ2J1aGUyMDA4QDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.