
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 04 October 2022
Sec. Hematologic Malignancies
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.992137
This article is part of the Research TopicCOVID-19 and Hematologic Malignancies: Volume IIIView all 4 articles
 Maria Stefania Infante1†§
Maria Stefania Infante1†§ Jon Salmanton-García2,3*†§
Jon Salmanton-García2,3*†§ Ana Fernández-Cruz4†§
Ana Fernández-Cruz4†§ Francesco Marchesi5§
Francesco Marchesi5§ Ozren Jaksic6§Barbora Weinbergerová7§Caroline Besson8§
Ozren Jaksic6§Barbora Weinbergerová7§Caroline Besson8§ Rafael F. Duarte4Federico Itri9§Toni Valković10,11,12§Tomáš Szotkovski13
Rafael F. Duarte4Federico Itri9§Toni Valković10,11,12§Tomáš Szotkovski13 Alessandro Busca14§Anna Guidetti15§
Alessandro Busca14§Anna Guidetti15§ Andreas Glenthøj16§
Andreas Glenthøj16§ Graham P. Collins17Valentina Bonuomo18§Uluhan Sili19§
Graham P. Collins17Valentina Bonuomo18§Uluhan Sili19§ Guldane Cengiz Seval20§Marina Machado21§
Guldane Cengiz Seval20§Marina Machado21§ Raul Cordoba22§Ola Blennow19§Ghaith Abu-Zeinah23§Sylvain Lamure24§
Raul Cordoba22§Ola Blennow19§Ghaith Abu-Zeinah23§Sylvain Lamure24§ Austin Kulasekararaj25,26§
Austin Kulasekararaj25,26§ Iker Falces-Romero27§
Iker Falces-Romero27§ Chiara Cattaneo28§Jaap Van Doesum29§Klára Piukovics30§
Chiara Cattaneo28§Jaap Van Doesum29§Klára Piukovics30§ Ali S. Omrani31§Gabriele Magliano32§Marie-Pierre Ledoux33§Cristina de Ramon34,35§Alba Cabirta36,37,38§Luisa Verga39,40§Alberto López-García41§Maria Gomes Da Silva42§Zlate Stojanoski43§
Ali S. Omrani31§Gabriele Magliano32§Marie-Pierre Ledoux33§Cristina de Ramon34,35§Alba Cabirta36,37,38§Luisa Verga39,40§Alberto López-García41§Maria Gomes Da Silva42§Zlate Stojanoski43§ Stef Meers44
Stef Meers44 Tobias Lahmer45Sonia Martín-Pérez46Julio Dávila-Vals46
Tobias Lahmer45Sonia Martín-Pérez46Julio Dávila-Vals46 Jens Van Praet47§Michail Samarkos48Yavuz M. Bilgin49§Linda Katharina Karlsson16Josip Batinić50Anna Nordlander19Martin Schönlein51§Martin Hoenigl52,53,54§Zdeněk Ráčil55§Miloš Mladenović56Michaela Hanakova55Giovanni Paolo Maria Zambrotta39,40
Jens Van Praet47§Michail Samarkos48Yavuz M. Bilgin49§Linda Katharina Karlsson16Josip Batinić50Anna Nordlander19Martin Schönlein51§Martin Hoenigl52,53,54§Zdeněk Ráčil55§Miloš Mladenović56Michaela Hanakova55Giovanni Paolo Maria Zambrotta39,40 Nick De Jonge57§Tatjana Adžić-Vukičević56Raquel Nunes-Rodrigues42Lucia Prezioso58§Milan Navrátil59Monia Marchetti60§
Nick De Jonge57§Tatjana Adžić-Vukičević56Raquel Nunes-Rodrigues42Lucia Prezioso58§Milan Navrátil59Monia Marchetti60§ Annarosa Cuccaro61§Maria Calbacho62§Antonio Giordano63,64§
Annarosa Cuccaro61§Maria Calbacho62§Antonio Giordano63,64§ Oliver A. Cornely2,3,65,66,67§José-Ángel Hernández-Rivas1‡§
Oliver A. Cornely2,3,65,66,67§José-Ángel Hernández-Rivas1‡§ Livio Pagano64‡§
Livio Pagano64‡§Patients with lymphoproliferative diseases (LPD) are vulnerable to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Here, we describe and analyze the outcome of 366 adult patients with chronic lymphocytic leukemia (CLL) or non-Hodgkin Lymphoma (NHL) treated with targeted drugs and laboratory-confirmed COVID-19 diagnosed between February 2020 and January 2022. Median follow-up was 70.5 days (IQR 0-609). Most used targeted drugs were Bruton-kinase inhibitors (BKIs) (N= 201, 55%), anti-CD20 other than rituximab (N=61, 16%), BCL2 inhibitors (N=33, 9%) and lenalidomide (N=28, 8%).Only 16.2% of the patients were vaccinated with 2 or more doses of vaccine at the onset of COVID-19. Mortality was 24% (89/366) on day 30 and 36%(134/366) on the last day of follow-up. Age >75 years (p<0.001, HR 1.036), active malignancy (p<0.001, HR 2.215), severe COVID-19 (p=0.017, HR 2.270) and admission to ICU (p<0.001, HR 5.751) were risk factors for mortality at last day of follow up. There was no difference in OS rates in NHL vs CLL patients (p=0.306), nor in patients treated with or without BKIs (p=0.151). Mortality in ICU was 66% (CLL 61%, NHL 76%). Overall mortality rate decreased according to vaccination status, being 39% in unvaccinated patients, 32% and 26% in those having received one or two doses, respectively, and 20% in patients with a booster dose (p=0.245). Overall mortality rate dropped from 41% during the first semester of 2020 to 25% at the last semester of 2021. These results show increased severity and mortality from COVID-19 in LPDs patients treated with targeted drugs.
The coronavirus disease 2019 (COVID-19) pandemic has challenged particularly vulnerable individuals such as those with cancer (1–4). Even among patients with cancer, the overall outcome, degree of immunodeficiency, and effect of cancer therapy on immunocompetence vary widely, leading to very different outcomes, depending on the underlying malignancy and its treatment.
Lymphoproliferative diseases (LPD) are a group of malignancy associated with a marked immunodeficiency, characterized by hypogammaglobulinemia, qualitative and quantitative B- and T-cell defects (5), CD4+ lymphopenia, as well as innate immune dysfunction and neutropenia (6). These immunodeficiencies are a result of the disease itself and its treatment, and lead to impaired immune response to common pathogens and poor response to vaccination (7, 8)
The introduction of targeted agents in the treatment of B-cell malignancies has changed their management. These therapies attempt to harness power from the patient’s immune system to eradicate lymphoma. In chronic lymphoid leukemia (CLL), oral Bruton tyrosine-kinase inhibitors (BKIs) such as ibrutinib and acalabrutinib, and the BCL2 inhibitor (venetoclax) have been increasingly used, replacing conventional chemotherapy in frontline treatment because of their improved progression-free survival (9–13). In indolent lymphomas, several phosphoinositide 3-kinase (PIK3) inhibitors have been approved in patients with relapse disease (14–16), but the use of these agents has been limited due to toxicities, including infection. A combination of lenalidomide and rituximab is a safe and effective therapy for patients with refractory indolent lymphoma (17). Anti-CD30 and anti-PD1 have improved the prognosis of naïve (18) and relapsed (19) Hodgkin lymphomas, and the new antibody conjugate polatuzumab vedotin has been introduced in the treatment of diffuse large B-cell lymphoma (20).
Targeted drugs differ from conventional chemotherapy regarding the risk for infection. Opportunistic infections have been reported in patients receiving ibrutinib (21). Therapy with idelalisib has been associated with an overall risk of infection, especially fungal (16, 22, 23), and in combination with rituximab-bendamustine (RB), high rates of cytomegalovirus (CMV) reactivation have been reported (24). By contrast, venetoclax does not seem to be associated with additional risks of infection (23). The risk of infection in patients with LPD treated with brentuximab (25, 26) are variable while neutropenia is a common side effect.
Focusing on COVID-19 infection, several studies have reported impaired serologic response after COVID-19 vaccination in CLL patients, especially those treated with anti-CD20 antibodies in the 12 months prior to infection, followed by BKIs and venetoclax-treated patients (27–29).
Several small series of CLL patients with COVID-19, mostly treated with ibrutinib, have been published to date, reporting a high rate of mortality and severity of infection (30, 31). Ibrutinib was initially thought to improve the outcome of COVID-19, based on retrospective studies (32, 33), but several subsequent clinical trials failed to confirm such benefit (34).
To date, only limited data are available on the clinical course of COVID-19 in patients with different underlying LPD treated with targeted drugs. We undertook a retrospective international multicenter study to evaluate the outcome of COVID-19 in patients with LPD treated with targeted drugs and in order to identify potential predictors of outcome.
In this retrospective observational, multicenter study, we collected data on adult patients with LPD who received targeted therapy and were diagnosed with COVID-19 between February 2020 and January 2022 across 25 countries that participated in the survey promoted by the European Hematology Association (EHA) – Scientific Working Group Infection in Hematology EPICOVIDEHA survey (35, 36).Targeted drugs included: BKIs (acalabrutinib, ibrutinib, zanabrutinib), BCL2 inhibitors (venetoclax), anti-CD20 antibodies (obinutuzumab, ofatumumab) anti-CD30 (brentuximab), anti-CD79 (polatuzumab), anti-PD1 (pembrolizumab, nivolumab), immunomodulatory drugs (IMiDs) (lenalidomide) and PI3K inhibitors (idelalisib). Patients treated with rituximab were not specifically included in this study as another analysis has been performed by the EPICOVIDEHA survey (35, 36). Confirmed cases of COVID-19 were defined by a positive reverse transcriptase-polymerase chain reaction (RT-PCR) assay of a specimen collected by a nasopharyngeal swab. Pandemic waves were defined in time as follows: January-June 2020 (n=108), July-December 2020 (n=144), January-June 2021 (n=62), July-January 2022 (n=52). Each institutional review board independently approved the study. The study was conducted following the Declaration of Helsinki. Researchers at each center collected data using an online questionnaire hosted at www.clinicalsurveys.net (EFS Fall 2018, Questback, Cologne, Germany). EPICOVIDEHA is registered at http://www.clinicaltrials.gov, with the identifier NCT 04733729. Only de-identified data were entered and analyzed. We obtained demographic data, comorbidities, and underlying hematological disease including clinically significant outcomes (hospital admission and intensive care unit [ICU] admission, vital status) and COVID-19 management strategies. The severity of COVID-19 at admission was graded according to the China Centers for Disease Control and Prevention definitions: mild (non-pneumonia and mild pneumonia), severe (dyspnea, respiratory frequency ≥30 breaths per min, SpO2 ≤93%, PaO2/FiO2 50%), and critical (respiratory failure, septic shock, or multiple organ dysfunction or failure).
SPSSv25.0 was used for statistical analyses (SPSS, IBM Corp., Chicago, IL, United States). Categorical variables were presented as frequencies and percentages, while continuous variables by the median, interquartile range (IQR), and absolute range. Additionally, overall mortality was evaluated by a Cox proportional hazard model. A Univariable Cox regression model was performed including variables that potentially played a role in the mortality of patients. Variables with a p-value ≤0.1 were considered for the multivariable analysis. The Multivariable Cox regression model was calculated by the Wald backward method, and only statistically significant variables were reported. A p-value ≤0.05 was considered statistically significant.
In the study period, we identified 366 patients with LPD receiving targeted drugs at diagnosis of COVID-19. The median age at COVID-19 diagnosis was 68 years (IQR 58-77, range 25-96).
Baseline characteristics for the entire cohort are described in Table 1. Of the 366 patients, 204 (55.7%) were CLL and 162 (44.3%) NHL. The population had a male predominance (n= 222, 60.7%) Contributing countries are listed in Figure 1. Around 33.1% (n= 132) of the patients had two or more comorbidities: chronic cardiopathy (n=125, 34.2%), chronic pulmonary disease (n=80, 21.9%) and diabetes (n= 64,17.5%) were the most common ones.
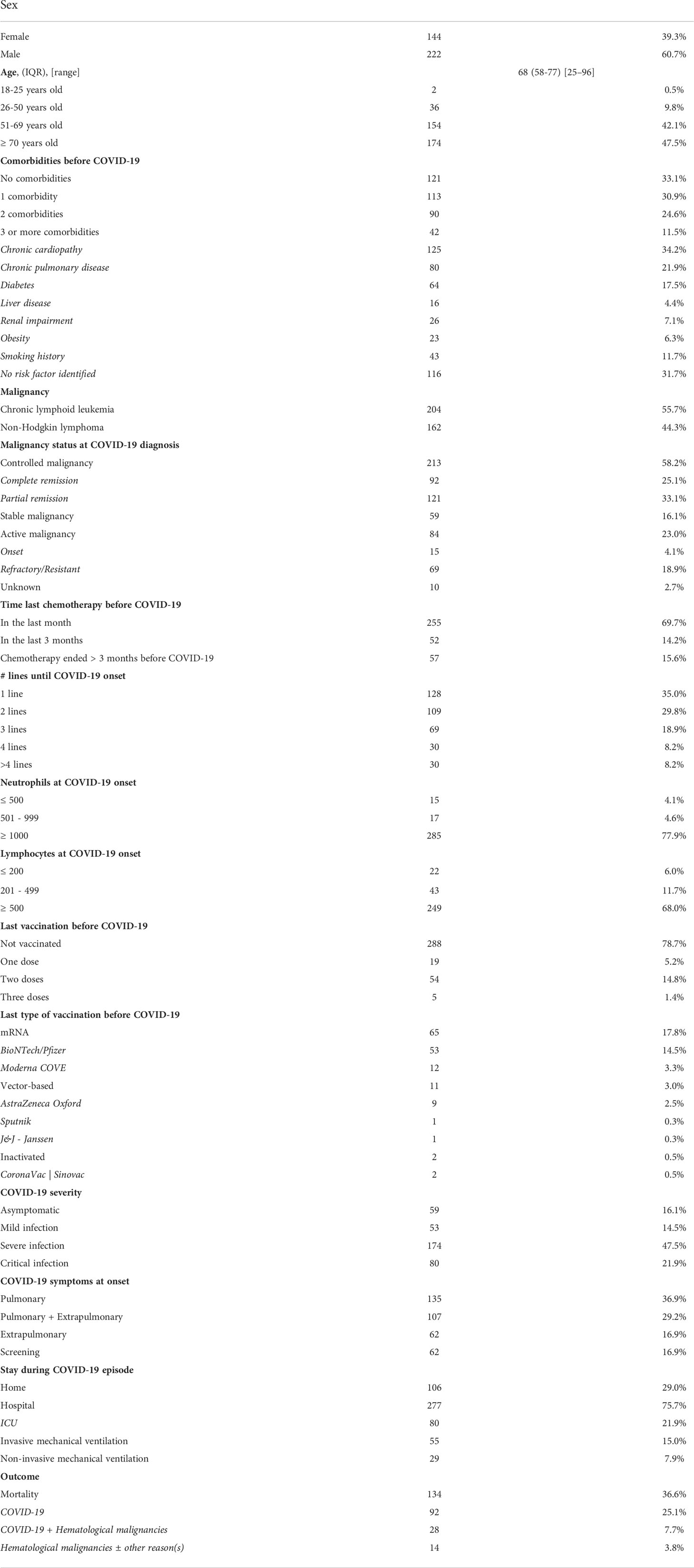
Table 1 Patients’ characteristics.
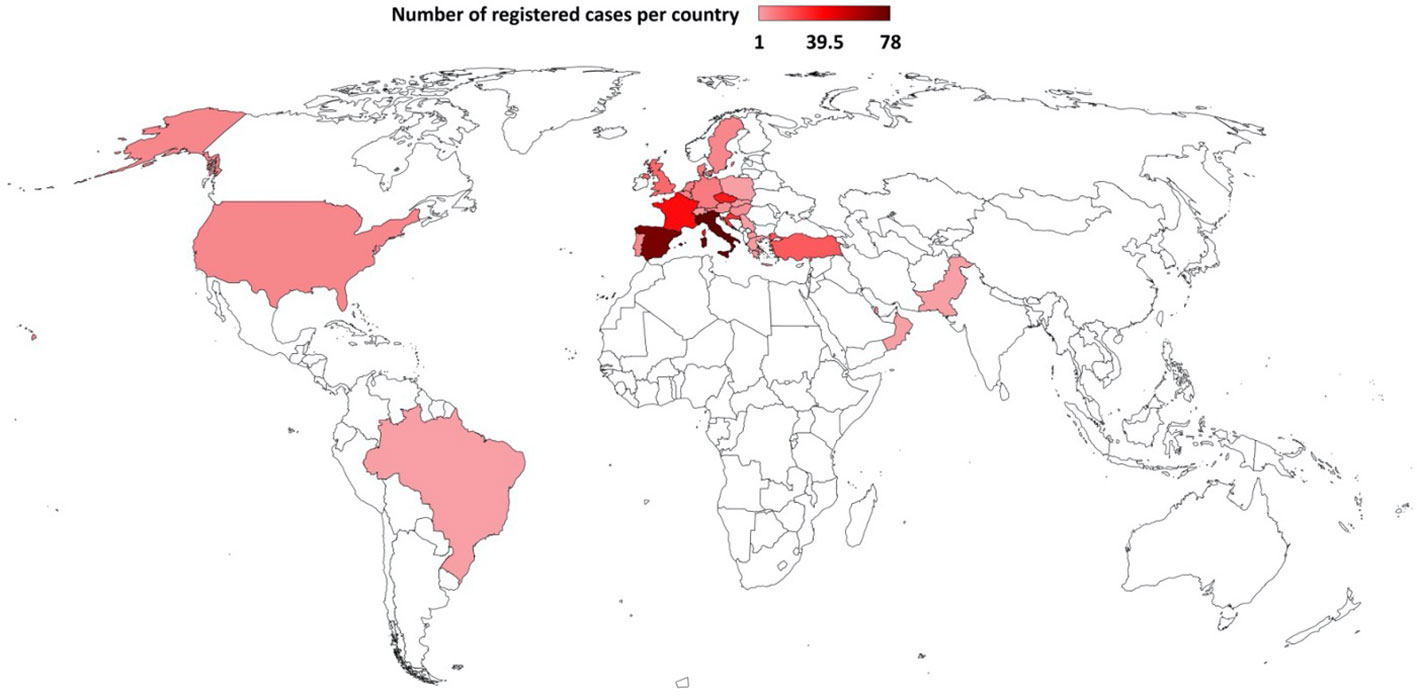
Figure 1 Countries contributing CLL and NHL cases to EPICOVIDEHA receiving targeted malignancy treatment, as of January 2022. Italy (n=78), Spain (n=72), France (n=37), Czech Republic (n=33), Croatia (n=27), Turkey (n=18), United Kingdom (n=14), Denmark (n=10), Germany (n=10), Netherlands (n=9), Belgium (n=8), Sweden and United States (n=7, each), Portugal (n=6), Austria, Hungary and Qatar (n=5, each), North Macedonia and Switzerland (n=3, each), Greece and Slovakia (n=2, each) and Brazil, Oman, Pakistan, Poland and Serbia (n=1, each).
Thirty-five percent (n=128) of the patients were receiving the targeted drug as first-line therapy, 29.8% (n= 109) as 2nd line, 18.9% (n=69) as 3rd line, and 16.4% (n=60) had been heavily pretreated with 4 or more prior lines of therapy.
The most commonly used targeted drugs were BKIs (n=201,54.9%), anti-CD20 other than rituximab (n=60,16.4%), BCL2 inhibitors (n=33, 9%) and lenalidomide (n=28,7.7%) (Table 2). Of note, only 21.0% of the patients had received two or more doses of SARS-CoV-2 vaccine at the onset of COVID-19: mRNA vaccines were administered in 83% patients. Respiratory symptoms were present in 66.1% of patients (n= 242) while 16.9% (n= 62) presented with extrapulmonary symptoms. Of note, our series includes 16.9% (n=62) asymptomatic COVID-19 patients detected upon screening.
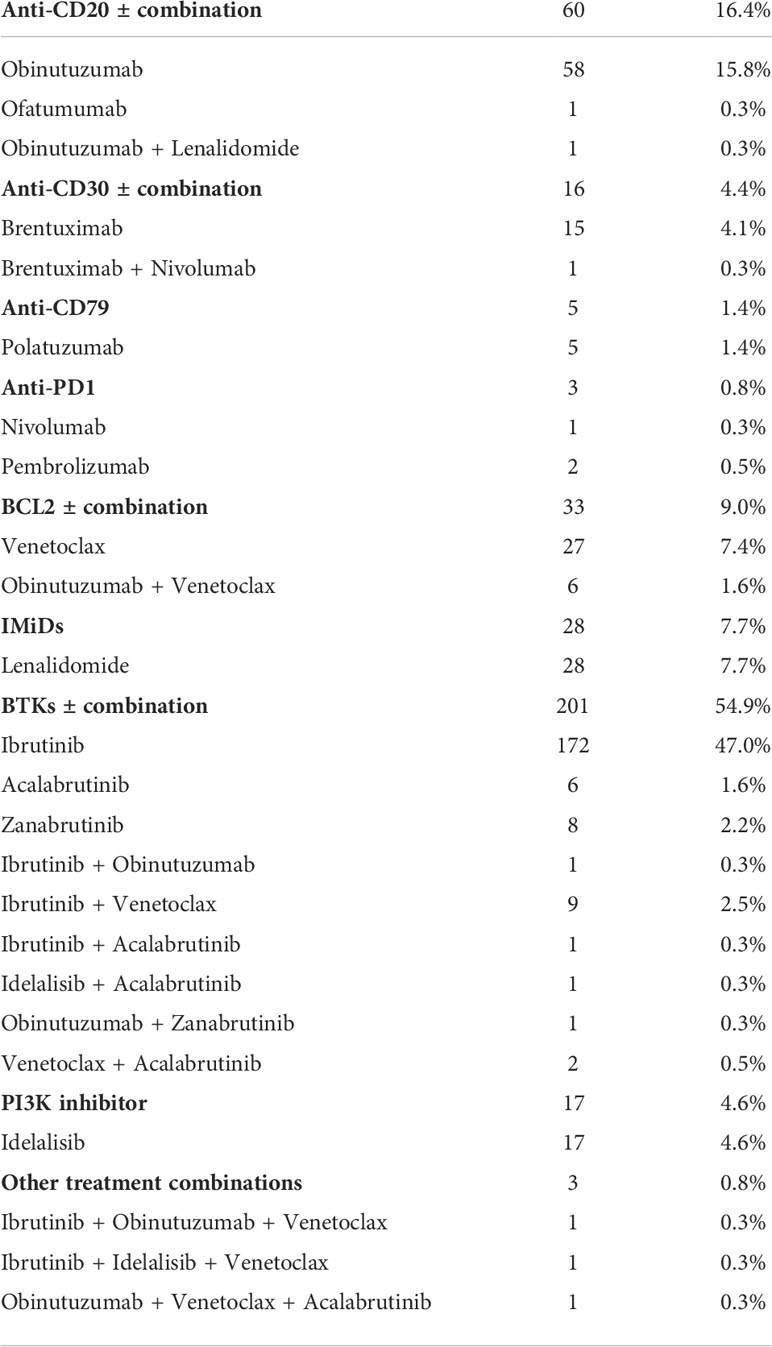
Table 2 LPD directed therapy at time of COVID-19 diagnosis.
The majority of patients (n=277, 75.7%) were hospitalized, with a median stay of 16 days (IQR 8-26, range, 1-137).
Severe COVID-19 was observed in 47.5% (n=174) of patients, including 21.9% (n=80) who were admitted to intensive care unit (ICU). Among the latter, 55 (68.8%) were CLL patients, and 25 (31.3%) were non-Hodgkin lymphoma (NHL) patients. Fifty-five (44%) of the ICU-admitted patients underwent invasive mechanical ventilation. The median ICU stay in the entire cohort was 9 days (IQR 2-50, range, 6-14).
The presence of comorbidities was significantly associated with severe COVID-19 infection in the entire cohort (p= 0.002) as well as in the CLL and NHL subsets and BKIs cohort. Severe infection was more frequent in the first COVID-19 pandemic wave comparing to more recent waves (p=0.001). Another factor associated with severe infection was male sex (p=0.001). Age (both >65 or >75), type of targeted drug therapy and time from the last treatment of the hematologic malignancy to COVID-19 infection were not associated with severe infection in any subgroup analysis. No significant risk factor for severe COVID-19 was found in patients receiving BLC-2 inhibitors plus anti-CD20 monoclonal antibodies.
Overall, 134 patients (36.6%) died (Table 3). The primary cause of death was COVID-19 in 92 patients (68.7%), LPD in 14 patients (10.4%), and a combination of both in 28 patients (20.9%). The mortality rate was 24.3% (89/366) on day 30 of COVID-19 diagnosis and 36.6% (134/366) on the last day of follow-up. The median follow-up at the time of this analysis was 70.5 days (IQR 19-159, range 0-609 days). Distribution of registered cases along time is shown in Figure 2.
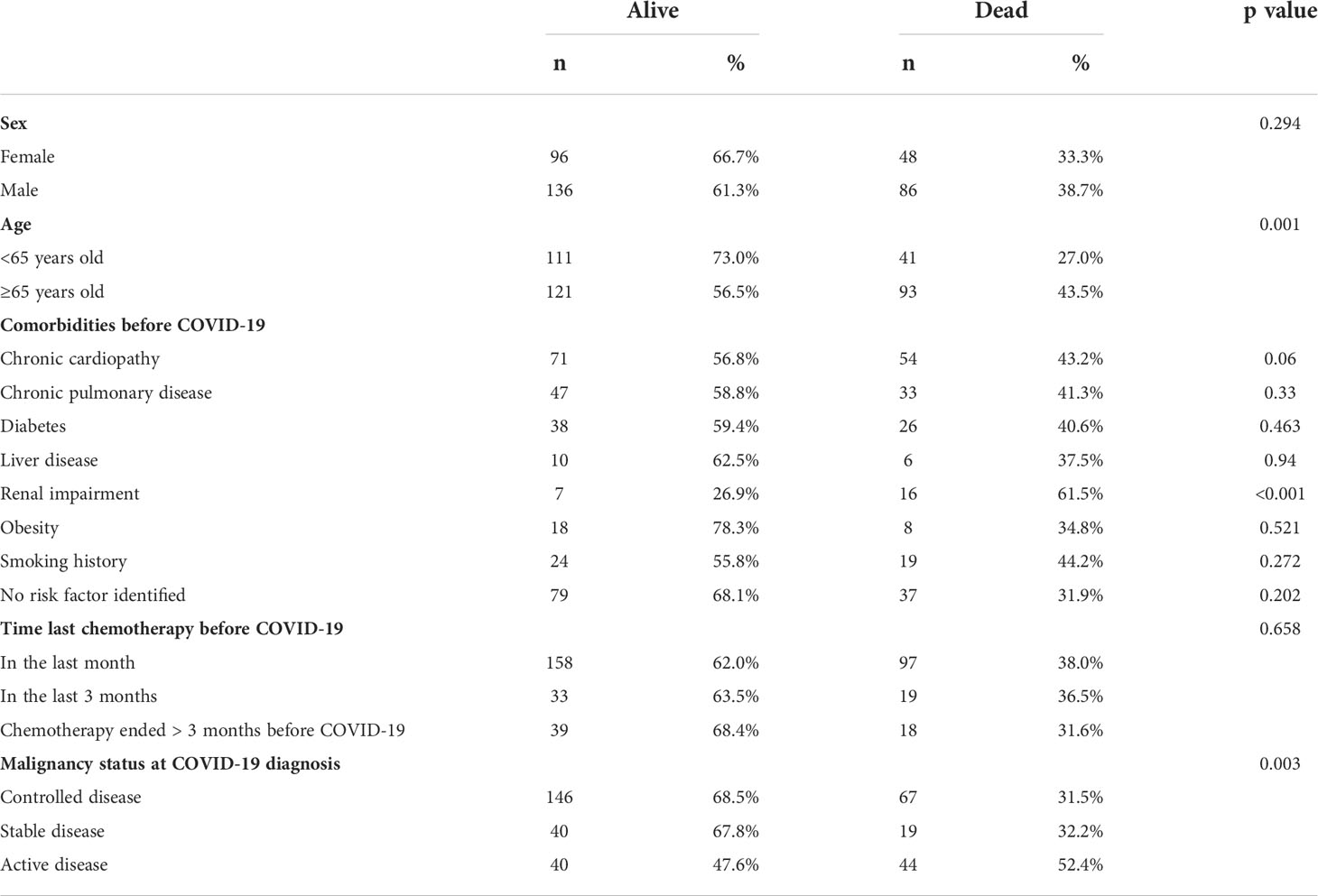
Table 3 Patient’s disposition based on mortality.
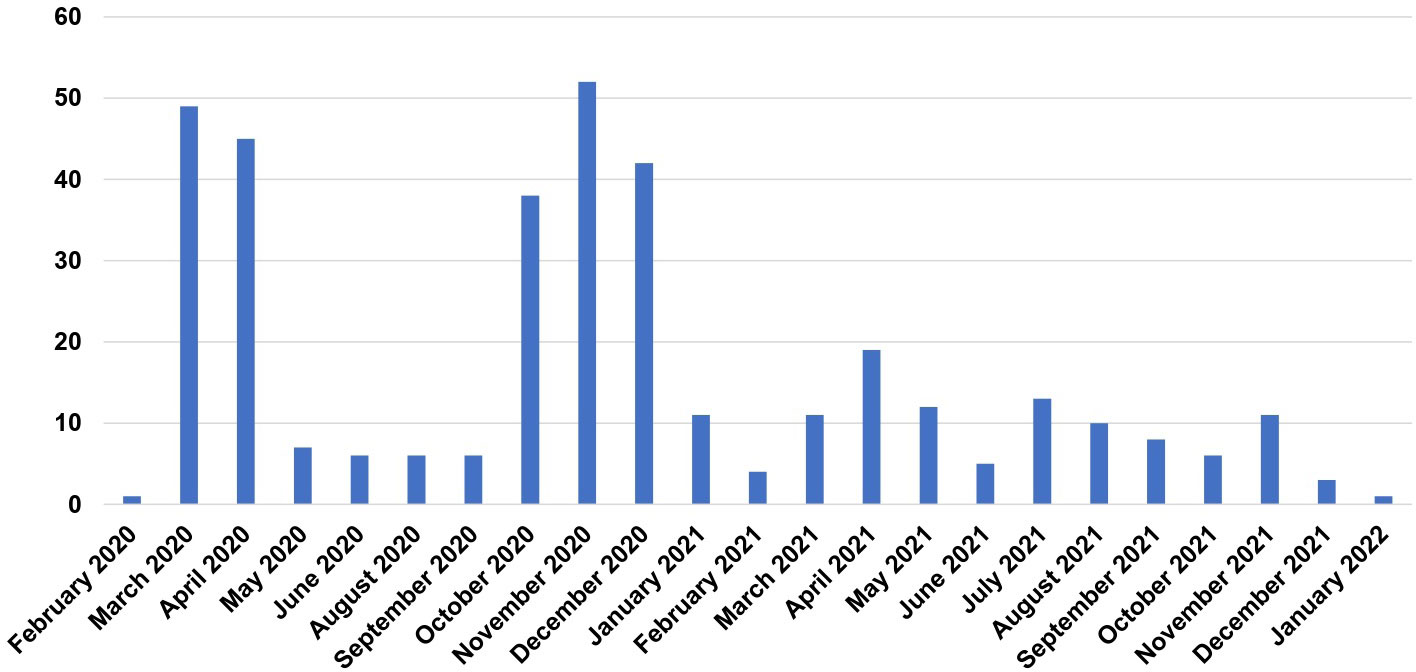
Figure 2 Distribution of registered cases along time.
Survival in patients admitted to ICU was 33.7% (CLL 38.1%, NHL 24%). The overall mortality rate decreased with vaccination, being 34.2% in unvaccinated patients, 15.9-18% with one or two doses, and 9.7% in patients with a booster dose (p<0.001) (Figure 3). Additionally, the mortality rate dropped from the first semester of 2020 (41.3%) to the last semester of 2021 (25%).
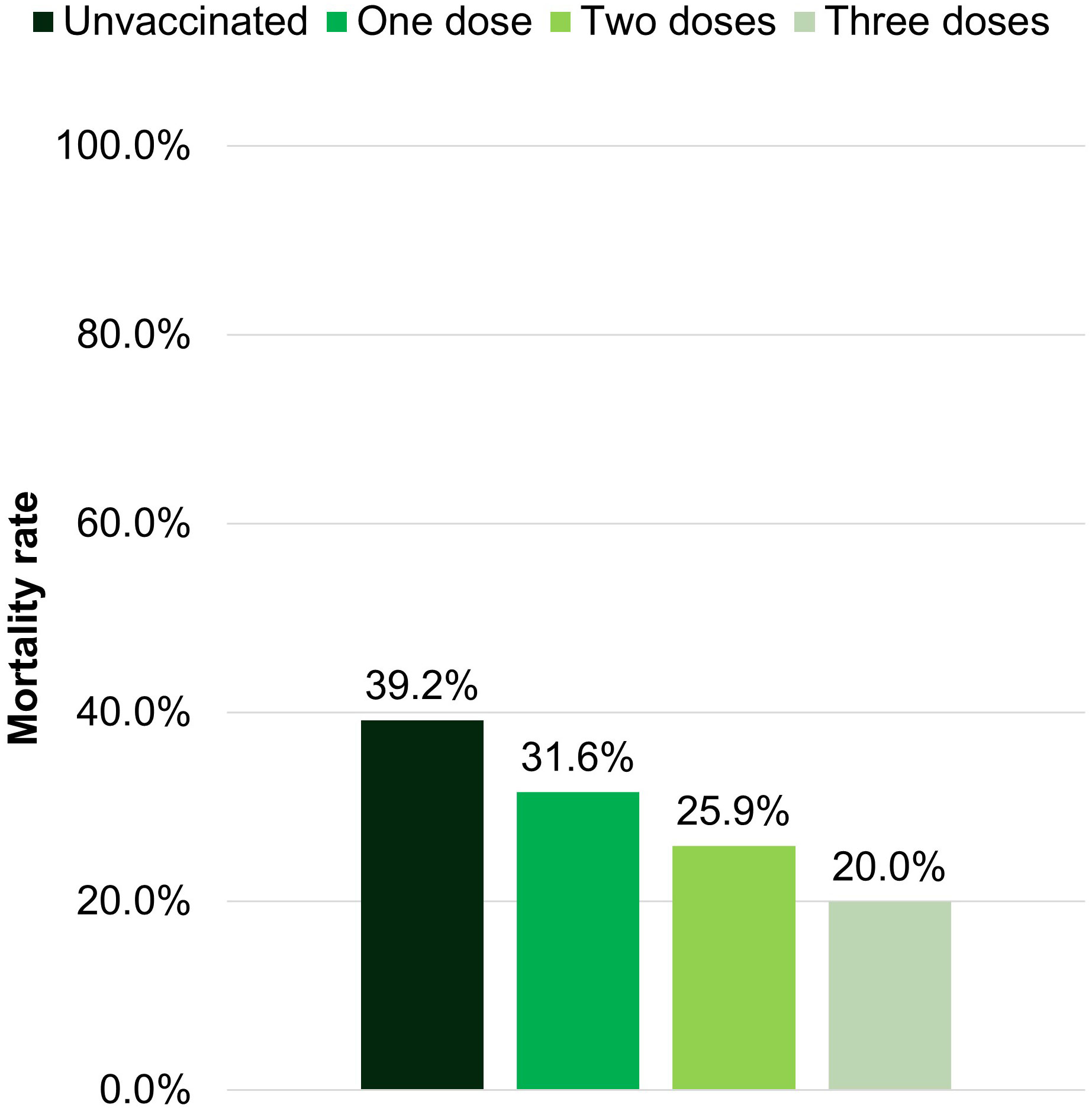
Figure 3 Mortality rate depending on the vaccination status.
Table 4A summarizes the univariable and multivariable analyses of baseline characteristics as predictors of OS in the entire cohort and in the subsets of CLL and NHL patients (Tables 4B, C in supplementary materials). In univariable analysis, age >75 years, active hematological disease, severe and critical COVID-19 infection, heart disease, and renal impairment were associated with an increased mortality rate.
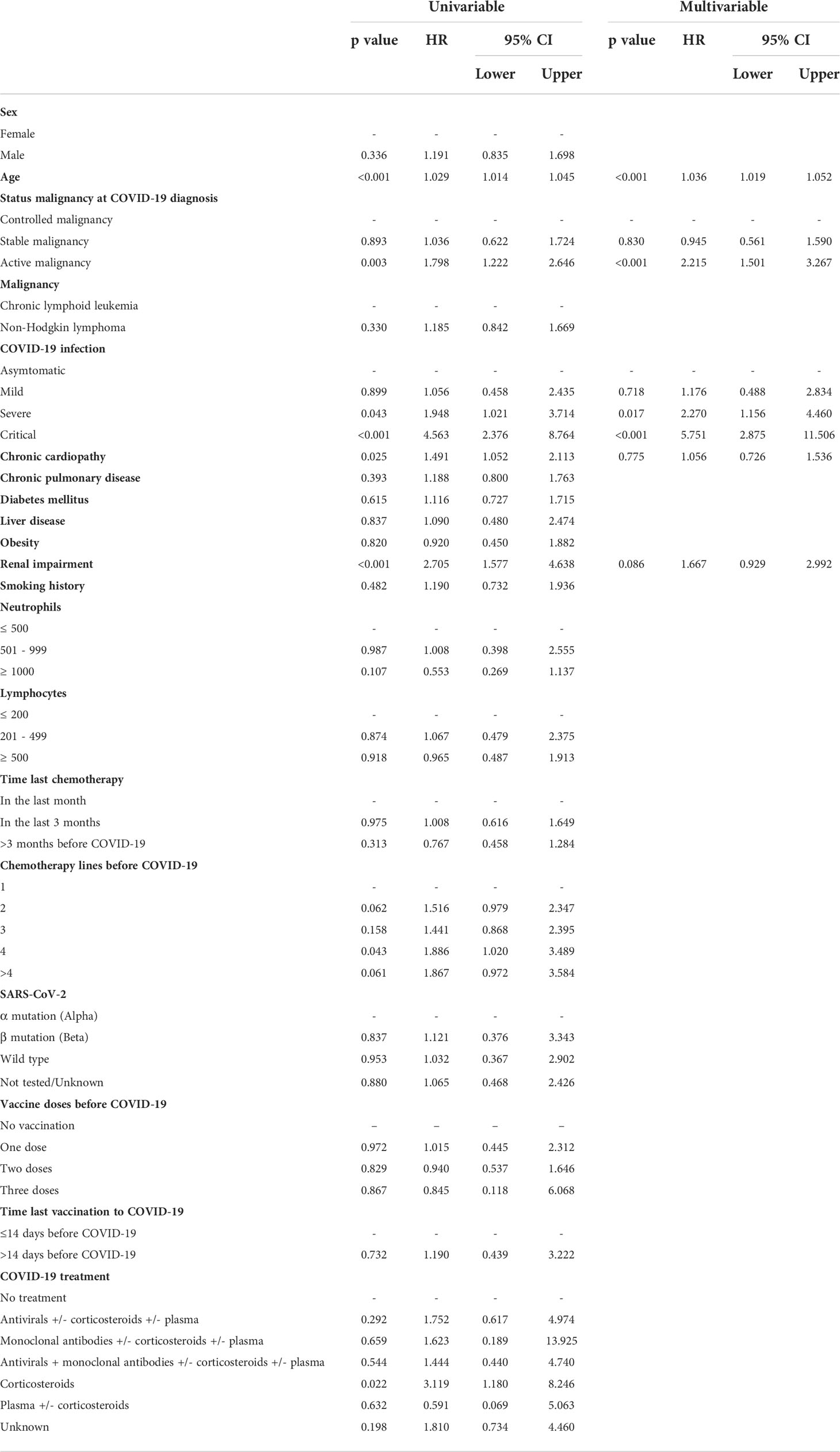
Table 4A Univariable and multivariable analysis of predictors of mortality in the entire cohort.
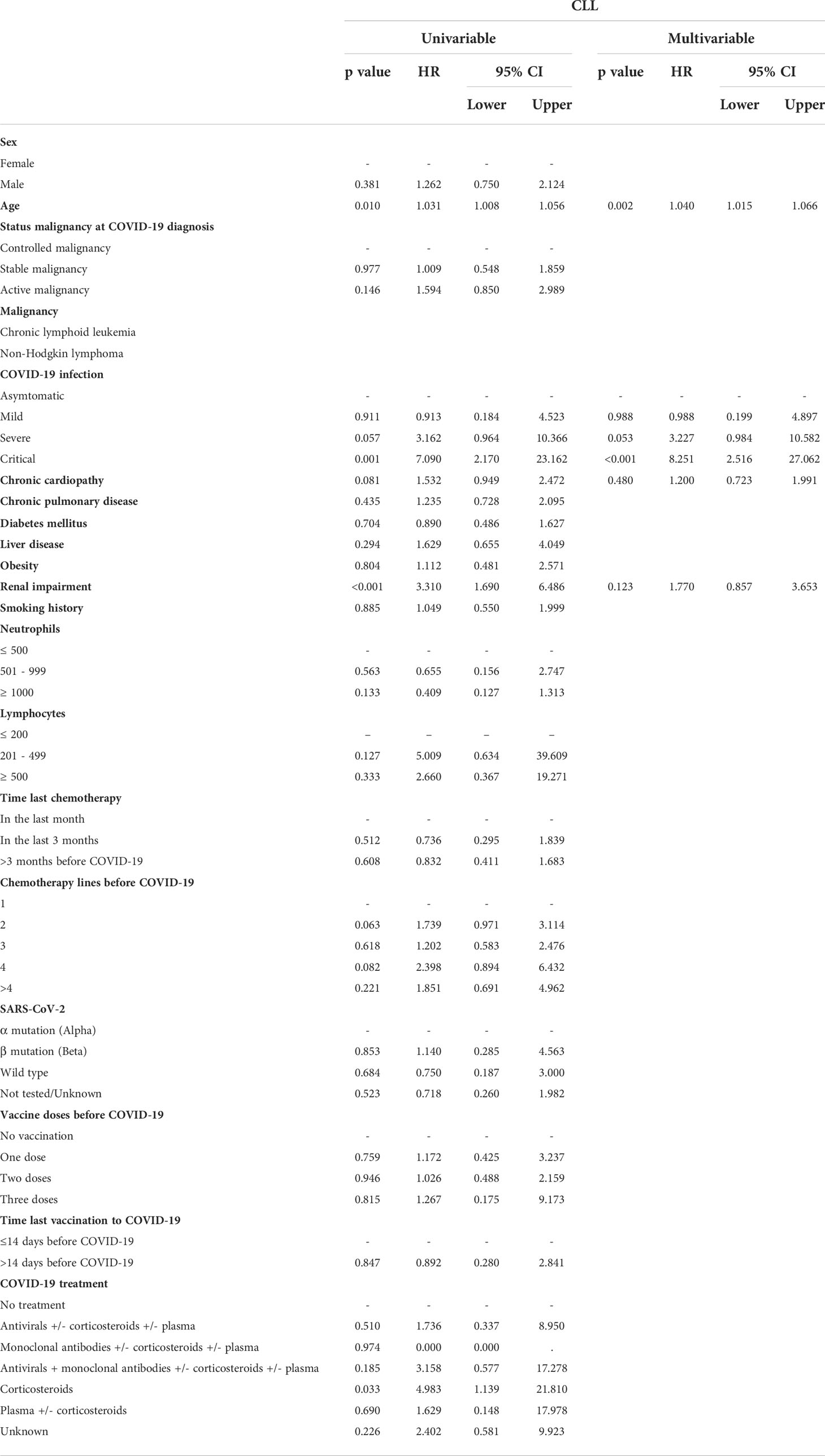
Table 4B Univariable and multivariable analysis of predictors of mortality in the CLL patients.
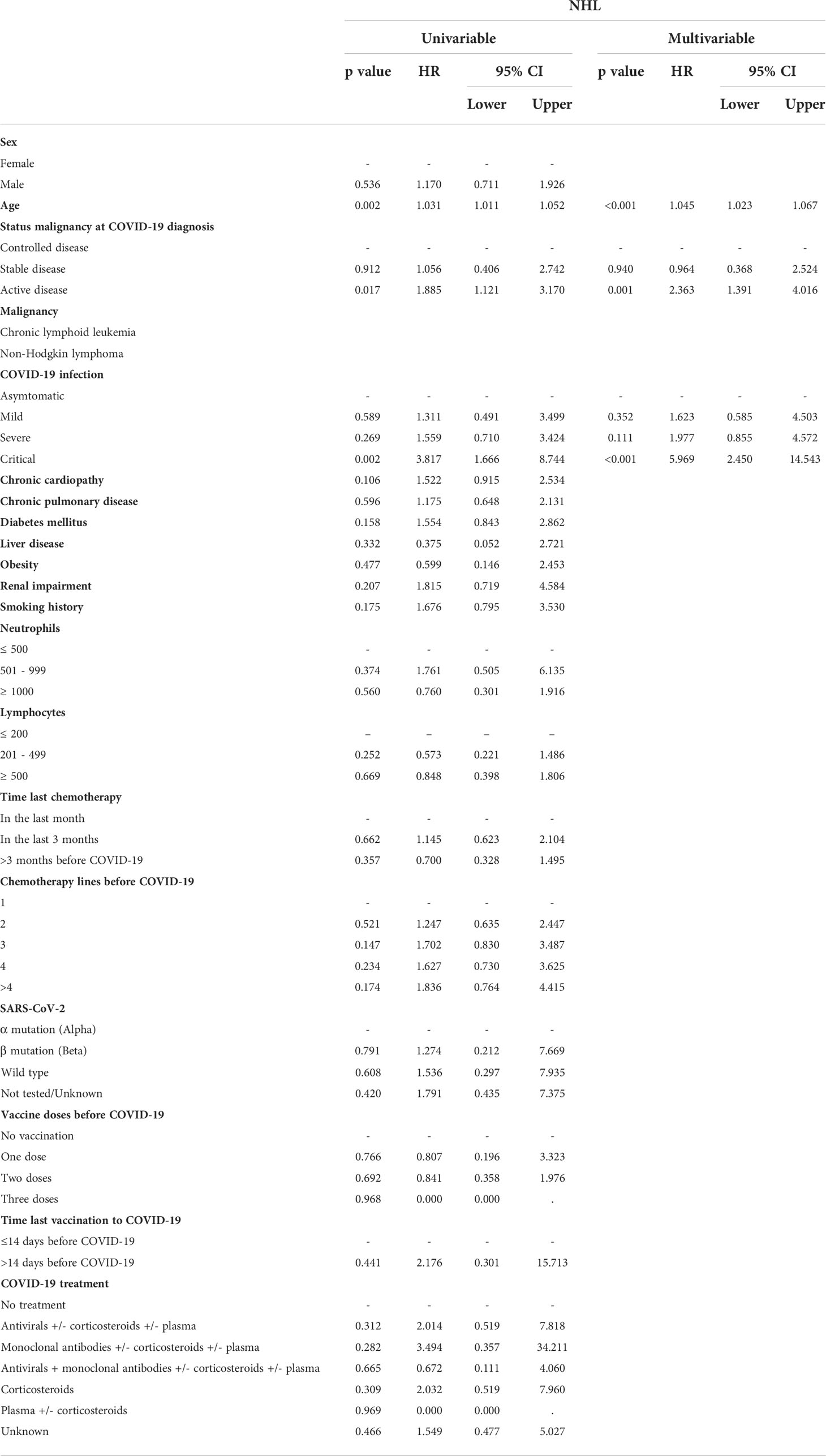
Table 4C Univariable and multivariable analysis of predictors of mortality in the NHL patients.
By multivariable analysis, age >75 years (hazard ratio [HR] 1.036, 95% confidence interval [CI] 1.019-1.052, p<0.001), active hematological malignancy (HR 2.215, 95% CI 1.501-3.267, p<0.001), severe COVID-19 disease (HR 2.270, 95% CI 1.156-4.460 p=0.017) and critical COVID-19 disease (HR 5.751, 95% CI 2.875-11.506, p<0.001) remained as risk factors for mortality in the entire cohort. All factors remained significant for NHL, while in CLL patients all but active malignancy was significant.
There was no difference in OS in NHL vs CLL patients (p=0.344), in BKIs vs no BKIs-treated patients (p=0.137), nor when comparing patients treated with different targeted drugs (p=0.343) (Figure 4). We did not observe a clear protective or detrimental effect of BKIs on the outcome when compared with other targeted drugs.
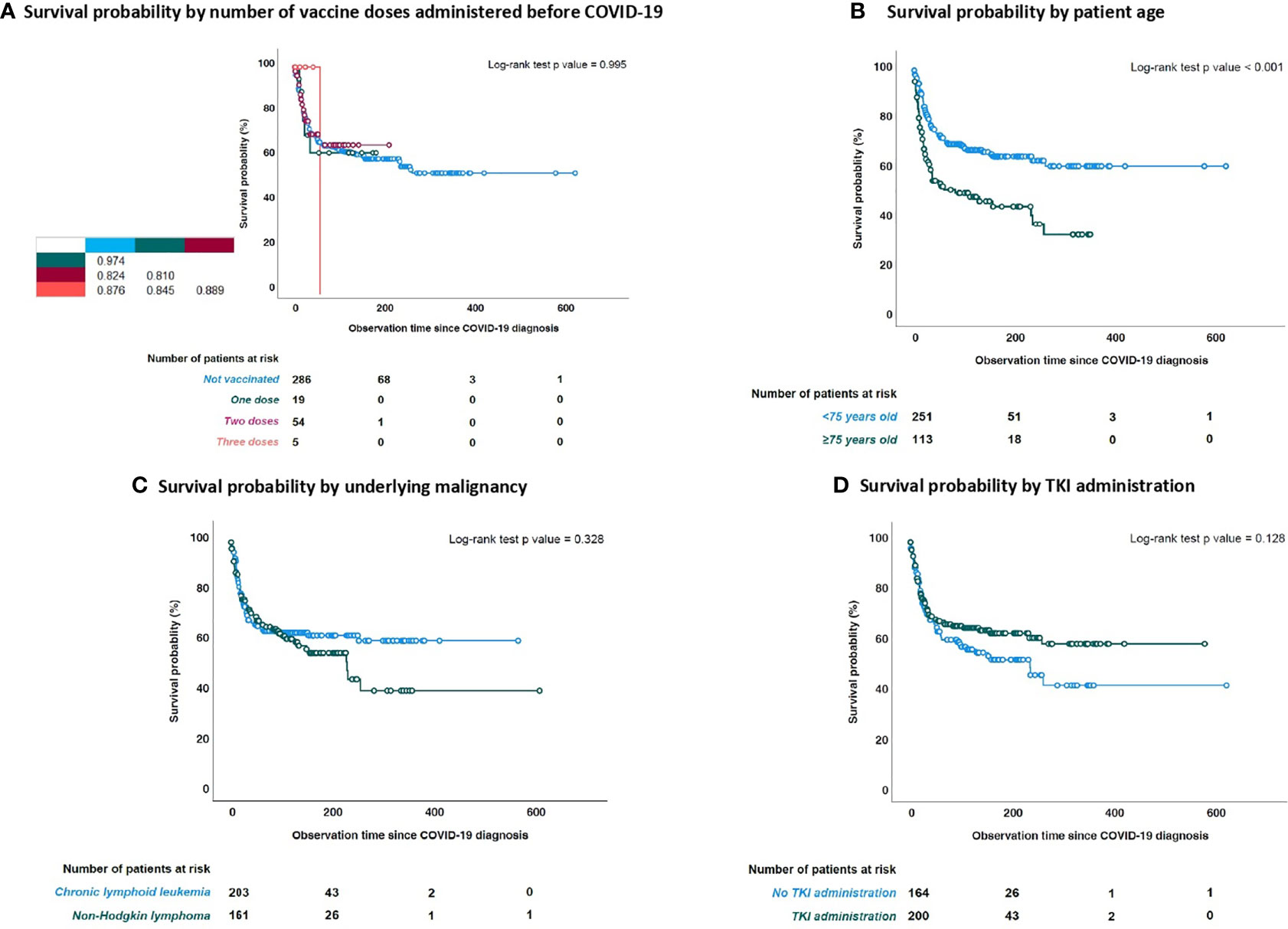
Figure 4 Survival probability (SP) from time of COVID-19 diagnosis stratified by number of vaccine doses, age, underlying malignancy and use of BKi at time of COVID-19 diagnosis. (A) SP stratified by number of vaccine doses administered; (B) SP stratified by age; (C) SP by underlying malignancy; (D) SP by BKi status.
To the best of our knowledge, we describe a large international series of LPD patients receiving targeted drug treatment at the time of COVID-19 infection. The rates of severe infection and overall mortality were 47.5% and 36.6%, respectively. The presence of comorbidities and lack of vaccination were associated with higher mortality rate. Prior vaccination was a protective factor. There were no significant differences in mortality across different targeted drugs. Patients treated with targeted chemotherapy were matched to controls treated with any other strategy for hematological malignancy before COVID-19. Cases and controls were matched in age, sex, hematological malignancy, malignancy status at COVID-19 and time of last chemotherapy strategy before COVID-19 (<3 months or >3 months). No statistically significant differences were observed in mortality probability between groups (p=0.056).
Patients with hematological malignancy have been heavily hit by the COVID-19 pandemic, and several reports confirm high rates of severe disease and mortality (2–4). Patients with B-malignancies have been particularly affected due to their intrinsic immune dysregulation (30, 31, 37–39). Moreover, the potential impact of LPD targeted therapies on the course of COVID-19 still needs to be fully understood.
The high mortality rates in our series appear similar to that of other series of hematological patients with COVID-19 infection (30, 31, 40–42). Surprisingly, despite the number of asymptomatic patients included in our study (diagnosed through screening for COVID-19) the rates of hospital admission and ICU admission were high. This data suggests that our cohort is at high risk of severe/critical COVID-19 when admitted to the hospital for symptomatic COVID-19.
Vaccination reduced mortality in our series, even after only 2 doses. Doubts have been raised about the efficacy of vaccination in patients with altered B cell immunity. Specifically in patients treated with anti-CD20, BKIs, or venetoclax, data demonstrating seroconversion failure after COVID-19 vaccination have been published (43, 44). Despite the lack of seroprevalence data in our series, we do consider that the COVID vaccines were a protective prognostic factor against mortality in these patients as mortality rates decreased as their vaccination status was increasing.
The mortality rate has decreased across the different COVID-19 waves, possibly reflecting improvements in patients care and the development of COVID-19 treatments: while we did not specifically examine COVID-19 treatment in our cohort, we can speculate that the early initiation of corticosteroids, heparin and the introduction of tocilizumab in the management of these patients might have improved the outcome. At the beginning of the pandemic, there was some reluctance about the use of corticosteroids and tocilizumab in hematological patients, due to the fear of stressing their immunodepression. Over time, the early initiation of those therapies was beneficial in those patients as well as the general population.
In our study, we did not find any association between specific targeted drugs and mortality. The majority of patients in our cohort were treated with BKIs. In the initial phase of the pandemic, some data suggested that BKIs could modulate the immune response to COVID-19 infection through blockade of inflammatory cytokines in the lungs, with a reduction of hyperinflammatory response (45, 46). The widespread use of early dexamethasone treatment in patients with severe COVID-19, based on the RECOVERY trial (47), achieved a more effective suppression of the host humoral response through the downregulation of proinflammatory cytokine production. We did not find significant differences in OS among patients treated or not with BKIs, independently from the time of the initiation of the drug, nor in the most prevalent cohorts of targeted patients after BKIs: BCL2-inhibitors and anti- CD20. In addition, due to the limited number of patients treated with other therapies, we cannot draw any conclusion about their role in this asset.
In the present series, age >75 years, severe and critical COVID-19 infection, and active hematological disease were independent predictors of mortality. This is consistent with recent data from the EPICOVIDEHA (36) survey that described, in addition to those, other risk factors for mortality such as chronic cardiac disease, liver disease, renal impairment, smoking history, and ICU stay in a cohort of patients with various hematological malignancies. Description of risk factors in hematological patients is of great importance to identify patients at high risk and implement rapidly prophylactic measures such as vaccination, masking, social distancing, and antiCOVID19 specific prevention and treatment.
Limitations of our study include its retrospective design, which implies dependence on the accuracy of medical records, and possible selection bias. The heterogeneity of underlying diseases and drug exposure could be another limitation, as a confounding factor for infection risk in this series. We could not perform a direct comparison between targeted drug-treated patients and chemotherapy patients as those groups would be too heterogeneous to compare.
Another limitation is the lack of patients from the latest waves infected with the delta and omicron variants and an analysis to determine if the new vaccine boosters can continue to reduce mortality in those patients. Specifically, patients treated with anti-CD20, BTKi, and BCL2-inhibitors were seroconversion failure after COVID-19 vaccination have been described, could be considered to receive early treatment with antivirals and monoclonal antibodies (48–50) or pre-exposure prophylaxis (51).
We acknowledge the potential underscoring of the real incidence of COVID-19 in this population, as we included asymptomatic patients with positive screening for COVID-19 while we must account for several asymptomatic patients not tested and therefore not diagnosed.
Our contribution is the largest international multicentric series of LPD patients under targeted drug treatment with COVID-19 infection, with a long follow-up, providing real-world evidence for increased severe disease and mortality from COVID-19 in patients with LPD treated with targeted drugs. Targeted drugs do not seem to have an impact on the survival of these patients. Efforts to prevent and aggressively manage COVID-19 should be focused on patients at a high risk of developing COVID-19 complications such as those older than 75 years, with comorbidities, especially heart disease, and active malignancy at COVID-19 onset. The importance of vaccination should be stressed, even in this population with humoral immunity impairment where it was a protective factor for mortality. New insights into the management of the infection throughout the pandemic and the development of COVID-19 treatments showed benefits in this particularly vulnerable population.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The EPICOVIDEHA study has been approved by the local Institutional Review Board and Ethics Committee of the Fondazione Policlinico Universitario Agostino Gemelli— IRCCS, Università Cattolica del Sacro Cuore of Rome, Italy (Study ID: 3226). The corresponding local ethics committee of each participating institution may approve additionally the EPICOVIDEHA study when applicable. EPICOVIDEHA is registered at http://www.clinicaltrials.gov, with the identifier (NCT number): NCT 04733729. The patients/participants provided their written informed consent to participate in this study.
MI, JS-G and AF-C contributed to the study conception and design. All authors contributed to data collection. Material preparation and analysis were performed by JS-G. The first draft of the manuscript was written by MI and JS-G and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
EPICOVIDEHA has received funds from Optics COMMITTM (COVID-19 Unmet Medical Needs and Associated Research Extension) COVID-19 RFP program by GILEAD Science, United States (Project 2020-8223).
We would like to thank the following: Pavel Žák Guillemette Fouquet, Francesca Farina, Fatih Demirkan, Laman Rahimli, Christian Bjørn Poulsen, Malgorzata Mikulska, Sandra Malak, Jorge Labrador, Moraima Jiḿenez, Stefanie Gräfe, Maria Chiara Tisi, Noemí Fernaandez, Ľuboš Drgona, Rui Bergantim, Laura Serrano, Jög Schubert, Giuseppe Sapienza, Juergen Prattes, Irati Ormazabal-Vélez, Marcio Nucci, Lisset Lorenzo De La Peña, Alexandra Serris, Carolina Garćia-Vidal, Nicola Fracchiolla, Nurettin Erben, Giulia Dragonetti, Roberta Di Blasi, Martin Cernan, Elena Busch, Monika M. Biernat, Murtadha Al-Khabori, Florian Reizine, Natasha Ali, Verena Petzer, Maria Merelli, Johan Maertens, Nina Khanna, Tomás-José González-López.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest of this work.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
BKIs, Bruton tyrosine-kinase inhibitors; CLL, chronic lymphocytic leukemia; COVID19 Coronavirus disease 2019; CMV, cytomegalovirus; HR, hazard ratio; IMiDs, immunomodulatory drugs; ICU, intensive care unit; IQR, Interquartile Range; LPD, lymphoproliferative diseases; NHL, non-Hodgkin lymphoma; OS, overall survival; PIK3, phosphoinositide 3-kinase; RT-PCR, reverse transcriptase-polymerase chain reaction; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; RB, rituximab-bendamustine.
1. Guan W-J, Ni Z-Y, Hu Y, Liang W-H, Ou C-Q, He J-X, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
2. Vijenthira A, Gong IY, Fox TA, Booth S, Cook G, Fattizzo B, et al. Outcomes of patients with hematologic malignancies and COVID-19: a systematic review and meta-analysis of 3377 patients. Blood (2020) 136:2881–92. doi: 10.1182/blood.2020008824
3. Wood WA, Neuberg DS, Thompson JC, Tallman MS, Sekeres MA, Sehn LH, et al. Outcomes of patients with hematologic malignancies and COVID-19: a report from the ASH research collaborative data hub. Blood Adv (2020) 4:5966–75. doi: 10.1182/bloodadvances.2020003170
4. Yigenoglu TN, Ata N, Altuntas F, Bascı S, Dal MS, Korkmaz S, et al. The outcome of COVID-19 in patients with hematological malignancy. J Med Virol (2021) 93:1099–104. doi: 10.1002/jmv.26404
5. Moreira J, Rabe KG, Cerhan JR, Kay NE, Wilson JW, Call TG, et al. Infectious complications among individuals with clinical monoclonal b-cell lymphocytosis (MBL): a cohort study of newly diagnosed cases compared to controls. Leukemia (2013) 27:136–41. doi: 10.1038/leu.2012.187
6. Law N, Taplitz RA. How I manage infection risk and prevention in patients with lymphoid cancer. Blood (2022) 139:1517–28. doi: 10.1182/blood.2019003687
7. Ochoa-Grullón J, Peña Cortijo A, Guevara-Hoyer K, Jiménez García C, de la Fuente E, de la Peña AR, et al. B-cell haematological malignancies and SARS-CoV-2 infection: Could immunological interventions influence the outcome? EJHaem (2021) 2(3):503–7. doi: 10.1002/jha2.249
8. Perry C, Luttwak E, Balaban R, Shefer G, Morales MM, Aharon A, et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with b-cell non-Hodgkin lymphoma. Blood Adv (2021) 5:3053–61. doi: 10.1182/bloodadvances.2021005094
9. Burger JA, Tedeschi A, Barr PM, Robak T, Owen C, Ghia P, et al. Ibrutinib as initial therapy for patients with chronic lymphocytic leukemia. N Engl J Med (2015) 373:2425–37. doi: 10.1056/NEJMoa1509388
10. Shanafelt TD, Wang XV, Kay NE, Hanson CA, O’Brien S, Barrientos J, et al. Ibrutinib-rituximab or chemoimmunotherapy for chronic lymphocytic leukemia. N Engl J Med (2019) 381:432–43. doi: 10.1056/NEJMoa1817073
11. Sharman JP, Egyed M, Jurczak W, Skarbnik A, Pagel JM, Flinn IW, et al. Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzmab for treatment-naive chronic lymphocytic leukaemia (ELEVATE TN): a randomised, controlled, phase 3 trial. Lancet (2020) 395:1278–91. doi: 10.1016/S0140-6736(20)30262-2
12. Al-Sawaf O, Zhang C, Tandon M, Sinha A, Fink A-M, Robrecht S, et al. Venetoclax plus obinutuzumab versus chlorambucil plus obinutuzumab for previously untreated chronic lymphocytic leukaemia (CLL14): follow-up results from a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol (2020) 21:1188–200. doi: 10.1016/S1470-2045(20)30443-5
13. Hiddemann W, Barbui AM, Canales MA, Cannell PK, Collins GP, Dürig J, et al. Immunochemotherapy with obinutuzumab or rituximab for previously untreated follicular lymphoma in the GALLIUM study: Influence of chemotherapy on efficacy and safety. J Clin Oncol (2018) 36:2395–404. doi: 10.1200/JCO.2017.76.8960
14. Dreyling M, Santoro A, Mollica L, Leppä S, Follows G, Lenz G, et al. Long-term safety and efficacy of the PI3K inhibitor copanlisib in patients with relapsed or refractory indolent lymphoma: 2-year follow-up of the CHRONOS-1 study. Am J Hematol (2020) 95:362–71. doi: 10.1002/ajh.25711
15. Flinn IW, Miller CB, Ardeshna KM, Tetreault S, Assouline SE, Mayer J, et al. DYNAMO: A phase II study of duvelisib (IPI-145) in patients with refractory indolent non-Hodgkin lymphoma. J Clin Oncol (2019) 37:912–22. doi: 10.1200/JCO.18.00915
16. Salles G, Schuster SJ, de Vos S, Wagner-Johnston ND, Viardot A, Blum KA, et al. Efficacy and safety of idelalisib in patients with relapsed, rituximab- and alkylating agent-refractory follicular lymphoma: a subgroup analysis of a phase 2 study. Haematologica (2017) 102:e156–9. doi: 10.3324/haematol.2016.151738
17. Morschhauser F, Fowler NH, Feugier P, Bouabdallah R, Tilly H, Palomba ML, et al. Rituximab plus lenalidomide in advanced untreated follicular lymphoma. N Engl J Med (2018) 379:934–47. doi: 10.1056/NEJMoa1805104
18. Straus DJ, Długosz-Danecka M, Alekseev S, Illés Á, Picardi M, Lech-Maranda E, et al. Brentuximab vedotin with chemotherapy for stage III/IV classical Hodgkin lymphoma: 3-year update of the ECHELON-1 study. Blood (2020) 135:735–42. doi: 10.1182/blood.2019003127
19. Ansell SM, Lesokhin AM, Borrello I, Halwani A, Scott EC, Gutierrez M, et al. PD-1 blockade with nivolumab in relapsed or refractory hodgkin’s lymphoma. N Engl J Med (2015) 372:311–9. doi: 10.1056/NEJMoa1411087
20. Sehn LH, Herrera AF, Flowers CR, Kamdar MK, McMillan A, Hertzberg M, et al. Polatuzumab vedotin in relapsed or refractory diffuse Large b-cell lymphoma. J Clin Oncol (2020) 38:155–65. doi: 10.1200/JCO.19.00172
21. Rogers KA, Mousa L, Zhao Q, Bhat SA, Byrd JC, Boghdadly ZE, et al. Incidence of opportunistic infections during ibrutinib treatment for b-cell malignancies. Leukemia (2019) 33:2527–30. doi: 10.1038/s41375-019-0481-1
22. Zinzani PL, Rambaldi A, Gaidano G, Girmenia C, Marchetti M, Pane F, et al. Infection control in patients treated for chronic lymphocytic leukemia with ibrutinib or idelalisib: recommendations from Italian society of hematology. Leuk Res (2019) 81:88–94. doi: 10.1016/j.leukres.2019.04.016
23. Teh BW, Tam CS, Handunnetti S, Worth LJ, Slavin MA. Infections in patients with chronic lymphocytic leukaemia: Mitigating risk in the era of targeted therapies. Blood Rev (2018) 32:499–507. doi: 10.1016/j.blre.2018.04.007
24. Stefania Infante M, Fernández-Cruz A, Núñez L, Carpio C, Jiménez-Ubieto A, López-Jiménez J, et al. Severe infections in patients with lymphoproliferative diseases treated with new targeted drugs: A multicentric real-world study. Cancer Med (2021) 10(21):7629–40. doi: 10.1002/cam4.4293
25. Drgona L, Gudiol C, Lanini S, Salzberger B, Ippolito G, Mikulska M. ESCMID study group for infections in compromised hosts (ESGICH) consensus document on the safety of targeted and biological therapies: an infectious diseases perspective (Agents targeting lymphoid or myeloid cells surface antigens [II]: CD22, CD30, CD33, CD38, CD40, SLAMF-7 and CCR4). Clin Microbiol Infect (2018) 24 Suppl 2:S83–94. doi: 10.1016/j.cmi.2018.03.022
26. Connors JM, Jurczak W, Straus DJ, Ansell SM, Kim WS, Gallamini A, et al. Brentuximab vedotin with chemotherapy for stage III or IV hodgkin’s lymphoma. N Engl J Med (2018) 378:331–44. doi: 10.1056/NEJMoa1708984
27. Herishanu Y, Rahav G, Levi S, Braester A, Itchaki G, Bairey O, et al. Efficacy of a third BNT162b2 mRNA COVID-19 vaccine dose in patients with CLL who failed standard 2-dose vaccination. Blood (2022) 139:678–85. doi: 10.1182/blood.2021014085
28. Parry H, McIlroy G, Bruton R, Ali M, Stephens C, Damery S, et al. Antibody responses after first and second covid-19 vaccination in patients with chronic lymphocytic leukaemia. Blood Cancer J (2021) 11:136. doi: 10.1038/s41408-021-00528-x
29. Shen Y, Freeman JA, Holland J, Solterbeck A, Naidu K, Soosapilla A, et al. COVID-19 vaccine failure in chronic lymphocytic leukaemia and monoclonal b-lymphocytosis; humoural and cellular immunity. Br J Haematol (2021) 197(1):41–51. doi: 10.1111/bjh.18014
30. Mato AR, Roeker LE, Lamanna N, Allan JN, Leslie L, Pagel JM, et al. Outcomes of COVID-19 in patients with CLL: a multicenter international experience. Blood (2020) 136:1134–43. doi: 10.1182/blood.2020006965
31. Scarfò L, Chatzikonstantinou T, Rigolin GM, Quaresmini G, Motta M, Vitale C, et al. COVID-19 severity and mortality in patients with chronic lymphocytic leukemia: a joint study by ERIC, the European research initiative on CLL, and CLL campus. Leukemia (2020) 34:2354–63. doi: 10.1038/s41375-020-0959-x
32. Thibaud S, Tremblay D, Bhalla S, Zimmerman B, Sigel K, Gabrilove J. Protective role of bruton tyrosine kinase inhibitors in patients with chronic lymphocytic leukaemia and COVID-19. Br J Haematol (2020) 190:e73–6. doi: 10.1111/bjh.16863
33. Treon SP, Castillo JJ, Skarbnik AP, Soumerai JD, Ghobrial IM, Guerrera ML, et al. The BTK inhibitor ibrutinib may protect against pulmonary injury in COVID-19-infected patients. Blood (2020) 135:1912–5. doi: 10.1182/blood.2020006288
34. Coutre SE, Barnett C, Osiyemi O, Hoda D, Ramgopal M, Fort AC, et al. Ibrutinib for hospitalized adults with severe COVID-19 infection: Results of the randomized, double-blind, placebo-controlled iNSPIRE study. Open Forum Infect Dis (2022) 9(5):ofac104. doi: 10.1093/ofid/ofac104
35. Salmanton-García J, Busca A, Cornely OA, Corradini P, Hoenigl M, Klimko N, et al. EPICOVIDEHA: A ready to use platform for epidemiological studies in hematological patients with COVID-19. Hemasphere (2021) 5:e612. doi: 10.1097/HS9.0000000000000612
36. Pagano L, Salmanton-García J, Marchesi F, Busca A, Corradini P, Hoenigl M, et al. COVID-19 infection in adult patients with hematological malignancies: a European hematology association survey (EPICOVIDEHA). J Hematol Oncol (2021) 14:168. doi: 10.1186/s13045-021-01177-0
37. Langerbeins P, Eichhorst B. Immune dysfunction in patients with chronic lymphocytic leukemia and challenges during COVID-19 pandemic. Acta Haematol (2021) 144:508–18. doi: 10.1159/000514071
38. Roeker LE, Eyre TA, Thompson MC, Lamanna N, Coltoff AR, Davids MS, et al. COVID-19 in patients with CLL: improved survival outcomes and update on management strategies. Blood (2021) 138:1768–73. doi: 10.1182/blood.2021011841
39. Chatzikonstantinou T, Kapetanakis A, Scarfò L, Karakatsoulis G, Allsup D, Cabrero AA, et al. COVID-19 severity and mortality in patients with CLL: an update of the international ERIC and campus CLL study. Leukemia (2021) 35:3444–54. doi: 10.1038/s41375-021-01450-8
40. Infante M-S, González-Gascón Y Marín I, Muñoz-Novas C, Churruca J, Foncillas M-Á, Landete E, et al. COVID-19 in patients with hematological malignancies: A retrospective case series. Int J Lab Hematol (2020) 42:e256–9. doi: 10.1111/ijlh.13301
41. Malard F, Genthon A, Brissot E, van de Wyngaert Z, Marjanovic Z, Ikhlef S, et al. COVID-19 outcomes in patients with hematologic disease. Bone Marrow Transplant (2020) 55(11):2180–4. doi: 10.1038/s41409-020-0931-4
42. Martín-Moro F, Marquet J, Piris M, Michael BM, Sáez AJ, Corona M, et al. Survival study of hospitalized patients with concurrent covid-19 and haematological malignancies. Br J Haematol 190(1):e16–e20. doi: 10.1111/bjh.16801
43. Ghione P, Gu JJ, Attwood K, Torka P, Goel S, Sundaram S, et al. Impaired humoral responses to COVID-19 vaccination in patients with lymphoma receiving b-cell-directed therapies. Blood (2021) 138:811–4. doi: 10.1182/blood.2021012443
44. Passamonti F, Romano A, Salvini M, Merli F, Porta MGD, Bruna R, et al. COVID-19 elicits an impaired antibody response against SARS-CoV-2 in patients with haematological malignancies. Br J Haematol (2021) 195:371–7. doi: 10.1111/bjh.17704
45. Jacobs CF, Eldering E, Kater AP. Kinase inhibitors developed for treatment of hematologic malignancies: implications for immune modulation in COVID-19. Blood Adv (2021) 5:913–25. doi: 10.1182/bloodadvances.2020003768
46. Rezaei M, Barati S, Babamahmoodi A, Dastan F, Marjani M. The possible role of bruton tyrosine kinase inhibitors in the treatment of COVID-19: A review. Curr Ther Res Clin Exp (2022) 96:100658. doi: 10.1016/j.curtheres.2021.100658
47. The RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with covid-19. N Engl J Med (2021) 384:693–704. doi: 10.1056/NEJMoa2021436
48. Cruz-Teran C, Tiruthani K, McSweeney M, Ma A, Pickles R, Lai SK. Challenges and opportunities for antiviral monoclonal antibodies as COVID-19 therapy. Adv Drug Delivery Rev (2021) 169:100–17. doi: 10.1016/j.addr.2020.12.004
49. Zhang J, Zhang H, Sun L. Therapeutic antibodies for COVID-19: is a new age of IgM, IgA and bispecific antibodies coming? MAbs (2022) 14:2031483. doi: 10.1080/19420862.2022.2031483
50. Gaborit B, Vanhove B, Vibet M-A, Le Thuaut A, Lacombe K, Dubee V, et al. Evaluation of the safety and efficacy of XAV-19 in patients with COVID-19-induced moderate pneumonia: study protocol for a randomized, double-blinded, placebo-controlled phase 2 (2a and 2b) trial. Trials (2021) 22:199. doi: 10.1186/s13063-021-05132-9
Keywords: SARS-CoV-2, targeted drugs, infection risk, immune system COVID19, lymphoproliferative diseases (LPD), chronic lymphocytic leukemia (CLL), non-Hodgkin lymphoma (NHL)
Citation: Infante MS, Salmanton-García J, Fernández-Cruz A, Marchesi F, Jaksic O, Weinbergerová B, Besson C, Duarte RF, Itri F, Valković T, Szotkovski T, Busca A, Guidetti A, Glenthøj A, Collins GP, Bonuomo V, Sili U, Seval GC, Machado M, Cordoba R, Blennow O, Abu-Zeinah G, Lamure S, Kulasekararaj A, Falces-Romero I, Cattaneo C, Van Doesum J, Piukovics K, Omrani AS, Magliano G, Ledoux M-P, de Ramon C, Cabirta A, Verga L, López-García A, Da Silva MG, Stojanoski Z, Meers S, Lahmer T, Martín-Pérez S, Dávila-Vals J, Van Praet J, Samarkos M, Bilgin YM, Karlsson LK, Batinić J, Nordlander A, Schönlein M, Hoenigl M, Ráčil Z, Mladenović M, Hanakova M, Zambrotta GPM, De Jonge N, Adžić-Vukičević T, Nunes-Rodrigues R, Prezioso L, Navrátil M, Marchetti M, Cuccaro A, Calbacho M, Giordano A, Cornely OA, Hernández-Rivas J-Á and Pagano L (2022) B-cell malignancies treated with targeted drugs and SARS-CoV-2 infection: A European Hematology Association Survey (EPICOVIDEHA). Front. Oncol. 12:992137. doi: 10.3389/fonc.2022.992137
Received: 12 July 2022; Accepted: 31 August 2022;
Published: 04 October 2022.
Edited by:
Mohamed A. Yassin, Hamad Medical Corporation, QatarReviewed by:
Mervat Mattar, Cairo University, EgyptCopyright © 2022 Infante, Salmanton-García, Fernández-Cruz, Marchesi, Jaksic, Weinbergerová, Besson, Duarte, Itri, Valković, Szotkovski, Busca, Guidetti, Glenthøj, Collins, Bonuomo, Sili, Seval, Machado, Cordoba, Blennow, Abu-Zeinah, Lamure, Kulasekararaj, Falces-Romero, Cattaneo, Van Doesum, Piukovics, Omrani, Magliano, Ledoux, de Ramon, Cabirta, Verga, López-García, Da Silva, Stojanoski, Meers, Lahmer, Martín-Pérez, Dávila-Vals, Van Praet, Samarkos, Bilgin, Karlsson, Batinić, Nordlander, Schönlein, Hoenigl, Ráčil, Mladenović, Hanakova, Zambrotta, De Jonge, Adžić-Vukičević, Nunes-Rodrigues, Prezioso, Navrátil, Marchetti, Cuccaro, Calbacho, Giordano, Cornely, Hernández-Rivas and Pagano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jon Salmanton-García, am9uLnNhbG1hbnRvbi1nYXJjaWFAdWsta29lbG4uZGU=
†These authors have contributed equally to this work
‡These authors have contributed equally to this work and share senior authorship
§ORCID: Maria Stefania Infante, orcid.org/0000-0003-0096-9359
Jon Salmanton-García, orcid.org/0000-0002-6766-8297
Ana Fernández-Cruz, orcid.org/0000-0003-1189-1120
Francesco Marchesi, orcid.org/0000-0001-6353-2272
Ozren Jaksic, orcid.org/0000-0003-4026-285X
Barbora Weinbergerová, orcid.org/0000-0001-6460-2471
Caroline Besson, orcid.org/0000-0003-4364-7173
Federico Itri, orcid.org/0000-0002-3532-5281
Toni Valković, orcid.org/0000-0001-6083-8815
Alessandro Busca, orcid.org/0000-0001-5361-5613
Anna Guidetti, orcid.org/0000-0002-9186-1353
Andreas Glenthøj, orcid.org/0000-0003-2082-0738
Valentina Bonuomo, orcid.org/0000-0001-6491-8337
Uluhan Sili, orcid.org/0000-0002-9939-9298
Guldane Cengiz Seval, orcid.org/0000-0001-9433-2054
Marina Machado, orcid.org/0000-0002-8370-2248
Raul Cordoba, orcid.org/0000-0002-7654-8836
Ola Blennow, orcid.org/0000-0002-7167-7882
Ghaith Abu-Zeinah, orcid.org/0000-0002-1881-3670
Sylvain Lamure, orcid.org/0000-0001-5980-305X
Austin Kulasekararaj, orcid.org/0000-0003-3180-3570
Iker Falces-Romero, orcid.org/0000-0001-5888-7706
Chiara Cattaneo, orcid.org/0000-0003-0031-3237
Jaap Van Doesum, orcid.org/0000-0003-0214-3219
Klára Piukovics, orcid.org/0000-0003-4480-3131
Ali S. Omrani, orcid.org/0000-0001-5309-6358
Gabriele Magliano, orcid.org/0000-0002-9129-1530
Marie-Pierre Ledoux, orcid.org/0000-0002-3261-3616
Cristina De Ramón-Sánchez, orcid.org/0000-0002-8167-6410
Alba Cabirta, orcid.org/0000-0001-7198-8894
Luisa Verga, orcid.org/0000-0003-1142-8435
Alberto López-García, orcid.org/0000-0002-5354-5261
Maria Gomes Da Silva, orcid.org/0000-0002-6993-2450
Zlate Stojanoski, orcid.org/0000-0001-7502-8356
Jens Van Praet, orcid.org/0000-0002-7125-7001
Yavuz M. Bilgin, orcid.org/0000-0003-4854-5424
Martin Schönlein, orcid.org/0000-0002-1010-0975
Martin Hoenigl, orcid.org/0000-0002-1653-2824
Zdeněk Ráčil, orcid.org/0000-0003-3511-4596
Nick De Jonge, orcid.org/0000-0002-9901-0887
Lucia Prezioso, orcid.org/0000-0003-1660-4960
Monia Marchetti, orcid.org/0000-0001-7615-0572
Annarosa Cuccaro, orcid.org/0000-0002-0237-1839
Maria Calbacho, orcid.org/0000-0001-8106-4863
Antonio Giordano, orcid.org/0000-0001-7143-6758
Oliver A. Cornely, orcid.org/0000-0001-9599-3137
José-Ángel Hernández-Rivas, orcid.org/0000-0003-4550-757X
Livio Pagano, orcid.org/0000-0001-8287-928X
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.