
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 23 November 2022
Sec. Hematologic Malignancies
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.989984
This article is part of the Research Topic Myeloproliferative Neoplasms: Biology and Treatment View all 11 articles
 Ja Min Byun1†
Ja Min Byun1† Ho Young Kim2†Seung-Hyun Nam3Ho-Jin Shin4Seulki Song5Jinny Park6Sang Hoon Han7Yong Park8Young Jin Yuh9Yeung-Chul Mun10Young Rok Do11Sang Kyun Sohn12Sung Hwa Bae13
Ho Young Kim2†Seung-Hyun Nam3Ho-Jin Shin4Seulki Song5Jinny Park6Sang Hoon Han7Yong Park8Young Jin Yuh9Yeung-Chul Mun10Young Rok Do11Sang Kyun Sohn12Sung Hwa Bae13 Dong-Yeop Shin1*Sung-Soo Yoon1*
Dong-Yeop Shin1*Sung-Soo Yoon1*As the discussion of first-line anagrelide treatment is ongoing, we aimed to prospectively examine the efficacy and safety of anagrelide in cytoreduction therapy-naïve high risk essential thrombocythemia (ET) patients in Korea. Seventy patients from 12 centers were treated with anagrelide monotherapy for up to 8 weeks, followed up until 24 months. At week 8, 50.0% of the patients were able to achieve platelet < 600 x 109/L, and by 12 months, 55/70 (78.6%) patients stayed on anagrelide, and 40.0% patients showed platelet normalization. 14 patients required additional hydroxyurea (HU) for cytoreduction. The median daily dose of needed HU was 500mg (range 250mg – 1500mg). The efficacy was independent of the somatic mutation status. There were 4 thromboembolic events and 7 bleeding events during the follow-up period. The most common adverse events associated with anagrelide use were headache, followed by palpitation/chest discomfort, edema and generalized weakness/fatigue. 7 patients wished to discontinue anagrelide treatment due to adverse events (3 due to headache; 2 due to edema; 1 due to palpitation and 1 due to skin eruption). All in all, first-line anagrelide treatment showed a favorable response with tolerable safety profiles regardless of somatic mutation status.
Essential thrombocythemia (ET) is a type of myeloproliferative neoplasm characterized by abnormal proliferation of megakaryocytes in the bone marrow leading to elevated platelet counts (1). Since ET patients have an almost normal survival, any survival effect of treatment is very difficult to prove. Thus, the goal of ET treatment is reduction of thrombotic and hemorrhagic complications, and platelet reduction to <400 x10 9/L. While cytoreductive therapy with or without low-dose aspirin is the mainstay of thrombosis risk reduction, the optimal choice of a therapeutic agent is less clear. Several agents, including hydroxyurea, anagrelide, and interferon are used for this purpose, but there are only a handful of data directly comparing these agents (2–7). As such, there is a gap in preferred therapeutic agents among the continents: based on the ANAHYDRET study which showed non-inferiority of anagrelide to hydroxyurea (5), anagrelide is used as first-line therapy for high-risk ET patients in Korea. On the other hand, due to concerns about leukemogenesis observed in the EXELS study (6, 8, 9) and conflicting results of PT-1 trial data (7), anagrelide remains a second-line therapy in Europe.
Anagrelide is an amidazoquinazolin derivative, originally developed as an anticoagulation drug, which was shown to have a potent platelet reducing effect (10). It is the only platelet-specific cytoreductive drug known, having no inhibitory effects on red or white cell progenitor proliferation. It reduces platelet production by inhibiting megakaryocyte colony development, thus producing a left-shift in megakaryocyte maturation, reducing megakaryocyte size, and maturation (11). As discussion of anagrelide efficacy and safety is ongoing and a consensus has not been reached, we aimed to prospectively examine the efficacy and safety of anagrelide as cytoreduction therapy-naïve high-risk ET patients in Korea.
This was a multi-center, prospective observation study (ClinicalTrials.gov identifier: NCT03232177). The aim of the study was to examine the efficacy and safety of first-line anagrelide treatment in high-risk Korean ET patients. The primary objective was to determine the percentage of patients who had hematologic response, defined as platelet count < 600 x 10 9/L by week 8 on anagrelide monotherapy. The secondary objectives included (1) platelet normalization rates (platelet < 400 x 109/L) at week 8 and 12 months per European LeukemiaNet guidelines (12) (2); platelet reduction by more than 50% at week 8 and 12 months; (3) anagrelide safety, tolerability and compliance at 12 months. We also evaluated somatic mutation profiles and anagrelide efficacy as an exploratory objective. The interest in mutation profiling was instigated by 2 recent small studies suggesting that anagrelide may be more effective in JAK2 positive patients than CALR positive patients (13, 14). Specifics target sequencing methods are available in Supplementary Materials.
Patients older than 18 years with ET diagnosed according to 2016 WHO classification (1) were screened. Those participants with high-risk ET [age older than 60 years or a history of vascular complications (15–17)] and cytoreductive treatment naïve were invited to participate in the study, regardless of mutational status. Patients with underlying medical conditions requiring active interventions, inadequate organ (cardiac, hepatic, renal, pancreatic) functions, pregnancy, concurrent malignancies, or taking phosphodiesterase III/IV drugs were excluded. The study was conducted according to the Declaration of Helsinki and was approved by the institutional review board (IRB) of each hospital. Informed consent was taken from all patients before participating in any study-related procedure.
From week 1 to week 8, anagrelide monotherapy was required. Patients were started on anagrelide 0.5mg twice a day and after 1-week dose escalation was allowed. From week 9, additional agents for cytoreduction were allowed per attending physician’s discretion. The maximum anagrelide dose allowed was 10mg/day (2.5mg four times a day). Patients were followed up at week 1, week 4, week 8, 3 months, 6 months, 9 months, 12 months, 18 months and 24 months for lab testing and drug compliance monitoring. The adverse events (AE) were assessed according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.03 (available at: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf). The bleeding and thrombotic complications were graded according to International Society on Thrombosis and Hemostasis (ISTH) (18), which are presented in Supplementary Materials in details.
Fisher’s exact test was used for nominal variables, and Mann-Whitney U test was used for continuous variables. For all statistical analyses of effective variables, two-tailed tests were performed. p-values of <0.05 were considered statistically significant. All data were analyzed using the Statistical Package for the Social Sciences software (IBM® SPSS®Statistics, version 25.0).
Table 1 shows the baseline characteristics of all 70 patients (34 males and 36 females) enrolled. The median age at ET diagnosis was 69 years (range 24 – 90), and time to study enrollment from diagnosis was median 13 days. The majority of the patients harbored JAK2V617F mutation (48/69, 68.6%) and there were 13 (18.8%) triple-negative patients. As for the adjunct anticoagulation therapy, 51/70 (72.9%) took aspirin, 14/70 (20.0%) plavix, 2/70 (2.9%) enoxaparin, 2/70 (2.9%) edoxaban and 1/70 (1.4%) dabigatran.
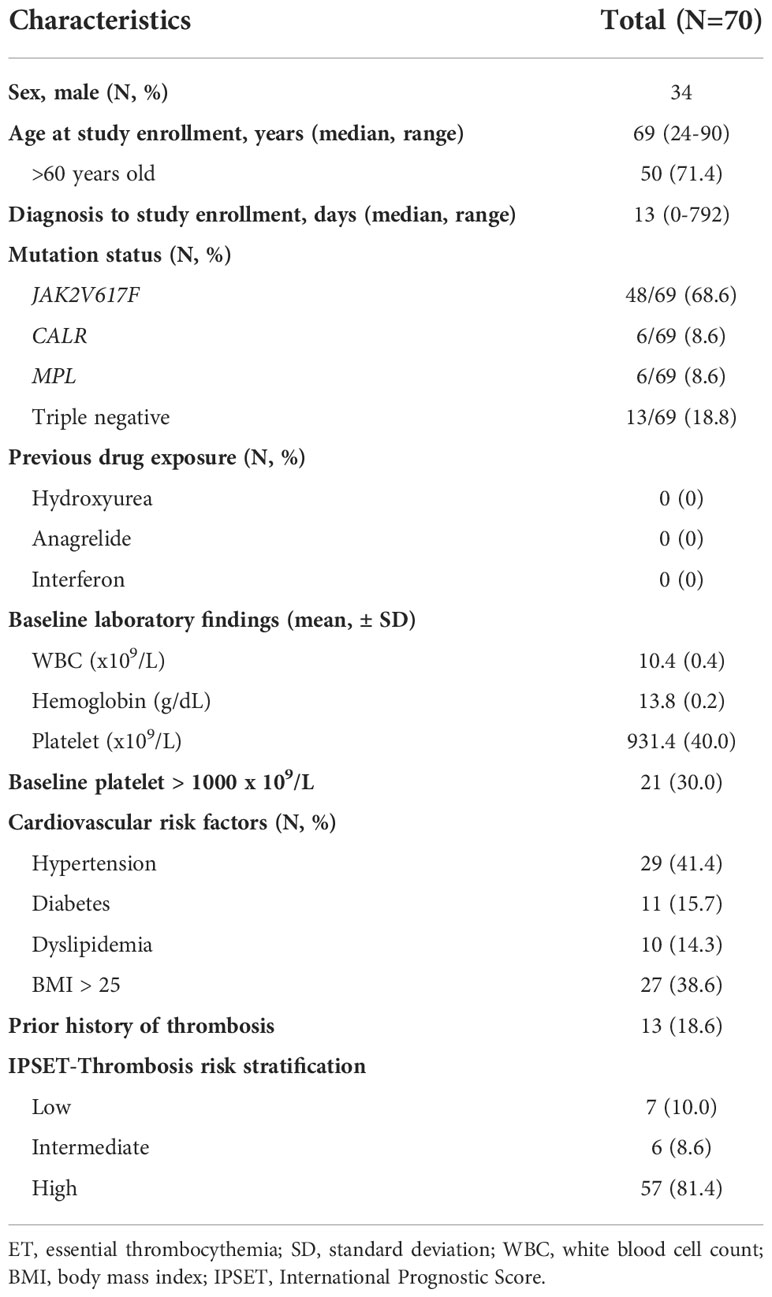
Table 1 Baseline characteristics.
The response was evaluated in the 64 patients who stayed on anagrelide treatment at week 8 (Table 2). Platelet normalization was documented in 20.3% of the patients by week 8, and 40.0% by month 12. Platelet reduction by more than 50% was seen in 18.8% of the patients by week 8, and in 43.6% of the patients by month 12.
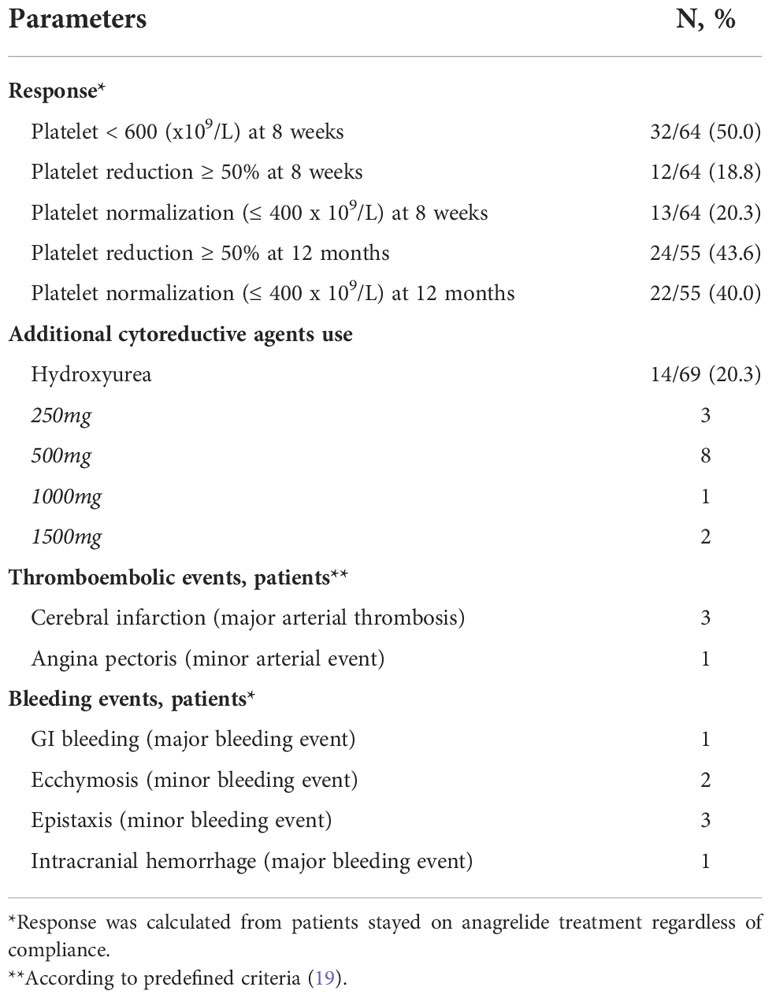
Table 2 Treatment related outcomes.
As shown in Table 2, there were 4 thromboembolic events (20) (3 major arterial thromboses; 1 minor arterial event) and 7 bleeding events (2 major bleeding events; 5 minor bleeding events) during the follow-up period. There were no venous thrombosis/events during the follow-up. One patient with a history of carotid artery stenosis and hepatitis B suffered from an angina pectoris attack requiring intervention. Of the 3 patients who experienced cerebral infarction, one had the previous history of transient ischemic attack, one had a history of thyroid cancer, and one had alcoholic liver cirrhosis. As for the bleeding events, the patient who had intracranial hemorrhage had a history of cerebral infarction and hypertension.
As for tolerability, 64/70 (91.4%) patients remained on anagrelide monotherapy by week 8. Among the 64 patients remaining on anagrelide, all but 1 had taken ≥80% of the prescribed medication. By 12 months, 55/70 (78.6%) patients stayed on anagrelide and 54/55 patients showed good compliance to the drug (Table 3).
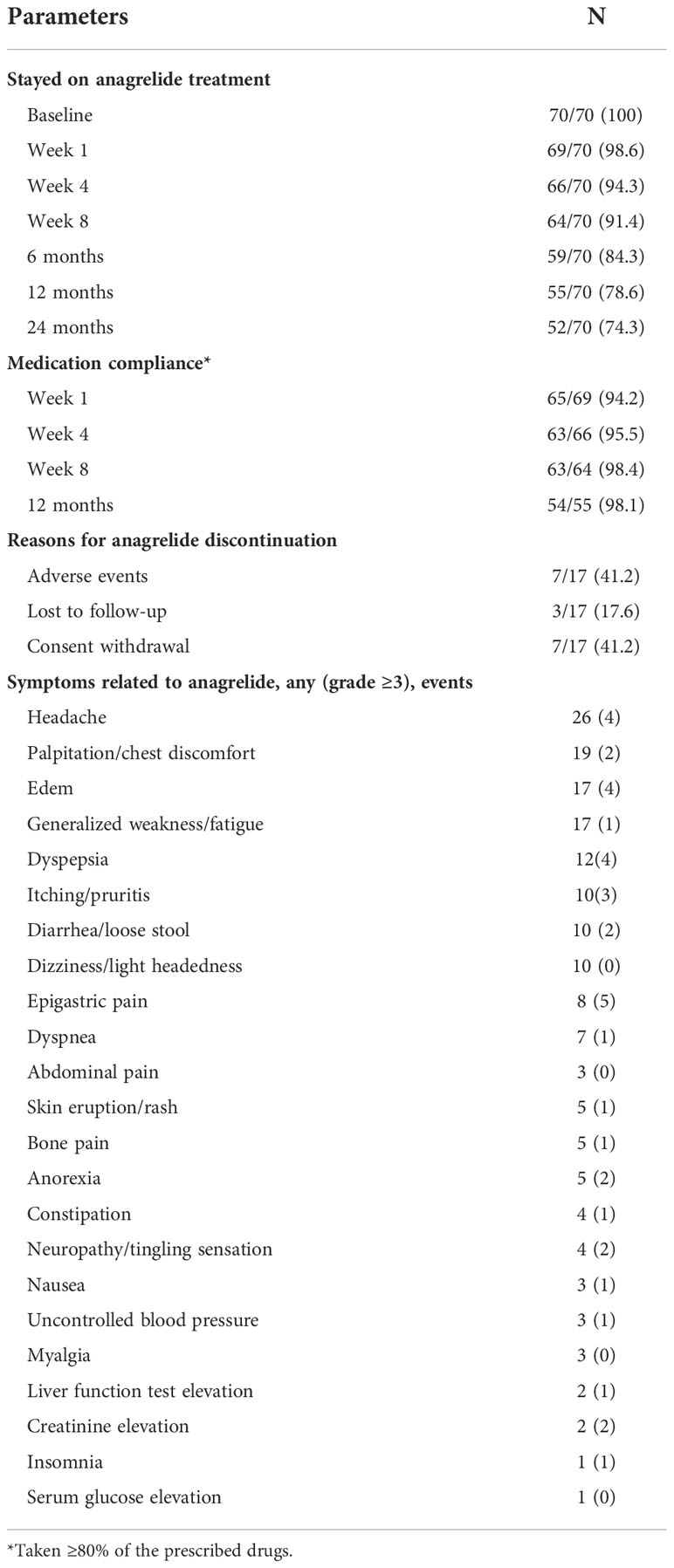
Table 3 Adverse events.
Anagrelide treatment had minimal effects on white blood cell counts and hemoglobin level as shown in Figure 1. The median dose of anagrelide required was 2.5mg per day (Figure 2). Fourteen patients required additional hydroxyurea (HU) for cytoreduction. The median dose of needed HU was 500mg (range, 250mg – 1500mg). Fortunately, there were no differences in adverse events profile among those taking additional hydroxyurea versus those who did not.
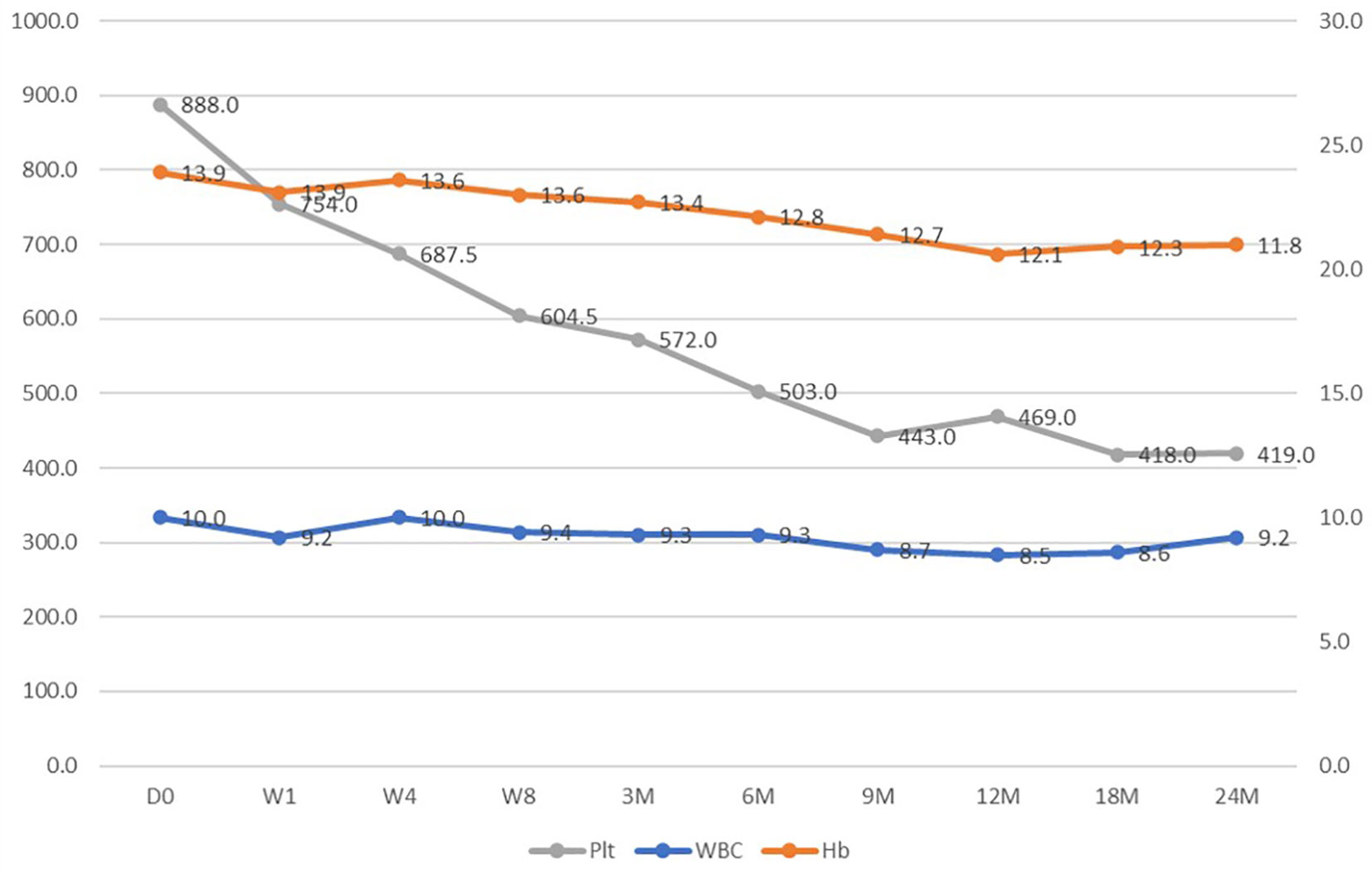
Figure 1 Hemogram changes over the treatment course.
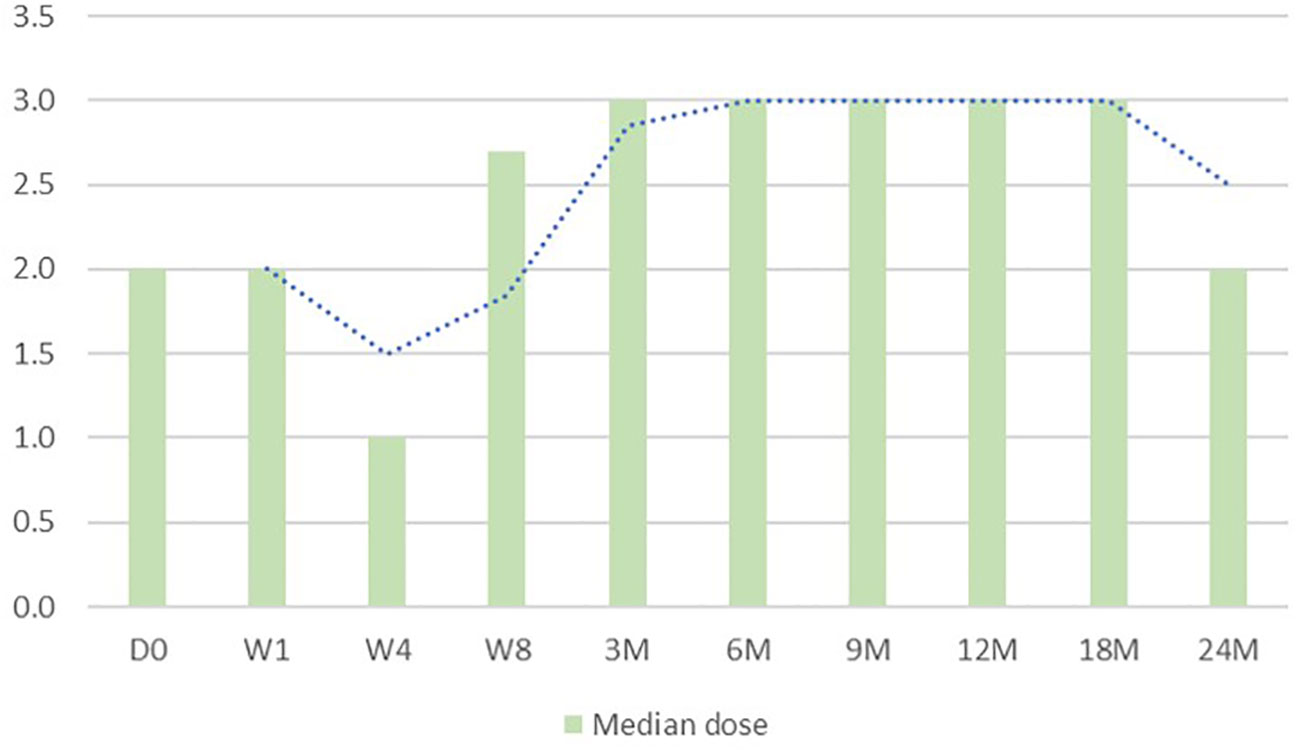
Figure 2 Changes in anagrelide dose over the treatment course.
The most frequent AE associated with anagrelide use was headache, followed by palpitation/chest discomfort, edema and generalized weakness/fatigue. The most common AE ≥ grade 3 was epigastric pain, followed by headache, edema and dyspepsia. 7 patients wished to discontinue anagrelide treatment due to adverse events (3 due to headache; 2 due to edema; 1 due to palpitation and 1 due to skin eruption). There were no acute leukemia transformation or myelofibrosis transformation during the follow-up.
The overall somatic mutational profile is shown in Figure 3. Interestingly, 4 patients showed concurrent JAK2V617F mutation and MPL mutation. There were no patients harboring JAK2 exon 12 mutation. Other than the known driver mutations, ASXL1 was identified in 21/70 (30.0%) patients, followed by TET2 10/70 (9.8%) and KIT 6/70 (8.6%).
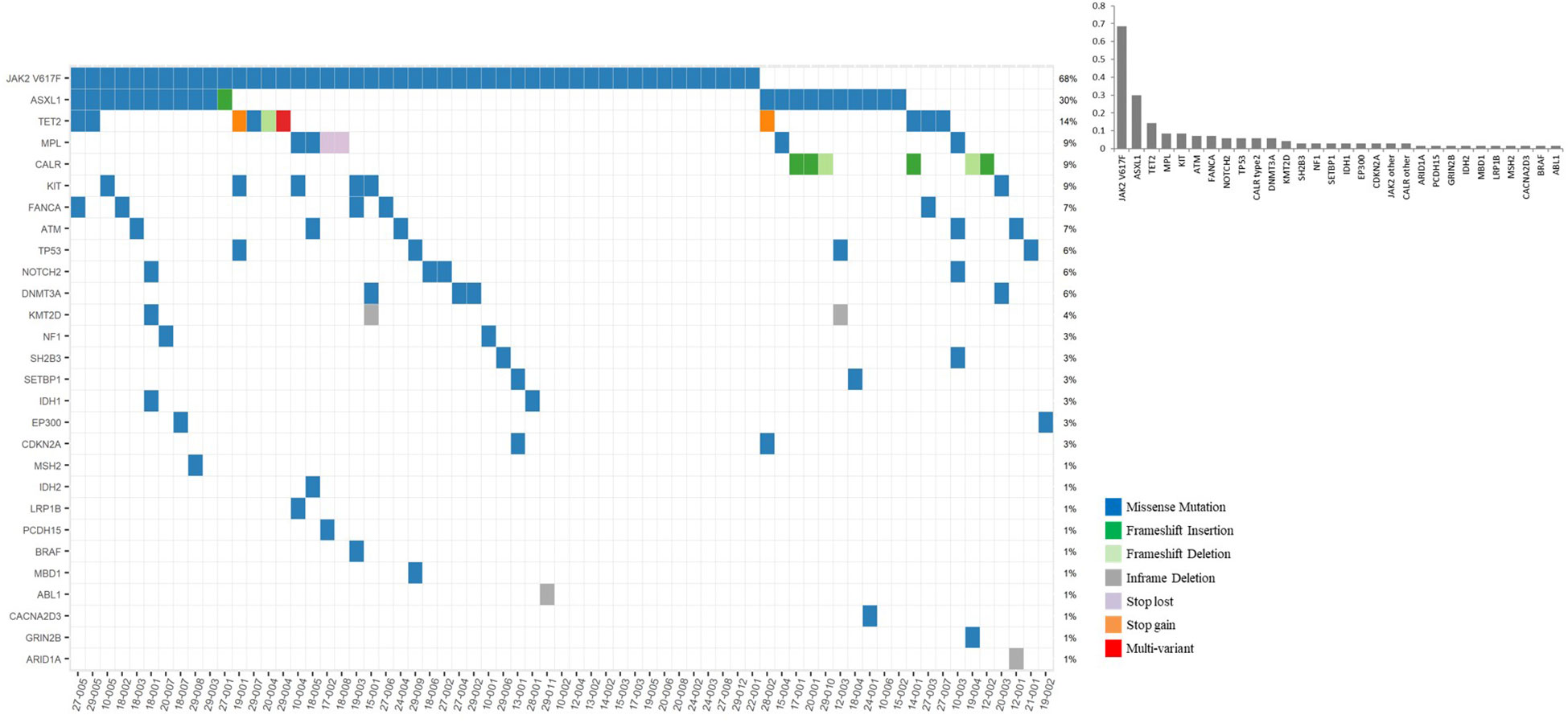
Figure 3 Baseline somatic mutation profiles of essential thrombocythemia patients treated with anagrelide.
Figure 4 shows the mutation status according to treatment efficacy. The mutation status was not related to anagrelide treatment response. More specifically, among patients meeting primary endpoint of platelet count < 600 x 109/L by week 8 74.2% harbored JAK2V617F mutation while 65.6% of the non-responders harbored JAK2V617F mutation (p=0.459). Non-JAK2V617F mutations were noted in 8 responders (25.8%), while 10 (31.3%) non-responders harbored mutations other than JAK2V617F (p=0.438).
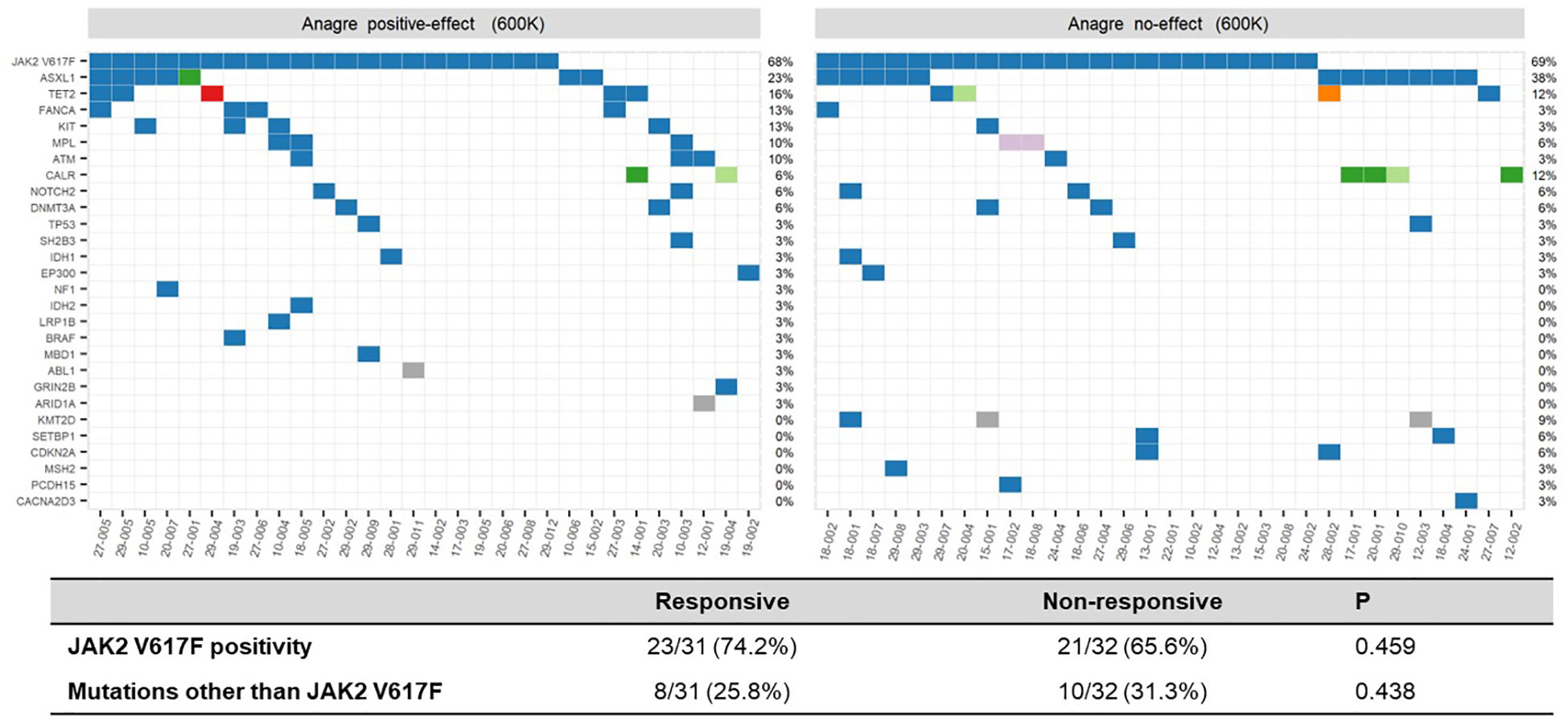
Figure 4 Somatic mutation landscape according to treatment efficacy, patients reaching platelet level < 600 x 109/L versus ≥600 x 109/L at week 8.
In this study, we present the efficacy and safety results of first-line anagrelide treatment for high-risk ET based on prospective clinical data. The importance of our study lies in that 1) this is a rare prospective study using anagrelide as first-line; 2) the efficacy of anagrelide monotherapy was tested, and in relation to genetic background; 3) ethnically homogeneous population with high-risk ET were enrolled. Overall, we report a 50% response rate with anagrelide monotherapy and a 40% complete remission rate at 1 year with 78.6% of the patients staying on the medication with good tolerability.
It is known that approximately 60% of ET patients harbor JAK2V617F mutation (21). Likewise, 68.6% (48/69) of our patients showed JAK2V617F mutation (Figure 1). Although relatively small in number, along with a previous Japanese study reporting JAK2V617F mutation rate at 64.2% for ET (22), there seem to be no ethnical differences in ET mutational profiles. Interestingly, there were only 6 patients (8.6%) harboring CALR mutation. This is probably because our study enrolled only high-risk ET patients defined as older than 60 years old or having a history of vascular complications. It is well-known that CALR-mutated ET patients show higher platelet count and lower thrombotic risk compared to JAK2V617F-positive ET patients (23).
Interestingly, there were 4 patients who harbored both JAK2V617F and MPL mutations. MPL mutations were noncanonical mutation (T374A) in 3 patients, but a canonical mutation in the other one patient (W515L). Somatic mutations in TP53, an important prognostic factor in MPN, was found in 4 patients (5.8%). Another DNA repair gene, ATM mutation was found in 5/69 (7.2%) patients. Longer follow-ups are required to determine the prognostic values of these mutations.
The efficacy of anagrelide, on the other hand, was not determined by mutational status. Half of the enrolled patients achieved platelet level < 600 x 10 9/L by week 8 with anagrelide monotherapy, irrespective of driver mutation status (Table 2; Figure 4; Supplementary Figure). This is numerically lower than the one reported by Ito et al. (22), who reported response rate of 83%. We believe such discrepancy is due to the difference in study schema and study population. At 12 months, regardless of driver mutation status, 40.0% of the patients achieved platelet normalization and 43.6% of the patients saw more than 50% reduction in platelet level from baseline. Since anagrelide is not a specific targeted agent but rather its platelet-reducing effect is mediated through reduction in pro-platelet formation (6, 8), it is understandable that the mutation status does not affect the drug’s efficacy.
The medication was relatively well tolerated: 74.3% of the patients stayed on anagrelide at 24 months with a median dose of 2 mg. Fortunately, no one experienced anemia development with anagrelide treatment. As with previous reports (3, 19, 22), the 2 most common adverse events were headaches and palpitations. In our study, 3 patients decided to discontinue anagrelide due to headache and 1 due to palpitation. Overall, there were only 4 thromboembolic events and 7 bleeding events during the 24-month follow-up period. Numerically, these are fewer compared to previous studies, which reported 11.5% (14/122) major events and 36.9% (45/122) minor events (5). Interpretation of such discrepancy warrants caution: traditionally Asians have been associated with lower incidence of thromboembolism (19, 24, 25) but recently it was reported that Korean patients have similar frequency of thrombosis compared to Western patients (26, 27). In fact, one of the major limitations of our study is that we are not able to determine if anagrelide can significantly decrease thrombosis or bleeding risk because this was a single-arm study without a control arm and because only 4 thrombotic events occurred during a follow-up time of 24 months. Since the fundamental goal of treatment in high-risk ET is a reduction of thrombosis and hemorrhage through platelet reduction to preferably normal range, we aim to investigate further if platelet response correlates with vascular events through a longer follow-up. Lastly, also due to short follow-up period, we were not able to document secondary transformation of ET. This, too, warrants a longer follow-up study.
In conclusion, our study supports the use of anagrelide as a first-line cytoreductive agent in high-risk ET. Longer and more detailed follow-up on thrombotic and bleeding complications should ensue.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://www.ncbi.nlm.nih.gov/, PRJNA853096.
The studies involving human participants were reviewed and approved by Seoul National University Hospital. The patients/participants provided their written informed consent to participate in this study.
Contribution: D-YS and S-SY created the concept and design; all authors provided the study materials or patients; JB and D-YS collected and assembled the data; and all authors contributed to the writing and the final approval of the manuscript.
Anagrelide was provided by Yuhan Corporation. This work was partially supported by the National Research Foundation of Korea (NRF-2020R1F1A1076106).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.989984/full#supplementary-material
1. Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM. The 2016 revision to the world health organization classification of myeloid neoplasms and acute leukemia. Blood (2016) 127:2391–405. doi: 10.1182/blood-2016-03-643544
2. Samuelson B, Chai-Adisaksopha C, Garcia D. Anagrelide compared with hydroxyurea in essential thrombocythemia: a meta-analysis. J Thromb Thrombol (2015) 40:474–9. doi: 10.1007/s11239-015-1218-2
3. Verstovsek S, Mesa R, Mascarenhas J, Tashi T, Shih W, Sato T, et al. MPN-545 surpass-ET: Ropeginterferon Alfa-2b (P1191) versus anagrelide as second line therapy in essential thrombocythemia. Clin Lymphom Myeloma Leuk (2022) 22 Suppl 2:S342. doi: 10.1016/S2152-2650(22)01468-9
4. Mascarenhas J, Kosiorek HE, Prchal JT, Rambaldi A, Berenzon D, Yacoub A, et al. A randomized pahse 3 trial of interferon-alpha versus hydroxyurea in polycythemia and essential thrombocythemia. Blood (2022) 139:2931–41. doi: 10.1182/blood.2021012743
5. Gisslinger H, Gotic M, Holowiecki J, Penka M, Thiele J, Kvasnicka H-M, et al. Anagrelide compared with hydroxyurea in WHO-classified essential thrombocythemia: the ANAHYDRET study, a randomized controlled trial. Blood (2013) 121:1720–8. doi: 10.1182/blood-2012-07-443770
6. Besses C, Kiladjian J-J, Griesshammer M, Gugliotta L, Harrison C, Coll R, et al. Treatment of essential thrombocythemia in Europe: a prospective long-term observational study of 3649 high-risk patients in the evaluation of anagrelide efficacy and long-term safety study. Haematologica (2018) 103:51–60. doi: 10.3324/haematol.2017.174672
7. Birgegård G, Folkvaljon F, Garmo H, Holmberg L, Besses C, Griesshammer M, et al. Hydroxyurea compared with anagrelide in high-risk essential thrombocythemia. N Engl J Med (2005) 353:33–45. doi: 10.1056/NEJMoa043800
8. Birgegård G, Besses C, Griesshammer M, Gugliotta L, Harrison CN, Hamdani M, et al. Cytoreductive treatment patterns for essential thrombocythemia in europe. analysis of 3643 patients in the EXELS study. Leuk Res (2013) 37:162–8. doi: 10.1016/j.leukres.2012.11.004
9. Harrison CN, Campbell PJ, Buck G, Wheatley K, East CL, Bareford D, et al. Leukemic transformation and second cancers in 3649 patients with high-risk essential thrombocythemia in the EXELS study. Leuk Res (2018) 74:105–9. doi: 10.1016/j.leukres.2018.10.006
10. Abe Andes W, Noveck RJ, Fleming JS. Inhibition of platelet production induced by an antiplatelet drug, anagrelide, in normal volunteers. Thromb Haemost (1984) 52:325–8. doi: 10.1055/s-0038-1661206
11. Hong Y, Wang G, Arroyo del Gutierrez A, Hernandez J, Skene C, Erusalimsky JD, et al. Comparison between anagrelide and hydroxycarbamide in their activities against haematopoietic progenitor cell growth and differentiation: selectivity of anagrelide for the megakaryocytic lineage. Leukemia (2006) 20:1117–22. doi: 10.1038/sj.leu.2404180
12. Barosi G, Mesa R, Finazzi G, Harrison C, Kiladjian J-J, Lengfelder E, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood (2013) 121:4778–81. doi: 10.1182/blood-2013-01-478891
13. Cascavilla N, De Stefano V, Pane F, Pancrazzi A, Iurlo A, Gobbi M, et al. Impact of JAK2(V617F) mutation status on treatment response to anagrelide in essential thrombocythemia: an observational, hypothesis-generating study. Drug Des Devel Ther (2015) 9:2687–94. doi: 10.2147/DDDT.S79576
14. Iurlo A, Cattaneo D, Orofino N, Bucelli C, Fabris S, Cortelezzi A, et al. Anagrelide and mutational status in essential thrombocythemia. BioDrugs (2016) 30:219–23. doi: 10.1007/s40259-016-0170-9
15. Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. Prognostic factors for thrombosis, myelofibrosis, and leukemia in essential thrombocythemia: a study of 605 patients. Haematologica (2008) 93:1645–51. doi: 10.3324/haematol.13346
16. Passamonti F, Rumi E, Arcaini L, Boveri E, Elena C, Pietra D, et al. Clinical course of essential thrombocythemia in 147 cases. Cancer (1990) 66:549–56. doi: 10.1002/1097-0142(19900801)66:3<549::aid-cncr2820660324>3.0.co;2-6
17. Fenaux P, Simon M, Caulier MT, Lai JL, Goudemand J, Bauters F, et al. Major vascular complications in essential thrombocythemia: a study of the predictive factors in a series of 148 patients. Leukemia (1999) 13:150–4. doi: 10.1038/sj.leu.2401270
18. Schulman S, Kearon C. Subcommittee on control of anticoagulation of the s, standardization committee of the international society on T, haemostasis. definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost (2005) 3:692–4. doi: 10.1111/j.1538-7836.2005.01204.x
19. Schulman S, Kearon C, Subcommittee on Control of Anticoagulation of the Scientific, Standardization Committee of the International Society on Thrombosis and Haemostasis. A phase III randomized, multicentre, double blind, active controlled trial to compare the efficacy and safety of two different anagrelide formulations in patients with essential thrombocythaemia - the TEAM-ET 2.0 trial. Br J Haematol (2019) 185:691–700. doi: 10.1111/bjh.15824
20. Steurer M, Gastl G, Jedrzejczak W-W, Pytlik R, Lin W, Schlögl E, et al. Anagrelide for thrombocytosis in myeloproliferative disorders: a prospective study to assess efficacy and adverse event profile. Cancer (2004) 101:2239–46. doi: 10.1002/cncr.20646
21. Kralovics R, Passamonti F, Buser AS, Teo S-S, Tiedt R, Passweg JR, et al. A gain-of-function mutation of JAK2 in myeloproliferative disorders. N Engl J Med (2005) 352:1779–90. doi: 10.1056/NEJMoa051113
22. Ito T, Hashimoto Y, Tanaka Y, Nakaya A, Fujita S, Satake A, et al. Efficacy and safety of anagrelide as a first-line drug in cytoreductive treatment-naive essential thrombocythemia patients in a real-world setting. Eur J Haematol (2019) 103:116–23. doi: 10.1111/ejh.13265
23. Zini R, Guglielmelli P, Pietra D, Rumi E, Rossi C, Rontauroli S, et al. CALR mutational status identifies different disease subtypes of essential thrombocythemia showing distinct expression profiles. Blood Cancer J (2017) 7:638. doi: 10.1038/s41408-017-0010-2
24. Gisslinger H, Buxhofer-Ausch V, Hodisch J, Radinoff A, Karyagina E, Kyrcz-Krzemień S, et al. Incidence of venous thromboembolism in Korea from 2009 to 2013. PloS One (2018) 13:e0191897. doi: 10.1371/journal.pone.0191897
25. Hong J, Lee JH, Yhim H-Y, Choi WI, Bang S-M, Lee H, et al. Venous thromboembolism in patients with pancreatic adenocarcinoma: lower incidence in Asian ethnicity. Thromb Res (2008) 122:485–90. doi: 10.1016/j.thromres.2007.12.015
26. Oh SY, Kim JH, Lee K-W, Bang S-M, Hwang J-H, Oh D, et al. Low incidence of clinically apparent thromboembolism in Korean patients with multiple myeloma treated with thalidomide. Ann Hematol (2010) 89:201–6. doi: 10.1007/s00277-009-0807-6
Keywords: essential thrombocythemia, high risk, Anagrelide, phase IV clinical trial, myeloproliferative neoplasms
Citation: Byun JM, Kim HY, Nam S-H, Shin H-J, Song S, Park J, Han SH, Park Y, Yuh YJ, Mun Y-C, Do YR, Sohn SK, Bae SH, Shin D-Y and Yoon S-S (2022) A multicenter, open-label study for efficacy and safety evaluation of anagrelide in patients with treatment-naïve, high-risk essential thrombocythemia as a primary treatment. Front. Oncol. 12:989984. doi: 10.3389/fonc.2022.989984
Received: 09 July 2022; Accepted: 31 October 2022;
Published: 23 November 2022.
Edited by:
Gabriela Baerlocher, University of Bern, SwitzerlandReviewed by:
Marta Sobas, Wroclaw Medical University, PolandCopyright © 2022 Byun, Kim, Nam, Shin, Song, Park, Han, Park, Yuh, Mun, Do, Sohn, Bae, Shin and Yoon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dong-Yeop Shin, c2hpbmRvbmd5ZW9wQHNudS5hYy5rcg==; Sung-Soo Yoon, c3N5c21jQHNudS5hYy5rcg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.