 Yang Xia
Yang Xia Min Lin
Min Lin Jin Huang*
Jin Huang*
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 15 September 2022
Sec. Cardio-Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.976711
The proportion of non-cancer death in patients with esophagus cancer (EC) still increasing, especially cardiovascular disease (CVD) related death. The aim of this study was assess non-cancer causes of death and identified independent risk factors of CVD related death in EC patients. Patients diagnosed with EC were extracted from the Surveillance, Epidemiology, and End Result database (SEER) database for analysis. Standardized mortality rates (SMRs) for non-EC deaths were calculated, the risk of death were assessed and compared with US general population. Multivariate competitive risk analysis were performed to select independent risk factors for death from CVD in EC patients. A total of 43739 EC patients were enrolled and 35139 died during follow-up, of which 4248 died from non-cancer cause of death. The risk of non-cancer death in EC patients was 2.27-fold higher than in the general population (SMR=2.27; 95% CI, 2.20-2.34). CVD were the most important cause of non-cancer death in EC patients, accounting for 43.4% of non-cancer of deaths. Compare with the general population, EC patients have higher risk of death from disease of heart (SMR, 2.24; 95% CI, 2.13-2.35), pneumonia and influenza (SMR, 2.92; 95% CI, 2.50-3.39), septicemia (SMR, 5.01; 95% CI, 4.30-5.79), along with other causes. Patients with advanced age and patients who received radiotherapy has higher risk of death caused by CVD, patients with female sex, poor differentiated and undifferentiated, regional and distant stage, married, diagnosed between 2010-2016 has lower risk of CVD related death, compared with patients without any treatment measures, patients received chemotherapy alone has lower risk of death from CVD. Non-cancer cause of death has become an important cause of death in EC patients. Improving public awareness of the major risk factors for non-cancer death is beneficial to the prevention and treatment of malignant tumors.
Esophagus cancer (EC) is seventh common cancers and the sixth leading cause of cancer death worldwide, with 604100 new cases and 544076 deaths in 2020, respectively (1).
With recent advances in cancer prevention, diagnosis and treatment measures, the number of cancer survivors continues to rise, these patients are not only at risk for recurrence, but may also have a variety of disease states, result the risk of non-cancer death becoming a huge threat to the health of cancer survivors (2, 3). Due to the improvement of treatments and the popularity of endoscopic screening of the upper gastrointestinal tract has led to more EC patients being diagnosed at an earlier stage, the 5-years overall survival rates of EC patients has improved in recent years (4–9). This part of EC patients may live long enough after the initial diagnosis, resulting in non-cancer-related comorbidities that may have a dramatic impact on overall survival. Recent years, the proportion of non-cancer death in EC patients were increasing, especially cardiovascular disease (CVD) related death (2, 10). Therefore, understanding the proportion and risk factor of different causes of death after EC diagnosis can be helpful in EC patient’s follow up and management. This study was designed to comprehensively assess non-cancer causes of death and identified independent predictors of CVD related death in EC patients, to provide a constructive basis for follow-up management of EC patients and optimize their quality of life.
This retrospective cohort study used data from the Surveillance, Epidemiology, and End Results (SEER) database, it’s a population-based cancer registry sponsored by the National Cancer Institute which includes morbidity, survival, and mortality data and covering approximately 27.8% of the total US population. Because of its population-based program design, data selected in SEER program can be used for comparison with the general population, and therefore can be used to estimate cancer incidence, mortality, and survival (11). We used SEER*stat software to extract primary EC patients diagnosed between 2000-2016, patients diagnosed only at autopsy or on death certificates were not included. Public information provided by the SEER program does not require ethical approval.
EC Patients (Site recode International Classification of Diseases for Oncology-3 (ICD-O-3)/WHO 2008: Esophagus) with malignant behavior between 2000-2016 were extracted from SEER database. The exclusion criteria were as follow (1): Multiple primary tumor; (2) Unknown cause of death; the specific process is shown in Figure 1. Patient’s detailed information were extracted including age at diagnosis, sex, race, diagnosis year, insurance status, marital status, grade, primary site, SEER summary stage, surgery, radiotherapy and chemotherapy. Well-differentiated and moderately differentiated tumors were defined as grade I + II, poorly differentiated and undifferentiated tumors were defined as grade III + IV.
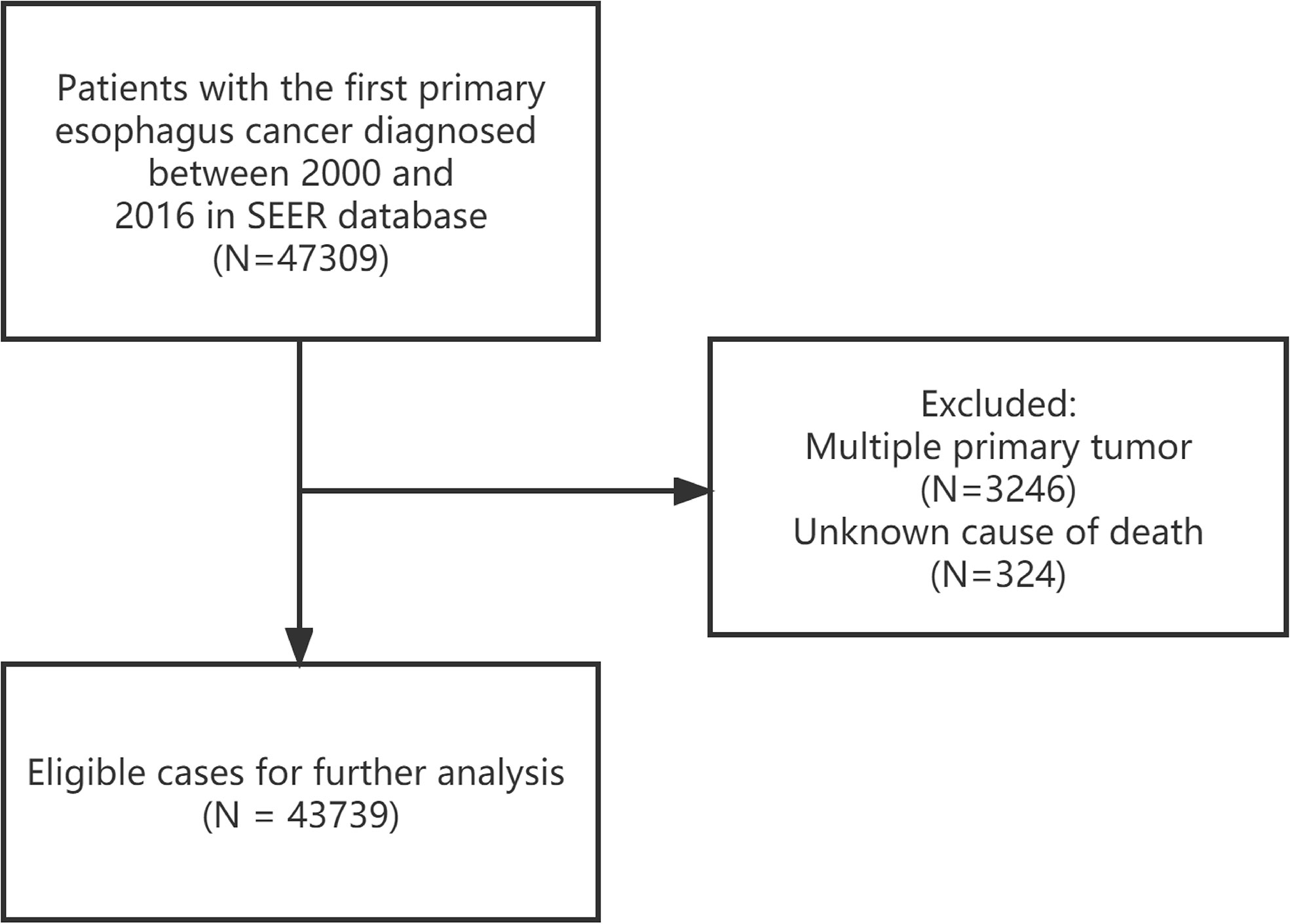
Figure 1 Inclusion and exclusion flowchart.
In the SEER database, the cause of death classification is coded according to the International Classification of Diseases, Version 9 (ICD-9) and ICD-10 used by the registry, information about cause of death categories in the general population originate in the Wide-ranging Online Data for Epidemiologic Research tool from the Centers for Disease Control and Prevention and which can available through the SEER*stat software (12). SEER database through systematic and standard data collection procedure to ensure the accuracy of cause of death determinations, thereby mitigating the possible impacts of potential biases on study findings (13). All cause of death was referring to the total number of deaths during the follow-up period, non-cancer death included seven categories: cardiovascular disease, infectious disease, respiratory disease, kidney disease, gastrointestinal disease, external injury, and other causes of death. CVD included disease of heart, hypertension without heart disease, cerebrovascular diseases, aortic aneurysm and dissection, atherosclerosis and other diseases of arteries, arterioles, capillaries (14).
We examined non-cancer causes of death in EC patients, mortality events were classified according to the time interval from diagnosis to death, these intervals contained: <1 year, 1-5 years, 5-10 years and >10 years. The relative risk of non-cancer death among EC patients was compared with that of US general population and expressed as standardized mortality rates (SMRs), which was defined as the radio of observed number divide expected number, ”Observed” was defined as the actual death number of a specific cause in a specific interval, and “Expected” was defined as the expected number of deaths from the same cause in a demographically similar population (regarding sex, race, and age) within the same interval (15).
SMR and 95% confidence intervals (95%CI) were calculated in different interval after diagnosis (<1 year, 1-5 years, 5-10 years and >10 years), we used the Poisson exact method to compute the 95% CI for SMR. The hazard ratios (HRs) and 95% CI were used to estimate the associations between patient characteristics and CVD related death in EC patients through multivariate competing risk analysis. Death from CVD were defined as events of primary concern, while competitive events were defined as deaths from other causes. All tests were double-sided, P < 0.05 were considered statistically significant. Data analysis was performed by SEER*stat (version 8.4.0) and R software (version 4.0.0).
After above exclusion criteria, 43739 EC patients were extracted from the SEER database for further analysis. Most patients died within 5 years after diagnosis (94.6%). The majority of patients were male (78.7%), white patients accounted for 83.7% of the total. Most included patients were poor differentiation and undifferentiation (41.8%), married (55.3%), insured (48.5%), 50-70 years old (56.7%) and were located in the lower third of the esophagus (60.6%). Most esophageal malignancies were found in regional stage (33.6%) and distant stage (34.2%), while only a minority of patients were diagnosed in the localized stage (21.5%). The rate of surgery, radiotherapy and chemotherapy in our cohort were 28%, 59.4% and 64.5%, respectively. Some patients received multiple treatment measures, as shown in Table 1 for specific information.
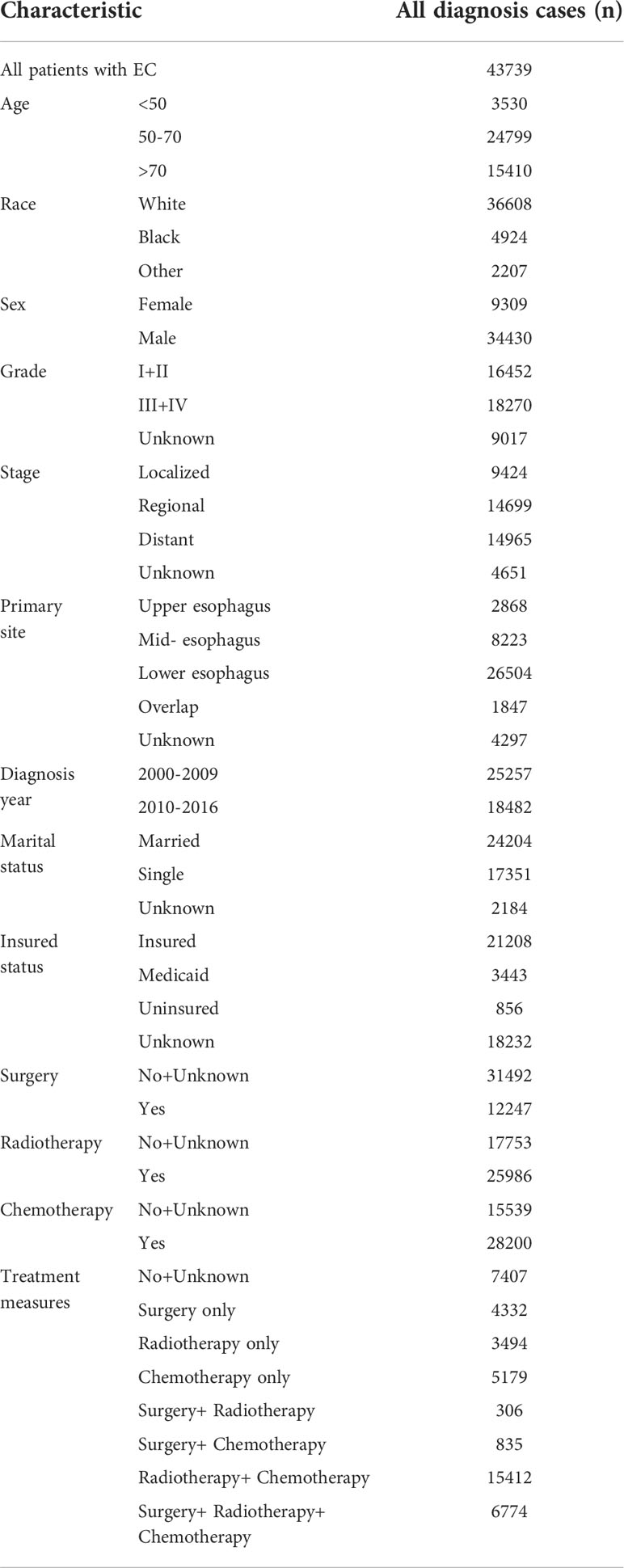
Table 1 Baseline characteristics of EC patients.
A total of 35,193 patients died during follow-up, of which 4248 (12.1%) died from non-cancer causes, including CVD (1843, 43.4%), other cause of death (1109, 26.1%), infectious diseases (451, 10.6%), respiratory diseases (439, 10.3%), external injuries (228, 5.4%), renal diseases (91, 2.1%) and gastrointestinal diseases (87, 2.0%). Throughout the follow-up period, patients had a higher risk of death from disease of heart (SMR, 2.24; 95% CI, 2.13-2.35), cerebrovascular diseases (SMR, 1.56; 95% CI, 1.35-1.78), pneumonia and influenza (SMR, 2.92; 95% CI, 2.50-3.39), septicemia (SMR, 5.01; 95% CI, 4.30-5.79), COPD (SMR, 2.75; 95% CI, 2.50-3.02), suicide and self-inflicted injury (SMR, 4.08; 95% CI, 3.24-5.06) and nephritis, nephrotic syndrome and nephrosis (SMR, 1.79; 95% CI, 1.44-2.20) compared with US general population, along with other cause (Table 2).
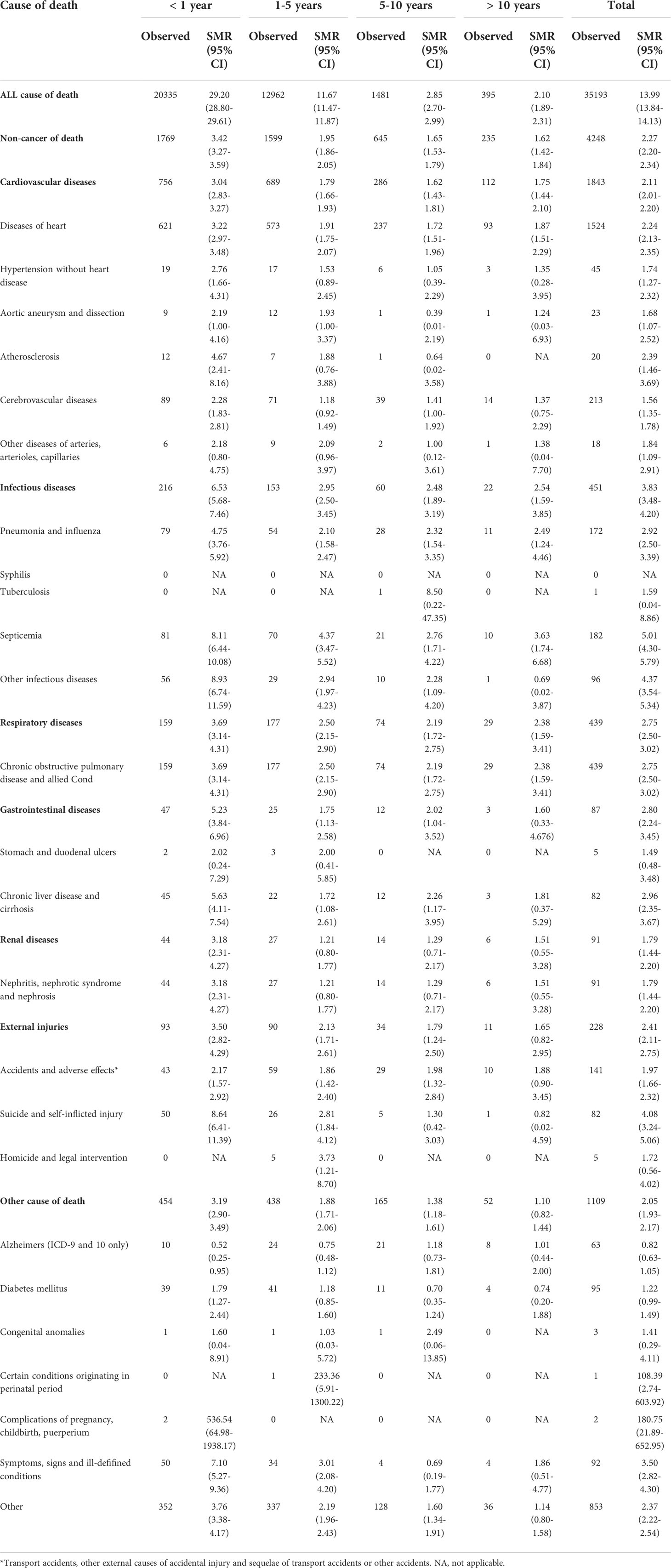
Table 2 Standardized-mortality ratios for each cause of death following esophagus cancer diagnosis.
A total of 20335 patients died within 1 year after diagnosis, of which 1769 (8.7%) died because of non-cancer causes. The most common causes of death were CVD (756; 42.7%), followed by other cause of death (454; 25.7%) and infectious diseases (216; 12.2%). Compared with US general populations, EC patients has the higher risk of death from disease of heart (SMR, 3.22; 95% CI, 2.97-3.48), cerebrovascular diseases (SMR, 2.28; 95% CI, 1.83-2.81), pneumonia and influenza (SMR, 4.75; 95% CI, 3.76-5.92), septicemia (SMR, 8.11; 95% CI, 6.44-10.08), COPD (SMR, 3.69; 95% CI, 3.14-4.31), suicide and self-inflicted injury (SMR, 8.64; 95% CI, 6.41-11.39) and diabetes mellitus (SMR, 1.79; 95% CI, 1.27-2.44), along with other cause. In addition, EC patients have a significantly decreased risk of Alzheimer’s disease compare with general populations within 1 year (SMR, 0.52; 95% CI, 0.25–0.95) (Table 2).
A total of 12962 patients died within 1-5 years of diagnosis, of which 1599 (12.3%) died because of non-cancer causes. The most common causes of death were CVD (689; 43.1%), followed by other cause of death (438; 27.4%) and respiratory diseases (177; 11.1%). Compared with the general population, EC patients had higher risk of death from disease of heart (SMR, 1.91; 95% CI, 1.75-2.07), pneumonia and influenza (SMR, 2.10; 95% CI, 1.58-2.47), septicemia (SMR, 4.37; 95% CI, 3.47-5.52), COPD (SMR, 2.50; 95% CI, 2.15-2.90), chronic liver disease and cirrhosis (SMR, 1.72; 95% CI, 1.08-2.61), suicide and self-inflicted injury (SMR, 2.81; 95% CI, 1.84-4.12), along with other cause. Patients’ risk of dying from Alzheimer’s disease was still reduced, but not statistically (SMR,0.75; 95% CI, 0.48-1.12) (Table 2).
A total of 1481 patients died within 5-10 years of diagnosis, of which 645 (43.6%) died because of non-cancer causes. The most common cause of death were CVD (286; 44.3%), followed by other cause of death (165; 25.6%) and COPD (74; 11.5%). Within 5-10 years of diagnosis, patients had a higher risk of death from disease of heart (SMR, 1.72; 95% CI, 1.51-1.96), pneumonia and influenza (SMR, 2.32; 95% CI, 1.54-3.35), septicemia (SMR, 2.76; 95% CI, 1.71-4.22), COPD (SMR, 2.19; 95% CI, 1.72-2.75), chronic liver disease and cirrhosis (SMR, 2.26; 95% CI, 1.17-3.95) and accidents and adverse effects (SMR, 1.98; 95% CI, 1.32-2.84) compared with US general population, along with other causes of death (Table 2).
A total of 395 patients died 10 years after diagnosis, including 235 deaths from non-cancer causes (59.5%) accounted for more than half. The most common causes of death were CVD (112; 47.7%), followed by other cause of death (52; 22.1%) and respiratory diseases (29; 12.3%). After more than 10 years of diagnosis, EC patients showed a higher risk of death from disease of heart (SMR, 1.87; 95% CI, 1.51–2.29), pneumonia and influenza (SMR, 2.49; 95% CI, 1.24–4.46), septicemia (SMR, 3.63; 95% CI, 1.74–6.68), COPD (SMR, 2.38; 95% CI, 1.59-3.41) compared with US general population, along with other causes of death (Table 2).
Given that CVD accounts for a large proportion of non-cancer deaths, we used a multivariate competitive risk analysis to identify predictors associated with CVD related death in EC patients, the results indicated that these following characteristics were independently associated with a higher risk of CVD: 50-70 years old (HR: 2.324; 95% CI: 1.731-3.120), > 70 years old (HR: 4.886; 95% CI: 3.636-6.565), patients who received radiotherapy (HR: 1.180; 95% CI: 1.052-1.324). On the other hand, we found that the following characteristics were independently associated with a lower risk of CVD: female sex (HR: 0.848; 95% CI: 0.755-0.953), poorly differentiated and undifferentiated (HR: 0.843; 95% CI: 0.757-0.938), regional (HR: 0.625; 95% CI: 0.558-0.701) or distant stage (HR: 0.315; 95% CI: 0.271-0.366), married state (HR: 0.883; 95% CI: 0.797-0.978) and diagnosed between 2010-2016 (HR: 0.697; 95% CI: 0.611-0.794) (Table 3).
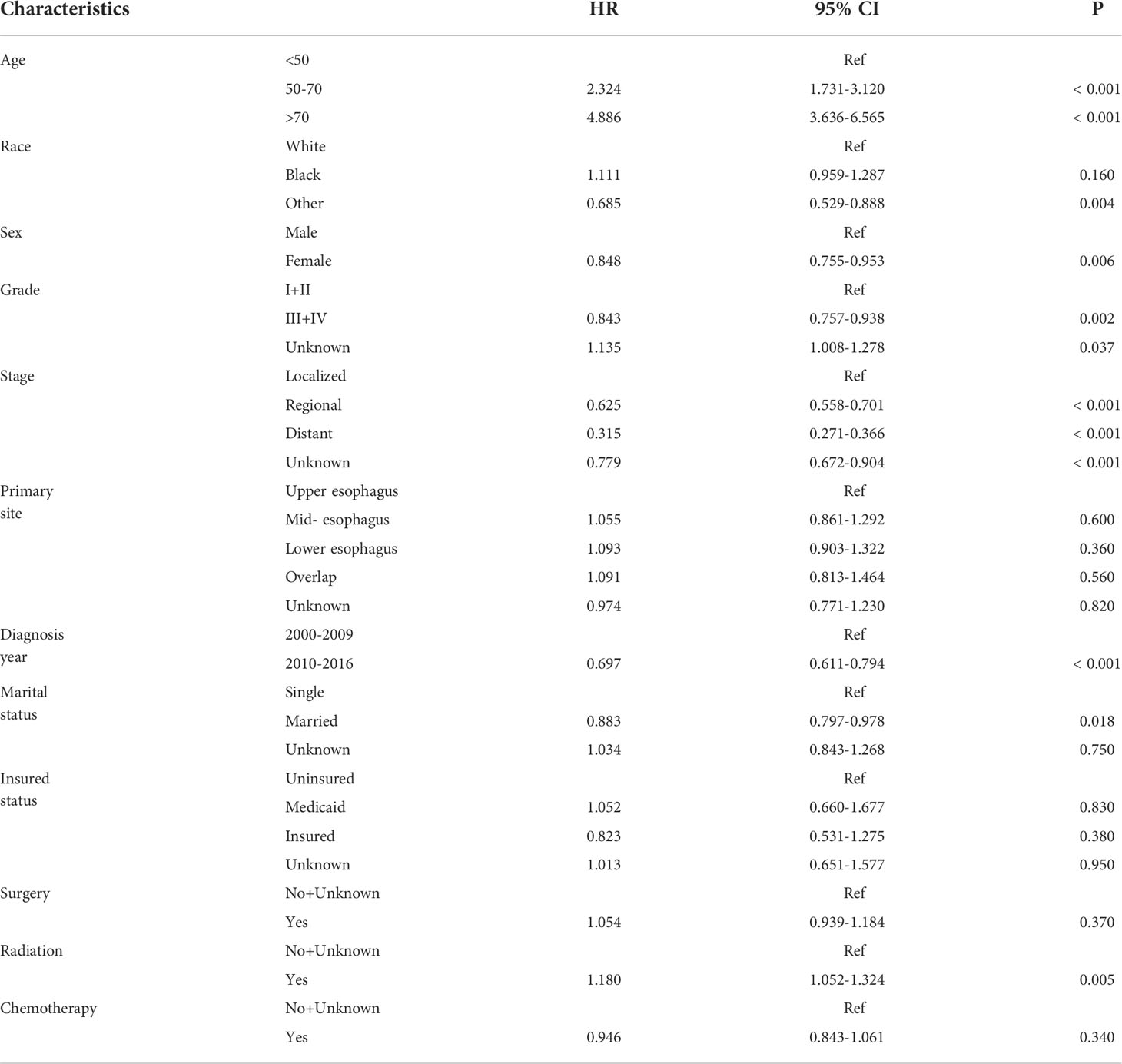
Table 3 Multivariate competing risk analysis for predictors of CVD related death in EC patients.
Multivariate competitive risk analysis suggested that radiotherapy was an independent risk factor for CVD related death in EC patients. Therefore, we further analyzed the effects of radiotherapy with different characteristics. we found that the following patients receive radiotherapy has higher risks of CVD related death: 50-70 years old (HR: 1.210; 95% CI: 1.013-1.446), >70 years old (HR: 1.229; 95% CI: 1.054-1.433), white patients (HR: 1.196; 95% CI: 1.053-1.358), male patients (HR: 1.174; 95% CI: 1.030-1.338), regional stage (HR: 1.280; 95% CI: 1.023-1.601), unmarried patients (HR: 1.210; 95% CI: 1.012-1.446), located at the middle third (HR: 1.297; 95% CI: 1.004-1.676) and lower third (HR: 1.234; 95% CI: 1.060-1.437) of the esophagus, specific information see in Table 4.
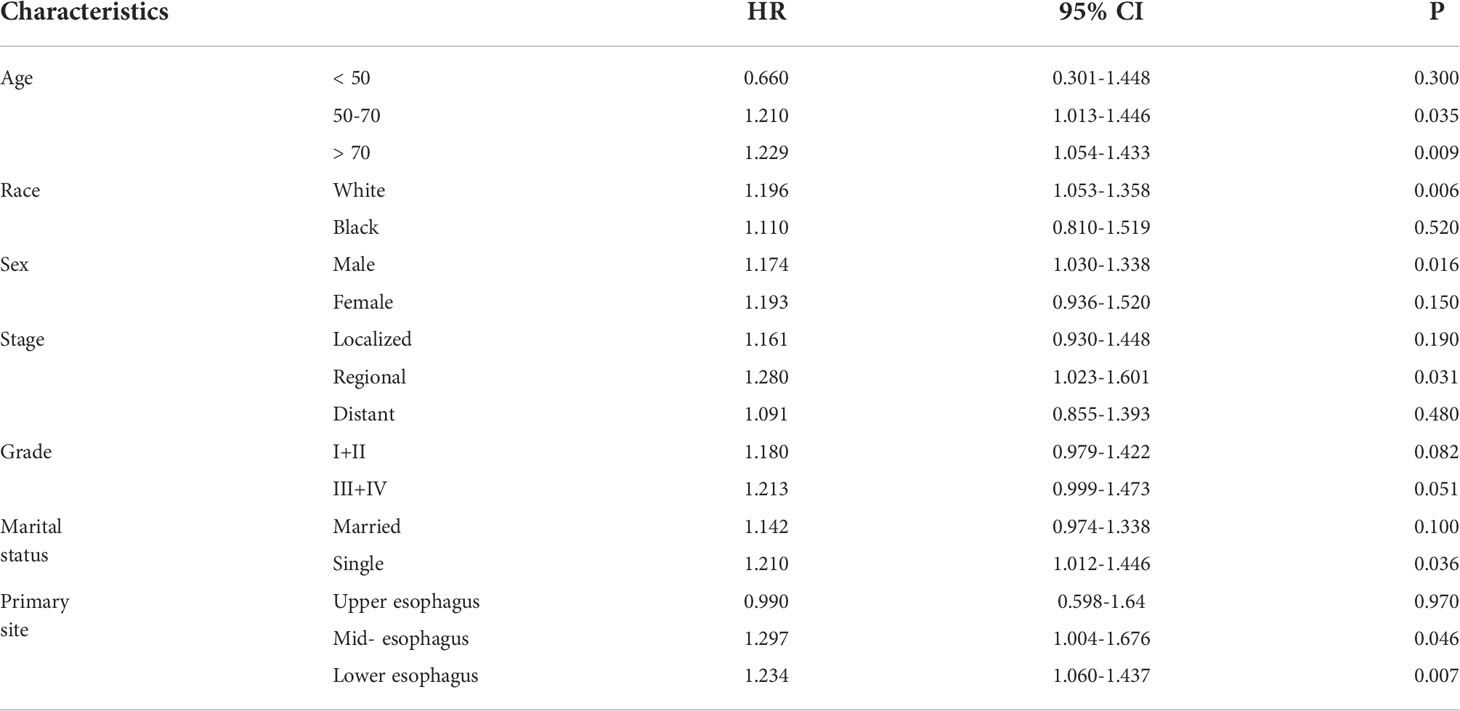
Table 4 Effects of radiotherapy on CVD related death in EC patients with different characteristics.
Because some patients in our cohort received combination therapies, we further divided patient treatment measures to determine the effects of different treatments on CVD related death in EC patients through multivariate competitive risk analysis, the results indicated that these following characteristics were independently associated with a higher risk of CVD: 50-70 years old (HR: 2.307; 95% CI: 1.719-3.097), > 70 years old (HR: 4.949; 95% CI: 3.608-6.516). On the other hand, we found that the following characteristics were independently associated with a lower risk of CVD: female sex (HR: 0.848; 95% CI: 0.755-0.953), poorly differentiated and undifferentiated (HR: 0.848; 95% CI: 0.762-0.944), regional (HR: 0.635; 95% CI: 0.565-0.713) or distant stage (HR: 0.333; 95% CI: 0.286-0.388), married (HR: 0.883; 95% CI: 0.797-0.979), diagnosed between 2010-2016 (HR: 0.696; 95% CI: 0.610-0.793) and patients received chemotherapy alone compared with patients without any treatment measures (HR: 0.702; 95% CI: 0.551-0.895) (Table 5).
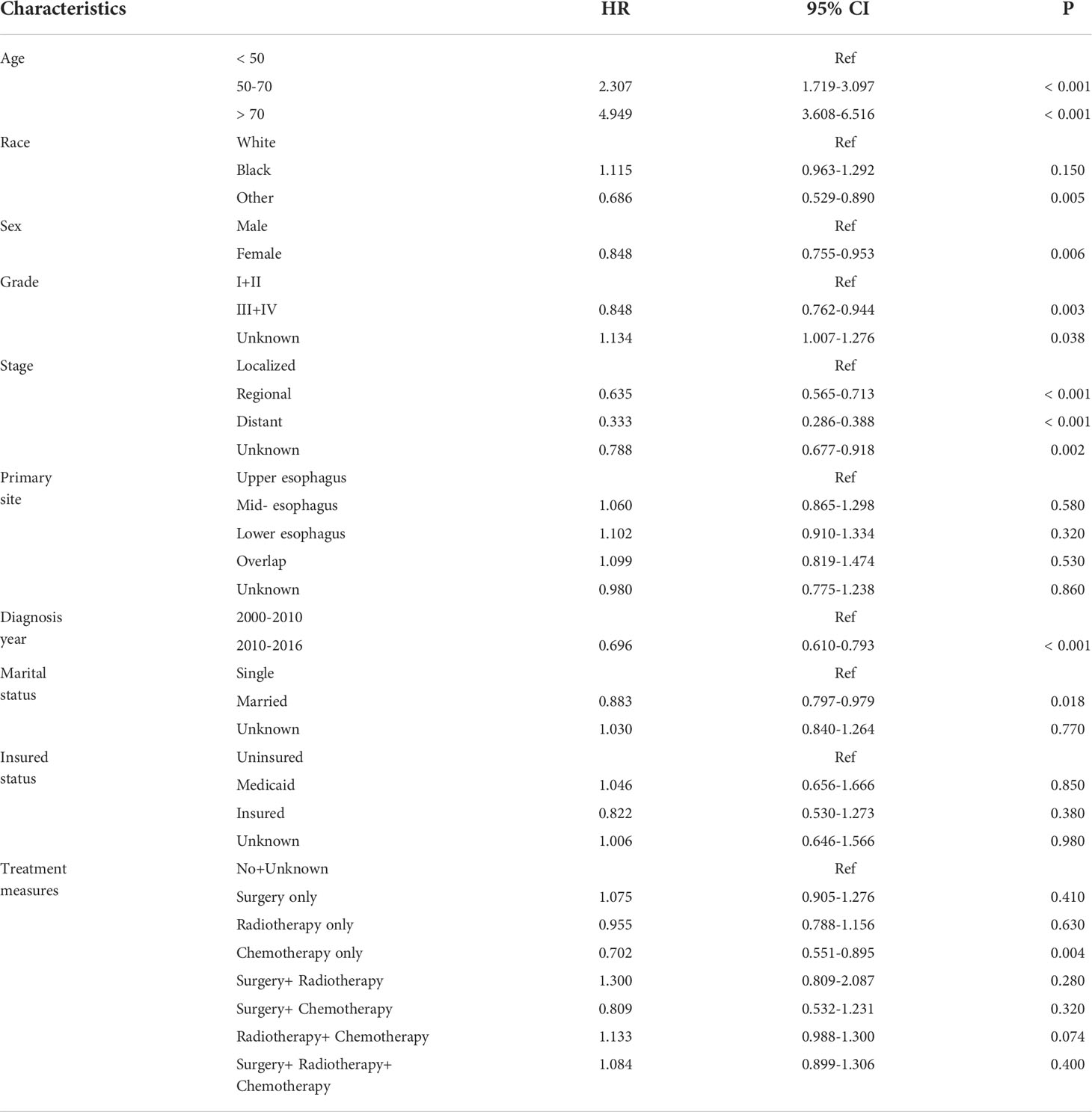
Table 5 Effects of comprehensive treatment measures on CVD related death in EC patients.
Analysis of the mortality rate and the main causes of death of malignant tumors are helpful to master the disease characteristics of malignant tumors, and is of great significance to the control and management of tumors. According to a study about the causes of death among cancer patients in China, EC is the fourth leading cause of in-hospital deaths among cancer patients (16). With the spread of neoadjuvant therapy, the current median survival time for EC patients has improved significantly (4). With the increasing number of long-term EC survivors, non-cancer causes have become one of the main causes of death in EC patients, especially CVD related death, which are currently the second leading cause of death, after cancer itself (10), and the trend is still rising. As the diversification of combination therapies leads to long-term survival in more cancer patients, it is increasingly important to identify non-cancer deaths due to comorbidities or side effects due to treatment toxicity.
Recent years, several studies have suggested that cancer patients have a higher risk of CVD related death compared with general population (12, 14). Wang’s study showed that the cardiovascular mortality rates of 1, 3 and 5 years in cancer patients were 6.0%, 10.8% and 17.9%, respectively, and the total cardiovascular mortality rates were 25.8% (17). According to previous report, cancer patients have a higher risk of thromboembolism compare with general population, especially in lung and pancreatic cancer (18). In our research, EC patients have a higher risk of death from CVD than the general population during the whole follow-up periods (SMR, 2.11; 95% CI, 2.01–2.20), the highest risk of death from CVD occurred within 1 year after diagnosis (SMR, 3.04; 95% CI, 2.83–3.27). At the beginning of cancer diagnosis, patients are often at increased risk of CVD due to psychological stress such as anxiety and stress, these emotional states may be increased pressure on the heart due to the increased burden of disease, leading to death from cardiovascular causes, this phenomenon were particularly pronounced in esophageal, liver, pancreatic and lung cancers (19). In addition, EC patients are at risk for long-term cardiac sequelae due to radiotherapy, chemotherapy or surgery during treatment, which may also contribute to the high incidence of CVD related death (20).
CVD are the most common cause of non-cancer death in EC patients, it is significant to select high-risk EC patients of CVD related death and develop appropriate measures to prevent potential risk of it. Previous studies indicated that male sex, black race, advanced age, receive radiotherapy were associated with a significantly increased risk of death from CVD (17, 20). Male cancer patients have a greater risk of death from CVD compared to women (17), our research came to the same conclusion, this phenomenon may be due to hormonal differences (21). Another possible reason were that men tend to have worse lifestyle habits, such as drinking and smoking, which have been reported to be independent risk factors for CVD (22–24). According to previous studies, black are more likely to died from CVD than other races (25, 26), this may be due to the higher risk of venous thromboembolism in black cancer patients (26). Our research showed that black patients are at greater risk of CVD related death, but there was no statistical significance (HR:1.111; P=0.160), this may be due to the small percentage of blacks in the overall study cohort (11.3%), so may be it doesn’t reflect actual CVD related death in the whole black population, therefore, further investigation about this issue in EC patients is still necessary. In our research, older patients are more likely to died from CVD, which is in line with previous study (17). The reason may be that elderly patients has a higher incidence of comorbidities, which may result higher risk of cardiovascular events, but the specific mechanism still needs further analysis. In addition, multivariate competitive risk analysis suggested that EC patients with poorly and undifferentiated (HR: 0.843; 95% CI: 0.757-0.938) and distant tumor stage (HR: 0.315; 95% CI: 0.271-0.366) has lower risk of CVD related death, low degree of differentiation and distant stage are adverse prognostic factors of EC patients (27, 28), since the proportion of CVD related death increased with the increase in years of diagnosis, leading to the possibility that these patients may not have a long enough life expectancy to died from CVD. Married patients showed a lower tendency to died from CVD than unmarried patients (HR: 0.883; 95% CI: 0.797-0.978), they often receive more physical and emotional care, encouragement and support than unmarried patients (29), that could be one of the reason. Our study revealed that EC patients diagnosed between 2010-2016 had a lower risk of CVD related death. With the advances in imaging and laboratory medicine, such as cardiac magnetic resonance imaging and echocardiography, as well as the widespread clinical use of troponin and n-terminal b-type natriuretic peptide, resulting more and more early detection and intervention of heart disease (30–32), in addition, the comprehensive treatment measures of EC continues to improve (4–8), these advances in medical technology may have significantly reduced heart-specific mortality in recent years.
Many studies established that cancer patients without surgery may lead to a significantly increased risk of CVD related death (17, 20, 33), but there have also been studies showing that surgery can increase the risk of venous thromboembolism (34, 35). Our study indicated that surgical treatment is an risk factor for CVD related death but there was no statistical significance (HR: 1.054; P=0.370). Khorana proposed that thromboembolism is the leading cause of death in cancer patients who received chemotherapy (10), in our research, patients who received chemotherapy alone had a lower risk of CVD related death than patients who did not received any treatments (HR: 0.702; P=0.004). It has been claimed that anticoagulant therapy can prolong the survival time of cancer patients, low molecular weight heparin and warfarin are more and more commonly used in cancer patients during chemotherapy in recent years, which to some extent reduces the probability of thromboembolic events in cancer patients (18). In addition, patients received regularly chemotherapy can have better health monitoring during treatment and receive more timely intervention when at risk for thromboembolism to avoid subsequent adverse events. These reasons may explain the lower risk of CVD related death in EC patients who receiving chemotherapy alone.
Advances in cancer treatment, while significantly reducing mortality from primary cancer, may increase the risk of death from causes other than primary cancer, such as non-cancer comorbidities. Radiotherapy can bring survival benefits to EC patients (4), but the short and long-term side effects of radiotherapy cannot be ignored. Our study indicated that EC patients who received radiotherapy had a higher risk of death from CVD (HR:1.180; P=0.005). This is consistent with the conclusions of previous analysis (20). Long-term cardiotoxicity caused by radiotherapy has been previously reported, mainly including myocardial fibrosis, pericardial disease, coronary artery disease, valvular disease and arrhythmias (20). It has been reported that abnormal increase of myocardial perfusion, decrease of ejection fraction and pericardial effusion occurred after chemoradiotherapy by imaging examination (36–38). In addition, given that the heart is anatomically located close to the esophagus, it is expected that the radiation process will affect the heart, these above side effects may lead to cardiovascular system injury, but the exact mechanism is still unclear and further research is still needed. Therefore, despite the survival benefits of radiotherapy for EC patients, its potential cardiac toxicity and side effects should not be ignored, radiation-induced cardiotoxicity should be considered in long-term follow-up management of EC patients.
Our study have several limitations: first, factors such as patient’s comorbidities (hyperlipidemia, diabetes, dyslipidemia, obesity and history of CVDs), bad habits (alcohol use and smoking habit), family history, detailed information of radiation and chemotherapy (type, dosage, and duration) may influence CVD related death in EC patients, but these information are not included in the SEER database (12, 14). Second, because only patients diagnosed between 2000 and 2016 were included, some patients diagnosed late do not have adequate follow-up time. Finally, this study was retrospective analysis, which may be biased in data selection.
Non-cancer deaths account for a significant proportion of death in EC patients, the highest numbers of non-cancer deaths were caused by CVD. Patients, who were 50-70 years old, >70 years old, male sex, well differentiated and moderately differentiated, localized stage, unmarried state, diagnosed between 2000-2009 and receive radiotherapy had a significantly higher risk of death from CVD. Compared with EC patients without any treatments, patients received chemotherapy alone has lower risk of CVD related death. Regular CVD screening and CVD risk factors control are of great significance for the follow-up of EC patients.
Publicly available datasets were analyzed in this study. This data can be found here: https://seer.cancer.gov/.
YX and LF designed the research. YX, ML, JH, LF performed the study and analyzed the data. YX and ML wrote the paper and interpreted the data. LF, ML and JH help to revised manuscript. All authors read and approved the final manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the Changzhou No.2 People’s Hospital Fund (2019HZD001).
The authors acknowledge contributions from SEER program.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Zaorsky NG, Churilla TM, Egleston BL, Fisher SG, Ridge JA, Horwitz EM, et al. Causes of death among cancer patients. Ann Oncol (2017) 28(2):400–7. doi: 10.1093/annonc/mdw604
3. Kakuta T, Kosugi S, Kanda T, Ishikawa T, Hanyu T, Suzuki T, et al. Prognostic factors and causes of death in patients cured of esophageal cancer. Ann Surg Oncol (2014) 21(5):1749–55. doi: 10.1245/s10434-014-3499-7
4. van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med (2012) 366(22):2074–84. doi: 10.1056/NEJMoa1112088
5. Gebski V, Burmeister B, Smithers BM, Foo K, Zalcberg J, Simes J, et al. Survival benefits from neoadjuvant chemoradiotherapy or chemotherapy in oesophageal carcinoma: A meta-analysis. Lancet Oncol (2007) 8(3):226–34. doi: 10.1016/S1470-2045(07)70039-6
6. Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, Nicolson M, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med (2006) 355(1):11–20. doi: 10.1056/NEJMoa055531
7. Walsh TN, Noonan N, Hollywood D, Kelly A, Keeling N, Hennessy TP. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med (1996) 335(7):462–7. doi: 10.1056/NEJM199608153350702
8. Cooper JS, Guo MD, Herskovic A, Macdonald JS, Martenson JA Jr, Al-Sarraf M, et al. Chemoradiotherapy of locally advanced esophageal cancer: Long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation therapy oncology group. JAMA (1999) 281(17):1623–7. doi: 10.1001/jama.281.17.1623
9. Tachibana M, Kinugasa S, Shibakita M, Tonomoto Y, Hattori S, Hyakudomi R, et al. Surgical treatment of superficial esophageal cancer. Langenbecks Arch Surg (2006) 391(4):304–21. doi: 10.1007/s00423-006-0063-3
10. Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost (2007) 5(3):632–4. doi: 10.1111/j.1538-7836.2007.02374.x
11. Chen J, Peng J, Zheng Y, Li S, Yang P, Wu X, et al. Primary renal lymphoma: A population-based study in the United States, 1980-2013. Sci Rep (2019) 9(1):15125. doi: 10.1038/s41598-019-51635-6
12. Yin X, Fan F, Zhang B, Hu Y, Sun C. Cardiovascular-specific mortality among multiple myeloma patients: A population-based study. Ther Adv Hematol (2022) 13:20406207221086755. doi: 10.1177/20406207221086755
13. Yang K, Zheng Y, Peng J, Chen J, Feng H, Yu K, et al. Incidence of death from unintentional injury among patients with cancer in the United States. JAMA Netw Open (2020) 3(2):e1921647. doi: 10.1001/jamanetworkopen.2019.21647
14. Wang Q, Zeng Z, Nan J, Zheng Y, Liu H. Cause of death among patients with thyroid cancer: A population-based study. Front Oncol (2022) 12:852347. doi: 10.3389/fonc.2022.852347
15. Afifi AM, Elmehrath AO, Ruhban IA, Saad AM, Gad MM, Al-Husseini MJ, et al. Causes of death following nonmetastatic colorectal cancer diagnosis in the U.S: A Population-Based Analysis. Oncologist (2021) 26(9):733–9. doi: 10.1002/onco.13854
16. Wang X, Song ZF, Xie RM, Pei J, Xiang MF, Wang H. Analysis of death causes of in-patients with malignant tumors in Sichuan cancer hospital of China from 2002 to 2012. Asian Pac J Cancer Prev (2013) 14(7):4399–402. doi: 10.7314/apjcp.2013.14.7.4399
17. Wang J, Yan X, Feng W, Shi W, Wang Q, Zhang Q, et al. Risk factors of death from vascular events among cancer survivors: A SEER database analysis. Med Clin (Barc) (2021) 156(2):49–54. doi: 10.1016/j.medcli.2020.02.007
18. Agnelli G, Gussoni G, Bianchini C, Verso M, Mandalà M, Cavanna L, et al. Nadroparin for the prevention of thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: A randomised, placebo-controlled, double-blind study. Lancet Oncol (2009) 10(10):943–9. doi: 10.1016/S1470-2045(09)70232-3
19. Fang F, Fall K, Mittleman MA, Sparén P, Ye W, Adami HO, et al. Suicide and cardiovascular death after a cancer diagnosis. N Engl J Med (2012) 366(14):1310–8. doi: 10.1056/NEJMoa1110307
20. Frandsen J, Boothe D, Gaffney DK, Wilson BD, Lloyd S. Increased risk of death due to heart disease after radiotherapy for esophageal cancer. J Gastrointest Oncol (2015) 6(5):516–23. doi: 10.3978/j.issn.2078-6891.2015.040
21. Riondino S, Guadagni F, Formica V, Ferroni P, Roselli M. Gender differences in cancer-associated venous thromboembolism. Curr Med Chem (2017) 24(24):2589–601. doi: 10.2174/0929867323666161018144505
22. Wong MD, Chung AK, Boscardin WJ, Li M, Hsieh HJ, Ettner SL, et al. The contribution of specific causes of death to sex differences in mortality. Public Health Rep (2006) 121(6):746–54. doi: 10.1177/003335490612100615
23. Levenson J, Simon AC, Cambien FA, Beretti C. Cigarette smoking and hypertension. factors independently associated with blood hyperviscosity and arterial rigidity. Arteriosclerosis (1987) 7(6):572–7. doi: 10.1161/01.atv.7.6.572
24. Briasoulis A, Agarwal V, Messerli FH. Alcohol consumption and the risk of hypertension in men and women: A systematic review and meta-analysis. J Clin Hypertens (Greenwich) (2012) 14(11):792–8. doi: 10.1111/jch.12008
25. He XJ, Wu YY, Xia MR, Li ZQ, Zhao M, Dai QD, et al. Risk factors associated with mortality from vascular thromboembolic events in patients diagnosed with non-small cell lung cancer: A population-based analysis. QJM (2017) 110(12):807–13. doi: 10.1093/qjmed/hcx166
26. Patel RK, Ford E, Thumpston J, Arya R. Risk factors for venous thrombosis in the black population. Thromb Haemost (2003) 90(5):835–8. doi: 10.1160/TH03-05-0311
27. Yu Z, Yang J, Gao L, Huang Q, Zi H, Li X. A competing risk analysis study of prognosis in patients with esophageal carcinoma 2006-2015 using data from the surveillance, epidemiology, and end results (SEER) database. Med Sci Monit (2020) 26:e918686. doi: 10.12659/MSM.918686
28. Shi M, Zhai GQ. Models for predicting early death in patients with stage IV esophageal cancer: A surveillance, epidemiology, and end results-based cohort study. Cancer Control (2022) 29:10732748211072976. doi: 10.1177/10732748211072976
29. Du B, Wang F, Wu L, Wang Z, Zhang D, Huang Z, et al. Cause-specific mortality after diagnosis of thyroid cancer: A large population-based study. Endocrine (2021) 72(1):179–89. doi: 10.1007/s12020-020-02445-8
30. Foley PW, Hamilton MS, Leyva F. Myocardial scarring following chemotherapy for multiple myeloma detected using late gadolinium hyperenhancement cardiovascular magnetic resonance. J Cardiovasc Med (Hagerstown) (2010) 11(5):386–8. doi: 10.2459/JCM.0b013e32832f3ff2
31. Dispenzieri A, Gertz MA, Kyle RA, Lacy MQ, Burritt MF, Therneau TM, et al. Serum cardiac troponins and n-terminal pro-brain natriuretic peptide: A staging system for primary systemic amyloidosis. J Clin Oncol (2004) 22(18):3751–7. doi: 10.1200/JCO.2004.03.029
32. Mathur P, Thanendrarajan S, Paydak H, Vallurupalli S, Jambhekar K, Bhatti S, et al. Cardiovascular complications of multiple myeloma in the elderly. Expert Rev Cardiovasc Ther (2017) 15(12):933–43. doi: 10.1080/14779072.2017.1409114
33. Trinh VQ, Karakiewicz PI, Sammon J, Sun M, Sukumar S, Gervais MK, et al. Venous thromboembolism after major cancer surgery: Temporal trends and patterns of care. JAMA Surg (2014) 149(1):43–9. doi: 10.1001/jamasurg.2013.3172
34. Osborne NH, Wakefield TW, Henke PK. Venous thromboembolism in cancer patients undergoing major surgery. Ann Surg Oncol (2008) 15(12):3567–78. doi: 10.1245/s10434-008-0151-4
35. Agnelli G, Bolis G, Capussotti L, Scarpa RM, Tonelli F, Bonizzoni E, et al. A clinical outcome-based prospective study on venous thromboembolism after cancer surgery: The @RISTOS project. Ann Surg (2006) 243(1):89–95. doi: 10.1097/01.sla.0000193959.44677.48
36. Gayed I, Gohar S, Liao Z, McAleer M, Bassett R, Yusuf SW. The clinical implications of myocardial perfusion abnormalities in patients with esophageal or lung cancer after chemoradiation therapy. Int J Cardiovasc Imaging (2009) 25(5):487–95. doi: 10.1007/s10554-009-9440-7
37. Tripp P, Malhotra HK, Javle M, Shaukat A, Russo R, De Boer S, et al. Cardiac function after chemoradiation for esophageal cancer: Comparison of heart dose-volume histogram parameters to multiple gated acquisition scan changes. Dis Esophagus (2005) 18(6):400–5. doi: 10.1111/j.1442-2050.2005.00523.x
Keywords: esophagus cancer, cause of death, cardiovascular disease, surveillance, epidemiology, and end result, standardized mortality rates
Citation: Xia Y, Lin M, Huang J and Fan L (2022) Cardiovascular disease related death among patients with esophagus cancer: A population-based competing risk analysis. Front. Oncol. 12:976711. doi: 10.3389/fonc.2022.976711
Received: 04 July 2022; Accepted: 29 August 2022;
Published: 15 September 2022.
Edited by:
Paolo Pedrazzoli, Medical Oncology - Fondazione IRCCS Policlinico San Matteo, ItalyReviewed by:
Gianpiero Rizzo, San Matteo Hospital Foundation (IRCCS), ItalyCopyright © 2022 Xia, Lin, Huang and Fan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Li Fan, MTU4NTUxODE0QHFxLmNvbQ==; Jin Huang, aGowNDIxNTNAcXEuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.