 Adrien Grancher1*
Adrien Grancher1* Ludivine Beaussire1,2Sylvain Manfredi3Karine Le Malicot3Marie Dutherage1Vincent Verdier1Claire Mulot4Olivier Bouché5Jean-Marc Phelip6Charles-Briac Levaché7Philippe Deguiral8Sophie Coutant1David Sefrioui1
Ludivine Beaussire1,2Sylvain Manfredi3Karine Le Malicot3Marie Dutherage1Vincent Verdier1Claire Mulot4Olivier Bouché5Jean-Marc Phelip6Charles-Briac Levaché7Philippe Deguiral8Sophie Coutant1David Sefrioui1 Jean-François Emile9Pierre Laurent-Puig10
Jean-François Emile9Pierre Laurent-Puig10 Frédéric Bibeau11Pierre Michel1
Frédéric Bibeau11Pierre Michel1 Nasrin Sarafan-Vasseur1Côme Lepage3Frederic Di Fiore1,2
Nasrin Sarafan-Vasseur1Côme Lepage3Frederic Di Fiore1,2- 1Normandie Univ, UNIROUEN, Inserm U1245, IRON group, Rouen University Hospital, Normandy Centre for Genomic and Personalized Medicine and Department of Hepatogastroenterology, Rouen, France
- 2Department of Medical Oncology, Henri Becquerel Centre, Rouen, Rouen, France
- 3Burgundy Digestive Cancer Registry, INSERM, Lipides, Nutrition, Cancers (LNC)-UMR1231, University Bourgogne Franche-Comté, Dijon, France
- 4Paris University, Biology Resources Center EPIGENETEC, Paris, France
- 5Department of Digestive Oncology, University Hospital of Reims, Reims, France
- 6Department of Gastroenterology and Digestive Oncology, University Hospital of Saint Etienne, Saint Etienne, France
- 7Department of Radiotherapy and Medical Oncology, Polyclinique Francheville, Périgueux, France
- 8Department of Gastroenterology, St Nazaire Hospital, Saint-Nazaire, France
- 9Department of Pathology, Hôpital Ambroise-Paré, Boulogne-Billancourt, France
- 10Department of Biology, Georges Pompidou Hospital, Assistance Publique des Hôpitaux de Paris (APHP), Paris, France
- 11Department of Pathology, Caen University Hospital, Caen, France
Circulating tumor DNA (ctDNA) is reported to be promising in localized colorectal cancer (CRC). The present study aimed to retrospectively evaluate the impact of ctDNA in patients with a resected stage II CRC from the PROGIGE 13 trial with available paired tumor and blood samples. A group of recurrent patients were matched one-to-one with nonrecurrent patients according to sex, tumor location, treatment sequence, and blood collection timing. CtDNA was analyzed by digital PCR according to NGS of tumors. Disease-free survival (DFS) and overall survival (OS) were analyzed based on ctDNA, and the risks of recurrence and death were determined. A total of 134 patients were included, with 67 patients in each group. At least one alteration was identified in 115/134 tumors. Postoperative ctDNA was detected in 10/111 (9.0%) informative samples and was detected more frequently in the recurrent group (16.7% versus 1.8%; p = 0.02). The median DFS of ctDNA+ versus ctDNA- patients was 16.8 versus 54 months (p = 0.002), respectively, and the median OS was 51.3 versus 69.5 months (p = 0.03), respectively. CtDNA was associated with recurrence (ORa = 11.13, p = 0.03) and death (HRa = 3.15, p = 0.01). In conclusion, the presence of postoperative ctDNA is associated with both recurrence and survival in stage II CRC.
Introduction
Colorectal cancer (CRC) represents the fourth most common cancer worldwide with an incidence rate of more than 1.8 million per year and approximately 800,000 related deaths (1). At first presentation, more than half of patients have localized disease, including 25% with stage II disease (2). For patients with stage II CRC, surgery alone has shown a high rate of cure of approximately 80% (3), and the role of adjuvant chemotherapy (ACT) is controversial, with a reported increase in survival below 5% (4, 5). Until now, there has been a consensus to propose an ACT in selected patients regarding the presence of high-risk features (6), such as a T4 tumor (7, 8), resection of fewer than 12 lymph nodes (8, 9), lymphovascular or perineural invasion (7, 8), poor differentiation (8, 10) and emergency surgery (10). However, it has been established that these factors are not yet sufficient to clearly identify high- versus low-risk patients (11–13), indicating that new factors are needed to improve patient decision-making.
In this context, the detection of circulating tumor DNA (ctDNA) may be a marker of choice (14, 15). CtDNA is potentially released in the bloodstream by tumor cells and harbors the same main alterations as tumor tissue. CtDNA has been recognized as biologically relevant to reflect tumor dynamics in many solid tumors, including the detection of minimal residual disease (MRD) after curative treatment (16). In patients with CRC, ctDNA has been widely investigated in the metastatic setting with studies showing that its value and variations may be clinically relevant for prognosis evaluation as well as treatment monitoring (17–22). While ctDNA released in the metastatic setting is frequently observed in approximately 80-90% of patients (17, 23–25), its detection remains scarce and more challenging in earlier stages with a postoperative ctDNA detection rate ranging from 5 to 30% in studies including localized CRC (26–31) and at a rate at 8.7% in the specific subgroup of stage II CRC in the Tie et al. study (32). While postoperative ctDNA detection has been reported to be associated with prognosis in patients treated for localized stage I-III CRC, its interest in patient decision making has been recently highlighted in the phase II randomized Australian DYNAMIC trial showing that its postoperative detection may guide adjuvant chemotherapy without compromising the risk of recurrence as compared to standard of care (32–34).
In this context, we conducted a matched case–control study to evaluate the impact of postoperative ctDNA detection in a set of stage II CRC patients from the prospective PRODIGE13 trial.
Material and methods
Patients
The present study was conducted based on the prospective French trial, PRODIGE 13, in which 1,925 patients were randomized from 2009 and 2013 into four arms to compare standard versus intensive monitoring as well as the usefulness of the carcinoembryonic antigen (CEA) value in resected stage II and III CRC. Based on a median follow-up of 6.5 years, the 2nd interim analysis results were recently reported without differences in terms of overall survival (OS) between the different strategies (35).
Patients treated for a stage II CRC with a known recurrence during follow-up and with available match paired tumor and blood sample collected after surgery were included in our study. Each recurrent patient with also available tumor and blood sample was then matched one-to-one with a patient without recurrence according to sex, tumor location, neoadjuvant treatment, ACT and the time of sample collection. Patients receiving ACT and/or preoperative chemoradiotherapy (CRT) for rectal tumors were also eligible. Blood samples were optional in the study and were collected after surgery and the timing was not planned. Each patient gave their written consent, and the study was approved by an ethics committee.
Detection of somatic mutations in primary tumor tissue
For each patient, DNA was extracted from archived formalin-fixed-paraffin embedded (FFPE) tumor tissue using the Maxwell 16 FFPE Plus Lev DNA Purification Kit® (Promega®, Fitchburg, Wisconsin, USA). NGS platform was based on AmpliSeq technology and an ion proton sequencer. Libraries were prepared using the colonlungV2 cancer panel. Clonal amplification and sequencing were done on the Ion Chef System (Ion PI Hi-Q Chef, Ion PI Chip Kit v3) and Ion Torrent Proton sequencer (Life Technologies). Data were analyzed by the Torrent Suite 5.0.4 (Life Technologies) using optimized parameters: minimal depth 300×, detection threshold of 2% and 1% for hotspots. Variant call files from the variant caller were loaded on a galaxy platform and annotated using the Safir2report tool (36). NGS coverage depth data were used to identify gene amplifications (in particular ERBB2) using an algorithm developed in the laboratory based on the identification of outliers from the expected coverage mean + 3 standard deviations and calculated using all of the run data (37). For samples with no detected alteration or with an uninterpretable result, a second analysis using another NGS platform was performed based on a QiaSeq targeted custom panel (Qiagen, Hilden, Germany) with 464 amplicons targeting hotspot mutations in CRC on the APC, BRAF, KRAS, NRAS, PIK3CA and TP53 genes. Library was realized using 100 ng of DNA FFPE repaired with NEBNext® FFPE DNA Repair Mix (New England Biolabs). Each sample had a minimal deep sequencing of 500X. Variants were called and annotated by VaScan2, SnpEFF 4.2 and AlamutBatch 1.9. Variant analysis was realized with different database like COSMIC, Clinvar, cBioportal and IARC TP53 database. Selected variants were those either previously described in CRC or class V pathogenic variants.”
Detection of postoperative ctDNA
Blood samples were collected in EDTA tubes and then centrifuged at 1500 g for 15 minutes to obtain plasma aliquots, which were stored at -80°C. CtDNA was extracted from 0.85 to 4.3 mL of plasma using the QIAamp® Circulating Nucleic Acid Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. A fluorometric technique was used to quantify ctDNA concentrations using the Quant-iT dsDNA high-sensitivity assay (Invitrogen, Life Technologies, Carlsbad, CA, USA) and a Twinkle LB970 microplate fluorometer (Berthold Technologies, France). Concentration of extracted ctDNA was very low due to low release from localized tumor. As we previously reported, a pre-amplification was performed with 10 ng of ctDNA using a PCR of 6 cycles with Q5 Hot Start High Fidelity DNA Polymerase (NEB) and a primer/probe mixture (Taqman SNP Genotyping Assay, Life Technologies) (38). CtDNA was analyzed by droplet digital PCR (ddPCR) based on a Qx200® ddPCR System (Bio–Rad®, Hercules, CA, USA) using 2 µL of preamplification, a very sensitive technique that amplify DNA fragment independently in the droplet with probe Taqman®. Quantasoft software was used for profile interpretation. DdPCR on ctDNA targeted one of the main somatic alterations identified in the tumor. In cases with no mutation detected by the NGS method, ctDNA analysis was not performed.
The assays performed for ctDNA detection were considered positive if the amount of ctDNA (variant allelic fraction (VAF)) was exceeded a predefined limit of detection (LOD). The threshold of positivity for each of the assays was determined from ctDNA extracted from 12 healthy plasma controls using the following equation: LOD = mean VAF + 1.645 x standard deviation.
Statistical analysis
The primary objective was to compare the ctDNA detection rate between the recurrent and nonrecurrent matched groups. The secondary objectives were to analyze characteristics of ctDNA+ and ctDNA- patients and evaluate the impact of ctDNA status on OS and disease-free survival (DFS). Patient data were prospectively monitored by the French Federation of Digestive Oncology (FFCD) for the PRODIGE 13 trial. For the purpose of the study, the group of cases was defined as patients with documented disease recurrence during follow-up and available tumor and plasm samples (recurrent group), and each of them was matched one-to-one with patients without recurrence (nonrecurrent group) according to sex, tumor location, neoadjuvant treatment, ACT and the time of sample collection.
The analysis between two groups was performed using Pearson’s chi-squared test, Yate’s continuity correction of the chi-squared test or Fischer’s exact as appropriate. Quantitative variables were compared using an unpaired Student’s t test with Welch’s correction or a Wilcoxon signed ranks test for paired samples. DFS and OS were analyzed using the Kaplan– Meier method and compared with the log rank test. Multivariate analysis of factors associated with the risk of recurrence and death from any cause was performed using logistic regression and a Cox model, respectively, including variables identified in univariate analysis with a p value ≤ 0.10. All statistical tests were two-sided, and statistical significance was set at 0.05. Statistical analyses were performed using SAS 4.0 (SAS Institute Inc., Cary, NC, USA) and R studio version 1.72 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
A total of 134 stage II patients with available paired blood and tumor samples were included with 67 patients in each of the recurrent and nonrecurrent groups corresponding to 13% of the entire population of stage II from the PRODIGE 13 trial (134/1,045). As shown in Figure 1, 126/134 tumors were successfully analyzed by NGS with at least one somatic mutation detected in 115/126 (91.3%). Among the 115 remaining patients, 111 had an informative blood sample, including 54 in the recurrent group and 57 in the matched nonrecurrent group. ACT was performed in 46 patients (41.4%), including 22 (40.7%) and 24 (42.1%) patients in the recurrent and nonrecurrent groups, respectively. For patients with rectal cancer, CRT was performed in 15 cases (60%), corresponding to 10 (76.9%) and 5 (41.7%) patients in the recurrent and nonrecurrent groups, respectively.
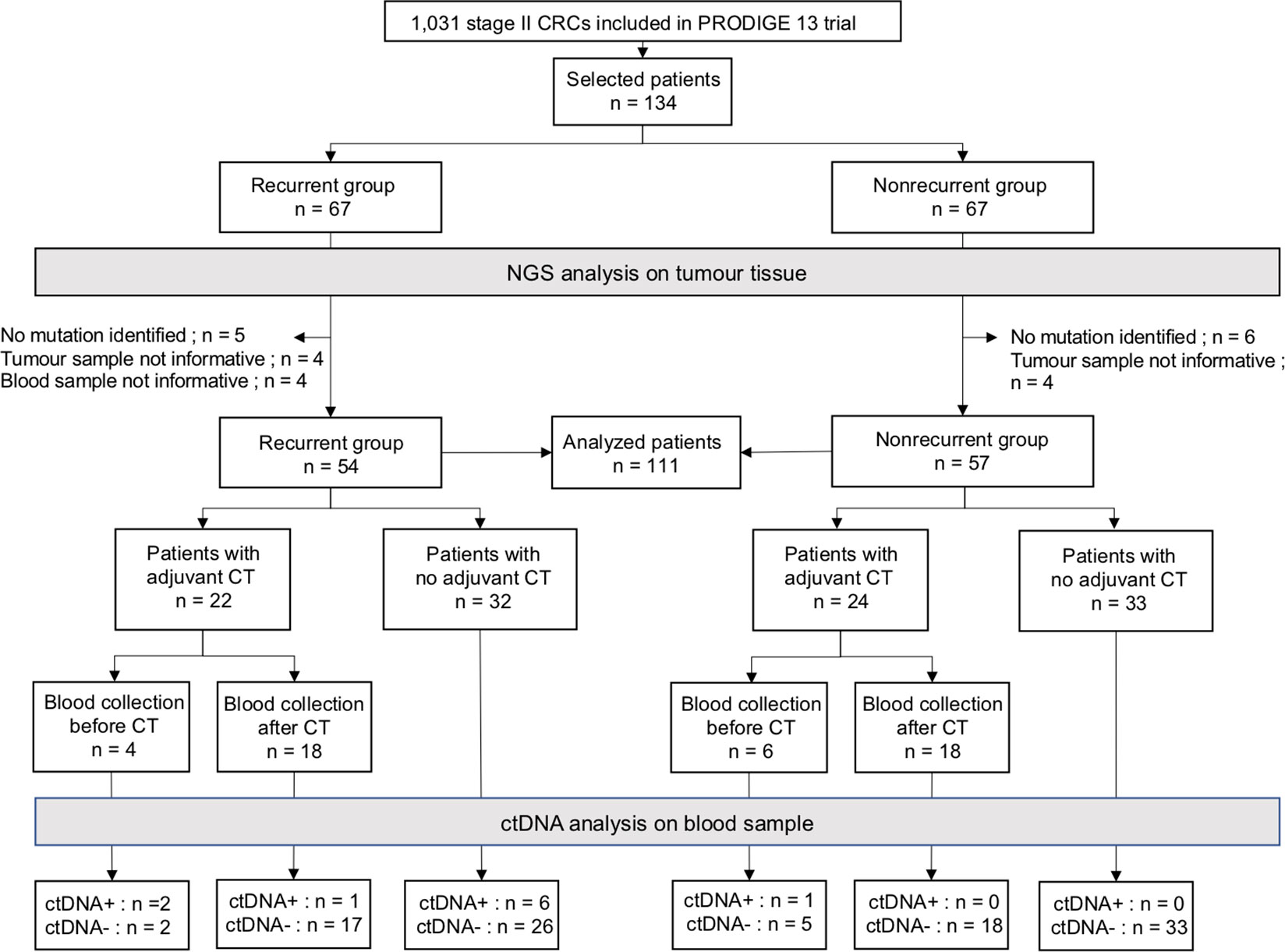
Figure 1 Flow chart of the study population. The overall population consisted of 134 patients with 67 in recurrent and matched nonrecurrent patients. The analysis of ctDNA was based on DNA somatic alterations from tumors detected using two successive NGS panels. At least one alteration was detected in 79/113 patients using the first NGS and in 36/55 remaining patients with the second NGS panel. A total of 115/134 tumors were identified with at least one alteration, corresponding to 58 and 57 patients in the recurrent and nonrecurrent group, respectively. For each patient, ctDNA detection was performed using ddPCR analysis targeting alterations identified with NGS. Timing of blood sample collection was also indicated according to chemotherapy initiation if chemotherapy was used. CRCs, colorectal cancers; CT, chemotherapy; ctDNA, circulating tumor DNA.
The main characteristics of the patients are shown in Table 1. As expected, no difference was observed for variables used for matching. Furthermore, no difference was found between the two groups in age, emergency surgery, tumor differentiation or the level of postoperative carcinoembryonic antigen (CEA). Moreover, patients with T4 tumors were more frequent in the recurrent group than in the nonrecurrent group (p=0.04). The median time from surgery to blood collection was 81 and 99 days in the recurrent and nonrecurrent groups, respectively (p=0.53).
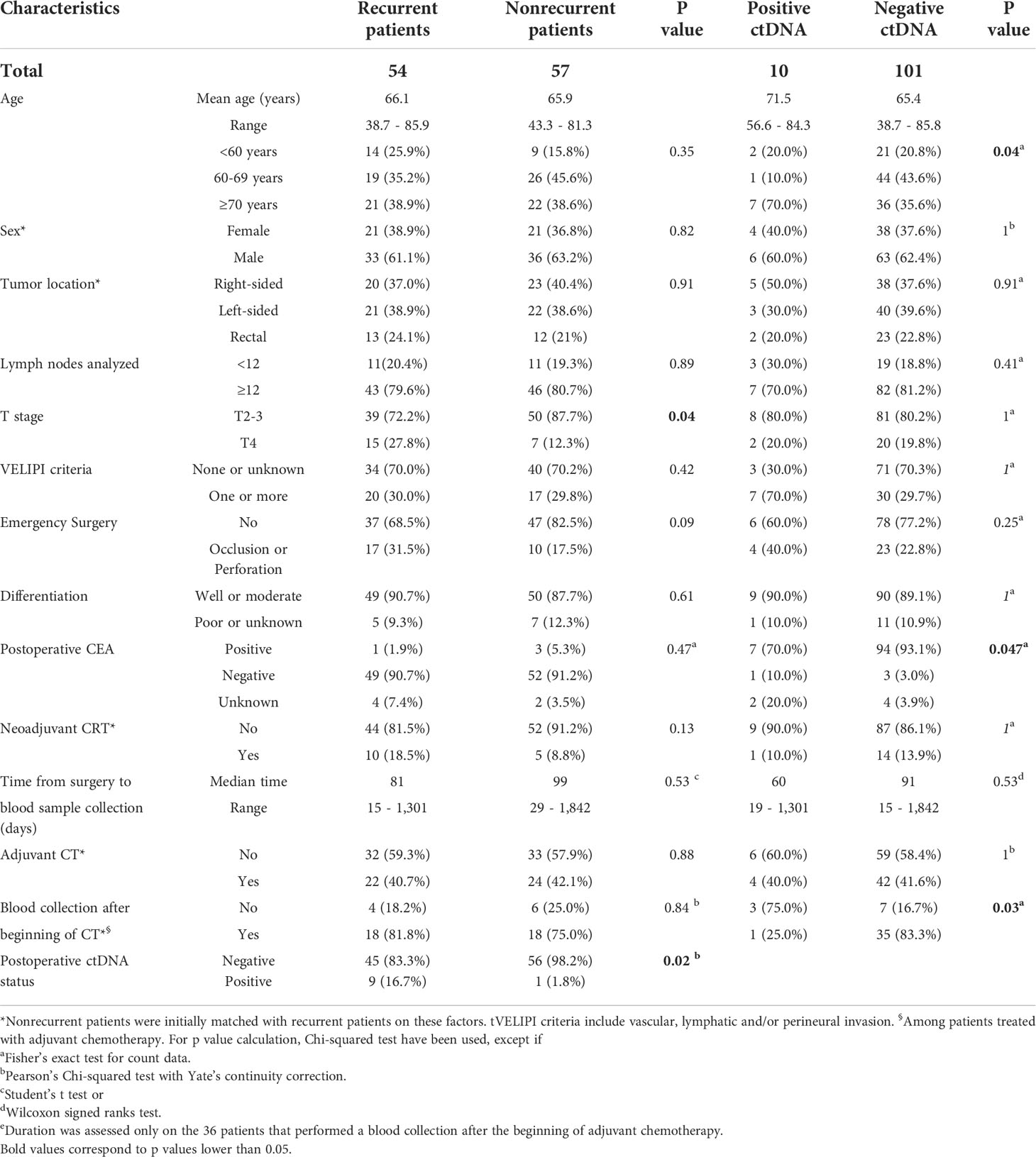
Table 1 Main characteristics of stage II CRC resected patients included in the study.
CtDNA detection rate and characteristics
Postoperative ctDNA was detected in 10/111 of all patients (9%), and it was significantly more frequent in the recurrent group than in the nonrecurrent group with 9/54 (16.7%) ctDNA+ versus 1/57 (1.8%) ctDNA+ patients (p=0.02). The characteristics of the somatic alterations are listed in Table 2 for ctDNA+ patients and Table 1S for all patients (see Supplementary Data). KRAS c.35G>A was the most frequent circulating mutation (40%). The variant allele fraction (VAF) was between 0.02% and 15.9% but mostly below 1% (70%), and the median VAF was 0.22% (Table 2). Moreover, we analyzed the main somatic mutation detected by NGS in tumor tissue. Comparing ctDNA+ to ctDNA- patients, KRAS mutation was found in 70% vs 42%, BRAF in 20% vs 3%, and TP53 in 10% vs 42%, respectively. Postoperative ctDNA was detected in 14.3% of KRAS-mutated patients, 40% of BRAF-mutated patients, and 2% of TP53-mutated patients (see Table 2S in Supplementary Data).
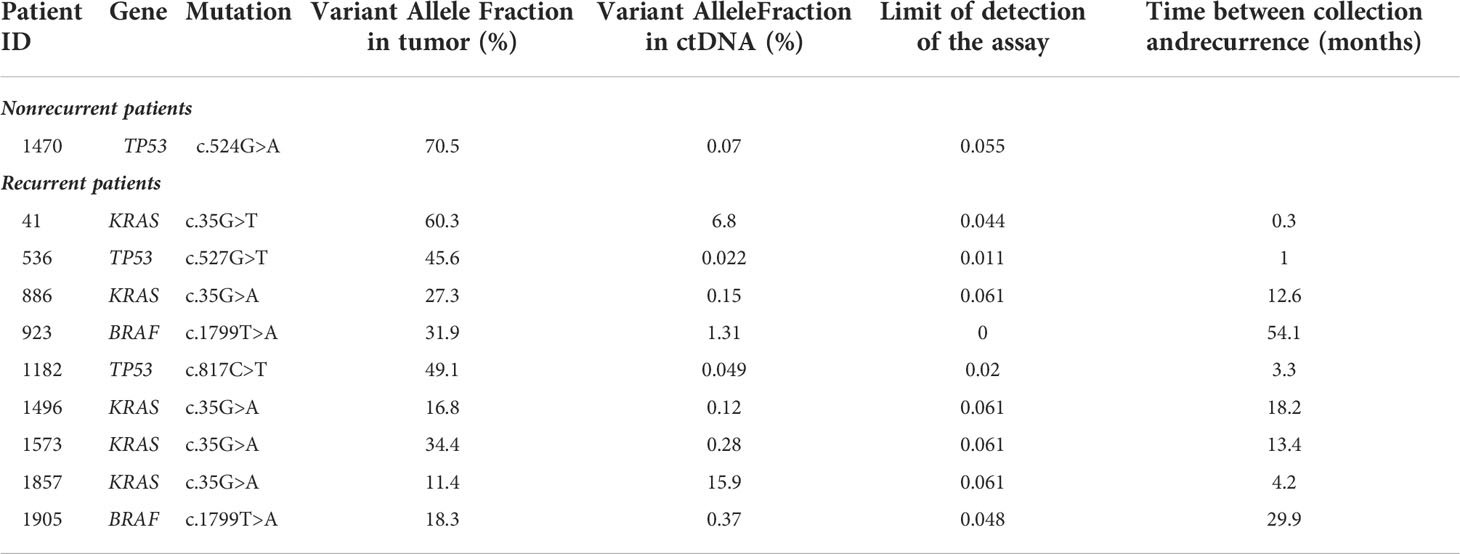
Table 2 Mutations and variant allele fractions detected in post-operative ctDNA+ patients.
As shown in Table 1, the presence of postoperative ctDNA was more frequently observed in patients older than 70 years (p=0.03) without a significant difference for other variables, except for postoperative CEA level. No significant difference was found concerning the median time from surgery to blood collection between ctDNA+ (60 days) and ctDNA- patients (91 days) (p=0.53). Among the 10 ctDNA+ patients, the median time between resection and blood sample collection was less than 2 months in 50% of patients, from 2 to 6 months in 20% of patients and more than 6 months in 30% of patients. Among patients treated with ACT (46/111, 41.4%), postoperative ctDNA was more frequently detected when blood samples were collected before (3/10, 30%) than after CT initiation (1/36, 2.8%) (p=0.03). Regarding the 9 ctDNA+ patients from the recurrent group, the median time was 12.8 months from blood collection to clinical recurrence (Table 2 and Figure 1S in Supplementary Data).
CtDNA and prognosis
The presence of postoperative ctDNA was significantly associated with survival in the whole population. The median DFS was 16.8 versus 54 months in ctDNA+ and ctDNA- patients (p=0.002), corresponding to a 3-year DFS of 30% versus 62.1%, respectively. The median OS was 51.3 versus 69.5 months in ctDNA+ and ctDNA- patients, respectively (p=0.03) (Figures 2A,B). The presence of postoperative ctDNA was also identified as an independent factor associated with the risk of recurrence in univariate analysis and multivariate analysis [OR=11.20 (95% CI: 1.37-91.71, p=0.02); and adjusted OR (ORa)= 11.13 (95% CI: 1.33-92.91; p=0.03)] (Table 3). The presence of postoperative ctDNA was also an independent factor associated with the risk of death in univariate and multivariate analyses [HR = 2.57 (95% CI: 1.07-6.18, p=0.03)] and adjusted HR [HRa = 3.15 (95% CI: 1.28-7.74; p=0.01)] (Table 4).
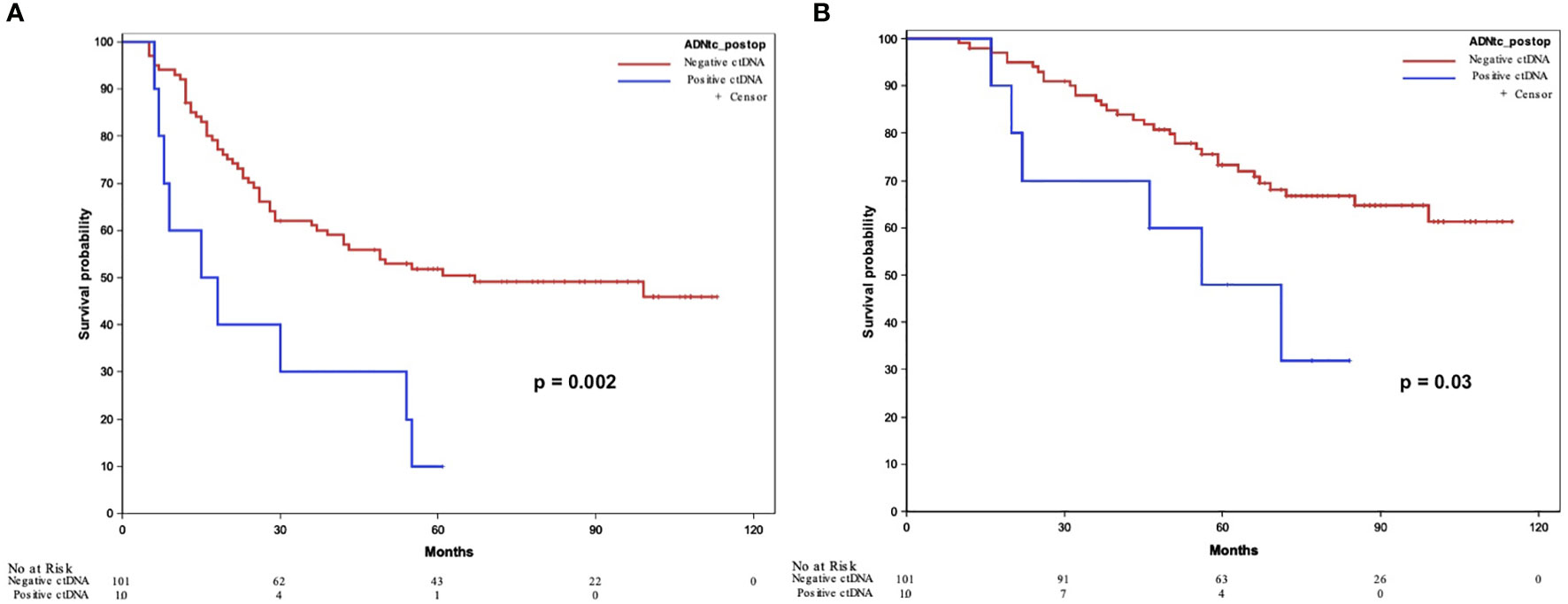
Figure 2 Disease-free survival (A) and overall survival (B) according to ctDNA detection. ctDNA, circulating tumor DNA.
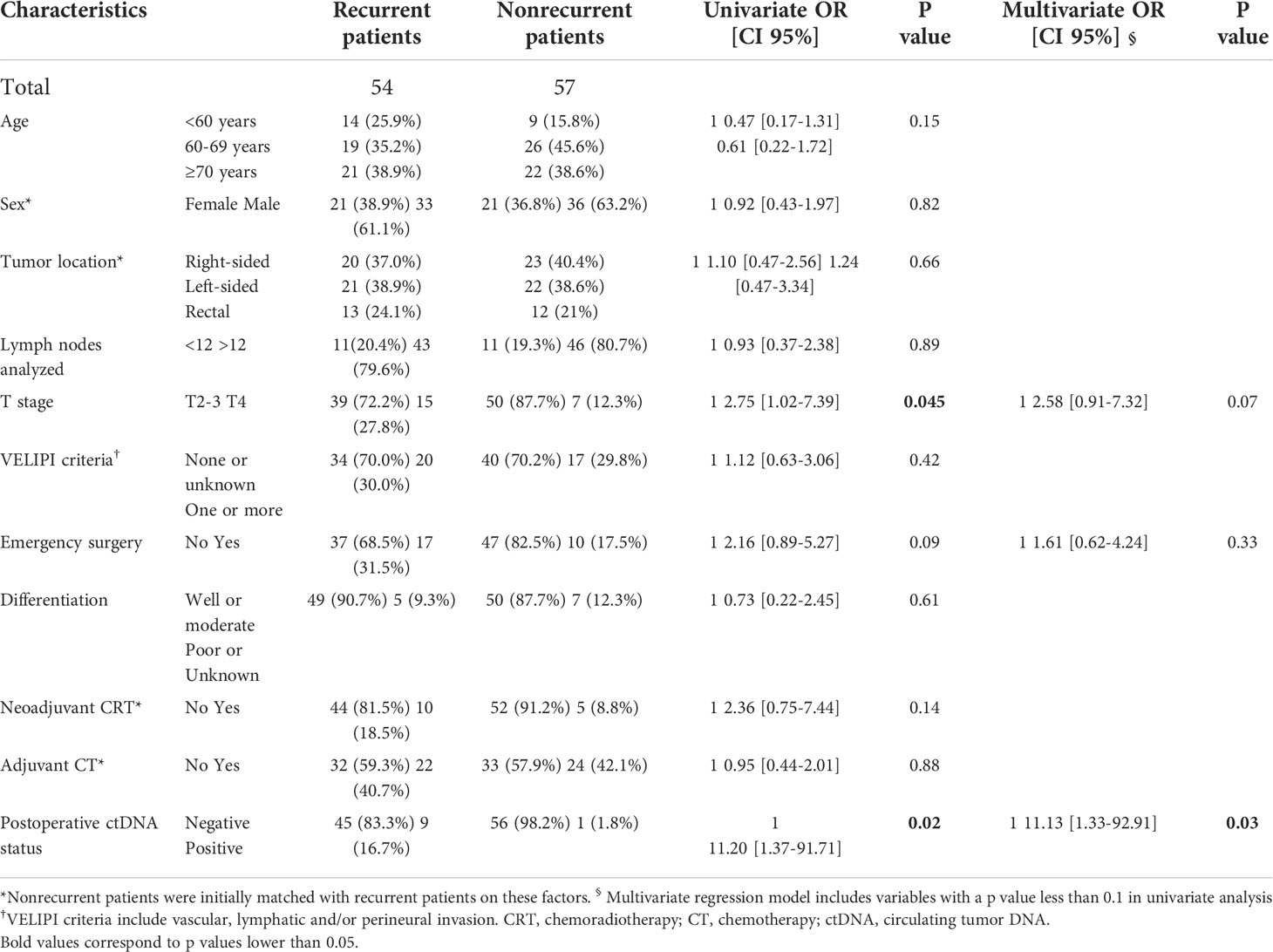
Table 3 Logistic regression (univariate and multivariate) assessing the impact of main characteristics on the risk of recurrence (reference: nonrecurrent patients).
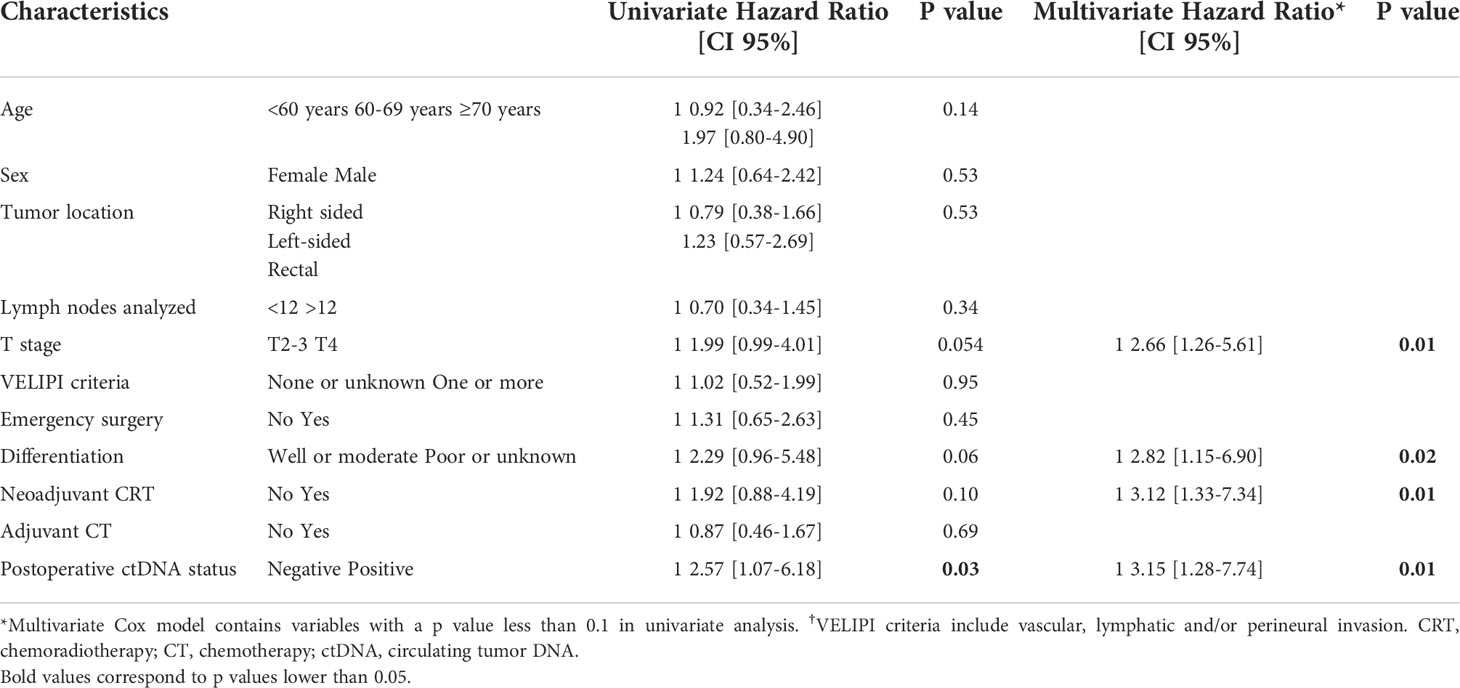
Table 4 Cox model assessing the impact of postoperative ctDNA status and other characteristics on overall survival.
Discussion
Our results showed that the presence of postoperative ctDNA was significantly associated with the risk of recurrence and shorter DFS and OS in stage II CRC patients. Using a specific ddPCR assay targeting the main alteration detected with NGS methods in tumor DNA, we detected postoperative ctDNA in 9.0% of all patients, and ctDNA was shown to be 9-fold more frequent in the recurrent group than in the nonrecurrent group (16.7% vs. 1.8%, p=0.02). Interestingly, we observed a median time of 12.8 months between ctDNA detection and the diagnosis of disease recurrence. Our results also highlighted that ctDNA status significantly impacted survival with a median DFS of 16.8 versus 54 months (p=0.002) and a median OS of 51.3 versus 69.5 months (p=0.03) in ctDNA+ and ctDNA- patients, respectively. Moreover, the presence of ctDNA was identified as an independent factor associated with the risk of recurrence and death with an adjusted OR of 11.13 (CI 95%:1.33-92.91; p=0.03) and an adjusted HR of 3.15 (CI 95%:1.28-7.74; p=0.01), respectively. Taken together, these results suggested that postoperative ctDNA detection may be a relevant marker to identify high versus low risk of disease recurrence in stage II patients.
The overall rate of postoperative ctDNA+ at 9.0% in our work was similar to previously reported data in stage II and III CRC, ranging from 5.8 to 15%. Indeed, using mixed ddPCR targeting tumor mutations or methylation markers, a recent study that included both stage IIIII patients has reported ctDNA detection at Day 5 after surgery in 6/102 (5.8%) patients in the stage II patient subgroup (39). Using a similar approach to the present study, Tie et al. reported that 20/230 (8.7%) patients were identified as ctDNA positive in their first cohort and 45/299 (15%) in the experimental arm of the DYMAMIC trial (32, 34). In these studies, the rate of postoperative ctDNA was also significantly increased in patients with disease recurrence ranging from 44% to 58%, and in a higher rate than in our work probably due to preanalytical considerations (34, 39). Taken together, these results suggest that postoperative ctDNA is a relatively rare event in localized disease that can be detected in approximately in 10 to 15% of all patients treated for stage II CRC and more frequently in patients with high risk of disease recurrence. However, the exact rate of ctDNA release and its mechanisms need to be further investigated in larger series, including appropriate and dedicated preanalytical processes.
Determining the most appropriate approach for ctDNA detection in early CRC remains challenging, and several factors that may influence the results, such as preanalytical parameters, assay characteristics and the treatment sequence (40). Regarding ctDNA assays, the use of an ultrasensitive method for ctDNA detection, such as a ddPCR assay targeting somatic alterations identified by NGS on tumor DNA, is considered the most efficient. Based on an NGS analysis potentialized with two panels of targeted genes, a somatic alteration was successfully identified in 115/134 (86%) of all tumors, which is close to results reported in the localized CRC stage by Tarazona et al. (132/150, 88%) (27) and Tie et al. (230/250, 92%) (32).
The timing of blood sample collection may also be an important factor to be considered. In our study, ACT was performed in approximately 40% of patients (22/54 in the recurrent group and 24/57 in the nonrecurrent group) on a sample collected after the start of CT in most cases (18/22 and 18/24, respectively). In this setting, we found that ctDNA was more frequently detected before than after ACT initiation (30% vs. 2.8%, respectively) (p=0.03). This finding was in accordance with knowledge about ctDNA kinetics, which is described to change according to treatment sequences, such as from pre- to postsurgery as well as from the start to the end of postoperative CT (31, 41). For example, Chen et al. studied 91 patients treated with perioperative CT and surgery for CRC liver metastasis, and they detected ctDNA in 88% of patients before neoadjuvant CT, in 57% of patients before surgery and in 41% of patients in the postoperative setting (31). Using serial monitoring during ACT in 6 patients with detectable postoperative ctDNA, Tie et al. also showed a complete decrease during the treatment sequence, both in recurrent and nonrecurrent cases. Furthermore, in a study including stage II-III CRC, the detection of ctDNA was observed in 49/178 (27.5%) in the preoperative setting and in 15/171 (10.5%) at Day 5 after surgery, both associated with time to disease recurrence with HRa of 3.58 and 3.22, respectively. Although the best timing for ctDNA detection remains unclear in patients with localized and/or resectable CCR, the postoperative period ranging from 4-8 weeks and the end of ACT are considered the two most relevant time points for the analysis of the prognostic impact of ctDNA detection (29, 31, 32, 34).
We found that ctDNA was found to be significantly associated with DFS, OS and risk of recurrence or death in multivariate analysis. These findings were in accordance with previous data on localized CRC (26, 27, 29, 31) as well as in the only study focusing on stage II (32–34).
This impact on prognosis also translated to the 3-year DFS, which was 30% and 62.1% in the ctDNA+ and ctDNA- patients, respectively, which agreed with the results reported by Tie et al. with a 3-year DFS of 0% and 90%, respectively (32). Interestingly in our work, we also observed that ctDNA detection may precede the diagnosis of disease recurrence using regular follow-up with a median time of 12.8 months, which also agreed with previous findings showing that a ctDNA-positive sample may anticipate imaging evidence of recurrence for at least 3 months (32–35). All these data highlighted that ctDNA is a relevant marker in localized CRC and that its use in routine basis needs to be investigated by prospective trials. In this context, the recent phase II randomized DYMAMIC trial randomized 455 patients to assess whether ctDNA-guided approach could be used for ACT decision without compromising the risk of recurrence as compared to standard of care non ctDNA-guided. The study met its primary endpoint with a non-inferiority in the 2 years recurrence between ctDNA-guided ACT and standard management, respectively 93.5 vs 92.4% (34). Until now, many trials are in progress in localized CRC and the results are awaited to provide additional validation of the ctDNA-guided strategy to individualize adjuvant chemotherapy (42).
The main limitation of the present study was its retrospective design. However, to minimize this limitation, we designed a case–control study with matching according to sex, tumor location, treatment sequence and timing of blood collection. Moreover, these two groups were formed based on the PRODIGE 13 prospective randomized trial and according to the planned prospective follow-up. The other limitations involved the nonstandardized preanalytical process, the presence of only one available and noncodified sample per patient and the use of ACT. Nevertheless, to circumvent these limitations, we specifically designed a molecular assay based on a two-step method using NGS from tumor DNA and dedicated ddPCR for ctDNA detection. Moreover, all these determinant factors involved in the sensitivity of the ctDNA detection rate need to be considered and are now integrated in all ongoing prospective trials. In conclusion, the present study highlighted that the presence of postoperative ctDNA is associated with a higher risk of recurrence and death and shorter DFS and OS in resected stage II CRC.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics statement
This work is an ancillary study from the PRODIGE13 trial, registered on the clinicaltrials.gov website (No. NCT00995202). Each patient included in the PRODIGE13 trial gave written consent. PRODIGE13 was authorized by AFSSAPS (Agence Française de Sécurité Sanitaire des Produits de Santé; No. 2009-A00536-51) on 22/06/2009. The study was performed in accordance with the Declaration of Helsinki. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
FF, SM, C-BL, KL, PM, and DS designed the study research; OB, J-MP, C-BL, and PD included a large number of patients; LB, CM, SC, J-FE, PL-P, FB, and NS-V performed the molecular analysis; AG, FF, KL, SM, MD, and VV contributed to data analysis and interpretation; and AG, FF, LB, DS, KL, SM, and C-BL wrote the paper. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the FARE funding from SNFGE (Société Nationale Française de Gastro-Entérologie).
Acknowledgments
This study used data collected by the French Digestive Cancerology Federation (FFCD).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.973167/full#supplementary-material
Supplementary Figure 1 | Timeline of patients with positive ctDNA. For recurrent patients, the precise time between blood collection and recurrence is shown in . Blue diamond = date of surgery; red point = date of blood sample; purple arrow = date of recurrence; green square = date of CT starting; blue line = last date of follow-up; and black arrow = date of death.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2018) 68:394–424. doi: 10.3322/caac.21492
2. Meng R, Venugopal K, Thomas H, D’Onise K. Cancer staging at diagnosis data comparisons in south Australia. Sci Rep (2020) 10:1008. doi: 10.1038/s41598-020-57704-5
3. Lacy AM, Delgado S, Castells A, Prins HA, Arroyo V, Ibarzabal A, et al. The long-term results of a randomized clinical trial of laparoscopy-assisted versus open surgery for colon cancer. Ann Surg (2008) 248:1–7. doi: 10.1097/SLA.0b013e31816a9d65
4. Quasar Collaborative Group, Gray R, Barnwell J, McConkey C, Hills RK, Williams NS, et al. Adjuvant chemotherapy versus observation in patients with colorectal cancer: A randomised study. Lancet (2007) 370:2020–9. doi: 10.1016/S0140-6736(07)61866-2
5. Cunningham D, Atkin W, Lenz H-J, Lynch HT, Minsky B, Nordlinger B, et al. Colorectal cancer. Lancet (2010) 375:1030–47. doi: 10.1016/S0140-6736(10)60353-4
6. Argilés G, Tabernero J, Labianca R, Hochhauser D, Salazar R, Iveson T, et al. Localised colon cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2020) 31:1291–305. doi: 10.1016/j.annonc.2020.06.022
7. Quah H-M, Chou JF, Gonen M, Shia J, Schrag D, Landmann RG, et al. Identification of patients with high-risk stage II colon cancer for adjuvant therapy. Dis Colon Rectum (2008) 51:503–7. doi: 10.1007/s10350-0089246-z
8. Niedzwiecki D, Bertagnolli MM, Warren RS, Compton CC, Kemeny NE, Benson AB, et al. Documenting the natural history of patients with resected stage II adenocarcinoma of the colon after random assignment to adjuvant treatment with edrecolomab or observation: Results from CALGB 9581. J Clin Oncol (2011) 29:3146–52. doi: 10.1200/JCO.2010.32.5357
9. Wells KO, Hawkins AT, Krishnamurthy DM, Dharmarajan S, Glasgow SC, Hunt SR, et al. Omission of adjuvant chemotherapy is associated with increased mortality in patients with T3N0 colon cancer with inadequate lymph node harvest. Dis Colon Rectum (2017) 60:15–21. doi: 10.1097/DCR.0000000000000729
10. Benson AB, Schrag D, Somerfield MR, Cohen AM, Figueredo AT, Flynn PJ, et al. American Society of clinical oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol (2004) 22:3408–19. doi: 10.1200/JCO.2004.05.063
11. André T, Boni C, Navarro M, Tabernero J, Hickish T, Topham C, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol (2009) 27:3109–16. doi: 10.1200/JCO.2008.20.6771
12. Teixeira L, Hickish T, Tournigand C, Bachet J, Bonetti A, Rivera F, et al. Efficacy of FOLFOX4 as adjuvant therapy in stage II colon cancer (CC): A new analysis of the MOSAIC trial according to risk factors. JCO (2010) 28:3524–4. doi: 10.1200/jco.2010.28.15_suppl.3524
13. O’Connor ES, Greenblatt DY, LoConte NK, Gangnon RE, Liou J-I, Heise CP, et al. Adjuvant chemotherapy for stage II colon cancer with poor prognostic features. J Clin Oncol (2011) 29:3381–8. doi: 10.1200/JCO.2010.34.3426
14. Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, et al. Circulating mutant DNA to assess tumor dynamics. Nat Med (2008) 14:985–90. doi: 10.1038/nm.1789
15. Takemasa I, Hamabe A, Ishii M. Perspectives for circulating tumor DNA in clinical management of colorectal cancer. Int J Clin Oncol (2021) 26:1420–30. doi: 10.1007/s10147-021-01937-5
16. Dasari A, Grothey A, Kopetz S. Circulating tumor DNA-defined minimal residual disease in solid tumors: Opportunities to accelerate the development of adjuvant therapies. J Clin Oncol (2018) 36:3437–40. doi: 10.1200/JCO.2018.78.9032
17. Tie J, Kinde I, Wang Y, Wong HL, Roebert J, Christie M, et al. Circulating tumor DNA as an early marker of therapeutic response in patients with metastatic colorectal cancer. Ann Oncol (2015) 26:1715. doi: 10.1093/annonc/mdv177
18. Kitahara M, Hazama S, Tsunedomi R, Takenouchi H, Kanekiyo S, Inoue Y, et al. Prediction of the efficacy of immunotherapy by measuring the integrity of cell-free DNA in plasma in colorectal cancer. Cancer Sci (2016) 107:1825–9. doi: 10.1111/cas.13085
19. Herbst A, Vdovin N, Gacesa S, Ofner A, Philipp A, Nagel D, et al. Methylated free-circulating HPP1 DNA is an early response marker in patients with metastatic colorectal cancer. Int J Cancer (2017) 140:2134–44. doi: 10.1002/ijc.30625
20. Garlan F, Laurent-Puig P, Sefrioui D, Siauve N, Didelot A, Sarafan-Vasseur N, et al. Early evaluation of circulating tumor DNA as marker of therapeutic efficacy in metastatic colorectal cancer patients (PLACOL study). Clin Cancer Res (2017) 23:5416–25. doi: 10.1158/1078-0432.CCR-16-3155
21. Parikh AR, Mojtahed A, Schneider JL, Kanter K, Van Seventer EE, Fetter IJ, et al. Serial ctDNA monitoring to predict response to systemic therapy in metastatic gastrointestinal cancers. Clin Cancer Res (2020) 26:1877–85. doi: 10.1158/1078-0432.CCR-19-3467
22. Sefrioui D, Beaussire L, Gillibert A, Blanchard F, Toure E, Bazille C, et al. CEA, CA19-9, circulating DNA and circulating tumour cell kinetics in patients treated for metastatic colorectal cancer (mCRC). Br J Cancer (2021) 125:725–33. doi: 10.1038/s41416-021-01431-9
23. Bettegowda C, Sausen M, Leary RJ, Kinde I, Wang Y, Agrawal N, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med (2014) 6:224ra24. doi: 10.1126/scitranslmed.3007094
24. Lin J-K, Lin P-C, Lin C-H, Jiang J-K, Yang S-H, Liang W-Y, et al. Clinical relevance of alterations in quantity and quality of plasma DNA in colorectal cancer patients: based on the mutation spectra detected in primary tumors. Ann Surg Oncol (2014) 21 Suppl 4:S680–686. doi: 10.1245/s10434-014-3804-5
25. Kim ST, Lee W-S, Lanman RB, Mortimer S, Zill OA, Kim K-M, et al. Prospective blinded study of somatic mutation detection in cell-free DNA utilizing a targeted 54-gene next generation sequencing panel in metastatic solid tumor patients. Oncotarget (2015) 6:40360–9. doi: 10.18632/oncotarget.5465
26. Schøler LV, Reinert T, Ørntoft M-BW, Kassentoft CG, Árnadóttir SS, Vang S, et al. Clinical implications of monitoring circulating tumor DNA in patients with colorectal cancer. Clin Cancer Res (2017) 23:5437–45. doi: 10.1158/1078-0432.CCR-17-0510
27. Tarazona N, Gimeno-Valiente F, Gambardella V, Zuñiga S, Rentero-Garrido P, Huerta M, et al. Targeted next-generation sequencing of circulating-tumor DNA for tracking minimal residual disease in localized colon cancer. Ann Oncol (2019) 30:1804–12. doi: 10.1093/annonc/mdz390
28. Wang Y, Li L, Cohen JD, Kinde I, Ptak J, Popoli M, et al. Prognostic potential of circulating tumor DNA measurement in postoperative surveillance of nonmetastatic colorectal cancer. JAMA Oncol (2019) 5:1118–23. doi: 10.1001/jamaoncol.2019.0512
29. Reinert T, Henriksen TV, Christensen E, Sharma S, Salari R, Sethi H, et al. Analysis of plasma cell-free DNA by ultradeep sequencing in patients with stages I to III colorectal cancer. JAMA Oncol (2019) 5:1124–31. doi: 10.1001/jamaoncol.2019.0528
30. Musher BL, Melson JE, Amato G, Chan D, Hill M, Khan I, et al. Evaluation of circulating tumor DNA for methylated BCAT1 and IKZF1 to detect recurrence of stage II/Stage III colorectal cancer (CRC). Cancer Epidemiol Biomarkers Prev (2020) 29:2702–9. doi: 10.1158/1055-9965.EPI-20-0574
31. Chen G, Peng J, Xiao Q, Wu H-X, Wu X, Wang F, et al. Postoperative circulating tumor DNA as markers of recurrence risk in stages II to III colorectal cancer. J Hematol Oncol (2021) 14:80. doi: 10.1186/s13045-021-01089-z
32. Tie J, Wang Y, Tomasetti C, Li L, Springer S, Kinde I, et al. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci Transl Med (2016) 8:346ra92. doi: 10.1126/scitranslmed.aaf6219
33. Tie J, Cohen JD, Lo SN, Wang Y, Li L, Christie M, et al. Prognostic significance of postsurgery circulating tumor DNA in nonmetastatic colorectal cancer: Individual patient pooled analysis of three cohort studies. Int J Cancer (2021) 148:1014–26. doi: 10.1002/ijc.33312
34. Tie J, Cohen JD, Lahouel K, Lo SN, Wang Y, Kosmider S, et al. Circulating tumor DNA analysis guiding adjuvant therapy in stage II colon cancer. N Engl J Med (2022) 386:2261–72. doi: 10.1056/NEJMoa2200075
35. Lepage C, Phelip J-M, Cany L, Faroux R, Manfredi S, Ain J-F, et al. Effect of 5 years of imaging and CEA follow-up to detect recurrence of colorectal cancer: The FFCD PRODIGE 13 randomised phase III trial. Dig Liver Dis (2015) 47:529–31. doi: 10.1016/j.dld.2015.03.021
36. Digan W, Countouris H, Barritault M, Baudoin D, Laurent-Puig P, Blons H, et al. An architecture for genomics analysis in a clinical setting using galaxy and docker. Gigascience (2017) 6:1–9. doi: 10.1093/gigascience/gix099
37. Legras A, Barritault M, Tallet A, Fabre E, Guyard A, Rance B, et al. Validity of targeted next-generation sequencing in routine care for identifying clinically relevant molecular profiles in non-Small-Cell lung cancer: Results of a 2-year experience on 1343 samples. J Mol Diagn (2018) 20:550–64. doi: 10.1016/j.jmoldx.2018.04.002
38. Sefrioui D, Mauger F, Leclere L, Beaussire L, Di Fiore F, Deleuze J-F, et al. Comparison of the quantification of KRAS mutations by digital PCR and e-ice-COLD-PCR in circulating-cell-free DNA from metastatic colorectal cancer patients. Clin Chim Acta (2017) 465:1–4. doi: 10.1016/j.cca.2016.12.004
39. Benhaim L, Bouché O, Normand C, Didelot A, Mulot C, Le Corre D, et al. Circulating tumor DNA is a prognostic marker of tumor recurrence in stage II and III colorectal cancer: multicentric, prospective cohort study (ALGECOLS). Eur J Cancer (2021) 159:24–33. doi: 10.1016/j.ejca.2021.09.004
40. Dasari A, Morris VK, Allegra CJ, Atreya C, Benson AB, Boland P, et al. ctDNA applications and integration in colorectal cancer: An NCI colon and rectal-anal task forces whitepaper. Nat Rev Clin Oncol (2020) 17:757–70. doi: 10.1038/s41571-020-0392-0
41. Tie J, Wang Y, Cohen J, Li L, Hong W, Christie M, et al. Circulating tumor DNA dynamics and recurrence risk in patients undergoing curative intent resection of colorectal cancer liver metastases: A prospective cohort study. PloS Med (2021) 18:e1003620. doi: 10.1371/journal.pmed.1003620
Keywords: circulating tumor DNA, liquid biopsy, colorectal cancer, stage II, next generation sequencing
Citation: Grancher A, Beaussire L, Manfredi S, Le Malicot K, Dutherage M, Verdier V, Mulot C, Bouché O, Phelip J-M, Levaché C-B, Deguiral P, Coutant S, Sefrioui D, Emile J-F, Laurent-Puig P, Bibeau F, Michel P, Sarafan-Vasseur N, Lepage C and Di Fiore F (2022) Postoperative circulating tumor DNA detection is associated with the risk of recurrence in patients resected for a stage II colorectal cancer. Front. Oncol. 12:973167. doi: 10.3389/fonc.2022.973167
Received: 19 June 2022; Accepted: 17 October 2022;
Published: 10 November 2022.
Edited by:
Claudia Cardone, G. Pascale National Cancer Institute Foundation (IRCCS), ItalyReviewed by:
Francesco Pepe, University of Naples Federico II, ItalyIvan Dr. Jelas, Charité Universitätsmedizin Berlin, Germany
Copyright © 2022 Grancher, Beaussire, Manfredi, Le Malicot, Dutherage, Verdier, Mulot, Bouché, Phelip, Levaché, Deguiral, Coutant, Sefrioui, Emile, Laurent-Puig, Bibeau, Michel, Sarafan-Vasseur, Lepage and Di Fiore. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adrien Grancher, Z3JhbmNoZXIuYWRyQGdtYWlsLmNvbQ==