 Theresa Guo
Theresa Guo Stephen Y. Kang2
Stephen Y. Kang2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Oncol., 18 August 2022
Sec. Head and Neck Cancer
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.966899
This article is part of the Research TopicConsiderations in the Surgical Management of HPV-Positive Oropharyngeal Squamous Cell CarcinomaView all 8 articles
In the recent years, the prevalence of HPV-positive oropharyngeal squamous cell carcinoma (OPSCC) has increased significantly. Currently, nearly 80-90% of all oropharynx tumors are HPV-positive. In addition, it is now recognized that HPV-positive tumor status is associated with good prognosis and improved response to chemoradiation. However, within this setting, there are still patients with HPV-positive OPSCC who will experience recurrence. With the increasing incidence of HPV-mediated OPSCC, recurrent HPV disease is also becoming more prevalent and there is an increasing need to understand the unique presentation and treatment of recurrent HPV-mediated disease. In this review, we will discuss epidemiology of recurrent HPV-positive OPSCC, role of surgical salvage, re-irradiation, and the role of upcoming novel treatments and immunotherapy. Historically, recurrent oropharyngeal disease has been associated with poor prognosis and high morbidity. However, recent advances have transformed the landscape for salvage treatment of HPV-mediated OPSCC. Liquid biomarkers offer potential for early detection of recurrence, robotic techniques may reduce morbidity of surgical salvage, improvements in re-irradiation approaches reduce toxicities, and novel immune based therapies on the horizon are offering promising results. These advances combined with the improved prognosis of HPV-positive disease offer to transform our approach to recurrent disease of the oropharynx.
Despite the improved prognosis conferred by human papillomavirus (HPV)-positive tumor status, recurrences and distant failures still occur in this population with progression free survival of 72-74% at 3-years (1, 2). Recurrence rates in HPV-positive oropharyngeal squamous cell carcinoma (OPSCC) patients are about half that of HPV-negative patients, with respect to both locoregional and distant failure. Results from RTOG 0522 showed that in HPV-positive compared to HPV-negative patients, 3-year locoregional failure rates were 17.3% vs 32.5% (P <.001) and distant metastatic rates were 6.5% vs. 17.0% (p=.005) (2). Recurrences tend to occur later in HPV-positive patients (3), but regardless of HPV-tumor status a majority of recurrences occur within 2 years of primary treatment (3–5).
Patterns of recurrence with regard to local, regional and distant sites do not differ significantly by HPV status (3, 4, 6). With regard to distant progression, the lung is the most common site of distant metastasis for both HPV-positive and HPV-negative patients (3–5, 7). Some studies have described unusual patterns of distant metastatic disease in HPV-positive OPSCC, including unusual sites such as brain metastases (8), and disseminated metastases to multiple organs sites (9, 10). However, recent evidence has not confirmed unusual metastatic disease patterns specific to the HPV-positive population (3–5, 7). Distant recurrences do occur later in HPV-positive OPSCC (3, 5), though the longer overall survival of HPV-positive patients may contribute to development these late recurrences (6, 11).
Smoking status and greater disease burden at the time of primary treatment are the main risk factors for recurrence in HPV-positive disease (1). Ang et al. recognized early on the impact of smoking history on HPV-positive disease, defining an intermediate risk group to include HPV-positive patients with >10 pack year smoking history (1). Subsequent studies have confirmed the increased risk of recurrence for smokers in this population (12). In prior studies, AJCC 7th edition stage was not independently associated with progression free survival in either p16-positive and p16-negative OPSCC patients (13). However, larger primary tumor burden, especially T4 disease, has been associated with increased risk for recurrence (14–16). High-risk nodal features have also been associated with risk of recurrence and distant progression including presence of N3 disease, extra nodal extension (ENE), and retropharyngeal adenopathy (16–18).
Recommended schedule of surveillance for oropharyngeal cancer does not currently differ by HPV status (19). One study demonstrated that recurrent HPV-positive disease was mainly diagnosed by imaging compared to HPV-negative disease which was mainly diagnosed through physical examination (3). As discussed above, patterns of recurrence generally do not differ between HPV-positive and HPV-negative disease, with majority of recurrences occurring within 2 years. However, recurrences may occur later in HPV-positive patients, and there is some evidence for late distant metastasis. Given these findings, some advocate for extended surveillance of HPV-positive patients.
Recently there has been increasing interest in the use of HPV DNA (primarily HPV-16) as a biomarker of treatment response and recurrent disease. Early studies established the relationship between detectable serum or saliva HPV DNA with increased risk for recurrent disease (20). In a prospective study of 396 patients, oral rinses were able to detect HPV DNA in 80% of HPV-positive patients at diagnosis, and persistent HPV detection after treatment was significantly associated with decreased recurrence free and overall survival (21). HPV protein (E6 & E7) antibody levels have also been proposed as a biomarker for monitoring disease. These antibody levels have been shown to decrease in both serum and saliva after treatment (22, 23). The biomarker with that has now been most studied is HPV cell free or circulating tumor (ct) DNA. Improvements in PCR techniques including digital droplet PCR and next generation sequencing have facilitated high sensitivity of these assays (24). For HPV-positive patients, HPV ctDNA can be detected at diagnosis in about 65-90% of patients (24). While patients with higher TNM stage are more likely to have detectable HPV ctDNA at baseline (25, 26), ctDNA can also be detected in early stage disease (27). In these patients, there is a rapid decline in ctDNA after both surgical treatment (28) and primary chemoradiation (29). Those with persistent HPV ctDNA after treatment were more likely to have adverse pathologic features, and increased risk for recurrence (28, 29). A recent study of 1076 patients evaluated circulating HPV-DNA serially after definitive therapy. In patients who were otherwise without evidence of disease, of those with positive HPV ctDNA, 93% were identified to have occult recurrence (30). ctDNA has also been proposed as an adjunct to post-treatment imaging for evaluation of treatment response (31). The utility of ctDNA for detection of residual or recurrent disease has also been demonstrated in HPV associated cervical cancer (32) and anal squamous cell carcinoma (33). While additional clinical validation is needed prior to incorporation to clinical practice to augment surveillance of HPV-positive disease, early results are promising (Table 1). Additional studies are also needed to better understand patients who do not have detectable HPV ctDNA at baseline, the role of ctDNA levels at the time of diagnosis, the role of ctDNA for early diagnosis and screening, and how to integrate these tests into current surveillance practices.
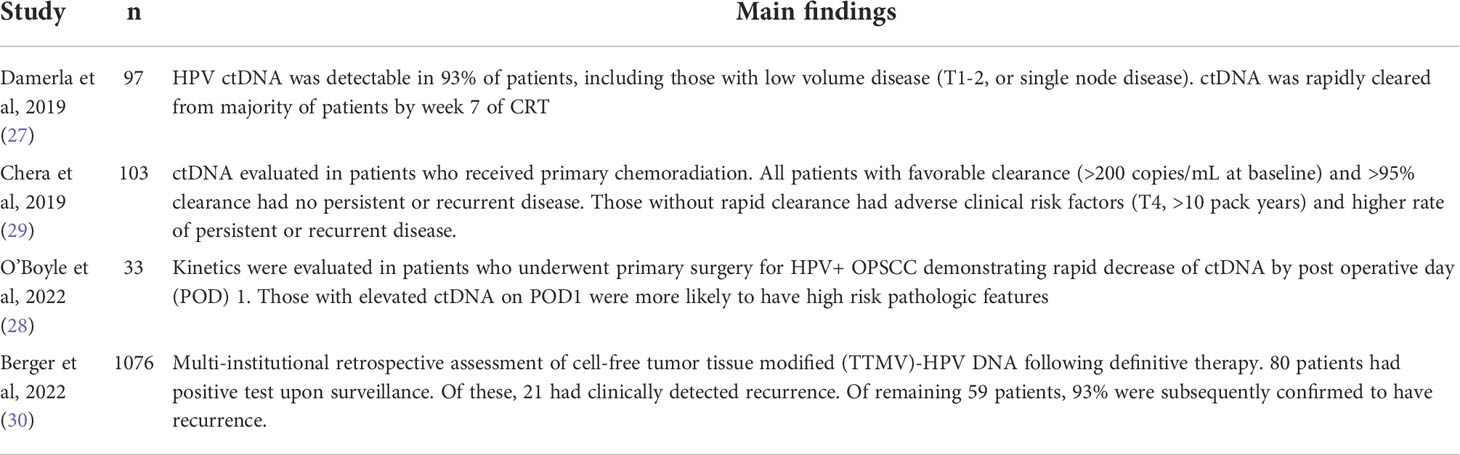
Table 1 HPV ctDNA clearance and recurrence detection in OPSCC.
After recurrence, HPV-positive patients still demonstrate improved outcomes compared to their HPV-negative counterparts (3–5, 7, 42, 56). Other factors that contribute to improved overall survival include longer disease free interval and lower disease burden at time of recurrence (3, 57, 58). Treatment of recurrent disease with surgical salvage with or without adjuvant therapy when feasible, is associated with significant improvement in survival after both locoregional and distant recurrence (3, 4, 7, 57, 59, 60). The retrospective nature of salvage surgery studies should be recognized, where patients with localized disease burden and higher performance status are more likely to be selected for surgical salvage. In addition, the recent FDA approval of immunotherapy for treatment of recurrent metastatic head and neck cancer may change the landscape of systemic treatment options in the future. A summary of salvage treatment options is detailed in Table 2.

Table 2 Salvage treatment options.
In cases of recurrent OPSCC, surgical salvage with curative intent should be offered when feasible. Historically, recurrent oropharyngeal disease has been associated with poor prognosis with lower rates of survival and higher rates of surgical complication compared to other head and neck subsites (57, 61, 62). In this context, surgical salvage was often considered unacceptably morbid for minimal benefit. In one case series of patients treated with surgical salvage for OPSCC did show improved survival, however, 46% experienced post-operative complications and 67% of patients developed another recurrence at a median of 8 months (57). However, the improved prognosis of increasingly prevalent HPV-positive disease has significantly improved overall survival for recurrent OPSCC. One meta-analysis demonstrated an increase in 5-year overall survival for recurrent OPSCC from 18% to 51% in patients treated before and after 2000 (63). Concurrently, advancements in minimally invasive transoral robotic techniques have reduced surgical morbidity through minimally invasive approaches (64, 65). With these changes in the modern era, surgical salvage has fallen back into favor. Multiple retrospective studies have demonstrated the significant survival benefit associated surgical salvage with 5-year survival rates of 43-49% compared to 16% for non-surgical therapy (62, 66, 67). Ability to achieve negative margins is one of the most important predictor of surgical salvage success (59, 67–69).
TORS for recurrent oropharyngeal disease has been associated with decreased post-operative complications, including lower long-term tracheostomy and feeding tube dependence (34, 70). White et al. performed a multi-institutional matched analysis comparing TORS-assisted salvage surgery compared to open surgery and found that TORS-assisted surgery reduced tracheostomy use, feeding tube use, and reduced hospital length of stay. In addition, TORS-assisted surgery in this study was also associated with improved oncologic outcomes with decreased positive margins and improved recurrence free survival (34). Multiple case series have demonstrated feasibility of TORS assisted surgical salvage in the oropharynx, which may include free flap reconstruction with TORS assisted flap inset (64, 65, 70).
A patient’s burden of recurrent disease and functional status play an important role in selecting patients most likely to benefit from surgical salvage. As previously discussed, selection for surgical salvage should foremost consider ability to achieve negative margins (57–60, 67–69). Other markers of aggressive tumor behavior such as short disease free interval or persistence, lymphovascular invasion and positive cervical nodal recurrence portend worse survival following salvage (57, 59, 71, 72). In addition, older patient age and laryngopharyngeal dysfunction are significant negative predictors of survival in the salvage setting (57, 72). Heft Neal et al. proposed a classification system which predicted survival following salvage surgery for recurrent oropharyngeal cancer following radiation. Class I patients (disease free interval > 2 years) had the highest five-year overall survival at 47% compared with 0% of Class III patients with short disease free interval of <2 years and laryngopharyngeal dysfunction (72). Other studies have also demonstrated that G-tube dependence is associated with decreased overall survival after surgical salvage (71, 73).
Given that patients with advanced primary disease are more likely to recur, 90-95% of patients who recur will have received prior radiation either in the primary or adjuvant setting (3, 59). In this setting, regional or free flap reconstruction of surgical defects are recommended for reconstruction to reduce risk of fistula and prevent vessel exposure (62, 64, 74). Free tissue transfer significantly reduces morbidity and major complications in salvage laryngeal surgery (75, 76) and has similarly been employed in salvage oropharyngeal surgery to bring vascularized tissue to the irradiated wound bed with high success rates (62). One of the most common reconstructive strategies involves an L-shaped soft tissue template as described by Chepeha et al. (77) Common donor sites include the radial forearm, anterolateral thigh, and lateral arm. The authors describe the three fundamental goals of primary oropharyngeal reconstruction: obliteration of the oropharynx, preservation of nasopharyngeal competence, and maintenance of base of tongue mobility (77). In the surgical salvage oropharyngectomy, where greater wound contraction is encountered, free tissue transfer plays a vital role in achieving these reconstructive principles. TORS techniques can assist with free flap inset, with vessel anastomosis performed in an open neck (78). In addition to free tissue transfer, use of the submental island flap has also been described after TORS (79). These techniques require specialized expertise and equipment; however, with appropriate patient selection they can reduce surgical morbidity (34, 70). These minimally invasive approaches are not always feasible, and patients with more extensive disease, severe trismus or requiring bony resection will require open resection. In the setting of prior radiation and when free flap reconstruction is required, tracheostomy and feeding tube placement are routinely utilized in conjunction with salvage surgery (57, 62, 70). Most patients can achieve decannulation and oral diet by six-months after surgery, but these rates are lower in those undergoing open surgery and in those with greater disease burden (57, 71).
Isolated neck recurrence may provide greater chance at complete resection of recurrent disease, however nodal recurrence is associated with high rates of further recurrence and metastasis (61, 73). Prior studies including all head and neck subsites have demonstrated that salvage neck dissection was associated with improved survival compared to non-surgical treatment (80). However, risk of recurrence after salvage neck dissection was greater when the neck was previously dissected (81).
For patients with resectable recurrence after prior radiation treatment, there is strong evidence that adjuvant therapy following salvage surgery reduces progression free survival and is recommended by NCCN guidelines (19, 82). OPSCC patients who experience recurrence are at high risk for developing second recurrence (68), and use of postoperative radiation is associated with improved survival after surgical salvage (72). Reconstruction in salvage surgery for recurrent local or neck disease can assist in reducing morbidity of re-irradiation in the adjuvant setting by providing vascularized tissue coverage (83).
For patients with unresectable disease or who are unable to undergo surgical resection, re-irradiation with or without chemotherapy is an option that has historically demonstrated limited benefit for non-nasopharyngeal sites, and carries high rates of toxicity (35, 61). Trials combining chemotherapy with hyper-fractionated reirradiation for recurrent head and neck cancer had fairly low overall survival (15.2% at two years), although patients with longer disease free interval had better outcomes (84). Advancements in radiation therapy technology have improved outcomes. Patients receiving intensity modulated radiation therapy (IMRT) in the re-irradiation setting demonstrate improved locoregional control (52% vs 20% at 2 years), and patients who underwent gross total resection also trended towards improved locoregional control (35). While salvage surgery has been associated with improved progression free survival (36), the advantages of surgical resection prior to re-irradiation have not been universally reported when compared to re-irradiation with curative intent (85). Re-irradiation with proton therapy has also recently demonstrated promising locoregional control results (68% locoregional control at 1 year) with tolerable toxicity profiles (37, 38). Additionally, stereotactic body radiotherapy (SBRT) has also demonstrated comparable disease control in the recurrent setting, with improved outcomes in HPV-positive patients (39, 40).
When distant metastasis occurs, generally systemic treatment options are favored. However, one recent study demonstrated increased survival associated with surgical salvage for distant metastases from OPSCC, with an increase of median survival from 12.5 to 35 months (3). A majority (87%) of patients were HPV-positive, and surgery included lung nodule resection, mediastinal lymphadenectomy, hepatectomy and craniotomy. Another review of OPSCC patients with distant metastases demonstrated significantly improved 3-year disease specific survival (40% vs 8%) in patients receiving curative therapy (surgery with negative margins or definitive radiation) for distant disease compared to palliative systemic treatment (7). For patients with oligometastatic lung disease, SBRT has shown up to 75% response rates (41) and over 50% 2-year overall survival in those without locoregional recurrence (35). While these retrospective studies are inevitably subject to selection bias, they still support the potential survival benefit that surgery and definitive radiation can offer select OPSCC patients with limited distant metastases.
For patients who do not have surgical or re-irradiation options, systemic chemotherapy regimens are the mainstay for recurrent metastatic head and neck cancer. The EXTREME regimen including cetuximab, platinum and 5-fluorouracil (5-FU) had been the standard treatment regimen for the past decade (42, 86). The EXTREME regimen demonstrated median overall survival of 12.6 months for p16+ patients and 9.7 months for p16- patients; both groups benefited from the addition of cetuximab to platinum/5-FU (42). Recently, the advent of immunotherapy through anti-PD1/PDL1 checkpoint inhibition has provided promising new options. For patients refractory to platinum therapy or cetuximab, overall response rates were 13-18% and overall survival was significantly improved for patients receiving immunotherapy (pembrolizumab or nivolimab) compared to standard chemotherapy (43, 44). Subgroup analysis demonstrated higher response rates in patients whose tumors expressed PD-L1, irrespective if this was on cancer or stromal cells (45–47). Despite, having on average a higher rate of immune cell infiltrate, the impact of HPV tumor status on immunotherapy response rate has not been clearly established, with some studies showing higher response rates in HPV-positive patients (48) and others showing greater survival benefit for HPV-negative patients (49). With the establishment of anti-PD1 agents in platinum refractory disease, pembrolizumab was tested either as monotherapy or in combination with chemotherapy (platinum and 5-FU) in patients with recurrent disease who were treatment naïve (87). Compared to the EXTREME regimen, pembrolizumab monotherapy improved overall survival in patients whose tumors expressed PDL1 and pembrolizumab with chemotherapy improved overall survival in all patients, irrespective of tumor PDL1 expression. Nonetheless, higher tumor PDL1 expression was associated with a greater benefit in both pembrolizumab-containing treatment arms further establishing this a predictive biomarker. It is also notable that, in long-term follow up, approximately 25% of subjects treated with pembrolizumab on either arm were alive suggesting that there is long-term benefit to immunotherapy (50).
In an effort to integrate the potential benefit of T cell stimulation via PD1 blockade and antibody dependent cellular cytotoxicity of IgG1 antibodies, Sacco et al. combined pembrolizumab and cetuximab in recurrent/metastatic HNSCC patients who were refractory to or poor candidates for platinum (51). This doublet regimen proved to be remarkably active with an objective response rate of 45% and median overall survival of 18 months, regardless of HPV status. The activity of PD1/EGFR inhibition has been confirmed by two independent subsequent studies and now represents a treatment option for patients who are not good candidates for platinum-based therapy in the recurrent/metastatic setting (88, 89).
Specific therapies for HPV related HNSCC are also being developed taking advantage of the unique antigens of a virally induced malignancy. These include therapeutic HPV vaccines and engineered T cells. Several therapeutic HPV vaccines are being tested in clinical trials with early promising results. For instance, ISA101b is a synthetic long peptide vaccine targeting HPV-16 E6 and E7 antigens which demonstrated an objective response rate in HPV-related oropharynx cancer of 33% in combination with nivolumab (52). This vaccine is currently being evaluated in a randomized study of cemiplimab, an anti-PD1 antibody, with or without ISA101b.
Cloning the T cell receptor (TCR) for a given HPV antigen and HLA type has introduced the possibility of engineering T cells to express the relevant TCR. These strategies have been tested in clinical trials using HPV-16 E6 and E7 TCRs. Interestingly, a clinical trial of an HPV-16 E7 TCR recently demonstrated a 50% response rate in refractory tumors (53). While this activity is promising, analysis of tumor biopsies at progression revealed emergence of resistance through loss of HPV-16 antigen presentation; a consequence that TCR strategies will need to overcome to demonstrate long-term benefit.
In this evolving field, novel combinations are under study that attempt to leverage the benefits demonstrated with anti-PD1 blockade including adding agents that target TIGIT, CD47, and LAG3 (54). Furthermore, applications for immunotherapy will continue to transform treatment options for patients with recurrent disease such as considerations for neoadjuvant immunotherapy before salvage surgery, or maintenance immunotherapy after salvage treatment. Promising results have been obtained administering neoadjuvant and adjuvant nivolumab and lirilumab, an anti-KIR antibody, in patients with recurrent and resectable HNSCC with 1-year disease-free and overall survival of 55% and 85%, respectively (55). These will need to validated in randomized studies but provides encouragement for improved outcomes in these difficult to treat patients.
Although HPV-mediated OPSCC is associated with improved prognosis and decreased rates of recurrence, recurrent disease still occurs. With the increasing incidence of HPV-mediated OPSCC, recurrent HPV disease is also becoming more prevalent and there is an increasing need to understand the unique presentation and treatment of recurrent HPV disease. Recurrences in HPV-positive patients may occur later, and patients may have improved outcomes after recurrence compared to HPV-negative counterparts. Emerging data demonstrates that detection of recurrences may be aided by evaluation of circulating tumor HPV DNA. Surgical salvage is the preferred treatment when feasible, and robotic approaches can decrease morbidity. New advances in re-irradiation and immune based therapies are offering promising results for this patient population.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
All authors (TG, SK, and EC) provided substantial contributions to the conception of this work, drafting and writing as well as approval of publication.
TG is supported by 1KL2TR001444 from NIH.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tân PF, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med (2010) 363(1):24–35. doi: 10.1056/NEJMoa0912217
2. Ang KK, Zhang Q, Rosenthal DI, Nguyen-Tan PF, Sherman EJ, Weber RS, et al. Randomized phase III trial of concurrent accelerated radiation plus cisplatin with or without cetuximab for stage III to IV head and neck carcinoma: RTOG 0522. J Clin Oncol Off J Am Soc Clin Oncol (2014) 32(27):2940–50. doi: 10.1200/JCO.2013.53.5633
3. Guo T, Qualliotine JR, Ha PK, Califano JA, Kim Y, Saunders JR, et al. Surgical salvage improves overall survival for patients with HPV-positive and HPV-negative recurrent locoregional and distant metastatic oropharyngeal cancer. Cancer (2015) 121(12):1977–84. doi: 10.1002/cncr.29323
4. Fakhry C, Zhang Q, Nguyen-Tan PF, Rosenthal D, El-Naggar A, Garden AS, et al. Human papillomavirus and overall survival after progression of oropharyngeal squamous cell carcinoma. J Clin Oncol Off J Am Soc Clin Oncol (2014) 32:3365–73. doi: 10.1200/JCO.2014.55.1937
5. Trosman SJ, Koyfman SA, Ward MC, Al-Khudari S, Nwizu T, Greskovich JF, et al. Effect of human papillomavirus on patterns of distant metastatic failure in oropharyngeal squamous cell carcinoma treated with chemoradiotherapy. JAMA Otolaryngol– Head Neck Surg (2015) 141:457–62. doi: 10.1001/jamaoto.2015.136
6. Faraji F, Eisele DW, Fakhry C. Emerging insights into recurrent and metastatic human papillomavirus-related oropharyngeal squamous cell carcinoma. Laryngoscope Investig Otolaryngol (2017) 2(1):10–8. doi: 10.1002/lio2.37
7. Sinha P, Thorstad WT, Nussenbaum B, Haughey BH, Adkins DR, Kallogjeri D, et al. Distant metastasis in p16-positive oropharyngeal squamous cell carcinoma: a critical analysis of patterns and outcomes. Oral Oncol (2014) 50(1):45–51. doi: 10.1016/j.oraloncology.2013.10.007
8. Ruzevick J, Olivi A, Westra WH. Metastatic squamous cell carcinoma to the brain: an unrecognized pattern of distant spread in patients with HPV-related head and neck cancer. J Neurooncol (2013) 112:449–54. doi: 10.1007/s11060-013-1075-9
9. Huang SH, Perez-Ordonez B, Weinreb I, Hope A, Massey C, Waldron JN, et al. Natural course of distant metastases following radiotherapy or chemoradiotherapy in HPV-related oropharyngeal cancer. Oral Oncol (2013) 49:79–85. doi: 10.1016/j.oraloncology.2012.07.015
10. Huang SH, Perez-Ordonez B, Liu FF, Waldron J, Ringash J, Irish J, et al. Atypical clinical behavior of p16-confirmed HPV-related oropharyngeal squamous cell carcinoma treated with radical radiotherapy. Int J Radiat Oncol Biol Phys (2012) 82:276–83. doi: 10.1016/j.ijrobp.2010.08.031
11. Guo T, Rettig E, Fakhry C. Understanding the impact of survival and human papillomavirus tumor status on timing of recurrence in oropharyngeal squamous cell carcinoma. Oral Oncol (2016) 52:97–103. doi: 10.1016/j.oraloncology.2015.10.016
12. Maxwell JH, Kumar B, Feng FY, Worden FP, Lee JS, Eisbruch A, et al. Tobacco use in human papillomavirus-positive advanced oropharynx cancer patients related to increased risk of distant metastases and tumor recurrence. Clin Cancer Res Off J Am Assoc Cancer Res (2010) 16:1226–35. doi: 10.1158/1078-0432.CCR-09-2350
13. Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, Pinto H, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst (2008) 100:261–9. doi: 10.1093/jnci/djn011
14. Sedaghat AR, Zhang Z, Begum S, Palermo R, Best S, Ulmer KM, et al. Prognostic significance of human papillomavirus in oropharyngeal squamous cell carcinomas. Laryngoscope (2009) 119(8):1542–9. doi: 10.1002/lary.20533
15. Matoscevic K, Graf N, Pezier TF, Huber GF. Success of salvage treatment: a critical appraisal of salvage rates for different subsites of HNSCC. Otolaryngol–Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg (2014) 151(3):454–61. doi: 10.1177/0194599814535183
16. Samuels SE, Vainshtein J, Spector ME, Ibrahim M, McHugh JB, Tao Y, et al. Impact of retropharyngeal adenopathy on distant control and survival in HPV-related oropharyngeal cancer treated with chemoradiotherapy. Radiother Oncol J Eur Soc Ther Radiol Oncol (2015) 116(1):75–81. doi: 10.1016/j.radonc.2015.06.006
17. Shevach J, Bossert A, Bakst RL, Liu J, Misiukiewicz K, Beyda J, et al. Extracapsular extension is associated with worse distant control and progression-free survival in patients with lymph node-positive human papillomavirus-related oropharyngeal carcinoma. Oral Oncol (2017) 74:56–61. doi: 10.1016/j.oraloncology.2017.09.014
18. Lin TA, Garden AS, Elhalawani H, Elgohari B, Jethanandani A, Ng SP, et al. Radiographic retropharyngeal lymph node involvement in HPV-associated oropharyngeal carcinoma: Patterns of involvement and impact on patient outcomes. Cancer (2019) 125(9):1536–46. doi: 10.1002/cncr.31944
19. Pfister DG, Spencer S, Adelstein D, Adkins D, Anzai Y, Brizel DM, et al. Head and neck cancers, version 2.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw JNCCN (2020) 18(7):873–98. doi: 10.6004/jnccn.2020.0031
20. Ahn SM, Chan JYK, Zhang Z, Wang H, Khan Z, Bishop JA, et al. Saliva and plasma quantitative polymerase chain reaction–based detection and surveillance of human papillomavirus–related head and neck cancer. JAMA Otolaryngol Neck Surg (2014) 140(9):846–54. doi: 10.1001/jamaoto.2014.1338
21. Fakhry C, Blackford AL, Neuner G, Xiao W, Jiang B, Agrawal A, et al. Association of oral human papillomavirus DNA persistence with cancer progression after primary treatment for oral cavity and oropharyngeal squamous cell carcinoma. JAMA Oncol (2019) 5(7):985–92. doi: 10.1001/jamaoncol.2019.0439
22. Fakhry C, Qualliotine JR, Zhang Z, Agrawal N, Gaykalova DA, Bishop JA, et al. Serum antibodies to HPV16 early proteins warrant investigation as potential biomarkers for risk stratification and recurrence of HPV-associated oropharyngeal cancer. Cancer Prev Res (Phila Pa) (2016) 9(2):135–41. doi: 10.1158/1940-6207.CAPR-15-0299
23. Hanna GJ, Sridharan V, Margalit DN, La Follette SK, Chau NG, Rabinowits G, et al. Salivary and serum HPV antibody levels before and after definitive treatment in patients with oropharyngeal squamous cell carcinoma. Cancer biomark (2017) 19(2):129–36. doi: 10.3233/CBM-160071
24. Haring CT, Dermody SM, Yalamanchi P, Kang SY, Old MO, Chad Brenner J, et al. The future of circulating tumor DNA as a biomarker in HPV related oropharyngeal squamous cell carcinoma. Oral Oncol (2022) 126:105776. doi: 10.1016/j.oraloncology.2022.105776
25. Dahlstrom KR, Li G, Hussey CS, Vo JT, Wei Q, Zhao C, et al. Circulating human papillomavirus DNA as a marker for disease extent and recurrence among patients with oropharyngeal cancer. Cancer (2015) 121(19):3455–64. doi: 10.1002/cncr.29538
26. Veyer D, Wack M, Mandavit M, Garrigou S, Hans S, Bonfils P, et al. HPV circulating tumoral DNA quantification by droplet-based digital PCR: A promising predictive and prognostic biomarker for HPV-associated oropharyngeal cancers. Int J Cancer (2020) 147(4):1222–7. doi: 10.1002/ijc.32804
27. Damerla RR, Lee NY, You D, Soni R, Shah R, Reyngold M, et al. Detection of early human papillomavirus-associated cancers by liquid biopsy. JCO Precis Oncol (2019) 3. doi: 10.1200/PO.18.00276
28. O’Boyle CJ, Siravegna G, Varmeh S, Queenan N, Michel A, Pang KCS, et al. Cell-free human papillomavirus DNA kinetics after surgery for human papillomavirus–associated oropharyngeal cancer. Cancer (2022) 128(11):2193–204. doi: 10.1002/cncr.34109
29. Chera BS, Kumar S, Beaty BT, Marron D, Jefferys S, Green R, et al. Rapid clearance profile of plasma circulating tumor HPV type 16 DNA during chemoradiotherapy correlates with disease control in HPV-associated oropharyngeal cancer. Clin Cancer Res Off J Am Assoc Cancer Res (2019) 25(15):4682–90. doi: 10.1158/1078-0432.CCR-19-0211
30. Berger B, Hanna GJ, Posner M, Genden E, Fitz CDV, Naber SP, et al. Detection of occult recurrence using circulating HPV tumor DNA among patients treated for HPV-driven oropharyngeal squamous cell carcinoma. Int J Radiat Oncol Biol Phys (2022) 112(5):e4. doi: 10.1016/j.ijrobp.2021.12.016
31. Tanaka H, Takemoto N, Horie M, Takai E, Fukusumi T, Suzuki M, et al. Circulating tumor HPV DNA complements PET-CT in guiding management after radiotherapy in HPV-related squamous cell carcinoma of the head and neck. Int J Cancer (2021) 148(4):995–1005. doi: 10.1002/ijc.33287
32. Jeannot E, Latouche A, Bonneau C, Calméjane M-A, Beaufort C, Ruigrok-Ritstier K, et al. Circulating HPV DNA as a marker for early detection of relapse in patients with cervical cancer. Clin Cancer Res (2021) 27(21):5869–77. doi: 10.1158/1078-0432.CCR-21-0625
33. Cabel L, Jeannot E, Bieche I, Vacher S, Callens C, Bazire L, et al. Prognostic impact of residual HPV ctDNA detection after chemoradiotherapy for anal squamous cell carcinoma. Clin Cancer Res (2018) 24(22):5767–71. doi: 10.1158/1078-0432.CCR-18-0922
34. Argiris A, Li S, Ghebremichael M, Egloff AM, Wang L, Forastiere AA, et al. Prognostic significance of human papillomavirus in recurrent or metastatic head and neck cancer: an analysis of Eastern cooperative oncology group trials. Ann Oncol Off J Eur Soc Med Oncol (2014) 25(7):1410–6. doi: 10.1093/annonc/mdu167
35. Vermorken JB, Psyrri A, Mesía R, Peyrade F, Beier F, de Blas B, et al. Impact of tumor HPV status on outcome in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck receiving chemotherapy with or without cetuximab: retrospective analysis of the phase III EXTREME trial. Ann Oncol Off J Eur Soc Med Oncol (2014) 25(4):801–7. doi: 10.1093/annonc/mdt574
36. Zafereo ME, Hanasono MM, Rosenthal DI, Sturgis EM, Lewin JS, Roberts DB, et al. The role of salvage surgery in patients with recurrent squamous cell carcinoma of the oropharynx. Cancer (2009) 115(24):5723–33. doi: 10.1002/cncr.24595
37. Agra IMG, Carvalho AL, Ulbrich FS, de Campos OD, Martins EP, Magrin J, et al. Prognostic factors in salvage surgery for recurrent oral and oropharyngeal cancer. Head Neck (2006) 28(2):107–13. doi: 10.1002/hed.20309
38. Su W, Rajeev-Kumar G, Kang M, Posner M, Liu JT, Westra W, et al. Long-term outcomes in patients with recurrent human papillomavirus-positive oropharyngeal cancer after upfront transoral robotic surgery. Head Neck (2020) 42(12):3490–6. doi: 10.1002/hed.26396
39. Patel SN, Cohen MA, Givi B, Dixon BJ, Gilbert RW, Gullane PJ, et al. Salvage surgery for locally recurrent oropharyngeal cancer. Head Neck (2016) 38 Suppl 1:E658–664. doi: 10.1002/hed.24065
40. Ho AS, Kraus DH, Ganly I, Lee NY, Shah JP, Morris LGT. Decision making in the management of recurrent head and neck cancer. Head Neck (2014) 36(1):144–51. doi: 10.1002/hed.23227
41. Kostrzewa JP, Lancaster WP, Iseli TA, Desmond RA, Carroll WR, Rosenthal EL. Outcomes of salvage surgery with free flap reconstruction for recurrent oral and oropharyngeal cancer. Laryngoscope (2010) 120(2):267–72. doi: 10.1002/lary.20743
42. Jayaram SC, Muzaffar SJ, Ahmed I, Dhanda J, Paleri V, Mehanna H. Efficacy, outcomes, and complication rates of different surgical and nonsurgical treatment modalities for recurrent/residual oropharyngeal carcinoma: A systematic review and meta-analysis. Head Neck (2016) 38(12):1855–61. doi: 10.1002/hed.24531
43. Genden EM, Park R, Smith C, Kotz T. The role of reconstruction for transoral robotic pharyngectomy and concomitant neck dissection. Arch Otolaryngol Head Neck Surg (2011) 137(2):151–6. doi: 10.1001/archoto.2010.250
44. Ghanem TA. Transoral robotic-assisted microvascular reconstruction of the oropharynx. Laryngoscope (2011) 121(3):580–2. doi: 10.1002/lary.21428
45. Kano S, Homma A, Hayashi R, Kawabata K, Yoshino K, Iwae S, et al. Salvage surgery for recurrent oropharyngeal cancer after chemoradiotherapy. Int J Clin Oncol (2013) 18(5):817–23. doi: 10.1007/s10147-012-0449-x
46. Nichols AC, Kneuertz PJ, Deschler DG, Lin DT, Emerick KS, Clark JR, et al. Surgical salvage of the oropharynx after failure of organ-sparing therapy. Head Neck (2011) 33(4):516–24. doi: 10.1002/hed.21480
47. Jones AS, Bin Hanafi Z, Nadapalan V, Roland NJ, Kinsella A, Helliwell TR. Do positive resection margins after ablative surgery for head and neck cancer adversely affect prognosis? a study of 352 patients with recurrent carcinoma following radiotherapy treated by salvage surgery. Br J Cancer (1996) 74(1):128–32. doi: 10.1038/bjc.1996.327
48. Joseph AW, Guo T, Hur K, Xie Y, Yin L, Califano JA, et al. Disease-free survival after salvage therapy for recurrent oropharyngeal squamous cell carcinoma. Head Neck (2016) 38 Suppl 1:E1501–1509. doi: 10.1002/hed.24268
49. White H, Ford S, Bush B, Holsinger FC, Moore E, Ghanem T, et al. Salvage surgery for recurrent cancers of the oropharynx: comparing TORS with standard open surgical approaches. JAMA Otolaryngol– Head Neck Surg (2013) 139(8):773–8. doi: 10.1001/jamaoto.2013.3866
50. Dean NR, Rosenthal EL, Carroll WR, Kostrzewa JP, Jones VL, Desmond RA, et al. Robotic-assisted surgery for primary or recurrent oropharyngeal carcinoma. Arch Otolaryngol Head Neck Surg (2010) 136(4):380–4. doi: 10.1001/archoto.2010.40
51. Goodwin WJ. Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: when do the ends justify the means? Laryngoscope (2000) 110(3 Pt 2 Suppl 93):1–18. doi: 10.1097/00005537-200003001-00001
52. Heft Neal ME, Brennan J, Haring CT, Brenner JC, Worden F, Swiecicki P, et al. Predictors of survival in patients undergoing oropharyngeal surgery for cancer recurrence after radiation therapy. Eur Arch Oto-Rhino-Laryngol Off J Eur Fed Oto-Rhino-Laryngol Soc EUFOS Affil Ger Soc Oto-Rhino-Laryngol - Head Neck Surg (2020) 277(7):2085–93. doi: 10.1007/s00405-020-05913-z
53. Sweeny L, Rosenthal EL, Clemons L, Stevens TM, Cook McIntosh ER, Carroll WR. Outcomes after surgical salvage for recurrent oropharyngeal squamous cell carcinoma. Oral Oncol (2016) 60:118–24. doi: 10.1016/j.oraloncology.2016.07.006
54. Paleri V, Drinnan M, van den Brekel MWM, Hinni ML, Bradley PJ, Wolf GT, et al. Vascularized tissue to reduce fistula following salvage total laryngectomy: a systematic review. Laryngoscope (2014) 124(8):1848–53. doi: 10.1002/lary.24619
55. Fung K, Teknos TN, Vandenberg CD, Lyden TH, Bradford CR, Hogikyan ND, et al. Prevention of wound complications following salvage laryngectomy using free vascularized tissue. Head Neck (2007) 29(5):425–30. doi: 10.1002/hed.20492
56. Microvascular committee of the American academy of otolaryngology-head & neck surgery*. salvage laryngectomy and laryngopharyngectomy: Multicenter review of outcomes associated with a reconstructive approach. Head Neck (2019) 41(1):16–29. doi: 10.1002/hed.25192
57. Chepeha DB, Sacco AG, Erickson VR, Lyden T, Haxer M, Moyer J, et al. Oropharyngoplasty with template-based reconstruction of oropharynx defects. Arch Otolaryngol Head Neck Surg (2009) 135(9):887–94. doi: 10.1001/archoto.2009.130
58. Gorphe P, Temam S, Moya-Plana A, Leymarie N, Kolb F, Bout-Roumazeilles A, et al. Indications and clinical outcomes of transoral robotic surgery and free flap reconstruction. Cancers (2021) 13(11):2831. doi: 10.3390/cancers13112831
59. Holcomb AJ, Richmon JD. Transoral robotic salvage oropharyngectomy with submental artery island flap reconstruction. Head Neck (2021) 43(2):E13–9. doi: 10.1002/hed.26543
60. Deschamps DR, Spencer HJ, Kokoska MS, Spring PM, Vural EA, Stack BC. Implications of head and neck cancer treatment failure in the neck. Otolaryngol–Head Neck Surg Off J Am Acad Otolaryngol-Head Neck Surg (2010) 142(5):722–7. doi: 10.1016/j.otohns.2010.01.026
61. Wong LY, Wei WI, Lam LK, Yuen APW. Salvage of recurrent head and neck squamous cell carcinoma after primary curative surgery. Head Neck (2003) 25(11):953–9. doi: 10.1002/hed.10310
62. Janot F, de Raucourt D, Benhamou E, Ferron C, Dolivet G, Bensadoun R-J, et al. Randomized trial of postoperative reirradiation combined with chemotherapy after salvage surgery compared with salvage surgery alone in head and neck carcinoma. J Clin Oncol Off J Am Soc Clin Oncol (2008) 26(34):5518–23. doi: 10.1200/JCO.2007.15.0102
63. Paderno A, Piazza C, Bresciani L, Vella R, Nicolai P. Microvascular head and neck reconstruction after (chemo)radiation: facts and prejudices. Curr Opin Otolaryngol Head Neck Surg (2016) 24(2):83–90. doi: 10.1097/MOO.0000000000000243
64. Lee N, Chan K, Bekelman JE, Zhung J, Mechalakos J, Narayana A, et al. Salvage re-irradiation for recurrent head and neck cancer. Int J Radiat Oncol Biol Phys (2007) 68(3):731–40. doi: 10.1016/j.ijrobp.2006.12.055
65. Spencer SA, Harris J, Wheeler RH, Machtay M, Schultz C, Spanos W, et al. Final report of RTOG 9610, a multi-institutional trial of reirradiation and chemotherapy for unresectable recurrent squamous cell carcinoma of the head and neck. Head Neck (2008) 30(3):281–8. doi: 10.1002/hed.20697
66. Lee HI, Kim JH, Ahn SH, Chung E-J, Keam B, Eom K-Y, et al. Re-irradiation for recurrent or second primary head and neck cancer. Radiat Oncol J (2021) 39(4):279–87. doi: 10.3857/roj.2021.00640
67. Takiar V, Garden AS, Ma D, Morrison WH, Edson M, Zafereo ME, et al. Reirradiation of head and neck cancers with intensity modulated radiation therapy: Outcomes and analyses. Int J Radiat Oncol Biol Phys (2016) 95(4):1117–31. doi: 10.1016/j.ijrobp.2016.03.015
68. Phan J, Sio TT, Nguyen TP, Takiar V, Gunn GB, Garden AS, et al. Reirradiation of head and neck cancers with proton therapy: Outcomes and analyses. Int J Radiat Oncol Biol Phys (2016) 96(1):30–41. doi: 10.1016/j.ijrobp.2016.03.053
69. Romesser PB, Cahlon O, Scher ED, Hug EB, Sine K, DeSelm C, et al. Proton beam reirradiation for recurrent head and neck cancer: Multi-institutional report on feasibility and early outcomes. Int J Radiat Oncol Biol Phys (2016) 95(1):386–95. doi: 10.1016/j.ijrobp.2016.02.036
70. Vargo JA, Ward MC, Caudell JJ, Riaz N, Dunlap NE, Isrow D, et al. A multi-institutional comparison of SBRT and IMRT for definitive reirradiation of recurrent or second primary head and neck cancer. Int J Radiat Oncol Biol Phys (2018) 100(3):595–605. doi: 10.1016/j.ijrobp.2017.04.017
71. Davis KS, Vargo JA, Ferris RL, Burton SA, Ohr JP, Clump DA, et al. Stereotactic body radiotherapy for recurrent oropharyngeal cancer - influence of HPV status and smoking history. Oral Oncol (2014) 50(11):1104–8. doi: 10.1016/j.oraloncology.2014.08.004
72. Bonomo P, Greto D, Desideri I, Loi M, Di Cataldo V, Orlandi E, et al. Clinical outcome of stereotactic body radiotherapy for lung-only oligometastatic head and neck squamous cell carcinoma: Is the deferral of systemic therapy a potential goal? Oral Oncol (2019) 93:1–7. doi: 10.1016/j.oraloncology.2019.04.006
73. Vermorken JB, Mesia R, Rivera F, Remenar E, Kawecki A, Rottey S, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med (2008) 359(11):1116–27. doi: 10.1056/NEJMoa0802656
74. Ferris RL, Blumenschein G, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med (2016) 375(19):1856–67. doi: 10.1056/NEJMoa1602252
75. Cohen EEW, Soulières D, Le Tourneau C, Dinis J, Licitra L, Ahn M-J, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet Lond Engl (2019) 393(10167):156–67. doi: 10.1016/S0140-6736(18)31999-8
76. Bauml J, Seiwert TY, Pfister DG, Worden F, Liu SV, Gilbert J, et al. Pembrolizumab for platinum- and cetuximab-refractory head and neck cancer: Results from a single-arm, phase II study. J Clin Oncol Off J Am Soc Clin Oncol (2017) 35(14):1542–9. doi: 10.1200/JCO.2016.70.1524
77. Ferris RL, Blumenschein G, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral Oncol (2018) 81:45–51. doi: 10.1016/j.oraloncology.2018.04.008
78. Emancipator K, Huang L, Aurora-Garg D, Bal T, Cohen EEW, Harrington K, et al. Comparing programmed death ligand 1 scores for predicting pembrolizumab efficacy in head and neck cancer. Mod Pathol Off J U S Can Acad Pathol Inc (2021) 34(3):532–41. doi: 10.1038/s41379-020-00710-9
79. Mehra R, Seiwert TY, Gupta S, Weiss J, Gluck I, Eder JP, et al. Efficacy and safety of pembrolizumab in recurrent/metastatic head and neck squamous cell carcinoma: pooled analyses after long-term follow-up in KEYNOTE-012. Br J Cancer (2018) 119(2):153–9. doi: 10.1038/s41416-018-0131-9
80. Wei W, Ji M, Wu CP, Yang X. p16 status and choice of chemotherapy in the KEYNOTE-040 study. Lancet Lond Engl (2019) 394(10206):1321–2. doi: 10.1016/S0140-6736(19)31261-9
81. Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M, de Castro G, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet Lond Engl (2019) 394(10212):1915–28. doi: 10.1016/S0140-6736(19)32591-7
82. Burtness B, Rischin D, Greil R, Soulières D, Tahara M, de Castro G, et al. Pembrolizumab alone or with chemotherapy for Recurrent/Metastatic head and neck squamous cell carcinoma in KEYNOTE-048: Subgroup analysis by programmed death ligand-1 combined positive score. J Clin Oncol Off J Am Soc Clin Oncol (2022), JCO2102198. 40(21):2321–32 doi: 10.1200/JCO.21.02198
83. Sacco AG, Chen R, Worden FP, Wong DJL, Adkins D, Swiecicki P, et al. Pembrolizumab plus cetuximab in patients with recurrent or metastatic head and neck squamous cell carcinoma: an open-label, multi-arm, non-randomised, multicentre, phase 2 trial. Lancet Oncol (2021) 22(6):883–92. doi: 10.1016/S1470-2045(21)00136-4
84. Chung CH, Li J, Steuer CE, Bhateja P, Johnson M, Masannat J, et al. Phase II multi-institutional clinical trial result of concurrent cetuximab and nivolumab in recurrent and/or metastatic head and neck squamous cell carcinoma. Clin Cancer Res Off J Am Assoc Cancer Res (2022) 28(11):2329–38. doi: 10.1158/1078-0432.CCR-21-3849
85. Kao H-F, Liao B-C, Huang Y-L, Huang H-C, Chen C-N, Chen T-C, et al. Afatinib and pembrolizumab for recurrent or metastatic head and neck squamous cell carcinoma (ALPHA study): A phase II study with biomarker analysis. Clin Cancer Res Off J Am Assoc Cancer Res (2022) 28(8):1560–71. doi: 10.1158/1078-0432.CCR-21-3025
86. Sousa LG, Rajapakshe K, Rodriguez Canales J, Chin RL, Feng L, Wang Q, et al. ISA101 and nivolumab for HPV-16+ cancer: updated clinical efficacy and immune correlates of response. J Immunother Cancer (2022) 10(2):e004232. doi: 10.1136/jitc-2021-004232
87. Nagarsheth NB, Norberg SM, Sinkoe AL, Adhikary S, Meyer TJ, Lack JB, et al. TCR-engineered T cells targeting E7 for patients with metastatic HPV-associated epithelial cancers. Nat Med (2021) 27(3):419–25. doi: 10.1038/s41591-020-01225-1
88. Mei Z, Huang J, Qiao B, Lam AKY. Immune checkpoint pathways in immunotherapy for head and neck squamous cell carcinoma. Int J Oral Sci (2020) 12(1):16. doi: 10.1038/s41368-020-0084-8
Keywords: oropharyngeal cancer (OPSCC), recurrent disease, surgical salvage, immunotherapy, human papillomavirus (HPV), head neck squamous carcinoma
Citation: Guo T, Kang SY and Cohen EEW (2022) Current perspectives on recurrent HPV-mediated oropharyngeal cancer. Front. Oncol. 12:966899. doi: 10.3389/fonc.2022.966899
Received: 11 June 2022; Accepted: 14 July 2022;
Published: 18 August 2022.
Edited by:
Shao Hui Huang, University Health Network, CanadaReviewed by:
Avinash Pilar, University College London Hospitals NHS Foundation Trust, United KingdomCopyright © 2022 Guo, Kang and Cohen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Theresa Guo, dHdndW9AaGVhbHRoLnVjc2QuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.