 Haoyang Bei
Haoyang Bei Weiheng Mai†
Weiheng Mai† Weifeng Chen
Weifeng Chen Yongguang Yang
Yongguang Yang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 06 October 2022
Sec. Gastrointestinal Cancers: Hepato Pancreatic Biliary Cancers
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.966821
This article is part of the Research TopicCombining Localised and Systemic Therapy Options for Advanced Hepatocellular CarcinomaView all 16 articles
Radical hepatectomy is the main treatment method to improve the prognosis of patients with intermediate and early-stage liver cancer. Most liver cancer patients in China are in the advanced stage at the initial diagnosis, losing the opportunity for surgical treatment. Therefore, it is essential to down-stage unresectable liver cancer to resectable liver cancer clinically, which is an important way to improve patients’ survival and a hotspot of current clinical research. In recent years, with the increase in effective treatment methods for liver cancer, the resection rate of conversion surgery for unresectable advanced liver cancer has been significantly improved, and a growing number of patients benefit from conversion therapy. This article mainly reviews the connotation of conversion therapy for liver cancer, the patient selection, the selection of conversion strategy, the timing of sequential operations, the scheme and safety, etc.
As one of the most common malignant tumors in the world, primary liver cancer ranks sixth in the incidence of malignant tumors worldwide in 2018, and is the fourth leading cause of tumor death (1). Primary liver cancer is the fourth most common malignant tumor and the second leading cause of tumor death in China, which seriously threatens the lives and health of the Chinese people. Hepatocellular carcinoma (HCC) (hereafter referred to as liver cancer) accounts for 75% of 85% of primary liver cancer cases. Risk factors for liver cancer include chronic viral hepatitis (hepatitis B virus infection, hepatitis C virus infection), alcoholic liver disease, consumption of food contaminated by aflatoxin, obesity and diabetes, etc. Among them, chronic hepatitis B virus (HBV) infection is the main risk factor for HCC in China (2). For patients with early-stage liver cancer, the main treatment methods include surgical resection, local ablation and liver transplantation. However, due to the latent onset and rapid progress of liver cancer, most patients are diagnosed at the intermediate and advanced stages including Barcelona Clinic Liver Cancer(BCLC) stage B, C or China liver cancer staging (CNCL) stage IIIa, IIIb and some stage IIb, when the surgical effect is poor or the opportunity for surgery is lost, and the median survival time is only 1 year (3). For such patients, the most important thing is to transform unresectable liver cancer into resectable liver cancer and perform successful surgery, which is also the key to long-term survival. In recent years, the development of tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs) has brought opportunities for the treatment of liver cancer at intermediate and advanced stages, and conversion therapy has become one of the current research hotspots.
As a treatment method for unresectable liver cancer, conversion therapy for liver cancer mainly adopts systematic drug therapy and or non-surgical local therapy to inhibit tumor progression, reduce tumor burden and improve clinical tumor staging, thereby providing patients the opportunity to undergo radical surgery (4, 5). The other category of conversion therapy is neoadjuvant therapy, which refers to HCC patients with technically resectable tumors and a high risk of recurrence. It aims to shrink the tumor, improve the radical resection rate, and reduce recurrence. When the treatment is applied to patients with surgically resectable but oncologically unresectable HCC, both treatments may be overlapped in the target population (5). At present, the commonly used conversion therapy methods in clinic include targeted therapy, immunotherapy, local therapy, radiotherapy and other combination therapy methods. With the in-depth investigation of various clinical studies, more and more patients with liver cancer at intermediate and advanced stages have benefited from conversion therapy. The regimen and efficacy of conversion therapy are described as follows:
Mainly TKIs drugs with representatives including sorafenib, lenvatinib, apatinib, etc. Sorafenib can directly inhibit tumor cell proliferation by inhibiting the rat sarcoma virus (Ras)/rapidly accelerated fibrosarcoma (Raf)/mitogen-activated protein kinase kinase (MEK)/extracellular signal-regulated kinase (ERK) signaling pathway, which was used in the treatment of renal cell carcinoma at first. It was approved by the U.S. Food and Drug Administration (FDA) in 2007 for the treatment of advanced HCC. In a large randomized controlled international multicenter clinical trial (SHARP study), 602 patients with advanced liver cancer who had not received systemic treatment were included and randomized to receive sorafenib or placebo. The results showed that the median overall survival (mOS) in the sorafenib group (n1 = 299) and the placebo group (n2 = 303) was 10.7 months vs. 7.9 months (P<0.001), and the median time to progression (mTTP) was 5.5 months vs. 2.8 months (P<0.001), indicating that sorafenib can postpone the progression of advanced liver cancer and prolong the survival of patients (6). Another clinical study on sorafenib (Oriental study) also came to similar conclusions (7). Sorafenib, as the first molecular targeted drug for the treatment of advanced liver cancer, has made a certain contribution to prolonging the survival of patients. However, due to its low objective response rate (ORR) (about 2.3%), significant adverse reactions, no obvious improvement in the overall survival rate in hepatitis B virus-positive patients, it still cannot fulfill the current needs for treatment of advanced liver cancer.
Lenvatinib is an oral multi-receptor tyrosine kinase inhibitor developed by Eisai. Its main targets are: vascular endothelial growth factor receptor (VEGFR) 1-3, fibroblast growth factor receptor (FGFR) 1-4, platelet-derived growth factor receptor (PDGFR) α, c-Kit, RET etc. A phase III randomized controlled global multicenter non-inferiority clinical study, the REFLECT trial (8), compared lenvatinib with sorafenib. For the primary endpoint of the trial, the mOS in the lenvatinib group was non-inferior to the sorafenib group with a trend of prolongation (13.6 months vs. 12.3 months, P>0.001); in terms of secondary endpoints comparing the lenvatinib with sorafenib, the median progression-free survival (mPFS) (7.4 vs. 3.7 months), mTTP (8.9 vs. 3.7 months), and ORR (24% vs. 9%) all improved. In terms of safety, there was no significant difference between lenvatinib and sorafenib with the incidences of treatment-related adverse events similar between the two groups. Meanwhile, for HBV-related HCC, lenvatinib showed more advantages in prolonging the survival. These data indicated that lenvatinib was not inferior to sorafenib in the efficacy for advanced HCC patients, was superior to sorafenib in secondary endpoints such as ORR and mPFS, and was applicable to a wider population. Therefore, it is recommended by many first-line guidelines to be used in the first-line treatment of unresectable HCC. Tomoko’s team (9) also conducted a clinical study of lenvatinib treatment after failure of PD-1/PD-L1 treatment for liver cancer, finding that the mPFS after lenvatinib treatment was 10 months, mOS was 15.8 months, ORR reached 55.6%, and Disease control rate (DCR) reached 86.1%. It showed that the use of lenvatinib could still increase the chance of conversion and prolong the survival after failure of immunotherapy.
Other drugs, for example, apatinib, a new small-molecule targeted drug independently developed by Jiangsu Hengrui Pharmaceuticals, was initially used for the treatment of advanced gastric cancer, and is now also used in patients with advanced liver cancer who fail or are intolerable to first-line systemic anti-tumor treatment, as a second-line therapeutic regimen for advanced liver cancer. The results of a phase III clinical study of advanced liver cancer in China showed that apatinib, compared with placebo, significantly prolonged the median survival in patients with advanced liver cancer receiving second-line treatment or above, and the ORR reached 10.7%. The risk of death was reduced by 21.5%, and the risk of disease progression was reduced by 52.9% (10).
Currently, targeted drugs combined with immunotherapy has become the first-line treatment strategy for advanced HCC. In the IMbrave150 study, atezolizumab combined with bevacizumab (T+A) achieved better positive results compared with sorafenib, showing significantly improved mOS (19.2 months vs. 13.4 months p < 0.001) and mPFS (6.9 months vs. 4.3 months p < 0.001) in liver cancer patients after treated with the T+A regimen (11). In addition to the T+A regimen, the combination of TKI drugs with PD-1/PD-L1 has also achieved good results. In the phase Ib study Keynote524 (12), the mPFS of lenvatinib combined with pembrolizumab was 9.7 months, the mOS was 20.4 months, and the ORR was 46.3%. In 2019, this regimen was used as the first-line treatment regimen for liver cancer at advanced stage. At the 2020 ASCO-GI meeting, a phase Ib study of lenvatinib combined with nivolumab as the first-line treatment for patients with unresectable liver cancer (13) was reported with the results showing the overall ORR 76.7%, DCR 96.7%, and the clinical benefit rate 83.3%. In the study reported by Zhongshan Hospital affiliated to Fudan University using lenvatinib combined with PD-1 monoclonal antibodies (including nivolumab, camrelizumab, pembrolizumab, sintilimab and toripalimab) in the treatment of advanced HCC (14), the results showed that 6 patients (10.2%) underwent the surgical resection as the tumor had shrunk. Another clinical study of lenvatinib combined with pembrolizumab and apatinib combined with toripalimab in the treatment of unresectable liver cancer was published (15), wherein 10 patients (15.9%) underwent surgical resection 3.2 months (2.4-8.3 months) after the start of treatment and 6 patients (60%) achieved pathological complete response (pCR). In a prospective, uncontrolled, open-label study led by Professor Lu Shichun (16), PD-1 monoclonal antibodies combined with lenvatinib were investigated for the efficacy in the treatment of liver cancer with macrovascular invasion, and the results showed that the ORR was 53.1%(26/49), and the imaging-based conversion rate reached 51.0%, and 15 patients (30.6%) underwent R0 surgical resection. In a retrospective analysis of lenvatinib combined with camrelizumab versus lenvatinib alone, the efficacy in the combination group was improved compared with the single agent group, showing mPFS increasing from 7.5 months to 10.3 months (P<0.05), ORR increasing from 20.5% to 41.7% (P<0.05) (17). It showed that TKI drugs combined with PD-1 is a more effective conversion regimen.
As the most commonly used local treatment method and one of the most common non-surgical treatment methods for liver cancer, Transarterial Chemoembolization (TACE) has certain effects in reducing tumor burden and prolonging patient survival, which is also recommended by many guidelines as the standard treatment for intermediate-stage liver cancer (18–20). However, when it is used alone, the conversion efficiency of TACE is low and recurrence often happens, moreover, multiple TACE can lead to poor efficacy or even resistance (21). Studies have shown that TACE combined with targeted therapy can improve the efficacy of TACE. A retrospective study led by Professor Shi Ming compared the efficacy of TACE combined with sorafenib versus sorafenib monotherapy in the treatment of advanced liver cancer complicated with hepatic vein tumor thrombus. The results showed that the OS and TTP in the TACE combined with sorafenib group were superior to sorafenib monotherapy (22). Ding et al. (23) conducted a study comparing the efficacy of sorafenib combined with TACE (TACE-S) and lenvatinib combined with TACE (TACE-L) in the treatment of advanced liver cancer complicated with portal vein tumor thrombus (PVTT). The results showed that TACE-L was superior to TACE-S in both mOS (14.5 months vs. 10.8 months) and mTTP (4.7 months vs. 3.1 months), and 17 patients (53.1%) in the TACE-L group achieved partial response, compared to 12 (25.0%) in the TACE-S group. Another study has also found that hepatic arterial infusion chemotherapy (HAIC) based on FOLFOX regimen is superior to TACE in efficacy, and HAIC combined with targeted therapy has also achieved good results. A prospective study found that sorafenib combined with HAIC significantly improved the survival and conversion rate compared with sorafenib alone, increasing mOS from 7.13 months to 13.37 months (p<0.05), PFS from 2.6 months to 7.03 months (p<0.05), and improving ORR from 5.7% to 54.4% (24). In a retrospective study reported by Mai at the American Society of Clinical Oncology in 2020 (25), 24 patients with advanced liver cancer who received FOLFOX regimen based HAIC combined with lenvatinib were analyzed showing that ORR and DCR were 66.7% and 79.2%, respectively. Among the targeted treatment combined with local treatment regimens, lenvatinib combined with HAIC achieved the best conversion effect.
Recent studies have shown that targeted immunotherapy combined with local therapy (TACE or HAIC) can further improve the surgical conversion rate of advanced unresectable liver cancer. In a study conducted to explore the efficacy of lenvatinib combined with TACE and pembrolizumab versus lenvatinib combined with TACE in the treatment of unresectable liver cancer, Chen et al. (26) found that the OS and PFS of triple therapy were 18.1 months and 9.2 months respectively, superior to 14.1 months and 5.5 months of dual therapy, and 18 patients (25.7%) in the triple therapy group were successfully downstaged to undergo surgery, while 8 (11.1%) in the dual therapy group underwent surgery. Another retrospective analysis investigating the conversion of triple therapy using anti-angiogenic drugs combined with PD-1 and HAIC for unresectable liver cancer showed that the objective response rate was 96% (24/25) with 14 patients (56%) undergoing surgical resection, including 7 cases achieving pathologic complete response (27). In the retrospective analysis to investigate the efficacy of TACE combined with lenvatinib and sintilimab, the mOS of this regimen was 23.6 months, the mPFS was 13.3 months, and the ORR was 46.7% (28). In the LTHAIC study, a prospective, single-arm phase II clinical study (29), the treatment regimen of lenvatinib + toripalimab + HAIC showed to have an ORR of 66.7% (95% CI, 43.3-75.1), including 5 (13.9%) patients achieving complete radiographic response and 8 patients successfully downstaged to meet the criteria for surgical resection (Table 1). At present, the triple therapy shows the highest conversion efficiency.
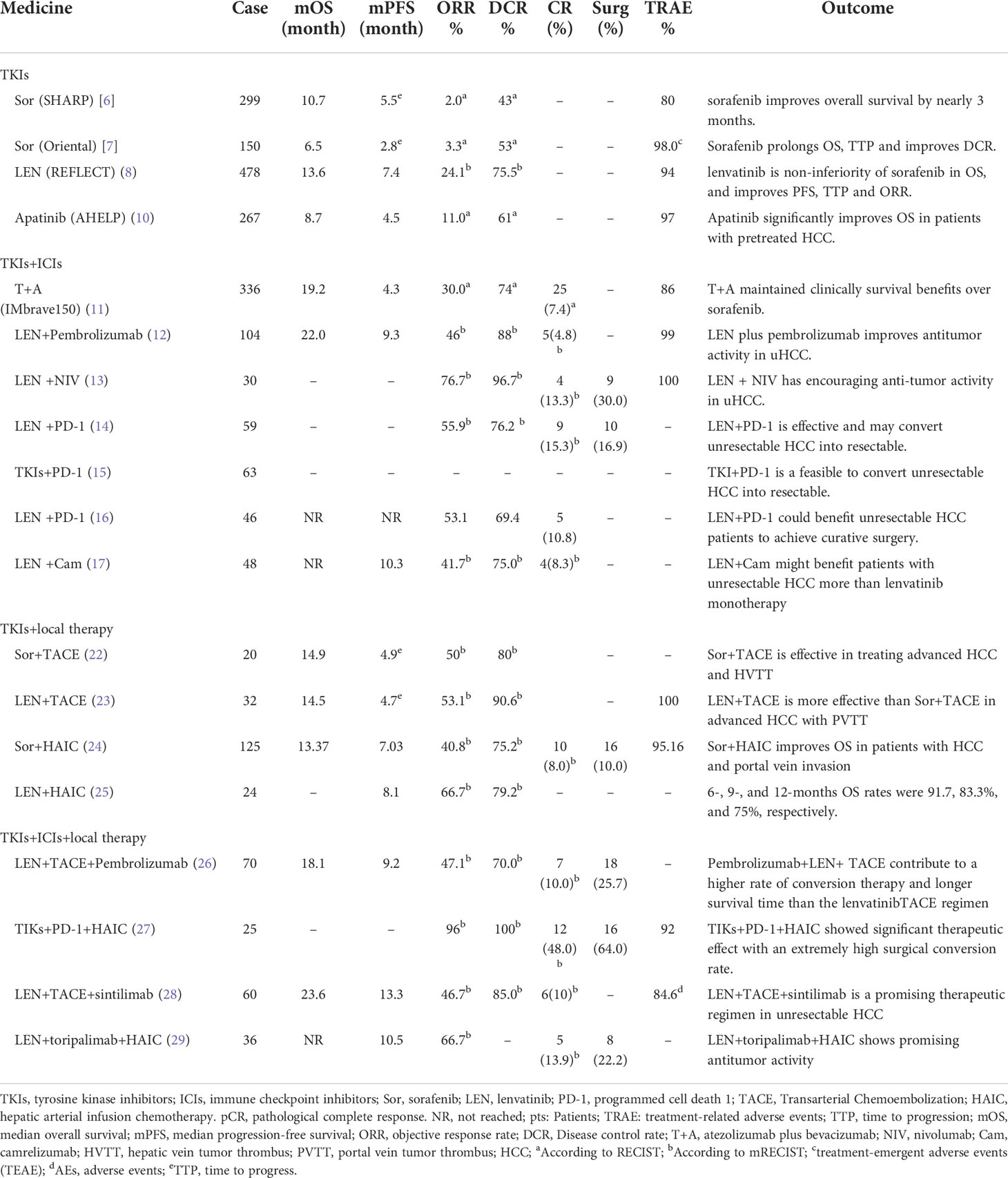
Table 1 Clinical studies of conversion therapy in unresectable HCC patients.
In addition, as portal vein metastasis is prone to occur for liver cancer, many patients complicated with portal vein tumor thrombus cannot undergo surgical resection or the resection effect is poor. Some studies have found that when liver cancer is complicated with portal vein tumor thrombus, combination with radiotherapy can make the tumor thrombus shrink or even disappear, creating conditions for surgery and improving patients’ survival. A large randomized controlled trial (RCT) comparing the efficacy of neoadjuvant radiotherapy followed by resection with direct resection in liver cancer patients with portal vein tumor thrombus showed that the 1-year survival rates of the two groups were 75.2% vs. 43.1%, and the 1-year tumor-free survival rates were 33.0% vs. 14.9%, respectively (30). Toshiya et al. compared the efficacy of radiotherapy followed by surgery with direct surgery. The pathological results after surgery showed that 83.3% of patients in the radiotherapy followed by surgery group achieved pathologically complete necrosis of the main portal vein tumor thrombus with the 5-year survival rate of 34.8%, compared to only 13.1% in the surgery alone group (31). There are also clinical data confirming the efficacy of Transarterial Radioembolization (TARE) in shrinking tumors and its role in the conversion therapy for liver cancer. For cases complicated with portal vein tumor thrombus, TARE shows higher local dose and more precise location than external beam radiotherapy, and also reduces radiation damage to normal liver tissue, with less effect on reserve function (32). Therefore, combination with radiotherapy can further improve the conversion rate and prolong the survival in patients withadvanced liver cancer complicated with portal vein tumor thrombus.
Decades ago, for patients with significant tumor load, many lesions, vascular invasion, or distant metastases, the only therapeutic options were TACE, sorafenib, or symptomatic therapy, and the prognosis was dismal, with a median overall survival rate of 6.5-10.7 months (6, 7, 33). Nowadays, In the era of systematic treatment, the application of TKI drugs and PD-1/PD-L1 has enriched the treatment of liver cancer, expanded the beneficiary group of patients, and median OS has reached 18.1 months or even longer (13, 14, 24, 26). Due to the decrease in tumor volume and stage(reducing the volume and number of primary lesions and eliminating portal vein tumor thrombus and metastatic lesions), part of advanced HCC patients have obtained the opportunity for radical surgery (Table 2) (34).
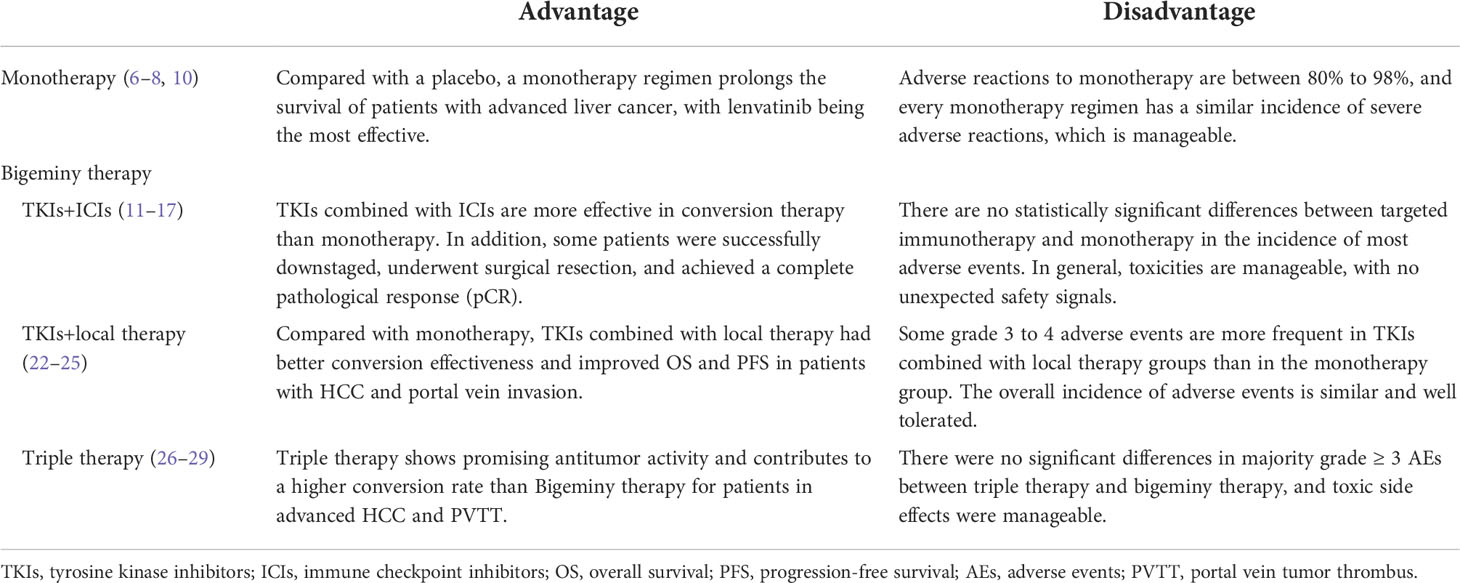
Table 2 Summary of the advantages and disadvantages of monotherapy and combination therapy.
Liver failure caused by insufficient residual liver volume after surgery has become a major restraining factor affecting the surgical resection for liver cancer. For patients undergoing surgery after conversion, the residual liver volume should be maintained over 40% as far as possible. When the requirements cannot be met, portal vein thrombosis (PVE) and associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) can be considered. The complications of PVE were mild, but it took 4-6 weeks to wait for the growth of liver. For some patients who may lose the opportunity for surgery due to tumor progression or insufficient growth of liver, combination with TACE therapy may be considered (35, 36). ALPPS can induce a 47%-192% increase in liver volume within 1-2 weeks, which is much higher than PVE, and the tumor resection rate can also reach 95-100% (37), but it has high incidence of perioperative complications. Therefore, it is necessary to comprehensively evaluate the patient’s condition before surgery, such as level of liver cirrhosis, patient age, the capacity to withstand two surgeries in a short period of time, and the rapid tumor progression (38).
While conversion therapy has achieved promising efficacy results, we need to pay attention to the adverse reactions during the treatment. Common adverse reactions of TKI drugs include hypertension, palmar-plantar erythrodysesthesia syndrome (PPES), loss of appetite, nausea, vomiting and fatigue (39). Immune-related adverse events (irAEs) caused by immune checkpoint inhibitors (ICIs) involve almost all organs, and common adverse reactions include rash and itching, diarrhea and colitis, hepatotoxicity, pneumonia, and thyroiditis (40, 41). The adverse reactions of TACE and HAIC are similar with post-embolization syndrome the most common, mainly manifested as fever, hepatalgia, nausea and vomiting, etc (42), and some adverse reactions caused by chemotherapeutic drugs. The assessment of the above adverse events (AEs) should be performed according to the Common Terminology Criteria for Adverse Events Version 5.0 (CTCEA Version 5.0). For mild adverse reactions, symptomatic treatment can be given. For severe adverse reactions, it is necessary to fully evaluate the patient’s condition, discontinue the current treatment and perform active symptomatic treatment, adjust the treatment dose or even change the regimen, etc. (40–43) Most cases are transient or can be resolved through dose reduction or symptomatic treatment. It has been reported in literature that the occurrence of some TKI-related AEs indicated favorable prognosis (44). Therefore, during the conversion therapy, the tolerance to some adverse reactions can be enhanced for patients, and at the same time, serious adverse reactions that occur during the treatment should be alerted for early detection and timely intervention to ensure the efficacy and safety of conversion.
Radical operation is the essential means of treating primary liver cancer, which is also a necessary means of achieving long-term survival. It is also the core of conversion therapy, which transforms unresectable liver cancer into resectable liver cancer for surgical resection. Usually, there are two reasons for unresectability: surgically unresectable and oncologically unresectable. The former is widely accepted, including the patient’s inability to withstand surgical trauma regarding their general condition, liver function, and insufficient remaining liver volume (surgically unresectable). The latter means Technically resectable but cannot acquire better effectiveness after resection than non-surgical treatment, which is dynamic and controversial (5). Clinically, for unresectable liver cancer, TKIs combined with ICIs can be used initially for conversion attempt, and the reasons for unresectable tumor should be analyzed and evaluated. In case of excessive tumor burden, TACE or HAIC can be added for tumor shrinkage (45, 46); in case of complication with portal vein tumor thrombus, HAIC or TARE can be added (47, 48), or external beam/Stereotactic Body Radiation Therapy (SBRT) radiotherapy can be combined (49) to achieve tumor thrombus shrinkage or even complete disappearance; in case of complication with extrahepatic oligometastasis, radical resection of the primary tumor + resection or ablation of metastasis can be selected if tolerable after sufficient assessment (50, 51).
Since conversion therapy methods can affect tumor, liver, and other organ functions, patients who have the opportunity for surgery after conversion therapy must be evaluated for organ function, target tumor burden, high-risk factor conversion, residual liver volume, and liver function (52). The evaluation includes regular review of enhanced CT, MRI and other imaging data to dynamically compare the changes of lesions and intra- and extra-hepatic metastasis; completion of the Child-Pugh (CTP) grading, indocyanine green (ICG) clearance test, and model for end-stage liver disease (MELD) score, HBV DNA level, etc. to assess liver function and tolerance to surgery; making full use of 3D visualization technology to use a wide incisal margin with tumor boundary >1 cm as the resection range as far as possible, and ensure that FLR accounts for more than 40% of the standard liver volume so as to ensure the safe implementation of surgery (3).
The treatment regimen should not be selected solely based on the staging of liver cancer as some patients with BCLC stage A (or some CNLC stage Ib), who are not suitable for surgical treatment due to excessive tumor burden at the initial diagnosis, should receive conversion therapy before radical resection; some patients with BCLC stage B/C (CNLC stage IIb/IIIa/IIIb) should not be completely considered as equivalent to the advanced stage for systemic therapy alone, but can undergo radical surgery after conversion therapy. It is recommended to use the multidisciplinary team (MDT) model (5) to fully assess the condition and formulate individualized follow-up and treatment strategies. Combined with the current research results, when the liver function, performance status, general condition is favorable, and the patient can tolerate the treatment, try to choose a regimen combining multiple treatment methods, such as targeted treatment combined with local therapy, to improve the tumor response rate and surgical conversion rate.
Surgical resection is an important way for patients to obtain long-term survival after successful conversion. An important condition for conversion resection is to achieve tumor response, or at least to keep the lesions stable for a period of time (3~4 months) (42). Studies have shown that the tumor-free survival of patients after liver cancer conversion resection is related to the degree of pathological response, and the postoperative tumor-free survival is longer in patients with pathological response. In addition, tumor response is only based on imaging, not equivalent to pathological response, and there may be residual cancer cells. Therefore, when the transformed patients achieve the surgically resectable criteria, concurrent surgical treatment should be evaluated as soon as possible to clear necrotic tumor cells or viable tumor cells to achieve the pathological response criteria (52, 53). Timely surgery can also avoid tumor drug resistance and achieve better survival (54).
After the conversion is assessed to be successful, the timing of surgery should also be determined according to the preoperative conversion regimen. Expert consensus recommends: Before surgery, small-molecule targeted drugs (lenvatinib, apatinib, sorafenib, etc.) should be discontinued for more than 1~2 weeks; PD-1 inhibitors should be discontinued for more than 2-4 weeks, bevacizumab should be discontinued for >6 weeks, and bevacizumab should not be used until the wound fully recovers; if TACE or radiotherapy is performed, the surgery should be performed 4 weeks after the last treatment to reduce perioperative complications incidence and ensure the safety of surgery (5).
There is still a lack of sufficient data and high-level evidence-based medical evidence to guide the selection of postoperative adjuvant therapy. However, the success of conversion implies that the tumor is sensitive to the regimen. Therefore, experts recommend that the original regimen or part of the drugs in the original regimen should be used for more than 6 months as appropriate according to the patient’s physical condition, adverse reactions and treatment tolerance. Re-examination should be performed every 3 months, and drug withdrawal can be considered when there is no tumor recurrence or metastasis in two consecutive imaging examinations, and tumor markers are normal for 3 consecutive months without upward trend (5).
Due to the complex pathogenic factors, highly malignant biological behavior of liver cancer, great differences in liver disease backgrounds and prognosis, as well as different individual responses to treatment and the multiple disciplines involved (55), a multidisciplinary team (MDT) is required to evaluate the patients based on the imaging results to further provide individualized treatment regimen. During the treatment, the tumor response should be actively monitored, and the conversion regimen should be adjusted if necessary to create the opportunity for radical surgery with the ultimate goal to enable high-quality long-term survival for patients.
Molecule targeted drugs, represented by TKIs, have achieved promising therapeutic efficacy in existing clinical trials. Combined immunotherapy and local treatment may improve the ORR, increase the proportion of conversion resection rate, and prolong the survival time to benefit more patients with advanced HCC. In addition, PVE and ALPPS increase the residual liver volume, reduce the risk of postoperative liver failure, and ensure the safety of resection. Before choosing the treatment regimen, evaluating the cause of the unresectable, the patient’s liver function and performance status, and selecting an appropriate conversion method are necessary. The application of systemic treatment provides an opportunity for conversion and downstaging for patients with liver cancer at an intermediate and advanced stage and provides the possibility for surgical resection after conversion, thereby bringing hope to prolong overall survival and tumor-free survival.
At present, the research on systemic treatment is in the ascendant, but there are still many problems and challenges: (1) How to better screen the population with efficacy? (2) How to better arrange systemic treatment and local therapy to achieve downstaging effect? (3) How to choose a combination regimen to improve the conversion rate? (4) How to determine the conversion therapy time and arrange the operation time window? (5) Can ctDNA dynamic monitoring make up for the detection effect in patients with negative tumor indicators. More high-quality RCT studies are still needed to provide evidence-based medical data. In the future, higher-definition imaging technology, in conjunction with liquid biopsy, next-generation sequencing (NGS), and other techniques, could be used to assess the liver cancer tumor burden and metastasis in a more accurate and detailed manner in order to create a reasonable, individualized treatment plan for patients, thereby further improving the success rate of conversion and survival rate.
HB, WM, and WC wrote the paper. ML and YY conceived the idea and supervised the manuscript. HB and WM contributed equally to this work. All authors contributed to the article and approved the submitted version.
The study was partly supported by Natural Science Foundation of Guangdong Province (2018A030307076), Medical Science and Technology Funding of Guangdong Province (A2018369) and Clinical Research Project of Affiliated Hospital of Guangdong Medical University (LCYJ2021B002).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol (2019) 16(10):589−604. doi: 10.1038/s41575−019−0186−y
2. Iguchi T, Shirabe K, Aishima S, Wang H, Fujita N, Ninomiya M, et al. New pathologic stratification of microvascular invasion in hepatocellular carcinoma: Predicting prognosis after living-donor liver transplantation. Transplantation (2015) 99(6):1236–42. doi: 10.1097/TP.0000000000000489
3. Zhou J, Sun H, Wang Z, Cong W, Wang J, Zeng M, et al. Guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 edition). Liver Cancer (2020) 9(6):682–720. doi: 10.1159/000509424
4. Zhou H, Song T. Conversion therapy and maintenance therapy for primary hepatocellular carcinoma. Biosci Trends (2021) 15(3):155–60. doi: 10.5582/bst.2021.01091
5. Sun HC, Zhou J, Wang Z, Liu X, Xie Q, Jia W, et al. Chinese Expert consensus on conversion therapy for hepatocellular carcinoma (2021 edition). Hepatobil Surg Nutr (2022) 11(2):227–52. doi: 10.21037/hbsn-21-328
6. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med (2008) 359(4):378–90. doi: 10.1056/NEJMoa0708857
7. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacy and safety of sorafenib in patients in the AsiaPacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo controlled trial. Lancet Oncol (2009) 10(1):25–34. doi: 10.1016/S1470-2045(08)70285-7
8. Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet (2018) 391(10126):1163–73. doi: 10.1016/S0140-6736(18)30207-1
9. Aoki T, Kudo M, Ueshima K, Morita M, Chishina H, Takita M, et al. Exploratory analysis of lenvatinib therapy in patients with unresectable hepatocellular carcinoma who have failed prior PD-1/PD-L1 checkpoint blockade. Cancers (Basel) (2020) 12(10):3048. doi: 10.3390/cancers12103048
10. Qin S, Li Q, Gu S, Chen X, Lin L, Wang Z, et al. Apatinib as second-line or later therapy in patients with advanced hepatocellular carcinoma (AHELP): A multicentre, double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Gastroenterol Hepatol (2021) 6(7):559–68. doi: 10.1016/S2468-1253(21)00109-6
11. Cheng A-L, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol (2021) 76(4):862–73. doi: 10.1016/j.jhep.2021.11.030
12. Finn RS, Ikeda M, Zhu AX, Sung MW, Baron AD, Kudo M, et al. Phase ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma. J Clin Oncol (2020) 38(26):2960–70. doi: 10.1200/JCO.20.00808
13. Kudo M, Ikeda M, Motomura K, Okusaka T, Kato N, Dutcus C, et al. A phase ib study of lenvatinib (LEN) plus nivolumab (NIV) in patients (pts) with unresectable hepatocellular carcinoma (uHCC): Study 117. J Clin Oncol (2020) 38(4):513–3. doi: 10.1200/jco.2020.38.4_suppl.513
14. Sun H-C, Zhu X-D, Huang C, Shen Y, Ge N, Chen Y, et al. Combination therapy with lenvatinib and anti-PD-1 antibodies for unresectable or advanced hepatocellular carcinoma: A real-world study. J Clin Oncol (2020) 38(15):e16610–0. doi: 10.1200/jco.2020.38.15_suppl.e16610
15. Zhu X-D, Huang C, Shen Y-H, Ji Y, Ge NL, Qu XD, et al. Downstaging and resection of initially unresectable hepatocellular carcinoma with tyrosine kinase inhibitor and anti-PD-1 antibody combinations. Liver Cancer (2021) 10(4):320–9. doi: 10.1159/000514313
16. Zhang W, Lu S, Hu B, Wan T, Wang H, Han J, et al. PD-1 inhibitor combined with lenvatinib for unresectable liver cancer as the conversion therapy: An open-label, non-randomized, phase IV study. J Clin Oncol (2022) 39:e16173-3. doi: 10.1200/jco.2021.39.15_suppl.e16173
17. Li Q, Cao M, Yuan G, Cheng X, Zang M, Chen M, et al. Lenvatinib plus camrelizumab vs. lenvatinib monotherapy as first-line treatment for unresectable hepatocellular carcinoma: A multicenter retrospective cohort study. Front Oncol (2022) 12:809709. doi: 10.3389/fonc.2022.809709
18. Benson AB, D’Angelica MI, Abbott DE, Anaya DA, Anders R, Are C, et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw (2021) 19:541–65. doi: 10.6004/jnccn.2021.0022
19. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet (2018) 391(10127):1301–14. doi: 10.1016/S0140-6736(18)30010-2
20. Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology (2018) 67(1):358–80. doi: 10.1002/hep.29086
21. Kudo M, Ueshima K, Ikeda M, Torimura T, Tanabe N, Aikata H, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut (2019) 69(8):1492–501. doi: 10.1136/gutjnl-2019-318934
22. Zhang Y-F, Wei W, Wang J-H, Xu L, Jian PE, Xiao CZ, et al. Transarterial chemoembolization combined with sorafenib for the treatment of hepatocellular carcinoma with hepatic vein tumor thrombus. Onco Targets Ther (2016) 9:4239–46. doi: 10.2147/OTT.S106659
23. Ding X, Sun W, Li W, Shen Y, Guo X, Teng Y, et al. Transarterial chemoembolization plus lenvatinib versus transarterial chemoembolization plus sorafenib as first-line treatment for hepatocellular carcinoma with portal vein tumor thrombus: A prospective randomized study. Cancer (2021) 127(20):3782–93. doi: 10.1002/cncr.33677
24. He M, Li Q, Zou R, Shen J, Fang W, Tan G, et al. Sorafenib plus hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin vs sorafenib alone for hepatocellular carcinoma with portal vein invasion: A randomized clinical trial. JAMA Oncol (2020) 5(7):953–60. doi: 10.1001/jamaoncol.2019.0250
25. Mai Q, Mo Z, Shi F, Chen X. Lenvatinib plus hepatic arterial infusion of modified FOLFOX regime in patients with advanced hepatocellular carcinoma. J Clin Oncol (2020) 38(15_suppl):e16603–3. doi: 10.1200/jco.2020.38.15_suppl.e16603
26. Chen S, Wu Z, Shi F, Mai Q, Wang L, Wang F, et al. Lenvatinib plus TACE with or without pembrolizumab for the treatment of initially unresectable hepatocellular carcinoma harbouring PD-L1 expression: A retrospective study. J Cancer Res Clin Oncol (2021) 148(8):2115–25. doi: 10.1007/s00432-021-03767-4
27. Zhang J, Zhang X, Mu H, Yu G, Xing W, Wang L, et al. Surgical conversion for initially unresectable locally advanced hepatocellular carcinoma using a triple combination of angiogenesis inhibitors, anti-PD-1 antibodies, and hepatic arterial infusion chemotherapy: A retrospective study. Front Oncol (2021) 11:729764. doi: 10.3389/fonc.2021.729764
28. Cao F, Yang Yi, Si T, Luo J, Zeng H, Zhang Z, et al. The efficacy of TACE combined with lenvatinib plus sintilimab in unresectable hepatocellular carcinoma: A multicenter retrospective study. Front Oncol (2021) 11:783480. doi: 10.3389/fonc.2021.783480
29. He M, Ming S, Lai Z, Li Q. A phase II trial of lenvatinib plus toripalimab and hepatic arterial infusion chemotherapy as a first-line treatment for advanced hepatocellular carcinoma (LTHAIC study). J Clin Oncol (2021) 39(15):4083–3. doi: 10.1200/jco.2021.39.15_suppl.4083
30. Wei X, Jiang Y, Zhang X, Feng S, Zhou B, Ye X, et al. Neoadjuvant three-dimensional conformal radiotherapy for resectable hepatocellular carcinoma with portal vein tumor thrombus: A randomized, open-label, multicenter controlled study. J Clin Oncol (2019) 37(24):2141–51. doi: 10.1200/JCO.18.02184
31. Kamiyama T, Nakanishi K, Yokoo H, Tahara M, Nakagawa T, Kamachi H, et al. Efficacy of preoperative radiotherapy to portal vein tumor thrombus in the main trunk or first branch in patients with hepatocellular carcinoma. Int J Clin Oncol (2007) 12(5):363–8. doi: 10.1007/s10147-007-0701-y
32. Kokabi N, Camacho JC, Xing M, El-Rayes BF, Spivey JR, Knechtle SJ, et al. Open-label prospective study of the safety and efficacy of glass-based yttrium 90 radioembolization for infiltrative hepatocellular carcinoma with portal vein thrombosis. Cancer (2015) 121(13):2164–74. doi: 10.1002/cncr.29275
33. Lin S, Hoffmann K, Schemmer P. Treatment of hepatocellular carcinoma: a systematic review. LIVER Cancer (2012) 1(3-4):144–58. doi: 10.1159/000343828
34. Zhao HT, Cai JQ. Chinese Expert consensus on neoadjuvant and conversion therapies for hepatocellular carcinoma. World J GASTROENTERO (2021) 27(47):8069–80. doi: 10.3748/wjg.v27.i47.8069
35. Piron L, Deshayes E, Escal L, Souche R, Herrero A, Pierredon-Foulongne MA, et al. Portal vein embolization: Present and future. Bull Cancer (2017) 104(5):407–16. doi: 10.1016/j.bulcan.2017.03.009
36. Ogata S, Belghiti J, Farges O, Varma D, Sibert A, Vilgrain V. Sequential arterial and portal vein embolizations before right hepatectomy in patients with cirrhosis and hepatocellular carcinoma. Br J Surg (2006) 93:1091–8. doi: 10.1002/bjs.5341
37. Wang Z, Peng Y, Hu J, Wang X, Sun H, Sun J, et al. Associating liver partition and portal vein ligation for staged hepatectomy for unresectable hepatitis b virus-related hepatocellular carcinoma: asingle center study of 45 patients. Ann Surg (2020) 271(3):534541. doi: 10.1097/SLA.0000000000002942
38. Hong deF, Zhang YB, Peng SY, Huang DS.. Percutaneous microwave ablation liver partition and portal vein embolization for rapid liver regeneration: A minimally invasive first step of ALPPS for hepatocellular carcinoma. Ann Surg (2016) 264:e1–2. doi: 10.1097/SLA.0000000000001707
39. Rimassa L, Danesi R, Pressiani T, Merle P. Management of adverse events associated with tyrosine kinase inhibitors: Improving outcomes for patients with hepatocellular carcinoma. Cancer Treat Rev (2019) 77:20–8. doi: 10.1016/j.ctrv.2019.05.004
40. Li ZC, Ren ZG. [Immune checkpoint inhibitors in the treatment and management of hepatocellular carcinoma-related adverse reactions]. Zhonghua Gan Zang Bing Za Zhi (2021) 29(6):600–3. doi: 10.3760/cma.j.cn501113-20191010-00368
41. Sangro B, Chan SL, Meyer T, Reig M, El-Khoueiry A, Galle PR. Diagnosis and management of toxicities of immune checkpoint inhibitors in hepatocellular carcinoma. J Hepatol (2020) 72(2):320–41. doi: 10.1016/j.jhep.2019.10.021
42. Chinese Society of Liver Cancer, China Anti-Cancer Association. Chinese Expert consensus on hepatic arterial infusion chemotherapy for hepatocellular carcinoma (2021 edition). Chin J Dig Surg (2021) 20(7):754–9. doi: 10.3760/cma.j.cn115610-20210618-00288.(inChinese)
43. Obi S, Sato T, Sato S, Kanda M, Tokudome Y, Kojima Y, et al. The efficacy and safety of lenvatinib for advanced hepatocellular carcinoma in a real-world setting. Hepatol Int (2019) 13(2):199–204. doi: 10.1007/s12072-019-09929-4
44. Reig M, Torres F, Rodriguez-Lope C, Forner A, LLarch N, Rimola J, et al. Early,dermatologic adverse events predict better outcome in HCC patients treated with sorafenib. J Hepatol (2014) 61:318–24. doi: 10.1016/j.jhep.2014.03.030
45. Orlacchio A, Chegai F, Merolla S, Francioso S, Giudice CD, Angelico M, et al. Downstaging disease in patients with hepatocellular carcinoma outside up-to-seven criteria: Strategies using degradable starch microspheres transcatheter arterial chemo-embolization. World J Hepatol (2015) 7(12):1694–700. doi: 10.4254/wjh.v7.i12.1694
46. He M-K, Le Y, Li Q-J, Yu ZS, Li SH, Wei W, et al. Hepatic artery infusion chemotherapy using mFOLFOX versus transarterial chemoembolization for massive unresectable hepatocellular carcinoma: A prospective non-randomized study. Chin J Cancer (2017) 36(1):83. doi: 10.1186/s40880-017-0251-2
47. Kudo M, Matsui O, Izumi N, Iijima H, Kadoya M, Imai Y, et al. JSH consensus-based clinical practice guidelines for the management of hepatocellular carcinoma: 2014 update by the liver cancer study group of Japan. Liver Cancer (2015) 3(3-4):458–68. doi: 10.1159/000343875
48. Salem R, Lewandowski RJ, Mulcahy MF, Riaz A, Ryu RK, Ibrahim S, et al. Radioembolization for hepatocellular carcinoma using yttrium-90 microspheres: A comprehensive report of long-term outcomes. Gastroenterology (2009) 138(1):52–64. doi: 10.1053/j.gastro.2009.09.006
49. Kim J, Lee I, Han K, Kim J, Kim K, Choi J, et al. Clinical features of hepatocellular carcinoma patients undergoing resection after concurrent chemoradiation therapy. Int J Radiat Oncol Biol Phys (2012) 84(3):S336–7. doi: 10.1016/j.ijrobp.2012.07.886
50. Hiraki T, Yamakado K, Ikeda O, Matsuoka T, Kaminou T, Yamagami T, et al. Percutaneous radiofrequency ablation for pulmonary metastases from hepatocellular carcinoma: Results of a multicenter study in Japan. J Vasc Interv Radiol (2011) 22(6):741–8. doi: 10.1016/j.jvir.2011.02.030
51. Lassandro G, Picchi SG, Bianco A, Di Costanzo G, Coppola A, Ierardi AM, et al. Effectiveness and safety in radiofrequency ablation of pulmonary metastases from HCC: a five years study. Med Oncol (2020) 37(4):25. doi: 10.1007/s12032-020-01352-2
52. Xiao Z, Chen Y. Hepatectomy after conversion therapy for unresectable advanced hepatocellular carcinoma. Chin J Pract Surg (2021) 41(3):275–80. doi: 10.19538/j.cjps.issn1005-2208.2021.03.08.(inchinese)
53. Cloughesy TF, Mochizuki AY, Orpilla JR, Hugo W, Lee AH, Davidson TB, et al. Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma. Nat Med (2019) 25(3):477–86. doi: 10.1038/s41591-018-0337-7
54. O’Donnell JS, Hoefsmit EsméeP, Smyth MJ, Blank CU, Teng MWL. The promise of neoadjuvant immunotherapy and surgery for cancer treatment. Clin Cancer Res (2019) 25(19):5743–51. doi: 10.1158/1078-0432.CCR-18-2641
Keywords: primary liver cancer, systemic treatment, conversion therapy, downstaging, surgical resection
Citation: Bei H, Mai W, Chen W, Li M and Yang Y (2022) Application of systemic treatment in conversion therapy options for liver cancer. Front. Oncol. 12:966821. doi: 10.3389/fonc.2022.966821
Received: 11 June 2022; Accepted: 21 September 2022;
Published: 06 October 2022.
Edited by:
Hong-Tao Hu, Henan Provincial Cancer Hospital, ChinaReviewed by:
Ming Yang, University of Missouri, United StatesCopyright © 2022 Bei, Mai, Chen, Li and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mingyi Li, bGltaW5neWk2M0AxNjMuY29t; Yongguang Yang, eW9uZ2d1YW5neWFuZzc5QDE2My5jb20=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.