
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Oncol., 19 July 2022
Sec. Molecular and Cellular Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.957580
This article is part of the Research TopicNew Understandings and Research in Anal Squamous Cell CarcinomaView all 9 articles
 Magali Rebucci-Peixoto1,2*
Magali Rebucci-Peixoto1,2* Angélique Vienot1,2,3
Angélique Vienot1,2,3 Olivier Adotevi1,2,3
Olivier Adotevi1,2,3 Marion Jacquin2,4
Marion Jacquin2,4 Francois Ghiringhelli5
Francois Ghiringhelli5 Christelle de la Fouchardière6Benoit You7Tristan Maurina1Elsa Kalbacher1Fernando Bazan1Guillaume Meynard1Anne-Laure Clairet8Christine Fagnoni-Legat8Laurie Spehner3Adeline Bouard3
Christelle de la Fouchardière6Benoit You7Tristan Maurina1Elsa Kalbacher1Fernando Bazan1Guillaume Meynard1Anne-Laure Clairet8Christine Fagnoni-Legat8Laurie Spehner3Adeline Bouard3 Dewi Vernerey1,9
Dewi Vernerey1,9 Aurélia Meurisse1,9
Aurélia Meurisse1,9 Stefano Kim2,3,10Christophe Borg1,2,3Laura Mansi1
Stefano Kim2,3,10Christophe Borg1,2,3Laura Mansi1Background: There is a strong rational of using anti–programmed cell death protein-1 and its ligand (anti–PD-1/L1) antibodies in human papillomavirus (HPV)–induced cancers. However, anti–PD-1/L1 as monotherapy induces a limited number of objective responses. The development of novel combinations in order to improve the clinical efficacy of an anti–PD-1/L1 is therefore of interest. Combining anti–PD-1/L1 therapy with an antitumor vaccine seems promising in HPV-positive (+) cancers. UCPVax is a therapeutic cancer vaccine composed of two separate peptides derived from telomerase (hTERT, human telomerase reverse transcriptase). UCPVax is being evaluated in a multicenter phase I/II study in NSCLC (non–small cell lung cancer) and has demonstrated to be safe and immunogenic. The aim of the VolATIL study is to evaluate the combination of atezolizumab (an anti-PD-L1) and UCPVax vaccine in a multicenter phase II study in patients with HPV+ cancers.
Methods: Patients with HPV+ cancer (anal canal, head and neck, and cervical or vulvar), at locally advanced or metastatic stage, and refractory to at least one line of systemic chemotherapy are eligible. The primary end point is the objective response rate (ORR) at 4 months. Patients will receive atezolizumab every 3 weeks at a fixed dose of 1,200 mg in combination with the UCPVax vaccine at 1 mg subcutaneously.
Discussion: Anti-cancer vaccines can restore cancer-immunity via the expansion and activation of tumor-specific T cells in patients lacking pre-existing anti-tumor responses. Moreover, preclinical data showed that specific TH1 CD4 T cells sustain the quality and homing of an antigen-specific CD8+ T-cell immunity. In previous clinical studies, the induction of anti-hTERT immunity was significantly correlated to survival in patients with advanced squamous anal cell carcinoma. Thus, there is a strong rational to combine an anti-cancer hTERT vaccine and an immune checkpoint inhibitor to activate and promote antitumor T-cell immunity. This pivotal proof of concept study will evaluate the efficacy and safety of the combination of a telomerase-based TH1 inducing vaccine (UCPVax) and an anti–PD-L1 (atezolizumab) immunotherapy in HPV+ cancers, as well as confirming their synergic mechanism, and settling the basis for a new combination for future clinical trials.
Clinical Trial Registration: https://www.clinicaltrials.gov/, identifier NCT03946358.
More than 90% of anal and cervical cancers and about 70% of oropharyngeal cancers are linked to the human papillomavirus (HPV) infection (1, 2), and their incidence is steadily increasing (3, 4). HPV oncogenic proteins are trans-activators of telomerase (5). Telomerase is an enzyme that is re-expressed in most tumor cells and it ensures the reconstitution of the telomeres, which are shortened at each cell division and prevents the entry of the cell in replicative senescence. This enzyme is composed of a catalytic subunit, human telomerase reverse transcriptase (hTERT) and a structural subunit composed of a telomerase RNA component (TERC). The main mechanism of telomere maintenance in cancers depends on the reactivation of hTERT, which is overexpressed in more than 90% of human cancers, thus conferring to cancer cells a form of immortality (6).
This overexpression of telomerase in tumor cells compared with normal cells confers to hTERT the property of a tumor antigen. Our group has conducted a clinical trial (Epitopes-HPV01 and Epitopes-HPV02) in advanced squamous cell anal cancer where a correlation was evidenced between the presence of anti-HPV immunity and anti-telomerase TH1 CD4 T-cell responses. We could unwaveringly establish that telomerase is an appropriate antigen in HPV-related cancers (7, 8).
Besides, tumor-reactive CD4+ T cells have been found to ensure efficient effector cytolytic T lymphocytes (CTLs) recruitment at the tumor site (9, 10). In consequence, the promotion of tumor specific TH1 CD4 activation might be an attractive therapeutic option to enhance anti–programmed cell death protein-1 and its ligand (anti–PD-1/L1) efficacy (11). However, no option is currently available to expand tumor specific TH1 lymphocytes in most patients. We have used an optimized reverse immunology approach to identify four novel MHC class II–restricted peptides derived from hTERT referred as “Universal Cancer Peptides” (UCP). UCPVax is a therapeutic cancer vaccine composed of two separate peptides called UCP2 and UCP4 derived from telomerase (12). This UCPVax vaccine is currently being evaluated in a multicenter phase I/II study in NSCLC (NCT2818426). Results from the phase I study indicated that UCPVax was safe, well tolerated, and immunogenic at the doses and schedule tested, and 1 mg of each peptide was recommended for phase II. UCPVax was immunogenic in 60% of NSCLC patients at least after three injections, with preliminary signals of clinical efficacy in this population. Accordingly, we selected this 1-mg dose of each peptide in the VolATIL study.
Preclinical and clinical data demonstrated PD-1/L1 immune checkpoint as a relevant target for immunotherapy in HPV+ cancers, based on the prominent role of PD-1 and PD-L1 in HPV-driven immune evasion. The role of PD-L1 in immune evasion of HPV-associated tumors was well described in head and neck squamous cell carcinoma (HNSCC). A membranous expression of PD-L1 on epithelial cells and macrophages was observed in tonsillar crypts of HPV-infected patients. Similarly, the majority of CD8+ T lymphocytes of these patients expressed high levels of PD-L1 (13–15). In mice, PD-1 neutralization synergized with HPV vaccine to promote an anti-tumor immunity (16).
Recent clinical trials also confirmed the interest of PD-1/L1 inhibitors in HPV+ cancers. In patients with advanced squamous cell carcinoma of the anus (SCCA), refractory to at least one line of treatment, five prospective phase I/II trials included 298 patients (11, 17–21). ORR was 13.4% including the 3.7% of complete responses. The median overall survival (OS) was approximately 11 months (Table 1). In cervical cancer patients with PD-L1–positive advanced disease and refractory to at least one systemic treatment, pembrolizumab induced an ORR in 15 of 101 (14.9%) patients including two (2%) complete responses in two prospective trials (22, 23). In HNSCC, the strongest available data for checkpoint inhibitors in refractory disease come from an initial and expansion cohort of a phase Ib study using pembrolizumab in the recurrent/metastatic setting. Among 192 patients enrolled, 18% presented an objective response including four complete responses (24).

Table 1 PD1/L-1 treatment in patients with refractory-advanced squamous cell carcinoma of the anus.
Even though anti–PD-1/L1 therapies in HPV+ cancers are effective, the benefit is limited to approximately 15% of patients in monotherapy, and only a few patients achieved a long-term remission. Therefore, the development of a novel combination in order to extend the clinical efficacy of anti–PD-1/L1 is of great interest.
Altogether, the combination of anti–PD-1/L1 therapy with an antitumor vaccine gains serious consideration in HPV+ cancers. In the present VolATIL clinical trial, we will evaluate the clinical interest and immunological efficacy of a treatment combining the UCPVax with anti–PD-L1 therapy (atezolizumab) in patients with HPV+ cancers (anal canal, cervix and vulvar, and oropharyngeal cancers) by evaluation of the objective response rate (ORR) at 4 months according to iRECIST criteria. We will also explore, as a secondary objective, the feasibility of specific tumor-infiltrating lymphocytes (TIL) production.
VolATIL study is a multicenter phase II trial to evaluate the combination of atezolizumab and UCPVax in advanced HPV+ cancer patients, refractory to at least one line of systemic chemotherapy. The study was developed by the “National Institute of Health and Medical Research (INSERM), Unit 1098” and “Clinical Investigational Center (CIC) 1431”. The study is sponsored by the CHU of Besançon and supported by INCa (French National Cancer Institute) and ROCHE. The data management is undertaken by the “Methodology and Quality of Life Unit in Oncology”* from the University Hospital of Besançon. The trial is registered on the clinicaltrials.gov database (NCT03946358).
The study has received a favorable opinion from the Ethic Committee “Sud-Est IV” and the authorization from the French National Agency for the Safety of Medicines and Health Products and will be conducted in accordance with the Declaration of Helsinki and the Good Clinical Practice.
* http://www.umqvc.org/en/index.html
The main objective of this clinical trial is to assess the efficacy of the strategy combining UCPVax and atezolizumab in patients with advanced refractory HPV+ cancer by evaluation of the ORR at 4 months according to iRECIST.
The secondary objectives are the following:
● OS
● Progression-free survival (PFS)
● Health-related quality of life (QoL)
● Safety of atezolizumab in combination with UCPVax
● Ability of UCPVax and atezolizumab to promote the activity of antigen specific T lymphocytes in the peripheral blood
● Ability of UCPVax and atezolizumab to enhance the tumor cell infiltration by specific lymphocytes (tumor-infiltrating lymphocytes, TIL)
● Feasibility of TIL expansion in HPV+ cancer patients
● Research of biomarkers
The study population consists of patients with HPV+ (defined by p16+ by immunohistochemistry or HPV genotyping) cancer, locally advanced or metastatic, and refractory to systemic chemotherapy, corresponding to one of the following selected types:
● Carcinoma of the anus
● Carcinoma of the head and neck
● Carcinoma of the cervix or vulva
Patients should have an ECOG-PS <2 and adequate organ function.
The main inclusion and exclusion criteria are listed in Table 2.
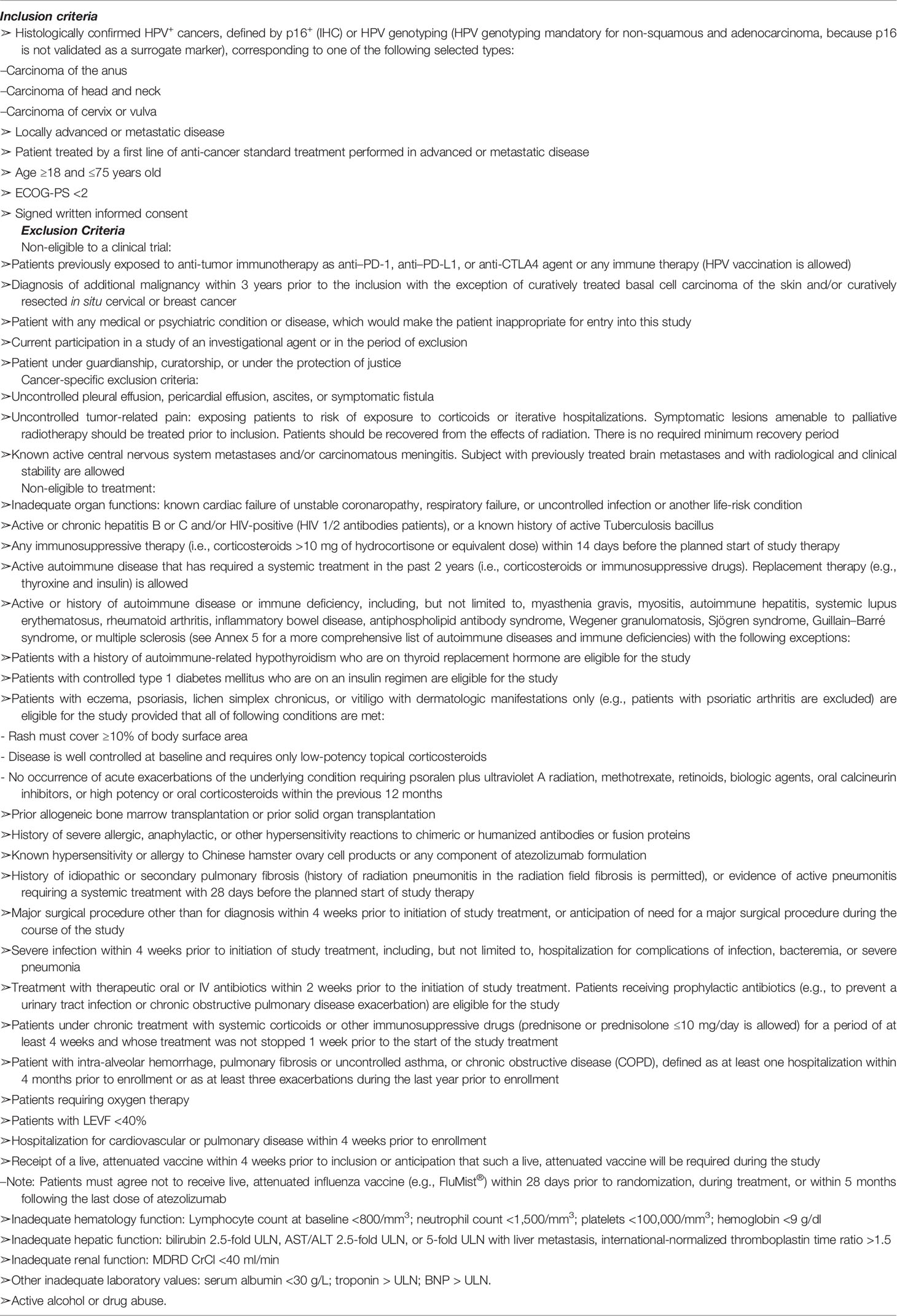
Table 2 Main inclusion and exclusion criteria.
Patients will receive atezolizumab every 3 weeks, at fixed dose of 1,200 mg in 60-min intravenous (IV) infusion before UCPVax injection, until disease progression or unacceptable toxicity or maximum of 2 years. If atezolizumab is well tolerated at the first cycle, atezolizumab perfusion can be reduced to 30 min in the following cycles. No dose adjustment is required. No premedication treatment is required before infusion of atezolizumab.
UCPVax is a telomerase-derived cancer vaccine developed by our academic research network at Besançon (Pr Adotevi, UMR1098 INSERM/EFS/UFC) and patented (n° EP: 12305319 and n° US: 61/621.075) by a consortium including the Regional University Hospital of Besançon and the University of Bourgogne Franche-Comté.
The Good Manufacturing Practice (GMP) drug substance of UCPVax was produced by PolyPeptide biotech (Strasbourg, France). Clinical grade peptide production and formulation will be performed according to GMP preparation and compliance by the Pharmacy Department of the University Hospital of Besançon like in the previous trial in lung cancer (Clinical Trial NCT02818426).
The two UCPVax peptides, UCP2 and UCP4 at 1 mg/ml (combined with Montanide ISA51 as adjuvant), will be injected subcutaneously in two separate sites (one site per peptide) (Figure 1) at days 1, 8, 15, 29, 36, and 43 (priming phase) following by boost vaccinations: every 6 weeks for the two first boosts (W13 and W19) and every 9 weeks afterward (W28, W37, and W46).
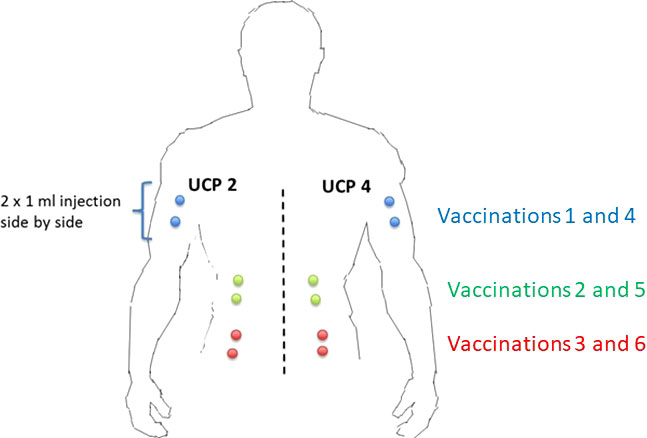
Figure 1 Injection sites of each peptide. The two UCPVax peptides, UCP2 and UCP4 at 1 mg/ml (combined with Montanide ISA51 as adjuvant), will be injected subcutaneously in two separate sites (one site per peptide) at days 1, 8, 15, 29, 36, and 43 (priming phase) following by boost vaccinations: every 6 weeks for the two first boosts (W13 and W19) and every 9 weeks afterward (W28, W37, and W46).
Initial assessments will be performed at baseline, within 28 days prior to the first administration of the combination atezolizumab and UCPVax. Treatment will include three phases (Figure 2):
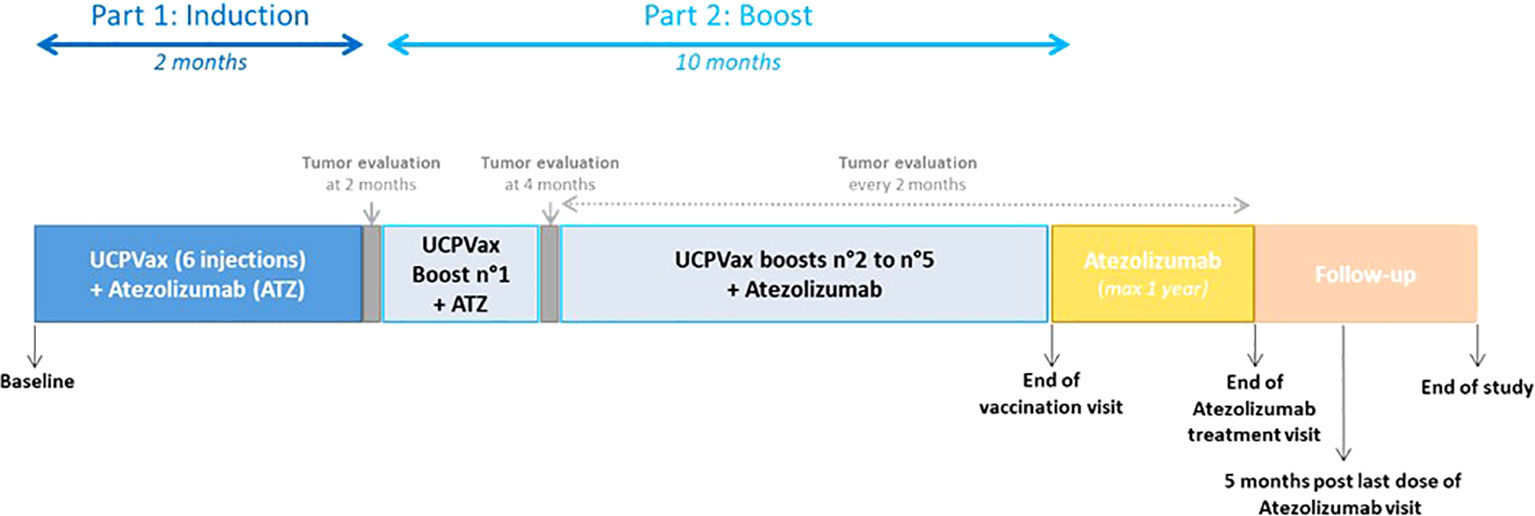
Figure 2 Therapeutic sequences. Part 1 Induction phase: Atezolizumab (1,200 mg IV) will be administrated every 3 weeks starting at day 1. UCPVax will be injected subcutaneously at weeks 1, 2, 3, 5, 6, and 7. The two peptides included (UCP2 and UCP4) in UCPVax will be injected subcutaneously in separate sites (one site per peptide) after emulsion in the adjuvant (Montanide ISA-51 VG). Part 2: Boost phase of UCPVax+. Atezolizumab: Atezolizumab will be administered at the standard dose of 1,200 mg IV every 3 weeks. UCPVax boosts vaccine will be performed every 6 weeks for the two first boosts (W13 and W19) and then every 9 weeks thereafter (W28, W37, and W46). Part 3: Atezolizumab in monotherapy will be administrated every 3 weeks until disease progression or unacceptable toxicities for a maximum of 1 year since the last vaccine.
Atezolizumab, 1,200 mg IV, will be administrated every 3 weeks starting at day 1. UCPVax will be injected subcutaneously (according to previous phase I/II study) at weeks 1, 2, 3, 5, 6, and 7. The two peptides included (UCP2 and UCP4) in UCPVax will be injected subcutaneously in separate sites (one site per peptide) after emulsion in the adjuvant (Montanide ISA-51 VG). Tumor assessment will be made according to iRECIST criteria every 8 weeks with a total body CT scan (if progressive disease, it could be confirmed by another total body CT scan 4 to 8 weeks after the precedent).
Only patients with stable, partial, or complete response at disease evaluation visit at 4 months will be included to Part II. Atezolizumab will be administered at the standard dose of 1,200 mg IV every 3 weeks. UCPVax boosts vaccine will be performed every 6 weeks for the two first boosts (W13 and W19) and then every 9 weeks thereafter (W28, W37, and W46).
Atezolizumab in monotherapy will be administrated every 3 weeks until disease progression or unacceptable toxicities for a maximum of 1 year since the last vaccine.
For the primary end-point analysis, a total body CT scan will be performed at baseline, and every 8 weeks until progression. Additional total body CT scan could be performed if clinically indicated.
For immunological safety assessment, three blood samples will be collected:
● Sample N°1: At inclusion visit before the first treatment
● Sample N°2: At week 5 (before vaccination n°4)
● Sample N°3: At 2 months from inclusion
In case of immune-related adverse event, these analyses will be performed:
- Immunological blood analysis: IgG, IgE, circulating antibodies (ANA and TPO), CRP, and ferritin. Serum (one dry tube, 6 ml) will be frozen for the measure of anti-telomerase peptide (anti-UCP) antibodies.
- Cytokines release measurement (one EDTA tube, 6 ml): Plasma will be frozen for analysis of IL-1b, IL-6, IL-8, IL-2, TNFα, IFN-g, IL-17, and sCD25.
For immunomonitoring analysis, four blood samples will be collected at the following:
● Sample N°1: at baseline
● Sample N°2: at 2 months from inclusion
● Sample N°3: at 4 months from inclusion
● Sample N°4: at the end of vaccine visit
Biomonitoring Blood Samples: Six 6-ml EDTA tubes for PBMC collection, one 6-ml EDTA tubes for plasma collection, and one 6-ml EDTA tube for ctDNA collection will be collected for analysis.
Specific anti-tumor immune responses and HPV circulating DNA analysis will be performed in collaboration with UMR1098 INSERM/EFS/UFC team and with the Cellular and Molecular Laboratory and the Pathological Laboratory of the University Hospital of Besançon
● Immunohistochemistry analysis of anti-tumor responses: Immunohistochemistry analysis will be performed to evaluate p53, p16, and anti-tumor responses to: Class I CMH, Foxp3, pSTAT3, T-bet and immune infiltrates, CD8, and GRZM. This analysis will be performed on tumor samples.
● Genotyping: Genotyping will be performed on tumor samples obtained by biopsies at diagnosis. This analysis will be performed to characterize the genomic profile of cancers and to determine the influence of the neoantigen charge on the combination therapy. If the tumor sample is sufficient, RNAseq analysis will be performed to determine biomarkers that predict the efficacy of the combination therapy. HPV genotyping will be carried out using the INNO-LiPA technique. In addition, a search for the viral genome integration via E6, E7, and E2 proteins will be carried out.
● Quantification of circulating HPV DNA in plasma by qPCR targeting E6 and E7 will be done before and during treatment.
● Peripheral blood immune phenotyping and plasma-derived biomarkers
- Monocytes and MDSC will be phenotyped by flow cytometry
- Regulatory T lymphocytes (CD3/CD4/CD25/Foxp3/CD45RA, CD15s, and CD127)
- Immune checkpoint and costimulatory molecules will be analyzed on CD8 and CD4 T-cell lymphocytes (PD-1, TIM3, TIGIT, LAG3, CD226, OX40, 41BB, CTLA4, and CD26)
- Angiogenic-related growth factors will be monitored in the plasma of included patients at baseline and 2 months after treatment initiation
● Assessment of antigen-specific T cells
- Peripheral blood mononuclear cells will be exposed to E6, E7, and hTert-derived peptides. CD4- and CD8-specific T-cell IFN-γ production will be monitored by ELISpot IFN-γ. Similar experiments will be performed using TIL.
These experiments will allow us to determine the presence of antigen-specific T cells before and after treatment as well as the ability of combined vaccination and atezolizumab therapy to enhance the diversity of immune responses (epitope spreading).
● A fresh tumor biopsy for TIL production proof of concept will be performed and centralized at baseline and at 2 months. Collection of tumor biopsies will be guided by ultrasound or CT scan. Methods for TIL culturing were the same as those used by the Rosenberg group (25).
● Tumor samples obtained by biopsies or surgery at diagnosis will be centralized for the translational research program.
A health-related QoL EORTC QLQ-C30 questionnaire will be collected:
- at inclusion,
- every 8 weeks until the end of treatment visit, and
- at the end of vaccine visit.
For each patient enrolled in VolATIL study, the investigators will document all required data in the corresponding source documents. These data will then be entered in the electronic case report form (eCRF), which will be accessible only to authorized persons via a secured web connection. One eCRF will be created for each patient. The investigator has the responsibility for its completion, proof reading, and its approval after the final verification for the authenticity and accuracy of all entered data. University Hospital of Besançon (Sponsor) will ensure that the study is conducted in accordance with the Good Clinical Practice guidelines and all applicable local laws and that the rights, security, and wellbeing of the patient are respected. The Sponsor will perform source document verification and validation as well as request clarification to ensure the accuracy, completeness, and reliability of data. At the end of the data handling process, a data review meeting will be held to prepare the database lock. After the database lock, data will be transferred into SAS format. Methodology and Quality of Life Unit in Oncology from the University Hospital of Besançon will produce statistical analyses.
VolATIL trial is a one-arm two-stage phase II design. The aim is to demonstrate that the ORR at 4 months according to iRECIST is clearly above a low rate (such as 20%) that would be not satisfactory. The following hypotheses will be considered:
- H0 (null): An ORR rate at 4 months of 20% is uninteresting
- H1 (alternative): An ORR rate at 4 months of 45% is expected
According to Simon two-stage design (optimum method) with a one-sided 2.5% type I error and power of 90%, 42 evaluable patients at 4 months will need to be included in order to test the previous hypotheses.
The hypotheses regarding an uninteresting rate of 20% are based on previous studies (17–20, 22–24, 26). An anticipated ORR rate at 4 months of 45% would be considered clinically meaningful.
Stage 1: After recruitment of the first 14 evaluable patients with a 4-month follow-up from inclusion,
● if three or less than three patients present an objective response at 4 months (21.4%), the treatment could be declared uninteresting. No more additional patients will be included in this arm
● if 4–14 patients present an objective response at 4 months, 28 additional patients will be enrolled in the study.
The probability to conclude for futility at the end of stage 1 whereas p = 45.0% is β1 = 6.3%. This early look interim analysis is planned to look for an early efficacy and safety data.
Stage 2: After recruitment of 42 evaluable patients with a follow-up of 4 months from inclusion,
● if 13 or less than 13 patients present an objective response at 4 months (≤ 31.0%), the treatment will be declared uninteresting
● if 14 or more than 14 patients present an objective response at 4 months (≥ 33.0%), the treatment will be regarded as interesting for further evaluation in a phase III trial.
Of note, the rational for H1 hypothesis is sustained by the results of HPV vaccination combined with nivolumab where an ORR of 33% was observed (27).
The probability to conclude for futility at the end of stage 2 whereas p = 45.0% is β2 = 9.3% (i.e. power = 90.7%). The probability to conclude for efficacy at the end of stage 2 whereas p = 20.0% is α2 = 2.5%. With an expected 10% rate of patients not evaluable or lost to follow-up at 4 months, it will be necessary to include (42*100)/90 = 47 patients in the study.
An Independent Data and Safety Monitoring Committee (IDMC) will be constituted and will meet for the validation of the passage from stage 1 to stage 2 for the monitoring of toxicities and also for the reviewing of SAEs every 6 months.
In parallel, given that the safety profile of UCPVax and atezolizumab combination has not been evaluated in patients with HPV-positive cancer so far, a semi-continuous monitoring for toxicity using Pocock-type boundary will be performed [probability of early stopping: 0.05, targeted dose-limiting toxicity (DLT) rate: 0.20]. Patient recruitment will be stopped and discussed with the DSMB (Data Safety Monitoring Board) at the end of stage 1 if 7 or more patients of 14 enrolled patients with a 4-month follow-up experience relevant DLT.
The primary analysis will be on modified intention-to-treat (mITT) population, i.e., including all evaluable patients regardless of their eligibility and treatment received. Confirmative analyses will be conducted firstly in the ITT population (not assessable patients and patients with dropout between inclusion and 4 months will be considered as progressive) and, secondly, in the Per Protocol population defined as patients who have received at least one dose of treatment and presenting no major deviations from the protocol.
Safety analyses will be conducted in all patients who have received at least one dose of allocated treatment.
This study will end once the 47 recruited patients have performed the “5 months post last dose of atezolizumab” visit.
Every patient participating in this study can stop the trial at any moment and has no need to justify the reason for this decision. In that case, patients will pursue the standard medical care.
The reason for an early end of the study must be declared as one of the following criteria: patient’s decision, severe adverse event, protocol deviation, loss of follow-up, or death.
An “Independent Data and Safety Monitoring Committee” (IDMC) represented by a multidisciplinary team, including physicians from relevant medical disciplines and biostatistical background, is implemented to the following:
✓ ensure the safety and wellbeing of the patients exposed to study treatment through the ongoing review of safety data
✓ assure the highest integrity about operation and performance of the trial
✓ evaluate ongoing safety data to detect the possibility of an unfavorable early treatment risk. IDMC will meet for the validation of the passage from stage 1 to stage 2 (see the Statistical considerations section) for the monitoring of toxicities and also for the reviewing of SAEs every 6 months. IDMC will meet also in case of unexpected toxicities or as requested.
IDMC’s responsibilities are as follows:
✓ to review safety data on an ongoing basis
✓ to recommend that the clinical study be stopped early if there is strong evidence that the investigational medicinal products are harming patients
✓ to make recommendations regarding modification of the study if there is strong evidence that such change would substantially contribute to the wellbeing of patients.
Safety results and opinion of the committee will be sent to the ANSM (French Health Products Safety Agency) within 10 days after the analyses of tolerance (additional meetings will be performed in any event of a signal that may affect patients’ safety).
The IDMC will independently make its recommendations for continuation or termination of the trial to the appropriate Sponsor contact. The IDMC will maintain records of all its meetings and activities related to the study.
These records will remain confidential until completion of the final analysis at which time they will be forwarded to the Sponsor for appropriate filing.
Members will be aware of data management and quality control procedures and ensure that the data are timely, accurate, and complete.
Current clinical trials have shown that less than one patient out of five achieved clinical responses to anti–PD-1 monotherapy. Combining such immune checkpoint inhibition treatment with vaccination might increase the number of patients achieving a clinical benefit. In this combination trial, more than 45% of objective responses are expected.
There is currently no consensus on standard of care for HPV+ squamous carcinoma previously exposed to platinum containing chemotherapies. Combining atezolizumab with TH1-promoting vaccine might constitute an alternative therapeutic option for these patients.
The studies involving human participants were reviewed and approved by The French National Agency for the Safety of Medicines and Health Products CPP Sud-Est IV. The patients/participants provided their written informed consent to participate in this study.
Conception and design: LM, TM, DV, SK, and CB; Protocol writing: LM, TM, MR-P, and CB; Methods: AV, DV, and CB. Study promotion: MJ and MR-P; Manuscript writing: MR-P, SK, and CB; Critical lecture and final approval of the manuscript: all authors.
Roche France provides atezolizumab. INCa (Institut National du Cancer) and Fondation ARC (Inca-ARC_13566) fund the study.
CB: Research grant from Bayer and Roche, advisory board for Bayer, Sanofi, MSD. FB: Novartis, Seagen, Daiichi Sankyo, Pierre Fabre, Astra-Zeneca, Clovis. SK: reports a consulting or advisory role for Ipsen, Incyte, Boehringer Ingelheim, Sanofi and BeiGene and has received research funding from Pfizer, Roche, Novartis, Bristol-Myers Squibb, Boehringer Ingelheim and Sanofi.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank Guadalupe Inés Tizón for English writing assistance. The authors would like to thank DRCI (Délégation de la Recherche Clinique et de l'Innovation) for assistance in submitting study to regulatory authorities.
ECOG-PS, Eastern Cooperative Oncology Group-performance status; eCRF, electronic case report form; HNSCC, Head and Neck Squamous Cell Carcinoma; HPV, human papilloma virus; HR, hazard ratio; IDMC, Independent Data and Safety Monitoring Committee; NSCLC, Non–Small Cell Lung Cancer; ORR, objective response rate; OS, overall survival; PD1/PD-L1, programmed cell death protein-1 immune checkpoint and its ligand; PFS, progression-free survival; QoL, health-related quality of life; SCCA, Squamous cell carcinoma of the anus.
1. Alemany L, Saunier M, Alvarado-Cabrero I, Quirós B, Salmeron J, Shin H-R, et al. Human Papillomavirus DNA Prevalence and Type Distribution in Anal Carcinomas Worldwide. Int J Cancer (2015) 136:98–107. doi: 10.1002/ijc.28963
2. Gillison ML, Castellsagué X, Chaturvedi A, Goodman MT, Snijders P, Tommasino M, et al. Eurogin Roadmap: Comparative Epidemiology of HPV Infection and Associated Cancers of the Head and Neck and Cervix. Int J Cancer (2014) 134:497–507. doi: 10.1002/ijc.28201
3. Chaturvedi AK, Engels EA, Pfeiffer RM, Hernandez BY, Xiao W, Kim E, et al. Human Papillomavirus and Rising Oropharyngeal Cancer Incidence in the United States. JCO (2011) 29:4294–301. doi: 10.1200/JCO.2011.36.4596
4. Almaazmi H, Taylor JP, Stem M, Yu D, Lo BD, Safar B, et al. Anal Squamous Cell Carcinoma: Radiation Therapy Alone Must Be Avoided. J Surg Res (2020) 247:530–40. doi: 10.1016/j.jss.2019.09.049
5. Veldman T, Horikawa I, Barrett JC, Schlegel R. Transcriptional Activation of the Telomerase hTERT Gene by Human Papillomavirus Type 16 E6 Oncoprotein. J Virol (2001) 75:4467–72. doi: 10.1128/JVI.75.9.4467-4472.2001
6. Liu X, Dakic A, Chen R, Disbrow GL, Zhang Y, Dai Y, et al. Cell-Restricted Immortalization by Human Papillomavirus Correlates With Telomerase Activation and Engagement of the hTERT Promoter by Myc. J Virol (2008) 82:11568–76. doi: 10.1128/JVI.01318-08
7. Kim S, François E, André T, Samalin E, Jary M, Hajbi El F, et al. Docetaxel, Cisplatin, and Fluorouracil Chemotherapy for Metastatic or Unresectable Locally Recurrent Anal Squamous Cell Carcinoma (Epitopes-HPV02): A Multicentre, Single-Arm, Phase 2 Study. Lancet Oncol (2018) 19:1094–106. doi: 10.1016/S1470-2045(18)30321-8
8. Kim S, Meurisse A, Spehner L, Stouvenot M, François E, Buecher B, et al. Pooled Analysis of 115 Patients From Updated Data of Epitopes-HPV01 and Epitopes-HPV02 Studies in First-Line Advanced Anal Squamous Cell Carcinoma. Ther Adv Med Oncol (2020) 12:1758835920975356. doi: 10.1177/1758835920975356
9. Wong SBJ, Bos R, Sherman LA. Tumor-Specific CD4+ T Cells Render the Tumor Environment Permissive for Infiltration by Low-Avidity CD8+ T Cells. J Immunol (2008) 180:3122–31. doi: 10.4049/jimmunol.180.5.3122
10. Ahrends T, Spanjaard A, Pilzecker B, Bąbała N, Bovens A, Xiao Y, et al. CD4+ T Cell Help Confers a Cytotoxic T Cell Effector Program Including Coinhibitory Receptor Downregulation and Increased Tissue Invasiveness. Immunity (2017) 47:848–861.e5. doi: 10.1016/j.immuni.2017.10.009
11. Spehner L, Boustani J, Cabel L, Doyen J, Vienot A, Borg C, et al. Present and Future Research on Anal Squamous Cell Carcinoma. Cancers (Basel) (2021) 13(15):3895. doi: 10.3390/cancers13153895
12. Godet Y, Fabre E, Dosset M, Lamuraglia M, Levionnois E, Ravel P, et al. Analysis of Spontaneous Tumor-Specific CD4 T-Cell Immunity in Lung Cancer Using Promiscuous HLA-DR Telomerase-Derived Epitopes: Potential Synergistic Effect With Chemotherapy Response. Clin Cancer Res (2012) 18:2943–53. doi: 10.1158/1078-0432.CCR-11-3185
13. Lyford-Pike S, Peng S, Young GD, Taube JM, Westra WH, Akpeng B, et al. Evidence for a Role of the PD-1:PD-L1 Pathway in Immune Resistance of HPV-Associated Head and Neck Squamous Cell Carcinoma. Cancer Res (2013) 73:1733–41. doi: 10.1158/0008-5472.CAN-12-2384
14. Badoual C, Hans S, Merillon N, Van Ryswick C, Ravel P, Benhamouda N, et al. PD-1-Expressing Tumor-Infiltrating T Cells Are a Favorable Prognostic Biomarker in HPV-Associated Head and Neck Cancer. Cancer Res (2013) 73:128–38. doi: 10.1158/0008-5472.CAN-12-2606
15. Oliveira-Costa JP, de Carvalho AF, da Silveira GG, Amaya P, Wu Y, Park K-JJ, et al. Gene Expression Patterns Through Oral Squamous Cell Carcinoma Development: PD-L1 Expression in Primary Tumor and Circulating Tumor Cells. Oncotarget (2015) 6:20902–20. doi: 10.18632/oncotarget.3939
16. Peng S, Tan M, Li Y-D, Cheng MA, Farmer E, Ferrall L, et al. PD-1 Blockade Synergizes With Intratumoral Vaccination of a Therapeutic HPV Protein Vaccine and Elicits Regression of Tumor in a Preclinical Model. Cancer Immunol Immunother (2021) 70:1049–62. doi: 10.1007/s00262-020-02754-x
17. Morris VK, Salem ME, Nimeiri H, Iqbal S, Singh P, Ciombor K, et al. Nivolumab for Previously Treated Unresectable Metastatic Anal Cancer (NCI9673): A Multicentre, Single-Arm, Phase 2 Study. Lancet Oncol (2017) 18:446–53. doi: 10.1016/S1470-2045(17)30104-3
18. Ott PA, Piha-Paul SA, Munster P, Pishvaian MJ, van Brummelen EMJ, Cohen RB, et al. Safety and Antitumor Activity of the Anti-PD-1 Antibody Pembrolizumab in Patients With Recurrent Carcinoma of the Anal Canal. Ann Oncol (2017) 28:1036–41. doi: 10.1093/annonc/mdx029
19. Marabelle A, Cassier PA, Fakih M, Kao SC-H, Nielsen D, Italiano A, et al. Pembrolizumab for Previously Treated Advanced Anal Squamous Cell Carcinoma: Pooled Results From the KEYNOTE-028 and KEYNOTE-158 Studies. JCO (2020) 38:4020–0. doi: 10.1200/JCO.2020.38.15_suppl.4020
20. Rao S, Capdevila J, Gilbert D, Kim S, Dahan L, Kayyal T, et al. LBA42 POD1UM-202: Phase II Study of Retifanlimab in Patients (Pts) With Squamous Carcinoma of the Anal Canal (SCAC) Who Progressed Following Platinum-Based Chemotherapy. Ann Oncol (2020) 31:S1170–1. doi: 10.1016/j.annonc.2020.08.2272
21. Lonardi S, Prete AA, Morano F, Messina M, Formica V, Corsi DC, et al. Randomized Phase II Trial of Avelumab Alone or in Combination With Cetuximab for Patients With Previously Treated, Locally Advanced, or Metastatic Squamous Cell Anal Carcinoma: The CARACAS Study. J Immunother Cancer (2021) 9(11):e002996. doi: 10.1136/jitc-2021-002996
22. Frenel J-S, Le Tourneau C, O’Neil B, Ott PA, Piha-Paul SA, Gomez-Roca C, et al. Safety and Efficacy of Pembrolizumab in Advanced, Programmed Death Ligand 1–Positive Cervical Cancer: Results From the Phase Ib KEYNOTE-028 Trial. JCO (2017) 35:4035–41. doi: 10.1200/JCO.2017.74.5471
23. Chung HC, Ros W, Delord J-P, Perets R, Italiano A, Shapira-Frommer R, et al. Efficacy and Safety of Pembrolizumab in Previously Treated Advanced Cervical Cancer: Results From the Phase II KEYNOTE-158 Study. JCO (2019) 37:1470–8. doi: 10.1200/JCO.18.01265
24. Mehra R, Seiwert TY, Gupta S, Weiss J, Gluck I, Eder JP, et al. Efficacy and Safety of Pembrolizumab in Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma: Pooled Analyses After Long-Term Follow-Up in KEYNOTE-012. Br J Cancer (2018) 119:153–9. doi: 10.1038/s41416-018-0131-9
25. Rosenberg SA, Restifo NP. Adoptive Cell Transfer as Personalized Immunotherapy for Human Cancer. Science (2015) 348:62–8. doi: 10.1126/science.aaa4967
26. Lonardi S, Pietrantonio F, Prete AA, Messina M, Formica V, Corsi DC, et al. 402mo Final Results of the CARACAS Study: Randomized Phase II Trial of Avelumab Alone or With Cetuximab for Unresectable, Locally Advanced or Metastatic Squamous Cell Anal Carcinoma Progressed to at Least One Line of Treatment. Ann Oncol (2020) 31:S412. doi: 10.1016/j.annonc.2020.08.513
Keywords: HPV-related cancer, anal carcinoma, head and neck, cervix, atezolizumab, immunotherapy, vaccine
Citation: Rebucci-Peixoto M, Vienot A, Adotevi O, Jacquin M, Ghiringhelli F, de la Fouchardière C, You B, Maurina T, Kalbacher E, Bazan F, Meynard G, Clairet A-L, Fagnoni-Legat C, Spehner L, Bouard A, Vernerey D, Meurisse A, Kim S, Borg C and Mansi L (2022) A Phase II Study Evaluating the Interest to Combine UCPVax, a Telomerase CD4 TH1-Inducer Cancer Vaccine, and Atezolizumab for the Treatment of HPV Positive Cancers: VolATIL Study. Front. Oncol. 12:957580. doi: 10.3389/fonc.2022.957580
Received: 31 May 2022; Accepted: 23 June 2022;
Published: 19 July 2022.
Edited by:
Oliver Kepp, U1138 Centre de Recherche des Cordeliers (CRC)(INSERM), FranceReviewed by:
Lucillia Bezu, Gustave Roussy Cancer Campus, FranceCopyright © 2022 Rebucci-Peixoto, Vienot, Adotevi, Jacquin, Ghiringhelli, de la Fouchardière, You, Maurina, Kalbacher, Bazan, Meynard, Clairet, Fagnoni-Legat, Spehner, Bouard, Vernerey, Meurisse, Kim, Borg and Mansi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Magali Rebucci-Peixoto, bXJlYnVjY2lAY2h1LWJlc2FuY29uLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.