
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol. , 12 August 2022
Sec. Thoracic Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.952393
This article is part of the Research Topic Optimizing Outcomes and Addressing Adversities of Immunotherapy in Lung Cancer View all 17 articles
 Natsuki Nakagawa
Natsuki Nakagawa Masanori Kawakami*
Masanori Kawakami*The treatment landscape of advanced non-small cell lung cancer (NSCLC) has changed dramatically since the emergence of immune checkpoint inhibitors (ICIs). Although some patients achieve long survival with relatively mild toxicities, not all patients experience such benefits from ICI treatment. There are several ways to use ICIs in NSCLC patients, including monotherapy, combination immunotherapy, and combination chemoimmunotherapy. Decision-making in the selection of an ICI treatment regimen for NSCLC is complicated partly because of the absence of head-to-head prospective comparisons. Programmed death-ligand 1 (PD-L1) expression is currently considered a standard biomarker for predicting the efficacy of ICIs, although some limitations exist. In addition to the PD-L1 tumor proportion score, many other clinical factors should also be considered to determine the optimal treatment strategy for each patient, including age, performance status, histological subtypes, comorbidities, status of oncogenic driver mutation, and metastatic sites. Nevertheless, evidence of the efficacy and safety of ICIs with some specific conditions of these factors is insufficient. Indeed, patients with poor performance status, oncogenic driver mutations, or interstitial lung disease have frequently been set as ineligible in randomized clinical trials of NSCLC. ICI use in these patients is controversial and remains to be discussed. It is important to select patients for whom ICIs can benefit the most from these populations. In this article, we review previous reports of clinical trials or experience in using ICIs in NSCLC, focusing on several clinical factors that are associated with treatment outcomes, and then discuss the optimal ICI treatment strategies for NSCLC.
In the last 10 years, immune-checkpoint inhibitors (ICIs) have changed treatment strategies for non-small cell lung cancer (NSCLC). The benefit of ICIs over previous standard therapy (cytotoxic chemotherapy) has been demonstrated both as monotherapy and as combination therapy, regardless of previous treatment history (1–7). Response duration of ICIs tends to be longer than cytotoxic chemotherapy (1, 2, 5, 6). Survival duration of some patients with advanced NSCLC treated with ICI exceeded 3 years and notably, the 5-years follow-up form KEYNOTE-024 shows an OS rate of 32% (6, 8–13). In clinical trials, the 2-year survival rate of advanced NSCLC patients is 37%–45% when treated with combination therapy of ICI and chemotherapy as the first-line treatment and 23%–29% with ICI monotherapy for previously treated patients, while 18%–29% in treatment-naive patients and 8%–16% in previously-treated patients when treated with chemotherapy (14–16). Despite of these improved treatment outcomes by ICIs in clinical trials, there are still issues to be addressed in daily clinical practice. First, it is difficult to determine which treatment regimen is most suitable for individual cases. Many treatment regimens are available for patients with advanced NSCLC. Most patients with NSCLC experience disease progression as a result of primary or acquired resistance to ICIs (17, 18). In this review, we discuss the clinical factors that could influence the efficacy and safety of drugs including ICIs. Second, many patients in clinical practice do not fulfil the eligibility criteria for clinical trials (19–23). For example, aged patients or patients with poor performance status (PS) are usually considered ineligible for prospective clinical trials. Generally, because of their poor condition, it is difficult to treat these patients with cytotoxic chemotherapy, and their prognosis is worse than that of patients who fulfill the eligibility criteria of clinical trials. ICIs have different toxicity profiles than standard chemotherapy, and their cytotoxicity is usually mild. Therefore, ICIs may be a good treatment option for patients who do not meet the criteria for chemotherapy. It is important to select patients for whom ICIs can benefit the most from this population. In this review, we will summarize previous clinical studies of ICIs used for NSCLC, and then discuss the optimal ICI treatment strategies, focusing on the clinical factors that potentially predict ICI effects.
Many studies on ICIs have been conducted in patients with advanced or recurrent NSCLC. Table 1 shows the major clinical trials that tested ICI regimens for treatment-naïve patients in which the primary endpoints were positive and negative, respectively. Tables 1A, C are for squamous NSCLC (Sq-NSCLC), while Tables 1B, D represent non-squamous NSCLC (NSq-NSCLC). The efficacy results were almost the same between Sq and non-Sq patients, except for the KEYNOTE-024 study. It should be noted that the results of KEYNOTE-024, KEYNOTE-042, IMPOWER-110, and KEYNOTE-598 includes both squamous and non-squamous NSCLC patients.
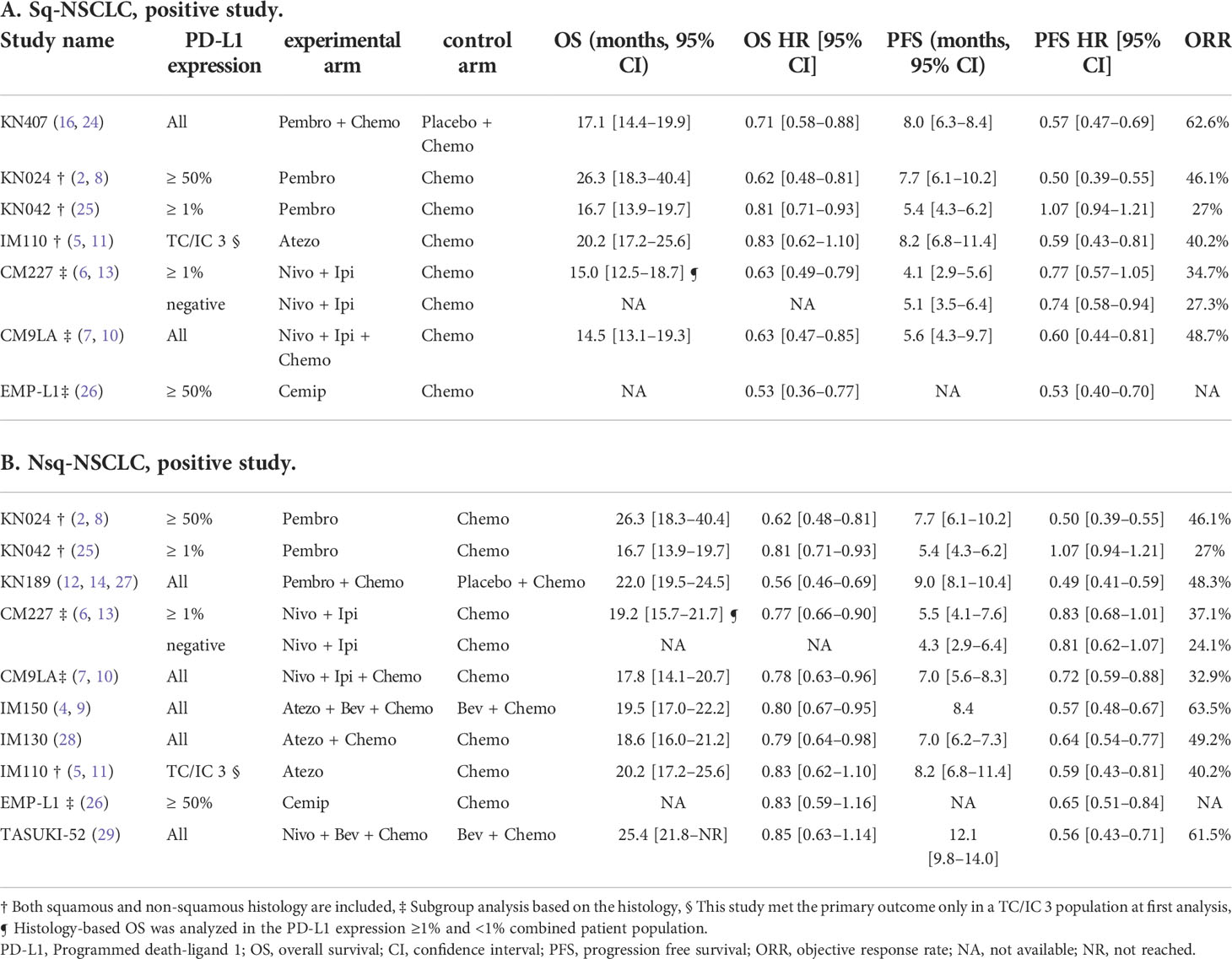
Table 1 Key clinical trials that tested ICI regimens for treatment-naïve patient.
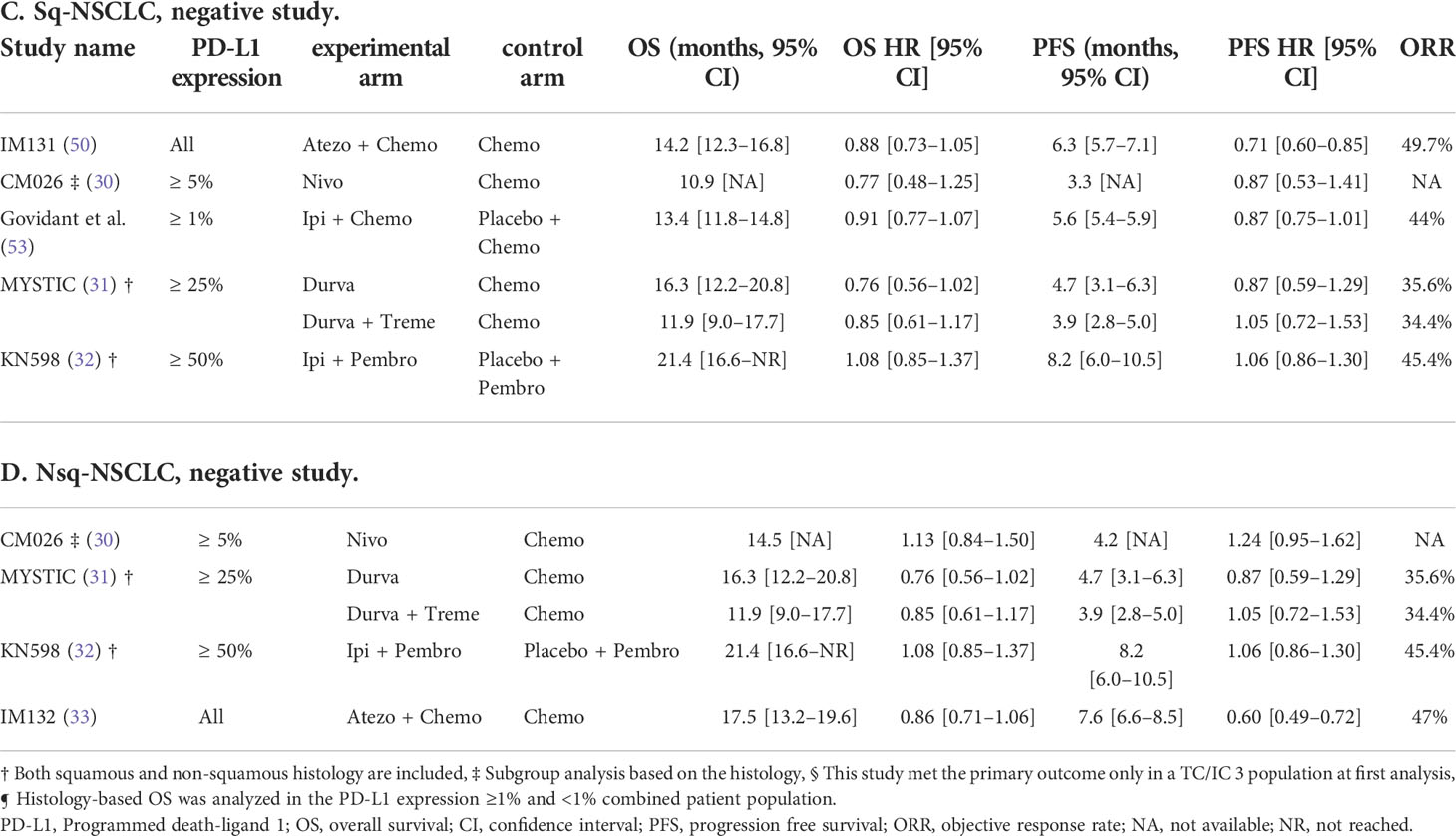
Table 1 Key clinical trials that tested ICI regimens for treatment-naïve patient.
PD-L1 tumor proportion score (TPS) is widely used to predict ICI effects. In the phase 2 KEYNOTE-001 trial, the objective response rates (ORR) of pembrolizumab for pre-treated NCSLC patients were 45%, 17%, and 11% in the subgroup with PD-L1 TPS score, assessed by the PD-L1 IHC 22C3 pharmDx, with ≥50%, 1%–49%, and <1%, respectively (34). Furthermore, the survival benefit of pembrolizumab was also associated with a high PD-L1 TPS. The superiority of pembrolizumab monotherapy over chemotherapy for treatment-naïve NSCLC patients was observed in both the PD-L1 TPS ≥ 50% and ≥1% groups in KEYNOTE-024 and 042 (2, 25). Subgroup analysis of these studies showed the association of higher PD-L1 TPS with better efficacy of pembrolizumab. This association was confirmed in real-world settings when limited to PD-L1 TPS ≥ 50% (35–37). These data support the notion that PD-L1 TPS assessed by 22C3 assay predicts the outcome of pembrolizumab monotherapy used in the first-line setting. Similar trends have been observed in clinical trials for other cancers (38–40).
The association between PD-L1 TPS and ICI effects was inconsistent when different methods were used to evaluate the TPS. In the Impower110 trial, the efficacy of atezolizumab monotherapy used as a first-line treatment in NSCLC patients was correlated with PD-L1 TPS assessed by SP142 assay, and superiority of atezolizumab over platinum-based chemotherapy was observed in the subgroup with PD-L1 TPS ≥ 50% (5). However, in the CheckMate 026 trial where nivolumab efficacy was tested, no superiority of nivolumab over platinum-based chemotherapy was seen either in the pre-planned group with PD-L1 TPS ≥ 5% or in the exploratory subgroup with PD-L1 TPS ≥ 50% (30). In this study, the PD-L1 TPS was assessed using the 28-8 antibody. This inconsistency among the studies may be attributed from the fact that the assessment assay used to evaluate PD-L1 expression differed in each clinical trial. On the other hand, Impower 110 trial compared PD-L1 scoring methods, SP142, 22C3 and SP263, as an exploratory analysis. Of note, median OS among patients with high PD-L1 TPS assessed by these three assays were similar. In clinical trials, PD-L1 assays often differ among different ICI drugs. Few information is available concerning analysis of the concordance among different PD-L1 assays (41).
In addition to the methods for TPS evaluation, the cut-off levels of PD-L1 expression are not fixed, and they sometimes change even in the middle of ongoing clinical trials (42–44). Another factor that may lead to these inconsistent results is heterogeneity of PD-L1 expression. The spatial and temporal heterogeneity of PD-L1 expression in the same tumor has been previously reported (45–49). PD-L1 expression tends to be high in primary sites, adrenal glands, liver, and lymph nodes, but low in the bone and brain (45, 46). When PD-L1 TPS of lymph node metastatic site was assessed, the association with ICI efficacy was not observed (45). In the clinical trials discussed above, the number of biopsy sites where PD-L1 TPS was evaluated varied among cases.
Inconsistency in the predictive value of PD-L1 expression among clinical trials was also observed in the setting of combination chemoimmunotherapy. PD-L1 expression was positively correlated with progression-free survival (PFS) in the combination of pembrolizumab with platinum plus pemetrexed for NSq-NSCLC; atezolizumab with carboplatin, paclitaxel, and bevacizumab for NSq-NSCLC; and atezolizumab with carboplatin plus nab-paclitaxel for Sq-NSCLC (4, 27, 50). However, this correlation was not proven in the atezolizumab with carboplatin plus nab-paclitaxel combination for NSq-NSCLC and pembrolizumab with carboplatin plus either paclitaxel or nab-paclitaxel for Sq-NSCLC (24, 28). The aforementioned ICIs are inhibitors of the PD-1/PD-L1 checkpoint pathway. In contrast, ipilimumab is a monoclonal antibody for cytotoxic T-lymphocyte associated protein 4 (CTLA-4), which is independent of the PD-1/PD-L1 pathway. It is reasonable that this agent can be effective even in PD-L1-negative population (6, 13). In fact, in the CheckMate 9LA trial, where the combination of nivolumab and ipilimumab with chemotherapy was studied, favorable outcomes were observed regardless of PD-L1 expression for both NSq-NSCLC and Sq-NSCLC (7, 10). This trend is consistent with previous clinical trials involving patients with melanoma and renal-cell carcinoma (51, 52). However, when nivolumab and ipilimumab are used without chemotherapy for patients with NSCLC, median overall survival (OS) was numerically greater in higher PD-L1 expression population in the CheckMate 227 trial (13). Considering the negative result of the KEYNOTE-598 study, where pembrolizumab plus ipilimumab for metastatic NSCLC with PD-L1 TPS ≥ 50% was tested (Tables 1C, D), the benefit of adding ipilimumab to an anti PD-1 antibody for patients with PD-L1 TPS ≥ 50% should be discussed carefully (32).
Overall, although the results are inconsistent, PD-L1 expression can be used as a predictive biomarker for ICI effects. Recently, a combined positive score has emerged as a new method instead of PD-L1 TPS to evaluate PD-L1 expression (54). A combined positive score is calculated as the proportion of tumor cells, lymphocytes, and macrophages that were positively stained by PD-L1 immunohistochemical staining of total tumor cells. The KEYNOTE-048 trial of pembrolizumab treatment for head and neck cancer demonstrated a positive association of favorable survival with PD-L1 expression level assessed by the combined positive score (43).
A correlation between driver mutation subtypes and ICI efficacy has been reported. The ImmunoTarget group retrospectively compared ORR after ICI treatment among NSCLC patients with various driver mutations. It was revealed that the KRAS-driven and BRAF-driven subgroups appreciated a greater benefit from ICI than EGFR-driven or ALK-driven subgroups (55).
Several clinical trials have suggested favorable efficacy of ICIs in NSCLC patients with KRAS mutations (1, 56–60). When pembrolizumab was used as monotherapy in NSq-NSCLC patients with PD-L1 TPS ≥ 50%, KRAS mutation was associated with longer OS, while this association was not observed when pembrolizumab was used as combined chemoimmunotherapy (61, 62). Notably, co-mutation of SKT11/LKB11 with KRAS mutation, which exists in approximately 30% of KRAS-mutated NSCLC, is associated with an unfavorable efficacy of ICIs (63, 64). This mutation was associated with lower PD-L1 expression and fewer tumoricidal immune infiltrates.
Many recent clinical trials of ICIs have excluded those with actionable driver mutations, such as EGFR mutations and ALK fusions. The decision for this exclusion is probably based on the results of a subgroup analysis in large randomized controlled trials conducted in the early days of the ICI era, such as CheckMate 017, CheckMate 057, KEYNOTE-010, and OAK, which compared ICIs and docetaxel for their efficacy and safety as second-line therapy in advanced NSCLC (1, 56, 65, 66). The meta-analysis of these trials demonstrated that the integrated OS hazard ratio of ICIs compared to docetaxel was 1.05 [95% confidence interval [CI]: 0.70–1.55] in the EGFR-mutant subgroup and 0.66 [95% CI: 0.58–0.76] in the EGFR wild-type subgroup (59, 60, 67). Retrospective studies have also shown generally low efficacy of ICIs in driver mutation-positive NSCLC (55, 68, 69). In addition, a recently published phase 2 study comparing nivolumab and carboplatin-pemetrexed for EGFR-mutated NSCLC with resistance to EGFR-tyrosine kinase inhibitors (TKI) revealed significantly worse survival in patients treated with nivolumab (70). Poor efficacy of ICIs for NSCLC patients with EGFR mutations is thought to be derived from a lower tumor mutation burden and an immunosuppressive tumor microenvironment (71, 72).
However, some prospective studies have shown comparable or superior efficacy of ICIs in NSCLC patients with driver mutations (73–77). An exploratory subgroup analysis of the IMpower150 trial demonstrated that in NSq-NSCLC patients with sensitizing EGFR mutations, OS of atezolizumab, carboplatin, paclitaxel, and bevacizumab combination group was longer than carboplatin, paclitaxel, and bevacizumab combination group. (median OS was26.1 months [95% CI 17.0–41.4] in the atezolizumab arm vs. 20.3 months [95% CI 13.4–33.6] in the control arm; hazard ratio [HR] 0.91 [95% CI 0.53–1.59]) (73, 74). Based on these results, two prospective studies are ongoing in Japan to verify the efficacy and safety of combination chemoimmunotherapy with atezolizumab, carboplatin, paclitaxel, and bevacizumab in EGFR-mutant NSCLC patients who were already treated with an EGFR-TKI (78, 79).
Usually, molecular-targeted therapies are more effective than ICIs or cytotoxic agents for NSCLC patients with actionable driver mutations (78–88). Combination therapy with TKIs and ICIs has failed due to severe adverse events (89–91). Based on the idea of “best drug first,” there is no doubt that the first-line therapies for NSCLC patients with actionable driver mutations are TKIs (92–94). However, to the best of our knowledge, there is no clear conclusion as to whether ICIs can be a treatment option for these patients at any late treatment line. Some retrospective studies have suggested that PD-L1 expression predicts ICI efficacy, even in EGFR-mutant NSCLC (95). Furthermore, interestingly, PD-L1 expression was upregulated after EGFR-TKI therapy via ERK1/2 pathway modulation (47, 48). It has also been reported that EGFR mutations can upregulate PD-L1 expression through the Ras/RAF/MEK/ERK, PI3K/AKT/mTOR, JAK/STAT, NF-kB, and YAP pathways (96–99). Further studies are warranted to clarify the association of driver mutations with PD-L1 expression or ICI efficacies.
Liver metastases have been validated as negative prognostic factors for NSCLC patients (100, 101). More metastases in the liver are correlated with worse survival (102). In addition, the presence of liver metastases predicts poor outcomes after ICI monotherapy (3, 36, 72, 103–106). One possible underlying mechanism is systemic immune tolerance which is mediated by a number of specialized antigen-presenting cells, including dendritic cells, Kupffer cells, liver sinusoidal endothelial cells, and hepatic stellate cells (102, 105, 107–110). From the viewpoint of PD-L1 spatial heterogeneity, PD-L1 expression was relatively higher in liver than other organs in NSCLC patients (45). Conversely, the presence of liver metastases was associated with a lower CD8+ T-cell count at the invasive tumor margin among patients with NSCLC and melanoma who received pembrolizumab (105). This suggests systemic activation of the regulatory immune microenvironment in patients with liver metastases, which results in a poor response to ICI treatments in the presence of liver metastases despite the relatively higher PD-L1 expression.
Currently, there is no consensus regarding the optimal treatment for NSCLC with liver metastases. Although cytotoxic agents and ICIs elicit relatively little efficacy in NSCLC with liver metastases when used alone, one retrospective study showed that combination chemotherapy may be effective (111). Some clinical trials have also suggested that the addition of bevacizumab to ICI treatment is effective for patients with NSCLC with liver metastases (29, 73, 112). Bevacizumab is an anti-vascular endothelial growth factor (VEGF) antibody. Preclinical and clinical data have demonstrated that bevacizumab normalizes vasculature, restores dendritic cell maturation, and reduces T-regulatory cells and myeloid-derived suppressor cells in cancer patients (113–117). Considering these pharmacological effects, treatment regimen containing bevacizumab may be reasonable for patients of NSCLC with liver metastases, where immunosuppressive microenvironment is an issue for ICI treatments as discussed above.
The presence of liver metastases is thought to be associated with the onset of hyperprogressive disease (HPD) (118–120). HPD is characterized by rapid disease progression after initiation of ICIs, often defined as a > 50% increase in tumor size within less than 2 months after initiation of ICIs, although currently there is no widely accepted definition (118, 121). HPD is associated with worse clinical outcomes (118). Other than liver metastases, high LDH levels, low Albumin levels, multiple metastatic sites, poor PS, and a Royal Marsden Hospital prognostic score of ≥ 2 were associated with the risk of HPD occurrence (118, 120). However, underlying mechanisms of HPD are not understood well. Treatment strategies for NSCLC patients at high risk of HPD have not yet been established.
Radiation therapy is the most important treatment strategy that should be considered first for NSCLC patients with brain metastases (BMs), especially when clinical symptoms derived from BMs are present (122). Thus the role of ICIs, with or without cytotoxic agents, can be discussed only for the regulation of BMs that are asymptomatic or already treated with radiation. The efficacy of ICI in patients with leptomeningeal disease requires further investigation (123).
The survival benefit of ICIs is similar regardless of the presence or absence of BMs based on a subgroup analysis of clinical trials of ICIs with or without cytotoxic agents, as listed in Table 1 (6, 10, 12, 26, 29, 124, 125). A meta-analysis of 10 clinical trials with ICIs in NSCLC showed an OS HR of 1.25 (95% CI = 1.09–1.44, I2 = 43.8%, P <.001) for BMs compared with those without BMs (104). A retrospective study showed that the presence of BMs and a larger maximum diameter of brain metastases were associated with worse prognosis of NSCLC patients after ICI monotherapy in the second or later treatment line (126). To our knowledge, there are few available data regarding intracranial response rates to ICIs in NSCLC patients. Phase 2 studies on melanoma demonstrated that combination therapy with nivolumab and ipilimumab achieved higher intracranial response rates than treatment with nivolumab alone (127). Considering these data, patients with BMs can be treated in the same way as those without BMs, but combination immunotherapy with anti-PD-1 and anti-CTLA-4 agents, with or without cytotoxic agents, may provide better outcomes (124, 128, 129).
Previous studies have reported that malignant pleural effusion is present in 11%–32% of patients with advanced NSCLC (130–132). Even a small amount of pleural effusion (< 10-mm thick on chest computed tomography) is an independent predictor of worse survival (130). This tendency was also observed in cases treated with ICIs, although the available data are limited to retrospective studies. The presence of malignant pleural effusion was associated with worse prognosis in NSCLC patients treated with a single ICI in either first-line or later treatment lines (126, 133–135). Recently reported retrospective study suggests that combination chemoimmunotherapy is more effective than pembrolizumab monotherapy as a first line treatment for NSCLC patients with malignant pleural effusion (136). As observed in liver metastases, malignant pleural effusion induces systemic immunosuppressive microenvironment through several mediators and pathways, including myeloid derived suppressor cells, neutrophils, macrophages, T-regulatory cells, and dysfunctional T cells that might result in low efficacy of ICIs (126, 137). As for safety, existence of pleural effusion before treatment with nivolumab was indicative of poor outcomes of interstitial lung disease (ILD) induced as an immune-related adverse event (irAE) when it occurs (138).
In the setting of combination chemoimmunotherapy, we could not find any studies to assess the effects of the presence of malignant pleural effusion on the efficacy of therapy or to evaluate which combination of drugs is better for use in cases with malignant pleural effusion. VEGF is thought to be one of the key factors that cause malignant plural effusion by increasing vascular and mesothelial permeability and capillary fluid leakage (139). In fact, several studies suggest the efficacy of bevacizumab for the management of malignant pleural effusion in Nsq-NSCLC (117, 140–144). VEGF also plays a principal role in immunosuppressive microenvironment as mentioned in the previous section (113–117). Therefore, the combination of bevacizumab and ICI is potentially a good treatment strategy for patients with malignant pleural effusion, although there is few evidence to support this, thus far.
An FDA meta-analysis of four randomized control trials in which ICI monotherapy and docetaxel were compared for patients with disease progression after platinum doublet treatment demonstrated similar survival benefits between these regimens, regardless of age (145). Another meta-analysis of clinical trials for other tumor types also showed a comparable efficacy of ICI monotherapy between patients aged ≥ 65 and < 65 years (19, 146). Furthermore, real-world data supported the evidence for efficacy and safety of ICI monotherapy for the elderly NSCLC patients (147–150). These data suggested that it is the PS or comorbidities rather than age that is associated with the outcome of ICI treatment in the elderly patients (19, 147, 148). It should be noted that the cutoff value for defining elderly varies among studies.
In combination chemoimmunotherapy, more attention should be paid to elderly patients. In the KEYNOTE-189 trials, in which treatment-naïve NSCLC patients were treated with a platinum agent and pemetrexed with or without pembrolizumab, the addition of pembrolizumab was associated with worse survival benefit in the elderly, which was defined as ≥ 75 years old (151). A retrospective study showed a similar result, that is, poor outcome of combination chemoimmunotherapy in the elderly group (152). In general, organ function declines with age, but it is difficult to evaluate these functions sufficiently with clinical examinations that are currently available. Clinical assessment tools for the elderly, such as the comprehensive geriatric assessment and Charlson comorbidity index, have been tested to predict the prognosis of anti-cancer therapy in many clinical trials, but their usefulness has not yet been established (153–157). Currently, there are no clinical assessment tools available to predict which elderly patients can tolerate chemoimmunotherapy well.
In the ECOG 1594 study, which revealed almost similar efficacy and safety profiles among four platinum doublet regimens, a subgroup analysis showed that adverse events increased, and prognosis worsened in patients with a PS of 2 compared to those with a PS of 0 or 1 (158, 159). Historically, this is a pivotal study. Thereafter, for more than 10 years, cytotoxic agent monotherapies have been standard therapies for patients with a PS of 2. On the other hand, the advantage of ICIs is their favorable toxicity profiles. Therefore, ICIs may be an alternative treatment option for this population. Many studies have suggested that PS is not associated with the frequency or severity of irAEs (39, 150, 160–162). For example, in CheckMate 153, a prospective study validating the safety of second-line treatment with nivolumab for NSCLC patients aged ≥ 70 years and with a PS of 2, the incidence rates of grades 3–5 and any grade adverse events were not increased in the population with a PS of 2 (9% and 29%, respectively) compared to the overall population, including a PS of 0–2 (6% and 37%, respectively), and toxicity profiles were comparable between these populations (150). The toxicities of ICIs seem to be acceptable for patients with poor PS.
Regarding prognosis, in both prospective and retrospective studies of ICI monotherapy for NSCLC, patients with a PS ≥ 2 who were treated with ICI monotherapy showed poor survival (150, 161–165). The hazard ratio of PFS ranged from 2.00 to 2.39 and OS ranged from 2.72 to 2.82 in patients with a PS ≥ 2 compared with a PS of 0 or 1. Studies on ICI monotherapy in a relatively large number of patients with a PS ≥ 2 are summarized in Table 2. Unlike PFS and OS, ORR results were inconsistent among the studies. As shown in Table 2, some studies have shown that the ORR of patients with a PS 2 was comparable to that of patients with a PS 0–1 after ICI monotherapy (162, 165). Poor PS of NSCLC patients may result from many different reasons, such as cancer burden, cancer progression rate, comorbidities unrelated to cancer, or a combination of these factors. The analysis of ICI efficacy in patients with a PS 2 based on the reasons for poor PS may help us better understand who is suitable for ICI treatment in this population.
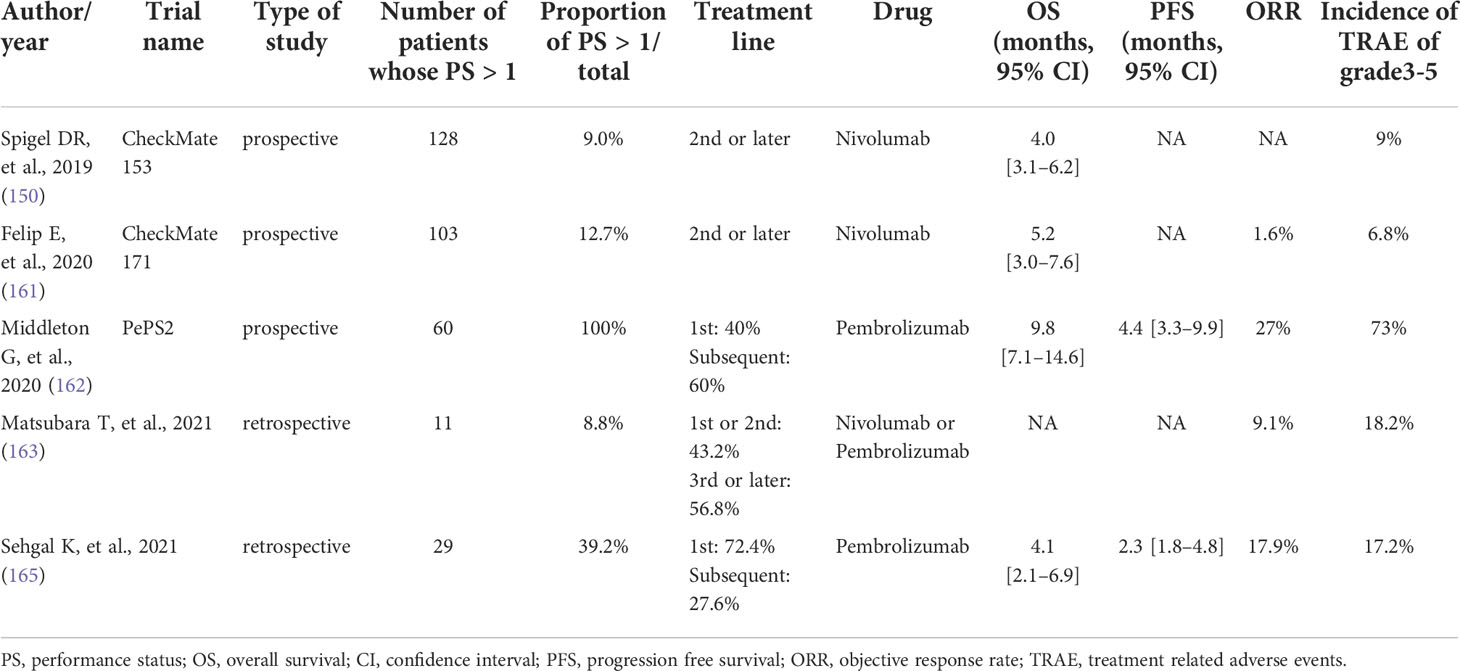
Table 2 ICI for PS2.
Patients with ILD have been excluded from most randomized controlled trials in which ICIs are involved. However, in the real world, ILD is seen frequently (at a rate of 14%) in treatment-naïve patients with NSCLC (166). ILD is an independent risk factor for drug-induced lung injuries, including ICI-related injuries and is associated with poor survival in NSCLC patients treated with ICIs (167–169). Drug-induced lung injuries caused by ICIs are the most common irAE that lead to the discontinuation of ICIs and are associated with worse survival (65, 66, 170). ILD includes a very wide spectrum, and its radiological classification is complex. Radiological assessments of ILD are different, even among radiologists (171, 172). This makes it difficult to stratify the degree of risks of pre-existing ILD for ICI-induced lung toxicities.
Several clinical trials have assessed the efficacy and safety of ICIs in patients with ILD. The AMBITIOUS trial is a prospective study of atezolizumab in NSCLC patients with idiopathic, chronic fibrotic interstitial pneumonia whose %VC was 70% or larger. This study was discontinued early because of the high incidence of pneumonitis (29.4%) (173). In this study, pre-existing honeycomb lung was associated with a high risk of frequency and severity of pneumonitis (57.1% of patients with pre-existing honeycomb lung suffered from drug-induced pneumonitis with a grade greater than or equal to 3). The honeycomb lung has also been reported to be associated with cytotoxic chemotherapy-related exacerbation of ILD (174). Another prospective study to evaluate the efficacy and safety of nivolumab in NSCLC patients with mild idiopathic interstitial pneumonia demonstrated favorable efficacy and a tolerable safety profile, where two out of 18 patients developed grade 2 pneumonitis (175). In this study, patients with mild idiopathic, classified as radiological possible or inconsistent with usual interstitial pneumonia (UIP), were included only when their %VC was 80% or more. Therefore, patients with radiological UIP patterns were excluded. These studies imply that the presence or absence of a honeycomb lung is the principal factor in predicting the safety of ICI treatment.
ILD related to ICIs may occur even in patients without ILD at the initiation of ICI therapy. Several risk factors for the onset and severity of ICI-induced lung toxicities have been suggested, including the primary tumor site of the lung, ICI combination therapy rather than ICI monotherapy, PD-1 inhibitors compared with PD-L1 inhibitors or CTLA-4 inhibitors, and the presence of pleural effusion before treatment (137, 176–179).
ICIs are now indispensable agents for NSCLC treatment and contribute to the extension of survival in NSCLC patients. Considering their relatively mild toxicities, ICIs could provide an opportunity of treatment for patients who cannot tolerate treatment with cytotoxic agents, such as elderly or patients with poor PS. As discussed in this paper, many clinical factors may affect the efficacy and safety of ICI treatment. PD-L1 is currently considered a predictive biomarker of ICI treatment, but clinicians should keep in mind that this is not a perfect biomarker as mentioned above. Emerging biomarkers, including tumor mutational burden, neoantigen load, tumor-infiltrating lymphocytes, immune-regulatory mRNA expression and blood biomarkers, are reported as possibly predictive (180). Further studies are warranted in this area.
This review was drafted by NN and critically revised by MK. All authors contributed to the article and approved the submitted version.
This work was supported by JSPS KAKENHI Grant Number 21H02776.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Herbst RS, Baas P, Kim DW, Felip E, Pérez-Gracia JL, Han JY, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet (2016) 387:1540–50. doi: 10.1016/S0140-6736(15)01281-7
2. Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus chemotherapy for PD-L1-Positive non-Small-Cell lung cancer. N Engl J Med (2016) 375:1823–33. doi: 10.1056/NEJMoa1606774
3. Vokes EE, Ready N, Felip E, Horn L, Burgio MA, Antonia SJ, et al. Nivolumab versus docetaxel in previously treated advanced non-small-cell lung cancer (CheckMate 017 and CheckMate 057): 3-year update and outcomes in patients with liver metastases. Ann Oncol (2018) 29:959–65. doi: 10.1093/annonc/mdy041
4. Socinski MA, Jotte RM, Cappuzzo F, Orlandi F, Stroyakovskiy D, Nogami N, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med (2018) 378:2288–301. doi: 10.1056/NEJMoa1716948
5. Herbst RS, Giaccone G, de Marinis F, Reinmuth N, Vergnenegre A, Barrios CH, et al. Atezolizumab for first-line treatment of PD-L1-Selected patients with NSCLC. N Engl J Med (2020) 383:1328–39. doi: 10.1056/NEJMOA1917346
6. Hellmann MD, Paz-Ares L, Bernabe Caro R, Zurawski B, Kim SW, Carcereny Costa E, et al. Nivolumab plus ipilimumab in advanced non-Small-Cell lung cancer. N Engl J Med (2019) 381:2020–31. doi: 10.1056/NEJMOA1910231
7. Paz-Ares L, Ciuleanu TE, Cobo M, Schenker M, Zurawski B, Menezes J, et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol (2021) 22:198–211. doi: 10.1016/S1470-2045(20)30641-0
8. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-Small-Cell lung cancer with PD-L1 tumor proportion score ≥ 50. J Clin Oncol (2021) 39:2339–49. doi: 10.1200/JCO.21.00174
9. Socinski MA, Nishio M, Jotte RM, Cappuzzo F, Orlandi F, Stroyakovskiy D, et al. IMpower150 final overall survival analyses for atezolizumab plus bevacizumab and chemotherapy in first-line metastatic nonsquamous NSCLC. J Thorac Oncol (2021) 16:1909–24. doi: 10.1016/j.jtho.2021.07.009
10. Reck M, Ciuleanu T-E, Cobo M, Schenker M, Zurawski B, Menezes J, et al. First-line nivolumab plus ipilimumab with two cycles of chemotherapy versus chemotherapy alone (four cycles) in advanced non-small-cell lung cancer: CheckMate 9LA 2-year update. ESMO Open (2021) 6:100273. doi: 10.1016/J.ESMOOP.2021.100273
11. Jassem J, de Marinis F, Giaccone G, Vergnenegre A, Barrios CH, Morise M, et al. Updated overall survival analysis from IMpower110: Atezolizumab versus platinum-based chemotherapy in treatment-naive programmed death-ligand 1–selected NSCLC. J Thorac Oncol (2021) 16:1872–82. doi: 10.1016/j.jtho.2021.06.019
12. Rodríguez-Abreu D, Powell SF, Hochmair MJ, Gadgeel S, Esteban E, Felip E, et al. Pemetrexed plus platinum with or without pembrolizumab in patients with previously untreated metastatic nonsquamous NSCLC: protocol-specified final analysis from KEYNOTE-189. Ann Oncol (2021) 32:881–95. doi: 10.1016/j.annonc.2021.04.008
13. Paz-Ares LG, Ramalingam SS, Ciuleanu TE, Lee JS, Urban L, Caro RB, et al. First-line nivolumab plus ipilimumab in advanced NSCLC: 4-year outcomes from the randomized, open-label, phase 3 CheckMate 227 part 1 trial. J Thorac Oncol (2022) 17:289–308. doi: 10.1016/J.JTHO.2021.09.010
14. Gadgeel S, Rodríguez-Abreu D, Speranza G, Esteban E, Felip E, Dómine M, et al. Updated analysis from KEYNOTE-189: Pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metastatic nonsquamous non-Small-Cell lung cancer. J Clin Oncol (2020) 38:1505–17. doi: 10.1200/JCO.19.03136
15. Horn L, Spigel DR, Vokes EE, Holgado E, Ready N, Steins M, et al. Nivolumab versus docetaxel in previously treated patients with advanced non-small-cell lung cancer: Two-year outcomes from two randomized, open-label, phase III trials (CheckMate 017 and CheckMate 057). J Clin Oncol (2017) 35:3924–33. doi: 10.1200/JCO.2017.74.3062
16. Paz-Ares L, Vicente D, Tafreshi A, Robinson A, Soto Parra H, Mazières J, et al. A randomized, placebo-controlled trial of pembrolizumab plus chemotherapy in patients with metastatic squamous NSCLC: Protocol-specified final analysis of KEYNOTE-407. J Thorac Oncol (2020) 15:1657–69. doi: 10.1016/J.JTHO.2020.06.015
17. Attili I, Tarantino P, Passaro A, Stati V, Curigliano G, de Marinis F. Strategies to overcome resistance to immune checkpoint blockade in lung cancer. Lung Cancer (2021) 154:151–60. doi: 10.1016/j.lungcan.2021.02.035
18. Sharma P, Hu-Lieskovan S, Wargo JA, Ribas A. Primary, adaptive, and acquired resistance to cancer immunotherapy. Cell (2017) 168:707–23. doi: 10.1016/j.cell.2017.01.017
19. Rzeniewicz K, Larkin J, Menzies AM, Turajlic S. Immunotherapy use outside clinical trial populations: never say never? Ann Oncol (2021) 32:866–80. doi: 10.1016/J.ANNONC.2021.03.199
20. Kawachi H, Fujimoto D, Morimoto T, Ito M, Teraoka S, Sato Y, et al. Clinical characteristics and prognosis of patients with advanced non-small-cell lung cancer who are ineligible for clinical trials. Clin Lung Cancer (2018) 19:e721–34. doi: 10.1016/J.CLLC.2018.05.014
21. Baggstrom MQ, Waqar SN, Sezhiyan AK, Gilstrap E, Gao F, Morgensztern D, et al. Barriers to enrollment in non-small cell lung cancer therapeutic clinical trials. J Thorac Oncol (2011) 6:98–102. doi: 10.1097/JTO.0B013E3181FB50D8
22. Al-Baimani K, Jonker H, Zhang T, Goss GD, Laurie SA, Nicholas G, et al. Are clinical trial eligibility criteria an accurate reflection of a real-world population of advanced non-small-cell lung cancer patients? Curr Oncol (2018) 25:e291–7. doi: 10.3747/CO.25.3978
23. Vardy J, Dadasovich R, Beale P, Boyer M, Clarke SJ. Eligibility of patients with advanced non-small cell lung cancer for phase III chemotherapy trials. BMC Cancer (2009) 9:130. doi: 10.1186/1471-2407-9-130
24. Paz-Ares L, Luft A, Vicente D, Tafreshi A, Tafreshi A, Gümüş M, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med (2018) 379:2040–51. doi: 10.1056/NEJMoa1810865
25. Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet (2019) 393:1819–30. doi: 10.1016/S0140-6736(18)32409-7
26. Sezer A, Kilickap S, Gümüş M, Bondarenko I, Özgüroğlu M, Gogishvili M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet (2021) 397:592–604. doi: 10.1016/S0140-6736(21)00228-2
27. Gandhi L, Rodríguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med (2018) 378:2078–92. doi: 10.1056/NEJMoa1801005
28. West H, McCleod M, Hussein M, Morabito A, Rittmeyer A, Conter HJ, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 tria. Lancet Oncol (2019) 20:924–37. doi: 10.1016/S1470-2045(19)30167-6
29. Sugawara S, Lee JS, Kang JH, Kim HR, Inui N, Hida T, et al. Nivolumab with carboplatin, paclitaxel, and bevacizumab for first-line treatment of advanced nonsquamous non-small-cell lung cancer. Ann Oncol (2021) 32:1137–47. doi: 10.1016/J.ANNONC.2021.06.004
30. Carbone DP, Reck M, Paz-Ares L, Creelan B, Horn L, Steins M, et al. First-line nivolumab in stage IV or recurrent non–Small-Cell lung cancer. N Engl J Med (2017) 376:2415–26. doi: 10.1056/nejmoa1613493
31. Rizvi NA, Cho BC, Reinmuth N, Lee KH, Luft A, Ahn MJ, et al. Durvalumab with or without tremelimumab vs standard chemotherapy in first-line treatment of metastatic non-small cell lung cancer: The MYSTIC phase 3 randomized clinical trial. JAMA Oncol (2020) 6:661–74. doi: 10.1001/jamaoncol.2020.0237
32. Boyer M, Şendur MAN, Rodríguez-Abreu D, Park K, Lee DH, Çiçin I, et al. Pembrolizumab plus ipilimumab or placebo for metastatic non–Small-Cell lung cancer with PD-L1 tumor proportion score ≥ 50%: Randomized, double-blind phase III KEYNOTE-598 study. J Clin Oncol (2021) 39:2327–38. doi: 10.1200/jco.20.03579
33. Nishio M, Barlesi F, West H, Ball S, Bordoni R, Cobo M, et al. Atezolizumab plus chemotherapy for first-line treatment of nonsquamous NSCLC: Results from the randomized phase 3 IMpower132 trial. J Thorac Oncol (2021) 16:653–64. doi: 10.1016/j.jtho.2020.11.025
34. Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med (2015) 372:2018–28. doi: 10.1056/NEJMOA1501824
35. Aguilar EJ, Ricciuti B, Gainor JF, Kehl KL, Kravets S, Dahlberg S, et al. Outcomes to first-line pembrolizumab in patients with non-small-cell lung cancer and very high PD-L1 expression. Ann Oncol (2019) 30:1653–9. doi: 10.1093/annonc/mdz288
36. Takeyasu Y, Yoshida T, Shibaki R, Matsumoto Y, Goto Y, Kanda S, et al. Differential efficacy of pembrolizumab according to metastatic sites in patients with PD-L1 strongly positive (TPS ≥ 50%) NSCLC. Clin Lung Cancer (2021) 22:127–33.e3. doi: 10.1016/j.cllc.2020.10.002
37. Tamiya M, Tamiya A, Hosoya K, Taniguchi Y, Yokoyama T, Fukuda Y, et al. Efficacy and safety of pembrolizumab as first-line therapy in advanced non-small cell lung cancer with at least 50% PD-L1 positivity: a multicenter retrospective cohort study (HOPE-001). Invest New Drugs (2019) 37:1266–73. doi: 10.1007/s10637-019-00843-y
38. Zhu AX, Finn RS, Edeline J, Cattan S, Ogasawara S, Palmer D, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol (2018) 19:940–52. doi: 10.1016/S1470-2045(18)30351-6
39. Balar AV, Castellano D, O’Donnell PH, Grivas P, Vuky J, Powles T, et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): a multicentre, single-arm, phase 2 study. Lancet Oncol (2017) 18:1483–92. doi: 10.1016/S1470-2045(17)30616-2
40. Bellmunt J, de Wit R, Vaughn DJ, Fradet Y, Lee JL, Fong L, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med (2017) 376:1015–26. doi: 10.1056/NEJMOA1613683
41. Jørgensen JT. An update on companion and complementary diagnostic assays for PD-1/PD-L1 checkpoint inhibitors in NSCLC. Expert Rev Mol Diagn (2021) 21:445–54. doi: 10.1080/14737159.2021.1920396
42. Fundytus A, Booth CM, Tannock IF. How low can you go? PD-L1 expression as a biomarker in trials of cancer immunotherapy. Ann Oncol (2021) 32:833–6. doi: 10.1016/j.annonc.2021.03.208
43. Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M, de Castro G Jr, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet (London England) (2019) 394:1915–28. doi: 10.1016/S0140-6736(19)32591-7
44. Cortes J, Cescon DW, Rugo HS, Nowecki Z, Im SA, Yusof MM, et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet (London England) (2020) 396:1817–28. doi: 10.1016/S0140-6736(20)32531-9
45. Hong L, Negrao MV, Dibaj SS, Chen R, Reuben A, Bohac JM, et al. Programmed death-ligand 1 heterogeneity and its impact on benefit from immune checkpoint inhibitors in NSCLC. J Thorac Oncol (2020) 15:1449–59. doi: 10.1016/j.jtho.2020.04.026
46. Schoenfeld AJ, Rizvi H, Bandlamudi C, Sauter JL, Travis WD, Rekhtman N, et al. Clinical and molecular correlates of PD-L1 expression in patients with lung adenocarcinomas. Ann Oncol (2020) 31:599–608. doi: 10.1016/j.annonc.2020.01.065
47. Omori S, Kenmotsu H, Abe M, Watanabe R, Sugino T, Kobayashi H, et al. Changes in programmed death ligand 1 expression in non-small cell lung cancer patients who received anticancer treatments. Int J Clin Oncol (2018) 23:1052–9. doi: 10.1007/s10147-018-1305-4
48. Jiang L, Guo F, Liu X, Li X, Qin Q, Shu P, et al. Continuous targeted kinase inhibitors treatment induces upregulation of PD-L1 in resistant NSCLC. Sci Rep (2019) 9:1–9. doi: 10.1038/s41598-018-38068-3
49. Wu J, Sun W, Yang X, Wang H, Liu X, Chi K, et al. Heterogeneity of programmed death-ligand 1 expression and infiltrating lymphocytes in paired resected primary and metastatic non-small cell lung cancer. Mod Pathol (2022) 35:218–27. doi: 10.1038/s41379-021-00903-w
50. Jotte R, Cappuzzo F, Vynnychenko I, Stroyakovskiy D, Rodríguez-Abreu D, Hussein M, et al. Atezolizumab in combination with carboplatin and nab-paclitaxel in advanced squamous NSCLC (IMpower131): Results from a randomized phase III trial. J Thorac Oncol (2020) 15:1351–60. doi: 10.1016/j.jtho.2020.03.028
51. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Lao CD, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med (2019) 381:1535–46. doi: 10.1056/NEJMOA1910836
52. Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med (2018) 378:1277–90. doi: 10.1056/NEJMOA1712126
53. Govindan R, Szczesna A, Ahn MJ, Schneider CP, Gonzalez Mella PF, Barlesi F, et al. Phase III trial of ipilimumab combined with paclitaxel and carboplatin in advanced squamous non–small-cell lung cancer. J Clin Oncol (2017) 35:3449–57. doi: 10.1200/JCO.2016.71.7629
54. de Ruiter EJ, Mulder FJ, Koomen BM, Speel EJ, van den Hout MFCM, de Roest RH, et al. Comparison of three PD-L1 immunohistochemical assays in head and neck squamous cell carcinoma (HNSCC). Mod Pathol (2021) 34:1125–32. doi: 10.1038/S41379-020-0644-7
55. Mazieres J, Drilon A, Lusque A, Mhanna L, Cortot AB, Mezquita L, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the IMMUNOTARGET registry. Ann Oncol (2019) 30:1321–8. doi: 10.1093/annonc/mdz167
56. Rittmeyer A, Barlesi F, Waterkamp D, Park K, Ciardiello F, von Pawel J, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet (2017) 389:255–65. doi: 10.1016/S0140-6736(16)32517-X
57. Fehrenbacher L, Spira A, Ballinger M, Kowanetz M, Vansteenkiste J, Mazieres J, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet (2016) 387:1837–46. doi: 10.1016/S0140-6736(16)00587-0
58. Jeanson A, Tomasini P, Souquet-Bressand M, Brandone N, Boucekine M, Grangeon M, et al. Efficacy of immune checkpoint inhibitors in KRAS-mutant non-small cell lung cancer (NSCLC). J Thorac Oncol (2019) 14:1095–101. doi: 10.1016/j.jtho.2019.01.011
59. Lee CK, Man J, Lord S, Cooper W, Links M, Gebski V, et al. Clinical and molecular characteristics associated with survival among patients treated with checkpoint inhibitors for advanced non-small cell lung carcinoma: A systematic review and meta-analysis. JAMA Oncol (2018) 4:210–6. doi: 10.1001/jamaoncol.2017.4427
60. Huang Q, Zhang H, Hai J, Socinski MA, Lim E, Chen H, et al. Impact of PD-L1 expression, driver mutations and clinical characteristics on survival after anti-PD-1/PD-L1 immunotherapy versus chemotherapy in non-small-cell lung cancer: A meta-analysis of randomized trials. Oncoimmunology (2018) 7:1–11. doi: 10.1080/2162402X.2017.1396403
61. Sun L, Hsu M, Cohen RB, Langer CJ, Mamtani R, Aggarwal C. Association between KRAS variant status and outcomes with first-line immune checkpoint inhibitor-based therapy in patients with advanced non-Small-Cell lung cancer. JAMA Oncol (2021) 7:937–9. doi: 10.1001/JAMAONCOL.2021.0546
62. Emerson MA, Banegas MP, Chawla N, Achacoso N, Alexeeff SE, Adams AS, et al. Disparities in prostate, lung, breast, and colorectal cancer survival and comorbidity status among urban American indians and alaskan natives. Cancer Res (2017) 77:6770–6. doi: 10.1158/0008-5472.CAN-17-0429
63. Skoulidis F, Goldberg ME, Greenawalt DM, Hellmann MD, Awad MM, Gainor JF, et al. STK11/LKB1 mutations and PD-1 inhibitor resistance in KRAS-mutant lung adenocarcinoma. Cancer Discovery (2018) 8:822–35. doi: 10.1158/2159-8290.CD-18-0099
64. Gu M, Xu T, Chang P. KRAS/LKB1 and KRAS/TP53 co-mutations create divergent immune signatures in lung adenocarcinomas. Ther Adv Med Oncol (2021) 13:1–13. doi: 10.1177/17588359211006950
65. Brahmer J, Reckamp KL, Baas P, Crinò L, Eberhardt WE, Poddubskaya E, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med (2015) 373:123–35. doi: 10.1056/NEJMoa1504627
66. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab versus docetaxel in advanced nonsquamous non-Small-Cell lung cancer. N Engl J Med (2015) 373:1627–39. doi: 10.1056/NEJMOA1507643
67. Lee CK, Man J, Lord S, Links M, Gebski V, Mok T, et al. Checkpoint inhibitors in metastatic EGFR-mutated non–small cell lung cancer–a meta-analysis. J Thorac Oncol (2017) 12:403–7. doi: 10.1016/j.jtho.2016.10.007
68. Gainor JF, Shaw AT, Sequist LV, Fu X, Azzoli CG, Piotrowska Z, et al. EGFR mutations and ALK rearrangements are associated with low response rates to PD-1 pathway blockade in non-small cell lung cancer: A retrospective analysis. Clin Cancer Res (2016) 22:4585–93. doi: 10.1158/1078-0432.CCR-15-3101
69. Hastings K, Yu HA, Wei W, Sanchez-Vega F, DeVeaux M, Choi J, et al. EGFR mutation subtypes and response to immune checkpoint blockade treatment in non-small-cell lung cancer. Ann Oncol (2019) 30:1311–20. doi: 10.1093/annonc/mdz141
70. Hayashi H, Sugawara S, Fukuda Y, Fujimoto D, Miura S, Ota K, et al. A randomized phase II study comparing nivolumab with carboplatin–pemetrexed for EGFR -mutated NSCLC with resistance to EGFR tyrosine kinase inhibitors (WJOG8515L). Clin Cancer Res (2022) 28:893–902. doi: 10.1158/1078-0432.ccr-21-3194
71. Soo RA, Lim SM, Syn NL, Teng R, Soong R, Mok TSK, et al. Immune checkpoint inhibitors in epidermal growth factor receptor mutant non-small cell lung cancer: Current controversies and future directions. Lung Cancer (2018) 115:12–20. doi: 10.1016/j.lungcan.2017.11.009
72. Qiao M, Jiang T, Liu X, Mao S, Zhou F, Li X, et al. Immune checkpoint inhibitors in EGFR-mutated NSCLC: Dusk or dawn? J Thorac Oncol (2021) 16:1267–88. doi: 10.1016/j.jtho.2021.04.003
73. Reck M, Mok TS, Nishio M, Jotte RM, Cappuzzo F, Orlandi F, et al. Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial. Lancet Respir Med (2019) 7:387–401. doi: 10.1016/S2213-2600(19)30084-0
74. Nogami N, Barlesi F, Socinski MA, Reck M, Thomas CA, Cappuzzo F, et al. IMpower150 final exploratory analyses for atezolizumab plus bevacizumab and chemotherapy in key NSCLC patient subgroups with EGFR mutations or metastases in the liver or brain. J Thorac Oncol (2022) 17:309–23. doi: 10.1016/j.jtho.2021.09.014
75. Garassino MC, Cho BC, Kim JH, Mazières J, Vansteenkiste J, Lena H, et al. Durvalumab as third-line or later treatment for advanced non-small-cell lung cancer (ATLANTIC): an open-label, single-arm, phase 2 study. Lancet Oncol (2018) 19:521–36. doi: 10.1016/S1470-2045(18)30144-X
76. Rizvi NA, Hellmann MD, Brahmer JR, Juergens RA, Borghaei H, Gettinger S, et al. Nivolumab in combination with platinum-based doublet chemotherapy for first-line treatment of advanced non-Small-Cell lung cancer. J Clin Oncol (2016) 34:2969–79. doi: 10.1200/JCO.2016.66.9861
77. Hellmann MD, Rizvi NA, Goldman JW, Gettinger SN, Borghaei H, Brahmer JR, et al. Nivolumab plus ipilimumab as first-line treatment for advanced non-small-cell lung cancer (CheckMate 012): results of an open-label, phase 1, multicohort study. Lancet Oncol (2017) 18:31–41. doi: 10.1016/S1470-2045(16)30624-6
78. National institute of public health (2022). Available at: https://rctportal.niph.go.jp/s/detail/um?trial_id=jRCTs031190066 (Accessed April 23, 2022).
79. UMIN-CTR (2019). Available at: https://upload.umin.ac.jp/cgi-open-in/ctr/ctr_view.cgi?recptno=R000043275 (Accessed April 23, 2022).
80. Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med (2010) 362:2380–8. doi: 10.1056/NEJMoa0909530
81. Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol (2010) 11:121–8. doi: 10.1016/S1470-2045(09)70364-X
82. Mok TS, Wu Y-L, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med (2009) 361:947–57. doi: 10.1056/NEJMOA0810699
83. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol (2012) 13:239–46. doi: 10.1016/S1470-2045(11)70393-X
84. Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol (2011) 12:735–42. doi: 10.1016/S1470-2045(11)70184-X
85. Sequist LV, Yang JCH, Yamamoto N, O'Byrne K, Hirsh V, Mok T, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol (2013) 31:3327–34. doi: 10.1200/JCO.2012.44.2806
86. Wu YL, Zhou C, Hu CP, Feng J, Lu S, Huang Y, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-lung 6): An open-label, randomised phase 3 trial. Lancet Oncol (2014) 15:213–22. doi: 10.1016/S1470-2045(13)70604-1
87. Solomon BJ, Mok T, Kim D-W, Wu YL, Nakagawa K, Mekhail T, et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med (2014) 371:2167–77. doi: 10.1056/NEJMOA1408440
88. Soria JC, Tan DSW, Chiari R, et al. First-line ceritinib versus platinum-based chemotherapy in advanced ALK-rearranged non-small-cell lung cancer (ASCEND-4): a randomised, open-label, phase 3 study. Lancet (2017) 389:917–29. doi: 10.1016/S0140-6736(17)30123-X
89. Oxnard GR, Yang JCH, Yu H, Kim SW, Saka H, Horn L, et al. TATTON: a multi-arm, phase ib trial of osimertinib combined with selumetinib, savolitinib, or durvalumab in EGFR-mutant lung cancer. Ann Oncol (2020) 31:507–16. doi: 10.1016/j.annonc.2020.01.013
90. Chih-Hsin Yang J, Shepherd FA, Kim DW, Lee GW, Lee JS, Chang GC, et al. Osimertinib plus durvalumab versus osimertinib monotherapy in EGFR T790M–positive NSCLC following previous EGFR TKI therapy: CAURAL brief report. J Thorac Oncol (2019) 14:933–9. doi: 10.1016/j.jtho.2019.02.001
91. Spigel DR, Reynolds C, Waterhouse D, Garon EB, Chandler J, Babu S, et al. Phase 1/2 study of the safety and tolerability of nivolumab plus crizotinib for the first-line treatment of anaplastic lymphoma kinase translocation — positive advanced non–small cell lung cancer (CheckMate 370). J Thorac Oncol (2018) 13:682–8. doi: 10.1016/j.jtho.2018.02.022
92. Hanna N, Johnson D, Temin S, Baker Jr Brahmer S J, Ellis PM, et al. Systemic therapy for stage IV non–Small-Cell lung cancer: American society of clinical oncology clinical practice guideline update. J Clin Oncol (2017) 35:3484–515. doi: 10.1200/JCO.2017.74.6065
93. Planchard D, Popat S, Kerr K, Novello S, Smit EF, Faivre-Finn C, et al. ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2018) 29:iv192–237. doi: 10.1093/annonc/mdy275
94. Akamatsu H, Ninomiya K, Kenmotsu H, Morise M, Daga H, Goto Y, et al. The Japanese lung cancer society guideline for non-small cell lung cancer, stage IV. Int J Clin Oncol (2019) 24:731–70. doi: 10.1007/S10147-019-01431-Z
95. Masuda K, Horinouchi H, Tanaka M, Higashiyama R, Shinno Y, Sato J, et al. Efficacy of anti-PD-1 antibodies in NSCLC patients with an EGFR mutation and high PD-L1 expression. J Cancer Res Clin Oncol (2021) 147:245–51. doi: 10.1007/s00432-020-03329-0
96. Lin K, Cheng J, Yang T, Li Y, Zhu B. EGFR-TKI down-regulates PD-L1 in EGFR mutant NSCLC through inhibiting NF-κB. Biochem Biophys Res Commun (2015) 463:95–101. doi: 10.1016/J.BBRC.2015.05.030
97. Chen N, Fang W, Zhan J, Hong S, Tang Y, Kang S, et al. Upregulation of PD-L1 by EGFR activation mediates the immune escape in EGFR-driven NSCLC: Implication for optional immune targeted therapy for NSCLC patients with EGFR mutation. J Thorac Oncol (2015) 10:910–23. doi: 10.1097/JTO.0000000000000500
98. Johnson DE, O’Keefe RA, Grandis JR. Targeting the IL-6/JAK/STAT3 signalling axis in cancer. Nat Rev Clin Oncol (2018) 15:234–48. doi: 10.1097/JTO.0000000000000500
99. Hsu PC, Jablons DM, Yang CT, You L. Epidermal growth factor receptor (EGFR) pathway, yes-associated protein (YAP) and the regulation of programmed death-ligand 1 (PD-L1) in non-small cell lung cancer (NSCLC). Int J Mol Sci (2019) 20:3821. doi: 10.3390/IJMS20153821
100. Riihimäki M, Hemminki A, Fallah M, Thomsen H, Sundquist K, Sundquist J, et al. Metastatic sites and survival in lung cancer. Lung Cancer (2014) 86:78–84. doi: 10.1016/j.lungcan.2014.07.020
101. Ren Y, Dai C, Zheng H, Zhou F, She Y, Jiang G, et al. Prognostic effect of liver metastasis in lung cancer patients with distant metastasis. Oncotarget (2016) 7:53245–53. doi: 10.18632/oncotarget.10644
102. Kitadai R, Okuma Y, Hakozaki T, Hosomi Y. The efficacy of immune checkpoint inhibitors in advanced non-small-cell lung cancer with liver metastases. J Cancer Res Clin Oncol (2020) 146:777–85. doi: 10.1007/s00432-019-03104-w
103. Shiroyama T, Suzuki H, Tamiya M, Amiya A, Tanaka A, Okamoto N, et al. Clinical characteristics of liver metastasis in nivolumabtreated patients with non-small cell lung cancer. Anticancer Res (2018) 38:4723–9. doi: 10.21873/anticanres.12779
104. Schmid S, Diem S, Li Q, Krapf M, Flatz L, Leschka S, et al. Organ-specific response to nivolumab in patients with non-small cell lung cancer (NSCLC). Cancer Immunol Immunother (2018) 67:1825–32. doi: 10.1007/s00262-018-2239-4
105. Tumeh PC, Hellmann MD, Hamid O, Tsai KK, Loo KL, Gubens MA, et al. Liver metastasis and treatment outcome with anti-PD-1 monoclonal antibody in patients with melanoma and NSCLC. Cancer Immunol Res (2017) 5:417–24. doi: 10.1158/2326-6066.CIR-16-0325
106. Huang Y, Zhu L, Guo T, Chen W, Zhang Z, Li W, et al. Metastatic sites as predictors in advanced NSCLC treated with PD-1 inhibitors: a systematic review and meta-analysis. Hum Vaccines Immunother (2021) 17:1278–87. doi: 10.1080/21645515.2020.1823779
107. Jenne CN, Kubes P. Immune surveillance by the liver. Nat Immunol (2013) 14:996–1006. doi: 10.1038/NI.2691
108. Doherty DG. Immunity, tolerance and autoimmunity in the liver: A comprehensive review. J Autoimmun (2016) 66:60–75. doi: 10.1016/J.JAUT.2015.08.020
109. Brodt P. Role of the microenvironment in liver metastasis: From pre- to prometastatic niches. Clin Cancer Res (2016) 22:5971–82. doi: 10.1158/1078-0432.CCR-16-0460
110. Lee JC, Green MD, Huppert LA, Chow C, Pierce RH, Daud AI. The liver–immunity nexus and cancer immunotherapy. Clin Cancer Res (2022) 28:5–12. doi: 10.1158/1078-0432.ccr-21-1193
111. Qiao M, Zhou F, Hou L, Li X, Zhao C, Jiang T, et al. Efficacy of immune-checkpoint inhibitors in advanced non-small cell lung cancer patients with different metastases. Ann Transl Med (2021) 9:34. doi: 10.21037/atm-20-1471
112. Sato H, Nagashima H, Akiyama M, Ito T, Hashimoto T, Saikawa H, et al. Analysis of bevacizumab treatments and metastatic sites of lung cancer. Cancer Treat Res Commun (2021) 26:100290. doi: 10.1016/J.CTARC.2020.100290
113. Jain RK. Normalizing tumor vasculature with anti-angiogenic therapy: a new paradigm for combination therapy. Nat Med (2001) 7:987–9. doi: 10.1038/NM0901-987
114. Osada T, Chong G, Tansik R, Hong T, Spector N, Kumar R, et al. The effect of anti-VEGF therapy on immature myeloid cell and dendritic cells in cancer patients. Cancer Immunol Immunother (2008) 57:1115–24. doi: 10.1007/S00262-007-0441-X
115. Terme M, Pernot S, Marcheteau E, Sandoval F, Benhamouda N, Colussi O, et al. VEGFA-VEGFR pathway blockade inhibits tumor-induced regulatory T-cell proliferation in colorectal cancer. Cancer Res (2013) 73:539–49. doi: 10.1158/0008-5472.CAN-12-2325
116. Kusmartsev S, Eruslanov E, Kübler H, Tseng T, Sakai Y, Su Z, et al. Oxidative stress regulates expression of VEGFR1 in myeloid cells: link to tumor-induced immune suppression in renal cell carcinoma. J Immunol (2008) 181:346–53. doi: 10.4049/JIMMUNOL.181.1.346
117. Khan KA, Kerbel RS. Improving immunotherapy outcomes with anti-angiogenic treatments and vice versa. Nat Rev Clin Oncol (2018) 15:310–24. doi: 10.1038/nrclinonc.2018.9
118. Chen Y, Hu J, Bu F, Zhang H, Fei K, Zhang P. Clinical characteristics of hyperprogressive disease in NSCLC after treatment with immune checkpoint inhibitor: A systematic review and meta-analysis. BMC Cancer (2020) 20:1–9. doi: 10.1186/s12885-020-07206-4
119. Sasaki A, Nakamura Y, Mishima S, Kawazoe A, Kuboki Y, Bando H, et al. Predictive factors for hyperprogressive disease during nivolumab as anti-PD1 treatment in patients with advanced gastric cancer. Gastric Cancer (2019) 22:793–802. doi: 10.1007/S10120-018-00922-8
120. Kim JY, Lee KH, Kang J, Borcoman E, Saada-Bouzid E, Kronbichler A, et al. Hyperprogressive disease during anti-PD-1 (PDCD1) / PD-L1 (CD274) therapy: A systematic review and meta-analysis. Cancers (Basel) (2019) 11:1–18. doi: 10.3390/cancers11111699
121. Kato S, Goodman A, Walavalkar V, Barkauskas DA, Sharabi A, Kurzrock R. Hyperprogressors after immunotherapy: Analysis of genomic alterations associated with accelerated growth rate. Clin Cancer Res (2017) 23:4242–50. doi: 10.1158/1078-0432.CCR-16-3133
122. Borgelt B, Gelber R, Kramer S, Brady LW, Chang CH, Davis LW, et al. The palliation of brain metastases: final results of the first two studies by the radiation therapy oncology group. Int J Radiat Oncol Biol Phys (1980) 6:1–9. doi: 10.1016/0360-3016(80)90195-9
123. Pillai RN, Behera M, Owonikoko TK, et al. Nivolumab versus docetaxel in previously treated patients with advanced non-small-cell lung cancer: Two-year outcomes from two randomized, open-label, phase III trials (CheckMate 017 and CheckMate 057). J Clin Oncol (2018) 15:2849–53. doi: 10.1016/j.annonc.2021.04.008
124. Powell SF, Rodríguez-Abreu D, Langer CJ, Tafreshi A, Paz-Ares L, Kopp HG, et al. Outcomes with pembrolizumab plus platinum-based chemotherapy for patients with NSCLC and stable brain metastases: Pooled analysis of KEYNOTE-021, -189, and -407. J Thorac Oncol (2021) 16:1883–92. doi: 10.1016/J.JTHO.2021.06.020
125. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non–small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol (2019) 37:537–46. doi: 10.1200/JCO.18.00149
126. Pantano F, Russano M, Berruti A, Mansueto G, Migliorino MR, Adamo V, et al. Prognostic clinical factors in patients affected by non-small-cell lung cancer receiving nivolumab. Expert Opin Biol Ther (2020) 20:319–26. doi: 10.1080/14712598.2020.1724953
127. Long GV, Atkinson V, Lo S, Sandhu S, Guminski AD, Brown MP, et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: a multicentre randomised phase 2 study. Lancet Oncol (2018) 19:672–81. doi: 10.1016/S1470-2045(18)30139-6
128. Grant MJ, Herbst RS, Goldberg SB. Selecting the optimal immunotherapy regimen in driver-negative metastatic NSCLC. Nat Rev Clin Oncol (2021) 18:625–44. doi: 10.1038/s41571-021-00520-1
129. Sheng L, Gao J, Xu Q, Zhang X, Huang M, Dai X, et al. Selection of optimal first-line immuno-related therapy based on specific pathological characteristics for patients with advanced driver-gene wild-type non-small cell lung cancer: a systematic review and network meta-analysis. Ther Adv Med Oncol (2021) 13:1–18. doi: 10.1177/17588359211018537
130. Ryu JS, Ryu HJ, Lee SN, Memon A, Lee SK, Nam HS, et al. Prognostic impact of minimal pleural effusion in non - small-cell lung cancer. J Clin Oncol (2014) 32:960–7. doi: 10.1200/JCO.2013.50.5453
131. Sugiura S, Ando Y, Minami H. Prognostic value of pleural effusion in patients with non-small-cell lung cancer. Clin Cancer Res (1997) 3:47–50.
132. Morgensztern D, Waqar S, Subramanian J, Trinkaus K, Govindan R. Prognostic impact of malignant pleural effusion at presentation in patients with metastatic non-small-cell lung cancer. J Thorac Oncol (2012) 7:1485–9. doi: 10.1097/JTO.0B013E318267223A
133. Morita M, Tamiya M, Fujimoto D, Tamiya A, Suzuki H, Hirano K, et al. Prediction of patients with a tumor proportion score > 50% who do not respond to first-line monotherapy with pembrolizumab. BMC Cancer (2020) 20:2–4. doi: 10.1186/s12885-020-6582-4
134. Adachi Y, Tamiya A, Taniguchi Y, Enomoto T, Azuma K, Kouno S, et al. Predictive factors for progression-free survival in non-small cell lung cancer patients receiving nivolumab based on performance status. Cancer Med (2020) 9:1383–91. doi: 10.1002/cam4.2807
135. Kawachi H, Tamiya M, Tamiya A, Ishii S, Hirano K, Matsumoto H, et al. Association between metastatic sites and first-line pembrolizumab treatment outcome for advanced non–small cell lung cancer with high PD-L1 expression: a retrospective multicenter cohort study. Invest New Drugs (2020) 38:211–8. doi: 10.1007/s10637-019-00882-5
136. Kawachi H, Tamiya M, Taniguchi Y, Yokoyama T, Yokoe S, Oya Y, et al. Efficacy of immune checkpoint inhibitor with or without chemotherapy for nonsquamous NSCLC with malignant pleural effusion: A retrospective multicenter cohort study. JTO Clin Res Rep (2022) 3:100355. doi: 10.1016/j.jtocrr.2022.100355
137. Murthy P, Ekeke CN, Russell KL, Butler SC, Wang Y, Luketich JD, et al. Making cold malignant pleural effusions hot: driving novel immunotherapies. Oncoimmunology (2019) 8:e1554969. doi: 10.1080/2162402X.2018.1554969
138. Saito Y, Sasaki S, Oikado K, Tominaga J, Sata M, Sakai F, et al. Radiographic features and poor prognostic factors of interstitial lung disease with nivolumab for non–small cell lung cancer. Cancer Sci (2021) 112:1495–505. doi: 10.1111/cas.14710
139. Ellis LM, Hicklin DJ. VEGF-targeted therapy: mechanisms of anti-tumour activity. Nat Rev Cancer (2008) 8:579–91. doi: 10.1038/NRC2403
140. Hegde PS, Wallin JJ, Mancao C. Predictive markers of anti-VEGF and emerging role of angiogenesis inhibitors as immunotherapeutics. Semin Cancer Biol (2018) 52:117–24. doi: 10.1016/J.SEMCANCER.2017.12.002
141. Kitamura K, Kubota K, Ando M, Takahashi S, Nishijima N, Sugano T, et al. Bevacizumab plus chemotherapy for advanced non-squamous non-small-cell lung cancer with malignant pleural effusion. Cancer Chemother Pharmacol (2013) 71:457–61. doi: 10.1007/S00280-012-2026-4
142. Tamiya M, Tamiya A, Yamadori T, Nakao K, Asami K, Yasue T, et al. Phase2 study of bevacizumab with carboplatin-paclitaxel for non-small cell lung cancer with malignant pleural effusion. Med Oncol (2013) 30:676. doi: 10.1007/S12032-013-0676-7
143. Tamiya M, Tamiya A, Yasue T, Nakao K, Omachi N, Shiroyama T, et al. Vascular endothelial growth factor in plasma and pleural effusion is a biomarker for outcome after bevacizumab plus carboplatin-paclitaxel treatment for non-small cell lung cancer with malignant pleural effusion. Anticancer Res (2016) 36:2939–44.
144. Noro R, Kobayashi K, Usuki J, Yomota M, Nishitsuji M, Shimokawa T, et al. Bevacizumab plus chemotherapy in nonsquamous non-small cell lung cancer patients with malignant pleural effusion uncontrolled by tube drainage or pleurodesis: A phase II study north East Japan study group trial NEJ013B. Thorac Cancer (2020) 11:1876–84. doi: 10.1111/1759-7714.13472
145. Marur S, Singh H, Mishra-Kalyani P, Larkins E, Keegan P, Sridhara R, et al. FDA Analyses of survival in older adults with metastatic non-small cell lung cancer in controlled trials of PD-1/PD-L1 blocking antibodies. Semin Oncol (2018) 45:220–5. doi: 10.1053/J.SEMINONCOL.2018.08.007
146. Elias R, Giobbie-Hurder A, McCleary NJ, Ott P, Hodi FS, Rahma O. Efficacy of PD-1 & PD-L1 inhibitors in older adults: a meta-analysis. J Immunother Cancer (2018) 6:26. doi: 10.1186/S40425-018-0336-8
147. Galli G, De Toma A, Pagani F, Randon G, Trevisan B, Prelaj A, et al. Efficacy and safety of immunotherapy in elderly patients with non-small cell lung cancer. Lung Cancer (2019) 137:38–42. doi: 10.1016/j.lungcan.2019.08.030
148. Muchnik E, Loh KP, Strawderman M, Magnuson A, Mohile SG, Estrah V, et al. Immune checkpoint inhibitors in real-world treatment of older adults with non–small cell lung cancer. J Am Geriatr Soc (2019) 67:905–12. doi: 10.1111/jgs.15750
149. Nebhan CA, Cortellini A, Ma W, Ganta T, Song H, Ye F, et al. Clinical outcomes and toxic effects of single-agent immune checkpoint inhibitors among patients aged 80 years or older with cancer: A multicenter international cohort study. JAMA Oncol (2021) 7:1856–61. doi: 10.1001/JAMAONCOL.2021.4960
150. Spigel DR, McCleod M, Jotte RM, Einhorn L, Horn L, Waterhouse DM, et al. Safety, efficacy, and patient-reported health-related quality of life and symptom burden with nivolumab in patients with advanced non–small cell lung cancer, including patients aged 70 years or older or with poor performance status (CheckMate 153). J Thorac Oncol (2019) 14:1628–39. doi: 10.1016/j.jtho.2019.05.010
151. European Medical agenc (2022). Available at: https://www.ema.europa.eu/en/documents/variation-report/keytruda-h-c-3820-ii-0043-epar-assessment-report-variation_en.pdf (Accessed April 23, 2022).
152. Morimoto K, Yamada T, Yokoi T, Kijima T, Goto Y, Nakao A, et al. Clinical impact of pembrolizumab combined with chemotherapy in elderly patients with advanced non-small-cell lung cancer. Lung Cancer (2021) 161:26–33. doi: 10.1016/J.LUNGCAN.2021.08.015
153. Hamaker ME, Jonker JM, de Rooij SE, Vos AG, Smorenburg CH, van Munster BC. Frailty screening methods for predicting outcome of a comprehensive geriatric assessment in elderly patients with cancer: a systematic review. Lancet Oncol (2012) 13:e437–44. doi: 10.1016/S1470-2045(12)70259-0
154. Garcia MV, Agar MR, Soo WK, To T, Phillips JL. Screening tools for identifying older adults with cancer who may benefit from a geriatric assessment: A systematic review. JAMA Oncol (2021) 7:616–27. doi: 10.1001/JAMAONCOL.2020.6736
155. Le Caer H, Borget I, Corre R, Locher C, Raynaud C, Decroisette C, et al. Prognostic role of a comprehensive geriatric assessment on the management of elderly patients with advanced non-small cell lung cancer (NSCLC): a pooled analysis of two prospective phase II trials by the GFPC group. J Thorac Dis (2017) 9:3747–54. doi: 10.21037/JTD.2017.09.51
156. Kanesvaran R, Li H, Koo KN, Poon D. Analysis of prognostic factors of comprehensive geriatric assessment and development of a clinical scoring system in elderly Asian patients with cancer. J Clin Oncol (2011) 29:3620–7. doi: 10.1200/JCO.2010.32.0796
157. Tammemagi CM, Neslund-Dudas C, Simoff M, Kvale P. Impact of comorbidity on lung cancer survival. Int J Cancer (2003) 103:792–802. doi: 10.1002/IJC.10882
158. Schiller JH, Harrington D, Belani CP, Langer C, Sandler A, Krook J, et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med (2002) 346:92–8. doi: 10.1056/NEJMoa011954
159. Sweeney CJ, Zhu J, Sandler AB, Schiller J, Belani CP, Langer C, et al. Outcome of patients with a performance status of 2 in Eastern cooperative oncology group study E1594: A phase III trial in patients with metastatic nonsmall cell lung carcinoma. Cancer (2001) 92:2639–47. doi: 10.1002/1097-0142(20011115)92:10<2639::AID-CNCR1617>3.0.CO;2-8
160. Balar AV, Galsky MD, Rosenberg JE, Powles T, Petrylak DP, Bellmunt J, et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet (2017) 389:67–76. doi: 10.1016/S0140-6736(16)32455-2
161. Felip E, Ardizzoni A, Ciuleanu T, Cobo M, Laktionov K, Szilasi M, et al. CheckMate 171: A phase 2 trial of nivolumab in patients with previously treated advanced squamous non-small cell lung cancer, including ECOG PS 2 and elderly populations. Eur J Cancer (2020) 127:160–72. doi: 10.1016/J.EJCA.2019.11.019
162. Middleton G, Brock K, Savage J, Mant R, Summers Y, Connibear J, et al. Pembrolizumab in patients with non-small-cell lung cancer of performance status 2 (PePS2): a single arm, phase 2 trial. Lancet Respir Med (2020) 8:895–904. doi: 10.1016/S2213-2600(20)30033-3
163. Matsubara T, Seto T, Takamori S, Fujishita T, Toyozawa R, Ito K, et al. Anti-PD-1 monotherapy for advanced NSCLC patients with older age or those with poor performance status. Onco Targets Ther (2021) 14:1961–8. doi: 10.2147/OTT.S301500
164. Dall’Olio FG, Maggio I, Massucci M, Mollica V, Fragomeno B, Ardizzoni A. ECOG performance status ≥2 as a prognostic factor in patients with advanced non small cell lung cancer treated with immune checkpoint inhibitors–a systematic review and meta-analysis of real world data. Lung Cancer (2020) 145:95–104. doi: 10.1016/j.lungcan.2020.04.027
165. Sehgal K, Gill RR, Widick P, Bindal P, McDonald DC, Shea M, et al. Association of performance status with survival in patients with advanced non-small cell lung cancer treated with pembrolizumab monotherapy. JAMA Netw Open (2021) 4:2–12. doi: 10.1001/jamanetworkopen.2020.37120
166. Nishino M, Cardarella S, Dahlberg SE, Araki T, Lydon C, Jackman DM, et al. Interstitial lung abnormalities in treatment-naïve advanced non-small-cell lung cancer patients are associated with shorter survival. Eur J Radiol (2015) 84:998–1004. doi: 10.1016/j.ejrad.2015.01.021
167. Kanai O, Kim YH, Demura Y, Kanai M, Ito T, Fujita K, et al. Efficacy and safety of nivolumab in non-small cell lung cancer with preexisting interstitial lung disease. Thorac Cancer (2018) 9:847–55. doi: 10.1111/1759-7714.12759
168. Yamaguchi T, Shimizu J, Hasegawa T, Horio Y, Inaba Y, Yatabe Y, et al. Pre-existing pulmonary fibrosis is a risk factor for anti-PD-1-related pneumonitis in patients with non-small cell lung cancer: A retrospective analysis. Lung Cancer (2018) 125:212–7. doi: 10.1016/J.LUNGCAN.2018.10.001
169. Nakanishi Y, Masuda T, Yamaguchi K, Sakamoto S, Horimasu Y, Nakashima T, et al. Pre-existing interstitial lung abnormalities are risk factors for immune checkpoint inhibitor-induced interstitial lung disease in non-small cell lung cancer. Respir Investig (2019) 57:451–9. doi: 10.1016/J.RESINV.2019.05.002
170. Watanabe S, Ota T, Hayashi M, Ishikawa H, Otsubo A, Shoji S, et al. Prognostic significance of the radiologic features of pneumonitis induced by anti-PD-1 therapy. Cancer Med (2020) 9:3070–7. doi: 10.1002/cam4.2974
171. Walsh SLF, Calandriello L, Sverzellati N, Wells AU, Hansell DM. Interobserver agreement for the ATS/ERS/JRS/ALAT criteria for a UIP pattern on CT. Thorax (2016) 71:45–51. doi: 10.1136/THORAXJNL-2015-207252
172. Widell J, Lidén M. Interobserver variability in high-resolution CT of the lungs. Eur J Radiol Open (2020) 7:100228. doi: 10.1016/J.EJRO.2020.100228
173. Ikeda S, Kato T, Kenmotsu H, Ogura T, Iwasawa S, Sato Y, et al. A phase 2 study of atezolizumab for pretreated NSCLC with idiopathic interstitial pneumonitis. J Thorac Oncol (2020) 15:1935–42. doi: 10.1016/j.jtho.2020.08.018
174. Kenmotsu H, Naito T, Kimura M, Ono A, Shukuya T, Nakamura Y, et al. The risk of cytotoxic chemotherapy-related exacerbation of interstitial lung disease with lung cancer. J Thorac Oncol (2011) 6:1242–6. doi: 10.1097/JTO.0b013e318216ee6b
175. Fujimoto D, Yomota M, Sekine A, Morita M, Morimoto T, Hosomi Y, et al. Nivolumab for advanced non-small cell lung cancer patients with mild idiopathic interstitial pneumonia: A multicenter, open-label single-arm phase II trial. Lung Cancer (2019) 134:274–8. doi: 10.1016/j.lungcan.2019.06.001
176. Nishino M, Giobbie-Hurder A, Hatabu H, Ramaiya NH, Hodi FS. Incidence of programmed cell death 1 inhibitor-related pneumonitis in patients with advanced cancer a systematic review and meta-analysis supplemental content. JAMA Oncol (2016) 2:1607–16. doi: 10.1001/jamaoncol.2016.2453
177. Naidoo J, Wang X, Woo KM, Iyriboz T, Halpenny D, Cunningham J, et al. Pneumonitis in patients treated with anti-programmed death-1/programmed death ligand 1 therapy. J Clin Oncol (2017) 35:709–17. doi: 10.1200/JCO.2016.68.2005
178. Khunger M, Rakshit S, Pasupuleti V, Hernandez AV, Mazzone P, Stevenson J, et al. Incidence of pneumonitis with use of programmed death 1 and programmed death-ligand 1 inhibitors in non-small cell lung cancer: A systematic review and meta-analysis of trials. Chest (2017) 152:271–81. doi: 10.1016/J.CHEST.2017.04.177
179. Weber JS, Yang JC, Atkins MB, Disis ML. Toxicities of immunotherapy for the practitioner. J Clin Oncol (2015) 33:2092–9. doi: 10.1200/JCO.2014.60.0379
Keywords: aged, interstitial lung disease (ILD), liver metastasis, performance status (PS), pleural effusion
Citation: Nakagawa N and Kawakami M (2022) Choosing the optimal immunotherapeutic strategies for non-small cell lung cancer based on clinical factors. Front. Oncol. 12:952393. doi: 10.3389/fonc.2022.952393
Received: 25 May 2022; Accepted: 04 July 2022;
Published: 12 August 2022.
Edited by:
Jun Zhang, University of Kansas Medical Center, United StatesReviewed by:
Jan Trøst Jørgensen, Dx-Rx Institute, DenmarkCopyright © 2022 Nakagawa and Kawakami. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Masanori Kawakami, bWFrYXdha2FtaS10a3lAdW1pbi5hYy5qcA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.