 Guo-qian He1,2
Guo-qian He1,2 Ling Xiao3Zhen Pan3Jian-rong Wu1,2Dong-ni Liang1,4
Ling Xiao3Zhen Pan3Jian-rong Wu1,2Dong-ni Liang1,4 Xia Guo1,2Ming-yan Jiang1,2*
Xia Guo1,2Ming-yan Jiang1,2* Ju Gao1,2
Ju Gao1,2- 1Key Laboratory of Birth Defects and Related Diseases of Women and Children, Ministry of Education, West China Second University Hospital, Sichuan University, Chengdu, China
- 2Department of Pediatrics, West China Second University Hospital, Sichuan University, Chengdu, China
- 3Sichuan University, Chengdu, China
- 4Department of Pathology, West China Second University Hospital, Sichuan University, Chengdu, China
Mucormycosis caused by Lichtheimia ramosa is an emerging and uncommon opportunistic infection in patients with hematological malignancies, with high mortality rates. Herein, we first report a case of pulmonary mucormycosis with Lichtheimia ramosa in a 3-year-old girl recently diagnosed with B-cell acute lymphoblastic leukemia. The diagnosis was made using computerized tomography of the lung, metagenomic next-generation sequencing (mNGS) of blood and sputum specimens, and microscopic examination to detect the development of Lichtheimia ramosa on the surgical specimen. She was effectively treated after receiving prompt treatment with amphotericin B and posaconazole, followed by aggressive surgical debridement. In our case, the fungal isolates were identified as Lichtheimia ramosa using mNGS, which assisted clinicians in quickly and accurately diagnosing and initiating early intensive treatment. This case also indicated the importance of strong clinical suspicion, as well as aggressive antifungal therapy combined with surgical debridement of affected tissues.
Introduction
Mucormycosis is the third most prevalent invasive fungal disease (IFD) caused by Mucoraceae, which is widespread in the environment (1–3). It usually acts as an opportunistic pathogen, mostly in immunocompromised patients, and is aggressive with high mortality and morbidity rates (1, 4, 5). IFD is more common in patients with acute myeloid leukemia than in those with acute lymphoblastic leukemia (ALL). However, a recent study had shown that despite the recent breathtaking development of antifungal drugs, patients of ALL with prolonged neutropenia were also associated with a higher risk of acquiring IFD (6, 7).
Mucoraceae are classified into filamentous fungi. Lichtheimia ramosa, formerly known as Absidia idahoensis, belongs to the order of Mucorales and is currently regarded as an emerging pathogen (8–11). Mucormycosis caused by Lichtheimia species has increased from 5% to more than 19% in the last decade, and it is associated with dissemination and life-threatening complications (12–14). Cases have been reported in patients with diabetes, severe burns, chronic granulomatous disease, and acute myeloid leukemia (AML). The infections often develop rapidly and can potentially be angioinvasive, predominantly with pulmonary manifestations (13, 15). However, the early symptoms are unusual, and traditional etiological detection methods are ineffective. Clinically, most Lichtheimia infections were treated empirically with no definite diagnosis (16, 17). Early diagnosis and treatment can result in a better prognosis (4).
Here, we first report a case of lung mucormycosis in a child following induction chemotherapy for B-cell ALL. This is the first known published case of a child surviving pulmonary mucormycosis caused by Lichtheimia ramosa after prompt antifungal medication and aggressive surgical treatment.
Case description
A 3-year-old girl was admitted to West China Second University Hospital who presented with fever and a pale appearance and diagnosed with early precursor B-cell ALL with ETV6-RUNX1 fusion after MICM (morphology, immunology, cytogenetics, and molecular biology) classification. No chromosomal abnormality was detected. Before chemotherapy, the brain and chest computed tomography (CT) scan showed a negative result (Figures 1A, B). The patient was stratified into the low-risk group and successfully treated with induction therapy using the Chinese Children Cancer Group 2020 (CCCG-ALL-2020) protocol. It consisted of dexamethasone (6 mg/m2 per day, 4 days), prednisone (45 mg/m2 per day, 24 days), vincristine, daunorubicin, pegaspargase, and intrathecal injection of cytarabine, methotrexate (MTX), and dexamethasone (triple IT) in our hospital. The bone marrow response on day 19 (calculated from the start of chemotherapy) was evaluated using bone marrow aspiration and minimal residual disease (MRD). The bone marrow smear suggested complete remission, and the MRD was negative (<0.01%). ETV6-RUNX1 fusion gene was negative.
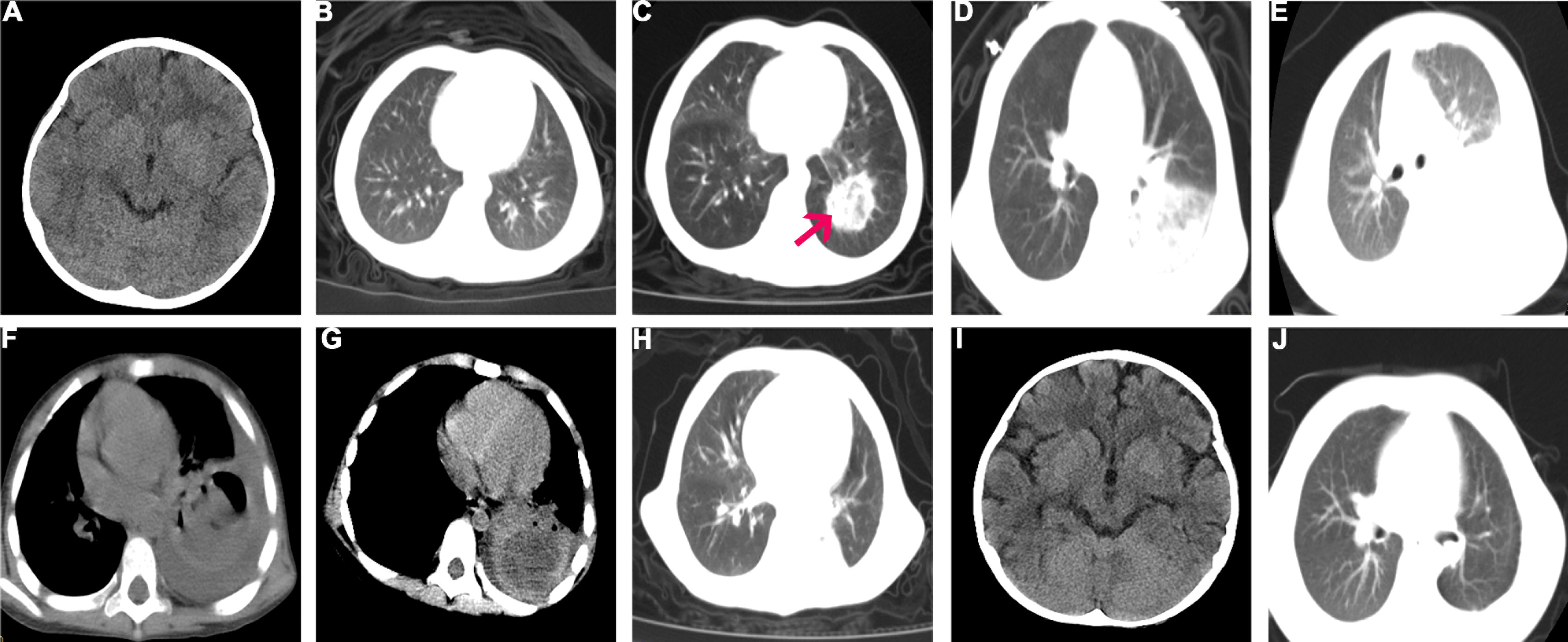
Figure 1 Brain and Chest CT before and after surgery. (A) Brain CT before chemotherapy; (B) Chest CT before chemotherapy; (C) Day 30, a nodular lesion (3.2 cm × 2.8 cm, red arrow) in the post-basal segment of the left lower lobe with ground glass opacification; (D) Day 38, the initial nodular lesion was larger, and new lesion in the upper lobe of the right lung; (E, F). Day 52, the initial nodular lesion was 4.7 cm × 24.3 cm with part consolidation and the balloon cavity; the initial regional hazy shadow was spread diffusely in the left lung. (G) No regression of lesions and fungal flora in blood vessel on CTA (I) Brain CT on 6 months after surgery; (J) Chest CT on 6 months after lung lobectomy, no progression of mucormycosis.
During the first course of induction chemotherapy, the patient experienced significant neutropenia for 21 days. On day 1, piperacillin sodium and tazobactam sodium were given as empiric antibiotics, and on day 14, micafungin (4 mg/kg daily, intravenously) was added as prophylaxis for antifungal therapy if neutropenia persisted. On day 23, she complained of oral pain. On presentation, her neutrophil count was 0.02 × 109/l with raised C-reactive protein (CRP) of 19.2 mg/l. Due to positive oral secretion cultures for Burkholderia polyphagy, the antibiotic therapy was switched to Tienam. On day 28, she complained of a fever (38.3°C), followed by a cough, dyspnea, and swelling of the face on day 30. Chemotherapy was discontinued. Results of the blood culture, serum galactomannan antigen (GM) test, and 1,3-β-D glucan test (G test) were negative. The patient was positive for rhinovirus in the throat swab and gram-positive coccus in the sputum smear. A blood count indicated that the patient had severe neutropenia (<0.05 × 109/l). Procalcitonin and serum CRP levels were 1.73 ng/ml and 176.3 mg/l, respectively. Chest CT showed a nodular lesion (3.2 cm × 2.8 cm) in the post-basal segment of the left lower lobe with ground glass opacification (Figure 1C). The CT scans of the abdomen, as well as the cerebrospinal fluid test, all showed normal results. However, the parents later refused for the patient to undergo head CT examination due to economic reasons. Given the possibility of an opportunistic pathogen infiltrating the fungi prophylaxis and causing pulmonary infection, the antifungal therapy was changed to voriconazole, added with vancomycin. However, the high fever and dyspnea persisted. On day 34, the CRP increased to 301.8 mg/l, and following positive evolution with metagenomic next-generation sequencing (mNGS) (identified by Hugo Biotech, China, free testing) in the genomic DNA of the blood and sputum specimen, Lichtheimia ramosa was detected. Meanwhile, mNGS identified gram-positive streptococcus in the sputum specimen but no pathogenic prokaryotic microorganisms or viruses in the blood specimen. mNGS in cerebrospinal fluid specimens was also performed to determine intracranial IFD, although the results were negative. Because the test results were consistent with the clinical manifestations, we adjusted the antifungal treatment regimen to amphotericin B (amphotericin B liposomes were not available) intravenously (the initial dose was 0.2 mg/kg and increased up to 1.5 mg/kg gradually within 4 days); the therapeutic dose was administered intravenously for 9 weeks. The antibiotic therapy was switched to linezolid combined with Tienam. Meanwhile, the renal function was monitored and found to be normal. She experienced transient hypokalemia (2.33 mmol/l, normal range 3.5–5.5 mmol/l), which was resolved with oral and intravenous potassium supplementation. On day 38, repeated CT showed a larger initial nodular lesion and a new lesion in the upper lobe of the right lung (Figure 1D). On day 44, the patient’s temperature was back to normal. On day 52, a repeat CT revealed that the initial nodular lesion had gotten larger (4.7 cm × 24.3 cm) with part consolidation and that the initial regional hazy shadow had disseminated diffusely in the left lung. New regional shadows were seen in the upper lobe of the right lung (Figures 1E, F). Computer tomography angiography (CTA) was conducted and demonstrated no fungal flora in the blood vessels (Figure 1G). A multidisciplinary team (MDT) met the recommended surgical treatment for the patient. Meanwhile, posaconazole was added (6 mg/kg oral q6h) combined with amphotericin B. The blood concentration of posaconazole was in the normal range. On day 66, surgical management involved the lower lobe of the left lung and pleura (Figure 1H). The yellow and white fungal lesions in the basal segment of the lower lobe of the left lung were observed during surgery. Irregular fungal balls (3.0 cm) and necrosis lesions were observed in the pulmonary alveoli. A microscopic examination revealed tissue necrosis (Figures 2A, B), fungal cenobium in the pulmonary alveoli (Figure 2C), and filamentous fungi in the removed pulmonary specimen (Figure 2D). It was positive for periodic acid Schiff (PAS) stain (Figure 2E) and Gomori methenamine silver stain (Figure 2F) but negative for acid-fast stain. On day 84, the patient started the second induction therapy with cyclophosphamide cytarabine and mercaptopurine. The chemotherapy was completed without the recurrence of the fungal infection. After every 3 months of follow-up, the patient was sequentially treated with posaconazole and was continuously in complete remission. There was no progression of mucormycosis in the chest CT (Figure 1J) on 6 months after surgery. Brain CT was conducted after active persuasion, and it showed a good image (Figure 1I). The clinical course and timeline of the treatment course are summarized in Figure 3 and Table 1.
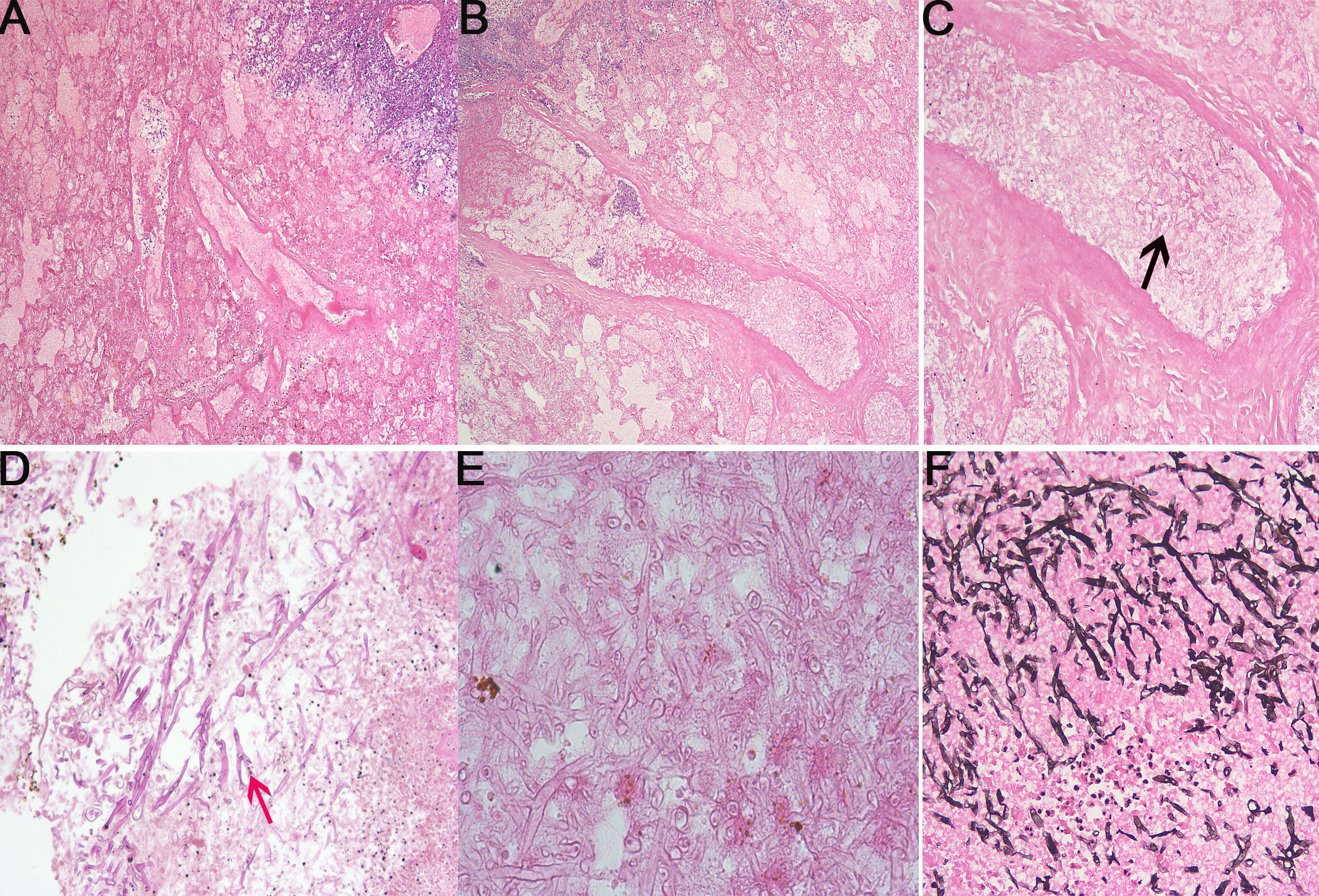
Figure 2 Microscopic examination of the removed lung. (A-D). The tissue specimens were stained with hematoxylin and eosin staining. (A) Tissue necrosis (×40). (B) Tissue necrosis (×200). (C) Fungal cenobium (black arrow) in the pulmonary alveoli (×200). (D) Filamentous fungi (red arrow) in the pulmonary (×100). (E) Filamentous fungi stained by PAS (×200). (F) Gomori methenamine silver stain of a fungal cenobium (Grocott, ×200).
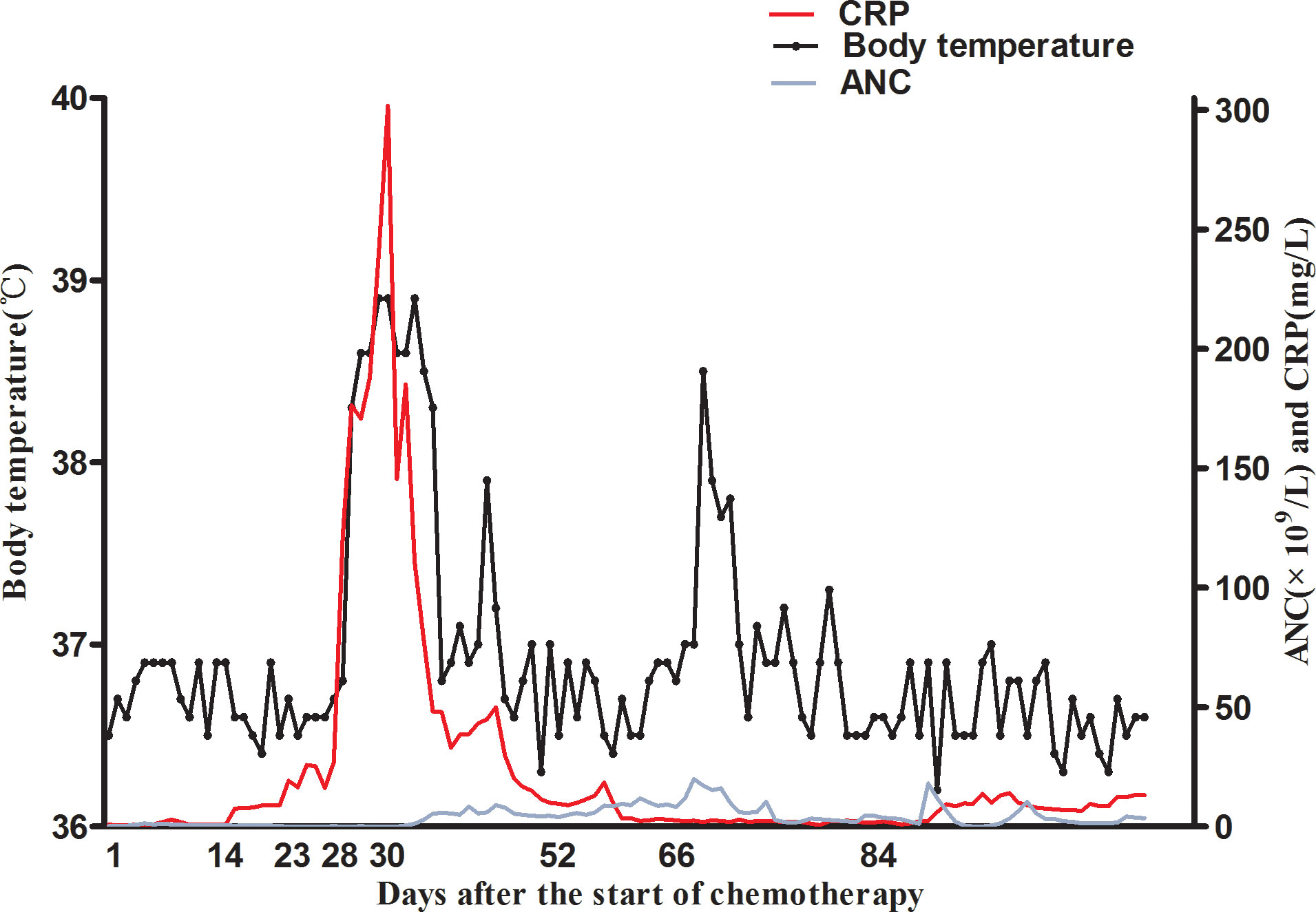
Figure 3 The clinical course of the patient. The patient had fever on day 28 and persistent fever for several days. Fever subsided after amphotericin B and posaconazole treatment. The ANC and CRP data were also obtained. The temperature was gradually increased on day 23 and peaked on day 34. A blood count revealed persistence of neutropenia and severe neutropenia on day 30. On day 66, surgical management was performed. On day 84, the patient started the second induction therapy.
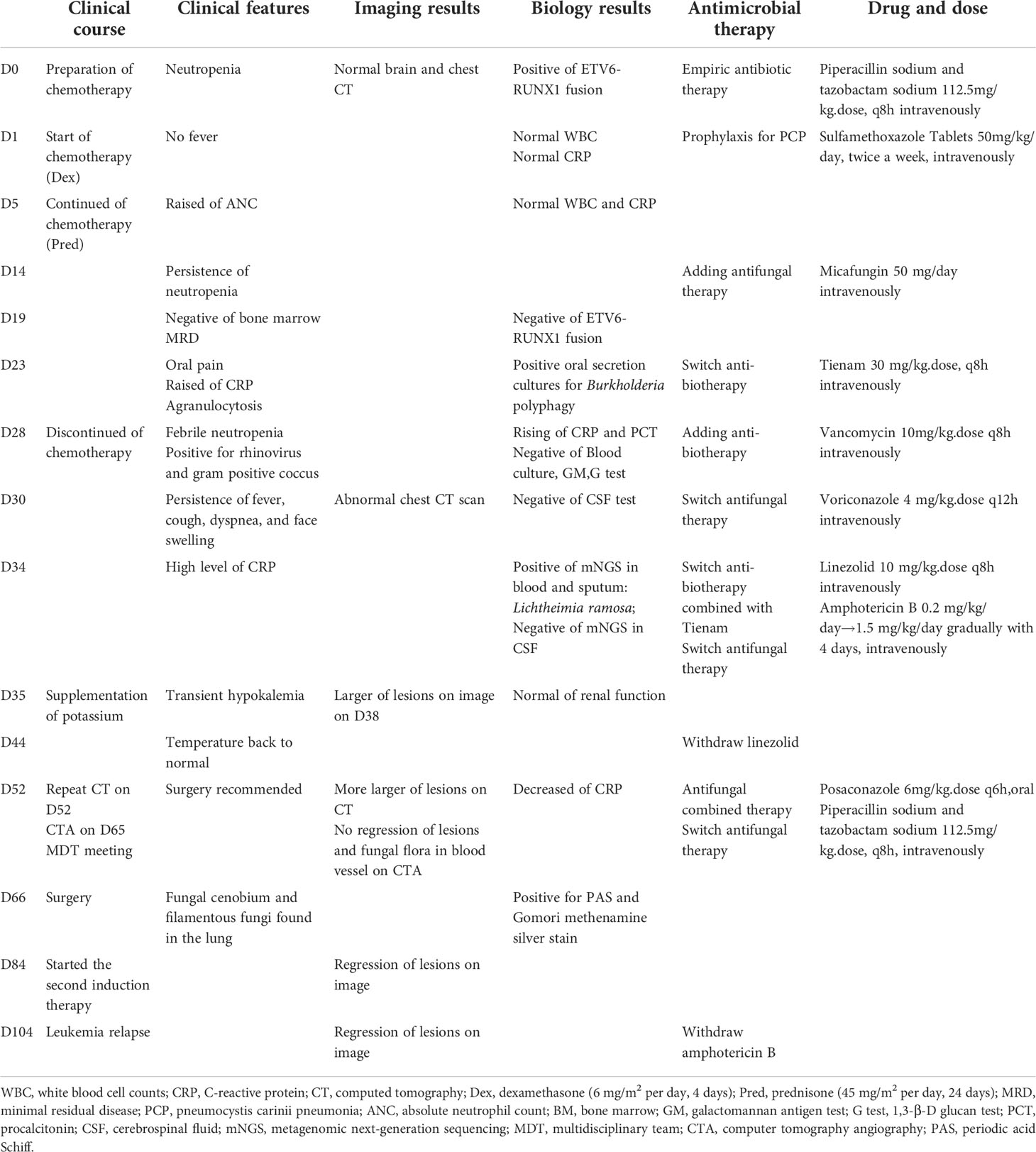
Table 1 Timeline of events.
Discussion and review of the literature
Mucormycosis is an opportunistic invasive fungal infection caused by Mucoralean and zygomycetes fungus, like the Lichtheimia species. This fungus is found almost ubiquitously in soil, farming products, and processed and unprocessed food products (12, 18). Despite being classified as a low-virulence pathogen, the percentage of Mucor infections caused by Lichtheimia species has increased from 5% to more than 19% in the last decade, according to recent reviews (13, 19). Lichtheimia ramosa is the most common pathogenic Lichtheimia species and a leading cause of mucormycosis (15). The clinical disease resembles infections with other mucoralean fungi. The pulmonary is the most common organ infected by Lichtheimia ramosa. Cutaneous and subcutaneous were also observed in some cases (18). Most patients with serious mucormycosis underlying diseases, such as hematological malignancies, are predominantly at risk (1). Classically, the risk of mucormycosis has been considered higher in AML and HSCT than in ALL (20–22). In this study, reports about Lichtheimia ramosa mucormycosis in leukemia published in literature were reviewed. Here, we performed a detailed review of Lichtheimia ramosa-induced mucormycosis events in leukemia based on available case reports (Table 2). For the cases reviewed, there have been rare reports of Lichtheimia ramosa infection in leukemia (23–25). The three cases were all reported with AML, with one case including an adult patient’s skin mucormycosis. The other child with AML had pulmonary and cerebral mucormycosis caused by Lichtheimia ramosa. However, the episode was rare in ALL for the patient infected with Lichtheimia ramosa. This is the first reported case of pediatric ALL in our study. Risk factors are indeed a matter of great concern to us. A thorough search for risk factors can aid in the reduction of opportunistic infections and improve patient prognosis. In the case of our patient, it would be reasonable to suppose that the infection occurrence was related to immunocompromised status induced by hematological malignancies; the ETV6-RUNX1 gene is a marker of good prognosis for ALL. However, clinical studies have shown that ALL patients carrying this gene are more susceptible to severe opportunistic infections, which may be associated with high susceptibility to chemotherapy, resulting in long-term severe granulocytosis. For this patient, in addition to the above risk factors, living near garbage sites, vegetable markets, and flower shops as well as poor sanitation may increase the risk of fungal infection. At the same time, long-term poor appetite and poor nutritional status may increase the risk of infection due to malnutrition and primary or secondary endocrine disorders, such as diabetes. Normal blood glucose levels were monitored, as was her nutrition level. During the diagnosis and treatment of the patient, blood glucose and urine glucose levels were monitored regularly. Strengthening nutritional support is beneficial for improving the prognosis.
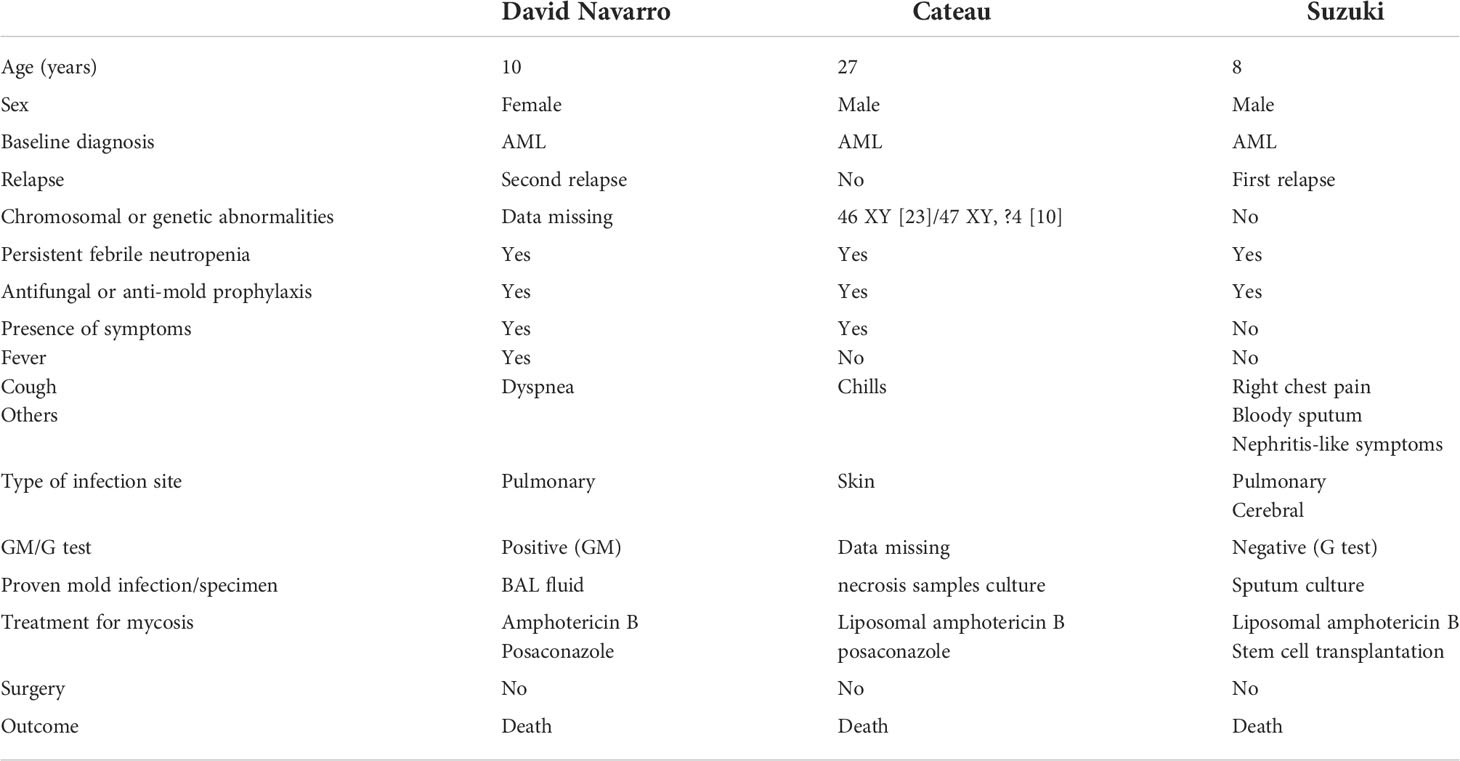
Table 2 Lichtheimia ramosa-related mucormycosis based on available case reports.
Early detection is critical for avoiding the aggressive clinical course and improving prognosis. The diagnosis is based on a combination of clinical examinations and histopathologic and radiological investigations. A biopsy and cultures on standard mycological media are typically required for a definitive diagnosis (26, 27). With the progression of the disease, persistent fever and respiratory system symptom may occur. While the early symptoms are not typical, they cannot be distinguished from other infective causes from other pathogens. Although CT data may be suggestive, they are frequently non-specific (27–29). As recommended by the ECIL guidelines, we also wanted to screen for intracranial infection, including the possibility of endocardial infection. In fact, we recommend that cranial imaging be as complete as possible, even if the patient does not have neurological signs and symptoms. Additionally, proper tissue sampling was performed mostly after a delay for the fungal detection. Microscopically, rhizoids are rarely observed on Lichtheimia strains. Bronchoalveolar lavage fluid (BAL fluid) and sputum cultures are clinically much feasible and safer than tissue biopsy (13, 30). Diagnosis of mucormycosis is often missed or delayed. In our case, the parents refused BALF due to risk. It is difficult to detect Lichtheimia ramosa using traditional etiological detection methods. Definitive identification requires molecular methods. mNGS is a rapid and non-invasive diagnostic method. Using mNGS as soon as possible is recommended when an infection with a rare pathogen is suspected, especially in immunocompromised individuals who need emergency treatment (31, 32). Early clinical trials of patients with meningitis or encephalitis, invasive fungal infections, community-acquired pneumonia, and other clinical indications revealed the potential of direct-from-specimen mNGS in enabling a difficult infection diagnosis. However, in published studies, the proportion of patient cases having a positive clinical impact as a result of mNGS testing is low, and the expense of testing is high, emphasizing the importance of improving our understanding of “when to test” and for which patients mNGS testing is appropriate (33–36). In our case, we used mNGS for detecting this rare species. It enabled us to effectively treat this child patient with lung mycosis caused by a Lichtheimia ramosa infection.
According to our literature review, the empiric antifungal treatment of Lichtheimia ramosa mucormycosis is amphotericin B and posaconazole. Lichtheimia is usually sensitive to amphotericin B and posaconazole. Amphotericin B is the most active drug against Lichtheimia species and is the only antifungal agent recommended in pediatric mucormycosis (37–39). Liposomal amphotericin B (LAmB) is a standard of care for a wide range of medically important opportunistic fungal pathogens. LAmB has a significantly improved toxicity profile compared with conventional amphotericin B. However, the adverse effects and especially nephrotoxicity of amphotericin B, even with the liposomal formulation, could be problematic. Moreover, amphotericin B liposomes were not available in the region of China, so we had to choose conventional amphotericin B and tried to exclude the intracranial fungal infection. However, it also has many side effects, which even causes the suspension of antifungal therapy. According to our experience, it usually causes severe vomiting and electrolyte disorder to start with the therapeutic dose on day 1, so we tried to increase the dose gradually. As we hoped, the intolerance of the patient was good. Her renal function was persistently normal, and she suffered transient mild hypokalemia only.
Posaconazole, possibly the recommended oral therapy, can be used to complement or substitute amphotericin B therapy (3, 40–42). However, there is no intravenous therapy, and it is not easy to monitor the blood drug concentration. The effectiveness of posaconazole is still controversial (43). It has been reported that voriconazole has no activity against Lichtheimia ramosa. Isavuconazole has been approved for adults as first-line therapy if amphotericin B treatment is not appropriate (21, 44). Isavuconazole has rarely been reported to be used in children with mucormycosis (45). As recommended by the guidelines, appropriate use of antifungal agents includes dosage, route of administration, and monitoring of blood concentration. We do want to monitor posaconazole blood concentrations, and we want to use an intravenous preparation when amphotericin B is combined with posaconazole during the patient’s hospital stay. However, due to the limited conditions, posaconazole intravenous preparations could not be obtained at that time, nor could blood drug concentration monitoring TDM be done. That is something we need to work on. It is also recommended that blood concentrations (effective therapeutic concentration) be monitored as much as possible. It has been reported that echinocandin (micafungin and caspofungin) in combination with amphotericin B also has a certain effect (42). Mucormycosis is treated with a combination of antifungal medications and surgical debridement of affected tissues. Surgery has been demonstrated to improve patient survival (43). Moreover, a combination strategy of intravenous inhalation and local inhalation and direct airway perfusion of amphotericin B may be an effective strategy for the treatment of pulmonary mucormycosis (46, 47). In our case, intravenous liposomal amphotericin B was started just after appearance of suspicious clinical presentation and radiological findings supporting mucormycosis. The patient was then given posaconazole in conjunction with amphotericin B, as well as prompt surgical debridement. Lichtheimia ramosa has characteristics comparable to invasive aspergillosis, including the potential for angioinvasion and dissemination (1, 48). Extensive angioinvasion results in tissue necrosis (49). Pulmonary hemorrhage, hemoptysis, asphyxia, and intracranial infection should be watched out for during diagnosis and treatment. Fortunately, the patient had no pulmonary hemorrhage and no abnormal cranial imaging and CSF findings. If IFD is diagnosed, antifungal treatment should be started immediately, and chemotherapy should be postponed until the IFD is under control, except in rare cases needing prompt anti-leukemic intervention. During the treatment, renal work and electrolyte (low potassium) were closely monitored (24). In this case, renal function was normal. She had transient hypokalemia, improved by oral and intravenous potassium supplementation and improved diet. In addition, the prompt recovery of chemotherapy-induced neutropenia is also necessary. Fortunately, the child in this case had low-risk ALL with sustained CR in BM after experiencing induction remission therapy. Since the risk factors for infection in this patient are of concern, ALL with Lichtheimia ramosa infection is extremely rare. The patient received amphotericin B monotherapy for 5 weeks, amphotericin B+ posaconazole for 4 weeks, and then posaconazole monotherapy. The specific doses are shown in the attached table. She then had entered the maintain chemotherapy of the CCCG-ALL-2020 therapy for the low-risk group and stop using antifungal drugs. During long-term follow-up, blood routine test, CRP test, and CT were taken. The head and chest CT scans were all normal. The parents and children had good compliance and tolerance.
Conclusion
Here, we report a rare case of an infrequent fungal mycosis associated with the causal species (Lichtheimia ramosa) in a child ALL and review Lichtheimia ramosa-related mycosis based on published case reports. This report summarizes the difficulty of making an early diagnosis and the importance of considering mucormycosis in subjects developing fever unresponsive to other antimicrobials and have breathing difficulty. The timing of proper medical therapy with antifungal medications and early surgical resection is critical. mNGS is more effective when used early in the diagnostic process.
Data availability satement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Center for Ethics in the West China Second University Hospital of Sichuan University. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
GH: analyzed the patient data and drafted the manuscript. LX: provided significant contributions to the interpretation of CT and CTA imaging. ZP: made significant contributions to the collection of patient data. DL provided significant contributions to the analysis of pathological data. JW and XG provided significant contributions to the analysis of the patient data. MJ: designed the case report and revised the manuscript. JG: writing–review and editing. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Sichuan Science and Technology Program, grant no. 2021YFSY0040-LH and 2022YFS0236 (to GQH), and the Universal Application Project of Sichuan Provincial Health and Family Planning Commission of China, grant no. 18PJ032(to GQH).
Acknowledgments
Wei Jiang and Juan Zou provided selfless assistance with the analysis of pathological data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mouronte-Roibas C, Leiro-Fernandez V, Botana-Rial M, Ramos-Hernandez C, Lago-Preciado G, Fiano-Valverde C, et al. Lichtheimia ramosa: A fatal case of mucormycosis. Can Respir J (2016) 2016:2178218. doi: 10.1155/2016/2178218
2. Chander J, Kaur M, Singla N, Punia RPS, Singhal SK, Attri AK, et al. Mucormycosis: Battle with the deadly enemy over a five-year period in India. J Fungi (2018) 4(2):46. doi: 10.3390/jof4020046
3. Cornely OA, Alastruey-Izquierdo A, Arenz D, Chen SCA, Dannaoui E, Hochhegger B, et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European confederation of medical mycology in cooperation with the mycoses study group education and research consortium. Lancet Infect Dis (2019) 19(12):e405–e21. doi: 10.1016/S1473-3099(19)30312-3
4. Gumral R, Yildizoglu U, Saracli MA, Kaptan K, Tosun F, Yildiran ST. A case of rhinoorbital mucormycosis in a leukemic patient with a literature review from Turkey. Mycopathologia (2011) 172(5):397–405. doi: 10.1007/s11046-011-9449-z
5. Yano S, Minami J, Nishiwaki K, Shimada T, Dobashi N, Yahagi Y, et al. Rapid progression and unusual premortal diagnosis of mucormycosis in patients with hematologic malignancies: Analysis of eight patients. Int J Hematol (2011) 93(3):344–50. doi: 10.1007/s12185-011-0780-4
6. Grundahl M, Wacker B, Einsele H, Heinz WJ. Invasive fungal diseases in patients with new diagnosed acute lymphoblastic leukaemia. Mycoses (2020) 63(10):1101–6. doi: 10.1111/myc.13151
7. Oh SM, Byun JM, Chang E, Kang CK, Shin DY, Koh Y, et al. Incidence of invasive fungal infection in acute lymphoblastic and acute myelogenous leukemia in the era of antimold prophylaxis. Sci Rep (2021) 11(1):22160. doi: 10.1038/s41598-021-01716-2
8. Kaneko Y, Oinuma KI, Terachi T, Arimura Y, Niki M, Yamada K, et al. Successful treatment of intestinal mycosis caused by a simultaneous infection with lichtheimia ramosa and aspergillus calidoustus. Internal Med (2018) 57(16):2421–4. doi: 10.2169/internalmedicine.0254-17
9. Hassan MIA, Voigt K. Pathogenicity patterns of mucormycosis: Epidemiology, interaction with immune cells and virulence factors. Med Mycol (2019) 57(Supplement_2):S245–S56. doi: 10.1093/mmy/myz011
10. Hassan MIA, Keller M, Hillger M, Binder U, Reuter S, Herold K, et al. The impact of episporic modification of lichtheimia corymbifera on virulence and interaction with phagocytes. Comput Struct Biotechnol J (2021) 19:880–96. doi: 10.1016/j.csbj.2021.01.023
11. Linde J, Schwartze V, Binder U, Lass-Florl C, Voigt K, Horn F. De novo whole-genome sequence and genome annotation of lichtheimia ramosa. Genome Announcements (2014) 2(5):e00888–14. doi: 10.1128/genomeA.00888-14
12. Colman S, Giusiano G, Colman C, Sosa MLA, Rojas F. Hepatic failure and malnutrition as predisposing factors of cutaneous mucormycosis in a pediatric patient. Med Mycol Case Rep (2022) 35:26–9. doi: 10.1016/j.mmcr.2021.12.005
13. Zhang Q, Liu H, Qiu S, Wang W, Yang L, Chen H, et al. A rare case of pulmonary coinfection by lichtheimia ramosa and aspergillus fumigatus in a patient with delayed graft function after renal transplantation. Transplant Proc (2019) 51(2):551–5. doi: 10.1016/j.transproceed.2018.12.006
14. Skiada A, Pagano L, Groll A, Zimmerli S, Dupont B, Lagrou K, et al. Zygomycosis in Europe: Analysis of 230 cases accrued by the registry of the European confederation of medical mycology (Ecmm) working group on zygomycosis between 2005 and 2007. Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis (2011) 17(12):1859–67. doi: 10.1111/j.1469-0691.2010.03456.x
15. Geng C, Lv X, Li J, Jiang Q, Yang R, Zhan P. Chronic subcutaneous infection due to lichtheimia ramosa. J Eur Acad Dermatol Venereol JEADV (2019) 33(1):e26–e9. doi: 10.1111/jdv.15137
16. Guymer C, Khurana S, Suppiah R, Hennessey I, Cooper C. Successful treatment of disseminated mucormycosis in a neutropenic patient with T-cell acute lymphoblastic leukaemia. BMJ Case Rep (2013) 2013: bcr2013009577. doi: 10.1136/bcr-2013-009577
17. Pan J, Tsui C, Li M, Xiao K, de Hoog GS, Verweij PE, et al. First case of rhinocerebral mucormycosis caused by lichtheimia ornata, with a review of lichtheimia infections. Mycopathologia (2020) 185(3):555–67. doi: 10.1007/s11046-020-00451-y
18. Schwartze VU, Jacobsen ID. Mucormycoses caused by lichtheimia species. Mycoses (2014) 57 Suppl 3:73–8. doi: 10.1111/myc.12239
19. Kutlu M, Ergin C, Bir F, Hilmioglu-Polat S, Gumral R, Necan C, et al. Pulmonary mucormycosis due to lichtheimia ramosa in a patient with hiv infection. Mycopathologia (2014) 178(1-2):111–5. doi: 10.1007/s11046-014-9761-5
20. Lanternier F, Dannaoui E, Morizot G, Elie C, Garcia-Hermoso D, Huerre M, et al. A global analysis of mucormycosis in France: The retrozygo study (2005-2007). Clin Infect Dis Off Publ Infect Dis Soc America (2012) 54 Suppl 1:S35–43. doi: 10.1093/cid/cir880
21. Groll AH, Pana D, Lanternier F, Mesini A, Ammann RA, Averbuch D, et al. 8th European conference on infections in leukaemia: 2020 guidelines for the diagnosis, prevention, and treatment of invasive fungal diseases in paediatric patients with cancer or post-haematopoietic cell transplantation. Lancet Oncol (2021) 22(6):e254–e69. doi: 10.1016/S1470-2045(20)30723-3
22. Winstead M, Ozolek J, Nowalk A, Williams J, Vander Lugt M, Lin P. Disseminated lichtheimia ramosa infection after hematopoietic stem cell transplantation in a child with chronic granulomatous disease. Pediatr Infect Dis J (2017) 36(12):1222–4. doi: 10.1097/INF.0000000000001589
23. Cateau E, Randriamalala E, Elsendoorn A, Giot JP, du Sorbier CM, Rodier MH. Fatal-mixed cutaneous zygomycosis-aspergillosis: A case report. Mycopathologia (2013) 176(5-6):423–7. doi: 10.1007/s11046-013-9706-4
24. Suzuki D, Kobayashi R, Hori D, Kishimoto K, Sano H, Yasuda K, et al. Stem cell transplantation for acute myeloid leukemia with pulmonary and cerebral mucormycosis. Pediatr Int Off J Japan Pediatr Soc (2016) 58(7):569–72. doi: 10.1111/ped.12866
25. Borras R, Rosello P, Chilet M, Bravo D, de Lomas JG, Navarro D. Positive result of the aspergillus galactomannan antigen assay using bronchoalveolar lavage fluid from a patient with an invasive infection due to lichtheimia ramosa. J Clin Microbiol (2010) 48(8):3035–6. doi: 10.1128/JCM.00902-10
26. Nicolato A, Nouer SA, Garnica M, Portugal R, Maiolino A, Nucci M. Invasive fungal diseases in patients with acute lymphoid leukemia. Leukemia Lymphoma (2016) 57(9):2084–9. doi: 10.3109/10428194.2016.1154957
27. Kara IO, Tasova Y, Uguz A, Sahin B. Mucormycosis-associated fungal infections in patients with haematologic malignancies. Int J Clin Pract (2009) 63(1):134–9. doi: 10.1111/j.1742-1241.2006.01145.x
28. Ruhnke M, Behre G, Buchheidt D, Christopeit M, Hamprecht A, Heinz W, et al. Diagnosis of invasive fungal diseases in haematology and oncology: 2018 update of the recommendations of the infectious diseases working party of the German society for hematology and medical oncology (Agiho). Mycoses (2018) 61(11):796–813. doi: 10.1111/myc.12838
29. Heinz WJ, Buchheidt D, Christopeit M, von Lilienfeld-Toal M, Cornely OA, Einsele H, et al. Diagnosis and empirical treatment of fever of unknown origin (Fuo) in adult neutropenic patients: Guidelines of the infectious diseases working party (Agiho) of the German society of hematology and medical oncology (Dgho). Ann Hematol (2017) 96(11):1775–92. doi: 10.1007/s00277-017-3098-3
30. Kaur R, Bala K, Ahuja RB, Srivastav P, Bansal U. Primary cutaneous mucormycosis in a patient with burn wounds due to lichtheimia ramosa. Mycopathologia (2014) 178(3-4):291–5. doi: 10.1007/s11046-014-9805-x
31. Liu Y, Zhang J, Han B, Du L, Shi Z, Wang C, et al. Case report: Diagnostic value of metagenomics next generation sequencing in intracranial infection caused by mucor. Front Med (2021) 8:682758. doi: 10.3389/fmed.2021.682758
32. Qian YY, Wang HY, Zhou Y, Zhang HC, Zhu YM, Zhou X, et al. Improving pulmonary infection diagnosis with metagenomic next generation sequencing. Front Cell Infect Microbiol (2020) 10:567615. doi: 10.3389/fcimb.2020.567615
33. Simner PJ, Miller S, Carroll KC. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis Off Publ Infect Dis Soc America (2018) 66(5):778–88. doi: 10.1093/cid/cix881
34. Naccache SN, Federman S, Veeraraghavan N, Zaharia M, Lee D, Samayoa E, et al. A cloud-compatible bioinformatics pipeline for ultrarapid pathogen identification from next-generation sequencing of clinical samples. Genome Res (2014) 24(7):1180–92. doi: 10.1101/gr.171934.113
35. Filkins LM, Bryson AL, Miller SA, Mitchell SL. Navigating clinical utilization of direct-from-Specimen metagenomic pathogen detection: Clinical applications, limitations, and testing recommendations. Clin Chem (2020) 66(11):1381–95. doi: 10.1093/clinchem/hvaa183
36. Han SY. Clinical value of metagenomic next-generation sequencing in complicated infectious diseases. Zhongguo Dang Dai Er Ke Za Zhi Chin J Contemp Pediatr (2022) 24(2):210–5. doi: 10.7499/j.issn.1008-8830.2110064
37. Garcia-Hermoso D, Hoinard D, Gantier JC, Grenouillet F, Dromer F, Dannaoui E. Molecular and phenotypic evaluation of lichtheimia corymbifera (Formerly absidia corymbifera) complex isolates associated with human mucormycosis: Rehabilitation of l. Ramosa J Clin Microbiol (2009) 47(12):3862–70. doi: 10.1128/JCM.02094-08
38. Yang C, Xue B, Song W, Kan B, Zhang D, Yu H, et al. Reducing the toxicity of amphotericin b by encapsulation using methoxy Poly(Ethylene glycol)-B-Poly(L-Glutamic acid-Co-L-Phenylalanine). Biomater Sci (2018) 6(8):2189–96. doi: 10.1039/c8bm00506k
39. Cornely OA, Leguay T, Maertens J, Vehreschild M, Anagnostopoulos A, Castagnola C, et al. Randomized comparison of liposomal amphotericin b versus placebo to prevent invasive mycoses in acute lymphoblastic leukaemia. J Antimicrobial Chemother (2017) 72(8):2359–67. doi: 10.1093/jac/dkx133
40. Courtney R, Sansone A, Smith W, Marbury T, Statkevich P, Martinho M, et al. Posaconazole pharmacokinetics, safety, and tolerability in subjects with varying degrees of chronic renal disease. J Clin Pharmacol (2005) 45(2):185–92. doi: 10.1177/0091270004271402
41. Pagano L, Cornely OA, Busca A, Caira M, Cesaro S, Gasbarrino C, et al. Combined antifungal approach for the treatment of invasive mucormycosis in patients with hematologic diseases: A report from the seifem and fungiscope registries. Haematologica (2013) 98(10):e127–30. doi: 10.3324/haematol.2012.083063
42. Reed C, Bryant R, Ibrahim AS, Edwards J Jr., Filler SG, Goldberg R, et al. Combination polyene-caspofungin treatment of rhino-Orbital-Cerebral mucormycosis. Clin Infect Dis Off Publ Infect Dis Soc America (2008) 47(3):364–71. doi: 10.1086/589857
43. Vehreschild JJ, Birtel A, Vehreschild MJ, Liss B, Farowski F, Kochanek M, et al. Mucormycosis treated with posaconazole: Review of 96 case reports. Crit Rev Microbiol (2013) 39(3):310–24. doi: 10.3109/1040841X.2012.711741
44. Marty FM, Ostrosky-Zeichner L, Cornely OA, Mullane KM, Perfect JR, Thompson GR 3rd, et al. Isavuconazole treatment for mucormycosis: A single-arm open-label trial and case-control analysis. Lancet Infect Dis (2016) 16(7):828–37. doi: 10.1016/S1473-3099(16)00071-2
45. Cornu M, Bruno B, Loridant S, Navarin P, Francois N, Lanternier F, et al. Successful outcome of disseminated mucormycosis in a 3-Year-Old child suffering from acute leukaemia: The role of isavuconazole? a case report. BMC Pharmacol Toxicol (2018) 19(1):81. doi: 10.1186/s40360-018-0273-7
46. Chen L, Su Y, Xiong XZ. Rhizopus microsporus lung infection in an immunocompetent patient successfully treated with amphotericin b: A case report. World J Clin cases (2021) 9(35):11108–14. doi: 10.12998/wjcc.v9.i35.11108
47. Huang HD, Li Q, Huang Y, Bai C, Wu N, Wang Q, et al. Pseudomembranous necrotizing tracheobronchial aspergillosis: An analysis of 16 cases. Chin Med J (2012) 125(7):1236–41. doi: 10.3760/cma.j.issn.0366-6999.2012.07.009
48. Iwanaga M, Kamikawa A, Imai N, Shimada K, Degawa Y, Hanafusa Y, et al. Striatal necrosis caused by lichtheimia ramosa in a neonatal calf. J Veterinary Med Sci Japanese Soc Veterinary Sci (2021) 83(12):1943–7. doi: 10.1292/jvms.21-0499
Keywords: Lichtheimia ramosa, fungal infection, mucormycosis, acute lymphoblastic leukemia, child
Citation: He G-q, Xiao L, Pan Z, Wu J-r, Liang D-n, Guo X, Jiang M-y and Gao J (2022) Case report: A rare case of pulmonary mucormycosis caused by Lichtheimia ramosa in pediatric acute lymphoblastic leukemia and review of Lichtheimia infections in leukemia. Front. Oncol. 12:949910. doi: 10.3389/fonc.2022.949910
Received: 21 May 2022; Accepted: 22 July 2022;
Published: 15 August 2022.
Edited by:
Peter Bader, University Hospital Frankfurt, GermanyReviewed by:
Andreas Groll, University Hospital Muenster, GermanyHenriette Rudolph, University Hospital Frankfurt, Germany
Copyright © 2022 He, Xiao, Pan, Wu, Liang, Guo, Jiang and Gao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ming-yan Jiang, amlhbmdteTA5NDBAMTYzLmNvbQ==