
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol. , 05 July 2022
Sec. Surgical Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.947933
This article is part of the Research Topic Surgical Approaches for the Treatment of Glioma View all 7 articles
 Hugues Duffau1,2*
Hugues Duffau1,2*Early maximal surgical resection is the first treatment in diffuse low-grade glioma (DLGG), because the reduction of tumor volume delays malignant transformation and extends survival. Awake surgery with intraoperative mapping and behavioral monitoring enables to preserve quality of life (QoL). However, because of the infiltrative nature of DLGG, relapse is unavoidable, even after (supra)total resection. Therefore, besides chemotherapy and radiotherapy, the question of reoperation(s) is increasingly raised, especially because patients with DLGG usually enjoy a normal life with long-lasting projects. Here, the purpose is to review the literature in the emerging field of iterative surgeries in DLGG. First, long-term follow-up results showed that patients with DLGG who underwent multiple surgeries had an increased survival (above 17 years) with preservation of QoL. Second, the criteria guiding the decision to reoperate and defining the optimal timing are discussed, mainly based on the dynamic intercommunication between the glioma relapse (including its kinetics and pattern of regrowth) and the reactional cerebral reorganization—i.e., mechanisms underpinning reconfiguration within and across neural networks to enable functional compensation. Third, how to adapt medico-surgical strategy to this individual spatiotemporal brain tumor interplay is detailed, by considering the perpetual changes in connectome. These data support early reoperation in recurrent DLGG, before the onset of symptoms and before malignant transformation. Repeat awake resection(s) should be integrated in a global management including (neo)adjuvant medical treatments, to enhance long-lasting functional and oncological outcomes. The prediction of potential and limitation of neuroplasticity at each step of the disease must be improved to anticipate personalized multistage therapeutic attitudes.
Early and maximal surgical resection currently represents the first treatment in diffuse low-grade glioma (DLGG), because the reduction of tumor volume enables to delay malignant transformation (MT) and to significantly extend the overall survival (OS) (1–6). This is particularly true following supratotal resection (i.e., with the removal of a security margin beyond the Fluid Attenuated Inversion Recovery FLAIR hypersignal visible on preoperative Magnetic Resonance Imaging MRI), because most patients are still alive after long-term follow-up (FU) (7–9). Beyond oncological considerations, awake surgery with intraoperative electrical mapping of neural networks critical for brain functions combined with real-time monitoring of conation, language, cognition, and emotion resulted in the preservation of quality of life (QoL) (10–12) or even in its improvement, especially in case of preoperative epilepsy with seizure freedom following glioma removal (13, 14). Indeed, recent series with accurate postsurgical neurological and neuropsychological examination reported a severe permanent deficit at a rate of about zero and a preservation of neurocognitive functions in most patients (15–17), including after resection of incidental DLGG (18). Furthermore, over 94% of patients were able to resume professional activities, reflecting an actual return to real life following awake surgery in the vast majority of cases (15, 18–20). A perfect illustration of long-lasting project is the desire for motherhood in women with DLGG, mixing the complexity to make such a decision with a chronic brain tumoral disease and the risk of negative impact of pregnancy on glioma behavior (21): A complete resection before being pregnant resulted in a significant longer OS after delivery while maintaining QoL (22).
Despite such drastic improvements of long-term outcomes in DLGG due to an active surgical attitude, because of the invasive feature of this neoplasm, a recurrence is almost unavoidable, even after (supra)total resection (7). Thus, besides chemotherapy and radiotherapy, the question of possible reoperation(s) is increasingly raised, especially because patients with DLGG are usually young and would like to continue to make plans in the long run (23). Here, the purpose is to review the literature in the emerging field of iterative surgeries in recurrent DLGG, regarding the following issues: (i) Did multiple surgeries in DLGG improve life expectancy while sparing QoL? (ii) What are the factors supporting the decision to reoperate and helping to define the optimal timing for subsequent resection? (iii) How to adapt surgical techniques to the individual spatiotemporal brain tumor interplay, based on dynamic interactions between glioma regrowth and reactional neural networks reshaping?
Despite the paucity of original studies that investigated multiple surgeries in DLGG identified in this qualitative review, namely, 15 series with 630 patients reported between 2003 and 2022, these results support a positive impact of reoperation(s) on long-term oncological and functional outcomes (Table 1).
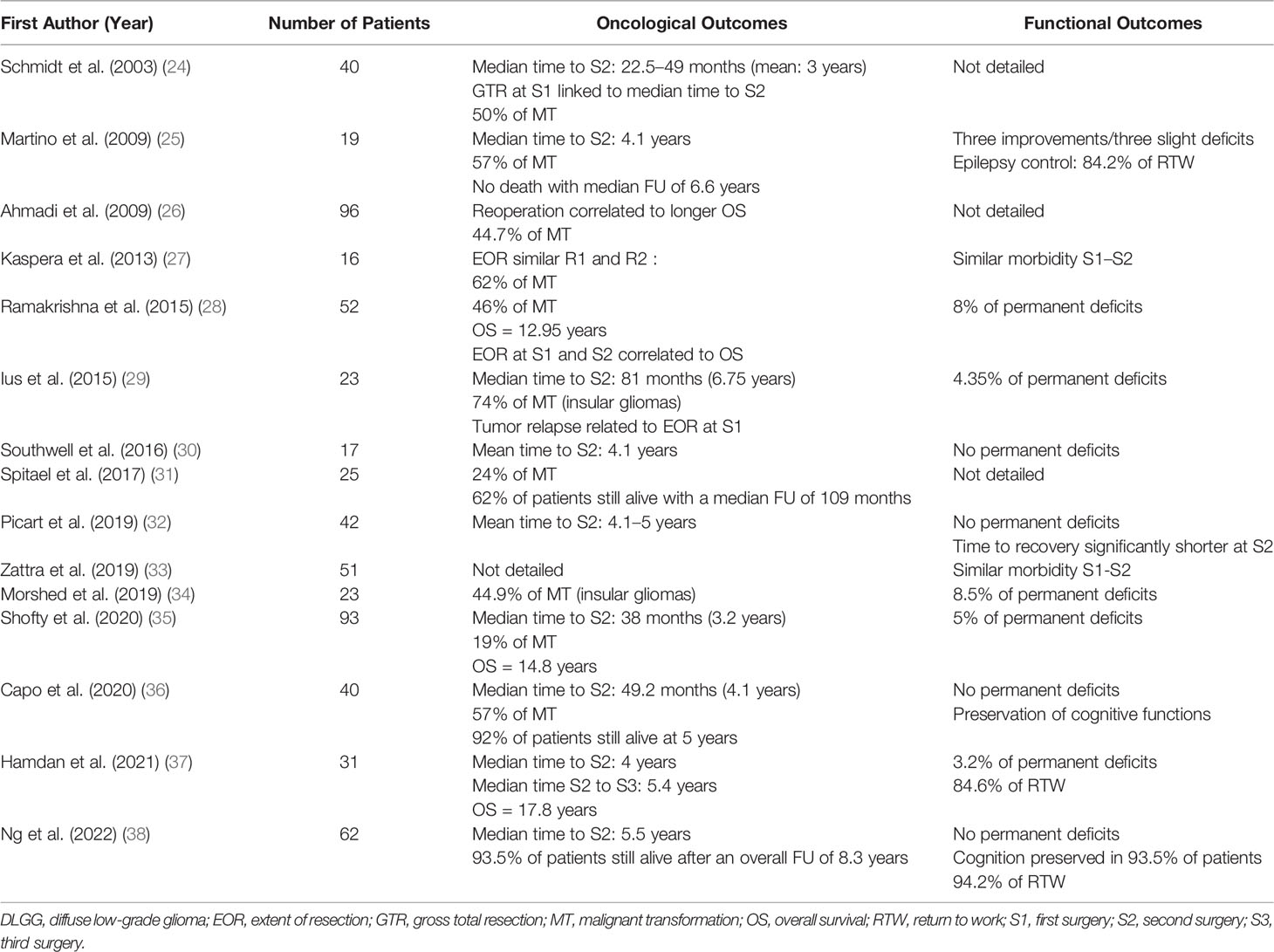
Table 1 Original series that reported outcomes following reoperation in patients with DLGG.
From an oncological perspective, the median survival was not yet reached at the last FU in several cohorts: no death with a median FU from initial diagnosis at 6.6 years in the study of Martino et al. (25); 62% of patients still alive following a median FU of 109 months in the study of Spitaels et al. (31); 92% of patients still alive at 5 years in the study of Capo et al. (36); and 93.5% still alive after an overall FU of 8.3 years in the study of Ng et al. (38). In studies with enough FU to report survival, the OS was 12.95 years in the study of Ramakrishna et al. (28) and 14.8 years in the study of Shofty et al. (35), namely, significantly longer in comparison with an OS of only 6.5 years in a control group of patients who experienced DLGG progression or transformation but who did not undergo a second surgery (p = 0.0001) (35). Similarly, Ahmadi et al. (26) reported a significantly prolonged OS in patients who had a second total resection in case of relapse without MT compared with patients who had a complete resection only once. Remarkably, in a recent consecutive series that detailed long-lasting outcomes after three iterative surgeries, an unprecedented median OS of 17.8 years has been reached (26).
Interestingly, OS is correlated to the extent of resection (EOR), because the presence of residual glioma at either the initial (p = 0.007) or second (p = 0.001) surgery was associated with significantly shorter OS (28). The EOR did not differ between initial surgery and reoperation, with a mean EOR from 72% to 94% and a mean tumor residual volume from 3.1 to 8.8 ml (27, 29, 34, 36–38). Therefore, the benefit of repeat operations on survival is likely related to the cytoreduction effect, capable to delay DLGG transformation, as already demonstrated after the first surgery (2). Indeed, in the study of Shofty et al. (35), the median time to transformation was significantly prolonged after reoperation (14.4 years) compared with a control group without the second surgery (3.5 years, p = 0.0002) (38). However, the rate of MT histologically confirmed at reoperation is high, i.e., in a range between 19% and 74% in the literature (24–26, 31, 35, 36, 39), with a lesser EOR (37) and a decreased OS when reoperation is performed after tumor transformation (28).
Interestingly, molecular subtypes were not associated with significant differences in malignant progression-free survival or in OS in several series (28, 37), whereas two other studies suggested that multiple surgeries delay tumor recurrence, MT, and prolong OS in DLGG, with a more significant impact in IDH-mutated gliomas (29, 35).
From a functional perspective, repeated surgery does not increase the risk of complications in comparison to the primary operation, by considering traumatic (related to the surgical manipulation), cerebrospinal fluid–related (leaks, hydrocephalus), septic, hemorrhagic, ischemic, epileptic, and general (non-neurological) factors (33, 40). In series specifically dedicated to DLGG, beyond the fact that no mortality was reported, all experiences supported the safety of multiple resections, with a low rate of permanent neurological impairment between 0% and 8.5%, similar to the morbidity rate of the first surgery (25, 26, 28–30, 32, 34–37). These favorable outcomes can be achieved with a high level of reproducibility regardless the DLGG location, including in challenging brain areas such as in eloquent sensorimotor and language structures (30, 32, 36) and in the insula (29, 34). Remarkably, these results were obtained because of the use of intraoperative electrical mapping in awake patients in most cohorts (25, 29, 30, 32, 34, 36–38).
Moreover, two recent series investigated cognitive outcomes by performing an extensive neuropsychological before and after repeat awake surgery in patients with DLGG (36, 38). Capo et al. (36) found a global preservation of the level of performance in 40 patients, despite changes in phonological fluency. Ng et al. (38) examined 62 patients, of which eight (12.9%) experienced a cognitive deficit before reoperation: 3 months following reoperation, four additional patients (6.5%) had a cognitive worsening, whereas eight (12.9%) patients improved in comparison with the preoperative status—the others were stable. Interestingly, the cognitive scores were not correlated to the EOR, knowing that the total or subtotal resections were performed in 91.9% of patients (mean EOR of 90.3%) (38). These findings support that multiple surgeries with awake mapping can be achieved with a large glioma removal and with an early recovery of neuropsychological abilities (38).
Multiple surgeries may even participate in improving QoL in patients who experienced more intense and/or frequent seizures at tumor relapse, by controlling epilepsy following reoperation (25). Another parameter critical for QoL is the capability to resume socio-professional activities. The rate of return to work was evaluated between 84.2% (25) and 94.2% (38) after the second surgery and at 84.6% after the third surgery (37), showing that the number of resections does not enhance the risk not to be able to resume an active life.
Thus, such data that show that iterative surgeries prolong OS while preserving QoL plead in favor of considering reoperation in a more systematic manner in DLGG (38, 41).
Despite infiltration of DLGG within the brain, reoperation(s) with optimization of the onco-functional balance can nonetheless be performed because of the mechanisms of neural reallocation elicited by the slow tumor progression over years (42, 43). An increase of both the gray matter volume and functional connectivity of the contralesional homologous areas was evidenced at diagnosis using non-invasive neuroimaging (44, 45). These insights into the individual pattern of structural and functional neuroplasticity are critical to tailor the therapeutic strategy, especially regarding surgical indication and planning (46). The principle is to achieve a connectome-guided surgery in awake patient, with intraoperative mapping enabling to adapt the resection according to the redistribution of the neural networks that occurred in the preoperative period (47). Postoperative cognitive rehabilitation is also able to generate further degrees of cerebral reorganization, allowing functional recovery after a transitory worsening that may occur immediately following resection (48). Furthermore, in case of DLGG reprogression, the brain will continue to reshape, as demonstrated by longitudinal functional neuroimaging investigations (49, 50).
Therefore, this additional neural redeployment opens the door to subsequent surgical resection(s), which can be based on the connectome modifications that had taken place since the initial operation (47). Indeed, when comparing results of the awake mapping performed during reoperation with those obtained during the first surgery, changes in the functional organization were detected (30, 32). Such a remapping has been made possible due to the slow kinetics of recurrent DLGG, as illustrated by the long delay between the initial and second surgery, i.e., with a mean interval between 3 to 6.75 years (24, 25, 29, 30, 32, 35–38). This neuroplastic potential explains why the EOR does not significantly differ between the first surgery and reoperation (27, 29, 34, 36, 37), or can even been greater with no additional neurological or neurocognitive deficit (38). It may also explain why the time needed to recover independence can be significantly shorter at reoperation than after the first surgery (32).
Remarkably, this reshaping process could be similar following a second surgery, namely, with the possibility for the brain to continue to adapt in case of new DLGG relapse: this may permit to achieve a third operation several years later (mean interval of 5.4 years) with a similar EOR while maintaining QoL due to additional mechanisms of functional reallocation that arose in the meantime, as evidenced by awake mapping (37).
This concept of multistage surgical approach may, nonetheless, have limitations related to the spatiotemporal pattern of DLGG relapse: The therapeutic management should be tailored accordingly (51, 52).
Regarding spatial considerations, recent atlases of neuroplasticity have evidenced that the main limitation of neural redistribution is represented by the subcortical connectivity (53–55). Therefore, if the recurrent DLGG after initial surgery exhibits a more migratory pattern, with a prominent diffusion along the white matter tracts, then the EOR has a high risk to be less at reoperation (32). Such a connectomal constraint plays a major role in the decision to reoperate (or not), because the plastic potential is low at the level of the axonal fibers (56)—conversely to a high plastic potential at the level of the cortex, thus pleading in favor of iterative surgeries for tumor relapse with a more bulky pattern and that mainly involves the cortical areas (32, 57).
Concerning the temporal considerations, because neuroplasticity is dependent on the time course of the lesion, i.e., with a higher potential of compensation in reaction to slow-growing tumor (43), in case of acceleration of the glioma kinetics due to MT, the EOR can be less if one would like to preserve QoL (37). Similarly, rapid reprogression following initial resection (less than 1 to 2 years) was correlated with a shorter time to MT and a decreased OS (35, 51). Thus, these findings suggest a window for treatment opportunity, i.e., to propose reoperation earlier in case of DLGG reprogression, before the tumor transformed in a higher grade of malignancy (25, 37). To this end, the occurrence of a hypermetabolic focus on a longitudinal multimodal imaging study (such as repeat MRI perfusion and spectroscopy and/or F-DOPA Positron Emission Tomography PET) (58) may represent an additional argument in favor of redo surgery, even in the absence of gadolinium enhancement. A “prophylactic” reoperation can especially be discussed in specific circumstances, for example, if a woman had a desire for motherhood after a partial surgical resection of DLGG—because of a higher risk of MT and death following pregnancy in case of incomplete tumor removal (22).
In addition to the considerable structural-functional variability across patients (57), the connectome is changing over time for each patient, based on constant glioma-brain dialogue (59, 60). This is particularly true at the level of the peritumoral zone, i.e., at the interface between the glioma core and the healthy brain, where intercommunication across tumoral cells and neural networks is maximal and where glioma relapse occurs most frequently (61). Cerebral circuits reconfiguration in reaction to the behavior of DLGG (pattern of proliferation versus migration, velocity diametric expansion) itself with constant modifications (spontaneously or consecutively to treatments) is possible, owing to the dynamics within and between networks in the framework of a meta-networking (network of networks) organization of brain processing (62). Surgical strategy should be adapted to this perpetual connectomal instability by detecting and preserving critical cortical hubs, often reallocated before (re)operation(s), as well as white matter tracts, because of direct electrostimulation (63). Because of frequent functional reshaping between the first and second surgery, or even between the second and third surgery, it is highly recommended to awake the patient to benefit not only from an accurate electrical mapping but also from an extensive cognitive and emotional monitoring performed in real time throughout the resection (12). With the aim of enhancing the sensitivity of such an actual neuropsychological evaluation into the operating theater, which should also take into consideration the spatial relationships between DLGG and surrounding eloquent pathways according to the tumor location (64, 65), the use of a multitasking protocol has been suggested, because it necessitates to recruit more neural circuits by increasing the cognitive demand—as a mirror of the meta-network (66). This protocol consists of a constant multitasking combining several tests performed simultaneously, during the transient presentation of a problem to solve on a computer screen while enabling to stimulate a specific cerebral structure in this time window, for example, movement combined with semantic association task while naming the pictures (66). Tasks should be selected on the basis of the expectations of the patient (e.g., monitoring of sensorimotor, language, visuospatial, executive, or behavioral functions), according to his/her familial, social, and professional activities as well as his/her environment (12). Nonetheless, in case of iterative surgeries, the patient’s wishes can change over years due to an evolution of the lifestyle. For example, at the time of the initial surgery, a 60-year-old patient may want to preserve a high level of executive functions because he/she is working full time, whereas at the time of reoperation several years later, the patient can be retired, with less requirement regarding higher-order cognition. In other words, the onco-functional balance should be reweighted at each moment with the ultimate aim to tailor a multistep medico-surgical management taking account of complex interactions between changes in patients’ needs, functional connectome, and DLGG course (67) (Figure 1).
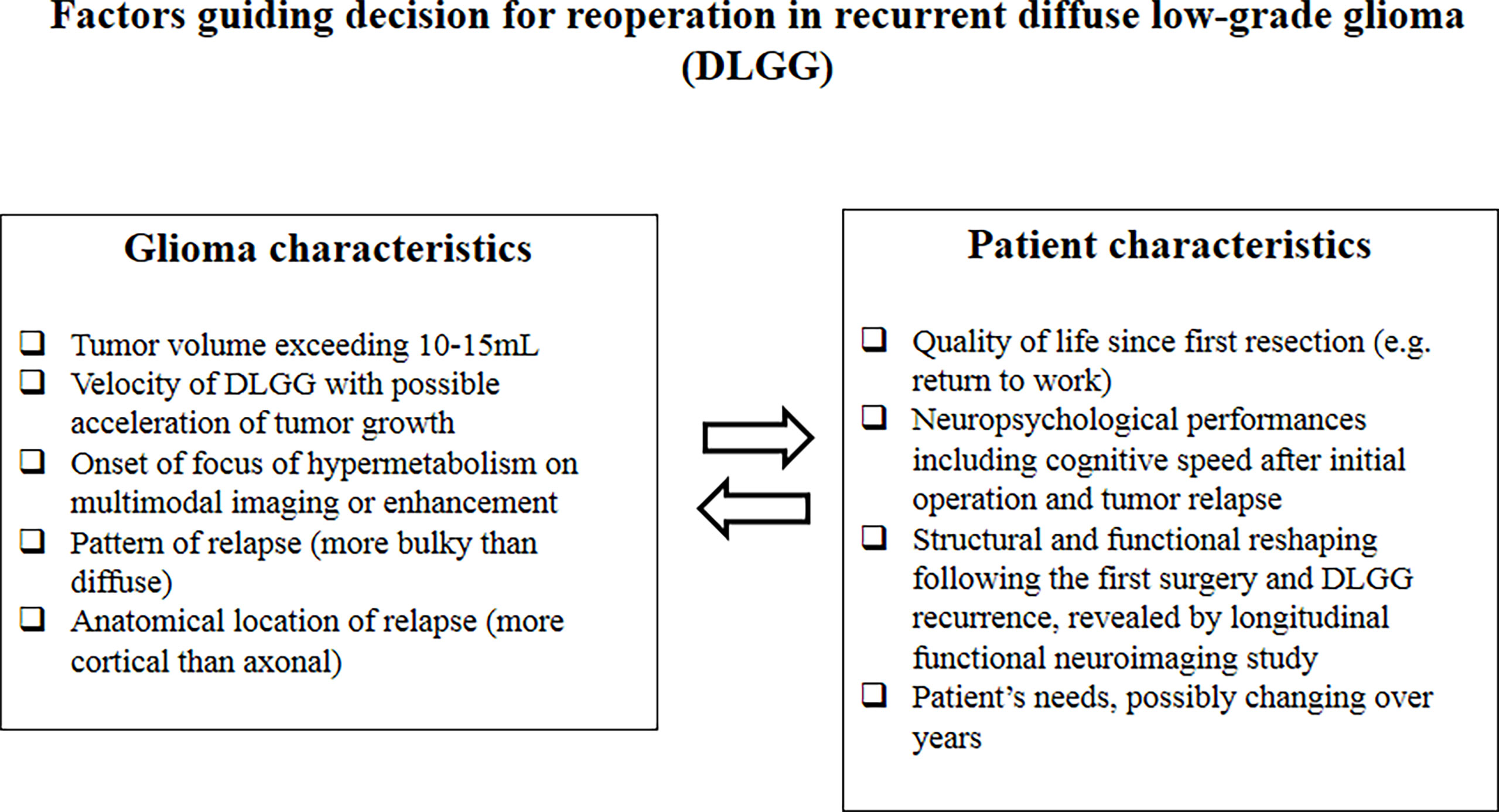
Figure 1 Factors guiding decision for reoperation in recurrent diffuse low-grade glioma (DLGG).
Repeat operations must be integrated in a more global multimodal therapeutic attitude, which also comprises chemotherapy and radiotherapy. In case of rapid postoperative DLGG reprogression, early reoperation should be considered if functionally feasible, with adjuvant treatment to be performed immediately after the last surgery. Conversely, if the regrowth is slow after the initial resection, then postponing adjuvant therapies can be proposed, especially concerning radiotherapy (67). Indeed, irradiation of the white matter tracts has a risk to generate delayed cognitive deteriorations (68, 69). Moreover, radiotherapy-induced alterations in the brain microenvironment also contribute to recurrent glioma aggressiveness (70). Therefore, in the event of a slow DLGG reprogression following the first surgery, particularly in case of large resection, a simple surveillance may be considered on the basis of regular MRI control with volumetric measurement and calculation of growth rate (23, 71)—including in DLGG with foci of MT in the middle of the tumor (72). However, although reoperation should be preferred at recurrence, when the DLGG relapse exhibits a more migratory pattern along the white matter tracts, because EOR has a high risk to be less (32), chemotherapy may be discussed (67). Beyond the fact that global QoL is usually preserved (73), chemotherapy may induce a tumor shrinkage with a lesser degree of infiltration of the subcortical fibers, then reopening the window to a reoperation with improvement of the EOR (74, 75). The same principle can be applied after a second or even a third surgery, allowing to reach an OS close to 18 years (37).
Finally, although histo-molecular aspects must also be incorporated in this complex equation for managing DLGG recurrence (76), they represent only a part of the story (77), in addition to the functional and radiological parameters (67)—especially taking account of modifications of the genetic profile which may arise at DLGG relapse. Indeed, although IDH1mutation represents the earliest genetic alteration in DLGG, longitudinal analyses at recurrence found a high mutational potential, especially with possible clonal expansion and epigenetic reprogramming after deletion or amplification of mutant IDH1 (78). These preliminary data show that multiple operation(s) may represent a unique opportunity to better investigate the spatiotemporal heterogeneity of DLGG.
As previously reported in high-grade glioma (79, 80), repeat surgery represents a safe and efficient therapeutic approach to enhance OS while preserving QoL in patients with DLGG. Favorable outcomes described in the recent literature support the proposal of early “preventive” reoperation in recurrent DLGG, before the onset of symptoms (e.g., seizures and cognitive or behavioral changes) and before MT.
These findings, however, may be limited by an intrinsic bias, namely, the patient selection, because by definition, reoperation was considered only when functionally feasible. Therefore, the next step would be to increase the number of surgical indications. To this end, a better prediction of the neuroplasticity reserve at every moment for each patient, based on an improved understanding of the perpetual interactions between the neural circuitry and the glioma course, would result in an optimization of the multistage and multimodal personalized management due to the anticipation of the next treatment(s) before DLGG transformation and/or onset of functional worsening. Integrating the concept of meta-plasticity (plasticity of the synaptic plasticity), i.e., a higher-order plastic phenomenon that regulates the learning rule as a function of the dynamical context (81), may help to reorient the spatiotemporal pattern of network reconfiguration (67). The principle would be to redirect the mechanisms of brain reshaping to generate a shift from a prior pattern with prominent perilesional recruitment (thus preventing to increase the EOR at the periphery of the previous surgical cavity) to a pattern predominantly recruiting remote circuits—ideally relying on contralateral homotopic structures (82). In this spirit, the concept of neuromodulation-induced cortical reallocation by using non-invasive transcranial stimulation tools starts to be developed, both for postoperative neurorehabilitation and for prehabilitation before (re)operation (83–85).
The author confirms being the sole contributor of this work and has approved it for publication.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Smith JS, Chang EF, Lamborn KR, Chang SM, Prados MD, Cha S, et al. Role of Extent of Resection in the Long-Term Outcome of Low-Grade Hemispheric Gliomas. J Clin Oncol (2008) 26(8):1338–45. doi: 10.1200/JCO.2007.13.9337
2. Chaichana KL, McGirt MJ, Laterra J, Olivi A, Quiñones-Hinojosa A. Recurrence and Malignant Degeneration After Resection of Adult Hemispheric Low-Grade Gliomas. J Neurosurg (2010) 112(1):10–7. doi: 10.3171/2008.10.JNS08608
3. Capelle L, Fontaine D, Mandonnet E, Taillandier L, Golmard JL, Bauchet L, et al. Spontaneous and Therapeutic Prognostic Factors in Adult Hemispheric World Health Organization Grade II Gliomas: A Series of 1097 Cases. J Neurosurg (2013) 118(6):1157–68. doi: 10.3171/2013.1.JNS121
4. Jakola AS, Skjulsvik AJ, Myrmel KS, Sjåvik K, Unsgård G, Torp SH, et al. Surgical Resection Versus Watchful Waiting in Low-Grade Gliomas. Ann Oncol (2017) 28(8):1942–8. doi: 10.1093/annonc/mdx230
5. Roelz R, Strohmaier D, Jabbarli R, Kraeutle R, Egger K, Coenen VA, et al. Residual Tumor Volume as Best Outcome Predictor in Low Grade Glioma - A Nine-Years Near-Randomized Survey of Surgery vs. Biopsy. Sci Rep (2016) 6:32286. doi: 10.1038/srep32286
6. Ius T, Isola M, Budai R, Pauletto G, Tomasino B, Fadiga L, et al. Low-Grade Glioma Surgery in Eloquent Areas: Volumetric Analysis of Extent of Resection and its Impact on Overall Survival. A Single-Institution Experience in 190 Patients. J Neurosurg (2012) 117(6):1039–52. doi: 10.3171/2012.8.JNS12393
7. Duffau H. Long-Term Outcomes After Supratotal Resection of Diffuse Low-Grade Gliomas: A Consecutive Series With 11-Year Follow-Up. Acta Neurochir (Wien) (2016) 158(1):51–8. doi: 10.1007/s00701-015-2621-3
8. Rossi M, Gay L, Ambrogi F, Conti Nibali M, Sciortino T, Puglisi G, et al. Association of Supratotal Resection With Progression-Free Survival, Malignant Transformation, and Overall Survival in Lower-Grade Gliomas. Neuro Oncol (2021) 23(5):812–26. doi: 10.1093/neuonc/noaa225
9. Motomura K, Ohka F, Aoki K, Saito R. Supratotal Resection of Gliomas With Awake Brain Mapping: Maximal Tumor Resection Preserving Motor, Language, and Neurocognitive Functions. Front Neurol (2022) 12(13):874826. doi: 10.3389/fneur.2022.874826
10. Bu LH, Zhang J, Lu JF, Wu JS. Glioma Surgery With Awake Language Mapping Versus Generalized Anesthesia: A Systematic Review. Neurosurg Rev (2021) 44(4):1997–2011. doi: 10.1007/s10143-020-01418-9
11. Zigiotto L, Annicchiarico L, Corsini F, Vitali L, Falchi R, Dalpiaz C, et al. Effects of Supra-Total Resection in Neurocognitive and Oncological Outcome of High-Grade Gliomas Comparing Asleep and Awake Surgery. J Neurooncol (2020) 148(1):97–108. doi: 10.1007/s11060-020-03494-9
12. Duffau H. New Philosophy, Clinical Pearls, and Methods for Intraoperative Cognition Mapping and Monitoring "a La Carte" in Brain Tumor Patients. Neurosurgery (2021) 88(5):919–30. doi: 10.1093/neuros/nyaa363
13. Zanello M, Roux A, Zah-Bi G, Trancart B, Parraga E, Edjlali M, et al. Predictors of Early Postoperative Epileptic Seizures After Awake Surgery in Supratentorial Diffuse Gliomas. J Neurosurg (2020) 134(3):683–92. doi: 10.3171/2020.1.JNS192774
14. Reitz SC, Behrens M, Lortz I, Conradi N, Rauch M, Filipski K, et al. Neurocognitive Outcome and Seizure Freedom After Awake Surgery of Gliomas. Front Oncol (2022) 12:815733. doi: 10.3389/fonc.2022.815733
15. Lemaitre A, Herbet G, Ng S, Moritz-gasser S, Duffau H. Cognitive Preservation Following Awake Mapping-Based Neurosurgery for Low-Grade Gliomas: A Longitudinal, Within-Patient Design Study. Neuro Oncol (2022) 24(5):781–93. doi: 10.1093/neuonc/noab275
16. Rossi M, Ambrogi F, Gay L, Gallucci M, Conti Nibali M, Leonetti A, et al. Is Supratotal Resection Achievable in Low-Grade Gliomas? Feasibility, Putative Factors, Safety, and Functional Outcome. J Neurosurg (2019) 132(6):1692–705. doi: 10.3171/2019.2.JNS183408
17. Campanella F, Palese A, Del Missier F, Moreale R, Ius T, Shallice T, et al. Long-Term Cognitive Functioning and Psychological Well-Being in Surgically Treated Patients With Low-Grade Glioma. World Neurosurg (2017) 103:799–808.e9. doi: 10.1016/j.wneu.2017.04.006
18. Ng S, Herbet G, Lemaitre AL, Cochereau J, Moritz-Gasser S, Duffau H. Neuropsychological Assessments Before and After Awake Surgery for Incidental Low-Grade Gliomas. J Neurosurg (2021) 135:871–80. doi: 10.3171/2020.7.JNS201507
19. Ng S, Herbet G, Moritz-Gasser S, Duffau H. Return to Work Following Surgery for Incidental Diffuse Low-Grade Glioma: A Prospective Series With 74 Patients. Neurosurgery (2020) 87(4):720–9. doi: 10.1093/neuros/nyz513
20. Duffau H. Awake Mapping With Transopercular Approach in Right Insular-Centered Low-Grade Gliomas Improves Neurological Outcomes and Return to Work. Neurosurgery (2022) 91(1):182–90. doi: 10.1227/neu.0000000000001966
21. Peeters S, Pagès M, Gauchotte G, Miquel C, Cartalat-Carel S, Guillamo JS, et al. Interactions Between Glioma and Pregnancy: Insight From a 52-Case Multicenter Series. J Neurosurg (2018) 128(1):3–13. doi: 10.3171/2016.10.JNS16710
22. Ng S, Duffau H. Factors Associated With Long-Term Survival in Women Who Get Pregnant After Surgery for WHO Grade II Glioma. Neurology (2022) 11:10.1212/WNL. doi: 10.1212/WNL.0000000000200523
23. Duffau H, Taillandier L. New Concepts in the Management of Diffuse Low-Grade Glioma: Proposal of a Multistage and Individualized Therapeutic Approach. Neuro Oncol (2015) 17(3):332–42. doi: 10.1093/neuonc/nou153
24. Schmidt MH, Berger MS, Lamborn KR, Aldape K, McDermott MW, Prados MD, et al. Repeated Operations for Infiltrative Low-Grade Gliomas Without Intervening Therapy. J Neurosurg (2003) 98(6):1165–9. doi: 10.3171/jns.2003.98.6.1165
25. Martino J, Taillandier L, Moritz-Gasser S, Gatignol P, Duffau H. Re-Operation is a Safe and Effective Therapeutic Strategy in Recurrent WHO Grade II Gliomas Within Eloquent Areas. Acta Neurochir (Wien) (2009) 151(5):427–36. doi: 10.1007/s00701-009-0232-6
26. Ahmadi R, Dictus C, Hartmann C, Zürn O, Edler L, Hartmann M, et al. Long-Term Outcome and Survival of Surgically Treated Supratentorial Low-Grade Glioma in Adult Patients. Acta Neurochir (Wien) (2009) 151(11):1359–65. doi: 10.1007/s00701-009-0435-x
27. Kaspera W, Majchrzak K, Bobek-Billewicz B, Hebda A, Stasik-Pres G, Majchrzak H, et al. Reoperations of Patients With Low-Grade Gliomas in Eloquent or Near Eloquent Brain Areas. Neurol Neurochir Pol (2013) 47(2):116–25. doi: 10.5114/ninp.2013.34399
28. Ramakrishna R, Hebb A, Barber J, Rostomily R, Silbergeld D. Outcomes in Reoperated Low-Grade Gliomas. Neurosurgery (2015) 77:175–84. doi: 10.1227/NEU.0000000000000753
29. Ius T, Pauletto G, Cesselli D, Isola M, Turella L, Budai R, et al. Second Surgery in Insular Low-Grade Gliomas. BioMed Res Int (2015) 2015:497610. doi: 10.1155/2015/497610
30. Southwell DG, Hervey-Jumper SL, Perry DW, Berger MS. Intraoperative Mapping During Repeat Awake Craniotomy Reveals the Functional Plasticity of Adult Cortex. J Neurosurg (2016) 124(5):1460–9. doi: 10.3171/2015.5.JNS142833
31. Spitaels J, Devriendt D, Sadeghi N, Luce S, De Witte O, Goldman S, et al. Management of Supratentorial Recurrent Low-Grade Glioma: A Multidisciplinary Experience in 35 Adult Patients. Oncol Lett (2017) 14(3):2789–95. doi: 10.3892/ol.2017.6543
32. Picart T, Herbet G, Moritz-Gasser S, Duffau H. Iterative Surgical Resections of Diffuse Glioma With Awake Mapping: How to Deal With Cortical Plasticity and Connectomal Constraints? Neurosurgery (2019) 85(1):105–16. doi: 10.1093/neuros/nyy218
33. Zattra CM, Zhang DY, Broggi M, Velz J, Vasella F, Seggewiss D, et al. Repeated Craniotomies for Intracranial Tumors: Is the Risk Increased? Pooled Analysis of Two Prospective, Institutional Registries of Complications and Outcomes. J Neurooncol (2019) 142:49–57. doi: 10.1007/s11060-018-03058-y
34. Morshed RA, Young JS, Han SJ, Hervey-Jumper SL, Berger MS. Perioperative Outcomes Following Reoperation for Recurrent Insular Gliomas. J Neurosurg (2019) 131:467–73. doi: 10.3171/2018.4.JNS18375
35. Shofty B, Haim O, Costa M, Kashanian A, Shtrozberg S, Ram Z, et al. Impact of Repeated Operations for Progressive Low-Grade Gliomas. Eur J Surg Oncol (2020) 46(12):2331–7. doi: 10.1016/j.ejso.2020.07.013
36. Capo G, Skrap M, Guarracino I, Isola M, Battistella C, Ius T, et al. Cognitive Functions in Repeated Glioma Surgery. Cancers (Basel) (2020) 12(5):1077. doi: 10.3390/cancers12051077
37. Hamdan N, Duffau H. Extending the Multistage Surgical Strategy for Recurrent Initially Low-Grade Gliomas: Functional and Oncological Outcomes in 31 Consecutive Patients Who Underwent a Third Resection Under Awake Mapping. J Neurosurg (2021) 136(4):1035–44. doi: 10.3171/2021.3.JNS21264
38. Ng S, Lemaitre AL, Moritz-Gasser S, Herbet G, Duffau H. Recurrent Low-Grade Gliomas: Does Reoperation Affect Neurocognitive Functioning? Neurosurgery (2022) 90(2):221–32. doi: 10.1227/NEU.0000000000001784
39. Chang J, Wang Y, Guo R, Guo X, Lu Y, Ma W, et al. The Effect of Operations in Patients With Recurrent Diffuse Low-Grade Glioma: A Qualitative Systematic Review. Clin Neurol Neurosurg (2020) 196:105973. doi: 10.1016/j.clineuro.2020.105973
40. Morshed RA, Young JS, Gogos AJ, Haddad AF, McMahon JT, Molinaro AM, et al. Reducing Complication Rates for Repeat Craniotomies in Glioma Patients: A Single-Surgeon Experience and Comparison With the Literature. Acta Neurochir (Wien) (2022) 164(2):405–17. doi: 10.1007/s00701-021-05067-9
41. Uppstrom TJ, Singh R, Hadjigeorgiou GF, Magge R, Ramakrishna R. Repeat Surgery for Recurrent Low-Grade Gliomas Should be Standard of Care. Clin Neurol Neurosurg (2016) 151:18–23. doi: 10.1016/j.clineuro.2016.09.013
42. Duffau H. Lessons From Brain Mapping in Surgery for Low-Grade Glioma: Insights Into Associations Between Tumour and Brain Plasticity. Lancet Neurol (2005) 4(8):476–86. doi: 10.1016/S1474-4422(05)70140-X
43. Desmurget M, Bonnetblanc F, Duffau H. Contrasting Acute and Slow-Growing Lesions: A New Door to Brain Plasticity. Brain (2007) 130(Pt 4):898–914. doi: 10.1093/brain/awl300
44. Almairac F, Duffau H, Herbet G. Contralesional Macrostructural Plasticity of the Insular Cortex in Patients With Glioma: A VBM Study. Neurology (2018) 91(20):e1902–8. doi: 10.1212/WNL.0000000000006517
45. Almairac F, Deverdun J, Cochereau J, Coget A, Lemaitre AL, Moritz-Gasser S, et al. Homotopic Redistribution of Functional Connectivity in Insula-Centered Diffuse Low-Grade Glioma. NeuroImage Clin (2021) 29:102571. doi: 10.1016/j.nicl.2021.102571
46. Duffau H. The Huge Plastic Potential of Adult Brain and the Role of Connectomics: New Insights Provided by Serial Mappings in Glioma Surgery. Cortex (2014) 58:325–37. doi: 10.1016/j.cortex.2013.08.005
47. Duffau H. Brain Connectomics Applied to Oncological Neuroscience: From a Traditional Surgical Strategy Focusing on Glioma Topography to a Meta-Network Approach. Acta Neurochir (Wien) (2021) 163(4):905–17. doi: 10.1007/s00701-021-04752-z
48. Mosca C, Zoubrinetzy R, Baciub M, Aguilar L, Minotti L, Kahane P, et al. Rehabilitation of Verbal Memory by Means of Preserved Nonverbal Memory Abilities After Epilepsy Surgery. Epilepsy Behav Case Rep (2014) 2:167–73. doi: 10.1016/j.ebcr.2014.09.002
49. Vassal M, Charroud C, Deverdun J, Le Bars E, Molino F, Bonnetblanc F, et al. Recovery of Functional Connectivity of the Sensorimotor Network After Surgery for Diffuse Low-Grade Gliomas Involving the Supplementary Motor Area. J Neurosurg (2017) 126(4):1181–90. doi: 10.3171/2016.4.JNS152484
50. Duffau H. Functional Mapping Before and After Low-Grade Glioma Surgery: A New Way to Decipher Various Spatiotemporal Patterns of Individual Neuroplastic Potential in Brain Tumor Patients. Cancers (Basel) (2020) 12(9):2611. doi: 10.3390/cancers12092611
51. Fukuya Y, Ikuta S, Maruyama T, Nitta M, Saito T, Tsuzuki S, et al. Tumor Recurrence Patterns After Surgical Resection of Intracranial Low-Grade Gliomas. J Neurooncol (2019) 144:519–28. doi: 10.1007/s11060-019-03250-8
52. Ferracci FX, Michaud K, Duffau H. The Landscape of Postsurgical Recurrence Patterns in Diffuse Low-Grade Gliomas. Crit Rev Oncol Hematol (2019) 138:148–55. doi: 10.1016/j.critrevonc.2019.04.009
53. Ius T, Angelini E, Thiebaut de Schotten M, Mandonnet E, Duffau H. Evidence for Potentials and Limitations of Brain Plasticity Using an Atlas of Functional Resectability of WHO Grade II Gliomas: Towards a "Minimal Common Brain". Neuroimage (2011) 56(3):992–1000. doi: 10.1016/j.neuroimage.2011.03.022
54. Herbet G, Maheu M, Costi E, Lafargue G, Duffau H. Mapping Neuroplastic Potential in Brain-Damaged Patients. Brain (2016) 139(Pt 3):829–44. doi: 10.1093/brain/awv394
55. Sarubbo S, Tate M, De Benedictis A, Merler S, Moritz-Gasser S, Herbet G, et al. Mapping Critical Cortical Hubs and White Matter Pathways by Direct Electrical Stimulation: An Original Functional Atlas of the Human Brain. Neuroimage (2020) 205:116237. doi: 10.1016/j.neuroimage.2019.116237
56. Duffau H. White Matter Tracts and Diffuse Lower-Grade Gliomas: The Pivotal Role of Myelin Plasticity in the Tumor Pathogenesis, Infiltration Patterns, Functional Consequences and Therapeutic Management. Front Oncol (2022) 12:855587. doi: 10.3389/fonc.2022.855587
57. Duffau H. A Two-Level Model of Interindividual Anatomo-Functional Variability of the Brain and its Implications for Neurosurgery. Cortex (2017) 86:303–13. doi: 10.1016/j.cortex.2015.12.009
58. Girard A, Le Reste PJ, Metais A, Carsin Nicol B, Chiforeanu DC, Bannier E, et al. Combining 18f-DOPA PET and MRI With Perfusion-Weighted Imaging Improves Delineation of High-Grade Subregions in Enhancing and non-Enhancing Gliomas Prior Treatment: A Biopsy-Controlled Study. J Neurooncol (2021) 155(3):287–95. doi: 10.1007/s11060-021-03873-w
59. Monje M. Synaptic Communication in Brain Cancer. Cancer Res (2020) 80(14):2979–82. doi: 10.1158/0008-5472.CAN-20-0646
60. Young JS, Morshed RA, Gogos AJ, Amara D, Villanueva-Meyer JE, Berger MS, et al. The Glioma-Network Interface: A Review of the Relationship Between Glioma Molecular Subtype and Intratumoral Function. Neurosurgery (2020) 87(6):1078–84. doi: 10.1093/neuros/nyaa362
61. Silva M, Vivancos C, Duffau H. The Concept of «Peritumoral Zone» in Diffuse Low-Grade Gliomas: Oncological and Functional Implications for a Connectome-Guided Therapeutic Attitude. Brain Sci (2022) 12(4):504. doi: 10.3390/brainsci12040504
62. Herbet G, Duffau H. Revisiting the Functional Anatomy of the Human Brain: Toward a Meta-Networking Theory of Cerebral Functions. Physiol Rev (2020) 100:1181–228. doi: 10.1152/physrev.00033.2019
63. Duffau H. Stimulation Mapping of White Matter Tracts to Study Brain Functional Connectivity. Nat Rev Neurol (2015) 11:255–65. doi: 10.1038/nrneurol.2015.51
64. Fernández Coello A, Moritz-Gasser S, Martino J, Martinoni M, Matsuda R, Duffau H. Selection of Intraoperative Tasks for Awake Mapping Based on Relationships Between Tumor Location and Functional Networks. J Neurosurg (2013) 119(6):1380–94. doi: 10.3171/2013.6.JNS122470
65. Mandonnet E, Herbet G. Intraoperative Mapping of Cognitive Networks. In: Mandonnet E, Herbet G, editors. Which Tasks for Which Locations. Springer Nature Switzerland: Springer (2021).
66. Duffau H, Ng S, Lemaitre AL, Moritz-Gasser S, Herbet G. Constant Multi-Tasking With Time Constraint to Preserve Across-Network Dynamics Throughout Awake Surgery for Low-Grade Glioma: A Necessary Step to Enable Patients Resuming an Active Life. Front Oncol (2022) 26(12):924762. doi: 10.3389/fonc.2022.924762.
67. Duffau H. Dynamic Interplay Between Lower-Grade Glioma Instability and Brain Metaplasticity: Proposal of an Original Model to Guide the Therapeutic Strategy. Cancers (Basel) (2021) 13(19):4759. doi: 10.3390/cancers13194759
68. Duffau H. Why Brain Radiation Therapy Should Take Account of the Individual Structural and Functional Connectivity: Toward an Irradiation "À La Carte". Crit Rev Oncol Hematol (2020) 154:103073. doi: 10.1016/j.critrevonc.2020.103073
69. Blonski M, Obara T, Brzenczek C, Pouget C, Dillier C, Meyer M, et al. Initial PCV Chemotherapy Followed by Radiotherapy Is Associated With a Prolonged Response But Late Neurotoxicity in 20 Diffuse Low-Grade Glioma Patients. Front Oncol (2022) 12:827897. doi: 10.3389/fonc.2022.827897
70. Gupta K, Burns TC. Radiation-Induced Alterations in the Recurrent Glioblastoma Microenvironment: Therapeutic Implications. Front Oncol (2018) 8:503. doi: 10.3389/fonc.2018.00503
71. Pallud J, Blonski M, Mandonnet E, Audureau E, Fontaine D, Sanai N, et al. Velocity of Tumor Spontaneous Expansion Predicts Long-Term Outcomes for Diffuse Low-Grade Gliomas. Neuro Oncol (2013) 15(5):595–606. doi: 10.1093/neuonc/nos331
72. Darlix A, Rigau V, Fraisse J, Gozé C, Fabbro M, Duffau H. Postoperative Follow-Up for Selected Diffuse Low-Grade Gliomas With WHO Grade III/IV Foci. Neurology (2020) 94(8):e830–41. doi: 10.1212/WNL.0000000000008877
73. Blonski M, Taillandier L, Herbet G, Maldonado IL, Beauchesne P, Fabbro M, et al. Combination of Neoadjuvant Chemotherapy Followed by Surgical Resection as a New Strategy for WHO Grade II Gliomas: A Study of Cognitive Status and Quality of Life. J Neurooncol (2012) 106(2):353–66. doi: 10.1007/s11060-011-0670-x
74. Blonski M, Pallud J, Gozé C, Mandonnet E, Rigau V, Bauchet L, et al. Neoadjuvant Chemotherapy may Optimize the Extent of Resection of World Health Organization Grade II Gliomas: A Case Series of 17 Patients. J Neurooncol (2013) 113(2):267–75. doi: 10.1007/s11060-013-1106-6
75. Spena G, Garbossa D, Barletta L, Prevost C, Versari P. Preoperative Chemotherapy for Infiltrative Low-Grade Oligoastrocytoma: A Useful Strategy to Maximize Surgical Resection. Neurol Med Chir (Tokyo) (2010) 50(5):410–3. doi: 10.2176/nmc.50.410
76. Nahed BV, Redjal N, Brat DJ, Chi AS, Oh K, Batchelor TT, et al. Management of Patients With Recurrence of Diffuse Low Grade Glioma: A Systematic Review and Evidence-Based Clinical Practice Guideline. J Neurooncol (2015) 125(3):609–30. doi: 10.1007/s11060-015-1910-2
77. European Low-Grade Glioma Network. Evidence-Based Management of Adult Patients With Diffuse Glioma. Lancet Oncol (2017) 18(8):e429. doi: 10.1016/S1470-2045(17)30510-7
78. Mazor T, Chesnelong C, Pankov A, Jalbert LE, Hong C, Hayes J, et al. Clonal Expansion and Epigenetic Reprogramming Following Deletion or Amplification of Mutant IDH1. Proc Natl Acad Sci U S A (2017) 114(40):10743–8. doi: 10.1073/pnas.1708914114
79. Chaichana KL, Zadnik P, Weingart JD, Olivi A, Gallia GL, Blakeley J, et al. Multiple Resections for Patients With Glioblastoma: Prolonging Survival. J Neurosurg (2013) 118(4):812–20. doi: 10.3171/2012.9.JNS1277
80. Hervey-Jumper SL, Berger MS. Reoperation for Recurrent High-Grade Glioma: A Current Perspective of the Literature. Neurosurgery (2014) 75(5):491–9. doi: 10.1227/NEU.0000000000000486
81. Abraham WC. Metaplasticity: Tuning Synapses and Networks for Plasticity. Nat Rev Neurosci (2008) 9(5):387. doi: 10.1038/nrn2356
82. Duffau H. Introducing the Concept of Brain Metaplasticity in Glioma: How to Reorient the Pattern of Neural Reconfiguration to Optimize the Therapeutic Strategy. J Neurosurg (2021) 136(2):613–7. doi: 10.3171/2021.5.JNS211214
83. Duffau H. Can Non-Invasive Brain Stimulation Be Considered to Facilitate Reoperation for Low-Grade Glioma Relapse by Eliciting Neuroplasticity? Front Neurol (2020) 11:582489. doi: 10.3389/fneur.2020.582489
84. Hamer RP, Yeo TT. Current Status of Neuromodulation-Induced Cortical Prehabilitation and Considerations for Treatment Pathways in Lower-Grade Glioma Surgery. Life (Basel) (2022) 12(4):466. doi: 10.3390/life12040466
Keywords: brain connectome, electrostimulation mapping, low-grade glioma, multistage management, neuroplasticity, quality of life, reoperation, awake brain surgery
Citation: Duffau H (2022) Repeated Awake Surgical Resection(s) for Recurrent Diffuse Low-Grade Gliomas: Why, When, and How to Reoperate? Front. Oncol. 12:947933. doi: 10.3389/fonc.2022.947933
Received: 19 May 2022; Accepted: 06 June 2022;
Published: 05 July 2022.
Edited by:
Giuseppe La Rocca, Agostino Gemelli University Polyclinic (IRCCS), ItalyReviewed by:
Emmanuel Mandonnet, Hôpital Lariboisière, FranceCopyright © 2022 Duffau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hugues Duffau, aC1kdWZmYXVAY2h1LW1vbnRwZWxsaWVyLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.