
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 14 October 2022
Sec. Molecular and Cellular Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.941676
This article is part of the Research TopicNew Understandings and Research in Anal Squamous Cell CarcinomaView all 9 articles
 Alice Debernardi1
Alice Debernardi1 Aurélia Meurisse2,3
Aurélia Meurisse2,3 Jean-Luc Prétet1,4
Jean-Luc Prétet1,4 David Guenat1,5Franck Monnien6
David Guenat1,5Franck Monnien6 Laurie Spehner3,7
Laurie Spehner3,7 Angélique Vienot3,7Patrick Roncarati8Thierry André9Laurent Abramowitz10,11Chloé Molimard12Christiane Mougin3,4Michael Herfs8
Angélique Vienot3,7Patrick Roncarati8Thierry André9Laurent Abramowitz10,11Chloé Molimard12Christiane Mougin3,4Michael Herfs8 Stefano Kim3,13,14Christophe Borg3,5,13*
Stefano Kim3,13,14Christophe Borg3,5,13*Squamous Cell Carcinoma of the Anal canal (SCCA) is a rare disease associated with a Human Papillomavirus (HPV) infection in most cases, predominantly the HPV16 genotype. About 15% of SCCA are diagnosed in metastatic stage and some will relapse after initial chemoradiotherapy (CRT). Treatment of patients by Docetaxel, Cisplatin and 5-fluorouracil (DCF) has been recently shown to improve their complete remission and progression-free survival. The aim of this retrospective study was to explore the impact of HPV infection, HPV DNA integration, TERT promoter mutational status and somatic mutations of oncogenes on both progression-free (PFS) and overall survivals (OS) of patients treated by DCF. Samples obtained from 49 patients included in the Epitopes-HPV02 clinical trial, diagnosed with metastatic or non-resectable local recurrent SCCA treated by DCF, were used for analyses. Median PFS and OS were not associated with HPV status. Patients with episomal HPV had an improved PFS compared with SCCA patients with integrated HPV genome (p=0.07). TERT promoter mutations were rarely observed and did not specifically distribute in a subset of SCCA and did not impact DCF efficacy. Among the 42 genes investigated, few gene alterations were observed, and were in majority amplifications (68.4%), but none were significantly correlated to PFS. As no biomarker is significantly associated with patients’ survival, it prompts us to include every patient failing CRT or with metastatic disease in DCF strategy.
Squamous cell carcinoma of the anal canal is a rare disease, representing less than 3% of all gastrointestinal malignancies in the world (1). Its incidence has been steadily increasing in recent decades in men as well as in women with 50 000 new cases diagnosed each year worldwide and it is estimated that it will continue to increase in the next future (2). This increase is likely due to its association with human papillomavirus infection (3), predominantly genotype HPV16, since HPV-related oncoproteins (E6 and E7) are expressed in more than 90% of patients with SCCA (4).
The great majority of SCCA patients are diagnosed at a localized stage. However, about 15% of patients are diagnosed at metastatic stage in US (https://seer.cancer.gov/statfacts/html/anus.html, accessed July 25th 2022), and between 25% to 40% of patients treated initially by chemoradiotherapy will develop locally advanced recurrences or metastases in Western countries (5–7). Treatment of patients with nonresectable local recurrences or with distant metastases relies on systemic chemotherapy. The combination of cisplatin (CDDP) and 5-Fluorouracil (5FU) was historically considered as the recommended treatment for advanced SCCA based in retrospective analysis (8, 9). However, complete remission was a rare event, and only about 15% of patients were progression-free at 1 year (10, 11).
Docetaxel is an anticancer agent which exerts cytotoxic functions by stabilizing tubulin polymerization leading to mitosis arrest and cell death. It has been previously proposed that a loss of normal p53 function confers sensitization to taxane chemotherapy by increasing G2/M arrest and apoptosis (12). Because the association between SCCA and HPV infection is strong and E6 oncoprotein encoded by High Risk (HR) HPV, such as HPV16 and 18, induces the degradation of p53, we previously hypothesized that SCCA might be sensitive to taxane-containing chemotherapies such as docetaxel (13). In addition, docetaxel has been shown to increase endoplasmic reticulum (ER) stress and to induce immunogenic cell death of cancer cells (14). In 2018, Epitopes-HPV02 trial confirmed the benefit of the addition of docetaxel to CDDP and 5FU (DCF) (15). A complete response was observed in 45% of patients, and the 1-year progression free survival rate was 47%. Therefore, DCF became one of the standard regimen at first-line in advanced SCCA (13, 15–17).
Here, we describe the molecular characterization of anal cancer biopsies with advanced SCCA, included in the Epitopes-HPV02 trial.
The cohort is constituted of patients included in the prospective multicenter phase II Epitopes-HPV02 study (NCT02402842). Patients with diagnosis of metastatic or non-resectable local recurrent SCCA were included, and were treated by DCF. The study was described in detail elsewhere (15–17). Among 66 patients included in the trial, 49 patients had available material for molecular analysis. The EDITH V cohort constituted of patients with diagnosis of SCCA at early stage was used as a validation cohort. The study was described elsewhere (18). Overall, 381 patients had available material for molecular analysis.
Prior to DNA extraction, separate hematoxylin-eosin-stained slides were reviewed by an experienced histopathologist and manually macro-dissected when appropriate to ensure tumor content greater than 20%. Depending on the size of the fixed tissue, between 3 and 8 formalin-fixed paraffin-embedded (FFPE) tissue sections of 10 µm thickness were processed for DNA extraction with the QIAamp DNA mini kit (QIAGEN) according to manufacturer’s instructions.
HPV genotyping was performed locally [Department of Cellular and Molecular Biology, University Hospital of Besançon, France as described previously (19)]. Briefly, genotyping was performed with the INNO-LiPA HPV Genotyping Extra® test (Fujirebio) allowing the identification of 28 different HPV genotypes as well as the HLA-DPB1 gene as internal control for sample quality for DNA detection. As recommended by the manufacturer, samples negative for the HLA-DPB1 gene and negative for HPV were excluded from the analysis.
To confirm the HPV infection, in situ hybridization experiments were performed according to the manufacturer’s instructions. The INFORM HPV III Family 16 Probe (Ventana Medical Systems) allowed the detection of 12 high-risk HPV genotypes.
As routinely performed, the physical status of HPV (episomal or mixed/integrated) was determined by assessing the disruption of the viral E2 gene (Table 1). Briefly, after DNA extraction and concentration measurement with NanoDrop 1000 spectrophotometer (Thermo Fisher Scientific), quantitative real-time PCR experiments were performed as follows: 95°C for 15 min, 40 cycles at 95°C for 30 sec, then 50°C for 1 min and 72°C for 1 min. Each experiment was performed in triplicate and the E6/E2 ratio cut-off value was determined, as previously described (20, 21). Importantly, to be able to compare the collected results, the amplification efficiency of each PCR reaction was determined (qPCR efficiency calculator, Thermo Fisher Scientific).
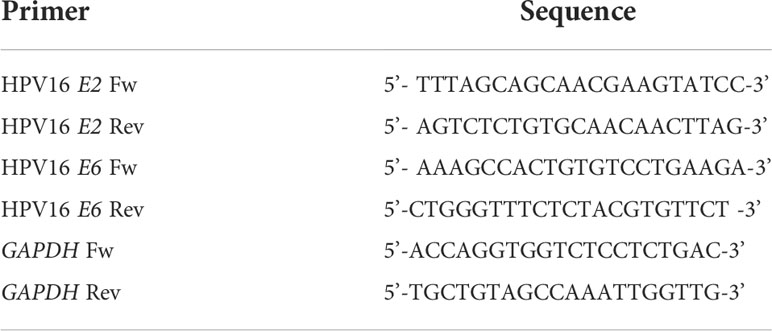
Table 1 Primer sequence used for E2, E6 and GAPDH qPCR.
Genomic sequence of promoter flanking region of TERT (ENSR00001274355) was obtained from Ensembl database (www.ensembl.org). Specific primers were designed (Table 2) using the online Primer-BLAST software (www.ncbi.nlm.nih.gov/tools/primer-blast/) (22). Targeted sequences were amplified by PCR using the Qiagen Multiplex PCR kit (QIAGEN) and 5% DMSO. PCR conditions were as follows: 94°C for 15 min, 40 cycles at 94°C for 1 min, then 64°C for 30 sec, 72°C for 45 sec and finally 7 min at 72°C. PCR products were purified using the gel extraction kit NucleoSpin Gel and PCR Clean-up (Macherey-Nagel). Bidirectional sequencing reaction was performed using the BigDye Terminator v3.1 Cycle Sequencing Kit (Life technologies-Thermofisher). The reactions were run according to the following protocol: one cycle at 96°C for 1 min; 15 cycles at 96°C for 10 s, 50°C for 5 s, 60°C for 1 min 15 s; 5 cycles at 96°C for 10 s, 50°C for 5 s, 60°C for 1 min 30 s; 5 cycles of 96°C for 10 s, 50°C for 5 s and 60°C for 2 min. After purification with a NucleoSEQ kit (Macherey-Nagel), samples were run and analyzed on an ABI 3130 sequencer (Life technologies-Thermofisher). Finally, the sequences obtained were compared with the reference sequence of TERT promoter using GeneScan analysis software.
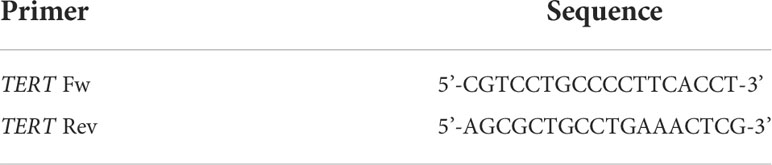
Table 2 Primer sequence used for TERT sequencing.
SNaPshot analysis was performed from the purified amplicons used for Sanger sequencing with the ABI Prism SNaPshot Multiplex kit (AB Life Technologies). Amplified TERT promoter was analyzed for the presence of mutations at position C228 and C250 using two primers that contained an additional poly(dC) tail at their 5’ end, allowing for their simultaneous detection (Table 3). Reactions were performed in a final volume of 5 µL, containing 1.5 µL of purified multiplex PCR product (2 to 10 ng/µL), 2.5 µL of SNaPshot Ready Multiplex Ready Reaction Mix, 0.5 µL of probe equimolar mix (each probe at 0.2 pmol/L final), and 0.5 µL of double-distilled water. Multiplex single base extensions were carried out for 25 cycles according to the following program: 10 seconds at 96°C, 5 seconds at 52°C, and 30 seconds at 60°C. SNaPshot products were then treated at 37°C for 15 min with 0.5µL of shrimp alkaline phosphatase at 1 U/µL diluted in 2.5 µL of shrimp alkaline phosphatase buffer 10X and 11.5 µL of double-distilled water. After heat inactivation of shrimp alkaline phosphatase for 10 minutes at 75°C, 2 µL of the labelled products were mixed with 9.5 µL of HiDi formamide and 0.5 µL of Genescan-120LIZ size standard. They were then separated using a 25 min run on an ABI Prism 3130 DNA sequencer with POP-7 matrix and 14 seconds for injection. The analysis was performed using GeneMapper ID software version 3.2.1 (Applied Biosystems).
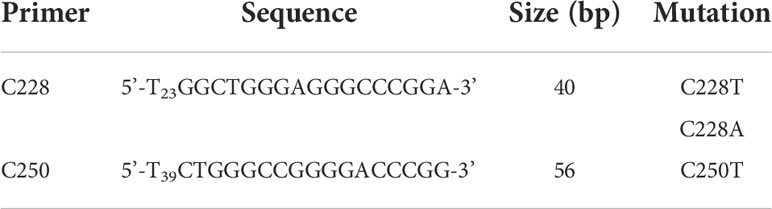
Table 3 SNaPshot primers used for detection of TERT promoter mutation.
Libraries were prepared from 50 ng of DNA or by using KAPA Hyperplus Library Preparation (KAPA Biosystem) and Solid Tumor Solution capture kits and protocol by SOPHIA GENETICS. They were sequenced on MiSeq sequencer (Illumina). Criteria used to select mutations were depth (≥100) and allele frequency (≥10%). Allele frequency variants ≈100% or described as benign in ClinVar database, with intronic, frameshift, splicing or synonymous mutations were excluded. A list of the targeted 42 genes is shown in Table 4.
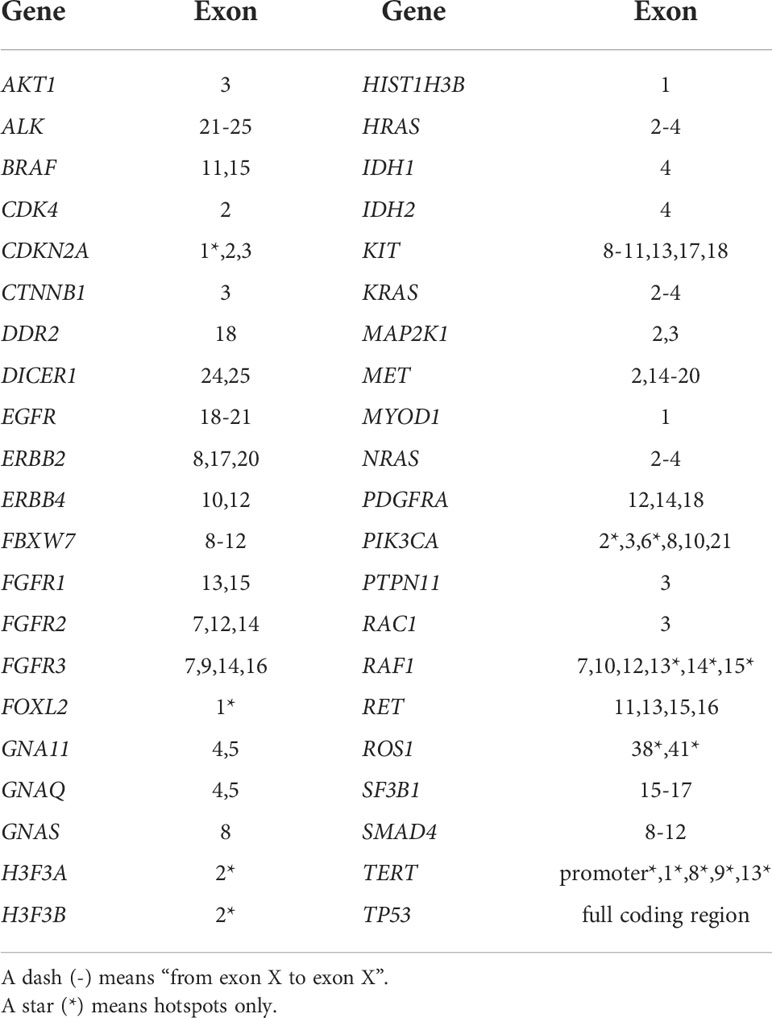
Table 4 List of the genes and their exons targeted by NGS.
Log-rank (Mantel-Cox) test was used for the analysis of PFS and OS according to HPV integration status and PIK3CA mutational status. PFS was determined at 12 months from the first DCF cycle. Fisher’s exact test was used for all other analysis.
Among patients included in the Epitopes-HPV02 study, there was a majority of female (83.7%) compared to male who represented only 16.3% (Table 5). Most of the patients (91.8%, 45 out of the 49 patients with available tumor material) presented an HPV16 infection. Two patients were infected with other HPV genotypes (HPV33 and HPV33-45) and two patients had SCCA without detectable HPV genome. Median PFS was 10.7 months (95% CI: 9.9-16.0) for patients displaying HPV16+ SCCA and 12.6 months (95% CI: 6.2-18.9) when HPV was not detected. Median OS was 36.3 months (95% CI: 24.2-NE) for HPV16+ SCCA and 26 months for HPV negative SCCA.
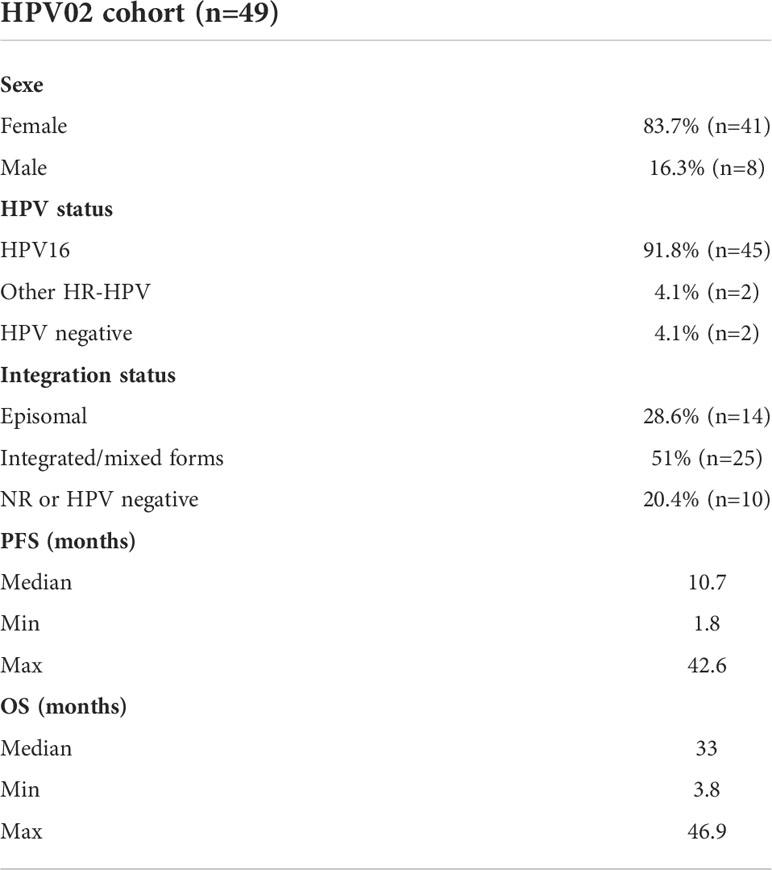
Table 5 Characteristics of the HPV02 cohort.
We next explored if the presence of HPV genome in an episomal or integrated form could influence clinical outcomes of SCCA patients treated with DCF (Table 6). There was a majority of integrated/mixed forms (51%, n=25) in all SCCA compared to episomal forms (28.6%, n=14). In about 20% (n=10/49, 20.4%) of patients, the HPV integration status was not determined (2 of them were actually HPV negative, 2 were infected with other HR-HPV infection than HPV16 and the others had no remaining material to perform analysis). Median PFS was 19.5 months (95% CI: 8.3-NE) for patients with HPV DNA under episomal form and 10.6 months (95% CI: 9.9-12.9) for patients with integrated/mixed forms (p=0.0734). Median OS was 32.3 months for patients with integrated/mixed forms and was not reached for SCCA with episomal HPV DNA (Figure 1). The possible correlation between episomal HPV DNA in DCF efficacy is outlined by the 57% complete response rate observed in this population vs 44% for SCCA wherein HPV DNA was integrated or in a mixed form.
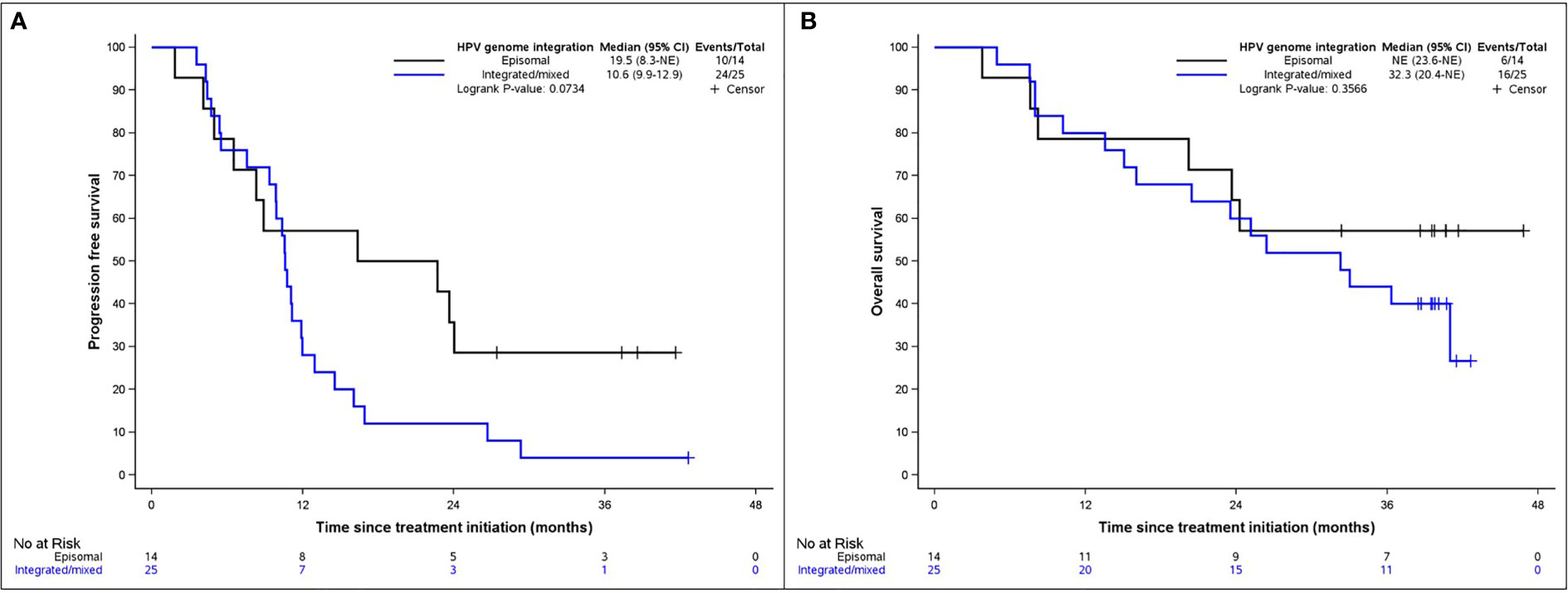
Figure 1 Kaplan-Meier diagrams representing (A) PFS and (B) OS according to the integration of HPV genome. Blue line symbolizes integrated/mixed forms, black line episomal forms.
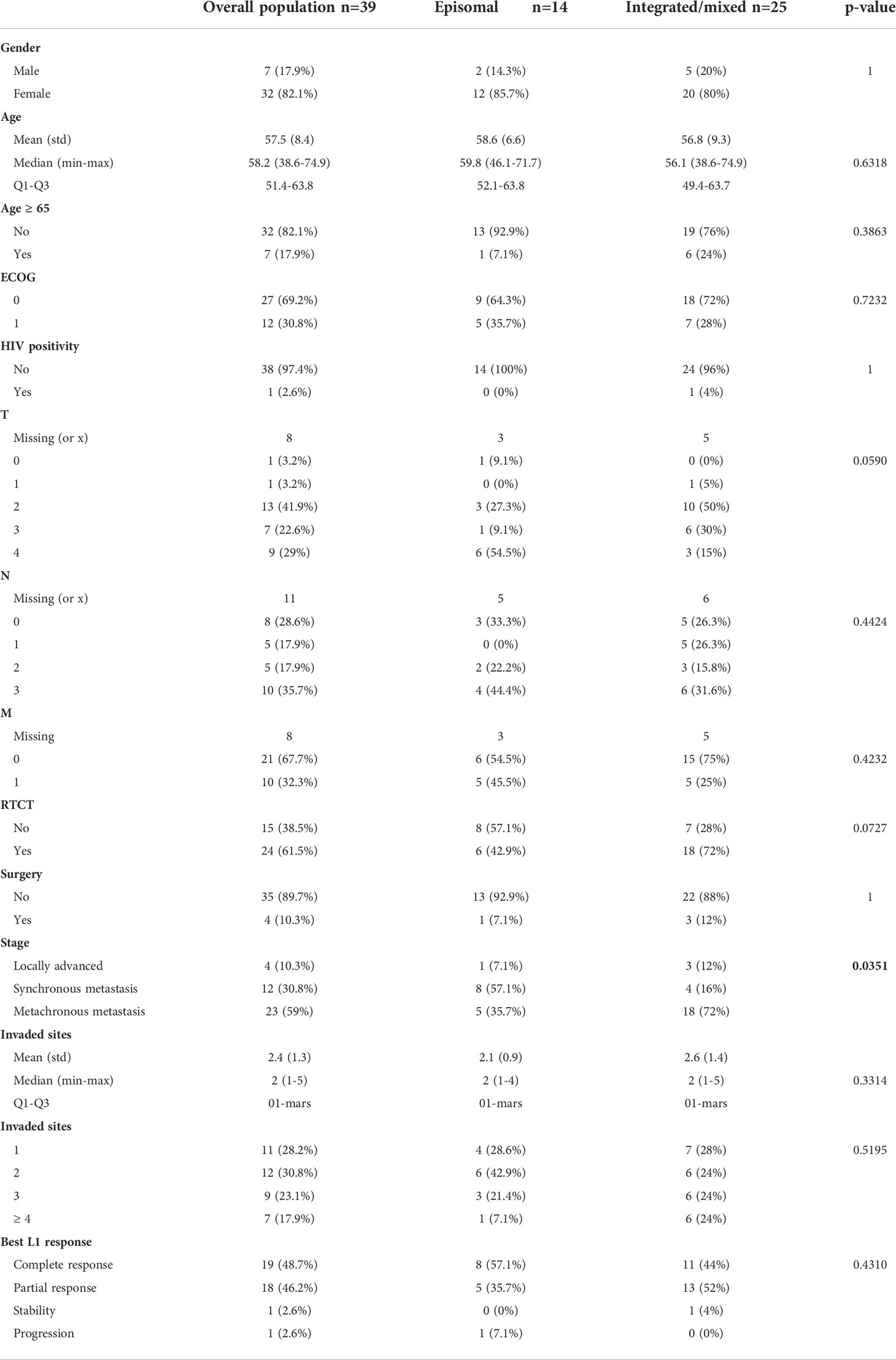
Table 6 Clinical characteristics of SCCA patients according to HPV genome status.
Transactivation of TERT is a critical signaling for HPV-mediated oncogenesis. E6-E6AP ubiquitin ligase complex are known to bind to TERT promoter, activating TERT gene transcription (23). Mutations of the TERT promoter are the major genomic alterations leading to TERT overactivation in most cancer types. However, the occurrence of TERT promoter mutations was never investigated in SCCA. We hypothesized that TERT promoter mutations might sustain resistance to DCF therapy. Therefore, these analyses were performed in 63 patients with available tumor materials. TERT promoter mutations occurred rarely and were observed in 5 patients (7.9%). Three types of TERT promoter mutations investigated have been observed. One HPV16+ SCCA patient had a C250T mutation, and another HPV16+ had a C228A mutation. Three other patients (2 HPV16+ and one HPV- SCCA) had C228T mutations. Three of the SCCA patients displaying TERT promoter mutations showed partial responses after exposition to DCF. These results addressed the question of the overall distribution of TERT mutations in SCCA population. To validate the prevalence of TERT mutations in SCCA, sequencing analysis of the telomerase catalytic subunit TERT was performed in the EDITH V cohort. Among the 381 patients with available DNA, TERT promoter mutations were identified in 30 patients (7.8%). The C228T mutation was predominant (73.3%, n=22), while the mutations C228A and C250T were observed in 1 and 7 patients respectively. Of note, one homozygote mutation of C228T was detected. Among the EDITH V cohort, there was a majority of patients with HPV positive SCCA (68%, n=259) including 210 (81%) patients with HPV16 or 18 infections and 49 (19%) patients with other HPV genotypes; 10 (2.6%) patients represented HPV negative SCCA. HPV status was not available for 112 (29.4%) patients. TERT promoter mutations were not specifically correlated to HPV status in SCCA (Figure 2). These results showed that the rare TERT promoter mutations observed in SCCA are not restricted to HPV negative SCCA and are not specifically correlated to a specific HPV type infection.
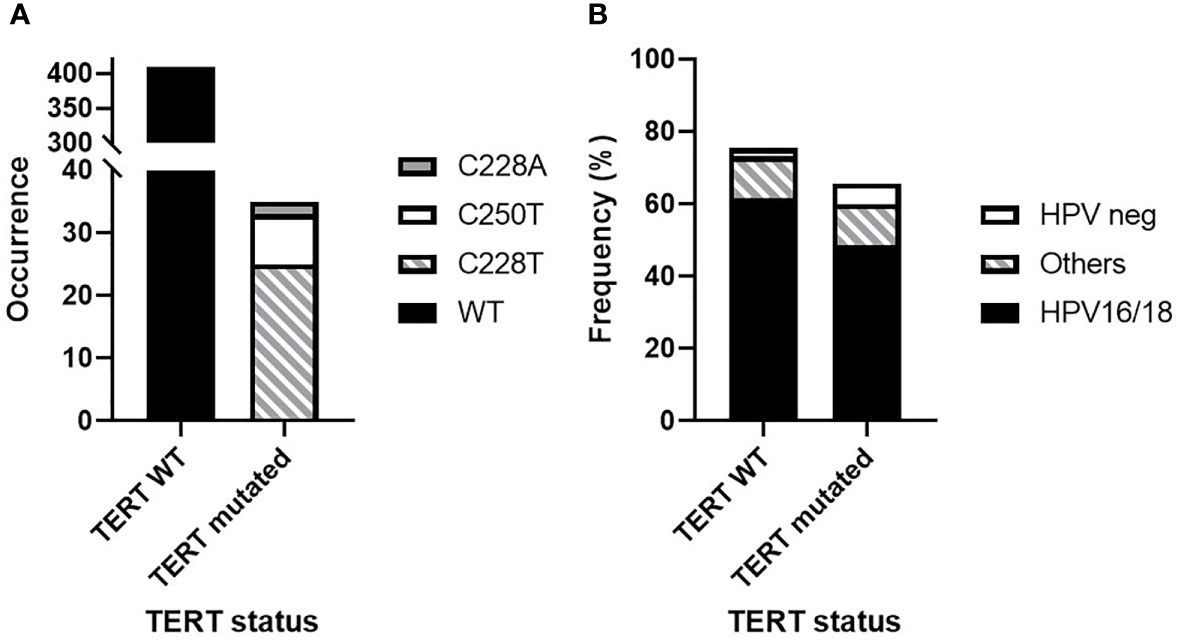
Figure 2 TERT promoter mutation distribution in human SCCA from the HPV02 and EDITH V cohorts (444 samples). (A) Wild-type (WT) TERT promoter prevalence versus C228T, C228A and C250T mutations. (B) Distribution of HPV status according to TERT promoter mutations.
Since HPV genotype, integration status or TERT promoter mutations did not account for DCF efficacy and SCCA patients’ prognosis in the Epitopes-HPV02 study, we next assessed the distribution of the main oncogenic alterations in SCCA metastatic or relapsing patients treated by DCF. NGS analysis targeting 42 oncogenic alterations was realized among patients of the HPV02 cohort. No alterations were found in AKT1, ALK, BRAF, DDR2, DICER1, ERBB4, FOXL2, GNAQ, GNAS, H3F3A, H3F3B, HIST1H3B, IDH1, IDH2, KIT, KRAS, MAP2K1, MET, PDGFRA, PTPN11, RAC1, RET, ROS1, SF3B1, SMAD4 and TP53. PIK3CA was the most altered gene with 10 amplifications and 6 mutations, followed by ERBB2 (3 amplifications and 3 mutations) and CDK4 (5 amplifications) (Table 7).

Table 7 Summary of somatic mutations retrieved among SCCA from the HPV02 cohort.
Nineteen out of the 49 (38.8%) patients with SCCA tested presented no alterations among the 42 screened genes. Most of them were HPV positive, with 89% (n=17/19) of HPV16 and 11% (n=2/19) of other HR-HPV. Forty-seven percent (n=9/19) of SCCA harbored integrated or mixed forms of HPV DNA, whereas 32% (n=6/19) harbored only episomal forms of oncogenic HPV DNA. On the contrary, 61.2% (n=30/49) patients with SCCA presented one alteration or more. A majority of them had an HPV16 infection (90%, n=27/30), one had an HPV16+33 infection and 2 were HPV negative. Almost 53% (n=16/30) had integrated or mixed forms, 26.6% (n=8/30) had an episomal HPV and 20% (n=6/30) were not identified. No difference was observed between the 2 groups concerning HPV status (p-values: 1 and 0.1581 between HPV positive/negative and HPV16/other HR-HPV respectively) nor integration status (p-value: 0.7397).
A heatmap was realized to cluster genomic alteration occurrence to PFS (more or less than 12 months) (Figure 3; Table 8). There was clearly no aggregation of a genomic alteration subset with the probability to be progression free after 12 months of follow up. Since PI3KCA amplification and mutations were the most frequent, we assessed the influence of these genomic alterations on SCCA patient overall survival. No difference of OS was observed between patients harboring PIK3CA alterations or WT PIK3CA (Figure 4, p-value: 0.1828).
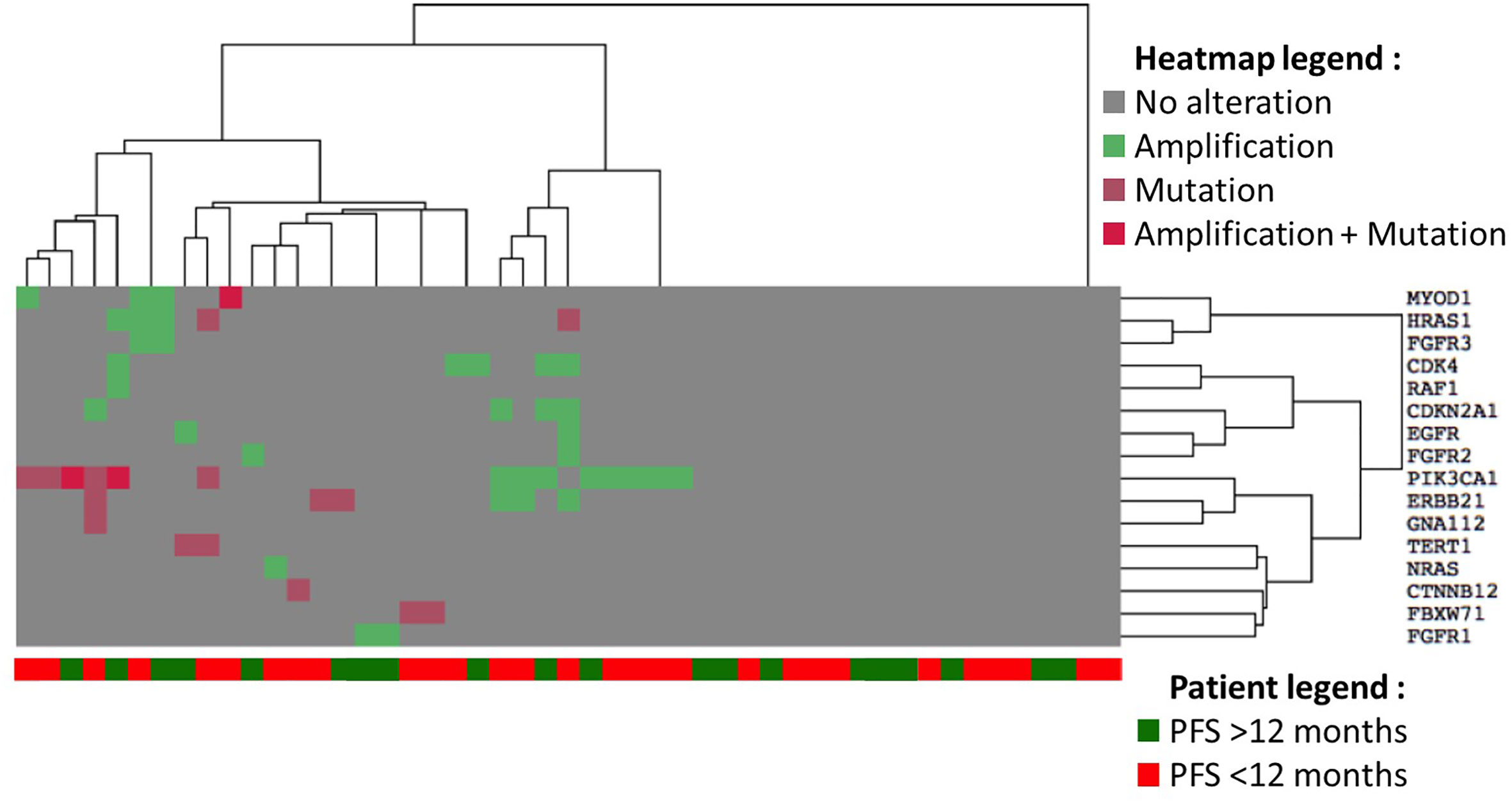
Figure 3 Heatmap of gene alteration frequency clustered by PFS (whether it reaches 12 months or not). The type of alterations is described in the heatmap legend, with the list of genes on the right, and PFS of patients is found at the bottom of the heatmap.
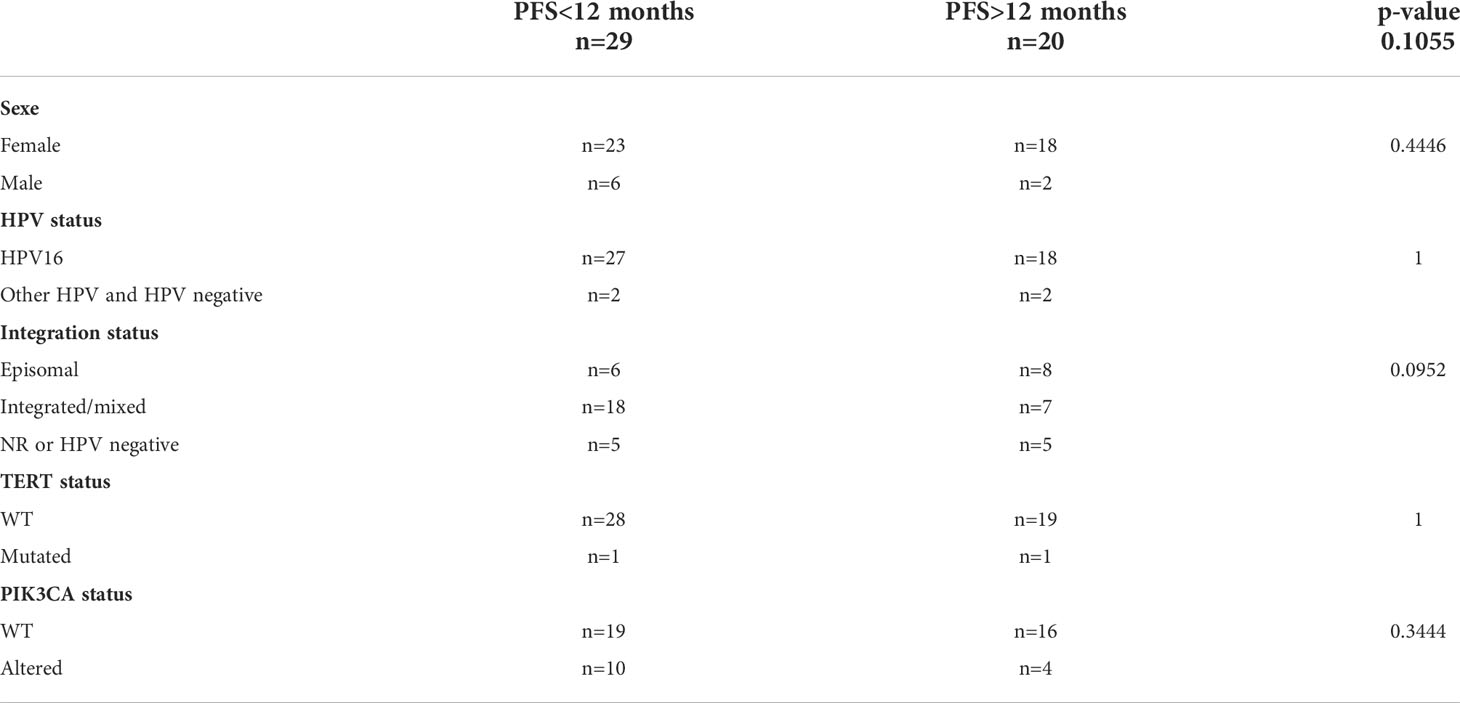
Table 8 Patient characteristics according to time of PFS.
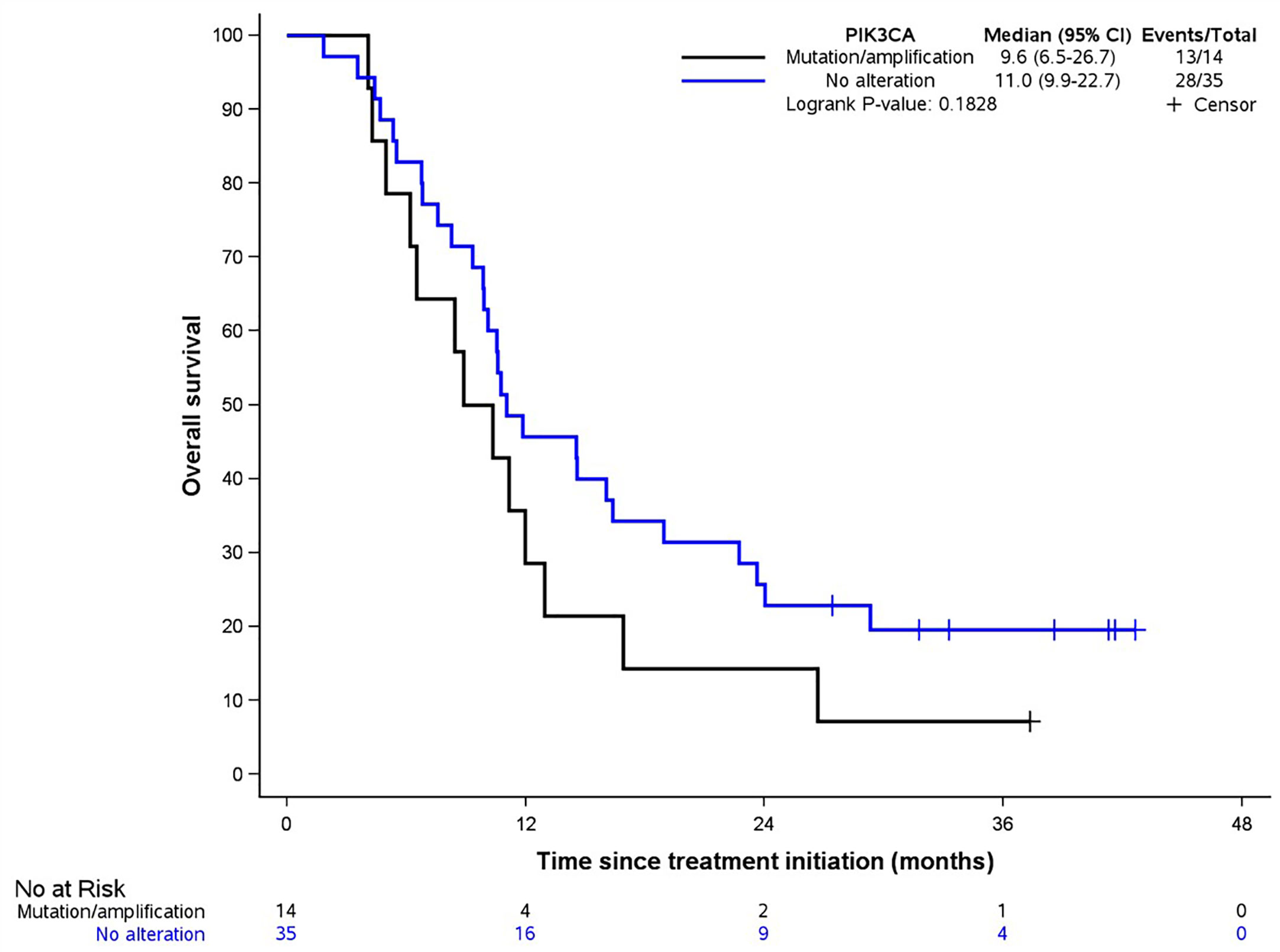
Figure 4 OS in presence of PIK3CA alteration. Blue line symbolizes no alteration, black line symbolizes the presence of a mutation and/or amplification.
Epitopes-HPV02 study was the first prospective clinical trial that included SCCA patients with advanced diseases and demonstrated the ability of Docetaxel-based polychemotherapy to induce long term remissions (15). An ancillary study was performed to analyze the distribution of HPV genotypes, integration status and oncogenic-related alterations in this population.
In our study, a majority of SCCA was HPV positive, mostly HPV16 which is the most frequent high risk type in this disease (24–26). Although HPV-negative SCCA are well-known for being associated with a poor outcome compared to their HPV-positive counterparts (24–26), no significant difference of PFS and OS between HPV-positive and -negative SCCA was observed in the present study, very likely due to the weak number (n=2) of HPV-unrelated samples contained in the present cohort.
Integration of HPV genome into the host genome has been shown to be correlated with disease progression in the context of both anal and cervical (pre-)cancers (21). However, it is important to notice that all HPV-mediated (pre-)cancers do not contain integrated forms of HPV. Indeed, while episomal HPV DNA is observed in the large majority (>90%) of low-grade squamous intraepithelial lesion, it can also be detected in up to 70% of high-grade intraepithelial lesions and invasive carcinoma (depending on both tumor stage and anatomical site) (27). E6 and E7 can be expressed in this case via the inhibition of the binding between E2 and its binding sites (E2BS) at the viral promoter due to the methylation of said E2BS (28). Several mechanisms of viral integration into host genome have been described in the literature (29) but, most often, HPV integration involves a break in the E2 gene, leading to the overexpression of E6 et E7. Integrated/mixed forms were approximately twice more frequent (51% vs 28.6%) in our study compared to episomal forms. Of note, the percentage of “pure” episomal HPV DNA is likely to be slightly overestimated in this study given that, in a minority of cases, HPV could be integrated in host genome without E2 disruption (these latter are actually only detectable by sequencing) (30). Despite this bias, the percentage of integrated/mixed forms in our study composed of relapsing and metastatic SCCA was similar to what can be observed in localized HPV-associated cancers (27). The better PFS observed in the case of patients harboring episomal HPV DNA raises the hypothesis of a predictive impact of HPV integration status on DCF efficacy in advanced SCCA. Further investigations should, however, be undertaken to confirm this observation.
Telomeres are nucleoprotein complexes playing a critical role in chromosome stability. Loss of telomere functions results in genetic instability and impairs cell viability. Telomeric complexes also participate to chromosome repair. Then, telomere nucleoprotein dysfunctions impaired DNA break repair capacities conferring to primary or cancer cells an enhanced sensitivity to ionizing radiation (31). The telomerase is the enzyme reconstituting telomeres and is constituted of several subunits in which the catalytic reverse transcriptase TERT is essential to telomerase activity, conferring in fine cellular immortalization by preventing replicative senescence. TERT promoter mutations are correlated to increased TERT expression and a worse prognosis as confirmed by a recent meta-analysis in glioma patients (32). TERT promoter mutations have been previously identified in glioblastoma (84%), urothelial carcinoma (64.5%), oligodendroglioma (70.0%), medulloblastoma (33.3%) and hepatocellular carcinoma (31.4%) (33). Of note, these mutations were not detected in most gastrointestinal cancers including gastric, cholangiocarcinoma and pancreatic cancers. The C228T and C250T mutations were the most frequent in TERT promoter [77.5% and 20.8% in glioma respectively (34)], inducing a consensus sequence bound by E-Twenty-Six (ETS) transcription factors (35). A similar distribution was observed in our study in TERT mutated SCCA wherein C228T and C250T were detected in 73% and 23.3% of the cases. However, TERT promoter mutation distribution remains scarce in SCCA, even in HPV negative cases where the absence of immortalization by E6 viral oncoprotein could have had an impact on mutational frequency of TERT promoter. Therefore, TERT promoter mutations are not correlated to HPV status, type, nor disease progression. As the EDITH V cohort, composed of localized SCCA, presented the same profile of TERT promoter mutation than the HPV02 cohort composed of metastatic SCCA, TERT promoter mutations also do not appear to be associated to SCCA status.
Furthermore, when analyzing somatic mutations in other genes, it appeared that SCCA were not highly mutated, the most frequently mutated being PIK3CA. This result was similar to others (36–41). In general, most common PIK3CA mutations are E542K and E545K, with 75% for the last one (37, 39). In our study we found 6 mutations in PIK3CA, all being E545K (1633G>A), which is mostly linked to an APOBEC (Apolipoprotein B mRNA editing enzyme catalytic polypeptide-like) alteration (42). As most substitutions (60%, n=6/10) retrieved in our study for all genes were C>T/G>A, it is possible that some of them may in part be due to the activity of APOBEC, creating “passenger mutations” opposed to “driver” to the oncogenesis. Indeed, it has been shown in Head and Neck Squamous Cell Carcinoma (HNSCC) that APOBEC activity and mutations are concordant between viral genome and host cell genome (43). We also found no TP53 mutations in HPV-positive SCCA, as opposed to HPV-negative SCCA (44). Even if mutations were not associated with PFS and OS in our study, we observed a high number of gene amplifications (39 amplifications on tumors of 23 patients), mostly in PIK3CA. Gene amplification could be a consequence of HPV integration into the host genome, as shown elsewhere (45, 46), which could explain the high proportion of this alteration in the present study. Indeed, as HPV genome is integrated into host genome, regions flanking the viral genome are amplified at the same time as HPV genes in a rolling circle manner (47, 48). Six out of ten patients with a PIK3CA amplification presented integrated HPV forms, which was not statistically different, whereas patients with CDK4 and CDKN2A amplifications presented integrated HPV forms in 5/5 and 3/4 cases respectively (p-values: 0.0079 and 0.485 respectively). The fact that HPV integration is sometimes located in or near amplification regions has been shown for other genes, like MYC (45), which is in favor of the impact of viral integration, in late stages of SCCA, on oncogenesis by deregulating oncogenes and mostly amplifying pro-oncogenes.
The main limitation of our study is its small sample size, and the HPV integration status analysis is based in 39 patients. However, to date, this clinical situation is in the scope of active clinical and translational research, and several prospective trials are ongoing (49). More robust confirmatory data are awaited in the near future.
Targeted therapy for patients with HPV-associated cancers resisting to standard treatments are ongoing. Bevacizumab (anti-VEGF antibody) and pembrolizumab (anti-PD1 antibody) were approved in progressive and metastatic cervical cancers (50), and were also evaluated in SCCA, as well as other anti-PD1 antibodies (nivolumab, retifanlimab) (51), and showed a promising result in a subgroup of patients (52–54).
In conclusion, as HPV status, integration status, TERT promoter mutations, and mutational profiling are not significantly correlated to PFS and/or OS in this study, DCF chemotherapy should be proposed to all SCCA patients failing radio-chemotherapy (CRT) or with metastatic disease. Further investigations are required to identify SCCA-related predictive biomarkers.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by The French ethic committee (NCT02402842). The patients/participants provided their written informed consent to participate in this study.
CB, SK, J-LP and DG contributed to conception of the whole study or a part of it, and CB coordinated the clinical trial. AD, DG and PR performed the experiments and CB, AD, MH and AM performed data analysis and/or statistical analysis. AD wrote the first draft of the manuscript and CB, SK, AM and MH wrote sections of the manuscript. FM, LS, AV, AT, AL, ChlM and ChrM allowed data collection. All authors contributed to the article and approved the submitted version.
Part of this work was funded by the Région Franche-Comté and the Belgian Fund for Scientific Research (FNRS; MIS F.4520.20).
The authors would like to thank Guadalupe Inés Tizón for English writing assistance. We also thank the biobank ‘Tumorothèque Régionale de Franche-Comté’ (registration number BB-0033-00024) for biobanking.
CB has received a research grant from companies Bayer and Roche, and was an advisory board member of Bayer, MSD and Pierre Fabre companies. None of them had a role in the study design, analysis, or interpretation of the results.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin (2018) 68(1):7−30. doi: 10.3322/caac.21442
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209−49. doi: 10.3322/caac.21660
3. Islami F, Ferlay J, Lortet-Tieulent J, Bray F, Jemal A. International trends in anal cancer incidence rates. Int J Epidemiol (2017) 46(3):924−38. doi: 1093/ije/dyw276
4. Ghosn M, Kourie HR, Abdayem P, Antoun J, Nasr D. Anal cancer treatment: current status and future perspectives. World J Gastroenterol (2015) 21(8):2294−302. doi: 10.3748/wjg.v21.i8.2294
5. Gunderson LL, Winter KA, Ajani JA, Pedersen JE, Moughan J, Benson AB, et al. Long-term update of US GI intergroup RTOG 98-11 phase III trial for anal carcinoma: Survival, relapse, and colostomy failure with concurrent chemoradiation involving Fluorouracil/Mitomycin versus Fluorouracil/Cisplatin. J Clin Oncol (2012) 30(35):4344−51. doi: 10.1200/JCO.2012.43.8085
6. James RD, Glynne-Jones R, Meadows HM, Cunningham D, Myint AS, Saunders MP, et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): a randomised, phase 3, open-label, 2 × 2 factorial trial. Lancet Oncol (2013) 14(6):516−24. doi: 10.1016/S1470-2045(13)70086-X
7. Peiffert D, Tournier-Rangeard L, Gérard JP, Lemanski C, François E, Giovannini M, et al. Induction chemotherapy and dose intensification of the radiation boost in locally advanced anal canal carcinoma: final analysis of the randomized UNICANCER ACCORD 03 trial. J Clin Oncol (2012) 30(16):1941−8. doi: 10.1200/JCO.2011.35.4837
8. Faivre C, Rougier P, Ducreux M, Mitry E, Lusinchi A, Lasser P, et al. [5-fluorouracile and cisplatinum combination chemotherapy for metastatic squamous-cell anal cancer]. Bull Cancer (1999) 86(10):861−5.
9. NCCN Guidelines. NCCN guidelines [Internet](2021). Available at: https://www.nccn.org/guidelines/guidelines-detail (Accessed 13 déc 2021).
10. Eng C, Chang GJ, You YN, Das P, Rodriguez-Bigas M, Xing Y, et al. The role of systemic chemotherapy and multidisciplinary management in improving the overall survival of patients with metastatic squamous cell carcinoma of the anal canal. Oncotarget (2014) 5(22):11133−42. doi: 10.18632/oncotarget.2563
11. Sclafani F, Morano F, Cunningham D, Baratelli C, Kalaitzaki E, Watkins D, et al. Platinum-fluoropyrimidine and paclitaxel-based chemotherapy in the treatment of advanced anal cancer patients. Oncologist (2017) 22(4):402−8. doi: 10.1634/theoncologist.2016-0241
12. Wahl AF, Donaldson KL, Fairchild C, Lee FY, Foster SA, Demers GW, et al. Loss of normal p53 function confers sensitization to taxol by increasing G2/M arrest and apoptosis. Nat Med (1996) 2(1):72−9. doi: 10.1038/nm0196-72
13. Kim S, Jary M, Mansi L, Benzidane B, Cazorla A, Demarchi M, et al. DCF (docetaxel, cisplatin and 5-fluorouracil) chemotherapy is a promising treatment for recurrent advanced squamous cell anal carcinoma. Ann Oncol (2013) 24(12):3045−50. doi: 10.1093/annonc/mdt396
14. Senovilla L, Vitale I, Martins I, Tailler M, Pailleret C, Michaud M, et al. An immunosurveillance mechanism controls cancer cell ploidy. Science (2012) 337(6102):1678−84. doi: 10.1126/science.1224922
15. Kim S, François E, André T, Samalin E, Jary M, El Hajbi F, et al. Docetaxel, cisplatin, and fluorouracil chemotherapy for metastatic or unresectable locally recurrent anal squamous cell carcinoma (Epitopes-HPV02): a multicentre, single-arm, phase 2 study. Lancet Oncol (2018) 19(8):1094−106. doi: 10.1016/S1470-2045(18)30321-8
16. Kim S, Jary M, André T, Vendrely V, Buecher B, François E, et al. Docetaxel, cisplatin, and 5-fluorouracil (DCF) chemotherapy in the treatment of metastatic or unresectable locally recurrent anal squamous cell carcinoma: a phase II study of French interdisciplinary GERCOR and FFCD groups (Epitopes-HPV02 study). BMC Cancer (2017) 17(1):574. doi: 10.1186/s12885-017-3566-0
17. Kim S, Meurisse A, Spehner L, Stouvenot M, François E, Buecher B, et al. Pooled analysis of 115 patients from updated data of epitopes-HPV01 and epitopes-HPV02 studies in first-line advanced anal squamous cell carcinoma. Ther Adv Med Oncol (2020) 12:175883592097535. doi: 10.1177/1758835920975356
18. Abramowitz L, Jacquard AC, Jaroud F, Haesebaert J, Siproudhis L, Pradat P, et al. Human papillomavirus genotype distribution in anal cancer in France: the EDiTH V study. Int J Cancer (2011) 129(2):433−9. doi: 10.1002/ijc.25671
19. Bretagne CH, Jooste V, Guenat D, Riethmuller D, Bouvier AM, Bedgedjian I, et al. Prevalence and distribution of HPV genotypes and cervical-associated lesions in sexually active young French women following HPV vaccine. J Gynecol Obstetrics Hum Reproduction (2018) 47(10):525−31. doi: 10.1016/j.jogoh.2018.05.011
20. Nagao S, Yoshinouchi M, Miyagi Y, Hongo A, Kodama J, Itoh S, et al. Rapid and sensitive detection of physical status of human papillomavirus type 16 DNA by quantitative real-time PCR. J Clin Microbiol (2002) 40(3):863−7. doi: 10.1128/JCM.40.3.863-867.2002
21. Cricca M, Morselli-Labate AM, Venturoli S, Ambretti S, Gentilomi GA, Gallinella G, et al. Viral DNA load, physical status and E2/E6 ratio as markers to grade HPV16 positive women for high-grade cervical lesions. Gynecol Oncol (2007) 106(3):549−57. doi: 10.1016/j.ygyno.2007.05.004
22. Ye J, Coulouris G, Zaretskaya I, Cutcutache I, Rozen S, Madden TL. Primer-BLAST: A tool to design target-specific primers for polymerase chain reaction. BMC Bioinf (2012) 13:134. doi: 10.1186/1471-2105-13-134
23. Liu X, Yuan H, Fu B, Disbrow GL, Apolinario T, Tomaić V, et al. The E6AP ubiquitin ligase is required for transactivation of the hTERT promoter by the human papillomavirus E6 oncoprotein*. J Biol Chem (2005) 280(11):10807−16. doi: 10.1074/jbc.M410343200
24. Serup-Hansen E, Linnemann D, Skovrider-Ruminski W, Høgdall E, Geertsen PF, Havsteen H. Human papillomavirus genotyping and p16 expression as prognostic factors for patients with American joint committee on cancer stages I to III carcinoma of the anal canal. J Clin Oncol (2014) 32(17):1812−7. doi: 10.1200/JCO.2013.52.3464
25. Meulendijks D, Tomasoa NB, Dewit L, Smits PHM, Bakker R, van Velthuysen MLF, et al. HPV-negative squamous cell carcinoma of the anal canal is unresponsive to standard treatment and frequently carries disruptive mutations in TP53. Br J Cancer (2015) 112(8):1358−66. doi: 10.1038/bjc.2015.20
26. Bruyere D, Monnien F, Colpart P, Roncarati P, Vuitton L, Hendrick E, et al. Treatment algorithm and prognostic factors for patients with stage I-III carcinoma of the anal canal: a 20-year multicenter study. Mod Pathol (2021) 34(1):116−30. doi: 10.1038/s41379-020-0637-6
27. Shulzhenko N, Lyng H, Sanson GF, Morgun A. Ménage à trois: an evolutionary interplay between human papillomavirus, a tumor, and a woman. Trends Microbiol (2014) 22(6):345−53. doi: 10.1016/j.tim.2014.02.009
28. Jacquin E, Baraquin A, Ramanah R, Carcopino X, Morel A, Valmary-Degano S, et al. Methylation of human papillomavirus type 16 CpG sites at E2-binding site 1 (E2BS1), E2BS2, and the Sp1-binding site in cervical cancer samples as determined by high-resolution melting analysis–PCR. J Clin Microbiol (2013) 51(10):3207−15. doi: 10.1128/JCM.01106-13
29. Kamal M, Lameiras S, Deloger M, Morel A, Vacher S, Lecerf C, et al. Human papilloma virus (HPV) integration signature in cervical cancer: identification of MACROD2 gene as HPV hot spot integration site. Br J Cancer (2021) 124(4):777−85. doi: 10.1038/s41416-020-01153-4
30. Holmes A, Lameiras S, Jeannot E, Marie Y, Castera L, Sastre-Garau X, et al. Mechanistic signatures of HPV insertions in cervical carcinomas. NPJ Genom Med 16 mars (2016) 1:16004. doi: 10.1038/npjgenmed.2016.4
31. Wong KK, Chang S, Weiler SR, Ganesan S, Chaudhuri J, Zhu C, et al. Telomere dysfunction impairs DNA repair and enhances sensitivity to ionizing radiation. Nat Genet (2000) 26(1):85−8. doi: 10.1038/79232
32. Wang X, Li X, Xu F, Zhang Y, Liu H, Tao Y. Association of telomerase reverse transcriptase promoter mutations with the prognosis of glioma patients: a meta-analysis. Mol Neurobiol (2016) 53(4):2726−32. doi: 10.1007/s12035-015-9400-2
33. Huang DS, Wang Z, He XJ, Diplas BH, Yang R, Killela PJ, et al. Recurrent TERT promoter mutations identified in a large-scale study of multiple tumor types are associated with increased TERT expression and telomerase activation. Eur J Cancer (2015) 51(8):969−76. doi: 10.1016/j.ejca.2015.03.010
34. Killela PJ, Reitman ZJ, Jiao Y, Bettegowda C, Agrawal N, Diaz LA, et al. TERT promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal. Proc Natl Acad Sci U S A (2013) 110(15):6021−6. doi: 10.1073/pnas.1303607110
35. Heidenreich B, Kumar R. TERT promoter mutations in telomere biology. Mutat Res Rev Mutat Res (2017) 771:15−31. doi: 10.1016/j.mrrev.2016.11.002
36. Cacheux W, Dangles-Marie V, Rouleau E, Lazartigues J, Girard E, Briaux A, et al. Exome sequencing reveals aberrant signalling pathways as hallmark of treatment-naive anal squamous cell carcinoma. Oncotarget (2017) 9(1):464−76. doi: 10.18632/oncotarget.23066
37. Koncar RF, Feldman R, Bahassi EM, Hashemi Sadraei N. Comparative molecular profiling of HPV-induced squamous cell carcinomas. Cancer Med (2017) 6(7):1673−85. doi: 10.1002/cam4.1108
38. Mondaca S, Chatila WK, Bates D, Hechtman JF, Cercek A, Segal NH, et al. FOLFCIS treatment and genomic correlates of response in advanced anal squamous cell cancer. Clin Colorectal Cancer (2019) 18(1):e39−52. doi: 10.1016/j.clcc.2018.09.005
39. Morris V, Rao X, Pickering C, Foo WC, Rashid A, Eterovic K, et al. Comprehensive genomic profiling of metastatic squamous cell carcinoma of the anal canal. Mol Cancer Res (2017) 15(11):1542−50. doi: 10.1158/1541-7786.MCR-17-0060
40. Mouw KW, Cleary JM, Reardon B, Pike J, Braunstein LZ, Kim J, et al. Genomic evolution after chemoradiotherapy in anal squamous cell carcinoma. Clin Cancer Res (2017) 23(12):3214−22. doi: 10.1158/1078-0432.CCR-16-2017
41. Smaglo BG, Tesfaye A, Halfdanarson TR, Meyer JE, Wang J, Gatalica Z, et al. Comprehensive multiplatform biomarker analysis of 199 anal squamous cell carcinomas. Oncotarget (2015) 6(41):43594−604. doi: 10.18632/oncotarget.6202
42. Henderson S, Chakravarthy A, Su X, Boshoff C, Fenton TR. APOBEC-mediated cytosine deamination links PIK3CA helical domain mutations to human papillomavirus-driven tumor development. Cell Rep (2014) 7(6):1833−41. doi: 10.1016/j.celrep.2014.05.012
43. Faden DL, Kuhs KAL, Lin M, Langenbucher A, Pinheiro M, Yeager M, et al. APOBEC mutagenesis is concordant between tumor and viral genomes in HPV-positive head and neck squamous cell carcinoma. Viruses (2021) 13(8):1666. doi: 10.3390/v13081666
44. Armstrong SA, Malley R, Wang H, Lenz HJ, Arguello D, El-Deiry WS, et al. Molecular characterization of squamous cell carcinoma of the anal canal. J Gastrointest Oncol (2021) 12(5):2423−37. doi: 10.21037/jgo-20-610
45. Aldersley J, Lorenz DR, Mouw KW, D’Andrea AD, Gabuzda D. Genomic landscape of primary and recurrent anal squamous cell carcinomas in relation to HPV integration, copy-number variation, and DNA damage response genes. Mol Cancer Res (2021) 19(8):1308−21. doi: 10.1158/1541-7786.MCR-20-0884
46. McBride AA, Warburton A. The role of integration in oncogenic progression of HPV-associated cancers. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5383336/ (Accessed 23 févr 2021).
47. Pinatti LM, Walline HM, Carey TE. Human papillomavirus genome integration and head and neck cancer. J Dent Res (2018) 97(6):691−700. doi: 10.1177/0022034517744213
48. Akagi K, Li J, Broutian TR, Padilla-Nash H, Xiao W, Jiang B, et al. Genome-wide analysis of HPV integration in human cancers reveals recurrent, focal genomic instability. Genome Res (2014) 24(2):185−99. doi: 10.1101/gr.164806.113
49. Spehner L, Boustani J, Cabel L, Doyen J, Vienot A, Borg C, et al. Present and future research on anal squamous cell carcinoma. Cancers (2021) 13(15):3895. doi: 10.3390/cancers13153895
50. Cohen AC, Roane BM, Leath CA. Novel therapeutics for recurrent cervical cancer: Moving towards personalized therapy. Drugs (2020) 80(3):217−27. doi: 10.1007/s40265-019-01249-z
51. Farias JPF, Rangel da Silva MHC, Jácome AA. Emerging and experimental agents for anal cancer: What is new? J Exp Pharmacol (2021) 13:433−40. doi: 10.2147/JEP.S262342
52. Rao S, Anandappa G, Capdevila J, Dahan L, Evesque L, Kim S, et al. A phase II study of retifanlimab (INCMGA00012) in patients with squamous carcinoma of the anal canal who have progressed following platinum-based chemotherapy (POD1UM-202)☆. ESMO Open [Internet] 7(4). https://www.esmoopen.com/article/S2059-7029(22)00150-8/fulltext. doi: 10.1016/j.esmoop.2022.100529
53. Marabelle A, Cassier PA, Fakih M, Kao S, Nielsen D, Italiano A, et al. Pembrolizumab for previously treated advanced anal squamous cell carcinoma: results from the non-randomised, multicohort, multicentre, phase 2 KEYNOTE-158 study. Lancet Gastroenterol Hepatol (2022) 7(5):446−54. doi: 10.1016/S2468-1253(21)00382-4
Keywords: NGS - next generation sequencing, SCCA, Somatic mutation analysis, TERT promoter mutation, HPV integration
Citation: Debernardi A, Meurisse A, Prétet J-L, Guenat D, Monnien F, Spehner L, Vienot A, Roncarati P, André T, Abramowitz L, Molimard C, Mougin C, Herfs M, Kim S and Borg C (2022) Prognostic role of HPV integration status and molecular profile in advanced anal carcinoma: An ancillary study to the epitopes-HPV02 trial. Front. Oncol. 12:941676. doi: 10.3389/fonc.2022.941676
Received: 11 May 2022; Accepted: 20 September 2022;
Published: 14 October 2022.
Edited by:
Sridhar Muthusami, Karpagam Academy of Higher Education, IndiaReviewed by:
Ulrike Wieland, University Hospital of Cologne, GermanyCopyright © 2022 Debernardi, Meurisse, Prétet, Guenat, Monnien, Spehner, Vienot, Roncarati, André, Abramowitz, Molimard, Mougin, Herfs, Kim and Borg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christophe Borg, Y2hyaXN0b3BoZS5ib3JnQHVuaXYtZmNvbXRlLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.