 Hainan Yang1†
Hainan Yang1† Lei Wen2†
Lei Wen2† Chao Zhao1
Chao Zhao1 Xuefei Li1
Xuefei Li1 Changguo Shan2Da Liu3Weiping Hong2
Changguo Shan2Da Liu3Weiping Hong2 Zhaoming Zhou2
Zhaoming Zhou2 Cheng Zhou2Linbo Cai2*Caicun Zhou1*
Cheng Zhou2Linbo Cai2*Caicun Zhou1*- 1Department of Oncology, Shanghai Pulmonary Hospital and Thoracic Cancer Institute, School of Medicine, Tongji University, Shanghai, China
- 2Department of Oncology, Guangdong Sanjiu Brain Hospital, Guangzhou, China
- 3Department of Neurosurgery, Guangdong Sanjiu Brain Hospital, Guangzhou, China
Background: Leptomeningeal metastases (LM) have become increasingly common in non-small cell lung cancer (NSCLC) patients who harbor epidermal growth factor receptor (EGFR) mutation treated with EGFR-TKI and are correlated with inferior prognosis. Evidence in prior research demonstrated that EGFR amplification was more likely presented in advanced clinical stages and was associated with worse survival. However, whether EGFR amplification is a prognostic marker in NSCLC–LM is still inconclusive.
Methods: This study enrolled patients diagnosed with NSCLC–LM from June 2019 to September 2021 and who had received previous EGFR-TKI at Guangdong Sanjiu Brain Hospital. Cerebrospinal fluid (CSF) samples were collected and subjected to targeted next-generation sequencing of 168 cancer-related genes. Clinical characteristics and overall survival (OS) were compared in patients with and without EGFR amplification.
Results: This study enrolled 53 NSCLC–LM patients, all of whom had EGFR mutations. TP53 and EGFR amplifications are the two most frequent mutations in the study cohort, presenting at 72% (38 of 53) and 40% (21 of 53), respectively. The rate of EGFR amplification was much higher at the time of leptomeningeal progression than at initial diagnosis (p < 0.01). Karnoskfy performance status was poorer (p = 0.021), and CSF pressure was higher (p = 0.0067) in patients with EGFR amplification than those without. A multivariable Cox proportional hazard regression model showed that EGFR amplification was an independent prognostic factor for poorer OS (8.3 vs. 15 months; p = 0.017). The median OS was shorter in NSCLC–LM patients with mutated TP53 than those with wild-type TP53, but the difference was not statistically significant (10 vs. 17.3 months, p = 0.184).
Conclusions: EGFR gene amplification could be a potential resistance mechanism to EGFR-TKI failure in NSCLC–LM and is associated with inferior clinical outcomes.
Introduction
Lung cancer is one of the most frequently diagnosed types of cancer (1). Although the 5-year overall survival (OS) rate for patients at all stages of lung cancer is 19%, most patients are diagnosed with advanced-stage disease, with the latter patients having a 5-year OS rate of only 3% (2, 3). The development of epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) has significantly prolonged the survival of selected patients who harbor EGFR mutations when compared with platinum-based combination chemotherapy (4, 5). However, the efficacy of EGFR-TKIs is likely limited by innate or acquired resistance. Osimertinib is a third-generation EGFR-TKI designed to overcome the resistance to other TKIs of tumors harboring EGFR-T790M (6, 7). The median progression-free survival (PFS) was 9.6 months for patients who were EGFR T790-positive and who had a progressive disease after a previous TKI treatment (8).
Leptomeningeal metastases (LM) of lung cancer have been associated with poor prognosis. LM has been observed in 9.4% of patients with EGFR mutation, compared with 1.7% of patients without EGFR mutations (9). Osimertinib has been shown to penetrate the blood–brain barrier in animal models (10) and has shown promising therapeutic efficacy in NSCLC–LM patients resistant to prior EGFR-TKI therapy (11). Resistance to osimertinib develops over time, although the potential resistance mechanism remains unclear. EGFR protein overexpression was much higher in metastatic lesions than in primary tumors, with high gene copy numbers indicating tumor progression (12). The association between EGFR amplification and prognosis in patients with NSCLC–LM has not been determined.
Patients and methods
Patients
The present study included 53 patients diagnosed with NSCLC–LM who were enrolled between June 2019 and September 2021 at Guangdong Sanjiu Brain Hospital. LM was diagnosed based on enhanced MRI results showing a linear or micronodular pial enhancement, as assessed by two experienced radiologists, or the detection of tumor cells in cerebrospinal fluid (CSF) samples. The patients were divided into groups, one with and the other without EGFR amplification.
Methods
Approximately 10 ml of CSF was obtained from each patient through a lumbar puncture at the time of leptomeningeal progression. Targeted next-generation sequencing (NGS) was performed to detect somatic mutations in a panel of 168 cancer-related genes. Genomic profiles were assessed using the core panel from Burning Rock Biotech (Guangzhou, China). Cytology findings, opening pressure of CSF, and Karnoskfy performance status (KPS) score were evaluated by the treating physician. The protocol of this study was approved by the Research Ethics Committee of Guangdong Three Nine Brain Hospital.
Statistical analysis
Continuous variables were reported as arithmetic medians or means and categorical variables as proportions with 95% confidence intervals (CIs). Differences between patients with and without EGFR amplification were evaluated by Pearson chi-square test, Fisher’s exact test, or Wilcoxon test. OS, defined as the time period from the date of diagnosis of LM to the date of death or last follow-up, was assessed by the Kaplan–Meier method and compared by log-rank tests. Statistical analyses were performed using SPSS 21, Graph Pad Prism 6, and R version 4.1.2 software, with p <0.05 defined as statistically significant.
Results
Clinicopathologic features of patients with NSCLC–LM
A total of 53 NSCLC patients with leptomeningeal progression were enrolled in this study, including 21 (40%) with and 32 (60%) without EGFR gene amplification. The demographic and clinical characteristics, mutation profiles, and treatment history of these patients are summarized in Table 1. The median age of the 53 patients was 56 years (range, 36 to 74 years) and was similar in the patients with (median age, 51 years; range, 38 to 72 years) and without (median age, 56.5 years; range, 36 to 74 years) EGFR amplification. The 53 patients included 24 (45%) women, with similar percentages in patients with (43%; 9/21) and without (47%; 15/32) EGFR amplification. The median KPS was 70 (range, 30–90) and was significantly lower in patients with than those without EGFR amplification (p = 0.021).
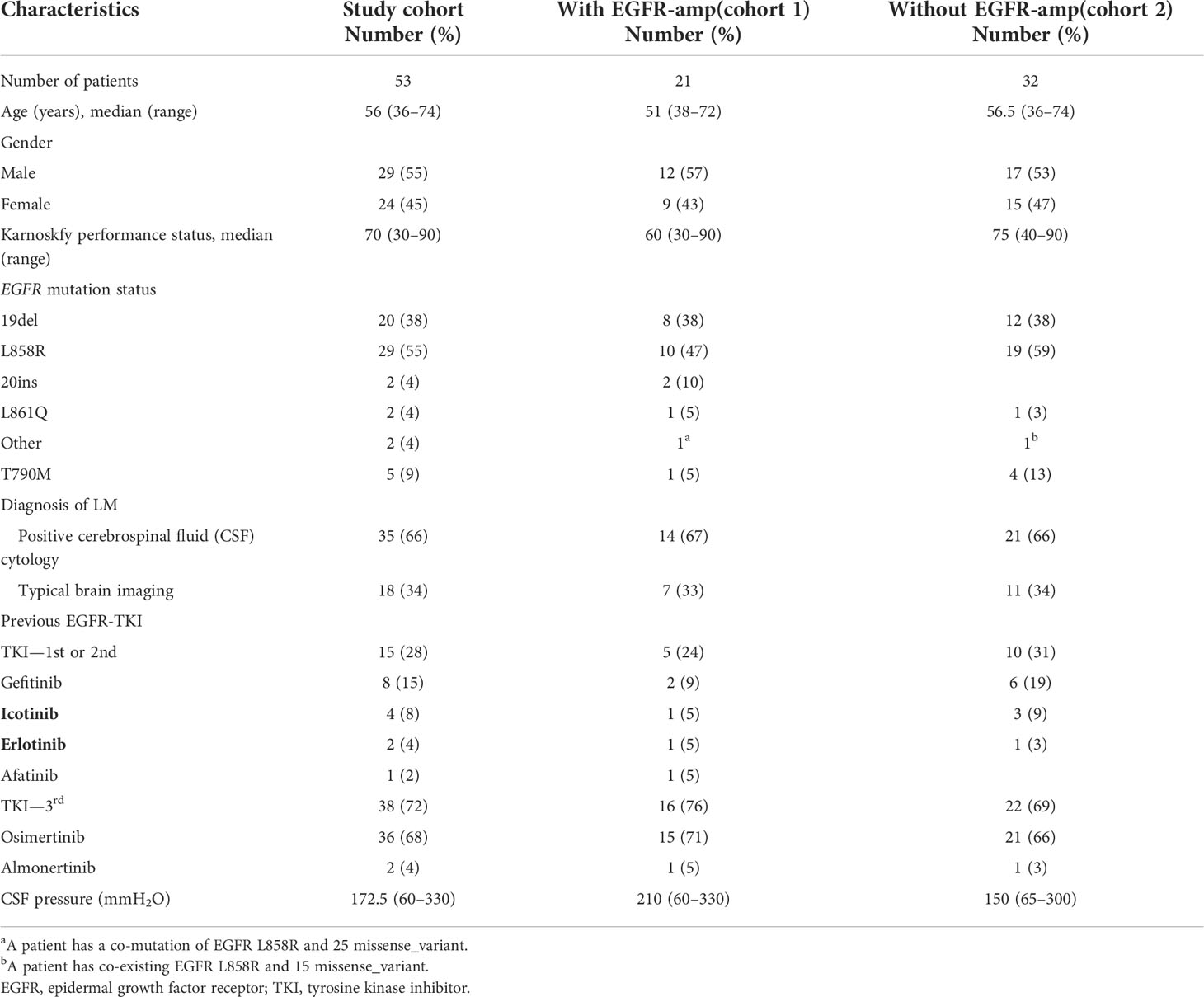
Table 1 Clinical characteristics of 53 non-small cell lung cancer–leptomeningeal metastases (LM) patients with EGFR mutation.
A total of 55 EGFR mutations were detected in the 53 patients. Twenty-nine patients, 10 with and 19 without EGFR amplification, had L858R mutations in exon 21; 20 (8 and 12, respectively) had deletions in exon 19, two (one in each group) had L861Q mutations in exon 21, and two, both with EGFR amplifications, had insertions in exon 20. Two patients had coexisting EGFR mutations: one, with an EGFR amplification, had the L858R mutation and a 25 missense_variant, and the other, without an EGFR amplification, had the L858R and a 15 missense_variant. Thirty-five (66%) patients had positive cytology in CSF samples, and all 53 had been treated with EGFR TKIs, including 38 (72%) who had received a third-generation TKI. The median CSF pressure was 172.5 mmH2O (range, 60–330 mmH2O) and was significantly higher in patients with (210 mmH2O; range, 60–330 mmH2O) than those without (150 mmH2O; range, 65–300 mmH2O) EGFR amplification (p = 0.0067).
Gene profiling of CSF samples from NSCLC–LM patients
NGS at the time of LM showed EGFR mutations in 100% of the 53 CSF ctDNA samples, including L858R mutations in 29 (55%), exon 19 deletions in 20 (38%), exon 20 insertions in two (4%), and L861Q mutations in two (4%). TP53 mutations and EGFR amplification were the two most frequent alterations in the study cohort, being present in 38 (72%) and 21 (40%) patients, respectively. In addition, CDKN2A, PMS2, and CCNE1 mutations were detected in 16 (30%), 10 (19%), and seven (13%) patients, respectively. The rate of EGFR amplification was found to be higher in patients resistant to icotinib/gefitinib (13), with the present study finding that the rate of EGFR amplification was higher in patients treated with a third-generation TKI (42%, 16/38) than those treated with a first- or second-generation TKI (33%, 5/15). Moreover, patients with EGFR variants co-existing with CDK4, CDK6, and MYC mutations had poorer outcomes than those with EGFR variants alone (14). Of the 53 patients in this study, 10 (19%) had CDK4 mutations in CSF samples, whereas three (6%) each had CDK6 and MYC mutations (Figure 1).
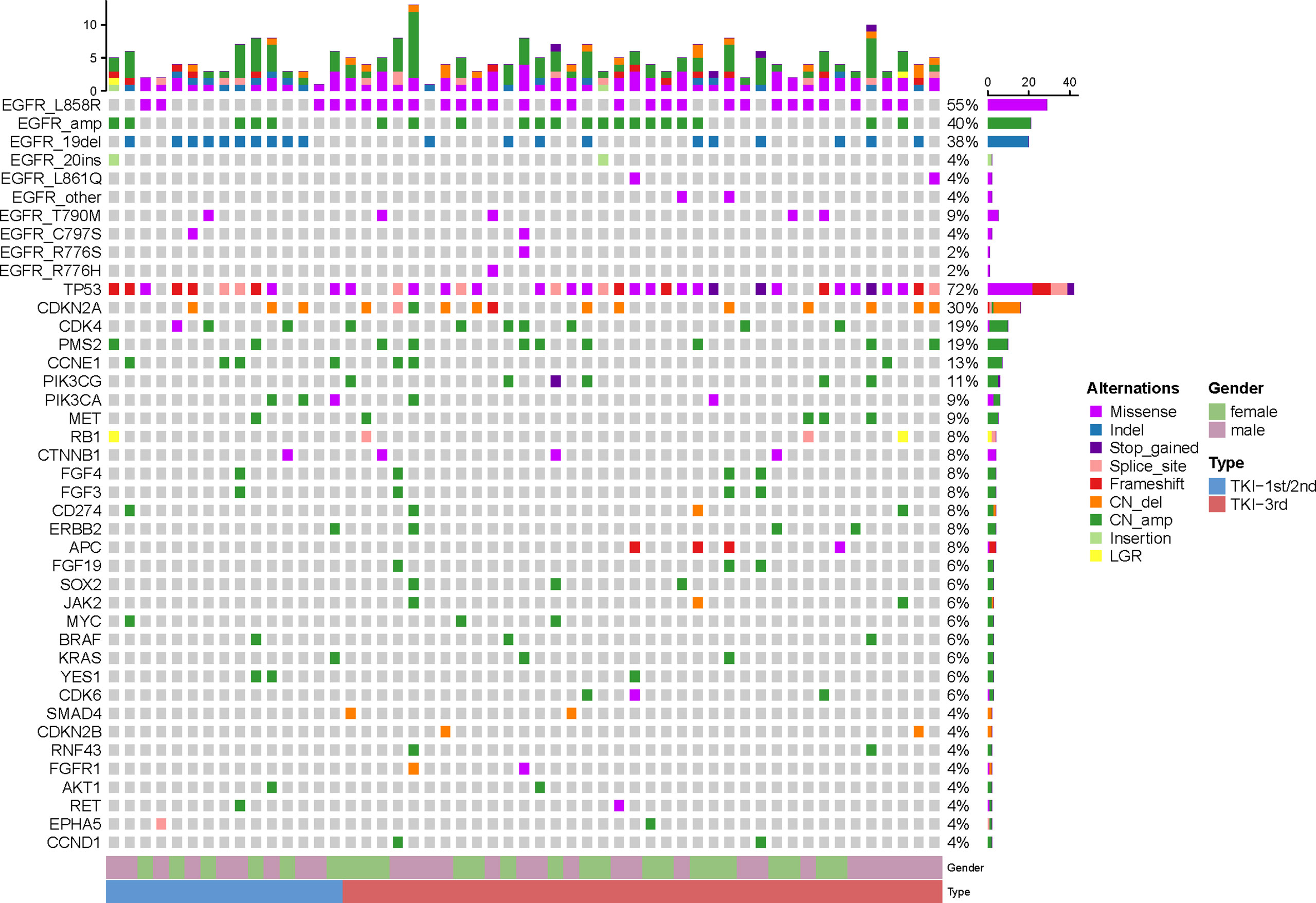
Figure 1 Next-generation sequencing results of 53 cerebrospinal fluid samples taken from non-small cell lung cancer patients with leptomeningeal metastases. The top bar shows the overall number of mutations in each patient. The right-side bar shows the percentage of patients harboring a specific mutation. Different colors denote different types of mutation. The bottom bar denotes patients grouped by gender or previous epidermal growth factor receptor tyrosine kinase inhibitor treatment history.
An evaluation of mechanisms conferring resistance to EGFR-TKIs (Table 2) showed that the EGFR T790M and C797S mutations were present in five (9%) and two (4%) patients, respectively. In addition, five patients (9%) had MET mutations, four (8%) each had RB1, ERBB2, and CTNNB1 mutations, and three (6%) had KRAS and BRAF mutations. The rates of detection of mutations in the RB1, ERBB2, CTNNB1, BRAF, and KRAS genes were similar in patients who have previously been treated with a third-generation TKI or a first- or second-generation TKI. In contrast, the detection rate of CCNE1 mutations was about threefold higher in patients treated with a first- or second-generation than in those treated with a third-generation TKI (27 vs. 8%), indicating that CCNE1 mutations may confer resistance to first- and second-generation TKIs. Conversely, the rates of detection of EGFR T790M and MET mutations were higher in patients treated with a third-generation TKI than those with a first- or second-generation TKI (11%, 4/38 vs. 7% 1/15 for both). In addition, mutations in FGF19, CCND1, and SOX2 were detected only in patients treated with a third-generation TKI. Interestingly, NGS showed that seven patients have not less than three different mutation genes, and among them, three patients have not less than four mutation genes (Table 2).
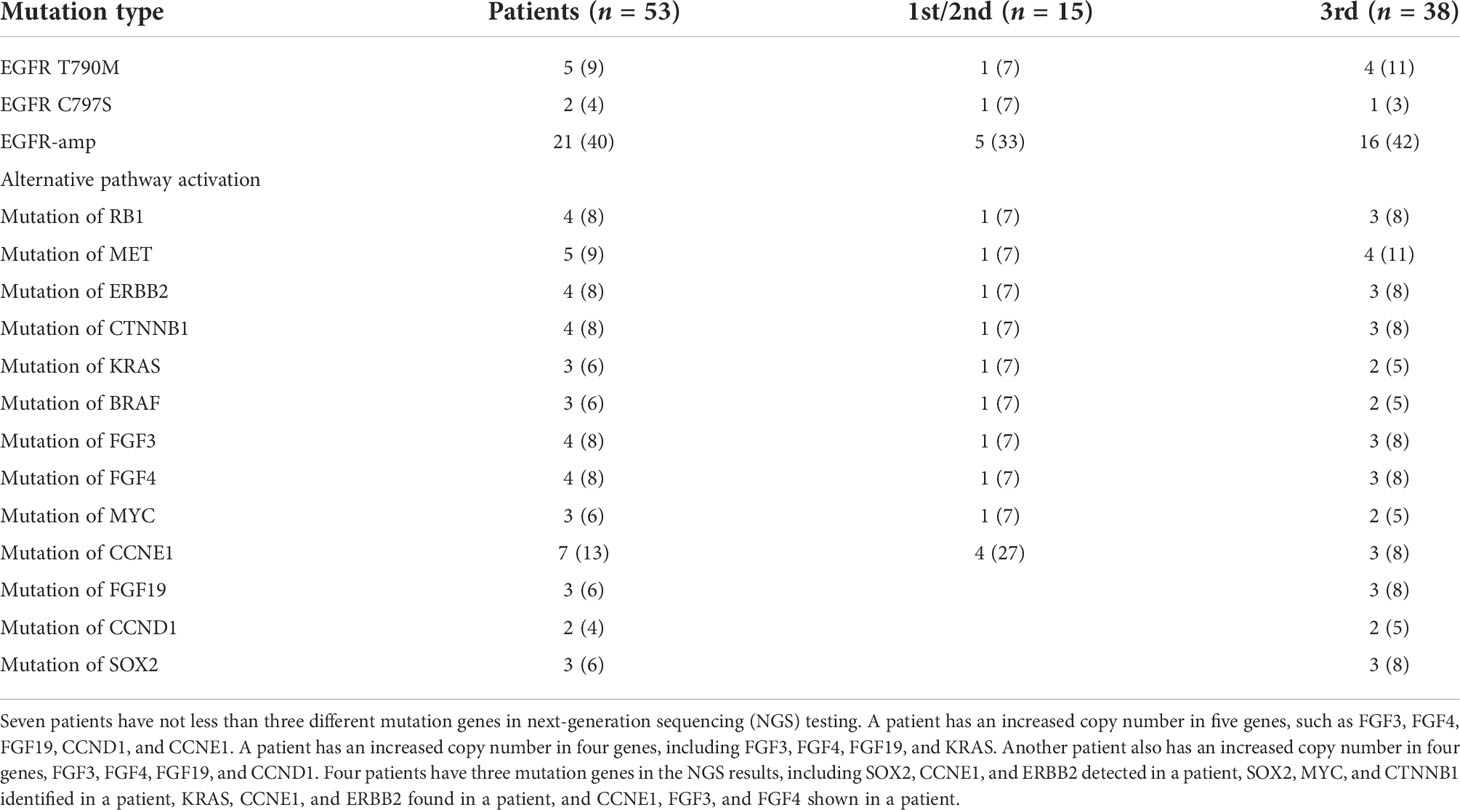
Table 2 Potential resistance mechanism to EGFR-TKI in non-small cell lung cancer–leptomeningeal metastases.
Comparison of characteristics in patients with and without EGFR amplification
To identify the putative resistance mechanism to EGFR-TKI, we reasoned that gene aberrations should be absent from or have a low detection rate before treatment, with emergence or a high detection rate at progression. The initial gene profiles of 50 (94%) of the 53 patients showed that the detection rate of EGFR amplification was much higher at the time of leptomeningeal progression than at initial diagnosis (p < 0.01) (Figure 2A). This finding indicated that EGFR amplification could be associated with tumor progression in NSCLC patients with LM.
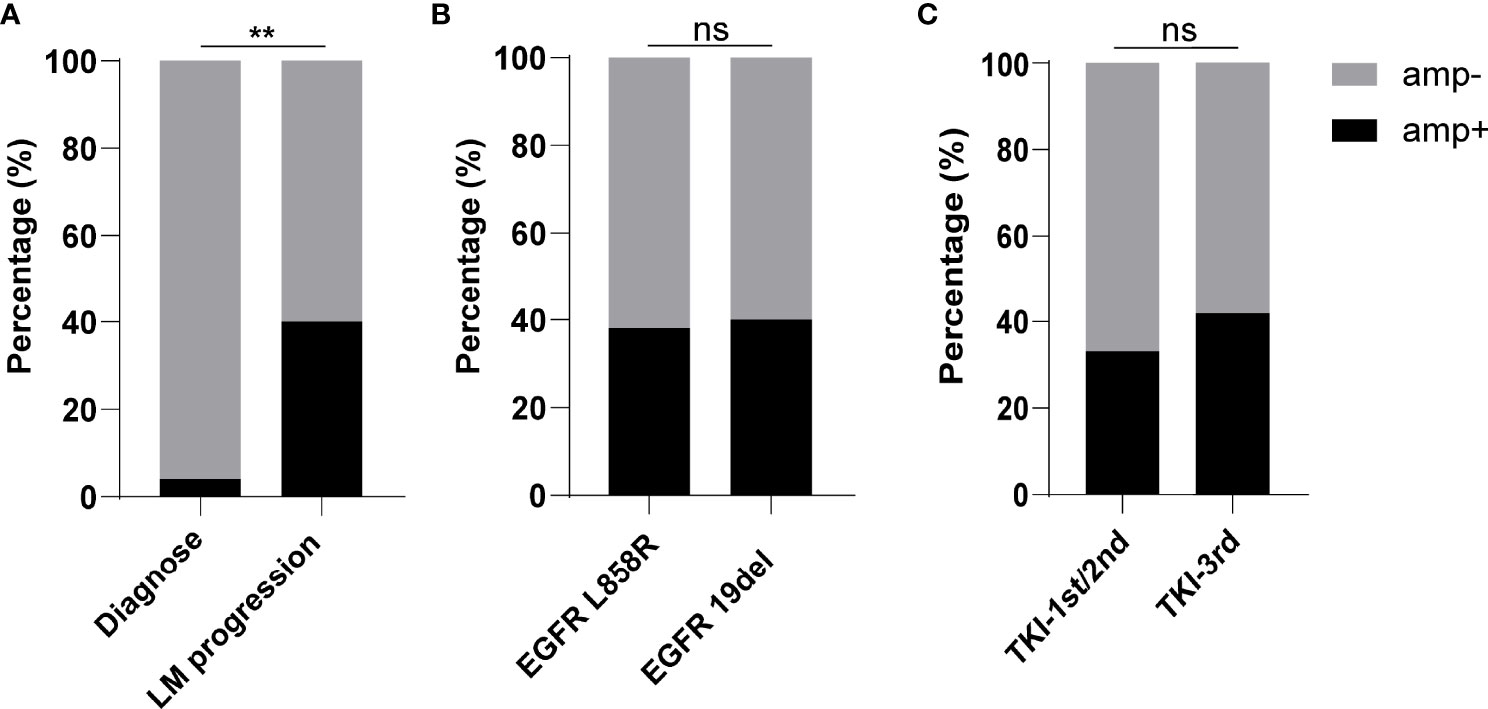
Figure 2 Characteristics of patients with or without epidermal growth factor receptor (EGFR) amplification. (A) Rate of detection of EGFR amplification at the time of initial diagnosis or leptomeningeal progression. (B) Rate of EGFR amplification in non-small cell lung cancer–leptomeningeal metastases patients harboring EGFR L858R or EGFR 19del. (C) Rate of EGFR amplification in patients previously treated with a first- or second-generation tyrosine kinase inhibitor (TKI) or a third-generation TKI. ** demonstrated p<0.01, and ns indicated no significance.
Deletions in exon 19 (19del) and mutations in exon 21 (L858R) are the two most common EGFR mutations. Although the rates of EGFR amplification were reported higher in lung adenocarcinoma patients with 19del than those with L858R mutations (15, 16), the present study found that EGFR amplification was present at similar percentages, being detected in 40% (8/20) of patients with 19del and 35% (10/29) of patients with L858R mutations (Figure 2B).
EGFR amplification is frequent in patients with acquired resistance to first- and second-generation TKIs (13), but less is known about the rate of amplification in patients resistant to third-generation TKIs. An evaluation of the clinical characteristics showed that the rate of EGFR amplification was slightly higher in patients treated with a third-generation than those with a first- or second-generation TKI, but the difference was not statistically significant (Figure 2C).
EGFR amplification correlates with poorer prognosis
The Kaplan–Meier analysis showed that the median OS was significantly shorter in patients with than those without EGFR amplification (8.3 vs. 15 months, p = 0.017, Figure 3A). The KPS scores were also significantly lower in patients with than those without EGFR amplification (p = 0.021, Figure 4A). The median CSF opening pressure was significantly higher in patients with than those without EGFR amplification (p = 0.0067, Figure 4B). In addition, open CSF pressure at or above the upper limit of the normal CSF range (80–180 mmH2O) was detected in 74% (14/19) of patients with but in only 31% (9/29) of patients without EGFR amplification. Moreover, Kaplan-Meier analysis showed that median OS was significantly shorter in patients with than without EGFR amplification (8.3 vs 15 months, p =0.017, Figure 4A).
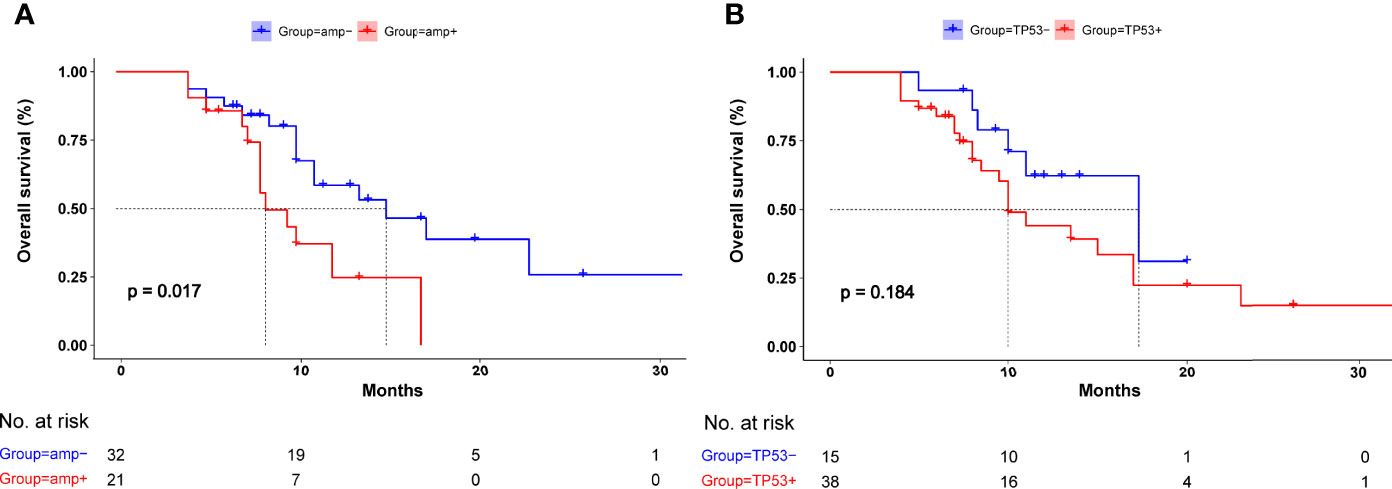
Figure 3 Kaplan–Meier analysis of overall survival in patients with and without (A) epidermal growth factor receptor (EGFR) amplification and (B) TP53 mutation. (A) Median overall survival was significantly poorer in patients with than those without EGFR amplification (p = 0.017). (B) Median overall survival was similar in patients with and without TP53 mutation.
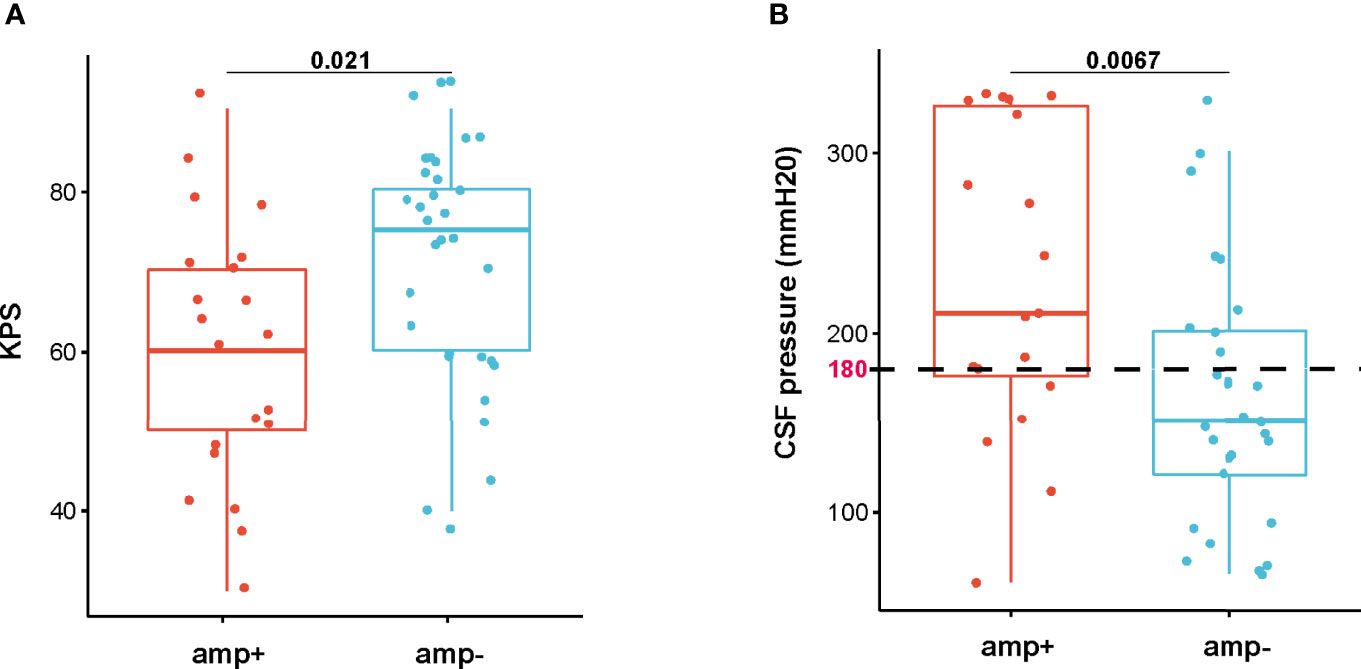
Figure 4 Distribution of (A) Karnoskfy performance status scores and (B) cerebrospinal fluid pressure in patients with and without epidermal growth factor receptor amplification.
An evaluation of the effect of TP53 mutation and OS showed that the median OS was shorter in NSCLC–LM patients with mutated than those with wild-type TP53, although the difference was not statistically significant (10 vs. 17.3 months, p = 0.184, Figure 3B).
Discussion
LM has become increasingly common in NSCLC patients harboring EGFR mutations and treated with EGFR-TKIs (17). The median OS in LM patients with EGFR mutations was found to be 8.9 months (95% CI: 7.2–10.7 months) (9). The potential mechanisms associated with poor prognosis remain unclear. EGFR amplification has been associated with significantly poorer outcomes in lung adenocarcinoma patients (15). Moreover, in addition to the EGFR T790M mutation, the rate of EGFR amplification was higher in patients with drug resistance than those with drug sensitivity (40 vs. 0%) (13). EGFR overexpression and high gene copy numbers have been associated with tumor progression in lung adenocarcinoma treated with EGFR inhibitors (12). Moreover, EGFR amplification is more likely to occur at advanced clinical stages and be associated with poorer disease-free survival (15). However, whether EGFR amplification is a prognostic marker in NSCLC–LM remains undetermined.
Previous research demonstrated that TP53 was the most frequently mutated gene in CSF samples obtained from NSCLC patients with CNS metastases (14), and a similar study of NSCLC–LM patients who experienced disease progression on osimertinib also found that TP53 was the most frequently detected concurrent gene in the CSF and that EGFR amplification and C797S mutation were also observed (18), shedding light on the potential resistance mechanisms among NSCLC–LM patients treated with EGFR-TKIs.
The present study compared 21 patients with EGFR mutations and concurrent EGFR amplification with 32 patients with EGFR mutations without concurrent EGFR amplification to assess the prognostic value of EGFR amplification in NSCLC–LM patients treated with EGFR-TKIs. OS was significantly shorter in patients with than those without EGFR amplification (p = 0.017). Moreover, patients with both EGFR and a co-mutation of amplification were more likely to have a poorer KPS score (p = 0.021) and a higher CSF pressure (p = 0.0067) than patients with a mutation but without EGFR amplification.
OS has also been reported as shorter in lung adenocarcinoma patients with than those without TP53 mutations, and in patients with both TP53 and EGFR mutations than in those lacking both (19). PFS was shown to be significantly longer in patients with mutated EGFR and wild-type TP53 than in patients with mutations in both genes (19 vs. 6.5 months, p = 0.035) 20). TP53 was also the most frequently mutated co-occurring gene in our study cohort, being present in 72% of patients, with the median OS being shorter in NSCLC–LM patients with mutated than wild-type TP53, although the difference was not statistically significant (p = 0.184).
The TP53 mutations were detected in 90% (19/21) of patients with and 59% (19/32) patients without EGFR amplification. To exclude the influence of TP53 mutation on the result of this study, we performed a multivariate analysis to assess the prognostic significance of EGFR amplification. Univariable and multivariable Cox proportional hazard regression analyses were performed to assess the effects on survival of alterations in the TP53, CDKN2A, CDK4, PMS2, CCNE1, and PIK3CG genes, which all had a detection rate above 10% in the study cohort. The univariable analysis showed that EGFR amplification (p = 0.017) and CDKN2A mutation (p = 0.019) were significant predictors of OS, with multivariable analysis confirming that EGFR amplification [hazard ratio (HR), 2.63; 95% confidence interval (CI), 1.18–5.86; p = 0.018] and CDKN2A (HR, 2.61; 95% CI, 1.17–5.84; p = 0.019) were independent adverse predictors of OS. These findings indicate that EGFR amplification is an independent predictor of reduced OS, regardless of other genetic variations (Table 3).
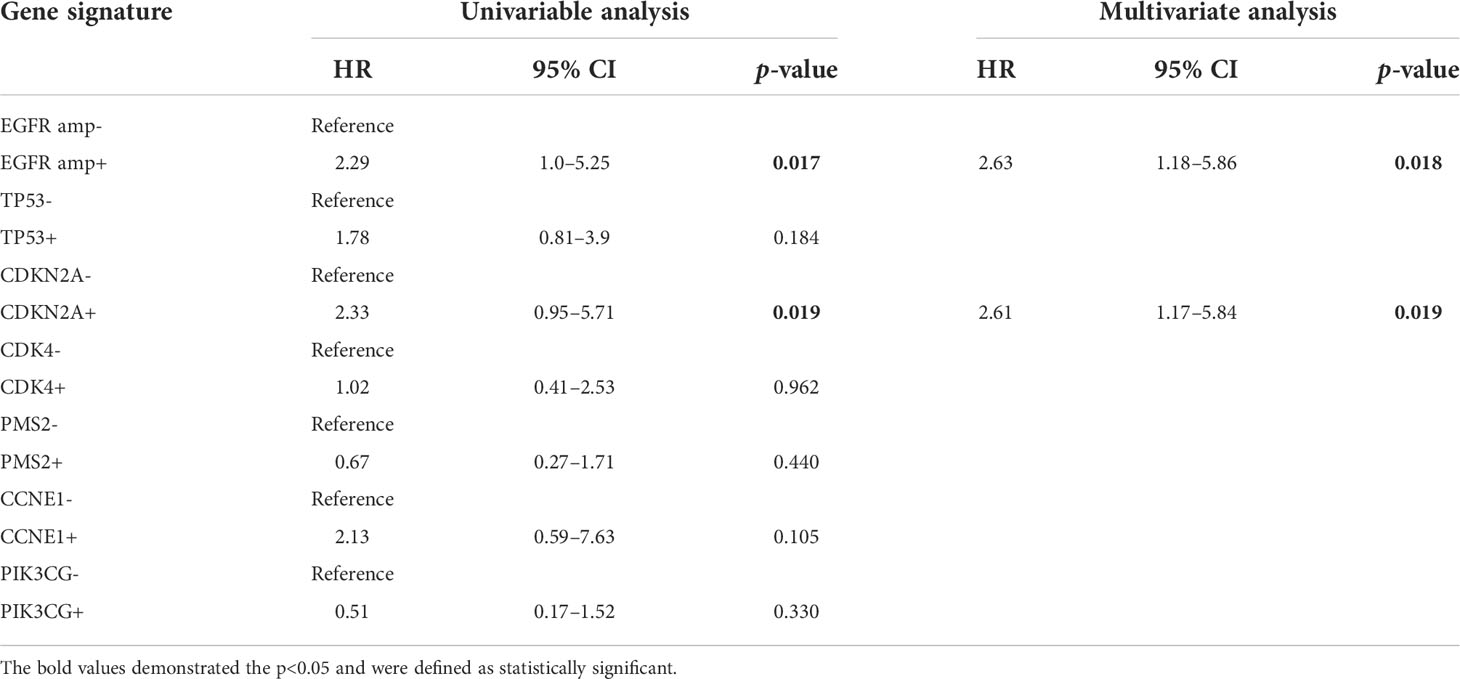
Table 3 Univariable and multivariable analyses of gene signature detected in not less than 10% of the study cohort, and the results shown were obtained by performing the Cox regression model (N = 53).
Additional coexisting mutations and the proportion of EGFR mutations can affect PFS (21), and immunohistochemical analyses of tumor tissue from NSCLC patients treated with first-line EGFR-TKIs have shown that co-occurring PTEN loss and IGFR overexpression correlated with poorer PFS and OS (22). In addition, the proapoptotic protein BIM and the negatively regulated apoptosis element of mTOR may account for the variable response of NSCLC patients to EGFR TKI therapy (23). These findings indicate that additional genetic alterations can affect the prognosis of patients treated with EGFR TKIs.
Evidence from prior research had shown that anti-EGFR antibody nimotuzumab could increase HLA class I expression in tumor cell lines (24), and another study found similar results showing that nimotuzumab can enhance NK cell activation and DC maturation and increase EGFR-specific T cell (25). A preclinical study found that, in vitro, nimotuzumab can enhance the radiotherapy effect in human esophageal squamous cell carcinoma cells, and this finding was also confirmed in cell xenografts, showing that radiation combined with nimotuzumab was correlated with tumor growth delay in contrast to radiation alone (26). Preclinical data have suggested that nimotuzumab enhances the antitumor activity, and evidence from several clinical trials further confirmed these findings. A phase 3 clinical trial in locally advanced head and neck cancer indicated that the addition of nimotuzumab could improve PFS when compared to the same schedule with weekly cisplatin (27). A similar research has also shown that adding another EGFR monoclonal antibody cetuximab indicated increased survival in advanced non-small-cell lung cancer patients compared with chemotherapy alone (28). Given the results showing a synergistic effect of nimotuzumab and chemotherapy or radiotherapy, it might be a choice to add nimotuzumab to treat NSCLC with LM.
In summary, the findings of this study demonstrate that, within a subset of EGFR-mutated NSCLC patients with LM, EGFR gene amplification is more likely to occur at the LM stage than at initial diagnosis. Moreover, EGFR gene amplification was associated with lower KPS and poorer OS. These findings suggested that EGFR gene amplification may be responsible for the resistance of NSCLC–LM patients to EGFR-TKIs, and the addition of nimotuzumab will be another choice for the treatment of EGFR-mutated NSCLC patients with LM.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Research Ethics Committee of Guangdong Three Nine Brain Hospital. The patients/participants provided their written informed consent to participate in this study.
Author contributions
HY, LW, and CS designed the experiments and wrote the manuscript. DL, WH, and XL helped in reviewing, acquiring, analyzing, and interpreting of clinical data for the work. ZZ and ChaZ did the statistical analysis. CheZ, LC, and CaZ critically revised the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the National Natural Science Foundation of China (no. 81871865), Natural Science Foundation of Guangdong Province (no. 2019A1515011943), Shanghai Science and Technology Committee Foundation (no. 19411950300), Shanghai Public Health Committee Foundation (NO. 2020CXJQ02) and Medical Scientific Research Foundation of Guangdong Province (no. B2021139). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2018) 68:394–424. doi: 10.3322/caac.21492
2. Barnet MB, O'toole S, Horvath LG, Selinger C, Yu B, Ng CC, et al. EGFR-Co-Mutated advanced NSCLC and response to EGFR tyrosine kinase inhibitors. J Thorac Oncol (2017) 12:585–90. doi: 10.1016/j.jtho.2016.09.001
3. Siegel RL, Miller KD, Jemal A. Cancer statistic. CA Cancer J Clin (2019) 69:7–34. doi: 10.3322/caac.21551
4. Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol (2010) 11:121–8. doi: 10.1016/S1470-2045(09)70364-X
5. Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol (2011) 12:735–42. doi: 10.1016/S1470-2045(11)70184-X
6. Pao W, Miller VA, Politi KA, Riely GJ, Somwar R, Zakowski MF, et al. Acquired resistance of lung adenocarcinomas to gefitinib or erlotinib is associated with a second mutation in the EGFR kinase domain. PloS Med (2005) 2:e73. doi: 10.1371/journal.pmed.0020073
7. Cross DA, Ashton SE, Ghiorghiu S, Eberlein C, Nebhan CA, Spitzler PJ, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discovery (2014) 4:1046–61. doi: 10.1158/2159-8290.CD-14-0337
8. Jänne PA, Yang JC, Kim DW, Planchard D, Ohe Y, Ramalingam SS, et al. AZD9291 in EGFR inhibitor-resistant non-small-cell lung cancer. N Engl J Med (2015) 372:1689–99. doi: 10.1056/NEJMoa1411817
9. Li YS, Jiang BY, Yang JJ, Tu HY, Zhou Q, Guo WB, et al. Leptomeningeal metastases in patients with NSCLC with EGFR mutations. J Thorac Oncol (2016) 11:1962–9. doi: 10.1016/j.jtho.2016.06.029
10. Ballard P, Yates JW, Yang Z, Kim DW, Yang JC, Cantarini M, et al. Preclinical comparison of osimertinib with other EGFR-TKIs in EGFR-mutant NSCLC brain metastases models, and early evidence of clinical brain metastases activity. Clin Cancer Res (2016) 22:5130–40. doi: 10.1158/1078-0432.CCR-16-0399
11. Yang JCH, Kim SW, Kim DW, Lee JS, Cho BC, Ahn JS, et al. Osimertinib in patients with epidermal growth factor receptor mutation-positive non-Small-Cell lung cancer and leptomeningeal metastases: The BLOOM study. J Clin Oncol (2020) 38:538–47. doi: 10.1200/JCO.19.00457
12. Tang X, Varella-Garcia M, Xavier AC, Massarelli E, Ozburn N, Moran C, et al. Epidermal growth factor receptor abnormalities in the pathogenesis and progression of lung adenocarcinomas. Cancer Prev Res (Phila) (2008) 1:192–200. doi: 10.1158/1940-6207.CAPR-08-0032
13. Shang Y, Li X, Liu W, Shi X, Yuan S, Huo R, et al. Comprehensive genomic profile of Chinese lung cancer patients and mutation characteristics of individuals resistant to icotinib/gefitinib. Sci Rep (2020) 10:20243. doi: 10.1038/s41598-020-76791-y
14. Li YS, Zheng MM, Jiang BY, Tu HY, Yang JJ, Zhang XC, et al. Association of cerebrospinal fluid tumor DNA genotyping with survival among patients with lung adenocarcinoma and central nervous system metastases. JAMA Netw Open (2020) 3:e209077. doi: 10.1001/jamanetworkopen.2020.9077
15. Sholl LM, Yeap BY, Iafrate AJ, Holmes-Tisch AJ, Chou YP, Wu MT, et al. Lung adenocarcinoma with EGFR amplification has distinct clinicopathologic and molecular features in never-smokers. Cancer Res (2009) 69:8341–8. doi: 10.1158/0008-5472.CAN-09-2477
16. Ruiz-Patiño A, Castro CD, Ricaurte LM, Cardona AF, Rojas L, Zatarain-Barrón ZL, et al. EGFR amplification and sensitizing mutations correlate with survival in lung adenocarcinoma patients treated with erlotinib (MutP-CLICaP). Target Oncol (2018) 13:621–9. doi: 10.1007/s11523-018-0594-x
17. Lee Y, Han JY, Kim HT, Yun T, Lee GK, Kim HY, et al. Impact of EGFR tyrosine kinase inhibitors versus chemotherapy on the development of leptomeningeal metastasis in never smokers with advanced adenocarcinoma of the lung. J Neurooncol (2013) 115:95–101. doi: 10.1007/s11060-013-1199-y
18. Zheng MM, Li YS, Tu HY, Jiang BY, Yang JJ, Zhou Q, et al. Genotyping of cerebrospinal fluid associated with osimertinib response and resistance for leptomeningeal metastases in EGFR-mutated NSCLC. J Thorac Oncol (2021) 16:250–8. doi: 10.1016/j.jtho.2020.10.008
19. Wang F, Zhao N, Gao G, Deng HB, Wang ZH, Deng LL, et al. Prognostic value of TP53 co-mutation status combined with EGFR mutation in patients with lung adenocarcinoma. J Cancer Res Clin Oncol (2020) 146:2851–9. doi: 10.1007/s00432-020-03340-5
20. Vanderlaan PA, Rangachari D, Mockus SM, Spotlow V, Reddi HV, Malcolm J, et al. Mutations in TP53, PIK3CA, PTEN and other genes in EGFR mutated lung cancers: Correlation with clinical outcomes. Lung Cancer (2017) 106:17–21. doi: 10.1016/j.lungcan.2017.01.011
21. Bria E, Pilotto S, Amato E, Fassan M, Novello S, Peretti U, et al. Molecular heterogeneity assessment by next-generation sequencing and response to gefitinib of EGFR mutant advanced lung adenocarcinoma. Oncotarget (2015) 6:12783–95. doi: 10.18632/oncotarget.3727
22. Ferrara MG, Martini M, D'argento E, Forcella C, Vita E, Di Noia V, et al. PTEN loss as a predictor of tumor heterogeneity and poor prognosis in patients with EGFR-mutant advanced non-small-cell lung cancer receiving tyrosine kinase inhibitors. Clin Lung Cancer (2021) 22:351–60. doi: 10.1016/j.cllc.2020.12.008
23. Karachaliou N, Codony-Servat J, Teixidó C, Pilotto S, Drozdowskyj A, Codony-Servat C, et al. BIM and mTOR expression levels predict outcome to erlotinib in EGFR-mutant non-small-cell lung cancer. Sci Rep (2015) 5:17499. doi: 10.1038/srep17499
24. Garrido G, Rabasa A, Garrido C, Chao L, Garrido F, García-Lora Á M, et al. Upregulation of HLA class I expression on tumor cells by the anti-EGFR antibody nimotuzumab. Front Pharmacol (2017) 8:595. doi: 10.3389/fphar.2017.00595
25. Mazorra Z, Lavastida A, Concha-Benavente F, Valdés A, Srivastava RM, García-Bates TM, et al. Nimotuzumab induces NK cell activation, cytotoxicity, dendritic cell maturation and expansion of EGFR-specific T cells in head and neck cancer patients. Front Pharmacol (2017) 8:382. doi: 10.3389/fphar.2017.00382
26. Zhao L, He LR, Xi M, Cai MY, Shen JX, Li QQ, et al. Nimotuzumab promotes radiosensitivity of EGFR-overexpression esophageal squamous cell carcinoma cells by upregulating IGFBP-3. J Transl Med (2012) 10:249. doi: 10.1186/1479-5876-10-249
27. Patil VM, Noronha V, Joshi A, Agarwal J, Ghosh-Laskar S, Budrukkar A, et al. A randomized phase 3 trial comparing nimotuzumab plus cisplatin chemoradiotherapy versus cisplatin chemoradiotherapy alone in locally advanced head and neck cancer. Cancer (2019) 125:3184–97. doi: 10.1002/cncr.32179
Keywords: non-small cell lung cancer, cerebrospinal fluid, leptomeningeal metastases, EGFR gene amplification, EGFR-TKI
Citation: Yang H, Wen L, Zhao C, Li X, Shan C, Liu D, Hong W, Zhou Z, Zhou C, Cai L and Zhou C (2022) EGFR amplification is a putative resistance mechanism for NSCLC–LM patients with TKI therapy and is associated with poor outcome. Front. Oncol. 12:902664. doi: 10.3389/fonc.2022.902664
Received: 23 March 2022; Accepted: 28 June 2022;
Published: 01 August 2022.
Edited by:
Dario de Biase, University of Bologna, ItalyReviewed by:
Emilio Bria, Comprehensive Cancer Center, Fondazione, Policlinico Universitario Agostino Gemelli, Università Cattolica del Sacro Cuore (IRCCS), ItalyHelei Hou, The Affiliated Hospital of Qingdao University, China
Copyright © 2022 Yang, Wen, Zhao, Li, Shan, Liu, Hong, Zhou, Zhou, Cai and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Linbo Cai, Y2FpbGluYm85OTlAMTYzLmNvbQ==; Caicun Zhou, ZHJfY2FpY3VuemhvdUAxMjYuY29t
†These authors have contributed equally to this work