 Tao Ouyang
Tao Ouyang Xuefeng Kan1,2†
Xuefeng Kan1,2†- 1Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
- 2Hubei Province Key Laboratory of Molecular Imaging, Wuhan, China
Hepatocellular carcinoma (HCC) is an important cause of cancer death and is considered the 3rd most lethal around the world. Hepatectomy, liver transplantation, and ablation therapy are considered curative treatments for early-stage HCC. Transarterial chemoembolization is the preferred therapy for intermediate stage HCC. Ssystemic therapy is recommended for advanced HCC. For more than a decade, sorafenib and lenvatinib were used as the first-line treatment for the advanced HCC. For the great success of immunotherapy in melanoma and lung cancer, some immune-based treatments, such as immune checkpoint inhibitors (ICIs), have been applied in the treatment of HCC. The anti-programmed cell death protein 1 (PD1) antibodies, including nivolumab and pembrolizumab, have been approved by the Food and Drug Administration for sorafenib-pretreated patients. Moreover, due to the results of durable antitumor responses attained from the phase 3 trials, atezolizumab in combination with bevacizumab is now the standard therapy for advanced HCC. Recently, there are a lot of clinical trials involving the ICIs, as monotherapy or combination therapy, with tyrosine kinase inhibitors, antiangiogenic drugs, cytotoxic agents, and locoregional treatments, providing a promising outcome for advanced HCC. Thus, this review summarized the role of ICIs for HCC patients with monotherapy or combination therapy. The success and failures of monotherapy and combination therapy involving ICIs have provided advanced insights into HCC treatment and led to novel avenues to improve therapy efficacy in HCC.
Introduction
Hepatocellular carcinoma (HCC) accounts for more than 90% of primary liver cancers and is the third leading cause of cancer-related lethal (1). Based on the Barcelona Clinic Liver Cancer staging (2), hepatectomy, liver transplantation, and ablation therapy were the curative therapies for early-stage HCC. Transarterial chemoembolization (TACE) is the standard treatment for intermediate-stage HCC, and systemic therapy was recommended for advanced HCC (3). Molecular targeted agents played an crucial role in the systemic therapy of advanced HCC. In 2007, based on the results of SHARP trial (NCT00105443) (4) and ORIENTAL trial (NCT00492752) (5), sorafenib, an small molecule multikinase inhibitor, was approved as the preferred therapy for unresectable HCC. Since that, great effort has been made in the research of novel targeted therapy drugs. In 2017, for the promising outcomes of RESORCE study (NCT01774344) (6), regorafenib, a small molecule multitarget inhibitor, was approved for second-line treatment of HCC. Furthermore, some clinical studies for advanced HCC obtained promising outcomes, resulting in the approval of lenvatinib (7) as preferred therapy, and cabozantinib (8) and ramucirumab (9) as second-line therapy for advanced HCC. However, these targeted agents generally have the characteristics of a lower response rate, a high treatment resistance, and frequent adverse events in the systemic therapy for advanced HCC patients (10).
Immune checkpoint inhibitors (ICIs), including the programmed death-1 (PD-1) and the programmed death-ligand 1 (PD-L1), have exhibited potential therapeutic effects for advanced HCC (11–13). Based on the survival efficacy from the results of phase II clinical trials, anti-PD1 inhibitors nivolumab and pembrolizumab were approved as the subsequent-line treatment for unresectable HCC (14, 15). However, the overall response rate (ORR) of nivolumab or pembrolizumab for advanced HCC was 15-20% (16). In order to improve the therapeutic effect of ICIs for HCC, a large number of register clinical trials on the combination treatment with ICIs are being carried out. In 2020, with the positive results obtained from the IMbrave150 study (NCT03434379) (17), atezolizumab (PD-L1 inhibitors) combined with bevacizumab (anti-VEGF agent) has been approved as the preferred therapy for advanced HCC.
To date, numerous clinical trials evaluating the therapeutic effects of ICIs for advanced HCC, including monotherapy and combination therapy. Therefore, in this review, we summarized the development and progress of immune checkpoint-based therapy for advanced HCC based on the completed and ongoing clinical trials around the world, and pointed out the possible future directions for the development of HCC therapeutic drugs.
Immune Checkpoint Inhibitors for HCC
The liver continuous exposed to over-stimulation, including hepatitis B virus or hepatitis C virus, aflatoxins, and alcohol, which can lead to pathological inflammation, immune system disorders, and destruction of tissue homeostasis, resulting in liver fibrosis, cirrhosis, and even development of cancer (18). HCC is a typical inflammation-related cancer, and the chronic inflammation enhances the tumor immunogenicity and evades the host immune surveillance (19–21). A series of cytokines, chemokines, and growth factors involved in the occurrence and progression of HCC, and the IL-6, IL-1β, and TGF-β are the major cytokines (22, 23). In addition, hepatic sinusoidal endothelial cells (LSECs) and regulatory T cell (Treg) release high levels of immunosuppressive cytokines, resulting in an immunosuppressive microenvironment of the liver, and a large number of immune checkpoint molecules expressed on immune cells (24–28).
Immune checkpoints are intrinsic to the immune system to prevent autoreactivity (Figure 1). PD-1, a co-inhibitory receptor molecule, which is mainly expressed in CD4+ T cells or antigen presenting cells, plays a vital role in regulating peripheral immune tolerance (29–31). PD-L1 is overexpressed on dendritic cells, macrophages, and liver parenchymal cells (32). The interaction of PD-1 and PD-L1 is one of the important mechanisms of tumor immune escape (33, 34). Moreover, the immune inhibitory molecule CTLA-4 are greatly expressed on highly activated Treg cells in the livers (35). The use of immune checkpoint inhibitors is a promising therapeutic to promote immunotherapy in the treatment of cancer, which could block immune checkpoint molecules and reactivate immune responses in the tumor microenvironment (36). To date, the approved ICIs in the treatment of HCC included the anti-PD1 inhibitors nivolumab and pembrolizumab, the anti-PDL1 inhibitor atezolizumab, and the anti-CTLA-4 ipilimumab (Figure 2). The monotherapy (Table 1) or combination therapy (Table 2) involving ICIs for HCC have made a clinical breakthrough.
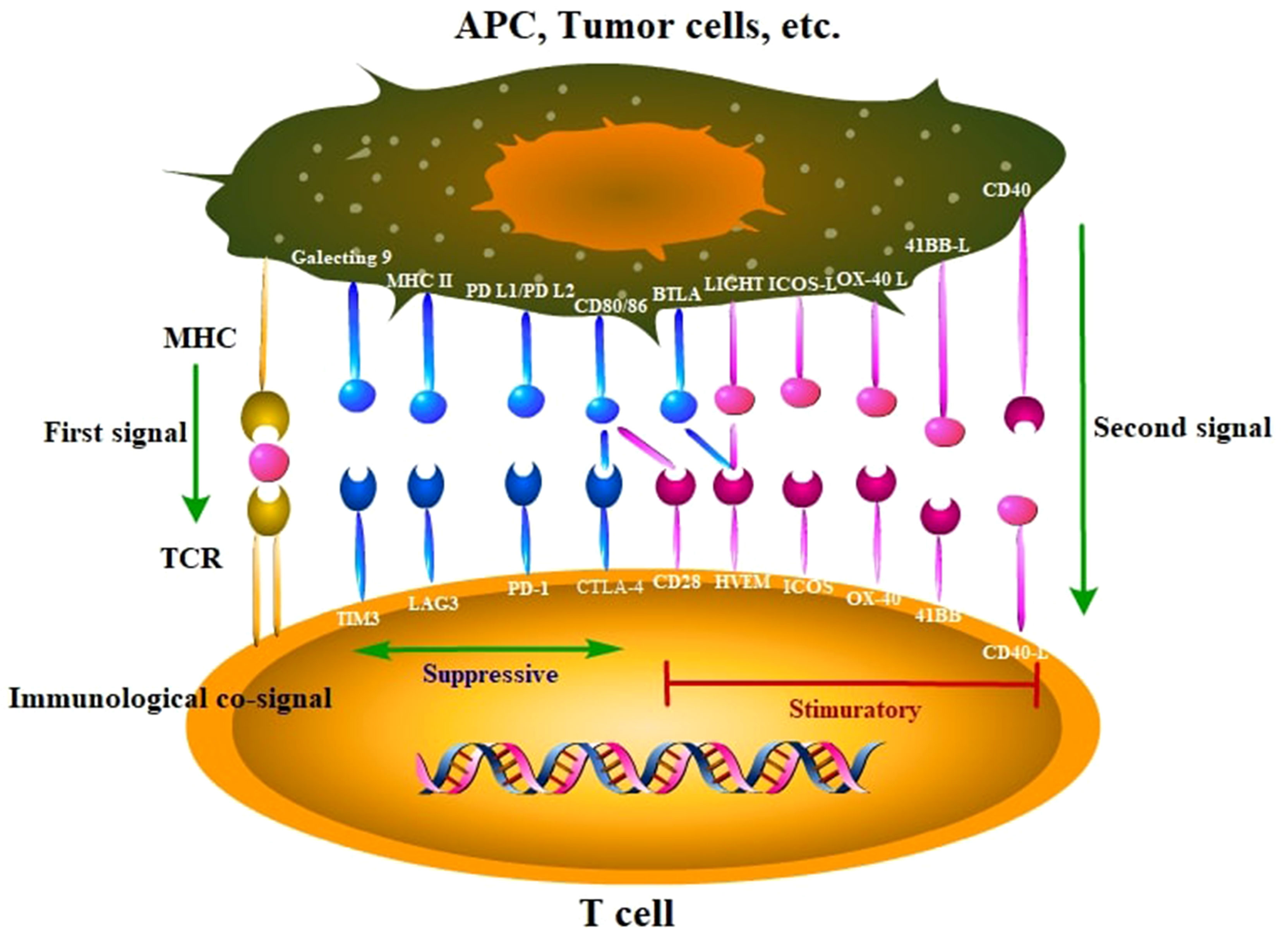
Figure 1 Main immune molecules and corresponding receptors that suppressive or stimulatory immune responses. These ligands and cognate receptors expressed in tumor cells and immune cells are known as immune checkpoints. APC, antigen presenting cell; MHC, major histocompatibility complex; TCR, T-cell receptor.
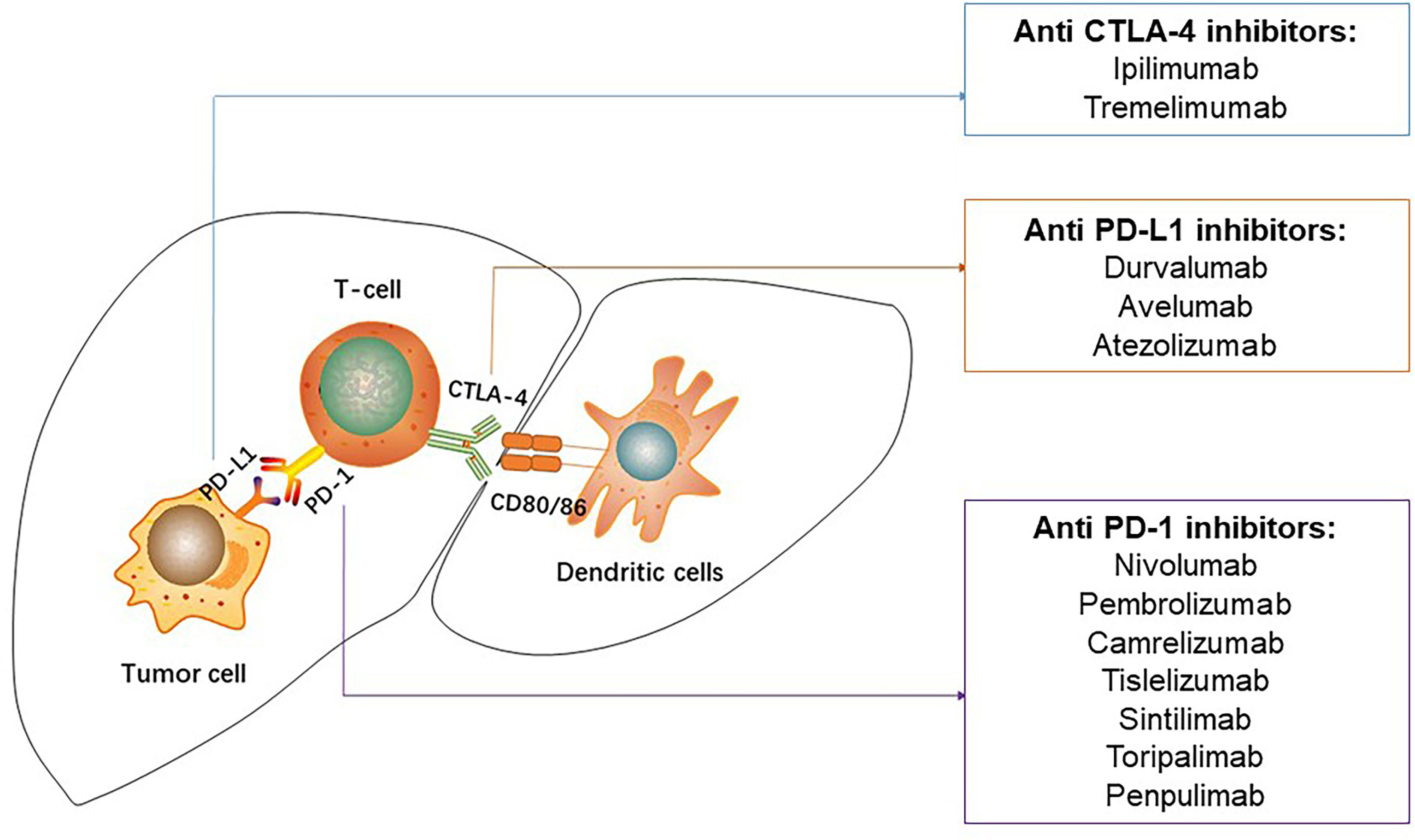
Figure 2 Immune checkpoint inhibitors used in hepatocellular carcinoma. PD-1, programmed death-1; PD-L1, programmed death-ligand 1; CTLA-4, cytotoxic T-lymphocyte associated protein-4.
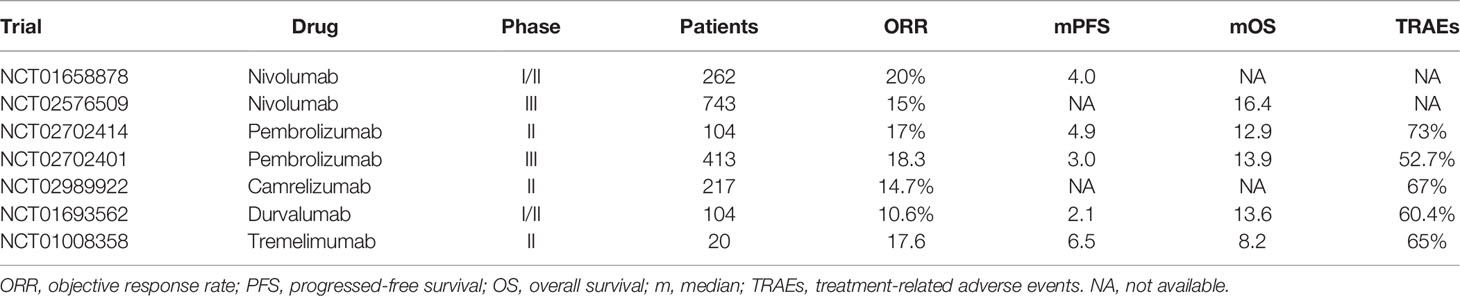
Table 1 Clinical trials of monotherapy of immune checkpoint inhibitors for advanced HCC.
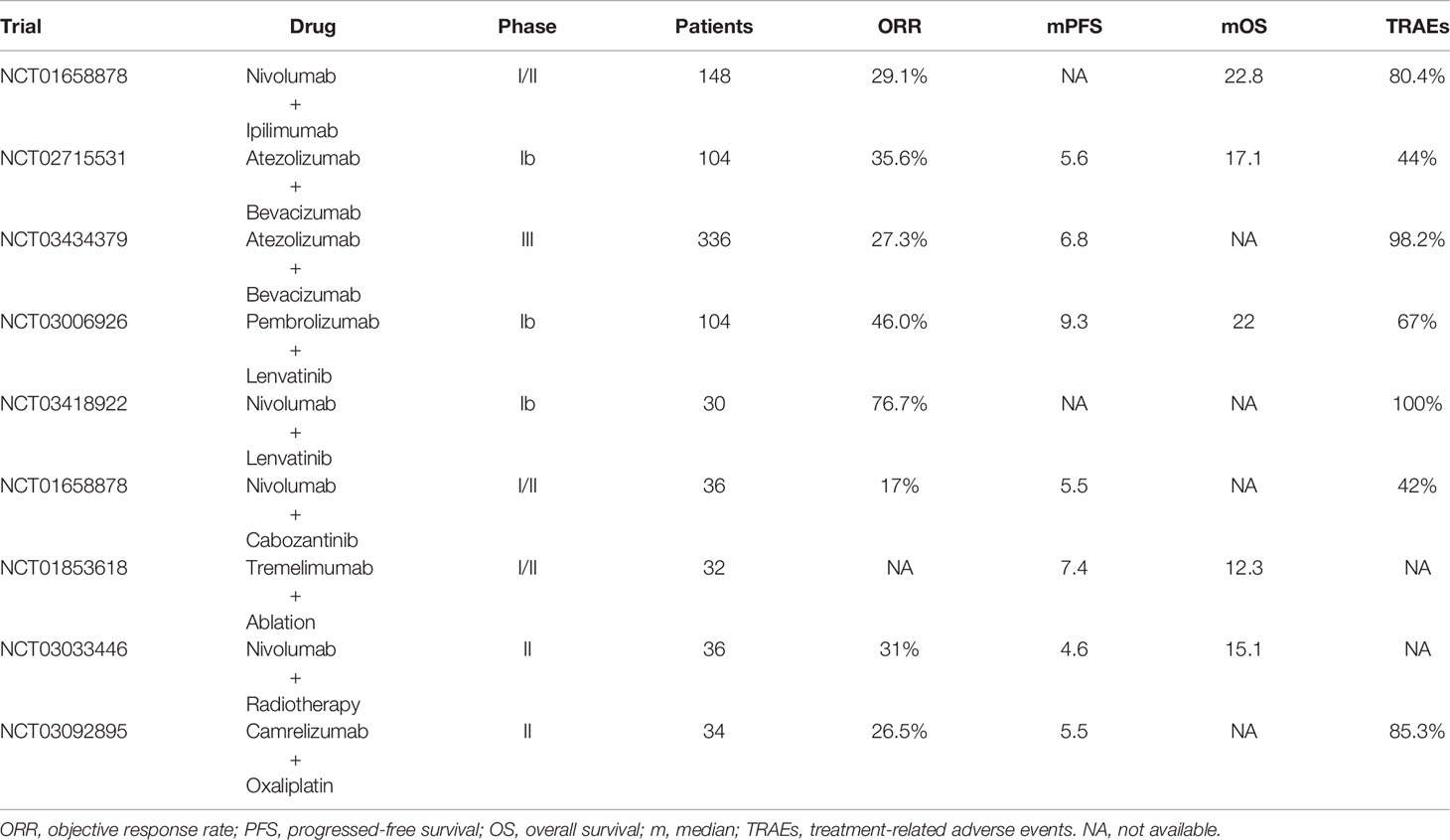
Table 2 Clinical trials of combined therapies based on immune checkpoint inhibitors for advanced HCC.
Except for PD-1 and CTLA-4, many coreceptors activate lymphocytes by regulating the antigen receptor signaling to optimize tumor immune responses. Lymphocyte activation gene-3 (LAG-3) is one of the most important targets in these coreceptors (37, 38). LAG-3 expressed on the CD4+ and CD8+ T cells under the stimulation of antigen (39). The T cells lose effector ability with the continued and high expression of LAG-3 inhibitory coreceptors. To date, LAG-3 inhibitors as monotherapies or in combination with PD-1/PD- L1 inhibitors are conducting clinical trials in multiple cancers (40).
Monotherapy of Immune Checkpoint Inhibitors
Nivolumab (Anti-PD1)
Nivolumab is the first fully humanized immunoglobulin G4 (IgG4) anti-PD1 monoclonal inhibitor, and the first ICIs that was approved for the HCC treatment (41). Nivolumab prevents the interaction of the PD-1 with its ligands PD-L1 by binding to PD-1, which can inhibit the immune suppression and immune escape, enhance the activity and proliferation of host T cells, and strengthen the ability of anti-tumor immune response in the tumor microenvironment (42). The superior survival result of nivolumab for the therapeutic of advanced HCC was firstly revealed in the multicenter, phase I/II, open-labeled CHECKMATE-040 trial (14). This is a dose-escalation and expansion study performed in advanced adult HCC patients with or without sorafenib pretreated. Drug dosage was given 0.1–10 mg/kg in the dose-escalation group and 3 mg/kg every 2 weeks in the dose-expansion group. Finally, 262 eligible HCC patients were included. The objective response rate (ORR) was 20% (95% CI: 15%–26%) in the dose-expansion group and 15% (95% CI: 6%–28%) in the dose-escalation group. Meanwhile, in the dose-escalation group, 12 patients suffered from grade 3/4 treatment-related adverse events (TRAEs) and 3 patients experienced treatment-related serious AEs (14).
Then, a phase 3 trial (CheckMate 459) compared the nivolumab with the sorafenib as the primary therapy for HCC patients (43). This study recruited 743 eligible patients, who were evenly randomly allocated to the nivolumab group and the sorafenib group. Nivolumab was given 240 mg every two weeks, and sorafenib was given 400 mg twice a day. Although the median overall survival (OS) was 16.4 months in the nivolumab group, which was significantly longer than 14.7 months in the sorafenib group, it did not reach the pre-defined statistical significance threshold (HR: 0.84, P = 0.0419). The anti-tumor efficacy of nivolumab is not better than that of sorafenib for advanced HCC based on the CheckMate 459 results. Thus, it has not been approved for HCC as preferred treatment.
Pembrolizumab (Anti-PD1)
Pembrolizumab is another IgG4 anti-PD1 inhibitor, and it was approved as the second-line systemic therapy for advanced HCC patients, according to the results of KEYNOTE-224 (15). The multicenter, phase 2 study included 104 eligible pathologically confirmed advanced HCC patients who were intolerant or progresses with sorafenib. Pembrolizumab was given 200 mg every 3 weeks durable 2 years or until disease progression. Eventually, the ORR was 17% (95% CI: 11%–26%). The median progression-free survival (PFS) was 4.9 months (95% CI: 3.4-7.2 months) and the median OS was 12.9 months (95% CI: 9.7-15.5 months). Any grade TRAEs was 73%, which included 24% grade 3 TRAEs.
Subsequently, a randomized, double-blind, phase 3 trial was conducted to compare the efficacy and safety of pembrolizumab with placebo in the treatment of advance HCC patients who previously received sorafenib (KEYNOTE-240) (44). Two hundred and seventy-eight patients received 200 mg pembrolizumab intravenously every 3 weeks durable about 2 years, and 135 patients received saline placebo. At the cutoff date, the median OS was 13.9 months (95% CI: 11.6-16.0 months) in the pembrolizumab group, and 10.6 months (95% CI: 8.3-13.5 months) in the placebo group (P = 0.024). The median PFS was 3.0 months (95% CI: 2.8-4.1months) in the pembrolizumab arm, and 2.8 months (95% CI: 1.6-3.0 months) in the placebo arm (P = 0.019). However, the primary endpoint of OS and PFS did not reach the prespecified boundaries of statistical significance. In addition, two phase 3 trials involving the monotherapy of pembrolizumab are currently ongoing (KEYNOTE-394 and KEYNOTE-937).
Camrelizumab (Anti-PD1)
Camrelizumab is a fully humanized anti-PD1 inhibitor, and the binding epitope is different from that of nivolumab and pembrolizumab (45). NCT02989922 trials was a multicenter, open-label, phase 2 single-arm study to assess the efficacy of camrelizumab for patients who were developed or intolerant to previous systemic drugs. In this study, 109 eligible participants received 3 mg/kg intravenously every 2 weeks, and 108 patients received 3 mg/kg intravenously every 3 weeks. Finally, the ORR of camrelizumab was 14.7% (95% CI: 10.3%-20.2%), and the 6-month OS rate was 74.4% (95% CI: 68.0%-79.9%). Meanwhile, grade 3/4 TRAEs was 22%, and the treatment-related death was 0.9% (45).
Durvalumab (Anti-PD-L1)
Durvalumab is a humanized IgG1 anti-PD-L1 monoclonal antibody (46). It plays the anti-tumor efficacy through binding to the PD-L1 receptor on the surface of cancer cells rather than the PD-1 receptor. NCT01693562 was a multicenter, open-label, phase 1/2 study to assess the clinical efficacy of durvalumab as monotherapy for HCC patients (47). Forty participants were given durvalumab 10 mg/kg intravenously every 2 weeks durable one year or until progressed. The results demonstrated that the ORR was 10.3%, and the median OS was 13.2 months (95% CI: 6.3–21.1 months). This study confirmed the potential clinical efficacy of durvalumab as the second-line therapy for HCC.
Tremelimumab (Anti-CTLA-4)
Tremelimumab is a humanized IgG2 monoclonal antibody that blocks the binding of CTLA-4, an extracellular inhibitory receptor expressed on T cells (48). CTLA-4 is a CD28 homolog, binding to B7 ligand on antigen-presenting cells, interferes with T cell activation and proliferation. An open-label, pilot phase 2 clinical study firstly evaluated the treatment effect of tremelimumab forHCC and chronic hepatitis C virus (HCV) infection (49). Twenty-one participants received tremelimumab 15 mg/kg intravenously every 3 months until disease development or intolerable adverse event. Finally, the study performed that the disease control rate was 76.4%, the median time to progression (TTP) was 6.48 months (95% CI: 3.95–9.14 months), and the median OS was 8.2 months (95% CI: 4.64–21.34 months). This promising results encouraged more future studies of CTLA-4 inhibitors for advanced HCC.
Combination Therapy With Immune Checkpoint Inhibitors for Advanced HCC
Combinations of the Two ICIs
Combinations of two ICIs, such as anti-PD-1 with anti-CTLA-4 inhibitors have been performed in numerous cancers, including HCC. The CheckMate 040 was a clinical trial to evaluate the effect of nivolumab (anti-PD1 agents) plus ipilimumab (anti-CTLA-4 agents) for advanced HCC patients pretreated sorafenib (50). In this study, 148 eligible participants were randomized 1:1:1 to three groups: group A was given at a dosage of nivolumab 1 mg/kg intravenously and ipilimumab 3 mg/kg intravenously, group B was given at a dosage of nivolumab 3 mg/kg intravenously and ipilimumab 1 mg/kg intravenously, and group C was given at a dosage of nivolumab 3 mg/kg intravenously and ipilimumab 1 mg/kg intravenously. The results showed that the ORR was 32% (95% CI: 20%-47%) in the group A, 27% (95% CI: 15%-41%) in the group B, and 29% (95% CI: 17%-43%) in the group C. Moreover, the median OS was 22.8 months in the group A, 12.5 months in the group B, 12.7 months in the group C. Based on these results, in 2020, the combination of nivolumab with ipilimumab was approved as the second-line treatment for advanced HCC patients who failed to sorafenib treatment (50).
Combination of ICIs With Angiogenesis Inhibitors
Vascular endothelial growth factor (VEGF) overexpression is one of the critical mechanisms of HCC tumor angiogenesis, and it is associated with immunosuppressive effects in the tumor microenvironment (51). VEGF inhibitors alleviate VEGF-mediated immunosuppression in tumors and the tumor microenvironment and promote infiltration of immune cells in tumors. Therefore, the combination therapy of ICIs with VEGF inhibitors may have a synergistic anti-tumor effect for advanced HCC. Atezolizumab is a humanized IgG1 monoclonal antibody, which selectively targets PDL1, and bevacizumab is a humanized IgG1 monoclonal antibody that targets VEGF (52, 53). A multicenter, open-label, phase 1b clinical trial (NCT02715531) evaluated the effectiveness of atezolizumab (anti-PD-L1 agent) combined with bevacizumab (anti-VEGF agent) in the treatment of HCC (54). In this study, the combination therapy group received atezolizumab 1200 mg intravenously and bevacizumab 15 mg/kg intravenously every 3 weeks until the disease progressed or intolerable adverse events. The results revealed that the ORR was 36% (95% CI: 26%-46%), the median OS was 17.1 months, and the median PFS was 5.6 months (95% CI: 3.6-7.4 months) in the combination therapy group, which significantly longer than that of in the atezolizumab monotherapy group (P = 0.011).
Subsequently, a global, phase 3 study (NCT03434379) was performed to compare the combination of atezolizumab with bevacizumab to sorafenib for HCC patients who never received systemic therapy (17). The eligible participants enrolled in this study were randomly assigned in a 2:1 ratio to receive either combined therapy of atezolizumab with bevacizumab or sorafenib alone therapy until the disease progressed or intolerable adverse events. Finally, a total of 336 participants received atezolizumab plus bevacizumab, and 165 patients received sorafenib alone treatment. The survival rates of 6 months (84.8%) and 12 months (67.2%) in the combined therapy group were significantly longer than that of the sorafenib alone group (P < 0.001). Moreover, the median PFS was 6.8 months (95% CI: 5.7-8.3 months) in the combination group, which were significantly longer than 4.3 months (95% CI: 4.0-5.6 months) in the sorafenib group (P < 0.001). The ORR of the atezolizumab–bevacizumab group was 27.3% (95% CI: 22.5%-32.5%), which was significantly higher than 11.9% (95% CI: 7.4%-18.0%) in the sorafenib group (P < 0.001). Based on the encouraging results from this trial, the combination treatment of atezolizumab with bevacizumab was approved as the preferred therapy for the advanced HCC.
Lenvatinib, a multi-kinase inhibitor of VEGF receptors, was permitted for standard therapy of unresectable HCC on the basis of REFLECT study results (7). A phase 1b trial was performed to assess the efficacy of lenvatinib combining with pembrolizumab for the treatment of Barcelona Clinic Liver Cancer (BCLC) stage B or C HCC (55). One hundred and four eligible participants received lenvatinib 12 mg/day or 8 mg/day orally and pembrolizumab 200 mg intravenously every 21 days. The results suggested that the ORR was 46.0% (95% CI: 36.0%-56.3%), and the median PFS was 9.3 months (95% CI: 5.6-9.7 months). According to the encouraging results of this study, the combination therapy of lenvatinib and pembrolizumab is defined as a breakthrough therapy designation in the first-line treatment of HCC. Therefore, a phase 3 trial comparing lenvatinib plus pembrolizumab with lenvatinib plus placebo as standard treatment for advanced HCC is underway. Additionally, the clinical effect of combination lenvatinib with nivolumab for unresectable HCC was investigated in an open-label, phase Ib trial (NCT03418922) (56). The results of this study showed the ORR was 76.7% with tolerable toxicity.
Cabozantinib is a small molecule tyrosine kinase inhibitor that can inhibit the phosphorylation of MET and VEGF receptor 2 in HCC (57). In a randomized, double-blind, phase 3 trial (NCT01908426), HCC patients treated with cabozantinib resulted in a significantly longer OS (median OS: 10.2 months versus 8.0 months) and PFS (median PFS: 5.2 months versus 1.9 months) than that of placebo. Thus, it was approved as the second-line therapy for advanced HCC (8). Recently, the combination of cabozantinib and ICIs showed promising results in the expansion arm from the CheckMate 040 study. In this study, 35 patients received the triple combination therapy of nivolumab, ipilimumab, and cabozantinib, and 36 patients received the doublet combination of nivolumab and cabozantinib. As the researchers envisioned, the ORR in triple combination arm was 26%, which was significantly higher than 17% in the doublet combination arm (P < 0.001), and the median PFS in the triple combination arm was significantly longer than that of in the doublet combination arm (6.8 months versus 5.5 months, P < 0.001) (58). The combination of cabozantinib with other ICIs, such as pembrolizumab (NCT04442581) and durvalumab (NCT03539822), is in progress.
Combination of ICIs With Locoregional Therapies
For unresectable HCC, numerous locoregional therapies, including TACE, RFA or microwave ablation, and radiation therapy, are always the limited first-line treatment option (59). Local treatment of HCC can improve anti-tumor immunity by releasing inflammatory factors and tumor-specific neoantigens from killing tumor cells (60, 61). Currently, some clinical trials are investigating the efficacy and safety of the combination of locoregional therapies with immunotherapeutic agents, such as ICIs. A non-randomized, phase 1/2, single-arm study involving 32 patients evaluated the safely and feasibly of tremelimumab combining with ablation for unresectable HCC (62). In this study, patients received tremelimumab at two dose levels (3.5 mg/kg and 10 mg/kg i.v.) every 4 weeks for 6 doses, followed by 3-monthly infusions until off-treatment criteria were met. On day 36, subsequently radiofrequency ablation or chemoablation was conducted. The results showed that the median TTP and OS were 7.4 months (95% CI: 4.7-19.4 months) and 12.3 months (95% CI: 9.3-15.4 months), respectively. Meanwhile, 12 of 14 patients with quantifiable HCV showed a significant reduction in viral load. In addition, a phase 2 study assessed the impact of ablation on unresectable HCC patients who had stable disease or atypical response to nivolumab or pembrolizumab inhibitor after resistance to sorafenib. Additional ablation treatment increased the response rate from 10% to 24% (12/50) with tolerable adverse events. Furthermore, the median TTP, PFS, and OS were 6.1 months (95% CI: 2.6-11.2 months), 5 months (95%CI: 2.9-7.1 months) and 16.9 months (95%CI: 7.7-26.1 months), respectively. Recently, the results of a phase II, non-randomized trial (NCT03033446) revealed that the combination of nivolumab with Y90-radioembolization (RE) was a promising option for Child-Pugh A advanced HCC patients (63). Among the evaluable 36 participants, the DCR was 58.3%, and the median PFS and OS were 4.6 months (95% CI: 2.3-8.4 months) and 15.1 months (95% CI: 7.8-unreached), respectively. Moreover, several clinical trials of drug eluting bead transarterial chemoembolization (DEB-TACE) in combination with nivolumab (NCT03143270), TACE in combination with bevacizumab and durvalumab (NCT03778957), and TACE in combination with pembrolizumab (NCT03397654) are currently underway (64).
Combination of ICIs With Chemotherapies
Several previous studies suggested that chemotherapy agents can improve anti-tumor immune response and induce immunogenic cell death by activating the dendritic cells, enhancing cross-priming of T cells, and downregulating of myeloid-derived suppressor cells and Treg cells (65, 66). A multicenter, phase 2, single-arm study evaluated the effectiveness of combination of camrelizumab with oxaliplatin-based chemotherapy for advanced HCC patients (67). In the study, 34 eligible patients received camrelizumab (3 mg/kg i.v., every 2 weeks) and typical FOLFOX4 (infusional fluorouracil, leucovorin and oxaliplatin) or GEMOX (gemcitabine and oxaliplatin) regimen. The results showed that the confirmed ORR was 26.5% and DCR was 79.4%. Median time to response (TTR) was 2.0 months. Furthermore, a phase 3 study that compares the combination therapy of camrelizumab with FOLFOX4 regimen to placebo with FOLFOX4 regimen for advanced HCC patients are currently ongoing (NCT03605706).
Current Challenges
To date, there are still many limitations and challenges in the application of immunotherapy for advanced HCC based on ICIs. First of all, the approved treatment, including monotherapy and combination therapy, for advanced HCC still have limited survival efficacy. Although the combination of ICIs with VEGF inhibitors improved the response rate and survival time, more than two-thirds of the patients still do not respond (68). In addition, some previous studies (14, 15) evaluated the PD-L1 expression and specific genomic alterations as the prognostic biomarkers for the immunotherapy of HCC. Nevertheless, the results of these studies revealed that positive expression of PD-L1 in HCC was not associated with treatment response to nivolumab or pembrolizumab. Furthermore, a lot of immune-related genes, such as TP53, were used to establish the prognostic signature of HCC (69–71). However, the prediction of single or multiple genes is not comprehensive and accurate for HCC.
Future Directions
Recently, some preclinical studies combined chimeric antigen receptor T (CAR-T) cells with ICIs for the treatment of HCC, attaining a significant progress (72). Thus, several studies which aimed to assess the effectiveness of CAR-T cells combining with chemotherapy agents or cytokine for advanced HCC is currently ongoing (NCT02905188, NCT04093648, and NCT03198546) (73). Furthermore, the cancer vaccine in combination with ICIs may be a promising treatment option for advanced HCC in the future. The combination of these two drugs may have a synergistic anti-tumor effect that the vaccine increases the number of tumor-infiltrating effector T cells, and ICIs activate these cells (74, 75). More clinical trials to investigate this combination therapy are warranted.
Transforming growth factor beta (TGF-β) promotes tumor immune evasion by inhibiting proliferation of lymphocytes and immune factors (76). The combination of monoclonal antibodies targeting TGF-β and PD-L1 may provide a novel treatment approach because their mechanisms of action are complementary. A preclinical study indicated that the application of TGF-β and PD-L1 inhibitors could reverse the sorafenib resistance in HCC (77). In addition, a previous clinical study (NCT02699515) also confirmed the safety and preliminary efficacy of the bifunctional fusion protein in HCC (78).Many recent studies revealed that the BRAF pathway plays an important role in HCC development (79, 80). However, the inhibition of single pathway could not be sufficient to prevent HCC progression. The combination treatment of BRAF inhibitors and tyrosine kinase inhibitors (TKI) and immunotherapy made a series of exciting results (81). The preclinical study demonstrated that magnolia combined with BRAF inhibitor SB590885 inhibited the proliferation and migration of HCC cells, by targeting the ERKs/RSK2 signaling pathway (82). Furthermore, a phase I trial of Pimasertib (AS703026) confirmed the safety in HCC (83). More clinical trials are conducting.
Author Contributions
CZ made substantial contributions to the design of the work. TO and XK drafted the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2021) 71:209–49. doi: 10.3322/caac.21660
2. Reig M, Forner A, Rimola J, Ferrer-Fabrega J, Burrel M, Garcia-Criado A, et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J Hepatol (2022) 76:681–93. doi: 10.1016/j.jhep.2021.11.018
3. Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A Global View of Hepatocellular Carcinoma: Trends, Risk, Prevention and Management. Nat Rev Gastroenterol Hepatol (2019) 16:589–604. doi: 10.1038/s41575-019-0186-y
4. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in Advanced Hepatocellular Carcinoma. N Engl J Med (2008) 359:378–90. doi: 10.1056/NEJMoa0708857
5. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacy and Safety of Sorafenib in Patients in the Asia-Pacific Region With Advanced Hepatocellular Carcinoma: A Phase III Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Oncol (2009) 10:25–34. doi: 10.1016/S1470-2045(08)70285-7
6. Bruix J, Qin S, Merle P, Granito A, Huang YH, Bodoky G, et al. Regorafenib for Patients With Hepatocellular Carcinoma Who Progressed on Sorafenib Treatment (RESORCE): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet (London England) (2017) 389:56–66. doi: 10.1016/S0140-6736(16)32453-9
7. Kudo M, Finn RS, Qin S, Han KH, Ikeda K, Piscaglia F, et al. Lenvatinib Versus Sorafenib in First-Line Treatment of Patients With Unresectable Hepatocellular Carcinoma: A Randomised Phase 3 non-Inferiority Trial. Lancet (London England) (2018) 391:1163–73. doi: 10.1016/S0140-6736(18)30207-1
8. Abou-Alfa GK, Meyer T, Cheng AL, El-Khoueiry AB, Rimassa L, Ryoo BY, et al. Cabozantinib in Patients With Advanced and Progressing Hepatocellular Carcinoma. N Engl J Med (2018) 379:54–63. doi: 10.1056/NEJMoa1717002
9. Zhu AX, Kang YK, Yen CJ, Finn RS, Galle PR, Llovet JM, et al. Ramucirumab After Sorafenib in Patients With Advanced Hepatocellular Carcinoma and Increased α-Fetoprotein Concentrations (REACH-2): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Oncol (2019) 20:282–96. doi: 10.1016/S1470-2045(18)30937-9
10. Choi WM, Choi J, Lee D, Shim JH, Lim YS, Lee HC, et al. Regorafenib Versus Nivolumab After Sorafenib Failure: Real-World Data in Patients With Hepatocellular Carcinoma. Hepatol Commun (2020) 4:1073–86. doi: 10.1002/hep4.1523
11. Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, et al. Safety and Tumor Responses With Lambrolizumab (Anti-PD-1) in Melanoma. N Engl J Med (2013) 369:134–44. doi: 10.1056/NEJMoa1305133
12. Yang JC, Hughes M, Kammula U, Royal R, Sherry RM, Topalian SL, et al. Ipilimumab (Anti-CTLA4 Antibody) Causes Regression of Metastatic Renal Cell Cancer Associated With Enteritis and Hypophysitis. J immunotherapy (Hagerstown Md. 1997) (2007) 30:825–30. doi: 10.1097/CJI.0b013e318156e47e
13. Xia L, Liu Y, Wang Y. PD-1/PD-L1 Blockade Therapy in Advanced Non-Small-Cell Lung Cancer: Current Status and Future Directions. Oncologist (2019) 24:S31–s41. doi: 10.1634/theoncologist.2019-IO-S1-s05
14. El-Khoueiry AB, Sangro B, Yau T, Crocenzi TS, Kudo M, Hsu C, et al. Nivolumab in Patients With Advanced Hepatocellular Carcinoma (CheckMate 040): An Open-Label, non-Comparative, Phase 1/2 Dose Escalation and Expansion Trial. Lancet (London England) (2017) 389:2492–502. doi: 10.1016/S0140-6736(17)31046-2
15. Zhu AX, Finn RS, Edeline J, Cattan S, Ogasawara S, Palmer D, et al. Pembrolizumab in Patients With Advanced Hepatocellular Carcinoma Previously Treated With Sorafenib (KEYNOTE-224): A non-Randomised, Open-Label Phase 2 Trial. Lancet Oncol (2018) 19:940–52. doi: 10.1016/S1470-2045(18)30351-6
16. Liu ZL, Liu JH, Staiculescu D, Chen J. Combination of Molecularly Targeted Therapies and Immune Checkpoint Inhibitors in the New Era of Unresectable Hepatocellular Carcinoma Treatment. Ther Adv Med Oncol (2021) 13:17588359211018026. doi: 10.1177/17588359211018026
17. Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, et al. Atezolizumab Plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med (2020) 382:1894–905. doi: 10.1056/NEJMoa1915745
18. Ramakrishna G, Rastogi A, Trehanpati N, Sen B, Khosla R, Sarin SK. From Cirrhosis to Hepatocellular Carcinoma: New Molecular Insights on Inflammation and Cellular Senescence. Liver Cancer (2013) 2:367–83. doi: 10.1159/000343852
19. Nakagawa H, Maeda S. Inflammation- and Stress-Related Signaling Pathways in Hepatocarcinogenesis. World J Gastroenterol (2012) 18:4071–81. doi: 10.3748/wjg.v18.i31.4071
20. Iñarrairaegui M, Melero I, Sangro B. Immunotherapy of Hepatocellular Carcinoma: Facts and Hopes. Clin Cancer Res (2018) 24:1518–24. doi: 10.1158/1078-0432.CCR-17-0289
21. Cariani E, Missale G. Immune Landscape of Hepatocellular Carcinoma Microenvironment: Implications for Prognosis and Therapeutic Applications. Liver Int (2019) 39:1608–21. doi: 10.1111/liv.14192
22. Berasain C, Castillo J, Prieto J, Avila MA. New Molecular Targets for Hepatocellular Carcinoma: The ErbB1 Signaling System. Liver Int (2007) 27:174–85. doi: 10.1111/j.1478-3231.2006.01424.x
23. Nakagawa H, Maeda S, Yoshida H, Tateishi R, Masuzaki R, Ohki T, et al. Serum IL-6 Levels and the Risk for Hepatocarcinogenesis in Chronic Hepatitis C Patients: An Analysis Based on Gender Differences. Int J Cancer (2009) 125:2264–9. doi: 10.1002/ijc.24720
24. Gao Q, Wang XY, Qiu SJ, Yamato I, Sho M, Nakajima Y, et al. Overexpression of PD-L1 Significantly Associates With Tumor Aggressiveness and Postoperative Recurrence in Human Hepatocellular Carcinoma. Clin Cancer Res (2009) 15:971–9. doi: 10.1158/1078-0432.CCR-08-1608
25. Guo M, Yuan F, Qi F, Sun J, Rao Q, Zhao Z, et al. Expression and Clinical Significance of LAG-3, FGL1, PD-L1 and CD8(+)T Cells in Hepatocellular Carcinoma Using Multiplex Quantitative Analysis. J Trans Med (2020) 18:306. doi: 10.1186/s12967-020-02469-8
26. Liu F, Liu Y, Chen Z. Tim-3 Expression and its Role in Hepatocellular Carcinoma. J Hematol Oncol (2018) 11:126. doi: 10.1186/s13045-018-0667-4
27. Shi F, Shi M, Zeng Z, Qi RZ, Liu ZW, Zhang JY, et al. PD-1 and PD-L1 Upregulation Promotes CD8(+) T-Cell Apoptosis and Postoperative Recurrence in Hepatocellular Carcinoma Patients. Int J Cancer (2011) 128:887–96. doi: 10.1002/ijc.25397
28. Xiao X, Lao XM, Chen MM, Liu RX, Wei Y, Ouyang FZ, et al. PD-1hi Identifies a Novel Regulatory B-Cell Population in Human Hepatoma That Promotes Disease Progression. Cancer Discovery (2016) 6:546–59. doi: 10.1158/2159-8290.CD-15-1408
29. Agata Y, Kawasaki A, Nishimura H, Ishida Y, Tsubata T, Yagita H, et al. Expression of the PD-1 Antigen on the Surface of Stimulated Mouse T and B Lymphocytes. Int Immunol (1996) 8:765–72. doi: 10.1093/intimm/8.5.765
30. Keir ME, Butte MJ, Freeman GJ, Sharpe AH. PD-1 and its Ligands in Tolerance and Immunity. Annu Rev Immunol (2008) 26:677–704. doi: 10.1146/annurev.immunol.26.021607.090331
31. Keir ME, Liang SC, Guleria I, Latchman YE, Qipo A, Albacker LA, et al. Tissue Expression of PD-L1 Mediates Peripheral T Cell Tolerance. J Exp Med (2006) 203:883–95. doi: 10.1084/jem.20051776
32. Freeman GJ, Long AJ, Iwai Y, Bourque K, Chernova T, Nishimura H, et al. Engagement of the PD-1 Immunoinhibitory Receptor by a Novel B7 Family Member Leads to Negative Regulation of Lymphocyte Activation. J Exp Med (2000) 192:1027–34. doi: 10.1084/jem.192.7.1027
33. Yamamoto R, Nishikori M, Kitawaki T, Sakai T, Hishizawa M, Tashima M, et al. PD-1-PD-1 Ligand Interaction Contributes to Immunosuppressive Microenvironment of Hodgkin Lymphoma. Blood (2008) 111:3220–4. doi: 10.1182/blood-2007-05-085159
34. Thompson RH, Dong H, Lohse CM, Leibovich BC, Blute ML, Cheville JC, et al. PD-1 is Expressed by Tumor-Infiltrating Immune Cells and is Associated With Poor Outcome for Patients With Renal Cell Carcinoma. Clin Cancer Res (2007) 13:1757–61. doi: 10.1158/1078-0432.CCR-06-2599
35. Peggs KS, Quezada SA, Chambers CA, Korman AJ, Allison JP. Blockade of CTLA-4 on Both Effector and Regulatory T Cell Compartments Contributes to the Antitumor Activity of Anti-CTLA-4 Antibodies. J Exp Med (2009) 206:1717–25. doi: 10.1084/jem.20082492
36. Hargadon KM, Johnson CE, Williams CJ. Immune Checkpoint Blockade Therapy for Cancer: An Overview of FDA-Approved Immune Checkpoint Inhibitors. Int Immunopharmacol (2018) 62:29–39. doi: 10.1016/j.intimp.2018.06.001
37. Andrews LP, Yano H, Vignali DAA. Inhibitory Receptors and Ligands Beyond PD-1, PD-L1 and CTLA-4: Breakthroughs or Backups. Nat Immunol (2019) 20:1425–34. doi: 10.1038/s41590-019-0512-0
38. Triebel F. LAG-3: A Regulator of T-Cell and DC Responses and its Use in Therapeutic Vaccination. Trends Immunol (2003) 24:619–22. doi: 10.1016/j.it.2003.10.001
39. Okazaki T, Okazaki IM, Wang J, Sugiura D, Nakaki F, Yoshida T, et al. PD-1 and LAG-3 Inhibitory Co-Receptors Act Synergistically to Prevent Autoimmunity in Mice. J Exp Med (2011) 208:395–407. doi: 10.1084/jem.20100466
40. Ascierto PA, Bono P, Bhatia S, Melero I, Nyakas MS, Svane IM, et al. Efficacy of BMS-986016, A Monoclonal Antibody That Targets Lymphocyte Activation Gene-3 (LAG-3), in Combination With Nivolumab in Pts With Melanoma Who Progressed During Prior Anti-PD-1/PD-L1 Therapy (Mel Prior IO) in All-Comer and Biomarker-Enriched Populations. Ann Oncol (2017) 28:v611–2. doi: 10.1093/annonc/mdx440.011
41. Guo L, Zhang H, Chen B. Nivolumab as Programmed Death-1 (PD-1) Inhibitor for Targeted Immunotherapy in Tumor. J Cancer (2017) 8:410–6. doi: 10.7150/jca.17144
42. Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, et al. Safety, Activity, and Immune Correlates of Anti-PD-1 Antibody in Cancer. N Engl J Med (2012) 366:2443–54. doi: 10.1056/NEJMoa1200690
43. Yau T, Park JW, Finn RS, Cheng AL, Mathurin P, Edeline J, et al. CheckMate 459: A Randomized, Multi-Center Phase III Study of Nivolumab (NIVO) vs Sorafenib (SOR) as First-Line (1L) Treatment in Patients (Pts) With Advanced Hepatocellular Carcinoma (aHCC). Ann Oncol (2019) 30:v874–5. doi: 10.1093/annonc/mdz394.029
44. Finn RS, Ryoo BY, Merle P, Kudo M, Bouattour M, Lim HY, et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J Clin Oncol (2020) 38:193–202. doi: 10.1200/JCO.19.01307
45. Qin S, Ren Z, Meng Z, Chen Z, Chai X, Xiong J, et al. Camrelizumab in Patients With Previously Treated Advanced Hepatocellular Carcinoma: A Multicentre, Open-Label, Parallel-Group, Randomised, Phase 2 Trial. Lancet Oncol (2020) 21:571–80. doi: 10.1016/S1470-2045(20)30011-5
46. Syed YY. Durvalumab: First Global Approval. Drugs (2017) 77:1369–76. doi: 10.1007/s40265-017-0782-5
47. Wainberg ZA, Segal NH, Jaeger D, Lee K-H, Marshall J, Antonia SJ, et al. Safety and Clinical Activity of Durvalumab Monotherapy in Patients With Hepatocellular Carcinoma (HCC). J Clin Oncol (2017) 35:4071–1. doi: 10.1200/JCO.2017.35.15_suppl.4071
48. Comin-Anduix B, Escuin-Ordinas H, Ibarrondo FJ. Tremelimumab: Research and Clinical Development. Onco Targets Ther (2016) 9:1767–76. doi: 10.2147/OTT.S65802
49. Sangro B, Gomez-Martin C, de la Mata M, Iñarrairaegui M, Garralda E, Barrera P, et al. A Clinical Trial of CTLA-4 Blockade With Tremelimumab in Patients With Hepatocellular Carcinoma and Chronic Hepatitis C. J Hepatol (2013) 59:81–8. doi: 10.1016/j.jhep.2013.02.022
50. Yau T, Kang YK, Kim TY, El-Khoueiry AB, Santoro A, Sangro B, et al. Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients With Advanced Hepatocellular Carcinoma Previously Treated With Sorafenib: The CheckMate 040 Randomized Clinical Trial. JAMA Oncol (2020) 6:e204564. doi: 10.1001/jamaoncol.2020.4564
51. Hilmi M, Neuzillet C, Calderaro J, Lafdil F, Pawlotsky JM, Rousseau B. Angiogenesis and Immune Checkpoint Inhibitors as Therapies for Hepatocellular Carcinoma: Current Knowledge and Future Research Directions. J Immunother Cancer (2019) 7:333. doi: 10.1186/s40425-019-0824-5
52. Herbst RS, Soria JC, Kowanetz M, Fine GD, Hamid O, Gordon MS, et al. Predictive Correlates of Response to the Anti-PD-L1 Antibody MPDL3280A in Cancer Patients. Nature (2014) 515:563–7. doi: 10.1038/nature14011
53. Ferrara N, Hillan KJ, Novotny W. Bevacizumab (Avastin), a Humanized Anti-VEGF Monoclonal Antibody for Cancer Therapy. Biochem Biophys Res Commun (2005) 333:328–35. doi: 10.1016/j.bbrc.2005.05.132
54. Lee MS, Ryoo BY, Hsu CH, Numata K, Stein S, Verret W, et al. Atezolizumab With or Without Bevacizumab in Unresectable Hepatocellular Carcinoma (GO30140): An Open-Label, Multicentre, Phase 1b Study. Lancet Oncol (2020) 21:808–20. doi: 10.1016/S1470-2045(20)30156-X
55. Finn RS, Ikeda M, Zhu AX, Sung MW, Baron AD, Kudo M, et al. Phase Ib Study of Lenvatinib Plus Pembrolizumab in Patients With Unresectable Hepatocellular Carcinoma. J Clin Oncol (2020) 38:2960–70. doi: 10.1200/JCO.20.00808
56. Kudo M, Ikeda M, Motomura K, Okusaka T, Kato N, Dutcus CE, et al. A Phase Ib Study of Lenvatinib (LEN) Plus Nivolumab (NIV) in Patients (Pts) With Unresectable Hepatocellular Carcinoma (uHCC): Study 117. J Clin Oncol (2020) 38:513–3. doi: 10.1200/JCO.2020.38.4_suppl.513
57. Yakes FM, Chen J, Tan J, Yamaguchi K, Shi Y, Yu P, et al. Cabozantinib (XL184), a Novel MET and VEGFR2 Inhibitor, Simultaneously Suppresses Metastasis, Angiogenesis, and Tumor Growth. Mol Cancer Ther (2011) 10:2298–308. doi: 10.1158/1535-7163.MCT-11-0264
58. Yau T, Zagonel V, Santoro A, Acosta-Rivera M, Choo SP, Matilla A, et al. Nivolumab (NIVO) + Ipilimumab (IPI) + Cabozantinib (CABO) Combination Therapy in Patients (Pts) With Advanced Hepatocellular Carcinoma (aHCC): Results From CheckMate 040. J Clin Oncol (2020) 38:478–8. doi: 10.1200/JCO.2020.38.4_suppl.478
59. Inchingolo R, Posa A, Mariappan M, Spiliopoulos S. Locoregional Treatments for Hepatocellular Carcinoma: Current Evidence and Future Directions. World J Gastroenterol (2019) 25:4614–28. doi: 10.3748/wjg.v25.i32.4614
60. Ayaru L, Pereira SP, Alisa A, Pathan AA, Williams R, Davidson B, et al. Unmasking of Alpha-Fetoprotein-Specific CD4(+) T Cell Responses in Hepatocellular Carcinoma Patients Undergoing Embolization. J Immunol (Baltimore Md. 1950) (2007) 178:1914–22. doi: 10.4049/jimmunol.178.3.1914
61. Nobuoka D, Motomura Y, Shirakawa H, Yoshikawa T, Kuronuma T, Takahashi M, et al. Radiofrequency Ablation for Hepatocellular Carcinoma Induces Glypican-3 Peptide-Specific Cytotoxic T Lymphocytes. Int J Oncol (2012) 40:63–70. doi: 10.3892/ijo.2011.1202
62. Duffy AG, Ulahannan SV, Makorova-Rusher O, Rahma O, Wedemeyer H, Pratt D, et al. Tremelimumab in Combination With Ablation in Patients With Advanced Hepatocellular Carcinoma. J Hepatol (2017) 66:545–51. doi: 10.1016/j.jhep.2016.10.029
63. Tai WMD, Loke KSH, Gogna A, Tan SH, Ng DCE, Hennedige TP, et al. A Phase II Open-Label, Single-Center, Nonrandomized Trial of Y90-Radioembolization in Combination With Nivolumab in Asian Patients With Advanced Hepatocellular Carcinoma: CA 209-678. J Clin Oncol (2020) 38:4590–0. doi: 10.1200/JCO.2020.38.15_suppl.4590
64. Harding JJ, Yarmohammadi H, Reiss KA, Chou JF, Capanu M, Do RKG, et al. Nivolumab (NIVO) and Drug Eluting Bead Transarterial Chemoembolization (Deb-TACE): Preliminary Results From a Phase I Study of Patients (Pts) With Liver Limited Hepatocellular Carcinoma (HCC). J Clin Oncol (2020) 38:525–5. doi: 10.1200/JCO.2020.38.4_suppl.525
65. Garg AD, Dudek-Peric AM, Romano E, Agostinis P. Immunogenic Cell Death. Int J Dev Biol (2015) 59:131–40. doi: 10.1387/ijdb.150061pa
66. Zheng Y, Dou Y, Duan L, Cong C, Gao A, Lai Q, et al. Using Chemo-Drugs or Irradiation to Break Immune Tolerance and Facilitate Immunotherapy in Solid Cancer. Cell Immunol (2015) 294:54–9. doi: 10.1016/j.cellimm.2015.02.003
67. Qin S, Chen Z, Liu Y, Xiong J, Ren Z, Meng Z, et al. A Phase II Study of Anti–PD-1 Antibody Camrelizumab Plus FOLFOX4 or GEMOX Systemic Chemotherapy as First-Line Therapy for Advanced Hepatocellular Carcinoma or Biliary Tract Cancer. J Clin Oncol (2019) 37:4074–4. doi: 10.1200/JCO.2019.37.15_suppl.4074
68. Mpekris F, Voutouri C, Baish JW, Duda DG, Munn LL, Stylianopoulos T, et al. Combining Microenvironment Normalization Strategies to Improve Cancer Immunotherapy. Proc Natl Acad Sci USA (2020) 117:3728–37. doi: 10.1073/pnas.1919764117
69. Long J, Wang A, Bai Y, Lin J, Yang X, Wang D, et al. Development and Validation of a TP53-Associated Immune Prognostic Model for Hepatocellular Carcinoma. EBioMedicine (2019) 42:363–74. doi: 10.1016/j.ebiom.2019.03.022
70. Pan L, Fang J, Chen MY, Zhai ST, Zhang B, Jiang ZY, et al. Promising Key Genes Associated With Tumor Microenvironments and Prognosis of Hepatocellular Carcinoma. World J Gastroenterol (2020) 26:789–803. doi: 10.3748/wjg.v26.i8.789
71. Zhang FP, Huang YP, Luo WX, Deng WY, Liu CQ, Xu LB, et al. Construction of a Risk Score Prognosis Model Based on Hepatocellular Carcinoma Microenvironment. World J Gastroenterol (2020) 26:134–53. doi: 10.3748/wjg.v26.i2.134
72. Guo X, Jiang H, Shi B, Zhou M, Zhang H, Shi Z, et al. Disruption of PD-1 Enhanced the Anti-Tumor Activity of Chimeric Antigen Receptor T Cells Against Hepatocellular Carcinoma. Front Pharmacol (2018) 9:1118. doi: 10.3389/fphar.2018.01118
73. Kole C, Charalampakis N, Tsakatikas S, Vailas M, Moris D, Gkotsis E, et al. Immunotherapy for Hepatocellular Carcinoma: A 2021 Update. Cancers (2020) 12:2859. doi: 10.3390/cancers12102859
74. Lai X, Friedman A. Combination Therapy of Cancer With Cancer Vaccine and Immune Checkpoint Inhibitors: A Mathematical Model. PLoS One (2017) 12:e0178479. doi: 10.1371/journal.pone.0178479
75. Kleponis J, Skelton R, Zheng L. Fueling the Engine and Releasing the Break: Combinational Therapy of Cancer Vaccines and Immune Checkpoint Inhibitors. Cancer Biol Med (2015) 12:201–8. doi: 10.7497/j.issn.2095-3941.2015.0046
76. Batlle E, Massagué J. Transforming Growth Factor-β Signaling in Immunity and Cancer. Immunity (2019) 50:924–40. doi: 10.1016/j.immuni.2019.03.024
77. Shrestha R, Prithviraj P, Bridle KR, Crawford DHG, Jayachandran A. Combined Inhibition of TGF-β1-Induced EMT and PD-L1 Silencing Re-Sensitizes Hepatocellular Carcinoma to Sorafenib Treatment. J Clin Med (2021) 10:1889. doi: 10.3390/jcm10091889
78. Doi T, Fujiwara Y, Koyama T, Ikeda M, Helwig C, Watanabe M, et al. Phase I Study of the Bifunctional Fusion Protein Bintrafusp Alfa in Asian Patients With Advanced Solid Tumors, Including a Hepatocellular Carcinoma Safety-Assessment Cohort. oncologist (2020) 25:e1292–302. doi: 10.1634/theoncologist.2020-0249
79. Hoffmann K, Shibo L, Xiao Z, Longerich T, Büchler MW, Schemmer P. Correlation of Gene Expression of ATP-Binding Cassette Protein and Tyrosine Kinase Signaling Pathway in Patients With Hepatocellular Carcinoma. Anticancer Res (2011) 31:3883–90.
80. Zuo Q, Huang H, Shi M, Zhang F, Sun J, Bin J, et al. Multivariate Analysis of Several Molecular Markers and Clinicopathological Features in Postoperative Prognosis of Hepatocellular Carcinoma. Anatomical Rec (Hoboken N.J. 2007) (2012) 295:423–31. doi: 10.1002/ar.21531
81. Gnoni A, Licchetta A, Memeo R, Argentiero A, Solimando AG, Longo V, et al. Role of BRAF in Hepatocellular Carcinoma: A Rationale for Future Targeted Cancer Therapies. Medicina (Kaunas Lithuania) (2019) 55:754. doi: 10.3390/medicina55120754
82. Wang W, Xiao Y, Li S, Zhu X, Meng L, Song C, et al. Synergistic Activity of Magnolin Combined With B-RAF Inhibitor SB590885 in Hepatocellular Carcinoma Cells via Targeting PI3K-AKT/mTOR and ERK MAPK Pathway. Am J Trans Res (2019) 11:3816–24.
Keywords: monotherapy, combination therapy, hepatocellular carcinoma, immune, PD-1
Citation: Ouyang T, Kan X and Zheng C (2022) Immune Checkpoint Inhibitors for Advanced Hepatocellular Carcinoma: Monotherapies and Combined Therapies. Front. Oncol. 12:898964. doi: 10.3389/fonc.2022.898964
Received: 18 March 2022; Accepted: 25 May 2022;
Published: 16 June 2022.
Edited by:
Jie Xu, Fudan University, ChinaReviewed by:
Antonio Giovanni Solimando, University of Bari Aldo Moro, ItalyWeicheng Liang, Sun Yat-sen University, China
Jiang Chen, Zhejiang University, China
Copyright © 2022 Ouyang, Kan and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chuansheng Zheng, aHF6Y3N4aEBzaW5hLmNvbQ==
†These authors have contributed equally to this work