 Tizian Rosenstock1,2*
Tizian Rosenstock1,2* Paul Pöser1
Paul Pöser1 David Wasilewski1
David Wasilewski1 Hans-Christian Bauknecht3
Hans-Christian Bauknecht3 Ulrike Grittner4
Ulrike Grittner4 Thomas Picht1,5
Thomas Picht1,5 Martin Misch1
Martin Misch1 Julia Sophie Onken1
Julia Sophie Onken1 Peter Vajkoczy1
Peter Vajkoczy1- 1Department of Neurosurgery, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany
- 2Berlin Institute of Health at Charité – Universitätsmedizin Berlin, BIH Biomedical Innovation Academy, BIH Charité Digital Clinician Scientist Program, Berlin, Germany
- 3Institute of Neuroradiology, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany
- 4Institute of Biometry and Clinical Epidemiology, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany
- 5Cluster of Excellence: “Matters of Activity. Image Space Material,” Humboldt University, Berlin, Germany
Object: Recent studies demonstrated that gross total resection of brain metastases cannot always be achieved. Subtotal resection (STR) can result in an early recurrence and might affect patient survival. We initiated a prospective observational study to establish a MRI-based risk assessment for incomplete resection of brain metastases.
Methods: All patients in whom ≥1 brain metastasis was resected were prospectively included in this study (DRKS ID: DRKS00021224; Nov 2020 – Nov 2021). An interdisciplinary board of neurosurgeons and neuroradiologists evaluated the pre- and postoperative MRI (≤48h after surgery) for residual tumor. Extensive neuroradiological analyses were performed to identify risk factors for an unintended STR which were integrated into a regression tree analysis to determine the patients’ individual risk for a STR.
Results: We included 150 patients (74 female; mean age: 61 years), in whom 165 brain metastases were resected. A STR was detected in 32 cases (19.4%) (median residual tumor volume: 1.36ml, median EORrel: 93.6%), of which 6 (3.6%) were intended STR (median residual tumor volume: 3.27ml, median EORrel: 67.3%) - mainly due to motor-eloquent location - and 26 (15.8%) were unintended STR (uSTR) (median residual tumor volume: 0.64ml, median EORrel: 94.7%). The following risk factors for an uSTR could be identified: subcortical metastasis ≥5mm distant from cortex, diffuse contrast agent enhancement, proximity to the ventricles, contact to falx/tentorium and non-transcortical approaches. Regression tree analysis revealed that the individual risk for an uSTR was mainly associated to the distance from the cortex (distance ≥5mm vs. <5mm: OR 8.0; 95%CI: 2.7 – 24.4) and the contrast agent patterns (diffuse vs. non-diffuse in those with distance ≥5mm: OR: 4.2; 95%CI: 1.3 – 13.7). The preoperative tumor volume was not substantially associated with the extent of resection.
Conclusions: Subcortical metastases ≥5mm distant from cortex with diffuse contrast agent enhancement showed the highest incidence of uSTR. The proposed MRI-based assessment allows estimation of the individual risk for uSTR and can help indicating intraoperative imaging.
Introduction
Metastasis to the brain is a common complication of systemic cancer with an incidence of 20-40%, with lung cancer (20–56% of patients), breast cancer (5–20%) and melanoma (7–16%) representing the most common primary tumor entities (1–3). They can severely compromise patients’ quality of life due to symptoms (such as focal neurologic deficits and epileptic seizures) and can directly lead to death in 31% - 52% of these patients (2, 4, 5).
Due to novel targeted therapies, systemic control is more often achieved, resulting in prolonged survival and thus increasing the incidence of cerebral metastases (4, 6). Since the blood brain barrier and the specific tumor microenvironment limit the efficacy of many therapeutic agents, surgical resection and radiation therapy are the primary options for local control (3, 7–9). Local recurrence could be related to subtotal resection, emphasizing the importance of objectively assessing the extent of resection (EOR). So far, EOR in brain metastases has only been analyzed in retrospective studies. They showed that the rate of gross total resection (GTR) is lower than assumed in the past, and that surgical assessment alone cannot serve as an objective measure (10–13).
The use of intraoperative imaging such as MRI (iopMRI) or ultrasound (iopUS) is well established in primary brain tumors to improve the extent of resection (14–16). The cost of an iopMRI unit ranges from $3 million to $7 million, plus the cost of remodeling the operating room. Since radiological staff is also required, iopMRI is not available in every hospital (17). In contrast, iopUS is a relatively cost-effective technology, but one that requires significant expertise and thus also hinder its application (14). The estimated incremental cost per case are $1813 for iopMRI and $333 for iopUS (18). Rational resource allocation and individual evaluation (considering the advantages and disadvantages of iopMRI and iopUS) are necessary to accurately identify cases that may benefit.
The aim of this prospective study was to identify risk factors for a subtotal brain metastasis resection. In addition, a statistical model based on patient characteristics and the preoperative MRI will be established to determine the patients’ individual risk for a subtotal resection (STR).
Methods
Study Design
This prospective, observational study started in November 2020, was approved by the Ethics Committee of the Charite - Universitätsmedizin Berlin (EA2/232/20) and is in accordance with the STROBE Guidelines (19) and the ethical standards of the Declaration of Helsinki. This unicentric analysis is part of a prospective brain metastasis database, registered with the German Clinical Trials Register (DRKS-ID: DRKS00021224).
Patients
A prospective database of all patients (age ≥18 years) who underwent neurosurgical resection of one or more brain metastases between 11/2020 and 11/2021 was established using the Research Electronic Data Capture (REDCap) platform (20). Exclusion criteria were the missing of a (preoperative) MR imaging (e.g. due to an emergency craniotomy or a non-MRI capable pacemaker). All patients were examined preoperatively and postoperatively for the presence of neurologic deficits by the treating neurosurgical team. The degree of disability/dependence in daily living was estimated using the Karnofsky Performance Scale (KPS) and the modified Rankin Scale (mRS). The primary tumor and the presence or number of intra/extracranial metastases were recorded in addition to oncological history.
Neurosurgical Resection
All operations were performed in microsurgical technique using the microscope and neuronavigation. The treating neurosurgeon decided about using intraoperative neuromonitoring (IOM) to ensure the integrity of the motor system based on a previously published risk stratification (21, 22). Warning criteria were a decrease in MEP amplitudes >50% and a subcortical stimulation intensity <5mA which we described in detail elsewhere (23). No awake craniotomies were performed in this series. If a metastasis was intentionally resected incompletely (e.g., because of infiltration of the skull base or because of eloquent location such as near the motor cortex), this was documented separately. If residual tumor was found postoperatively, it was at the discretion of the treating neurosurgeon to decide on re-resection based on the size of the residual tumor and the presence of further metastases.
MR Imaging
Following the EANO guidelines (24), all included patients received a 1.5T or 3T MRI scan before and after surgery (≤48h). T1-weighted 3D gradient echo sequences (MP-Rage, 1mm isotropic voxel size) with gadoterate meglumine (0.2ml/kg body weight; Dotarem; Guerbet; France) were used to characterize the metastases. In addition, T2 sequences were used to assess perifocal edema, SWI sequences (or cerebral computer tomography if available) to analyze hemorrhage, and diffusion-weighted imaging to assess ischemia. The following characteristics were analyzed preoperatively with the planning software Elements (Brainlab AG): number of brain metastases, localization, volume, tumoral cyst/necrosis, perifocal edema, hemorrhage, opening of a ventricle probable (threshold ≤5 mm), contact with dura/distance to brain surface, tumor-cortex angle (Figure 1), signs of meningeosis and detection of hydrocephalus. The contrast agent patterns were also evaluated to determine whether a metastasis was circumscribed if it showed a) clear margin to the healthy brain tissue and b) round, circumscribed contrast medium uptake without filiform/finger-shaped spreading. If the criteria were not met or there was an unclear assessment, the contrast agent patterns were classified as diffuse.
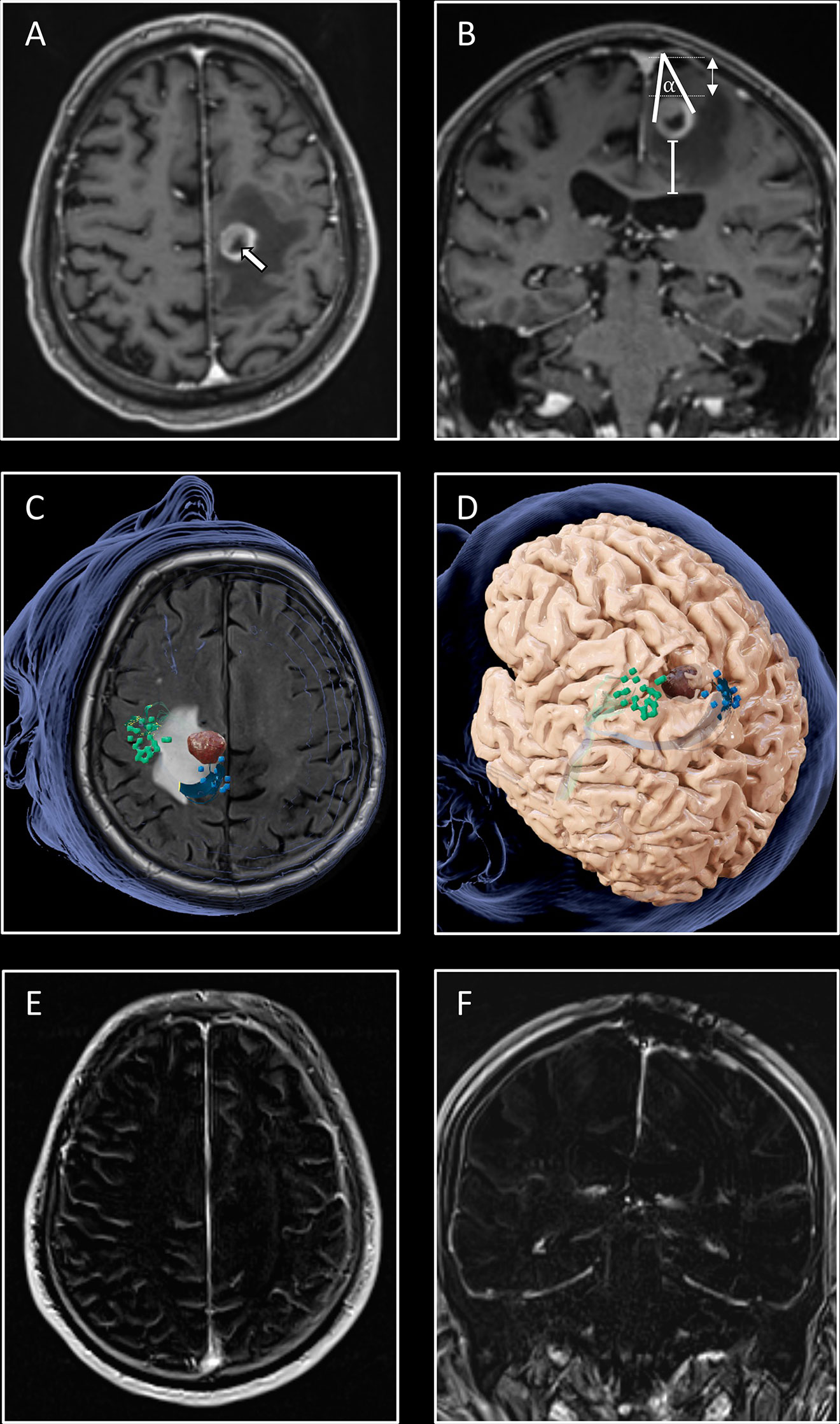
Figure 1 Illustration of the workflow. An 80-year-old patient presented to the emergency department with inability to walk and with leg accentuated hemiparesis. MRI (A, B) revealed a circumscribed contrast agent enhancing tumor with a central necrosis (white arrow) in the left hemisphere in precentral locaton. Volume of the tumor (2.5ml), edema (26ml), the distance from the cortex (white double arrow; 19mm) and from the ventricle (white line; 29mm) were measured. The tumor-cortex angle (α; 35°) was determined only for subcortical metastases, with the angle legs defined by the largest diameter and the apex defined by the cortical approach. The cortical nTMS motor mapping (C) for the upper (green bullets) and lower extremity (blue bullets) showed approximation of the tumor to the motor cortex. The minimum distance between the tumor and the corticospinal tract was 8mm (D), indicating a motor-associated location with higher risk for postoperative motor worsening (22). An interhemispheric approach under intraoperative neuromonitoring guidance was chosen for tumor removal. The patient recovered postoperatively with ability to walk again. No residual contrast agent enhancement was detected in the postoperative T1 subtraction sequences, confirming a GTR (E, F).
Patients with presumed motor- or language-associated tumor location underwent navigated transcranial magnetic stimulation (nTMS) mapping for localization of cortical functional areas (22, 25). These functional data were used as seeding regions for the diffusion tensor imaging (DTI) tractography to visualize the corticospinal tract (for motor cases) and/or the language network as previously published elsewhere (22, 25). The institutional’s neuroimaging experts and the treating neurosurgical team decided about a motor-/language-associated tumor location based on the individual risk analysis (22, 26).
An independent neuroradiologist with more than 15 years of experience validated and reviewed the extent of resection (EOR) analysis, which was evaluated primarily by an interdisciplinary panel of neurosurgeons (including the treating neurosurgical team) and neuroradiologists. The T1 subtraction sequences (27) were used to divide the cases into gross total resection (GTR = complete resection of the contrast-enhancing tumor parts without hints of residual tumor tissue), intended subtotal resection (iSTR = intentionally left tumor parts, e.g. due to proximity to the corticospinal tract) and unintended subtotal resection (uSTR). Any contrast uptake on the postoperative MRI was considered as residual tumor. In these cases, the volume as well as the relative extent of resection [EORrel = 1 – (volumetumor postop./volumetumor preop.)] were measured.
Statistical Analysis
SPSS Statistics 25.0 (IBM Corp., Armonk, N.Y., USA) and R (R Core Team) were used to analyze the data in collaboration with the Institute of Biometry and Clinical Epidemiology – Charité. For the bivariate analysis, we used descriptive statistics and standardized mean differences (SMD) based on approaches of Austin (28) and Yang & Dalton (29) for dichotomous and multinomial variables to examine extent of group differences between those patients with GTR compared to those with uSTR. In this exploratory study, the interpretation of the results is based on the effect size estimates. To account for the dependency of measures in the same individuals, the calculation of the significance level α was performed cautiously, as group differences were tested with binary logistic generalized estimating equations (GEE). For the multiple analysis (aiming to determine relevant risk factors for an uSTR), we used the package rpart of the R statistical platform (4.0.2) to calculate regression trees with 10-fold cross validation (minimum number of patients in node for split: 18, minimum number of patients in bucket: 6, splitting index: Gini coefficient). The following independent factors were tested as potential risk factors.: side/location of brain metastases, tumor volume, distance from cortex, metastasis recurrency, presence of cystic/necrotic parts, bleeding, peritumoral edema, hydrocephalus, proximity to the ventricular system (cut-off value: 5mm), contract to falx/tentorium, signs for leptomeningeal disease, contrast agent patterns, tumor-cortex angle and the used surgical approach.
Results
Patients Sample
A total of 150 patients were included, in whom 165 metastases were resected. A detailed description of the patient characteristics is outlined in Table 1. The study population had a mean age of 61 years (range: 28-86 years; IQR: 14 years), with equal proportions of women and men (74 women; 49.3%).
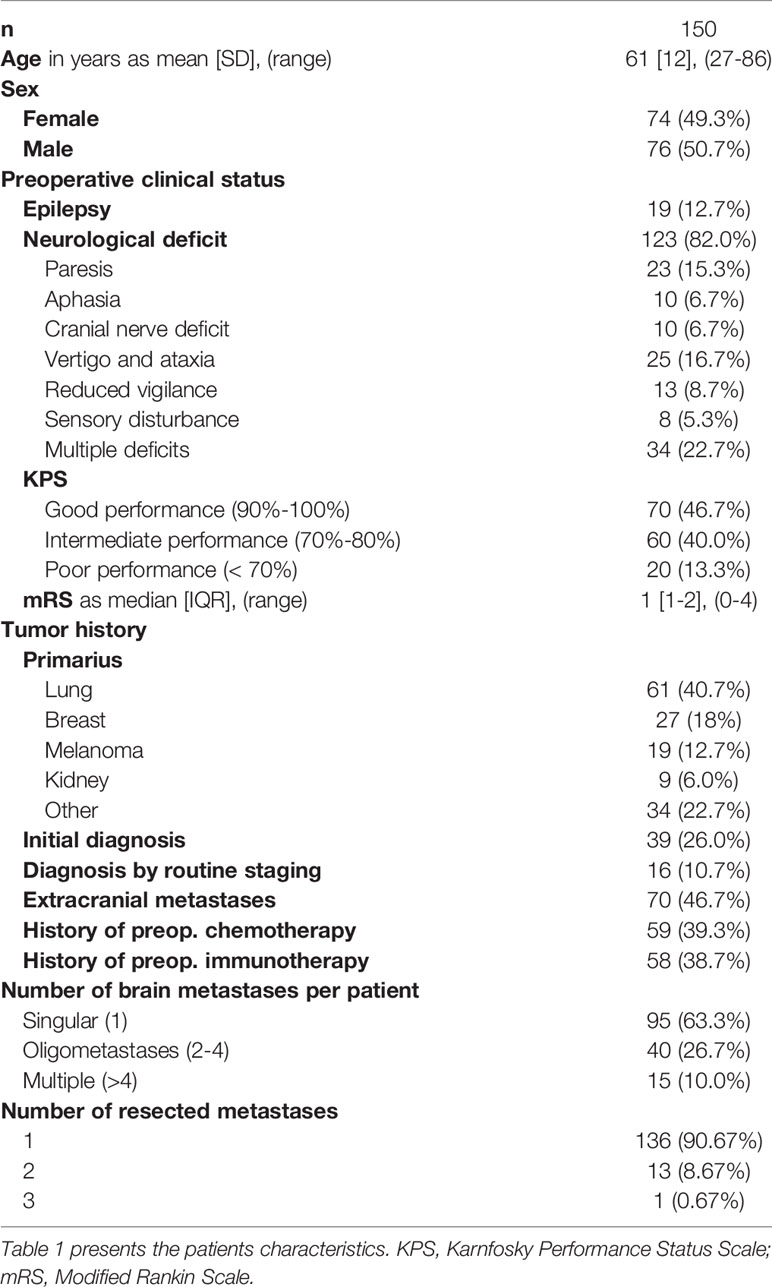
Table 1 Patient Sample.
One hundred and twenty-three patients (82.0%) had a preoperative neurologic deficit, with paresis (23 cases; 15.3%) and vertigo/ataxia (25 cases; 16.7%) being the most common entities. The preoperative neurologic deficits improved postoperatively in 53 of the 123 patients (43.1%). A new postoperative neurological deficit occurred in 14 cases (9.3%), of which 8 (5.3%) had new paresis, 3 (2.0%) had aphasia and 5 (3.3%) had other deficits such as ataxia. The new deficits were transient in 6 cases (4.0%) and permanent in 2 cases (1.3%), whereas no data could be obtained for 6 patients (4.0%) (loss of follow-up). Surgical revisions were required in 13 cases (8.7%) due to wound healing disorder (8 cases; 5.3%), postoperative hydrocephalus (2 cases; 1.3%) or postoperative bleeding (3 cases; 2.0%). Two patients (1.3%) developed a postoperative meningitis.
Metastases Characteristics
Most metastases were located supratentorially (125; 75.8%) and here most frequently in the frontal lobe (41; 24.8%). The metastases had a median tumor volume of 9.0ml (range 0.3ml – 124.0ml; IQR: 13.35ml) and an overall equal incidence in the right and left (cerebellar) hemispheres (78 cases each (47.3%)). In 39 cases (26.0%), the brain metastasis was the initial manifestation of cancer, with lung carcinoma being the most common primarius. Fourteen cases (8.5%) were metastatic recurrence. Seventy-three metastases (44.2%) grew to the cortex surface, whereas 92 metastases (55.8%) were located solely subcortically.
Extent of Resection Analysis
A gross total resection (GTR) was achieved in 133 metastases (80.6%). In cases of a STR (32 cases; 19.4%), the median residual tumor volume was 1.36ml (range 0.03ml – 8.70ml; IQR: 1.14ml) and the median EORrel was 93.6% (range 48% - 99%; IQR: 0.21). In 6 metastases (3.6%), an iSTR was performed for the following reasons: motor eloquent location (4 cases; 2.4%), skull base infiltration (1 case; 0.6%) and brainstem infiltration (1 case; 0.6%). The postoperative MRI revealed an uSTR in 26 metastases (15.8%), in which 2 metastases (1.2%; 7.7% of uSTR) were decided to undergo a re-resection and 24 metastases (14.6%; 92.3% of uSTR) were no re-resected. Residual tumor volume was significantly larger in the iSTR group (median absolute volume 3.27ml, range 1.45ml – 8.70ml; IQR: 4.01ml) compared to the uSTR group (median 0.64ml; range 0.03ml – 2.46ml; IQR: 0.89ml) (p <.001; SMD = 1.80) which could also be observed with the relative extent of resection (uSTR: median EORrel = 94.7%, range 52% - 99%, IQR: 0.17; iSTR: median EORrel = 67.3%, range 48% - 93%, IQR: 0.36; p = .003, SMD = 1.38).
Table 2 shows the bivariate analysis of the metastases’ characteristics and the EOR to identify risk factors for an uSTR. The iSTR were excluded from this analysis (Supplement 1). Cortical metastases had a low risk of an uSTR while subcortical locations ≥5mm distant from cortex and non-transcortical approaches were associated with higher risk of uSTR (Figure 2; distance from cortex: p <.001, SMD = 1.08; surgical approach: p = .004; SMD = 1.03). Patients in whom the metastasis showed well-defined/circumscribed contrast agent enhancement were less likely to have an uSTR (Figure 2, p = .017, SMD = 0.67). Falx/tentorium contact and proximity to the ventricles were also associated with a higher risk of uSTR (Figure 2, falx/tentorium contact: p = .020, SMD = 0.55; proximity to ventricles: p = .003, SMD = 0.65). Patients with an intratumoral cyst/necrosis were more likely to have an uSTR (Table 2, p = .063; SMD = 0.40). Neither other metastases’ characteristics (such as the preoperative tumor volume) nor the application of IOM showed any substantial association to the risk of uSTR (Table 2).
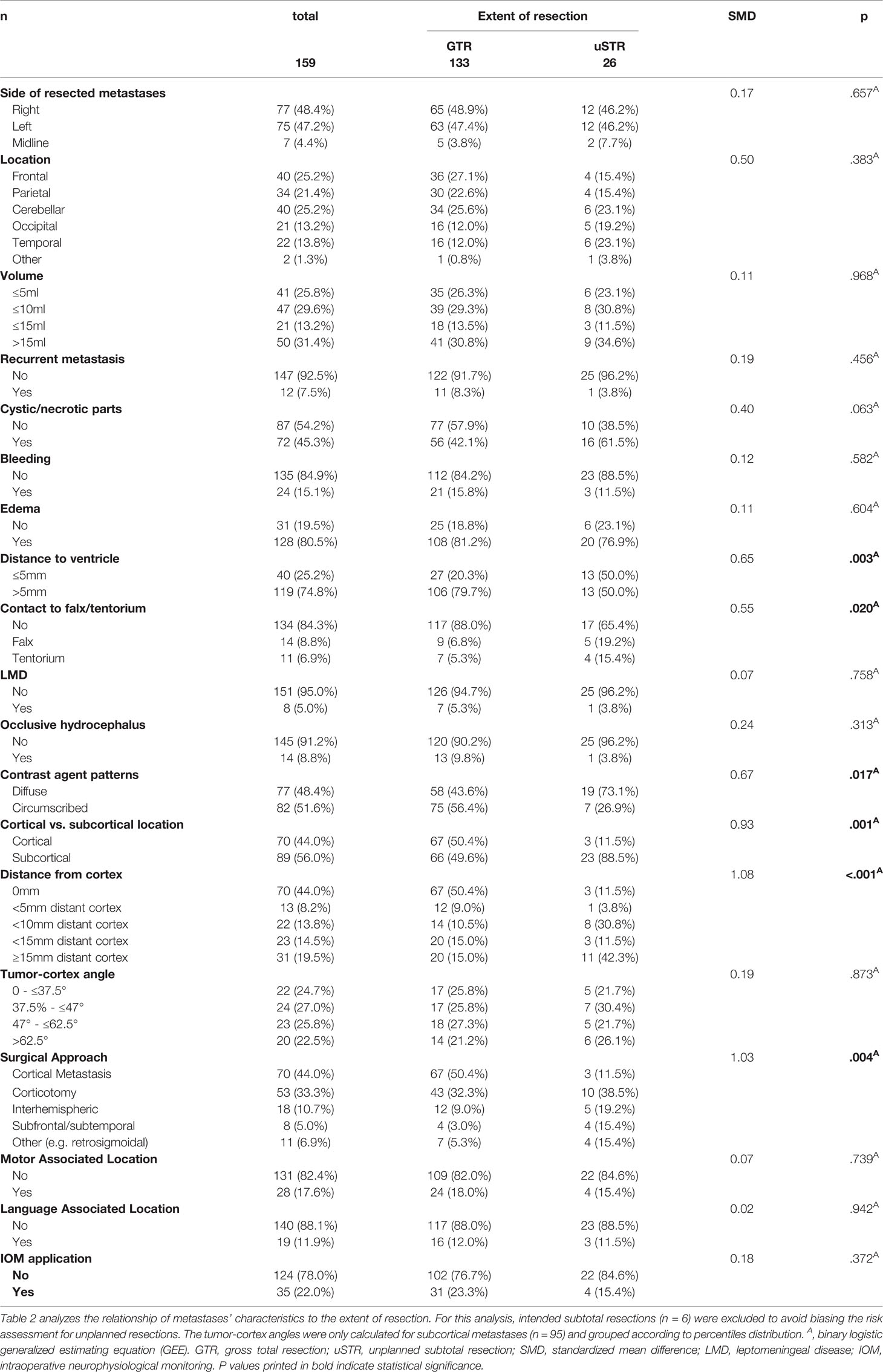
Table 2 Bivariate Analysis for Unintended Subtotal Resections.

Figure 2 Univariate analysis of the EOR. Bar graphs showing the relationship between the EOR and the tumor location (A), the distance to the ventricle system (B)/to the cortex (C), the contrast agent patterns (D), the chosen surgical approach (E) and to the falx-tentorium contact (F). GTR, gross total resection, uSTR, unintended subtotal resection.
Regression Tree Analysis
The before mentioned parameters were included in the regression tree analysis (Figure 3). The distinction between cortical and subcortical location (with a calculated threshold of 5mm) was the most impacting risk parameter (rate of uSTR: 4.8% vs. 28.9%). The first node of the tree (distance from cortex ≥ 5mm) shows a sensitivity of 84.6%, specificity of 59.4%, positive predictive value (PPV) of 28.9% and a negative predictive value (NPV) of 95.2%. In case of a subcortical metastasis (≥ 5mm distant from cortex), the regressions tree analysis revealed that a diffuse contrast agent enhancement was associated with a risk for an uSTR (43.2% vs. 15.4%). The analysis of the entire regression tree with both nodes shows an accuracy of 80.5%, a sensitivity of 61.5%, a specificity of 84.2%, a PPV of 43.2% and a NPV of 91.8%. The clinical applicability of the regression tree is illustrated in Figure 4.
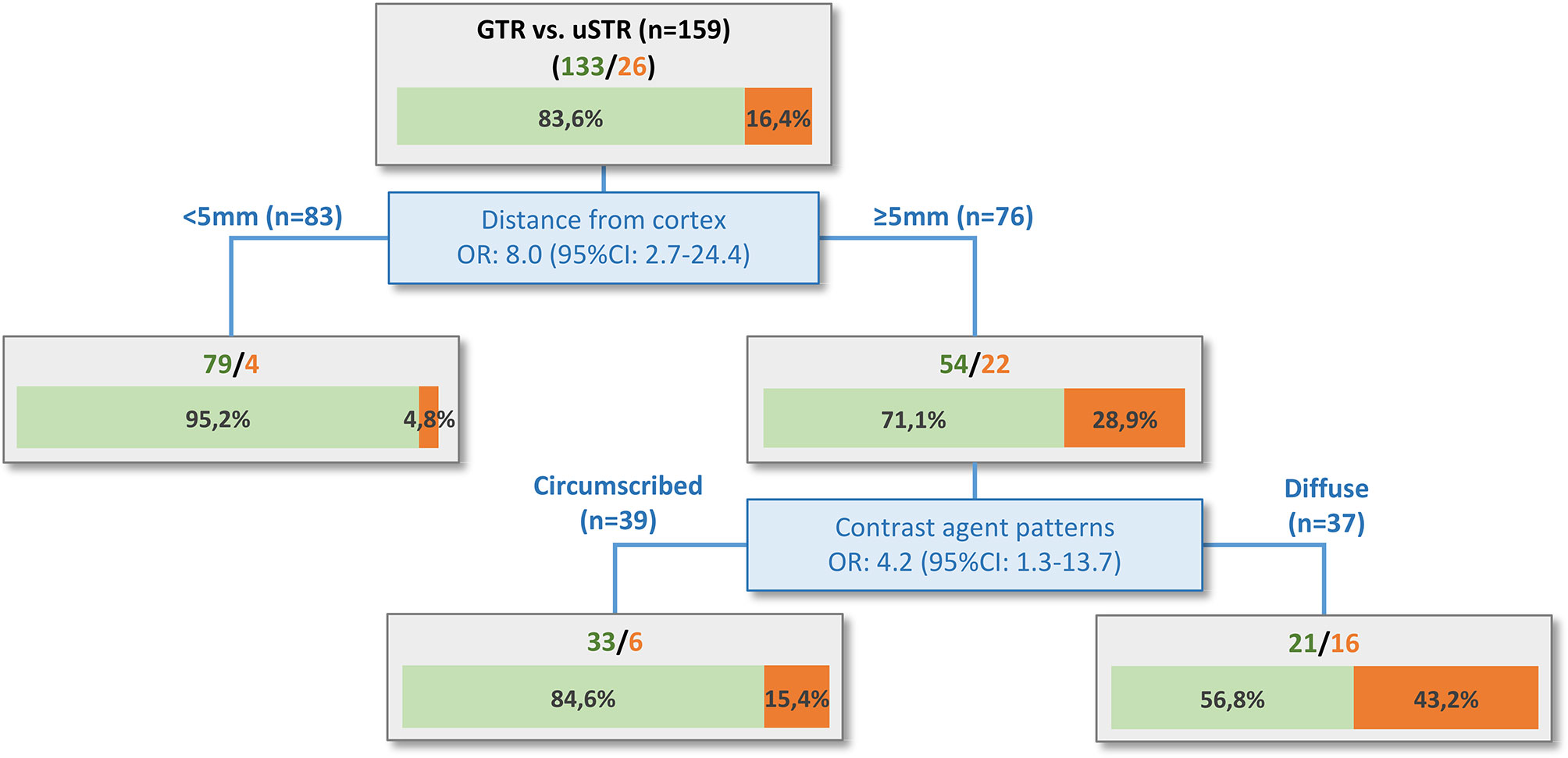
Figure 3 Regression tree analysis. The distance of the metastasis from the cortex is the most relevant risk factor, with 5mm being the cut-off value for higher (28.9%) or lower (4.8%) probability of an uSTR. The risk for patients with metastasis ≥5mm distant from cortex can be further stratified based on the contrast agent patterns. Subcortical metastases with clear margins to the healthy brain tissue and round, circumscribed contrast agent enhancement without filiform/finger-shaped spreading had a lower risk (15.4%) for an uSTR. In contrast, subcortical metastases with diffuse contrast agent enhancement had the highest risk (43.2%) for an uSTR. The tree diagram also shows the individual odds ratios (OR) with 95% confidence interval (95%CI) of the parameters.
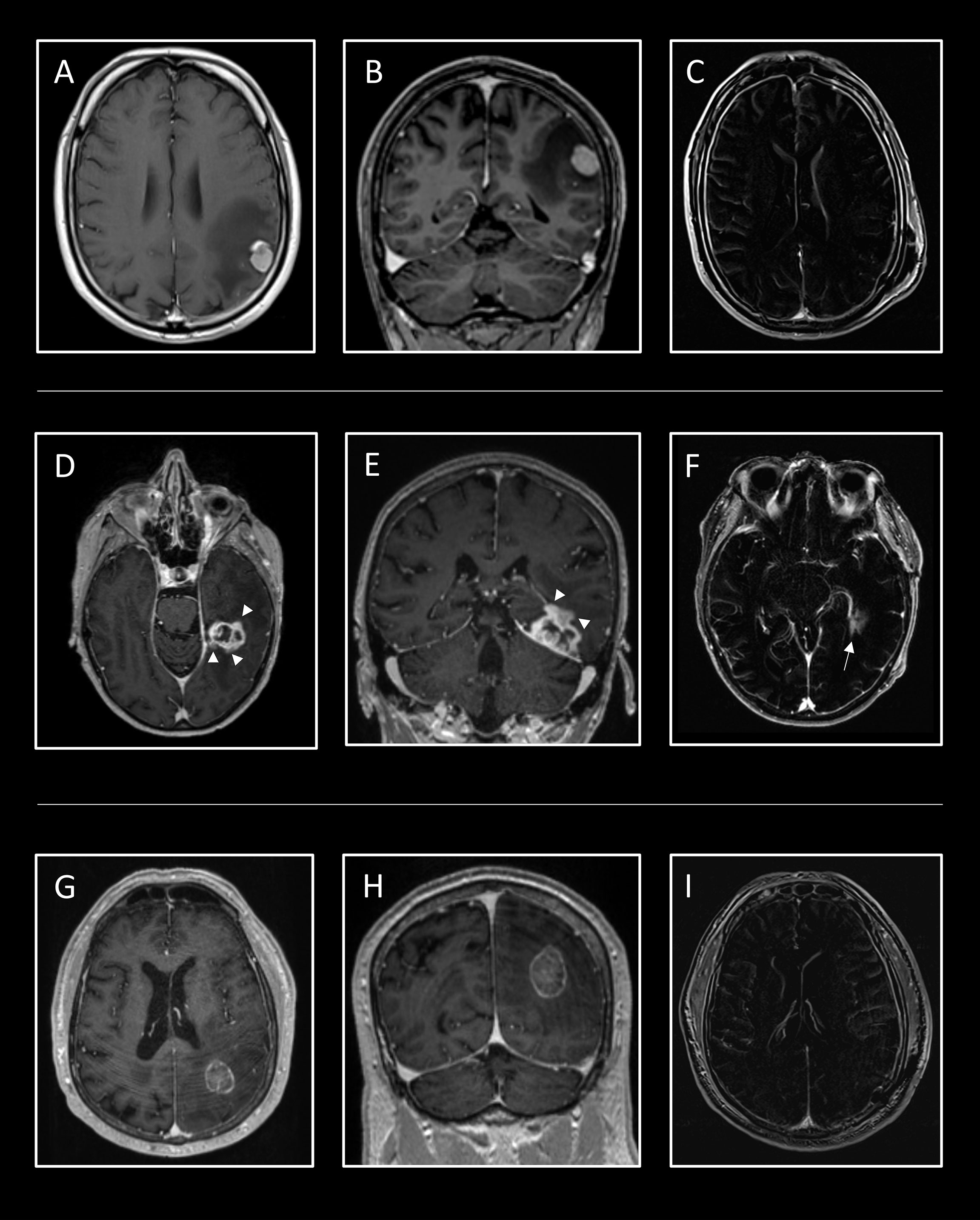
Figure 4 Case examples for the application of the regression tree. In the first line, the case of a 56-year-old man is shown who presented to the emergency department with an epileptic seizure and aphasia. Cerebral MRI showed a homogeneous contrast-enhancing cortical tumor in the parietal lobe with a volume of 2.2ml and extensive perifocal edema (A, B). The risk of uSTR is very low at 4.8%, thus a GTR was confirmed in the postoperative T1 subtraction sequence (C). Additionally, the preoperative aphasia improved. The second case shows a 69-year-old woman whose temporal metastasis of esophageal carcinoma grew progressively to 9.5ml despite radiation (D, E). Neurological examination revealed mild aphasia. Detailed analysis revealed an irregular/diffuse contrast agent enhancement (white arrowheads), which, in combination with a distance of 15.4mm from the cortex, indicates a high risk of an uSTR at 43.2%. The aphasia improved postoperatively, but a residual tumor (white arrow) of 0.6ml (EORrel = 94%) was detected (F). At the bottom, the MRI of a 70-year-old man who suffered from ataxia and visual disturbance presents a subcortical tumor in the parietal lobe with a volume of 9.0ml (G, H). The tumor has circumscribed contrast agent enhancement, with 11mm distant from the cortex, thus the risk for uSTR is moderate at 15.4%. Postoperatively, the ataxia and visual impairment improved and a GTR was obtained (I).
Discussion
Main Finding of the Study
This is the first study which prospectively analyzed the extent of resection in brain metastases. A GTR was achieved in 80.6%, whereas an iSTR was observed in 3.6% and an uSTR in 15.8%. The interdisciplinary neurosurgical and neuroradiological analysis of the preoperative MRIs allowed us to identify risk factors for uSTR, with patients having a subcortical metastasis (≥5mm distant from cortex) with diffuse contrast enhancement being at highest risk. Regression tree analysis allows easy clinical application to decide whether to use intraoperative imaging techniques such as iopMRI or iopUS to allow complete resection.
Preoperative neurologic deficits improved in 43.1% of our patients and the incidence of new postoperative permanent deficits was very low, emphasizing the role of brain metastasis resection in oncological treatment. Analogous to gliomas, the EOR of brain metastases has recently become a research focus, although only data from retrospective studies are available to date (10, 13, 30).
Extent of Resection in Brain Metastases
The incidence of GTR was 80.6% in our cohort, but numbers of so far published retrospective MRI studies varied widely (ranging from 61% to 86%) (10, 11, 13, 30, 31). Different influencing factors are conceivable, such as heterogeneous patient populations, varying use of neuronavigation, neuromonitoring, sodium fluorescein, and intraoperative imaging (iopMRI, iopUS). In addition, the methods used to assess the EOR differed in those studies or were not defined precisely. In the present series, all cases were discussed in an interdisciplinary board and were reviewed by an independent neuroradiologist with many years of experience.
Recently, it was shown that the surgeon’s estimation was misleading in 29-40% of brain metastases cases, thus recommending the routine use of postoperative MRI to assess the EOR (10, 11). Kamp et al. showed in a retrospective analysis of 116 patients an increased risk of local recurrence, if residual tumor was present in the postoperative MRI (OR 8.2; p <.001) (13). Another retrospective study of 64 patients demonstrated a shortened mean survival of 5.6 months in patients with STR compared with 12 months in patients with GTR (p = .025) (10). Another retrospective study of 373 patients reported the same figures, underscoring the importance of GTR in improving survival (30). In contrast, one report found no significant association between STR and shorter survival, indicating the need for prospective studies (32). Additionally, there is currently no study on whether patients with oligo- or multiple metastases benefit from a GTR. In the previous studies, there are also no data on a cut-off postoperative tumor volume/EORrel indicating re-resection, which may also explain the low re-resection rate in our cohort.
In this study, we identified the following risk factors for uSTR: subcortical metastasis (≥5mm distant from cortex), diffuse contrast agent patterns, contact to the falx/tentorium and non-transcortical approaches. Surgical view can be limited in cases with contact to the falx/tentorium and when using non-transcortical approaches, since tumor tissue can be located behind these structures/”behind the corner”. Thus, the chosen surgical approach also influences the EOR. In patients with cystic/necrotic metastasis, the incidence of uSTR was higher, as it was in a similar retrospective study (11). After opening the tumor cyst/resecting the necrosis, collapse of the tumor walls may occur, which could cause brain shift and increase the risk for uSTR. In contrast, a motor/language associated localization was not associated to a higher risk for uSTR, since we analyzed iSTR separately. Risk stratification and standardized surgical planning with nTMS and DTI tractography are well established in our department for balancing between optimizing the EOR and preventing new neurological deficits (22, 26). The use of these technologies in those challenging cases showed improved functional outcome as well as EOR at the same time (33, 34). Standardized criteria for the use of IOM, particularly in high-risk cases, may explain why it was not substantially associated with EOR in this cohort. Interestingly, patients with a larger tumor volume had no higher risk of uSTR in our series, which contrasts with the results of the aforementioned study (11). The differences may be related to selection bias in their retrospective analysis and to different patient populations – e.g. the median tumor volume and the rate of GTR differed. The multivariate regression tree analysis revealed subcortical metastases (≥5mm distant from cortex) and diffuse contrast agent enhancement to be the most important risk factors. Thus, the probability of uSTR (ranging from 4.8% to 43.2%) can be estimated preoperatively for the first time, thereby determining the necessity for intraoperative imaging to evaluate for residual tumor.
Intraoperative Imaging
The iopMRI has become an established intraoperative imaging technique for glioma resections showing an improved EOR and progression-free survival (15, 35, 36). To date, resection control of brain metastases by iopMRI has not been investigated. The use of iopMRI is associated with some limitations, since it requires technical, personnel and financial effort, which necessitates a rational, resource-oriented patient allocation (17). Additionally, iopMRI prolongs operating times and causes a large logistical burden, so not all tumor resections can be performed with iopMRI, especially since it is not available in all hospitals (37, 38).
Several observational studies have evaluated iopUS as imaging technique for real-time guidance during brain tumor resection and for improving the EOR (14, 39). The easy and cost-effective application are very important advantages in addition to the ability to localize the tumor despite the intraoperative brain shift (39, 40). However, the use of intraoperative ultrasound is accompanied by the common limitations such as high inter-operator variability, necessary experience, as well as image artifacts occurring in the course of surgery, which can hinder residual tumor detection (39, 41).
Another intraoperative imaging technique is the application of 5-aminolevulinic acid (5-ALA) which is converted to the fluorescent agent protoporphyrin IX and allows selective visualization of tumor tissue after blue-light illumination (42). Similar to iopMRI and iopUS, the use of 5-ALA for resection guidance was mainly investigated in high-grade glioma and showed improved EOR as well as improved (overall) survival (43). Only a few studies examined 5-ALA in brain metastases, but the rate of 5-ALA derived fluorescence was significantly lower (ranging between from 40.5% to 69%) compared to glioma, with no correlation to location or subtype (44–46). Thus, routine use of 5-ALA for resection guidance of brain metastases is severely limited.
Sodium fluorescein is another widely used fluochrome which is extravasated at locations harboring breached blood-brain barrier (e.g. in brain tumors) and equally demonstrated an advantage for EOR as well as survival (47, 48). In contrast to 5-ALA, sodium fluorescein provided higher fluorescence rates in brain metastases (ranging from 90% to 95%), making it more suitable for routine metastases resection guidance (49, 50). A prospective study is warranted to assess whether the incidence of uSTR can be reduced by standard application of sodium fluorescein in high-risk patients.
Limitations
The current analysis allows for a preoperative MRI-based risk assessment for uSTR. Unfortunately, the use of fluochrome was not part of the prospective study protocol, so we cannot evaluate its benefit for the EOR. Due to the monocenter study design, center-specific decisions and treatments may have influenced the results. No conclusions can be drawn whether local recurrences are more frequent in patients with uSTR and whether this impacts oncological outcome. For this purpose, only retrospective data are available to date, demanding prospective studies to confirm the relevance of intraoperative imaging or re-resections. Moreover, systemic disease burden must be considered in the survival analysis of these patients as local (brain) tumor control is only one variable. Our analysis is limited by the small sample size in some subgroups (e.g., contact with tentorium/falx), therefore some statistically significant changes may have been missed. Future studies may comparatively investigate the role of individual imaging modalities such as iopMRI, iopUS, and sodium fluorescein in reducing the risk for uSTR.
Conclusions
Based on the preoperative MRI, the risk for uSTR in brain metastases can be estimated in a simple way for clinical routine. Subcortical metastases (>5mm distant from cortex) with diffuse contrast enhancement had the highest risk for an uSTR at 43.2% in contrast to cortical metastases at 4.8%. Thus, the utilization of intraoperative imaging techniques can be decided on an individual basis, whereas the efficiency of these should be investigated in the future.
Data Availability Statement
The datasets presented in this article are not readily available because of restrictions due to the Data Protection Act. Requests to access the datasets should be directed to TR.
Ethics Statement
The studies involving human participants were reviewed and approved by ethics committee of the Charité – Universitätsmedizin Berlin; EA2/232/20. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
Substantial contributions to the conception or design of the work: TR, JO, MM, PV. Data acquisition: TR, PP, H-CB. Analysis or interpretation of data for the work: TR, UG, JO, PV. Drafting the work or revising it critically for important intellectual content; TR, PP, DW, H-CB, UG, TP, PV. All authors contributed to the article and approved the submitted version.
Funding
The authors acknowledge the support of the Cluster of Excellence Matters of Activity. Image Space Material funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany´s Excellence Strategy – EXC 2025. Dr. Rosenstock is participant in the BIH Charité Digital Clinician Scientist Program funded by the Charité – Universitätsmedizin Berlin, and the Berlin Institute of Health at Charité (BIH).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.873175/full#supplementary-material
References
1. Patchell RA. The Management of Brain Metastases. Cancer Treat Rev (2003) 29(6):533–40. doi: 10.1016/S0305-7372(03)00105-1
2. Achrol AS, Rennert RC, Anders C, Soffietti R, Ahluwalia MS, Nayak L, et al. Brain Metastases. Nat Rev Dis Primers (2019) 5(1):5. doi: 10.1038/s41572-018-0055-y
3. Hatiboglu MA, Akdur K, Sawaya R. Neurosurgical Management of Patients With Brain Metastasis. Neurosurg Rev (2020) 43(2):483–95. doi: 10.1007/s10143-018-1013-6
4. McTyre ER, Johnson AG, Ruiz J, Isom S, Lucas JT Jr, Hinson WH, et al. Predictors of Neurologic and Nonneurologic Death in Patients With Brain Metastasis Initially Treated With Upfront Stereotactic Radiosurgery Without Whole-Brain Radiation Therapy. Neuro Oncol (2017) 19(4):558–66. doi: 10.1093/neuonc/now184
5. Neal MT, Chan MD, Lucas JT Jr., Loganathan A, Dillingham C, Pan E, et al. Predictors of Survival, Neurologic Death, Local Failure, and Distant Failure After Gamma Knife Radiosurgery for Melanoma Brain Metastases. World Neurosurg (2014) 82(6):1250–5. doi: 10.1016/j.wneu.2013.02.025
6. Zugazagoitia J, Guedes C, Ponce S, Ferrer I, Molina-Pinelo S, Paz-Ares L. Current Challenges in Cancer Treatment. Clin Ther (2016) 38(7):1551–66. doi: 10.1016/j.clinthera.2016.03.026
7. Patchell RA, Tibbs PA, Walsh JW, Dempsey RJ, Maruyama Y, Kryscio RJ, et al. A Randomized Trial of Surgery in the Treatment of Single Metastases to the Brain. N Engl J Med (1990) 322(8):494–500. doi: 10.1056/NEJM199002223220802
8. Vecht CJ, Haaxma-Reiche H, Noordijk EM, Padberg GW, Voormolen JH, Hoekstra FH, et al. Treatment of Single Brain Metastasis: Radiotherapy Alone or Combined With Neurosurgery? Ann Neurol (1993) 33(6):583–90. doi: 10.1002/ana.410330605
9. Bindal AK, Bindal RK, Hess KR, Shiu A, Hassenbusch SJ, Shi WM, et al. Surgery Versus Radiosurgery in the Treatment of Brain Metastasis. J Neurosurg (1996) 84(5):748–54. doi: 10.3171/jns.1996.84.5.0748
10. Olesrud IC, Schulz MK, Marcovic L, Kristensen BW, Pedersen CB, Kristiansen C, et al. Early Postoperative MRI After Resection of Brain Metastases-Complete Tumour Resection Associated With Prolonged Survival. Acta Neurochir (2019) 161(3):555–65. doi: 10.1007/s00701-019-03829-0
11. Kiesel B, Prihoda R, Borkovec M, Mercea PA, Steindl A, Berghoff AS, et al. Postoperative Magnetic Resonance Imaging After Surgery of Brain Metastases: Analysis of Extent of Resection and Potential Risk Factors for Incomplete Resection. World Neurosurg (2020) 143:e365–e73. doi: 10.1016/j.wneu.2020.07.150
12. Kiesel B, Thome CM, Weiss T, Jakola AS, Darlix A, Pellerino A, et al. Perioperative Imaging in Patients Treated With Resection of Brain Metastases: A Survey by the European Association of Neuro-Oncology (EANO) Youngsters Committee. BMC Cancer (2020) 20(1):410. doi: 10.1186/s12885-020-06897-z
13. Kamp MA, Rapp M, Buhner J, Slotty PJ, Reichelt D, Sadat H, et al. Early Postoperative Magnet Resonance Tomography After Resection of Cerebral Metastases. Acta Neurochir (2015) 157(9):1573–80. doi: 10.1007/s00701-015-2479-4
14. Mahboob S, McPhillips R, Qiu Z, Jiang Y, Meggs C, Schiavone G, et al. Intraoperative Ultrasound-Guided Resection of Gliomas: A Meta-Analysis and Review of the Literature. World Neurosurg (2016) 92:255–63. doi: 10.1016/j.wneu.2016.05.007
15. Li P, Qian R, Niu C, Fu X. Impact of Intraoperative MRI-Guided Resection on Resection and Survival in Patient With Gliomas: A Meta-Analysis. Curr Med Res Opin (2017) 33(4):621–30. doi: 10.1080/03007995.2016.1275935
16. Shi J, Zhang Y, Yao B, Sun P, Hao Y, Piao H, et al. Application of Multiparametric Intraoperative Ultrasound in Glioma Surgery. BioMed Res Int (2021) 2021:6651726. doi: 10.1155/2021/6651726
17. Golub D, Hyde J, Dogra S, Nicholson J, Kirkwood KA, Gohel P, et al. Intraoperative MRI Versus 5-ALA in High-Grade Glioma Resection: A Network Meta-Analysis. J Neurosurg (2020) 134(2):1–15. doi: 10.3171/2019.12.JNS191203
18. Eljamel MS, Mahboob SO. The Effectiveness and Cost-Effectiveness of Intraoperative Imaging in High-Grade Glioma Resection; a Comparative Review of Intraoperative ALA, Fluorescein, Ultrasound and MRI. Photodiagnosis Photodyn Ther (2016) 16:35–43. doi: 10.1016/j.pdpdt.2016.07.012
19. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet (2007) 370(9596):1453–7. doi: 10.1016/S0140-6736(07)61602-X
20. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J BioMed Inform (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
21. Schebesch KM, Brawanski A, Hohenberger C, Hohne J. Fluorescein Sodium-Guided Surgery of Malignant Brain Tumors: History, Current Concepts, and Future Project. Turk Neurosurg (2016) 26(2):185–94. doi: 10.5137/1019-5149.JTN.16952-16.0
22. Rosenstock T, Häni L, Grittner U, Schlinkmann N, Ivren M, Schneider H, et al. Bicentric Validation of the nTMS Motor Risk Stratification Model. J Neurosurg (2021) 136(4):1194–206. doi: 10.3171/2021.3.JNS2138
23. Rosenstock T, Tuncer MS, Munch MR, Vajkoczy P, Picht T, Faust K. Preoperative nTMS and Intraoperative Neurophysiology - A Comparative Analysis in Patients With Motor-Eloquent Glioma. Front Oncol (2021) 11:676626. doi: 10.3389/fonc.2021.676626
24. Le Rhun E, Guckenberger M, Smits M, Dummer R, Bachelot T, Sahm F, et al. EANO-ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up of Patients With Brain Metastasis From Solid Tumours. Ann Oncol (2021) 32(11):1332–47. doi: 10.1016/j.annonc.2021.07.016
25. Raffa G, Bahrend I, Schneider H, Faust K, Germano A, Vajkoczy P, et al. A Novel Technique for Region and Linguistic Specific nTMS-Based DTI Fiber Tracking of Language Pathways in Brain Tumor Patients. Front Neurosci (2016) 10:552. doi: 10.3389/fnins.2016.00552
26. Tuncer MS, Salvati LF, Grittner U, Hardt J, Schilling R, Bahrend I, et al. Towards a Tractography-Based Risk Stratification Model for Language Area Associated Gliomas. NeuroImage Clin (2021) 29:102541. doi: 10.1016/j.nicl.2020.102541
27. Ellingson BM, Wen PY, Cloughesy TF. Modified Criteria for Radiographic Response Assessment in Glioblastoma Clinical Trials. Neurotherapeutics (2017) 14(2):307–20. doi: 10.1007/s13311-016-0507-6
28. Austin PC. Using the Standardized Difference to Compare the Prevalence of a Binary Variable Between Two Groups in Observational Research. Commun Stat Simul Comput (2009) 38(6):1228–34. doi: 10.1080/03610910902859574
29. Yang D, Dalton JE. A Unified Approach to Measuring the Effect Size Between Two Groups Using SAS®, in: SAS Global Forum, Vol. 335. Cleveland, OH, USA (2012) pp. 1–6.
30. Winther RR, Hjermstad MJ, Skovlund E, Aass N, Helseth E, Kaasa S, et al. Surgery for Brain Metastases-Impact of the Extent of Resection. Acta Neurochir (2022). doi: 10.1007/s00701-021-05104-7
31. Benveniste RJ, Ferraro N, Tsimpas A. Yield and Utility of Routine Postoperative Imaging After Resection of Brain Metastases. J Neurooncol (2014) 118(2):363–7. doi: 10.1007/s11060-014-1440-3
32. Junger ST, Pennig L, Schodel P, Goldbrunner R, Friker L, Kocher M, et al. The Debatable Benefit of Gross-Total Resection of Brain Metastases in a Comprehensive Treatment Setting. Cancers (Basel) (2021) 13(6):1435. doi: 10.3390/cancers13061435
33. Krieg SM, Picht T, Sollmann N, Bahrend I, Ringel F, Nagarajan SS, et al. Resection of Motor Eloquent Metastases Aided by Preoperative nTMS-Based Motor Maps-Comparison of Two Observational Cohorts. Front Oncol (2016) 6:261. doi: 10.3389/fonc.2016.00261
34. Raffa G, Scibilia A, Conti A, Ricciardo G, Rizzo V, Morelli A, et al. The Role of Navigated Transcranial Magnetic Stimulation for Surgery of Motor-Eloquent Brain Tumors: A Systematic Review and Meta-Analysis. Clin Neurol Neurosurg (2019) 180:7–17. doi: 10.1016/j.clineuro.2019.03.003
35. Albuquerque LAF, Almeida JP, de Macedo Filho LJM, Joaquim AF, Duffau H. Extent of Resection in Diffuse Low-Grade Gliomas and the Role of Tumor Molecular Signature-A Systematic Review of the Literature. Neurosurg Rev (2021) 44(3):1371–89. doi: 10.1007/s10143-020-01362-8
36. Li XZ, Li YB, Cao Y, Li PL, Liang B, Sun JD, et al. Prognostic Implications of Resection Extent for Patients With Glioblastoma Multiforme: A Meta-Analysis. J Neurosurg Sci (2017) 61(6):631–9. doi: 10.23736/S0390-5616.16.03619-5
37. Kubben PL, Scholtes F, Schijns OE, Ter Laak-Poort MP, Teernstra OP, Kessels AG, et al. Intraoperative Magnetic Resonance Imaging Versus Standard Neuronavigation for the Neurosurgical Treatment of Glioblastoma: A Randomized Controlled Trial. Surg Neurol Int (2014) 5:70. doi: 10.4103/2152-7806.132572
38. Senft C, Bink A, Franz K, Vatter H, Gasser T, Seifert V. Intraoperative MRI Guidance and Extent of Resection in Glioma Surgery: A Randomised, Controlled Trial. Lancet Oncol (2011) 12(11):997–1003. doi: 10.1016/S1470-2045(11)70196-6
39. Sastry R, Bi WL, Pieper S, Frisken S, Kapur T, Wells W 3rd, et al. Applications of Ultrasound in the Resection of Brain Tumors. J Neuroimaging (2017) 27(1):5–15. doi: 10.1111/jon.12382
40. Gerard IJ, Kersten-Oertel M, Hall JA, Sirhan D, Collins DL. Brain Shift in Neuronavigation of Brain Tumors: An Updated Review of Intra-Operative Ultrasound Applications. Front Oncol (2020) 10:618837. doi: 10.3389/fonc.2020.618837
41. Steno A, Buvala J, Babkova V, Kiss A, Toma D, Lysak A. Current Limitations of Intraoperative Ultrasound in Brain Tumor Surgery. Front Oncol (2021) 11:659048. doi: 10.3389/fonc.2021.659048
42. Stummer W, Stocker S, Wagner S, Stepp H, Fritsch C, Goetz C, et al. Intraoperative Detection of Malignant Gliomas by 5-Aminolevulinic Acid-Induced Porphyrin Fluorescence. Neurosurgery (1998) 42(3):518–25; discussion 25-6. doi: 10.1097/00006123-199803000-00017
43. Eatz TA, Eichberg DG, Lu VM, Di L, Komotar RJ, Ivan ME. Intraoperative 5-ALA Fluorescence-Guided Resection of High-Grade Glioma Leads to Greater Extent of Resection With Better Outcomes: A Systematic Review. J Neurooncol (2022) 156(2):233–56. doi: 10.1007/s11060-021-03901-9
44. Kamp MA, Fischer I, Buhner J, Turowski B, Cornelius JF, Steiger HJ, et al. 5-ALA Fluorescence of Cerebral Metastases and its Impact for the Local-in-Brain Progression. Oncotarget (2016) 7(41):66776–89. doi: 10.18632/oncotarget.11488
45. Marhold F, Mercea PA, Scheichel F, Berghoff AS, Heicappell P, Kiesel B, et al. Detailed Analysis of 5-Aminolevulinic Acid Induced Fluorescence in Different Brain Metastases at Two Specialized Neurosurgical Centers: Experience in 157 Cases. J Neurosurg (2019) 133(4):1–12. doi: 10.3171/2019.6.JNS1997
46. Mercea PA, Mischkulnig M, Kiesel B, Wadiura LI, Roetzer T, Prihoda R, et al. Prognostic Value of 5-ALA Fluorescence, Tumor Cell Infiltration and Angiogenesis in the Peritumoral Brain Tissue of Brain Metastases. Cancers (Basel) (2021) 13(4):603. doi: 10.3390/cancers13040603
47. Stummer W, Suero Molina E. Fluorescence Imaging/Agents in Tumor Resection. Neurosurg Clin N Am (2017) 28(4):569–83. doi: 10.1016/j.nec.2017.05.009
48. Schupper AJ, Rao M, Mohammadi N, Baron R, Lee JYK, Acerbi F, et al. Fluorescence-Guided Surgery: A Review on Timing and Use in Brain Tumor Surgery. Front Neurol (2021) 12:682151. doi: 10.3389/fneur.2021.682151
49. Schebesch KM, Hoehne J, Hohenberger C, Proescholdt M, Riemenschneider MJ, Wendl C, et al. Fluorescein Sodium-Guided Resection of Cerebral Metastases-Experience With the First 30 Patients. Acta Neurochir (2015) 157(6):899–904. doi: 10.1007/s00701-015-2395-7
Keywords: brain metastasis, magnetic resonance imaging (MRI), neurosurgical resection, extent of resection, (GTR) gross total resection, (STR) subtotal resection
Citation: Rosenstock T, Pöser P, Wasilewski D, Bauknecht H-C, Grittner U, Picht T, Misch M, Onken JS and Vajkoczy P (2022) MRI-Based Risk Assessment for Incomplete Resection of Brain Metastases. Front. Oncol. 12:873175. doi: 10.3389/fonc.2022.873175
Received: 10 February 2022; Accepted: 07 April 2022;
Published: 16 May 2022.
Edited by:
Seunggu Jude Han, Natividad Medical Center, United StatesReviewed by:
Stephen Bowden, Oregon Health and Science University, United StatesMaleeha Ahmad, Stanford University, United States
Copyright © 2022 Rosenstock, Pöser, Wasilewski, Bauknecht, Grittner, Picht, Misch, Onken and Vajkoczy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tizian Rosenstock, dGl6aWFuLnJvc2Vuc3RvY2tAY2hhcml0ZS5kZQ==