
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 08 June 2022
Sec. Head and Neck Cancer
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.870319
This article is part of the Research Topic Next Generation Staging in Head and Neck Cancers View all 11 articles
 Sebastian Zschaeck1,2,3,4,5
Sebastian Zschaeck1,2,3,4,5 Julian Weingärtner1,2Elia Lombardo6
Julian Weingärtner1,2Elia Lombardo6 Sebastian Marschner6,7
Sebastian Marschner6,7 Marina Hajiyianni1Marcus Beck1
Marina Hajiyianni1Marcus Beck1 Daniel Zips1,8,9Yimin Li10
Daniel Zips1,8,9Yimin Li10 Qin Lin10Holger Amthauer11Esther G. C. Troost3,4,5,12,13,14,15Jörg van den Hoff16
Qin Lin10Holger Amthauer11Esther G. C. Troost3,4,5,12,13,14,15Jörg van den Hoff16 Volker Budach1Jörg Kotzerke4,5,17Konstantinos Ferentinos18Efstratios Karagiannis18
Volker Budach1Jörg Kotzerke4,5,17Konstantinos Ferentinos18Efstratios Karagiannis18 David Kaul1
David Kaul1 Vincent Gregoire19
Vincent Gregoire19 Adrien Holzgreve20
Adrien Holzgreve20 Nathalie L. Albert20Pavel Nikulin16
Nathalie L. Albert20Pavel Nikulin16 Michael Bachmann16
Michael Bachmann16 Klaus Kopka16
Klaus Kopka16 Mechthild Krause3,4,5,12,13,14,15Michael Baumann3,4,5,12,21Joanna Kazmierska22,23
Mechthild Krause3,4,5,12,13,14,15Michael Baumann3,4,5,12,21Joanna Kazmierska22,23 Paulina Cegla24Witold Cholewinski22,24Iosif Strouthos18Klaus Zöphel4,5,17,25Ewa Majchrzak26
Paulina Cegla24Witold Cholewinski22,24Iosif Strouthos18Klaus Zöphel4,5,17,25Ewa Majchrzak26 Guillaume Landry6
Guillaume Landry6 Claus Belka6,7
Claus Belka6,7 Carmen Stromberger1
Carmen Stromberger1 Frank Hofheinz16*
Frank Hofheinz16*Purpose: 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) is utilized for staging and treatment planning of head and neck squamous cell carcinomas (HNSCC). Some older publications on the prognostic relevance showed inconclusive results, most probably due to small study sizes. This study evaluates the prognostic and potentially predictive value of FDG-PET in a large multi-center analysis.
Methods: Original analysis of individual FDG-PET and patient data from 16 international centers (8 institutional datasets, 8 public repositories) with 1104 patients. All patients received curative intent radiotherapy/chemoradiation (CRT) and pre-treatment FDG-PET imaging. Primary tumors were semi-automatically delineated for calculation of SUVmax, SUVmean, metabolic tumor volume (MTV) and total lesion glycolysis (TLG). Cox regression analyses were performed for event-free survival (EFS), overall survival (OS), loco-regional control (LRC) and freedom from distant metastases (FFDM).
Results: FDG-PET parameters were associated with patient outcome in the whole cohort regarding clinical endpoints (EFS, OS, LRC, FFDM), in uni- and multivariate Cox regression analyses. Several previously published cut-off values were successfully validated. Subgroup analyses identified tumor- and human papillomavirus (HPV) specific parameters. In HPV positive oropharynx cancer (OPC) SUVmax was well suited to identify patients with excellent LRC for organ preservation. Patients with SUVmax of 14 or less were unlikely to develop loco-regional recurrence after definitive CRT. In contrast FDG PET parameters deliver only limited prognostic information in laryngeal cancer.
Conclusion: FDG-PET parameters bear considerable prognostic value in HNSCC and potential predictive value in subgroups of patients, especially regarding treatment de-intensification and organ-preservation. The potential predictive value needs further validation in appropriate control groups. Further research on advanced imaging approaches including radiomics or artificial intelligence methods should implement the identified cut-off values as benchmark routine imaging parameters.
In head and neck squamous cell carcinomas (HNSCC) beside computed tomography (CT), positron emission tomography (PET) with the radiotracer 18f-fluorodeoxyglucose (FDG) is frequently used for tumor staging and treatment planning in clinical routine (1). Various PET parameters have been investigated regarding their prognostic value in HNSCC. One requirement of imaging parameters is that these parameters bear independent prognostic value compared to established clinical parameters. In FDG-PET, metabolic tumor volume (MTV), maximum and mean standardized uptake value (SUVmax and SUVmean), and the derived parameter total lesion glycolysis TLG (defined as MTV × SUVmean) can be seen as standard parameters that can be easily evaluated in clinical routine. Currently, the prognostic impact of these parameters is not well defined, especially in biologically heterogeneous sub-groups of HNSCC. A meta-analysis of studies investigating the prognostic value of pre-therapeutic FDG-PET in patients treated with definitive chemoradiation (CRT) reported that only MTV has significant prognostic impact on patients´ outcome (2). However, outcome parameters were only available for a minority of patients. Especially concerning the important endpoint loco-regional control (LRC), only four out of 25 studies included sufficient information. Additionally, the included studies used different tumor segmentation methods, therefore MTV delineation can differ considerably and the MTV values cannot be directly compared between studies. These limitations hamper any valid conclusions regarding the prognostic value of FDG-PET in HNSCC treated with definitive CRT. The aim of this study was to perform a multicenter analysis of original FDG-PET data from HNSCC patients treated with definitive CRT. All images were centrally analyzed by the same observer with the same software and semi-automatic delineation methods. Results of a small subgroup of patients with nasopharyngeal cancer (NPC) have already been published, here we report a larger cohort with additional NPC patients and all other tumor locations (3).
Inclusion criteria for this study were: histologically confirmed HNSCC without evidence of distant metastases, definitive radiotherapy or CRT with curative intent, and availability of pre-treatment FDG-PET. We analyzed PET images and patient data from one Chinese and seven European centers plus additional images and patient data from the cancer imaging archive (4), in particular: Head-Neck-PET-CT, QIN-HEADNECK, HNSCC, TCGA-HNSC, Head-Neck-Radiomics-HN1 (5–12). TNM classification was bases on American Joint Committee on cancer staging manual version number seven.
Details on the imaging of the patients from public databases can be found in the original publications cited above. Patients from Berlin, Xiamen, Dresden, Brussels, Tuebingen, Limassol, Poznan and Munich received hybrid-imaging (usually PET-CT) with the following equipment: Gemini TF 16 (Philips Medical Systems, Cleveland, OH, USA), Discovery STE (General Electric Medical Systems, Milwaukee, WI, USA), Biograph 16 PET/CT scanner (Siemens Medical Solutions Inc., Knoxville, TN), Gemini TF PET-CT (Philips Medical Systems, Cleveland, OH, USA), Biograph mCT (Siemens Healthineers), Discovery IQ (General Electric Medical Systems, Milwaukee, WI, USA), Gemini TF TOF 16 (Philips Healthcare Inc., Andover, MA) and Discovery (General Electric Medical Systems, Milwaukee, WI, USA)/Biograph (Siemens Medical Solutions Inc., Knoxville, TN), respectively.
All patients received primary radiotherapy with curative intent. Radiotherapy was performed as three-dimensional, intensity modulated or volumetric modulated treatment. Prescribed radiation doses ranged between 66 and 77 Gray (Gy). In most cases radiotherapy was combined with simultaneous chemotherapy or cetuximab. 804 patients received concomitant systemic therapy. Most patients with individual data on chemotherapy received platinum-based CRT regimes (371 of 439 patients; 85%), 165 patients received radiotherapy only (15%) and 135 patients (12%) had no information available on concomitant therapy. Commonly only patients with early stage disease were treated by radiotherapy only, while CRT was prescribed in locally advanced stages.
The metabolically active part of the primary tumor was delineated in the PET data by a semi-automatic algorithm based on adaptive thresholding considering the local background (13, 14).
Manual delineation was only performed in case of low or diffuse tracer accumulation. In case of lacking tracer accumulation the voxel with highest activity within the primary tumor site (i.e. with the highest SUVmax uptake) was contoured as a single voxel for further analyses, this was the case in 30 patients (2.7%). This approach was chosen to avoid bias by excluding all patients without significant FDG uptake from the analyses. For the resulting regions of interest (ROIs), the metabolic active tumor volume (MTV), maximum and mean standardized uptake value (SUVmax and SUVmean), and the total lesion glycolysis (MTV × SUVmean, TLG) were computed. Delineation was performed by an experienced radiation oncologist (SZ) and verified by an experienced Nuclear Medicine physician (KZ). ROI definition and ROI analyses were performed using the software ROVER version 3.0.41 (ABX GmbH, Radeberg, Germany).
Survival analysis was performed with respect to event free survival (EFS), overall survival (OS), locoregional control (LRC), and freedom from distant metastases (FFDM). The association of endpoints with clinical and quantitative PET parameters was analyzed using univariate and multivariate Cox proportional hazard regression in which the PET parameters were included as metric parameters. Parameters were further analyzed in univariate Cox regression using binarized PET parameters. The cut-off values were calculated by minimizing the p-value in univariate Cox regression as described in (15). The optimal cut-off was determined separately for EFS, OS, LRC, and FFDM. Cut-off values leading to p<0.05 were tested for stability (i.e., sensibility of the prognostic value against variation of the cut-off value). In this test, the range of cut-off values still leading to a significant effect in univariate analysis was computed by successively decreasing/increasing the cut-off value (starting at the optimal value) and repeating univariate Cox regression. Probability of event occurrence was computed and rendered as Kaplan–Meier curves. Statistical significance was defined as a p-value of less than 0.05. Statistical analysis was performed with the R language and environment for statistical computing version 4.0.5 (16).
For validation of previously published cut-off values, all 25 studies included in the meta-analysis were searched for reported significant cut-off values, published endpoints, and tumor locations (2). Supplementary Table 1 summarizes these data (only analyses of the primary tumor parameters were considered).
1104 patients with individual patient and outcome data and original PET images for analysis were included in this study. Supplementary Table 2 summarizes available clinical data of all 16 cohorts. Median age of patients was 60 years and 79% of patients were male. The vast majority of patients presented locally advanced stages of HNSCC (87% > UICC stage II) and oropharynx (OPC) was the most frequent primary tumor location (51%). Detailed patient characteristics are reported in Supplementary Table 3. In the whole cohort, median MTV, TLG, SUVmax and SUVmean were 7.0 ml, 61.6 ml, 13.0 and 8.4, respectively. Details and distribution of the parameters are reported in Supplementary Table 4. There were significant differences of PET parameters depending on tumor location. Broadly speaking, tumors located within the oral cavity (OCC) had higher values and larynx carcinomas (LC) showed lower values of some parameters. Details on the distribution can be found in Supplementary Figure 1 and comparison between groups is shown in Supplementary Table 5. Since tumor location is a known prognostic factor in HNSCC, we checked for prognostic relevance of this parameter in this cohort (see Supplementary Figure 2) and added the information in uni- and multivariate cox regression analyses. When analyzing oncological outcome of the whole cohort, all PET parameters showed a significant association with all investigated clinical endpoints (EFS, OS, LRC and FFDM). Details are reported in Table 1. Note that not all parameters/endpoints were available for all patients. Patients with missing information were excluded in the respective analysis. The number of included patients is listed in column ‘N’ in Table 1. The results are more or less unchanged when patients with missing information are exclude completely (see Supplementary Table 6). Upon multivariate testing, MTV showed a robust association with EFS, OS and LRC, while SUVmax showed the highest association with FFDM. Details are reported in Table 2. Only those patients were included for which all information on all analyzed parameters/endpoints was available. The number of included patients is indicated at the top of the corresponding part of Table 2. Binarization and cutoff-stability testing of PET parameters revealed that MTV, TLG, and, in some cases, SUVmax are able to significantly discriminate between risk groups across a broad range of values (Supplementary Tables 7, 8). Several previously published cut-off values were successfully validated (Supplementary Table 9). Figures 1, 2 show Kaplan-Meier estimates for patients stratified according to PET parameters with the endpoints OS and LRC. Figures for EFS and FFDM are shown in Supplementary Figures 3, 4. Since tumor location and HPV status have a strong influence on the outcome of patients, PET parameters were optimized for each tumor subtype. Figures 3, 4 show Forest plots of the prognostic significance of PET parameters in different subgroups including primary tumor site for PET parameters MTV and SUVmax. MTV seems to bear the highest prognostic value especially in younger patients and in patients with NPC, which is partly correlated (average age of NPC patients in this cohort 52.4 years versus 61.1 years for non-NPC HNSCC, p < 0.001). Additionally, NPC did show a different behavior regarding FFDM compared to other locations (the only location with decreased risk of FFDM with increased MTV or SUVmax although not reaching statistical significance). A surprising finding was the very strong association of SUVmax with LRC in HPV-positive (HPV+) OPC. Figure 5 shows Kaplan-Meier estimates for HPV-positive OPC stratified according to the investigated PET parameters. The SUVmax cut-off of 14 was able to identify patients with excellent LRC after CRT/radiotherapy. While in general MTV seems to be an important risk factor regarding LRC, this does not seem to be the case in LC. Also other PET parameters did not show a convincing association in LC (Supplementary Figure 5).
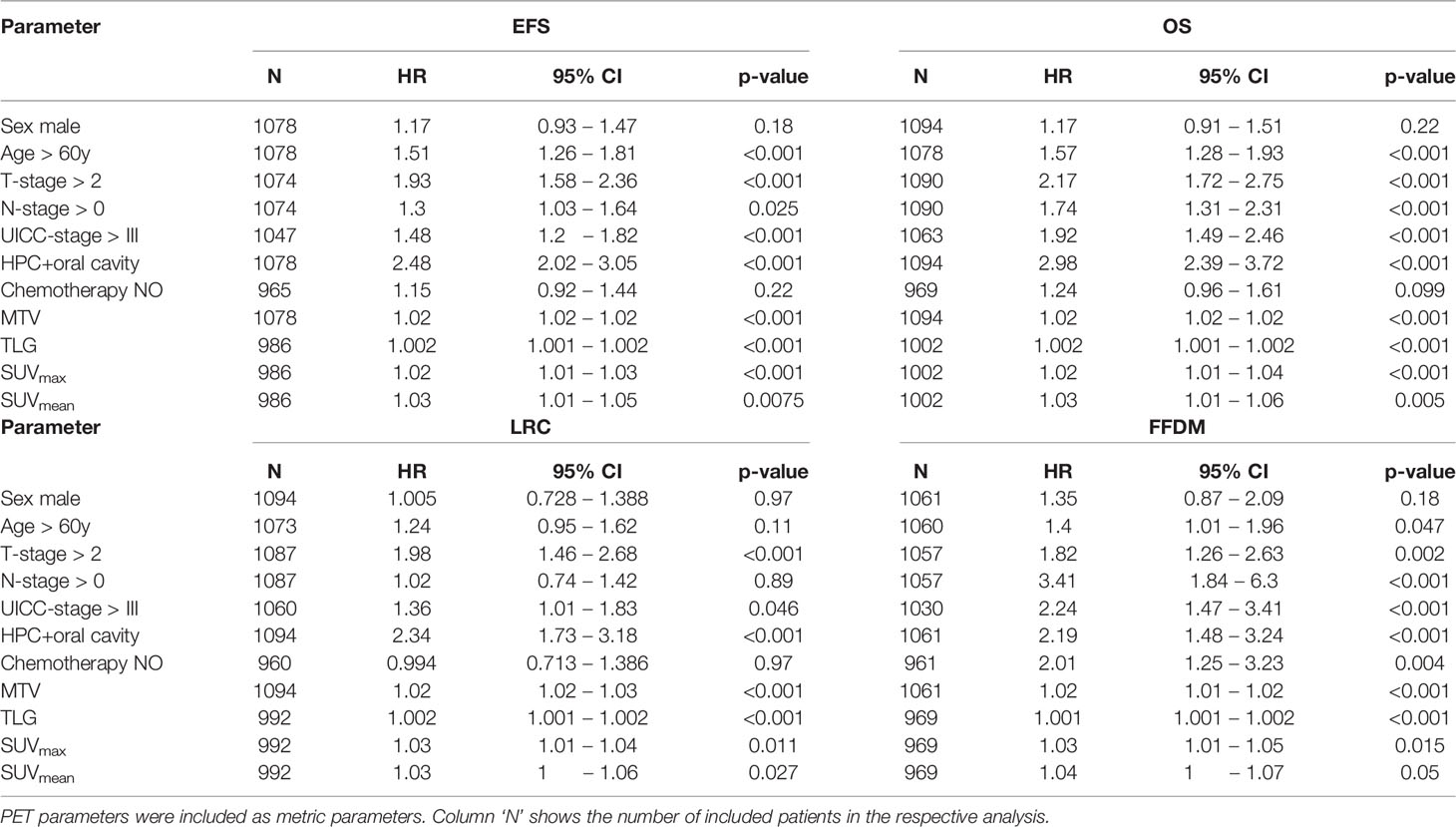
Table 1 Univariate cox regression analyses with respect to EFS, OS, LRC and FFDM.
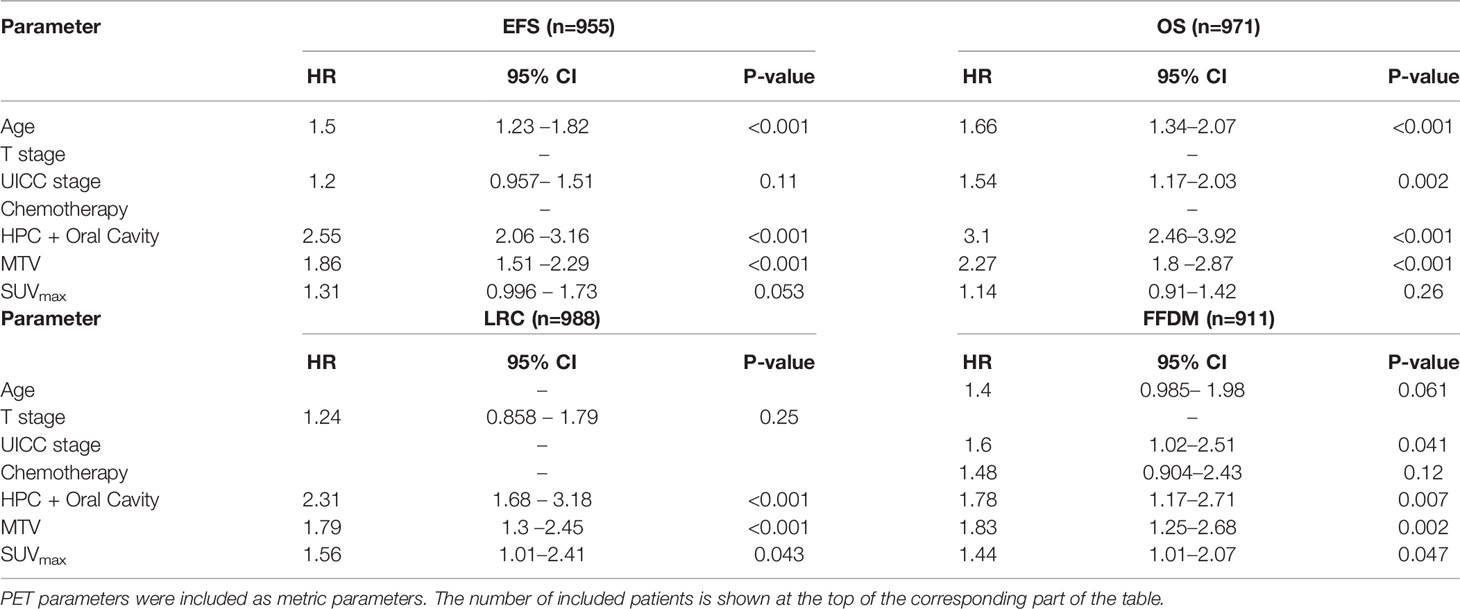
Table 2 Multivariate cox regression analyses with respect to EFS, OS, LRC and FFDM.
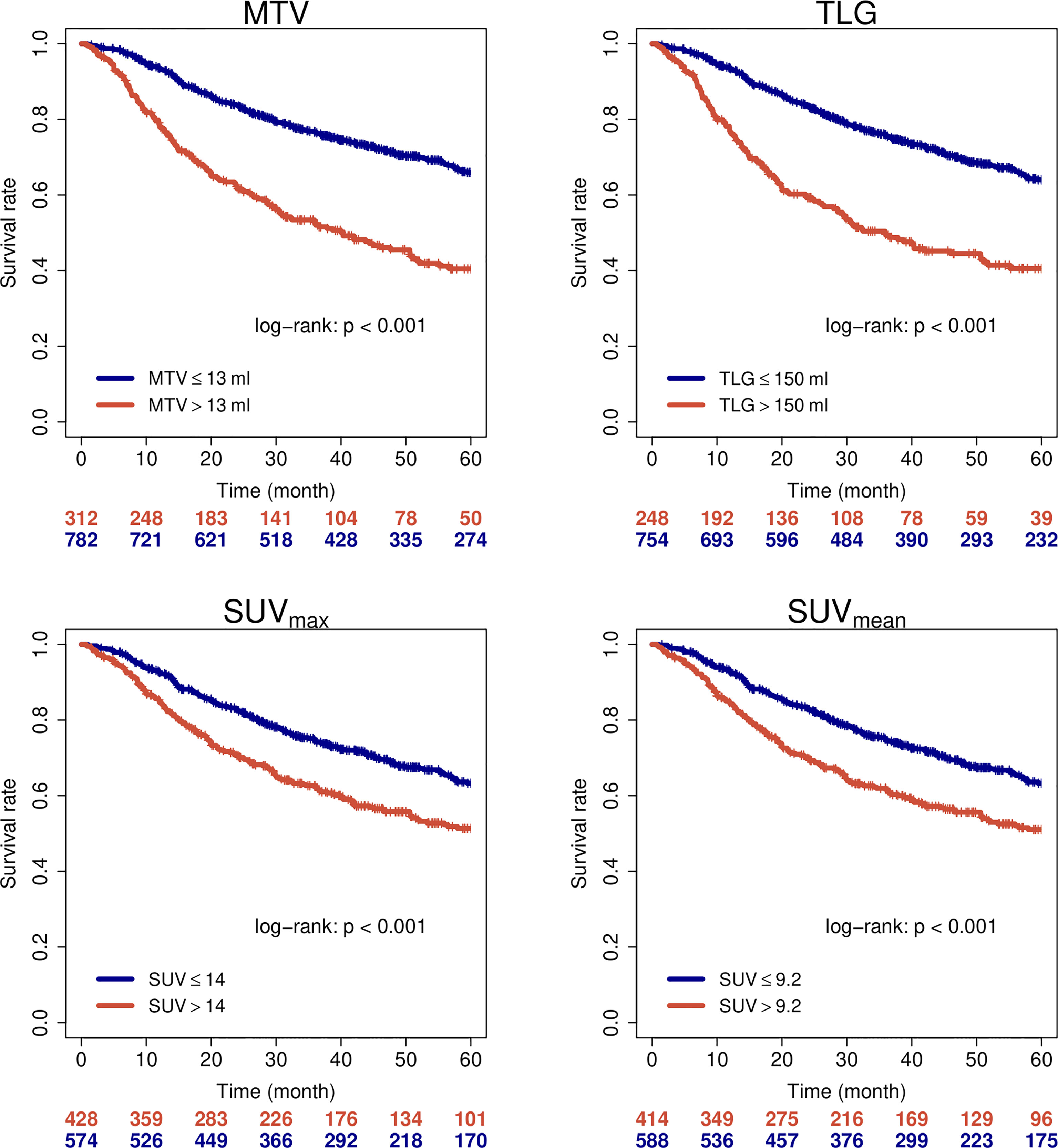
Figure 1 Overall survival of all patients when stratified by PET parameters.
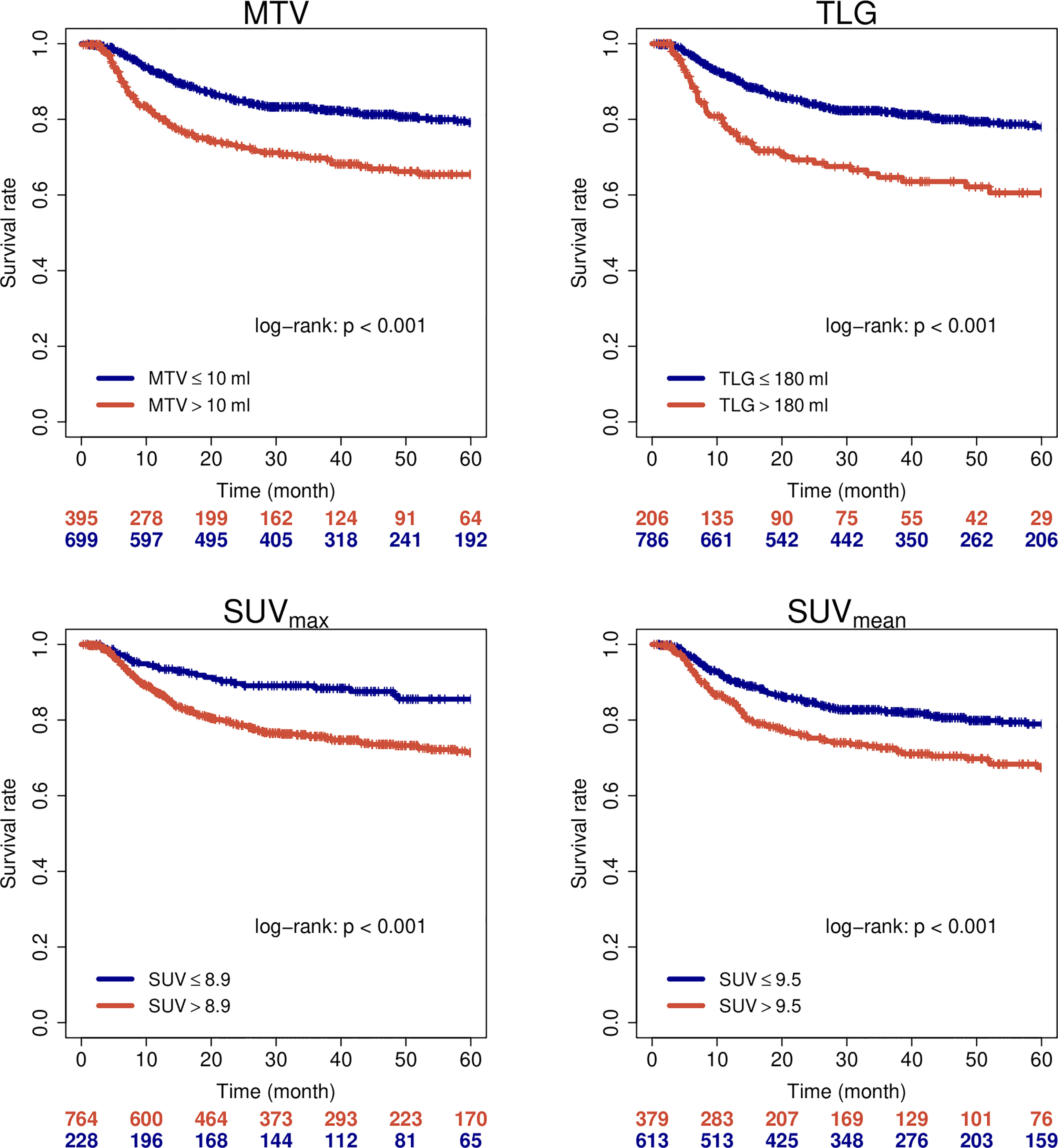
Figure 2 Loco-regional control of all patients when stratified by PET parameters.
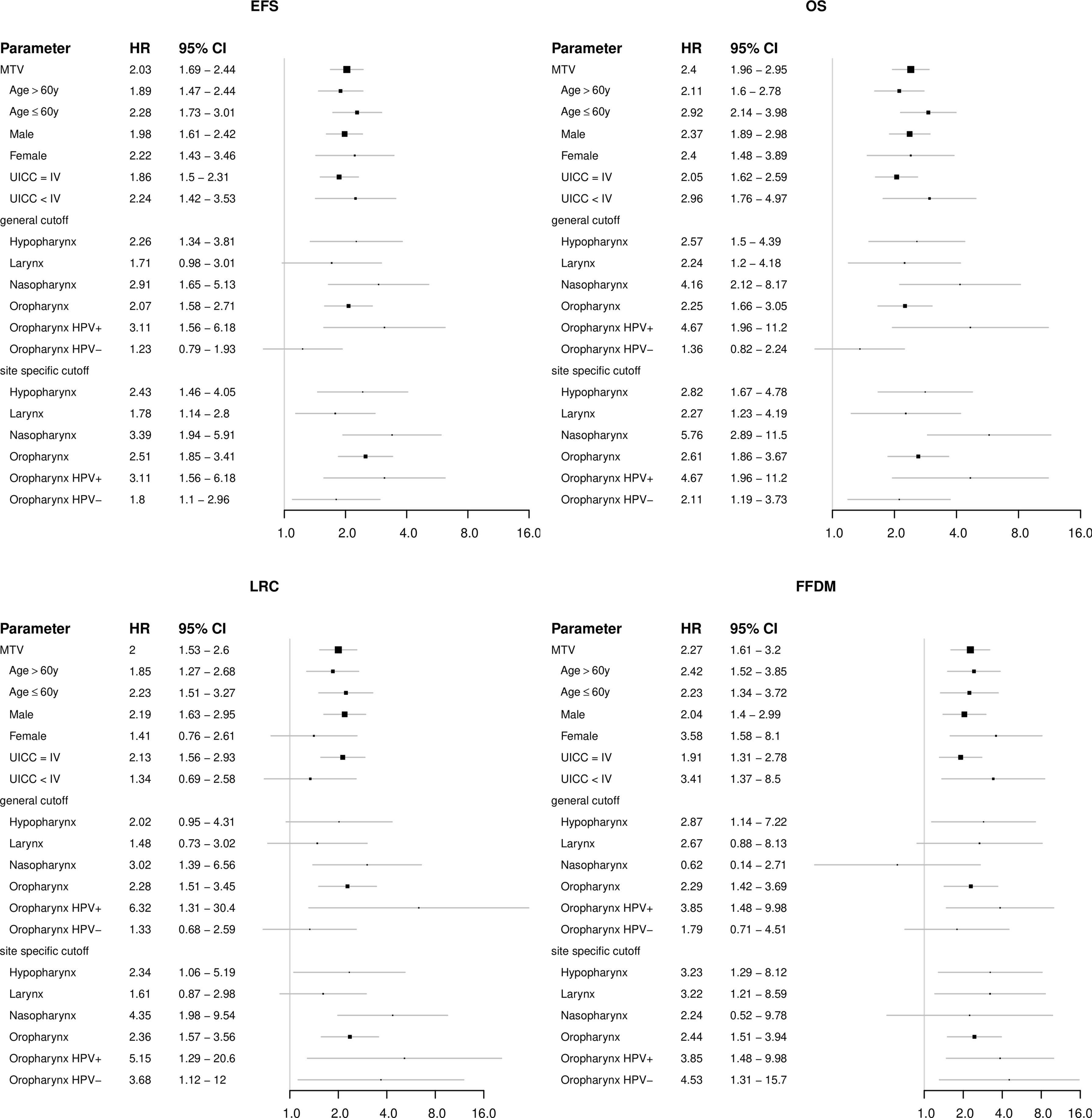
Figure 3 Forest plots showing the prognostic value of the FDG-PET parameter metabolic tumor volume (MTV) in subgroups of patients regarding the clinical endpoints EFS, OS, LRC and FFDM.
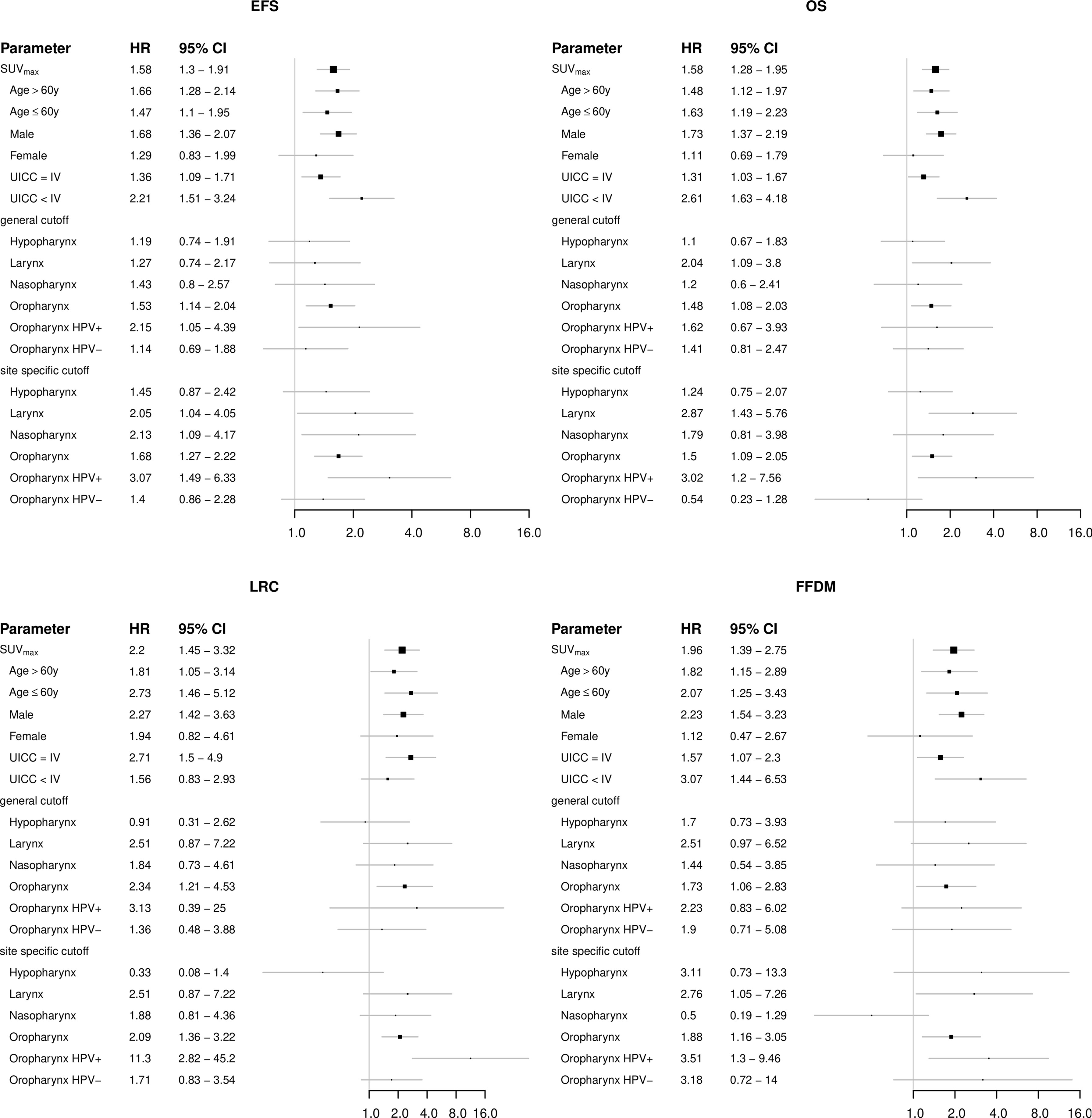
Figure 4 Forest plots showing the prognostic value of the FDG-PET parameter maximum standardized uptake value (SUVmax) in subgroups of patients regarding the clinical endpoints EFS, OS, LRC and FFDM.
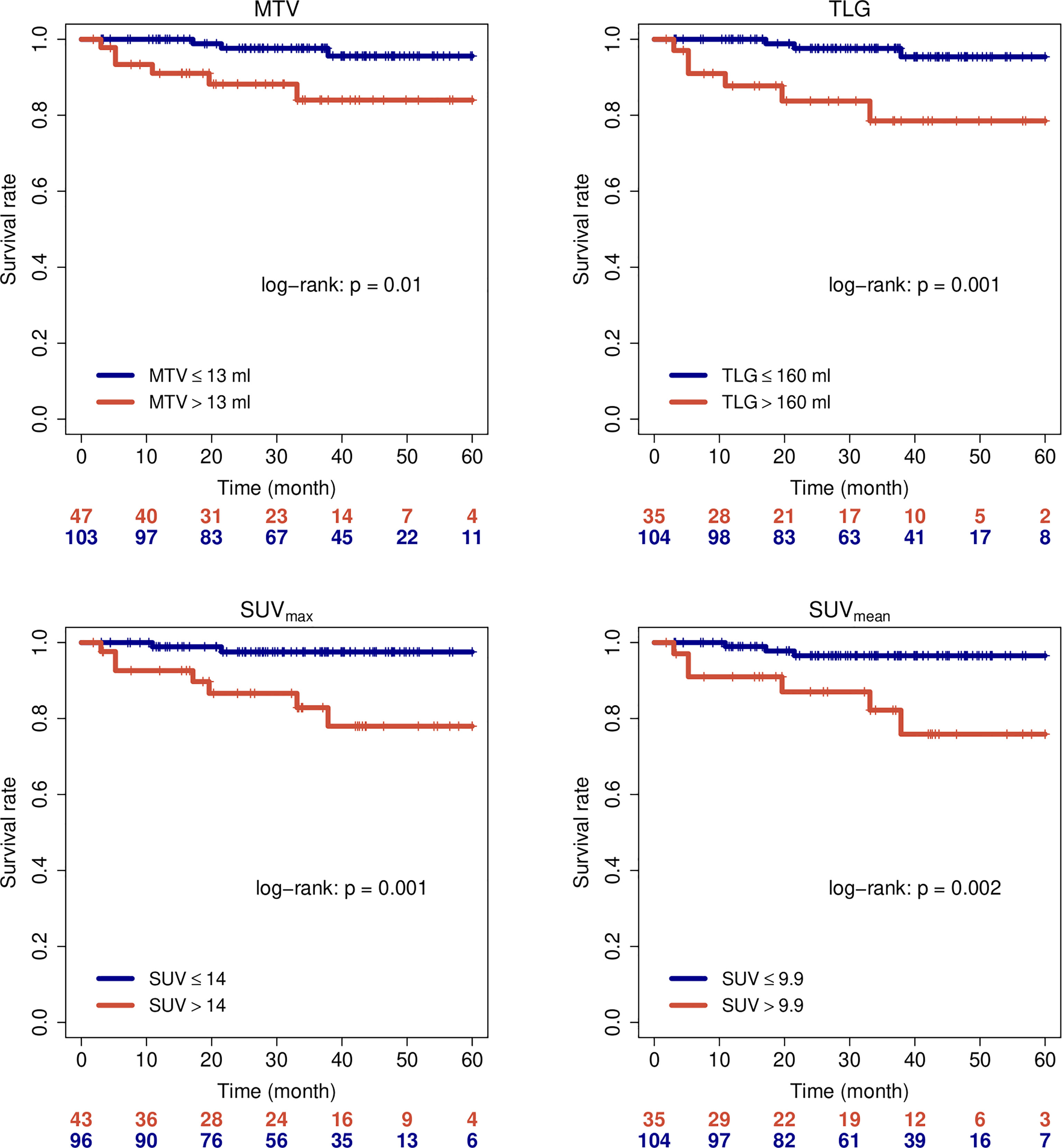
Figure 5 Loco-regional control of HPV-positive oropharyngeal carcinomas when stratified by PET parameters.
Based on a plethora of mostly retrospective single-center studies, FDG-PET parameters are considered significant prognostic and potentially predictive parameters for response to CRT in HNSCC. This is reflected by the use of high FDG uptake volumes for dose escalation in several trials (17–20). In a recent review article Clausen and colleagues argued that regarding its prognostic value FDG is beyond the exploratory phase; at the same time they found evidence for publication bias with potential overestimation of the prognostic effect size of FDG parameters in HNSCC (21). Their analysis, which was not based on individual patient data, included 1704 HNSCC patients from 20 studies with a median sample size of only 58 patients. Given the distinct biological features and prognosis of HNSCC subtypes, this implies that subgroup analyses are not useful in the majority of small sample size publications.
Here we report the, to our knowledge, largest individual patient and imaging based analyses of HNSCC with pre-treatment FDG-PET and primary CRT/radiotherapy. Our analyses confirm a moderate association of several PET parameters with clinical outcome of patients in the whole cohort. At the same time, considerable differences regarding primary tumor location and HPV status were found. This is an important observation for future aims to personalize radio-oncological treatment by the implementation of PET parameters. In early stage OPC, radiotherapy and transoral robotic surgery showed comparable quality of life and outcome, but with different toxicity profiles in a randomized phase-II study (22, 23). Although high-level evidence is lacking for other and more advanced HNSCC, CRT and primary surgery are often considered similar efficient primary treatment approaches. Since toxicity and late side effects are considerable in the head and neck region, biomarkers to individualize treatment are urgently needed for these patients.
LC and HPV positive OPC are probably two of the tumor locations with the strongest need for parameters to individualize treatment, i.e. schedule patients for primary surgery or CRT depending on the probability of LRC. Our analyses revealed that FDG-PET does not deliver convincing information in LC, however in HPV positive OPC, several PET parameters show a very high discriminatory ability. Even the most easily obtainable parameter SUVmax, assessed during every clinical routine PET scan, seems to be very well suited to select low-risk patients that could potentially be treated within dose de-escalation trials. To our opinion this is an unexpected finding especially in a multi-center analysis, since SUV parameters are known to be prone to several potential errors. They are uptake-time-dependent and time after injection differs considerably in routine care patients. Furthermore SUV is susceptible to scanner calibration errors and the correlation between systemic tracer distribution and body weight is only weak, adding additional variability in common SUV calculations. Especially in multicenter analyses, this can make quantitative comparison of SUV difficult and our group was able to show that the uptake time normalized ratio of tumor SUV and blood SUV (SUR) is superior to tumor SUV alone regarding correlation with glucose uptake of lesions, but also regarding outcome discrimination (24–27). However, determination of blood SUV requires a PET/CT scan of the thorax. Some of the included patients had missing corresponding CT scans or PET examination limited to the upper thorax and head and neck region. Therefore, calculation of SUR was not possible in the whole cohort, but is subject of ongoing research in a subgroup of patients with available imaging information. The strong prognostic value of SUVmax in this cohort of HPV positive OPC despite its methodological limitations, might be due to the relatively high cutoff value. Given the increasing incidence of HPV positive OPC in combination with the relatively good prognosis, further individually tailored treatment is an urgent medical need (28). Several phase-II studies reported promising outcome results with CRT dose de-escalation to 60 Gy (29, 30). Another phase-II study was able to show that normo-fractionated dose de-escalation down to 50 Gy is feasible after prior selection of patients with favorable biology using induction chemotherapy (31). However, current evidence does not suggest any benefit by induction chemotherapy for OPC patients (32). Therefore, other biomarkers, as our identified PET parameter, would be ideal candidates to guide future treatment de-escalation.
Our study has several limitations such as the retrospective nature of the data and partly missing information, especially in data from public repositories. Most obviously, this affects the HPV status of oropharyngeal carcinomas, which was not available for a relevant number of patients. Furthermore, the TNM staging classification was not according to the most current version number eight. There were substantial modifications from version seven to version eight, with emphasis on HPV positive oropharynx carcinomas (33). This is a major drawback when comparing the data with other current HNSCC data and should be considered when interpreting the data. Nonetheless, most of the basic parameters, including the important endpoints LRC and OS were available and the current analysis includes by far the largest dataset of FDG-PET from HNSCC patients. Therefore, our analysis can be regarded as reference benchmark for future research on the prognostic value of imaging parameters, i.e. the identified parameters should be considered when establishing novel radiomics and/or AI models for prognostication of HNSCC patients and novel signatures should outperform these parameters regarding patient stratification. This seems to be highly important as a recent analysis has shown that one of the most popular radiomics signatures, that has been independently validated, is highly correlated with tumor volume (34). Our analysis does not only identify promising future applications for standard parameters, but also shows for which tumor subtypes and outcome parameters further research on optimal stratification and treatment personalization is warranted. For example, standard PET parameters of primary tumors have not shown convincing results regarding the prediction of distant metastases. Analysis of affected lymph nodes and/or more sophisticated image analyses by convolutional neural networks have shown promising results and should probably be further developed to address this important issue (35–37). The same holds true for laryngeal carcinomas, for which some early radiomic analyses reported encouraging results (38, 39).
Standard FDG-PET parameters bear significant prognostic value in HNSCC treated with radiotherapy/CRT but moderate effect size regarding LRC and FFDM in the entire cohort. Subgroup specific analyses revealed SUVmax as a promising parameter to select HPV-positive OPC with excellent outcome after CRT/radiotherapy.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethikkomission der Charité, Charité Universitätsmedizin Berlin, Berlin, Germany. The patients/participants provided their written informed consent to participate in this study.
Study conception and design: SZ and FH; Drafting of manuscript: SZ and FH; Image processing and analysis: SZ, JW, EL, SM, MH, YL, JKo, KF, EK, VG, AH, PN, JKa, PC, KZ, and FH; Study Investigators: SZ, DZ, QL, HA, ET, JvdH, VB, JKo, VG, NA, MK, MBau, WC, KZ, GL, CB, CS, and FH; Interpretation of data: all authors; Final approval of manuscript: all authors.
This work was partly supported by the Berliner Krebsgesellschaft (ZSF201720) and by the German Federal Ministry of Education and Research (BMBF contract 03ZIK42/OncoRay). The funders had no role in the design of the study; the collection, analysis, and interpretation of the data; the writing of the manuscript; and the decision to submit the manuscript for publication.
In the past 5 years, MBau received funding for his research projects and for educational grants to the University of Dresden by Bayer AG (2016–2018), Merck KGaA (2014-open) and Medipan GmbH (2014–2018). He is on the supervisory board of HI-STEM gGmbH (Heidelberg) for the German Cancer Research Center (DKFZ, Heidelberg) and also member of the supervisory body of the Charité University Hospital, Berlin. As former chair of OncoRay (Dresden) and present CEO and Scientific Chair of the German Cancer Research Center (DKFZ, Heidelberg), he has been or is responsible for collaborations with a multitude of companies and institutions, worldwide. In this capacity, he has discussed potential projects and signed contracts for research funding and/or collaborations with industry and academia for his institute(s) and staff, including but not limited to pharmaceutical companies such as Bayer, Boehringer Ingelheim, Bosch, Roche and other companies such as Siemens, IBA, Varian, Elekta, Bruker, etc. In this role, he was/is also responsible for the commercial technology transfer activities of his institute(s), including the creation of start-ups and licensing. This includes the DKFZ-PSMA617 related patent portfolio [WO2015055318 (A1), ANTIGEN (PSMA)] and similar IP portfolios. MBau confirms that, to the best of his knowledge, none of the above funding sources were involved in the preparation of this paper. In the past 5 years, MK received funding for her research projects by IBA (2016), Merck KGaA (2014-2018 for preclinical study; 2018-2020 for clinical study), Medipan GmbH (2014–2018). She is involved in an ongoing publicly funded (German Federal Ministry of Education and Research) project with the companies Medipan, Attomol GmbH, GA Generic Assays GmbH, Gesellschaft für medizinische und wissenschaftliche genetische Analysen, Lipotype GmbH and PolyAn GmbH (2019–2021). For the present manuscript, MK confirms that none of the above funding sources were involved in the preparation of this paper.
HA declares research grants, travel grants, and lecture fees from Sirtex Medical Europe; HA confirms that none of the above funding sources were involved in the preparation of this paper.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer FH declared a past co-authorship with one of the authors ET to the handling Editor.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.870319/full#supplementary-material
1. Cook GJR, Azad G, Owczarczyk K, Siddique M, Goh V. Challenges and Promises of PET Radiomics. Int J Radiat Oncol Biol Phys (2018) 102:1083–9. doi: 10.1016/j.ijrobp.2017.12.268
2. Bonomo P, Merlotti A, Olmetto E, Bianchi A, Desideri I, Bacigalupo A, et al. What Is the Prognostic Impact of FDG PET in Locally Advanced Head and Neck Squamous Cell Carcinoma Treated With Concomitant Chemo-Radiotherapy? A Systematic Review and Meta-Analysis. Eur J Nucl Med Mol Imaging (2018) 45:2122–38. doi: 10.1007/s00259-018-4065-5
3. Zschaeck S, Li Y, Lin Q, Beck M, Amthauer H, Bauersachs L, et al. Prognostic Value of Baseline [18F]-Fluorodeoxyglucose Positron Emission Tomography Parameters MTV, TLG and Asphericity in an International Multicenter Cohort of Nasopharyngeal Carcinoma Patients. PloS One (2020) 15:e0236841. doi: 10.1371/journal.pone.0236841
4. Clark K, Vendt B, Smith K, Freymann J, Kirby J, Koppel P, et al. The Cancer Imaging Archive (TCIA): Maintaining and Operating a Public Information Repository. J Digit Imaging (2013) 26:1045–57. doi: 10.1007/s10278-013-9622-7
5. Vallières M, Kay-Rivest E, Perrin L, Liem X, Furstoss C, Khaouam N, et al. Data From Head-Neck-PET-Ct. (2017). doi: 10.7937/K9/TCIA.2017.8OJE5Q00.
6. Beichel RR, Ulrich EJ, Bauer C, Wahle A, Brown B, Chang T, et al. Data From QIN-HEADNECK. (2015). doi: 10.7937/K9/TCIA.2015.K0F5CGLI.
7. Grossberg AJ, Mohamed ASR, Elhalawani H, Bennett WC, Smith KE, Nolan TS, et al. Imaging and Clinical Data Archive for Head and Neck Squamous Cell Carcinoma Patients Treated With Radiotherapy. Sci Data (2018) 5:180173. doi: 10.1038/sdata.2018.173
8. Vallières M, Kay-Rivest E, Perrin LJ, Liem X, Furstoss C, Aerts HJWL, et al. Radiomics Strategies for Risk Assessment of Tumour Failure in Head-and-Neck Cancer. Sci Rep (2017) 7:10117. doi: 10.1038/s41598-017-10371-5
9. Fedorov A, Clunie D, Ulrich E, Bauer C, Wahle A, Brown B, et al. DICOM for Quantitative Imaging Biomarker Development: A Standards Based Approach to Sharing Clinical Data and Structured PET/CT Analysis Results in Head and Neck Cancer Research. PeerJ (2016) 4:e2057. doi: 10.7717/peerj.2057
10. Grossberg A, Elhalawani H, Mohamed A, Mulder S, Williams B, White A, et al. HNSCC. Cancer Imaging Archive doi: 10.7937/k9/tcia.2020.a8sh-7363
12. Zuley ML, Jarosz R, Kirk S, Lee Y, Colen R, Garcia K, et al. Radiology Data From The Cancer Genome Atlas Head-Neck Squamous Cell Carcinoma [TCGA-HNSC] Collection. (2016). doi: 10.7937/K9/TCIA.2016.LXKQ47MS.
13. Hofheinz F, Pötzsch C, Oehme L, Beuthien-Baumann B, Steinbach J, Kotzerke J, et al. Automatic Volume Delineation in Oncological PET. Evaluation of a Dedicated Software Tool and Comparison With Manual Delineation in Clinical Data Sets. Nuklearmedizin (2012) 51:9–16. doi: 10.3413/Nukmed-0419-11-07
14. Hofheinz F, Langner J, Petr J, Beuthien-Baumann B, Steinbach J, Kotzerke J, et al. An Automatic Method for Accurate Volume Delineation of Heterogeneous Tumors in PET. Med Phys (2013) 40:082503. doi: 10.1118/1.4812892
15. Bütof R, Hofheinz F, Zöphel K, Stadelmann T, Schmollack J, Jentsch C, et al. Prognostic Value of Pretherapeutic Tumor-To-Blood Standardized Uptake Ratio in Patients With Esophageal Carcinoma. J Nucl Med (2015) 56:1150–6. doi: 10.2967/jnumed.115.155309
16. R Core Team. R: A Language and Environment for Statistical Computing. In: R Foundation for Statistical Computing. Vienna, Austria (2001).
17. Gouw ZAR, La Fontaine MD, Vogel WV, van de Kamer JB, Sonke J-J, Al-Mamgani A. Single-Center Prospective Trial Investigating the Feasibility of Serial FDG-PET Guided Adaptive Radiation Therapy for Head and Neck Cancer. Int J Radiat Oncol Biol Phys (2020) 108:960–8. doi: 10.1016/j.ijrobp.2020.04.030
18. Berwouts D, Madani I, Duprez F, Olteanu AL, Vercauteren T, Boterberg T, et al. Long-Term Outcome of 18 F-Fluorodeoxyglucose-Positron Emission Tomography-Guided Dose Painting for Head and Neck Cancer: Matched Case-Control Study. Head Neck (2017) 39:2264–75. doi: 10.1002/hed.24892
19. Duprez F, De Neve W, De Gersem W, Coghe M, Madani I. Adaptive Dose Painting by Numbers for Head-and-Neck Cancer. Int J Radiat Oncol Biol Phys (2011) 80:1045–55. doi: 10.1016/j.ijrobp.2010.03.028
20. Rasmussen JH, Håkansson K, Vogelius IR, Aznar MC, Fischer BM, Friborg J, et al. Phase I Trial of 18F-Fludeoxyglucose Based Radiation Dose Painting With Concomitant Cisplatin in Head and Neck Cancer. Radiother Oncol (2016) 120:76–80. doi: 10.1016/j.radonc.2016.03.005
21. Clausen MM, Vogelius IR, Kjær A, Bentzen SM. Multiple Testing, Cut-Point Optimization, and Signs of Publication Bias in Prognostic FDG-PET Imaging Studies of Head and Neck and Lung Cancer: A Review and Meta-Analysis. Diagnostics (Basel) (2020) 10. doi: 10.3390/diagnostics10121030
22. Nichols AC, Theurer J, Prisman E, Read N, Berthelet E, Tran E, et al. Radiotherapy Versus Transoral Robotic Surgery and Neck Dissection for Oropharyngeal Squamous Cell Carcinoma (ORATOR): An Open-Label, Phase 2, Randomised Trial. Lancet Oncol (2019) 20:1349–59. doi: 10.1016/S1470-2045(19)30410-3
23. Nichols AC, Theurer J, Prisman E, Read N, Berthelet E, Tran E, et al. Randomized Trial of Radiotherapy Versus Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma: Long-Term Results of the ORATOR Trial. J Clin Oncol (2022) 40:866–75. doi: 10.1200/JCO.21.01961
24. van den Hoff J, Oehme L, Schramm G, Maus J, Lougovski A, Petr J, et al. The PET-Derived Tumor-to-Blood Standard Uptake Ratio (SUR) Is Superior to Tumor SUV as a Surrogate Parameter of the Metabolic Rate of FDG. EJNMMI Res (2013) 3:77. doi: 10.1186/2191-219X-3-77
25. Bütof R, Hofheinz F, Zöphel K, Schmollack J, Jentsch C, Zschaeck S, et al. Prognostic Value of SUR in Patients With Trimodality Treatment of Locally Advanced Esophageal Carcinoma. J Nucl Med (2018) 56:1150–6. doi: 10.2967/jnumed.117.207670
26. Hofheinz F, van den HJ, IG S, Lougovski A, Ego K, Amthauer H, et al. Comparative Evaluation of SUV, Tumor-to-Blood Standard Uptake Ratio (SUR), and Dual Time Point Measurements for Assessment of the Metabolic Uptake Rate in FDG PET. EJNMMI Res (2016) 6:53. doi: 10.1186/s13550-016-0208-5
27. Hofheinz F, Li Y, Steffen IG, Lin Q, Lili C, Hua W, et al. Confirmation of the Prognostic Value of Pretherapeutic Tumor SUR and MTV in Patients With Esophageal Squamous Cell Carcinoma. Eur J Nucl Med Mol Imaging (2019) 46:1485–94. doi: 10.1007/s00259-019-04307-6
28. Mahal BA, Catalano PJ, Haddad RI, Hanna GJ, Kass JI, Schoenfeld JD, et al. Incidence and Demographic Burden of HPV-Associated Oropharyngeal Head and Neck Cancers in the United States. Cancer Epidemiol Biomarkers Prev (2019) 28:1660–7. doi: 10.1158/1055-9965.EPI-19-0038
29. Chera BS, Amdur RJ, Green R, Shen C, Gupta G, Tan X, et al. Phase II Trial of De-Intensified Chemoradiotherapy for Human Papillomavirus-Associated Oropharyngeal Squamous Cell Carcinoma. J Clin Oncol (2019) 37:2661–9. doi: 10.1200/JCO.19.01007
30. Yom SS, Torres-Saavedra P, Caudell JJ, Waldron JN, Gillison ML, Xia P, et al. Reduced-Dose Radiation Therapy for HPV-Associated Oropharyngeal Carcinoma (NRG Oncology Hn002). J Clin Oncol (2021) 39:956–65. doi: 10.1200/JCO.20.03128
31. Seiwert TY, Foster CC, Blair EA, Karrison TG, Agrawal N, Melotek JM, et al. OPTIMA: A Phase II Dose and Volume De-Escalation Trial for Human Papillomavirus-Positive Oropharyngeal Cancer. Ann Oncol (2019) 30:297–302. doi: 10.1093/annonc/mdy522
32. Blanchard P, Baujat B, Holostenco V, Bourredjem A, Baey C, Bourhis J, et al. MACH-CH Collaborative Group. Meta-Analysis of Chemotherapy in Head and Neck Cancer (MACH-NC): A Comprehensive Analysis by Tumour Site. Radiother Oncol (2011) 100:33–40. doi: 10.1016/j.radonc.2011.05.036
33. Lydiatt WM, Patel SG, O’Sullivan B, Brandwein MS, Ridge JA, Migliacci JC, et al. Head and Neck Cancers-Major Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual. CA Cancer J Clin (2017) 67:122–37. doi: 10.3322/caac.21389
34. Welch ML, McIntosh C, Haibe-Kains B, Milosevic MF, Wee L, Dekker A, et al. Vulnerabilities of Radiomic Signature Development: The Need for Safeguards. Radiother Oncol (2019) 130:2–9. doi: 10.1016/j.radonc.2018.10.027
35. Cacicedo J, Fernandez I, Del Hoyo O, Navarro A, Gomez-Iturriaga A, Pijoan JI, et al. Prognostic Value of Maximum Standardized Uptake Value Measured by Pretreatment 18F-FDG PET/CT in Locally Advanced Head and Neck Squamous Cell Carcinoma. Clin Transl Oncol (2017) 19:1337–49. doi: 10.1007/s12094-017-1674-6
36. Lombardo E, Kurz C, Marschner S, Avanzo M, Gagliardi V, Fanetti G, et al. Distant Metastasis Time to Event Analysis With CNNs in Independent Head and Neck Cancer Cohorts. Sci Rep (2021) 11:6418. doi: 10.1038/s41598-021-85671-y
37. Cheng N-M, Yao J, Cai J, Ye X, Zhao S, Zhao K, et al. Deep Learning for Fully Automated Prediction of Overall Survival in Patients With Oropharyngeal Cancer Using FDG-PET Imaging. Clin Cancer Res (2021) 27:3948–59. doi: 10.1158/1078-0432.CCR-20-4935
38. Chen L, Wang H, Zeng H, Zhang Y, Ma X. Evaluation of CT-Based Radiomics Signature and Nomogram as Prognostic Markers in Patients With Laryngeal Squamous Cell Carcinoma. Cancer Imaging (2020) 20:28. doi: 10.1186/s40644-020-00310-5
39. Agarwal JP, Sinha S, Goda JS, Joshi K, Mhatre R, Kannan S, et al. Tumor Radiomic Features Complement Clinico-Radiological Factors in Predicting Long-Term Local Control and Laryngectomy Free Survival in Locally Advanced Laryngo-Pharyngeal Cancers. Br J Radiol (2020) 93:20190857. doi: 10.1259/bjr.20190857
Keywords: head and neck squamous cell carcinoma (HNSCC), fluorodeoxyglucose positron emission tomography (FDG PET), radiotherapy, metabolic tumor volume (MTV), standardized uptake value (SUV)
Citation: Zschaeck S, Weingärtner J, Lombardo E, Marschner S, Hajiyianni M, Beck M, Zips D, Li Y, Lin Q, Amthauer H, Troost EGC, van den Hoff J, Budach V, Kotzerke J, Ferentinos K, Karagiannis E, Kaul D, Gregoire V, Holzgreve A, Albert NL, Nikulin P, Bachmann M, Kopka K, Krause M, Baumann M, Kazmierska J, Cegla P, Cholewinski W, Strouthos I, Zöphel K, Majchrzak E, Landry G, Belka C, Stromberger C and Hofheinz F (2022) 18F-Fluorodeoxyglucose Positron Emission Tomography of Head and Neck Cancer: Location and HPV Specific Parameters for Potential Treatment Individualization. Front. Oncol. 12:870319. doi: 10.3389/fonc.2022.870319
Received: 06 February 2022; Accepted: 29 April 2022;
Published: 08 June 2022.
Edited by:
Shao Hui Huang, University Health Network, CanadaReviewed by:
Patrick Veit Haibach, University Health Network (UHN), CanadaCopyright © 2022 Zschaeck, Weingärtner, Lombardo, Marschner, Hajiyianni, Beck, Zips, Li, Lin, Amthauer, Troost, van den Hoff, Budach, Kotzerke, Ferentinos, Karagiannis, Kaul, Gregoire, Holzgreve, Albert, Nikulin, Bachmann, Kopka, Krause, Baumann, Kazmierska, Cegla, Cholewinski, Strouthos, Zöphel, Majchrzak, Landry, Belka, Stromberger and Hofheinz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frank Hofheinz, Zi5ob2ZoZWluekBoemRyLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.