
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 13 April 2022
Sec. Radiation Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.863848
This article is part of the Research TopicStereotactic Body Radiotherapy for Prostate CancerView all 15 articles
 Wei Liu1
Wei Liu1 Andrew Loblaw2
Andrew Loblaw2 David Laidley3
David Laidley3 Hatim Fakir4
Hatim Fakir4 Lucas Mendez1
Lucas Mendez1 Melanie Davidson2Zahra Kassam5
Melanie Davidson2Zahra Kassam5 Ting-Yim Lee6Aaron Ward6
Ting-Yim Lee6Aaron Ward6 Jonathan Thiessen6Jane Bayani7John Conyngham8Laura Bailey9Joseph D. Andrews9
Jonathan Thiessen6Jane Bayani7John Conyngham8Laura Bailey9Joseph D. Andrews9 Glenn Bauman1*
Glenn Bauman1*Advances in imaging have changed prostate radiotherapy through improved biochemical control from focal boost and improved detection of recurrence. These advances are reviewed in the context of prostate stereotactic body radiation therapy (SBRT) and the ARGOS/CLIMBER trial protocol. ARGOS/CLIMBER will evaluate 1) the safety and feasibility of SBRT with focal boost guided by multiparametric MRI (mpMRI) and 18F-PSMA-1007 PET and 2) imaging and laboratory biomarkers for response to SBRT. To date, response to prostate SBRT is most commonly evaluated using the Phoenix Criteria for biochemical failure. The drawbacks of this approach include lack of lesion identification, a high false-positive rate, and delay in identifying treatment failure. Patients in ARGOS/CLIMBER will receive dynamic 18F-PSMA-1007 PET and mpMRI prior to SBRT for treatment planning and at 6 and 24 months after SBRT to assess response. Imaging findings will be correlated with prostate-specific antigen (PSA) and biopsy results, with the goal of early, non-invasive, and accurate identification of treatment failure.
External beam radiation therapy (EBRT) is a primary treatment modality for men with intermediate and high-risk prostate cancer. Conventional treatments are typically with fractions of 1.8–2.0 Gray (Gy)/day over a treatment duration of up to 8 weeks (70–80 Gy in 35–40 fractions). Biochemical failure (BF), as defined by the Phoenix Criteria (prostate-specific antigen [PSA] rise by 2 ng/ml or more above nadir PSA) (1), occurs in up to 35% of treated patients treated with standard EBRT by 10 years (2). Recent advances in image guidance and dose delivery have enabled new forms of EBRT, including stereotactic body radiation therapy (SBRT) (3) and focal intra-prostatic boost (4–6).
After radiation therapy, local recurrence occurs primarily at the sites of macroscopic dominant intraprostatic lesions (DILs) (7, 8). Comprehensive planning studies suggest that focal EBRT boost to DILs is dosimetrically feasible for a wide range of dose fractionations without exceeding normal tissue tolerances (9, 10). Most studies have used multiparametric MRI (mpMRI) to identify DILs in focal prostate radiation therapy (Table 1). The randomized controlled clinical trial FLAME showed that focal boost to DILs using standard fractionations improves the 5-year biochemical progression-free survival (bPFS) with acceptable toxicity (5, 12). DELINEATE, a single-center prospective phase II multicohort study, also confirmed the feasibility of DIL boost with standard and moderate fractionations with rectal and genitourinary (GU) toxicity comparable to contemporary series without intraprostatic boost (11). The safety and feasibility of DIL boost in extreme hypofractionation (five fractions) were validated in the Phase II 5STAR and Hypo-Flame trials (4, 6). These trials showed that toxicity for DIL boost with extreme hypofractionation compares to toxicity without boost and was lower than toxicity in the FLAME trial. Even with focal boost, however, intra-prostatic failure may be seen as a site of failure (13). Early detection of local recurrence after radiotherapy enables deployment of potentially curative salvage therapies (14, 15).
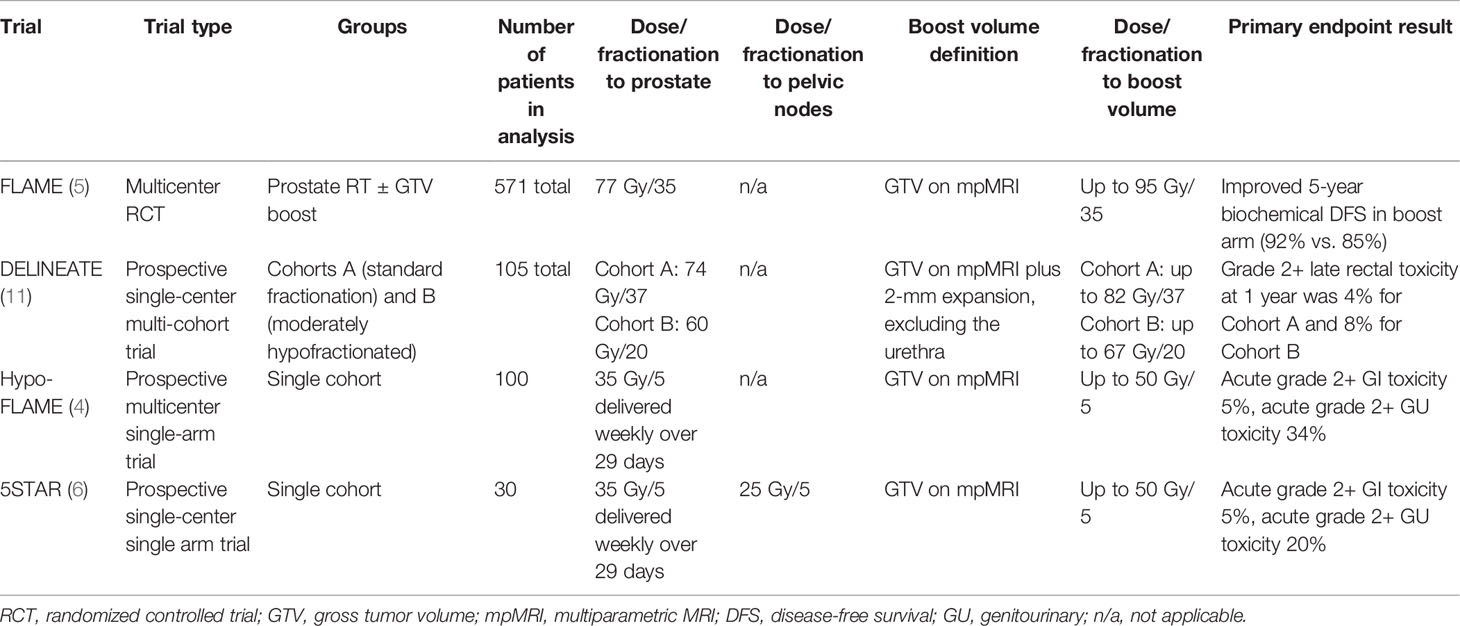
Table 1 Selected prospective evidence for focal intra-prostatic boost.
Multiple studies have evaluated the boost of DILs using mpMRI for target delineation. However, mpMRI can miss some intraprostatic lesions or significantly underestimate lesion size (16). Prostate-specific membrane antigen (PSMA)-targeted positron emission tomography (PET) complements mpMRI and improves the detection and characterization of intraprostatic cancer and nodal disease in the primary setting (17–20). As such, it may improve oncologic outcomes through more accurate delineation of focal boost volumes (17, 18, 21). Additionally, PSMA PET provides better distant staging and can identify extra-prostatic extension, especially among men with higher risk disease (22). 68Ga-PSMA-11 is the most widely studied and 18F-DCFPyL is the next most commonly studied PSMA radioligand (23, 24). The advantages of fluorinated compounds like 18F-DCFPyL compared to gallium-based compounds like 68Ga-PSMA-11 include improved spatial resolution and a longer half-life, which allows for centralized production and transportation to remote facilities (25). 18F-PSMA-1007 is a third PSMA radioligand with a growing body of evidence. The primary advantage of 18F-PSMA-1007 compared to 68Ga-PSMA-11 and 18F-DCFPyL is its reduced urinary clearance, which allows for improved assessment of the pelvic region, making it especially suitable for the evaluation of DILs in the base of the prostate (26). A potential disadvantage of 18F-PSMA-1007 is a higher number of false-positive bone marrow lesions noted in some series (26).
In recent years, the clinical use of 18F-labeled PSMA-targeted compounds has significantly increased. 18F-DCFPyL and 18F-PSMA-1007 are the most clinically established 18F-labeled radiotracers for PSMA-targeted PET imaging (25). For instance, 18F-DCFPyL demonstrated high sensitivity for the detection of clinically significant intraprostatic tumors and biochemically recurrent prostate cancer, in addition to a high potential to measure total tumor burden for treatment planning (27, 28). We have demonstrated through a prospective trial of the preoperative imaging that 18F-DCFPyL-PET/MRI could identify DILs as verified by whole-mount pathology images (29). The performance of delineation of DILs for focal treatment could be optimized by using a 67% threshold of the maximum intra-prostatic standard uptake value (SUV) with an 8-mm margin to maximize coverage of histologically defined lesions (30).
The alternate PSMA-targeting agent, 18F-PSMA-1007, offers additional advantages related to the delineation of intraprostatic lesions. While 18F-DCFPyL is excreted by renal clearance into the urinary bladder, 18F-PSMA-1007 is excreted by the hepatobiliary system and therefore causes no or minimal bladder activity. A comparison of 18F-PSMA-1007 PET/CT with radical prostatectomy histology and mpMRI (n = 10) showed a slightly better performance than mpMRI with fewer false negatives and fewer false positives (31). A clinical comparison of [18F]DCFPyL and 18F-PSMA-1007 (n = 12) found excellent image quality and identical clinical findings. Both radiotracers were equivalent for imaging of local and metastatic prostate cancer. However, the non-urinary excretion of 18F-PSMA-1007 offers advantages regarding the delineation of local recurrences and lymph node metastases (32). Prive et al. evaluated 18F-PSMA-1007 and mpMRI and compared their histopathology for the primary staging of prostate cancer in 53 patients diagnosed with intermediate and high-risk prostate cancer. PSMA improved the detection of seminal vesicle invasion, while MRI offered a better resolution in evaluating extracapsular extension (33). The study suggested that dual imaging may improve the staging of prostate cancer. A 20% SUVmax threshold using 18F-PSMA-1007 was recently demonstrated to offer the best combination of sensitivity and specificity in delineating DILs, and volumes so defined accounted for approximately 21% of the total prostate volume on average (18).
Another application for advanced imaging in SBRT prostate treatment is in response assessment. To date, evaluation of success following SBRT is most commonly by biochemical means, and successful SBRT is associated with low PSA nadirs comparable to those noted with brachytherapy (34). Biochemical control is a suboptimal method to assess recurrence in patients due to a lack of spatial information, potential false positives, and delayed identification of failure based on rising PSA. First, the lack of lesion identification using PSA-based criteria alone prevents successful local or metastasis-directed salvage without the use of imaging. Given the potential toxicity of local salvage, identification of isolated local recurrence is critical (14). Secondly, the Phoenix Criteria has a false-positive rate in patients who receive SBRT. In a multi-institutional pooled analysis of over 2,000 patients who received prostate SBRT, the Phoenix Criteria was associated with a false-positive rate of 30% (35). Finally, the Phoenix Criteria occurs late. Patients who have local failure may not reach the Phoenix Criteria for years and may lose the opportunity for successful local salvage. A retrospective study showed that up to 38% of patients who received SBRT to doses of 32.5 Gy or higher in 5 fractions had a positive prostate biopsy 2 years after SBRT (36). However, just 12.5% of these patients had reached the Phoenix Criteria at the time of biopsy. Even in patients with a PSA of less than 1 ng/ml prior to biopsy, up to 25% of patients had a positive biopsy (36). Most patients with a positive 2-year biopsy would reach BF at 5 years (57% vs. 7% as compared to those with a negative biopsy), even after 35% of patients with a positive 2-year biopsy received salvage therapies. In another retrospective study, 63 patients, mostly with high-risk prostate cancer (40/63, 64%), received PSMA-targeted PET/CT for rising PSA that did not meet the Phoenix Criteria after primary conventional or moderately hypofractionated EBRT (37). Median rise above nadir PSA prior to PET was 1.2 ng/ml, and median PSA was 1.3 ng/ml. Recurrence was detected in 84% of patients (53/63). While 21/63 patients (33%) had local recurrence only, 14/63 (22%) had nodal recurrence without distant metastases, and 18/63 (18%) had distant metastases. Given the efficacy and toxicity of curative-intent local salvage treatments, improved and early identification of isolated local recurrence is needed (14, 15).
Identification of local recurrence after EBRT has been explored with timed biopsy or mpMRI after radiotherapy (38). Prostate biopsy at 2 years posttreatment has been associated with clinical endpoints such as subsequent BF and distant metastases (36, 39). However, drawbacks of biopsy include unreliable results at earlier timepoints and potential morbidity (39). “Metabolic clearance” as defined by serial MRI with spectroscopy has been associated with durable biochemical control in retrospective series of men treated with conventional external beam radiotherapy (40–43). Recently, standardized mpMRI reporting for the locally recurrent disease has been proposed but has not yet been validated in larger prospective series (44). Additionally, there is a lack of prospective studies validating posttreatment mpMRI as a predictive biomarker in larger populations and men treated with SBRT.
PSMA-targeted PET/CT in addition to mpMRI improves detection of local recurrence after EBRT (45). However, while criteria for the response have been broadly defined (46), the significance of PSMA response and correlation with clinical endpoints are not known (47). As such, longitudinal monitoring of PSMA PET/CT changes post-radiotherapy, including changes in SUVmax and other PSMA PET based metrics, should be investigated as potential non-invasive biomarkers of treatment response after SBRT to the prostate. Integration of earlier PET-based response assessment, compared to triggered restaging at the time of BF, may provide an opportunity for earlier targeted salvage, but a lack of prospective longitudinal series of men so monitored is a gap in the current evidence base (23). Indeed, reports of false-positive PET scans in previously treated patients underscore the importance of systematically characterizing the normal patterns of PSMA PET/CT changes after SBRT and their correlation with clinical endpoints (48, 49).
Beyond identifying local recurrence, determining the presence and extent of extra-prostatic recurrence has historically been challenging to determine due to the poor sensitivity of CT and bone scans. PET-based imaging potentially addresses this gap (23). A number of PET tracers have been developed for the detection of recurrent prostate cancer, including 18F-NaF, 18F-FACBC (fluciclovine), 18F-choline, and 11C-choline (50). More recently, PSMA-targeted PET has demonstrated improved detection rates as compared to previous modalities and is recommended for restaging recurrent disease (23, 24, 50, 51). Specifically, for patients with BF after primary radiotherapy, a prospective trial showed that compared to conventional imaging, PSMA-targeted PET/CT detected extra-prostatic recurrence in twice as many patients (39% vs. 19%) (52, 53). Furthermore, in a network meta-analysis of intra-individual imaging studies of different radiotracers, PSMA-based tracers in general, and 18F-PSMA-1007 specifically, were found to have superior detection rates at any site as compared to other traces, including 18F-FACBC, 18F-choline, and 11C-choline (54). However, the strength of these findings was tempered by the relatively small number of 18F-1007 patients evaluated directly. While PSMA-targeted PET/CT has increased detection rates in recurrent prostate cancer, a drawback is the risk of false-positive findings. In a prospective trial that evaluated the positive predictive value of PSMA-targeted PET/CT in patients with recurrent prostate cancer, the per-region false-positive rate based on a clinical endpoint was 8% (55).
We plan to evaluate the safety of SBRT with PSMA PET/MRI-guided focal boost in a prospective early phase trial, “PSMA MRI Guided prOstate SBRT(ARGOS).” As noted, while the advanced imaging techniques described show promise for the characterization of primary or recurrent prostate cancer, no study has prospectively and longitudinally evaluated them after primary radiotherapy to characterize expected changes in response to treatment and to non-invasively identify early treatment failure. All patients in ARGOS will enter the translational component of the study Comprehensive, Longitudinal Evaluation of Imaging Biomarkers Post Radiotherapy (CLIMBER). We will use advanced imaging analysis techniques to evaluate longitudinal changes in a comprehensive battery of anatomic and functional prostate imaging panels using 18F-PSMA 1007 and mpMRI acquired prior to and after SBRT. 18F-PSMA-1007 is chosen given its favorable pharmacokinetics profile with primarily gastrointestinal elimination, reducing tracer accumulation in the bladder and allowing better visualization of prostate and pelvic lymph nodes. The knowledge obtained from ARGOS/CLIMBER will improve the understanding of imaging changes post-prostate SBRT and will have increasing clinical importance with increasing use of these techniques. The ARGOS/CLIMBER protocol as outlined below is due to open in early 2022, with a plan for accrual of 50 men over 3 years and with follow-up of up to 5 years for clinical endpoints.
This study is (NCT05269550) a prospective single-arm trial enrolling men with National Comprehensive Cancer Network (NCCN) unfavorable intermediate-fiducial risk, high-risk, or very-high-risk prostate cancer. The study schema is provided in Figure 1. All men will have PSMA-targeted PET (using the PSMA-targeting ligand 18F-PSMA-1007) and mpMRI including T2-weighted (T2W), diffusion-weighted imaging (DWI)/apparent diffusion coefficient (ADC), and dynamic contrast-enhanced (DCE) sequences. Delineation of intra-prostatic foci of cancer (using 20% SUVmax and suspicious mpMRI appearance) and any involved regional lymph nodes (based on MI-ES score of 2 or greater or suspicious mpMRI appearance suspicious for cancer) will be performed (16, 18). Tumor delineation will be performed by fusing the PSMA PET and mpMRI with planning CT simulation images. Fiducial marker implantation for treatment guidance will be mandatory, but the use of other organs at risk protection strategies (i.e., SpaceOAR and GU-Lok) will be allowed but not mandatory. Patients will be treated with image-guided SBRT using the fiducial markers for inter- and intra-fraction motion management. The prostate will receive 35 Gy/5 fractions, and the proximal or entire seminal vesicle will receive 25 Gy/5 fractions (Table 2). Dose escalation to imaging-defined targets will be accomplished through a simultaneous boost technique (targeted maximum dose of 50 Gy/5 fractions to imaging-defined prostatic lesion and 35 Gy/5 fractions to imaging-defined involved nodes; see Figure 2). Maintaining dose to organs at risk will take precedence over boost dose targets (Table 3). Patients with high-risk disease or calculated nodal involvement risk of more than 15% will receive 25 Gy/5 fractions delivered to the regional lymph nodes synchronously with the prostate treatment.
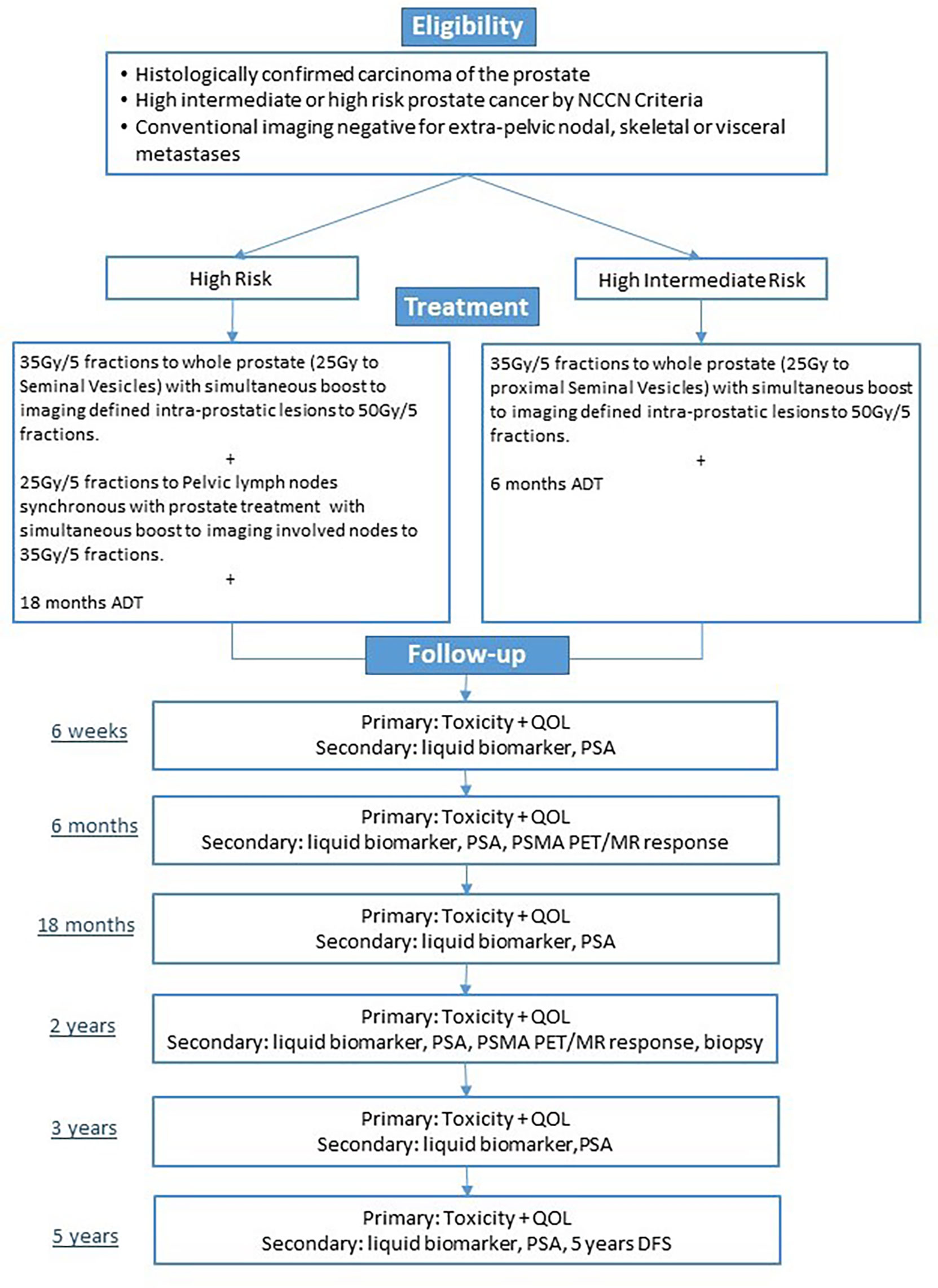
Figure 1 Study schema.
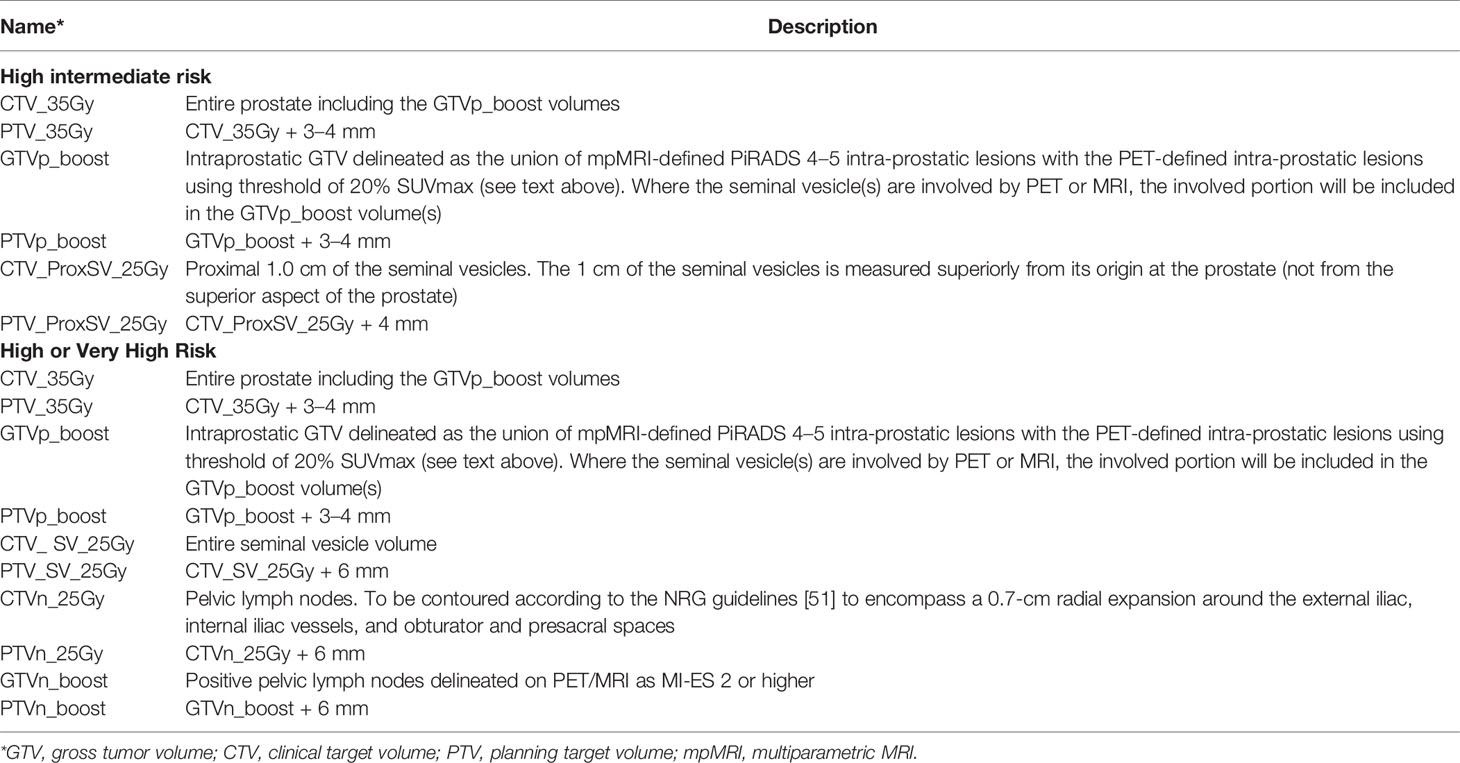
Table 2 Target structures nomenclature and descriptions.

Figure 2 Example of focal dose escalation.
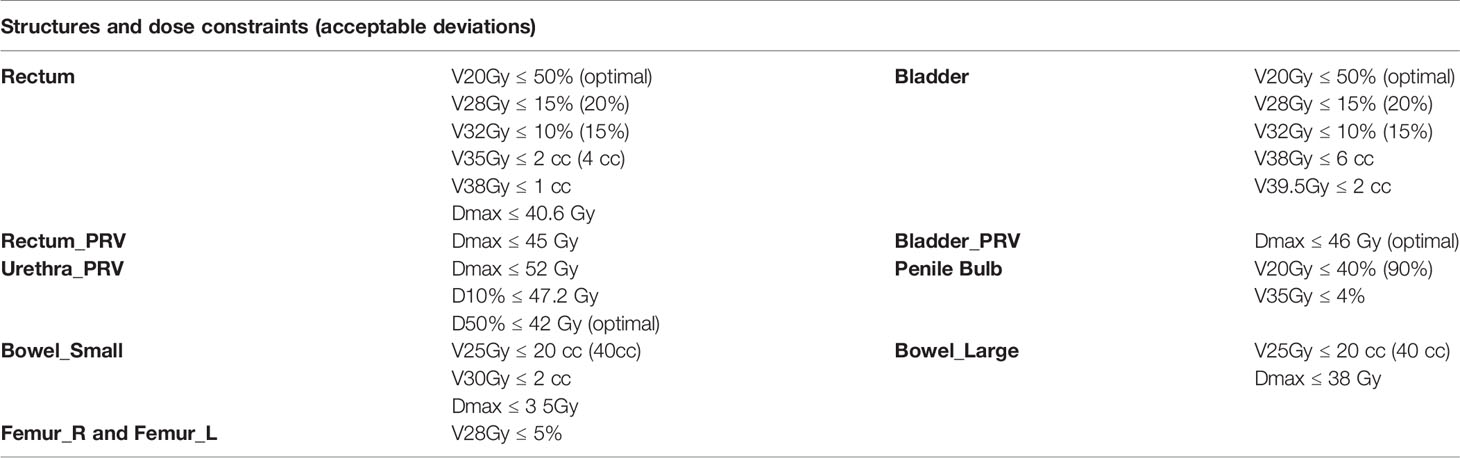
Table 3 Dose constraints.
The primary endpoints of the trial will be 6-week and 6-month gastrointestinal (GI) and GU toxicity using the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE v5.0). While other prospective trials have confirmed the safety of an mpMRI-defined intra-prostatic boost with external beam radiotherapy (4, 6), the proposed boost volume in ARGOS/CLIMBER will be based on mpMRI and PSMA PET-targeted PET (17), and thus there is a need to demonstrate the safety of such a multi-modality defined boost volume. Secondary endpoints include Quality of life measured by the Expanded Prostate Cancer Index Composite (EPIC-26) questionnaires and 5-year disease-free survival (DFS) as a composite of BF, patient death, or development of clinical metastases or institution of salvage ADT.
All grade 3 or higher toxicity will be reported to the principal investigator. An independent data and safety monitoring board (IDSMB) will perform a formal interim analysis for safety and toxicity when half of the patients have been accrued or after 1 year, whichever comes first. The study will be discontinued if the projected rate of grade 3 or higher urinary or bowel toxicity exceeds 30%. IDSMB will meet at least annually to review trial data.
Unique to the ARGOS/CLIMBER protocol is the integration of longitudinal imaging with PSMA-directed PET and mpMRI pretreatment and posttreatment. Serial PSMA PET/MR images will be collected at baseline, 6 months, and 2 years to characterize the imaging response of prostate cancer to treatment and potentially identify imaging biomarkers (including pharmacokinetics, radiomics, and quantitative PET and mpMRI metrics) that predict for 5-year DFS (Table 4). Additionally, baseline collection of diagnostic tissue biopsy samples and serial collection of blood and urine over multiple time points (baseline, 6 months, 1 year, and 2 years post-SBRT) will be performed for correlative biologic biomarker analyses with imaging changes, DFS, and toxicity posttreatment. Analysis of prostate biopsy at baseline and 2 years will allow for correlation of histopathology with PSMA PET/MR images. We will investigate whether a negative posttreatment PSMA PET/MRI is correlated with a negative 2-year posttreatment biopsy and long-term disease control (36, 39). We also plan to examine novel clinical prognostic biomarkers (i.e., absolute percentage of Gleason Pattern 4 on biopsy and 4-year PSA response rate) and their correlation with imaging findings and 5-year DFS.
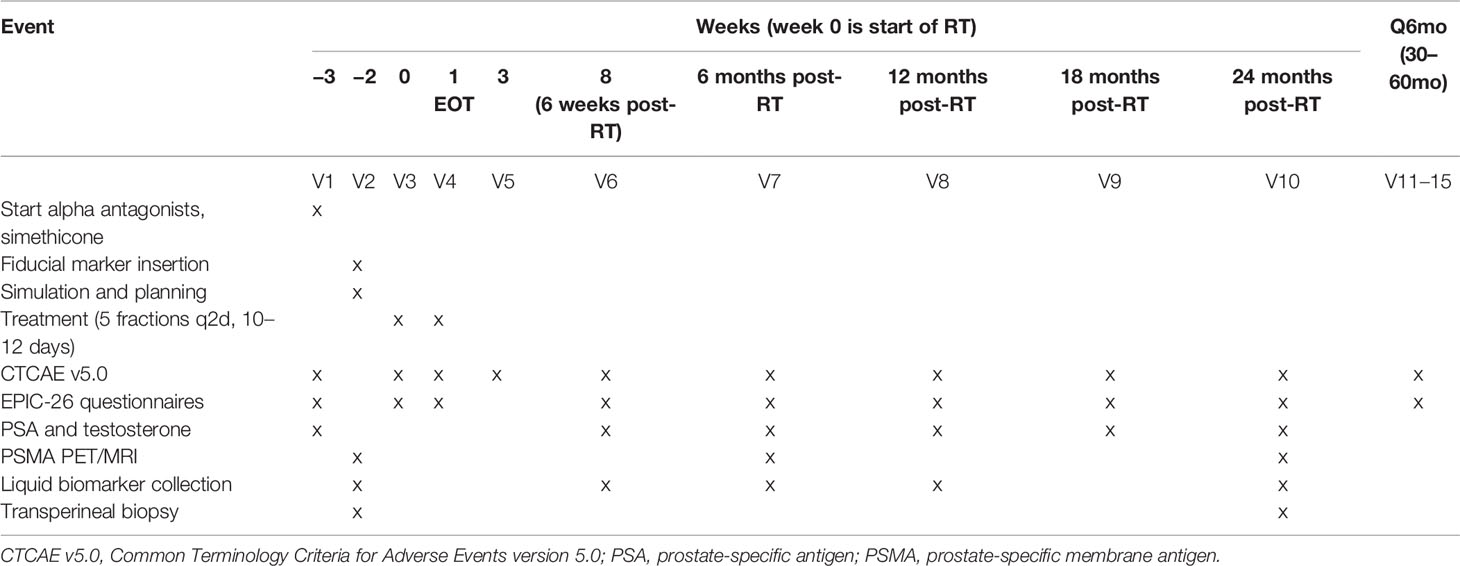
Table 4 Schedule of events.
Integrated PSMA PET/MRI is preferred with the goal of achieving co-registered PSMA PET and MR images with high spatial fidelity for planning and assessing response to treatment. PSMA PET/CT plus mpMRI are also allowed within the protocol if there is an unavailability of a PET/MRI scanner. We have previously demonstrated the value of early dynamic PET imaging in the identification of intra-prostatic lesions and will incorporate both dynamic and delayed PET imaging (56).
The evening before each PSMA PET examination, patients will be asked to take 30 ml of milk of magnesia, an over-the-counter laxative, which will be provided. Patients should be NPO overnight prior to the exam (~12 h). The bladder should be comfortably full and the rectum as empty as possible prior to image acquisition.
For dynamic PET imaging, the participants will be injected with 3–4 MBq/kg (up to a maximum 400 MBq) of 18F-PSMA-1007. Dynamic PET acquisitions will start immediately prior to 18F-PSMA 1007 injection and will be acquired simultaneously with the cross-sectional pelvic MR images (for PET/MRI) or CT images (for PET/CT). Dynamic PET acquisition will cover the whole prostate up to the iliac crest. An image-derived arterial time–activity curve required for kinetic analysis of dynamic PET data will be acquired from an internal iliac artery to generate parametric maps. Starting at the injection of 18F-PSMA-1007 as a bolus into an antecubital vein, the dynamic PET scan will be acquired over 22 min with seven framing intervals: 10, 20, 40, 60, and 180 s. Early time standardized uptake (SUVearly) in g/ml will be measured as the average of the last four dynamic PET volumes (10–22 min post-injection). The acquired dynamic volumes will be analyzed to generate parametric maps of the whole prostate, including influx rate constant (K1), efflux rate constant (k2), binding rate constant (k3), dissociation rate constant (k4), net uptake rate constant from plasma (Ki), and distribution volume (DV) maps by deconvolving the arterial time–activity curve from tissue time–activity curve using a flow-modified two-tissue compartment (F2TC) model. After dynamic pelvic PET, participants will be allowed to get up and take a break/empty their bladder prior to the acquisition of late uptake PSMA-1007 PET images (60–120 min post-injection). For PET/CT, the PET images will be acquired with corresponding axial CT images obtained (for anatomic correlation and attenuation correction).
For PET/MRI, a whole-body MRI scout scan (to plan the study) and B0 homogenization using gradient enhancement (HUGE) acquisition (to correct for truncation of arms) will be acquired first. In both acquisitions, the table moves continuously for approximately 1 min as it scans the subject from head to thigh. Whole-body PET/MRI is acquired in multiple bed positions. For men of average height, 5 overlapping table positions will be used, with taller subjects requiring an additional table position. At each table position, a 5-min PET acquisition will be acquired along with simultaneous MRI consisting of MRI-based attenuation correction, coronal T2-weighted fast spin-echo with Short-TI Inversion Recovery (STIR) sequence during flat breathing, and axial Half-Fourier Acquisition Single-shot Turbo spin-Echo (HASTE) single-shot T2-weighted sequence. For thoracic and abdominal table positions, the HASTE MRI will be captured over 4 breath-holds of 14 s. If unable to do so, these can be done with flat breathing only.
For men imaged with PET/MRI, the pelvic mpMRI will be acquired after whole-body PET/MRI on the PET/MRI scanner. For men imaged with PET/CT, mpMRI will be acquired as a separate study on a 3T magnetic resonance scanner. The bladder should be comfortably full and the rectum as empty as possible prior to the mpMRI scanning. For mpMRI scout scans, sagittal 2D T2-weighted, coronal 2D T2-weighted MRI, axial 3D T2-weighted, and 2D axial diffusion-weighted EPI will be acquired. Prior to a 3D DCE T1-weighted MRI, a radiologist or designate will administer an intravenous injection of GADOVIST® 1.0 (Gadobutrol) with the MEDRAD Injection System (0.1 mmol/kg). Following DCE-MRI, whole-body late gadolinium-enhanced MRI will be acquired with T1-weighted volumetric interpolated breath-hold examination (VIBE) with fat saturation and breath-hold in thoracic and abdominal table positions.
This will be a single-phase pilot study of 50 patients with a primary endpoint of GI and GU toxicity as measured by CTCAE v5.0.
Unacceptable toxicity will be defined as acute (6 weeks) or intermediate (6 months) grade >3 GI or GU toxicity. The proposed treatment will be deemed too toxic if >30% of patients have unacceptable toxicity. This study tests the hypothesis that acute toxicity is <30% (alpha = 0.05, power = 81%, one-sided, H0: p = .30, HA: p <.30), with an assumed true proportion in this study of 15%. These calculations were done based on a Z test (normal approximation). We will test this assumption with the exact test approach if we do not meet our target accrual of 50 men or the proportion of Grade 3 toxicity is significantly less than 15% (conditions where normal approximation is not met).
Given that the proPSMA study demonstrated that 16% of men with high-risk prostate cancer had extra-prostatic disease beyond regional nodal metastases at initial staging and the fact our population will be a mix of high-intermediate and high-risk men, we will plan to enroll a total of 55 men (22). Those men with extra-prostatic spread beyond regional pelvic lymph nodes on their pretreatment PSMA PET imaging will be treated off protocol at the attending physician’s discretion.
Descriptive statistics and diagrams will be used to characterize changes in Quality of Life metrics as measured by the EPIC-26. A linear mixed model with random intercept by an individual to account for the correlation present within individuals will be used to compare pretreatment vs. posttreatment quality of life measures at multiple timepoints with the goal of tracking minimally important differences in these parameters (57).
Five-year DFS will be determined as a composite of biochemical control, patient death or development of clinical metastases, or institution of salvage ADT. DFS will be estimated with a Kaplan–Meier (KM) curve, with the 5-year estimate extracted from the KM curve.
Changes in SUV metrics (SUVmax, SUVmean) within PSMA PET regions of interest (ROI) will be compared between the pre-RT PSMA PET and the 6-month post-RT PSMA PET. ROIs to be examined will include the dominant intra-prostatic lesions (DILs), the prostate as a whole, and, in the cases of men with PET-detected nodal disease, involved node ROIs. Descriptive statistics and diagrams (i.e., waterfall plots) will be used to characterize changes in SUV metrics. A linear mixed model with random intercept by an individual to account for the correlation present within individuals will be used to compare pretreatment vs. posttreatment SUV values at multiple timepoints. Overall response rates will be calculated in accordance with recent consensus guidelines (46).
Intra-prostatic mpMRI (T2W, DWI, and DCE-MRI) acquired pre-RT and 6 and 24 months post-RT will be reported by expert readers based on PI-RADS 2.1 and the complementary Prostate Imaging for Recurrence Reporting (PI-RR) system to identify intra-prostatic ROIs (44). Quantitative MRI metrics will be extracted, including ADC and pharmacokinetics parameters derived from dynamic PET and DCE-MRI. Radiomics approaches will be used to characterize the evolution of higher-level feature changes in PET and mpMRI over the course of treatment.
We will correlate changes in PET and mpMRI metrics at 6 and 24 months with 5-year DFS using linear regression models. We will also perform supervised machine learning to train support vector machines and random forest classifiers to predict response based on the pretreatment images. We will also perform a delta-radiomics analysis to predict response based on the radiomics trajectory computed from the first two time points. We will measure the performance of the classifiers using a cross-validation design, with metrics including the area under the receiver operating characteristic (ROC) curve and the error rate, false-positive rate, and false-negative rate computed at a point on the ROC curve that best balance the false-positive and false-negative rates. We will develop radiomics-based classifiers to predict 5-year DFS.
Baseline (pretreatment) and 24-month (posttreatment) tissue samples will be acquired for histopathologic correlations with PET/MR images. Specifically, baseline biopsy will provide histologic correlation for the PSMA- and mpMRI-identified dominant intra-prostatic lesions. Additionally, 24-month biopsies have been shown to correlate with long-term failure-free survival (36, 39), and rates of cancer clearance after stereotactic techniques have been shown to increase with increasing doses of radiation (58). Understanding histologic correlations and clearance of cancer from the boosted and non-boosted prostate areas will be of interest and will allow for correlation with PET/MR images to validate PET+MRI as non-invasive surrogates for identifying intra-prostatic cancer foci.
Advanced prostate imaging with mpMRI and novel PET agents has the potential to improve prostate cancer management across the disease spectrum (23). In the primary management of prostate cancer, improved imaging guidance has allowed for radiotherapy advances for prostate cancer, including prostate SBRT and focal boost (3–6, 11). Ongoing trials are evaluating SBRT with focal boost guided by mpMRI and PSMA-PET (NCT04243941, NCT04402151, and NCT04599699) (21, 59). The ARGOS/CLIMBER trial will explore the safety of SBRT with focal boost guided by mpMRI and 18F-PSMA-1007 PET.
In addition, advanced imaging has improved the ability to characterize patterns of disease recurrence and identify men with isolated local recurrence who may be suitable for local salvage or oligometastatic recurrence who may be eligible for metastasis-directed therapy (14, 45, 52, 60). To date, response to prostate SBRT is mostly commonly evaluated using biochemical response with the Phoenix Criteria for BF. The drawbacks of this approach include lack of lesion identification, a high false-positive rate, and delay in identifying treatment failure. An important knowledge gap is the expected evolution of imaging changes post-SBRT and whether patterns in these changes can serve as early biomarkers of disease recurrence. Patients in ARGOS/CLIMBER will receive dynamic 18F-PSMA-1007 PET and mpMRI prior to SBRT and at 6 and 24 months after SBRT. Imaging findings will be correlated with PSA and biopsy results, with the goal of early, non-invasive, and accurate identification of treatment failure.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Ontario Cancer Research Ethics Board. The patients/participants provided their written informed consent to participate in this study.
All authors contributed to the project design and manuscript drafting. All authors approved the publication of the content and agree to be accountable for all aspects of the work.
The ARGOS/CLIMBER study is supported by the Clinical Translation Program of the Ontario Institute for Cancer Research, grant identifier P.CTP.624.
T-YL declares receiving royalties from GE Healthcare. JB declares receiving grants from Thermo Fisher Scientific and payments or honoraria from Thermo Fisher Scientific and NanoString Technologies, Inc., and has two pending patents. GB declares grants from the Ontario Institute for Cancer Research, Ontario Health, and Centre for Probe Development and Commercialization and industry collaboration with Siemens Healthineers and InVicro.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Roach M, Hanks G, Thames H, Schellhammer P, Shipley WU, Sokol GH, et al. Defining Biochemical Failure Following Radiotherapy With or Without Hormonal Therapy in Men With Clinically Localized Prostate Cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys (2006) 65:965–74. doi: 10.1016/j.ijrobp.2006.04.029
2. Oh J, Tyldesley S, Pai HH, McKenzie MR, Halperin RM, Duncan GG, et al. An Updated Analysis of Survival Endpoints for ASCENDE-RT, A Randomized Trial Comparing a Low-Dose-Rate Brachytherapy Boost to a Dose-Escalated External Beam Boost for High- and Intermediate-Risk Prostate Cancer. Int J Radiat Oncol Biol Phys (2020) 108:S62. doi: 10.1016/j.ijrobp.2020.07.2194
3. Brand DH, Tree AC, Ostler P, van der Voet H, Loblaw A, Chu W, et al. Intensity-Modulated Fractionated Radiotherapy Versus Stereotactic Body Radiotherapy for Prostate Cancer (PACE-B): Acute Toxicity Findings From an International, Randomised, Open-Label, Phase 3, Non-Inferiority Trial. Lancet Oncol (2019) 20:1531–43. doi: 10.1016/S1470-2045(19)30569-8
4. Draulans C, van der Heide UA, Haustermans K, Pos FJ, van der Voort van Zyp J, De Boer H, et al. Primary Endpoint Analysis of the Multicentre Phase II Hypo-FLAME Trial for Intermediate and High Risk Prostate Cancer. Radiother Oncol: J Eur Soc Ther Radiol Oncol (2020) 147:92–8. doi: 10.1016/j.radonc.2020.03.015
5. Kerkmeijer LGW, Groen VH, Pos FJ, Haustermans K, Monninkhof EM, Smeenk RJ, et al. Focal Boost to the Intraprostatic Tumor in External Beam Radiotherapy for Patients With Localized Prostate Cancer: Results From the FLAME Randomized Phase III Trial. J Clin Oncol: Off J Am Soc Clin Oncol (2021) 39:787–96.
6. Alayed Y, Davidson M, Liu S, Chu W, Tseng E, Cheung P, et al. Evaluating the Tolerability of a Simultaneous Focal Boost to the Gross Tumor in Prostate SABR: A Toxicity and Quality-Of-Life Comparison of Two Prospective Trials. Int J Radiat Oncol Biol Phys (2020) 107:136–42. doi: 10.1016/j.ijrobp.2019.12.044
7. Chopra S, Toi A, Taback N, Evans A, Haider MA, Milosevic M, et al. Pathological Predictors for Site of Local Recurrence After Radiotherapy for Prostate Cancer. Int J Radiat Oncol Biol Phys (2012) 82(3):e441–48. doi: 10.1016/j.ijrobp.2011.05.035
8. Al-Mamgani A, van Putten WL, Heemsbergen WD, van Leenders GJ, Slot A, Dielwart MF, et al. Update of Dutch Multicenter Dose-Escalation Trial of Radiotherapy for Localized Prostate Cancer. Int J Radiat Oncol Biol Phys (2008) 72:980–8. doi: 10.1016/j.ijrobp.2008.02.073
9. Kim YJ, Yoon KJ, Kim YS. Simultaneous Integrated Boost With Stereotactic Radiotherapy for Dominant Intraprostatic Lesion of Localized Prostate Cancer: A Dosimetric Planning Study. Sci Rep (2020) 10(1). doi: 10.1038/s41598-020-71715-2
10. Goodman CD, Fakir H, Pautler S, Chin J, Bauman GS. Dosimetric Evaluation of PSMA PET-Delineated Dominant Intraprostatic Lesion Simultaneous Infield Boosts. Adv Radiat Oncol (2019) 5:212–20. doi: 10.1016/j.adro.2019.09.004
11. Murray JR, Tree AC, Alexander EJ, Sohaib A, Hazell S, Thomas K, et al. Standard and Hypofractionated Dose Escalation to Intraprostatic Tumor Nodules in Localized Prostate Cancer: Efficacy and Toxicity in the DELINEATE Trial. Int J Radiat Oncol Biol Phys (2020) 106:715–24. doi: 10.1016/j.ijrobp.2019.11.402
12. Monninkhof EM, van Loon JWL, van Vulpen M, Kerkmeijer LGW, Pos FJ, Haustermans K, et al. Standard Whole Prostate Gland Radiotherapy With and Without Lesion Boost in Prostate Cancer: Toxicity in the FLAME Randomized Controlled Trial. Radiother Oncol: J Eur Soc Ther Radiol Oncol (2018) 127:74–80. doi: 10.1016/j.radonc.2017.12.022
13. Groen VH, Haustermans K, Pos FJ, Draulans C, Isebaert S, Monninkhof EM, et al. Patterns of Failure Following External Beam Radiotherapy With or Without an Additional Focal Boost in the Randomized Controlled FLAME Trial for Localized Prostate Cancer. Eur Urol (2021). doi: 10.1016/J.EURURO.2021.12.012
14. Valle LF, Lehrer EJ, Markovic D, Elashoff D, Levin-Epstein R, Karnes RJ, et al. A Systematic Review and Meta-Analysis of Local Salvage Therapies After Radiotherapy for Prostate Cancer (MASTER). Eur Urol (2020) 80(3):280–92. doi: 10.1016/j.eururo.2020.11.010
15. Crook J, Rodgers JP, Pisansky TM, Trabulsi EJ, Amin MB, Bice W, et al. Salvage Low-Dose-Rate Prostate Brachytherapy: Clinical Outcomes of a Phase 2 Trial for Local Recurrence After External Beam Radiation Therapy (NRG Oncology/0526). Int J Radiat Oncol Biol Phys (2021) 112(5):1115–22. doi: 10.1016/j.ijrobp.2021.10.138
16. Gibson E, Bauman GS, Romagnoli C, Cool DW, Bastian-Jordan M, Kassam Z, et al. Toward Prostate Cancer Contouring Guidelines on Magnetic Resonance Imaging: Dominant Lesion Gross and Clinical Target Volume Coverage Via Accurate Histology Fusion. Int J Radiat Oncol Biol Phys (2016) 96:188–96. doi: 10.1016/j.ijrobp.2016.04.018
17. Bettermann AS, Zamboglou C, Kiefer S, Jilg CA, Spohn S, Kranz-Rudolph J, et al. [68ga-]PSMA-11 PET/CT and Multiparametric MRI for Gross Tumor Volume Delineation in a Slice by Slice Analysis With Whole Mount Histopathology as a Reference Standard – Implications for Focal Radiotherapy Planning in Primary Prostate Cancer. Radiother Oncol (2019) 141:214–19. doi: 10.1016/j.radonc.2019.07.005
18. Spohn SKB, Kramer M, Kiefer S, Bronsert P, Sigle A, Schultze-Seemann W, et al. Comparison of Manual and Semi-Automatic [18f]PSMA-1007 PET Based Contouring Techniques for Intraprostatic Tumor Delineation in Patients With Primary Prostate Cancer and Validation With Histopathology as Standard of Reference. Front Oncol (2020) 10:600690. doi: 10.3389/fonc.2020.600690
19. Chen M, Zhang Q, Zhang C, Zhao X, Marra G, Gao J, et al. Combination of 68Ga-PSMA PET/CT and Multiparametric MRI Improves the Detection of Clinically Significant Prostate Cancer: A Lesion-by-Lesion Analysis. J Nucl Med (2019) 60:944–9. doi: 10.2967/jnumed.118.221010
20. Emmett L, Buteau J, Papa N, Moon D, Thompson J, Roberts MJ, et al. The Additive Diagnostic Value of Prostate-Specific Membrane Antigen Positron Emission Tomography Computed Tomography to Multiparametric Magnetic Resonance Imaging Triage in the Diagnosis of Prostate Cancer (PRIMARY): A Prospective Multicentre Study. Eur Urol (2021) 80:682–9.
21. Zamboglou C, Spohn SKB, Adebahr S, Huber M, Kirste S, Sprave T, et al. PSMA-PET/MRI-Based Focal Dose Escalation in Patients With Primary Prostate Cancer Treated With Stereotactic Body Radiation Therapy (HypoFocal-SBRT): Study Protocol of a Randomized, Multicentric Phase III Trial. Cancers (2021) 13:5795.
22. Hofman MS, Lawrentschuk N, Francis RJ, Tang C, Vela I, Thomas P, et al. Prostate-Specific Membrane Antigen PET-CT in Patients With High-Risk Prostate Cancer Before Curative-Intent Surgery or Radiotherapy (proPSMA): A Prospective, Randomised, Multicentre Study. Lancet (London England) (2020) 395:1208–16. doi: 10.1016/S0140-6736(20)30314-7
23. Trabulsi EJ, Rumble RB, Jadvar H, Hope T, Pomper M, Turkbey B, et al. Optimum Imaging Strategies for Advanced Prostate Cancer: ASCO Guideline. J Clin Oncol (2020) 38:1963–96.
24. Perera M, Papa N, Roberts M, Williams M, Udovicich C, Vela I, et al. Gallium-68 Prostate-Specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer—Updated Diagnostic Utility, Sensitivity, Specificity, and Distribution of Prostate-Specific Membrane Antigen-Avid Lesions: A Systematic Review and Meta-Analysis. Eur Urol (2020) 77:403–17. doi: 10.1016/j.eururo.2019.01.049
25. Werner RA, Derlin T, Lapa C, Sheikbahaei S, Higuchi T, Giesel FL, et al. 18f-Labeled, PSMA-Targeted Radiotracers: Leveraging the Advantages of Radiofluorination for Prostate Cancer Molecular Imaging. Theranostics (2020) 10:1. doi: 10.7150/thno.37894
26. Dietlein F, Kobe C, Hohberg M, Zlatopolskiy BD, Krapf P, Endepols H, et al. Intraindividual Comparison of 18F-PSMA-1007 With Renally Excreted PSMA Ligands for PSMA-PET Imaging in Patients With Relapsed Prostate Cancer. J Nucl Med (2019) 61:729–34. doi: 10.2967/jnumed.119.234898
27. Gaur S, Mena E, Harmon SA, Lindenberg ML, Adler S, Ton AT, et al. Prospective Evaluation of 18 F-DCFPyL PET/CT in Detection of High-Risk Localized Prostate Cancer: Comparison With mpMRI. AJR Am J Roentgenology (2020) 215:652–9. doi: 10.2214/AJR.19.22042
28. Song H, Harrison C, Duan H, Guja K, Hatami N, Franc BL, et al. Prospective Evaluation of 18 F-DCFPyL PET/CT in Biochemically Recurrent Prostate Cancer in an Academic Center: A Focus on Disease Localization and Changes in Management. J Nucl Med: Off Publ Soc Nucl Med (2020) 61:549–51. doi: 10.2967/jnumed.119.231654
29. Bauman G, Martin P, Thiessen JD, Taylor R, Moussa M, Gaed M, et al. [ 18 F]-DCFPyL Positron Emission Tomography/Magnetic Resonance Imaging for Localization of Dominant Intraprostatic Foci: First Experience. Eur Urol Focus (2018) 4:702–6. doi: 10.1016/j.euf.2016.10.002
30. Alfano R, Bauman GS, Liu W, Thiessen JD, Rachinsky I, Pavlosky W, et al. Histologic Validation of Auto-Contoured Dominant Intraprostatic Lesions on [18F] DCFPyL PSMA-PET Imaging. Radiother Oncol (2020) 152:34–41. doi: 10.1016/j.radonc.2020.08.008
31. Kesch C, Vinsensia M, Radtke JP, Schlemmer HP, Heller M, Ellert E, et al. Intraindividual Comparison of 18 F-PSMA-1007 PET/CT, Multiparametric MRI, and Radical Prostatectomy Specimens in Patients With Primary Prostate Cancer: A Retrospective, Proof-Of-Concept Study. J Nucl Med: Off Publ Soc Nucl Med (2017) 58:1805–10. doi: 10.2967/jnumed.116.189233
32. Giesel FL, Will L, Lawal I, Lengana T, Kratochwil C, Vorster M, et al. Intraindividual Comparison of 18 F-PSMA-1007 and 18 F-DCFPyL PET/CT in the Prospective Evaluation of Patients With Newly Diagnosed Prostate Carcinoma: A Pilot Study. J Nucl Medicine: Off Publication Soc Nucl Med (2018) 59:1076–80. doi: 10.2967/jnumed.117.204669
33. Privé BM, Israël B, Schilham MGM, Muselaers CHJ, Zámecnik P, Mulders PFA, et al. Evaluating F-18-PSMA-1007-PET in Primary Prostate Cancer and Comparing It to Multi-Parametric MRI and Histopathology. Prostate Cancer Prostatic Dis (2021) 24:423–30. doi: 10.1038/s41391-020-00292-2
34. Levin-Epstein R, Wong JK, Stock RG, Demanes DJ, Collins SP, et al. Prostate-Specific Antigen Kinetics and Biochemical Control Following Stereotactic Body Radiation Therapy, High Dose Rate Brachytherapy, and Low Dose Rate Brachytherapy: A Multi-Institutional Analysis of 3502 Patients. Radiother Oncol (2020) 151:26–32. doi: 10.1016/j.radonc.2020.07.014
35. Ma TM, Roy S, Wu X, Mantz C, Fuller D, Miszczyk L, et al. Refining the Definition of Biochemical Failure in the Era of Stereotactic Body Radiation Therapy for Prostate Cancer: The Phoenix Definition and Beyond. Radiother Oncol (2022) 166:1–7. doi: 10.1016/j.radonc.2021.11.005
36. Zelefsky MJ, Goldman DA, Hopkins M, Pinitpatcharalert A, McBride S, Gorovets D, et al. Predictors for Post-Treatment Biopsy Outcomes After Prostate Stereotactic Body Radiotherapy. Radiother Oncol (2021) 159:33–8. doi: 10.1016/j.radonc.2021.02.008
37. Jansen BHE, van Leeuwen PJ, Wondergem M, van der Sluis TM, Nieuwenhuijzen JA, Knol RJJ, et al. Detection of Recurrent Prostate Cancer Using Prostate-Specific Membrane Antigen Positron Emission Tomography in Patients Not Meeting the Phoenix Criteria for Biochemical Recurrence After Curative Radiotherapy. Eur Urol Oncol (2021) 4:821–5. doi: 10.1016/j.euo.2020.01.002
38. Corkum MT, Mendez LC, Chin J, D’Souza D, Boldt RG, Bauman GS. A Novel Salvage Option for Local Failure in Prostate Cancer, Reirradiation Using External Beam or Stereotactic Radiotherapy: Systematic Review and Meta-Analysis. Adv Radiat Oncol (2020) 5(5):965–775. doi: 10.1016/j.adro.2020.04.022
39. Crook JM, Malone S, Perry G, Eapen L, Owen J, Robertson S, et al. Twenty-Four-Month Postradiation Prostate Biopsies Are Strongly Predictive of 7-Year Disease-Free Survival. Cancer (2009) 115:673–9. doi: 10.1002/cncr.24020
40. Kirilova A, Damyanovich A, Crook J, Jezioranski J, Wallace K, Pintilie M. 3d MR-Spectroscopic Imaging Assessment of Metabolic Activity in the Prostate During the PSA “Bounce” Following 125iodine Brachytherapy. Int J Radiat Oncol Biol Phys (2011) 79:371–8. doi: 10.1016/j.ijrobp.2009.10.066
41. Pickett B, Kurhanewicz J, Coakley F, Shinohara K, Fein B, Roach M. Use of MRI and Spectroscopy in Evaluation of External Beam Radiotherapy for Prostate Cancer. Int J Radiat Oncol Biol Phys (2004) 60:1047–55. doi: 10.1016/j.ijrobp.2004.05.015
42. Crehange G, Maingon P, Gauthier M, Parfait S, Cochet A, Mirjolet C, et al. Early Choline Levels From 3-Tesla MR Spectroscopy After Exclusive Radiation Therapy in Patients With Clinically Localized Prostate Cancer Are Predictive of Plasmatic Levels of PSA at 1 Year. Int J Radiat Oncol Biol Phys (2011) 81(4):e407–13. doi: 10.1016/j.ijrobp.2011.03.008
43. Valentini AL, Gui B, D’Agostino GR, Mattiucci G, Clementi V, Di Molfetta IV, et al. Locally Advanced Prostate Cancer: Three-Dimensional Magnetic Resonance Spectroscopy to Monitor Prostate Response to Therapy. Int J Radiat Oncol Biol Phys (2012) 84:719–24. doi: 10.1016/j.ijrobp.2011.12.089
44. Panebianco V, Villeirs G, Weinreb JC, Turkbey BI, Margolis DJ, Richenberg J, et al. Prostate Magnetic Resonance Imaging for Local Recurrence Reporting (PI-RR): International Consensus -Based Guidelines on Multiparametric Magnetic Resonance Imaging for Prostate Cancer Recurrence After Radiation Therapy and Radical Prostatectomy. Eur Urol Oncol (2021) 4:868–76. doi: 10.1016/j.euo.2021.01.003
45. Liu W, Fakir H, Randhawa G, Alfano R, Corkum M, Kassam Z, et al. Defining Radio-Recurrent Intra-Prostatic Target Volumes Using PSMA-Targeted PET/CT and Multi-Parametric MRI. Clin Trans Radiat Oncol (2022) 32:41–7. doi: 10.1016/j.ctro.2021.11.006
46. Fanti S, Goffin K, Hadaschik BA, Herrmann K, Maurer T, MacLennan S, et al. Consensus Statements on PSMA PET/CT Response Assessment Criteria in Prostate Cancer. Eur J Nucl Med Mol Imaging (2021) 48:469–76. doi: 10.1007/s00259-020-04934-4
47. Schöder H, Hope TA, Knopp M, Kelly WK, Michalski JM, Lerner SP, et al. Considerations on Integrating Prostate-Specific Membrane Antigen Positron Emission Tomography Imaging Into Clinical Prostate Cancer Trials by National Clinical Trials Network Cooperative Groups. J Clin Oncol: Off J Am Soc Clin Oncol (2022). doi: 10.1200/JCO.21.02440
48. Polinspedro V, Sistani G, Rachinsky I, Zukotynski K, Bauman G, Liu W. Case – Prostate-Specific Antigen Bounce: A Pitfall in Prostate-Specific Membrane Antigen Positron Emission Tomography/Computed Tomography Interpretation. Can Urological Assoc J (2021) 15(11). doi: 10.5489/cuaj.7257
49. Fendler WP, Calais J, Eiber M, Flavell RR, Mishoe A, Feng FY, et al. False Positive PSMA PET for Tumor Remnants in the Irradiated Prostate and Other Interpretation Pitfalls in a Prospective Multi-Center Trial. Eur J Nucl Med Mol Imaging (2020) 48(2):501–8. doi: 10.1007/s00259-020-04945-1
50. Young S, Liu W, Zukotynski K, Bauman G. Prostate-Specific Membrane Antigen Targeted PET/CT for Recurrent Prostate Cancer: A Clinician’s Guide. Expert Rev Anticancer Ther (2021). doi: 10.1080/14737140.2021.1878883
51. Parker C, Castro E, Fizazi K, Heidenreich A, Ost P, Procopio G, et al. Prostate Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol: Off J Eur Soc Med Oncol (2020) 31:1119–34. doi: 10.1016/j.annonc.2020.06.011
52. Liu W, Zukotynski K, Emmett L, Chung HT, Chung P, Wolfson R, et al. A Prospective Study of 18F-DCFPyL PSMA PET/CT Restaging in Recurrent Prostate Cancer Following Primary External Beam Radiotherapy or Brachytherapy. Int J Radiat Oncol Biol Phys (2019) 106:546–55. doi: 10.1016/j.ijrobp.2019.11.001
53. Liu W, Zukotynski K, Emmett L, Chung HT, Chung P, Wolfson R, et al. Utilization of Salvage and Systemic Therapies for Recurrent Prostate Cancer as a Result of 18F-DCFPyL PET/CT Restaging. Adv Radiat Oncol (2020). doi: 10.1016/j.adro.2020.08.010
54. Alberts IL, Seide SE, Mingels C, Bohn KP, Shi K, Zacho HD, et al. Comparing the Diagnostic Performance of Radiotracers in Recurrent Prostate Cancer: A Systematic Review and Network Meta-Analysis. Eur J Nucl Med Mol Imaging (2021) 48:2978–89. doi: 10.1007/s00259-021-05210-9
55. Fendler WP, Calais J, Eiber M, Flavell RR, Mishoe A, Feng FY, et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. in. JAMA Oncol (2019) 5:856–63. doi: 10.1001/jamaoncol.2019.0096
56. Yang DM, Alfano R, Bauman G, Thiessen JD, Chin J, Pautler S, et al. Short-Duration Dynamic [ 18 F]DCFPyL PET and CT Perfusion Imaging to Localize Dominant Intraprostatic Lesions in Prostate Cancer: Validation Against Digital Histopathology and Comparison to [ 18 F]DCFPyL PET/MR at 120 Minutes. EJNMMI Res (2021) 11. doi: 10.1186/s13550-021-00844-0
57. Skolarus TA, Dunn RL, Sanda MG, Chang P, Greenfield TK, Litwin MS, et al. Minimally Important Difference for the Expanded Prostate Cancer Index Composite Short Form. Urology (2015) 85:101–6. doi: 10.1016/j.urology.2014.08.044
58. Zelefsky MJ, Kollmeier M, McBride S, Varghese M, Mychalczak B, Gewanter R, et al. Five-Year Outcomes of a Phase 1 Dose-Escalation Study Using Stereotactic Body Radiosurgery for Patients With Low-Risk and Intermediate-Risk Prostate Cancer. Int J Radiat Oncol Biol Phys (2019) 104:42–9. doi: 10.1016/j.ijrobp.2018.12.045
59. Eade T, Kneebone A, Hruby G, Booth J, Hsiao E, Le A, et al. Early Outcomes and Decision Regret Using PSMA/MRI Guided Focal Boost for Prostate Cancer SBRT. Pract Radiat Oncol (2021). doi: 10.1016/J.PRRO.2021.09.008
60. Palma DA, Olson R, Harrow S, Gaede S, Louie AV, Haasbeek C, et al. Stereotactic Ablative Radiotherapy Versus Standard of Care Palliative Treatment in Patients With Oligometastatic Cancers (SABR-COMET): A Randomised, Phase 2, Open-Label Trial. Lancet (2019) 393(10185):2051–58. doi: 10.1016/S0140-6736(18)32487-5
Keywords: SBRT, prostate cancer, PSMA PET, MRI, stereotactic, ultrahypofractionated
Citation: Liu W, Loblaw A, Laidley D, Fakir H, Mendez L, Davidson M, Kassam Z, Lee T-Y, Ward A, Thiessen J, Bayani J, Conyngham J, Bailey L, Andrews JD and Bauman G (2022) Imaging Biomarkers in Prostate Stereotactic Body Radiotherapy: A Review and Clinical Trial Protocol. Front. Oncol. 12:863848. doi: 10.3389/fonc.2022.863848
Received: 27 January 2022; Accepted: 07 March 2022;
Published: 13 April 2022.
Edited by:
Amar U. Kishan, University of California, Los Angeles, United StatesReviewed by:
Thomas Zilli, Université de Genève, SwitzerlandCopyright © 2022 Liu, Loblaw, Laidley, Fakir, Mendez, Davidson, Kassam, Lee, Ward, Thiessen, Bayani, Conyngham, Bailey, Andrews and Bauman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Glenn Bauman, Z2xlbm4uYmF1bWFuQGxoc2Mub24uY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.