
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 14 July 2022
Sec. Genitourinary Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.858813
This article is part of the Research Topic Insights in Genitourinary Oncology: 2021 View all 19 articles
 Seung-hwan Jeong1
Seung-hwan Jeong1 Jang Hee Han1
Jang Hee Han1 Chang Wook Jeong1,2
Chang Wook Jeong1,2 Hyeon Hoe Kim1,2
Hyeon Hoe Kim1,2 Cheol Kwak1,2Hyeong Dong Yuk1,2*
Cheol Kwak1,2Hyeong Dong Yuk1,2* Ja Hyeon Ku1,2*
Ja Hyeon Ku1,2*Upper tract urothelial carcinoma (UTUC) occurs in urothelial cells from the kidney and the ureters. Carbohydrate antigen 19-9 (CA 19-9) is a tumor marker for pancreatic and gastrointestinal cancers, and its high levels are associated with poor prognosis in bladder cancer. In this study, prospective patients enrolled in the registry of Seoul National University were retrospectively examined to determine the clinical significance of CA 19-9 in UTUC. In 227 patients, high serum CA 19-9 levels reflected a high tumor burden represented by high T and N stages, leading to adverse prognosis in metastasis-free or overall survival. Subsequently, propensity score matching analysis showed that the CA 19-9 level is an independent prognostic factor of UTUC.
Urothelial carcinoma arises from epithelial cells lining the urinary system. Most urothelial carcinomas occur in the urinary bladder, whereas upper tract urothelial carcinoma (UTUC), involving the renal calyx, pelvis, and ureter, accounts for 5%–10% of urothelial carcinomas (1, 2). The prognosis of UTUC depends on the T stage, which shows a 5-year survival rate from 90.2% to 18.5% through stages T1 to T4 (3). Risk classification stratifies UTUC as low- or high-risk, with low-risk cases allowing kidney-sparing surgeries, such as segmental ureterectomy and endoscopic ablation (4). In contrast, definitive treatment with nephroureterectomy is required for high-risk patients with adverse features. In addition, perioperative chemotherapy provides benefits in overall survival (OS) and cancer-specific survival with much concrete evidence in an adjuvant setting (5). The clinical staging of UTUC is restricted because of the pitfalls of computed tomography (CT) urography in discriminating between the T stages of carcinoma in situ and T2 (6). Thus, appropriate tools are required to evaluate the disease burden and to stratify risk classification.
Carbohydrate antigen 19-9 (CA 19-9) is a sialylated Lewis antigen. It is a tumor marker that predicts tumor stage, disease burden, and recurrence in pancreatic and gastrointestinal cancers (7–9). Although CA 19-9 is not a diagnostic marker in urothelial carcinoma, it is reportedly associated with the disease burden and aggressive features of bladder cancer, implying poor prognosis (10–12). In the present study, serum CA 19-9 levels in patients with UTUC were evaluated to reveal its clinical relevance implicating tumor burdens and clinical outcomes.
The analyzed clinical data were of patients with UTUC enrolled in the Seoul National University Prospective Enrolled Registry for urothelial cancer from March 2016 to December 2020 with institutional review board approval (IRB No. 2201-032-1289) (13). From 420 patients, 227 patients whose preoperative serum CA 19-9 levels were measured were selected and stratified into low- (≤ 37 U/ml) and high-CA 19-9 (> 37 U/ml) level groups as normal value of CA 19-9 is considered to be lower than 37 U/ml (14). Preoperative and postoperative data, including the underlying disease, clinical and pathologic stage, and findings, were queried and compared.
Two-tailed t-tests were performed on parametric values, such as age, body mass index (BMI), and CA 19-9 level. The chi-square test was performed for categorical variables, including sex, underlying disease status, clinical and pathologic stage, hydronephrosis, perioperative chemotherapy, and tumor grade. Metastasis-free survival and OS were analyzed using Kaplan–Meier survival analysis, with the log-rank test for significance evaluation. To alleviate confounding effects derived from tumor burdens correlated with CA 19-9 levels, propensity score matching (PSM) was conducted to match pathologic T and N stages with a 1:4 ratio in both patient groups. Statistical analysis was performed using XLSTAT (version 2021.5-life sciences). Statistical significance was set at p < 0.05.
In a total of 227 patients, 199 and 28 patients were classified into low- and high-CA 19-9-level groups, respectively. The two groups were similar in terms of demographic findings, such as sex (male proportion of 71% vs. 57.1%, p = 0.126), age (70.4 vs. 71.8 years, p = 0.485), and BMI (24.7 vs. 24.1%, p = 0.388) (Table 1). Underlying diseases, including hypertension, diabetes mellitus, liver disease, and dyslipidemia, were also similar between the two groups. Cisplatin-based neoadjuvant chemotherapy was administered to 3.02% and 3.57% patients in the low- and high-CA 19-9-level groups, respectively (p = 0.873). All patients underwent nephroureterectomy via open, laparoscopic, or robotic procedures in similar proportions (p = 0.665). The clinical stage was significantly higher in the high-CA 19-9-level group, represented by 32.6% of the T3 or T4 stage population, compared with 21.1% in the low-CA 19-9-level group (p = 0.016). Accordingly, hydronephrosis was more prevalent in the high-CA 19-9-level group, without statistical significance. The pathologic T stage was higher in those with high CA 19-9 levels, with 69.9% of them having stage T3 or T4 tumors, compared to 36.7% of those with low CA 19-9 levels (p = 0.037). Furthermore, pathologic N1 or N2 stage was diagnosed in 21.5% of the patients in the high-CA 19-9 level group, which was higher than 4.0% in the low-CA 19-9 level group (p = 0.002). Cisplatin-based adjuvant chemotherapy was administered to similar proportion of patients in the two groups (22.6% vs. 28.6%, p = 0.485). Both the 2-year metastasis-free survival (77.0% vs. 22.5%, p = 0.003) and OS (96.4% vs. 79.8%, p = 0.007) rates were significantly higher in the low-CA 19-9-level group (Figure 1). COX regression analysis was performed to reveal factors associated with metastasis. Among the included variables, high CA19-9 level, high T stage and N stage were significantly associated with the risk of metastasis (Table 2).
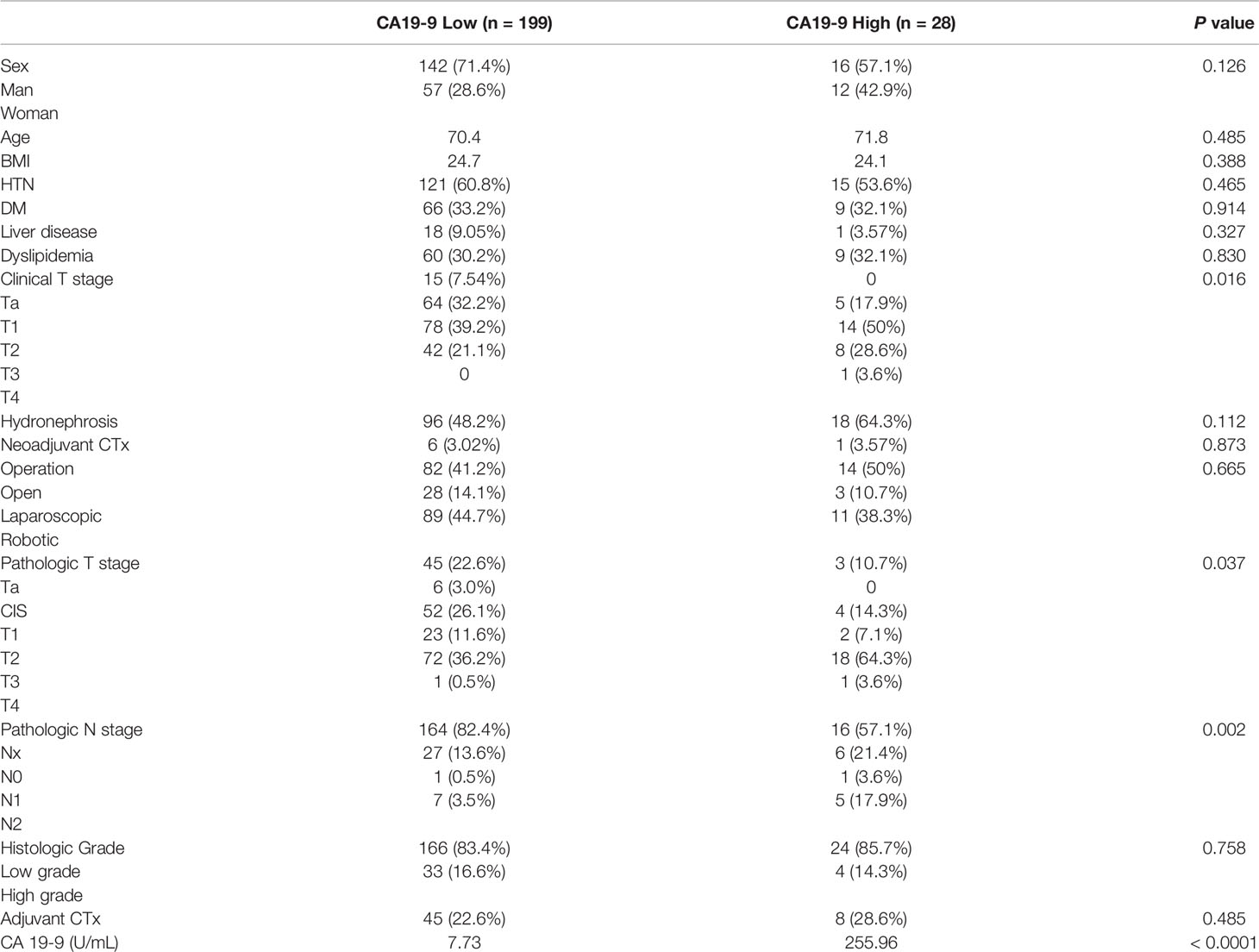
Table 1 Characteristics of patients with low or high CA19-9 level.
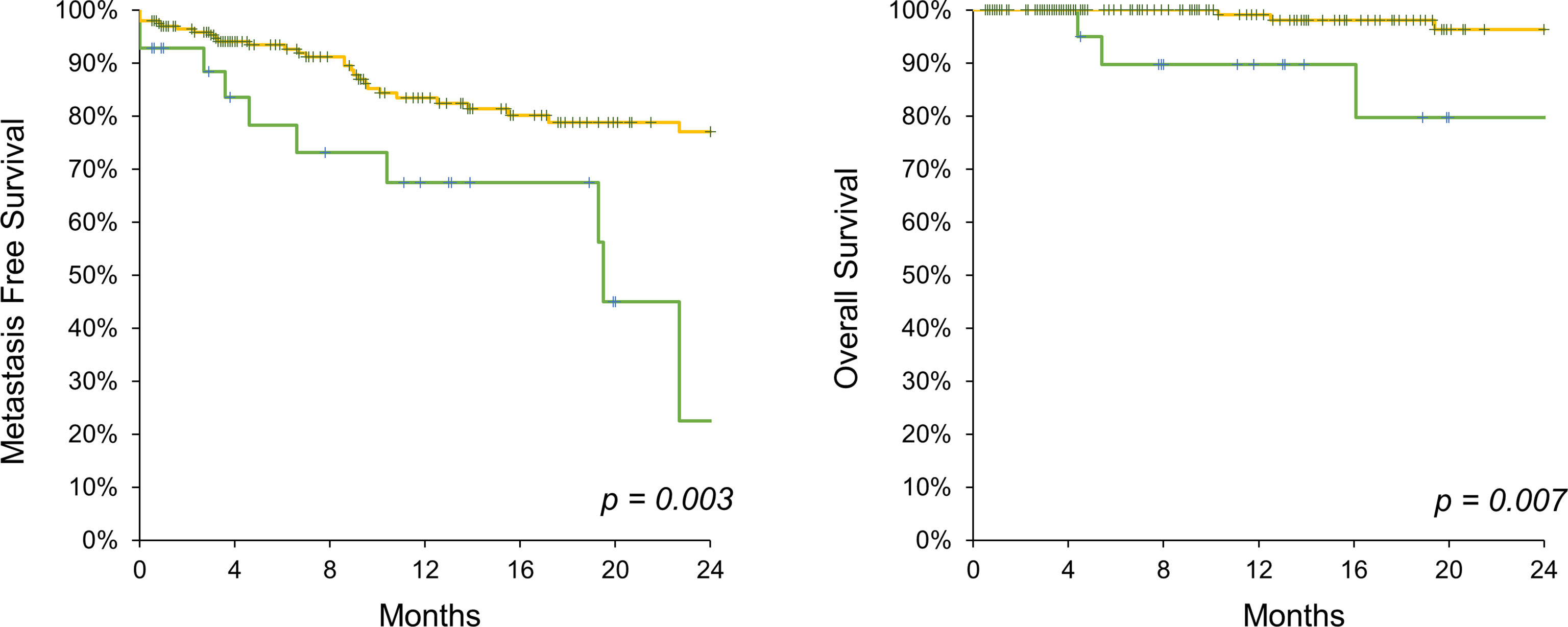
Figure 1 Kaplan-Meier analysis on metastasis free survival (left) and overall survival (right) comparing CA 19-9 high (green line) and low (yellow line) UTUC patients.
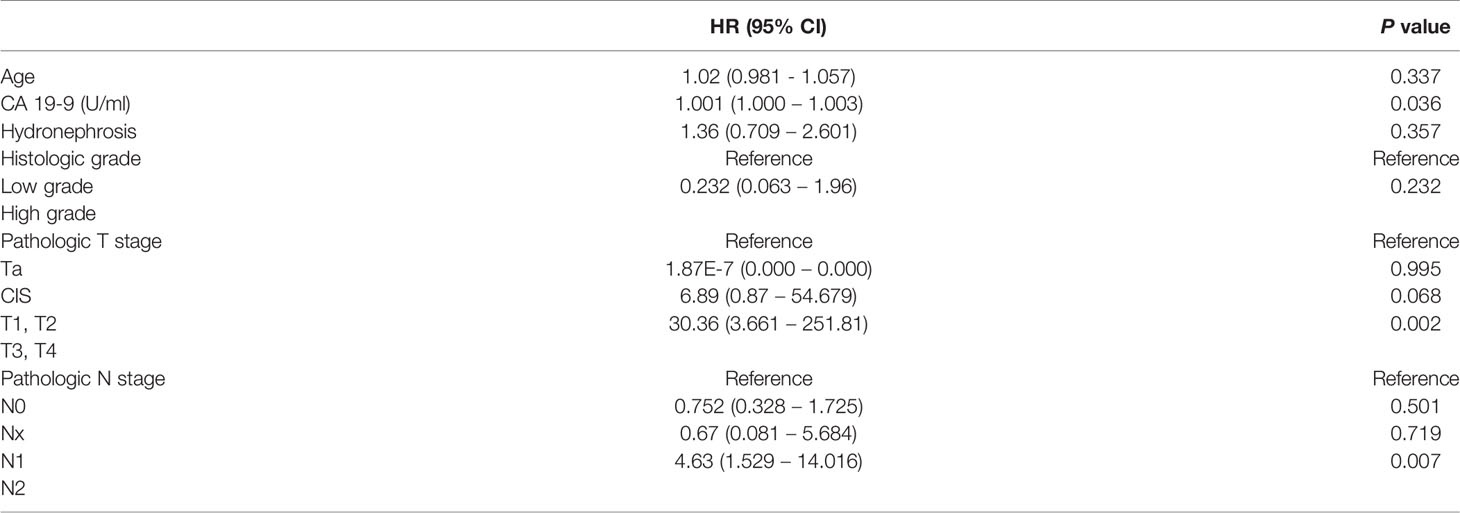
Table 2 COX regression analysis for metastasis.
In the high-CA 19-9-level group, the tumor burden was higher, leading to poor prognosis. To identify CA 19-9 as an independent prognostic factor, PSM analysis was performed for pathological T and N stages. In the PSM cases, demographic findings and underlying diseases remained relatively different between the two groups (Table 3). Clinical stage did not differ between the two groups (p = 0.123), which was reflected in the incidence of hydronephrosis (p = 0.269). Neoadjuvant or adjuvant chemotherapy was administered to similar proportion of patients in both groups. The pathologic T stage was matched in similar proportions between the two groups, represented by 64.3% and 67.9% of patients with T3 or higher stage in the low- and high-CA 19-9-level groups, respectively (p = 0.904). The pathologic N stage tended to be higher in the high-CA 19-9 level group, without statistical significance (p = 0.13). Interestingly, in the PSM analysis, the two-year metastasis free survival (71.2% vs. 22.5%, p = 0.031) and OS (95.4% vs. 79.8%, p = 0.029) rates were significantly higher in the low-CA 19-9-level group (Figure 2).
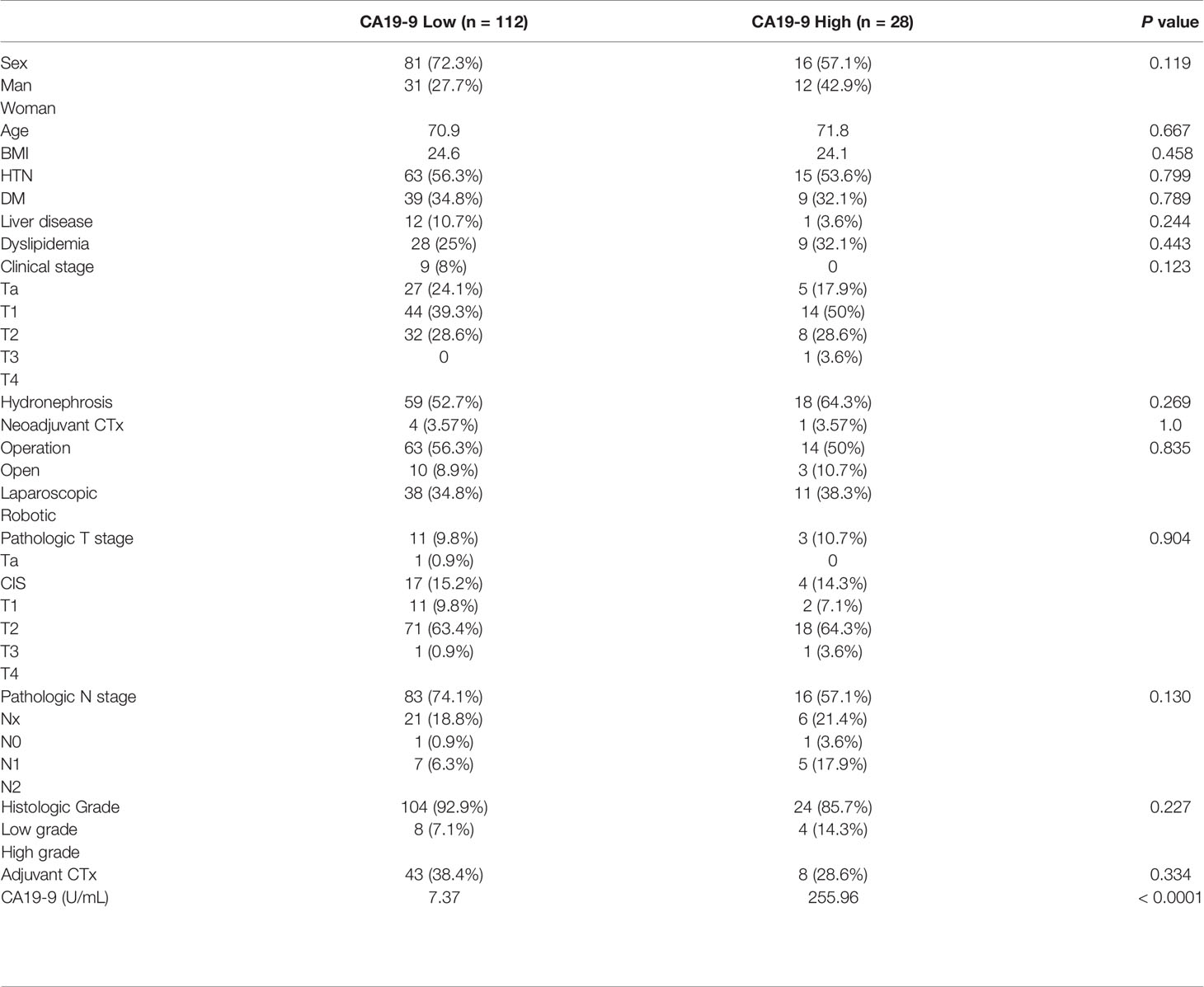
Table 3 Characteristics of propensity score matched patients.
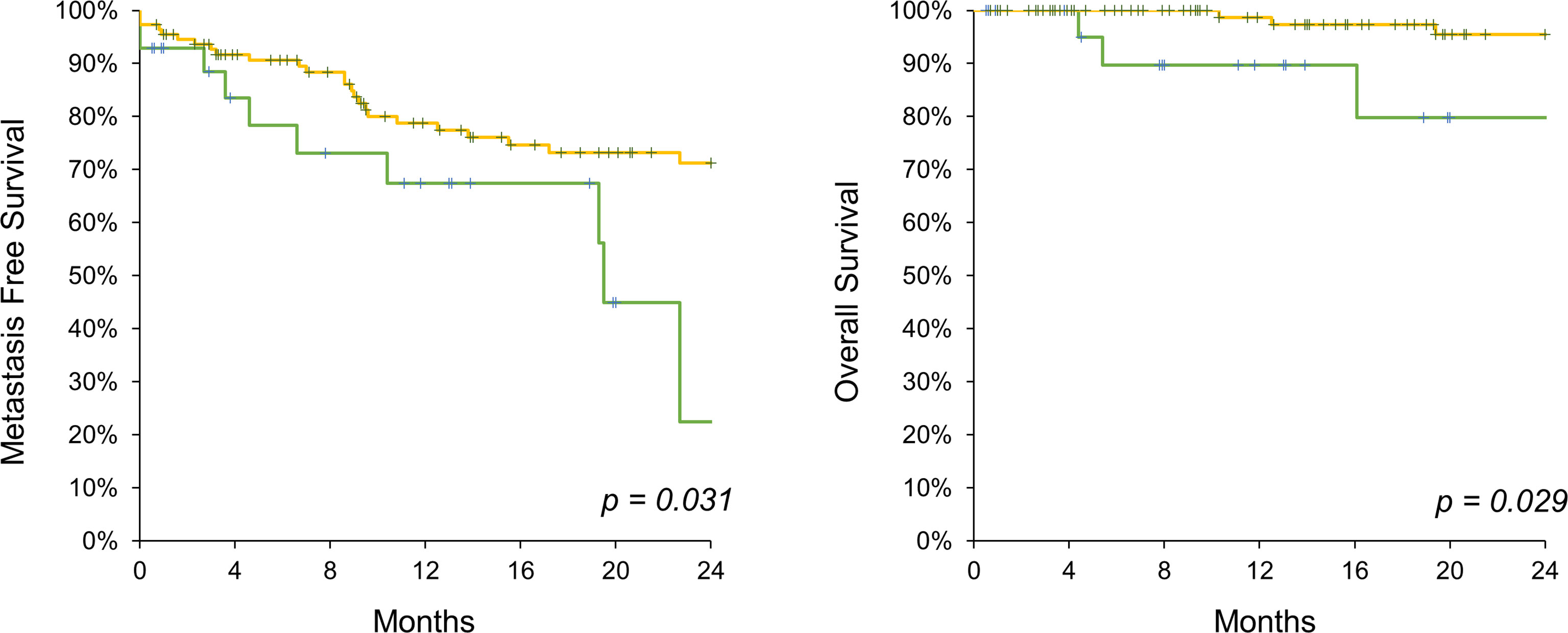
Figure 2 Kaplan-Meier analysis on metastasis free survival (left) and overall survival (right) comparing CA 19-9 high (green line) and low (yellow line) UTUC patients following propensity score matching.
In bladder cancer, CA 19-9 is associated with adverse pathologic stages, characterized by muscular layer invasion and metastasis, thereby leading to poorer survival rates in bladder cancer patients with high CA 19-9 levels (12, 15). Furthermore, accumulating data suggest that urothelial cancers might produce CA19-9 to reflect tumor aggressiveness and tumor burdens (10, 12, 16).
However, there have been no reports evaluating the prognostic value of CA 19-9 for UTUC. In the present study, CA 19-9 was associated with a high tumor burden represented by higher T and N stages, and led to worse outcomes in metastasis-free survival and OS. CA 19-9 is highly expressed in the serum of patients with pancreatic or colon cancer (17). In pancreatic cancer, CA 19-9 is a useful diagnostic and prognostic marker for evaluating the tumor stage, treatment response, and OS. Similar to the study on UTUC, preoperative CA 19-9 levels are associated with tumor resectability and pancreatic cancer stage. A decrease in CA 19-9 levels after surgery reflects favorable survival outcomes, and elevated CA 19-9 levels imply worse survival outcomes (18). In addition, the CA 19-9 level is useful for evaluating disease progression or remission in response to treatment (19, 20). This study investigated only preoperative CA 19-9 levels, but serial measurements following treatment would be valuable in predicting prognostic outcomes. The diagnostic value of CA 19-9 is disappointing because of high false-positive rates in normal conditions and other diseases, such as liver cirrhosis, pancreatitis, and benign gastrointestinal diseases (21). However, in discriminating between benign and malignant pancreatic nodules, it is valuable, with a specificity of 90%.
In this study, PSM analysis was conducted to mitigate adverse features, such as T and N stages, reflecting tumor burden, which is associated with poor outcomes. PSM corrected the imbalance between low- and high-CA 19-9 level groups regarding T and N stages, reflecting tumor burden. Interestingly, after PSM analysis, high CA 19-9 levels indicated worse prognosis, thereby affirming CA 19-9 as an independent prognostic marker, not only based on tumor burden but also its aggressiveness. Similar findings have been reported in pancreatic cancer, providing worse prognosis in multivariate analysis of CA 19-9 level, tumor grade, and tumor size (22). Furthermore, in colorectal cancer, high CA 19-9 levels are related to poor oncologic outcomes, including OS and disease-free survival on PSM analysis (23).
This study is limited by the fact that it had a relatively small sample size and a retrospective study design. However, this report is valuable, considering the low incidence of UTUC with concomitant measurement of CA 19-9 and data queries from a prospective patient enrollment system. Moreover, monitoring CA 19-9 levels may provide preoperative risk classification and facilitate strategic follow-up and adjuvant treatment. Thus, further studies are required to include a larger number of patients and serial follow-up of CA 19-9 in the treatment course.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional review board of Seoul National University Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Conceptualization: S-HJ. Data collection: S-HJ, JH, HY, CJ, HK, JK, CK. Data analysis: S-HJ, HY, JK. Data visualization: S-HJ. Data interpretation: S-HJ, JH, HY, CJ, HK, CK, JK. Manuscript writing: S-HJ. Supervision: S-HJ, HY, JK. All authors contributed to the article and approved the submitted version.
This research was supported by a Basic Science Research Program through National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2018R1D1A1B07041191) and by Seoul National University Hospital (0320202190).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank Editage (www.editage.co.kr) for editing and reviewing this manuscript for English language.
1. Soualhi A, Rammant E, George G, Russell B, Enting D, Nair R, et al. The Incidence and Prevalence of Upper Tract Urothelial Carcinoma: A Systematic Review. BMC Urol (2021) 21:1–11. doi: 10.1186/s12894-021-00876-7
2. Lughezzani G, Sun M, Perrotte P, Shariat SF, Jeldres C, Budäus L, et al. Gender-Related Differences in Patients With Stage I to III Upper Tract Urothelial Carcinoma: Results From the Surveillance, Epidemiology, and End Results Database. Urology (2010) 75:321–7. doi: 10.1016/j.urology.2009.09.048
3. Wang Q, Zhang T, Wu J, Wen J, Tao D, Wan T, et al. Prognosis and Risk Factors of Patients With Upper Urinary Tract Urothelial Carcinoma and Postoperative Recurrence of Bladder Cancer in Central China. BMC Urol (2019) 19:1–8. doi: 10.1186/s12894-019-0457-5
4. Seisen T, Peyronnet B, Dominguez-Escrig JL, Bruins HM, Yuan CY, Babjuk M, et al. Oncologic Outcomes of Kidney-Sparing Surgery Versus Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma: A Systematic Review by the EAU Non-Muscle Invasive Bladder Cancer Guidelines Panel. Eur Urol (2016) 70:1052–68. doi: 10.1016/j.eururo.2016.07.014
5. Leow JJ, Chong YL, Chang SL, Valderrama BP, Powles T, Bellmunt J. Neoadjuvant and Adjuvant Chemotherapy for Upper Tract Urothelial Carcinoma: A 2020 Systematic Review and Meta-Analysis, and Future Perspectives on Systemic Therapy. Eur Urol (2021) 79:635–54. doi: 10.1016/j.eururo.2020.07.003
6. Honda Y, Nakamura Y, Teishima J, Goto K, Higaki T, Narita K, et al. Clinical Staging of Upper Urinary Tract Urothelial Carcinoma for T Staging: Review and Pictorial Essay. Int J Urol (2019) 26:1024–32. doi: 10.1111/iju.14068
7. Gao Y, Wang J, Zhou Y, Sheng S, Qian SY, Huo X. Evaluation of Serum CEA, CA19-9, CA72-4, CA125 and Ferritin as Diagnostic Markers and Factors of Clinical Parameters for Colorectal Cancer. Sci Rep (2018) 8:1–9. doi: 10.1038/s41598-018-21048-y
8. Luo G, Jin K, Deng S, Cheng H, Fan Z, Gong Y, et al. Roles of CA19-9 in Pancreatic Cancer: Biomarker, Predictor and Promoter. Biochim Biophys Acta - Rev Cancer (2021) 1875:188409. doi: 10.1016/j.bbcan.2020.188409
9. Tsai S, George B, Wittmann D, Ritch PS, Krepline AN, Aldakkak M, et al. Importance of Normalization of CA19-9 Levels Following Neoadjuvant Therapy in Patients With Localized Pancreatic Cancer. Ann Surg (2020) 271:740–7. doi: 10.1097/SLA.0000000000003049
10. Pall M, Iqbal J, Singh SK, Rana SV. CA 19-9 as a Serum Marker in Urothelial Carcinoma. Urol Ann (2012) 4:98–101. doi: 10.4103/0974-7796.95555
11. Washino S, Hirai M, Matsuzaki A, Kobayashi Y. Clinical Usefulness of CEA, CA19-9, and CYFRA 21-1 as Tumor Markers for Urothelial Bladder Carcinoma. Urol Int (2011) 87:420–8. doi: 10.1159/000327517
12. Hegele A, Mecklenburg V, Varga Z, Olbert P, Hofmann R, Barth P. CA19.9 and CEA in Transitional Cell Carcinoma of the Bladder: Serological and Immunohistochemical Findings. Anticancer Res (2010) 30:5195–200.
13. Jeong CW, Suh J, Yuk HD, Tae BS, Kim M, Keam B, et al. Establishment of the Seoul National University Prospectively Enrolled Registry for Genitourinary Cancer (SUPER-GUC): A Prospective, Multidisciplinary, Bio-Bank Linked Cohort and Research Platform. Investig Clin Urol (2019) 60:235–43. doi: 10.4111/icu.2019.60.4.235
14. Marrelli D, Caruso S, Pedrazzani C, Neri A, Fernandes E, Marini M, et al. CA19-9 Serum Levels in Obstructive Jaundice: Clinical Value in Benign and Malignant Conditions. Am J Surg (2009) 198:333–9. doi: 10.1016/j.amjsurg.2008.12.031
15. Wang QH, Ji ZG, Chen ZG, Li HZ, Fan H, Fan XR, et al. Serum CA 19-9 as a Good Prognostic Biomarker in Patients With Bladder Cancer. Int J Surg (2015) 15:113–6. doi: 10.1016/j.ijsu.2015.01.031
16. Sashide K, Isobe H, Wakumoto Y, Hanazawa K, Fujita K, Fujime M. CA19-9 as a Serum Marker for Poor Prognosis in Urothelial Carcinoma. Urol Int (2004) 72:112–7. doi: 10.1159/000075963
17. Koprowski H, Herlyn M, Steplewski Z, Sears HF. Specific Antigen in Serum of Patients With Colon Carcinoma. Sci (80- ) (1981) 212:53–5. doi: 10.1126/science.6163212
18. Poruk KE, Gay DZ, Brown K, Mulvihill JD, Boucher KM, Scaife CL, et al. The Clinical Utility of CA 19-9 in Pancreatic Adenocarcinoma: Diagnostic and Prognostic Updates. Curr Mol Med (2013) 13:340–51. doi: 10.2174/156652413805076876
19. Lohrmann C, O’Reilly EM, O’Donoghue JA, Pandit-Taskar N, Carrasquillo JA, Lyashchenko SK, et al. Retooling a Blood-Based Biomarker: Phase I Assessment of the High-Affinity CA19-9 Antibody HuMAB-5B1 for Immuno-PET Imaging of Pancreatic Cancer. Clin Cancer Res (2019) 25:7014–23. doi: 10.1158/1078-0432.CCR-18-3667
20. Azizian A, Rühlmann F, Krause T, Bernhardt M, Jo P, König A, et al. CA19-9 for Detecting Recurrence of Pancreatic Cancer. Sci Rep (2020) 10:1–10. doi: 10.1038/s41598-020-57930-x
21. Kim S, Park BK, Seo JH, Choi J, Choi JW, Lee CK, et al. Carbohydrate Antigen 19-9 Elevation Without Evidence of Malignant or Pancreatobiliary Diseases. Sci Rep (2020) 10:1–9. doi: 10.1038/s41598-020-65720-8
22. Mattiucci GC, Morganti AG, Cellini F, Buwenge M, Casadei R, Farioli A, et al. Prognostic Impact of Presurgical CA19-9 Level in Pancreatic Adenocarcinoma: A Pooled Analysis. Transl Oncol (2019) 12:1–7. doi: 10.1016/j.tranon.2018.08.017
Keywords: CA 19-9, UTUC, prognosis, survival, metastasis
Citation: Jeong S-h, Han JH, Jeong CW, Kim HH, Kwak C, Yuk HD and Ku JH (2022) High Carbohydrate Antigen 19-9 Levels Indicate Poor Prognosis of Upper Tract Urothelial Carcinoma. Front. Oncol. 12:858813. doi: 10.3389/fonc.2022.858813
Received: 20 January 2022; Accepted: 13 June 2022;
Published: 14 July 2022.
Edited by:
Ronald M. Bukowski, Cleveland Clinic, United StatesCopyright © 2022 Jeong, Han, Jeong, Kim, Kwak, Yuk and Ku. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hyeong Dong Yuk, aGluYXl1a0BuYXZlci5jb20=; Ja Hyeon Ku, a3V1cm83MEBzbnUuYWMua3I=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.