 Yanlong Yang
Yanlong Yang Hongbo Zheng2†
Hongbo Zheng2† Longlong Gong
Longlong Gong Bin Lan
Bin Lan
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol. , 19 May 2022
Sec. Thoracic Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.841493
This article is part of the Research Topic New Insights Into Targeting ALK in Patients With Lung Cancer View all 8 articles
Background: Rearrangements of the anaplastic lymphoma kinase (ALK) gene comprise a small subset of non-small cell lung cancer (NSCLC). Patients with NSCLC harboring ALK fusion proteins are sensitive to ALK tyrosine kinase inhibitors (TKIs). Various fusion partners of ALK are being discovered with the application of next-generation sequencing (NGS).
Case presentation: Here, we report a female patient with metastatic lung adenocarcinoma harboring LMO7-ALK (L15, A20) rearrangement revealed by NGS. The patient received crizotinib as first-line treatment and has achieved partial response with a progression-free survival over 1 year.
Conclusions: We firstly found that the satisfactory response to crizotinib verified the oncogenic activity of LMO7-ALK fusion. Great progression and wide application of NGS facilitate the findings of rare fusion types.
The identification of driver genes including EGFR mutation and ALK rearrangements greatly promotes the precise therapy for non-small cell lung cancer (NSCLC). With the development of sequencing technology, molecular genotyping has been gradually conducted as a clinical routine to determine the therapeutic regimen. Meanwhile, novel mutations are being identified, providing more treatment opportunities for patients.
ALK is a receptor tyrosine kinase, and its rearrangements occur in about 3%–7% of patients with NSCLC (1). Until now, more than 90 fusion types of ALK have been reported (2), including EML4, KIF5B, KLC1, STRN, TFG, TPM, PPP4R3, GTF2IRD1, VCL, and DCTNA (3–8). The ALK fusion proteins produced by gene arrangements have aberrant kinase activity and promote proliferation and survival of cancer cells through downstream pathways such as RAS-ERK and PI3K-AKT (9). With the access of ALK inhibitors, long-term survival has been realized in patients with advanced NSCLC harboring ALK fusions, with a response rate (RR) of over 80% and a 5-year OS higher than 60% (10, 11).
LMO7-ALK fusion was also reported by previous studies. Ka-Won Noh et al. reported that LMO7-ALK (L15, A20) as a novel ALK fusion was discovered in NSCLC (12). Mengnan Li et al. found that an NSCLC patient with LMO7-ALK (L16, A20) benefited from a second-line ensartinib treatment (13). Here, we report an LMO7-ALK (L15, A20) fusion in a patient with stage IV lung adenocarcinoma who had favorable and durable response to crizotinib treatment.
A 33-year-old woman who had never smoked presented to our hospital with hoarseness in June 2020. There was a family history as her mother died of lung cancer. Positron emission tomography/computed tomography (PET/CT) showed a hypermetabolic mass in the middle lobe of the right lung with metastases of hilar and mediastinal lymph nodes, right supraclavicular lymph nodes, and right ilium (T1cN3M1c, stage IVB, Figure 1A). A biopsy through a fiber bronchoscope was performed and pathology revealed adenocarcinoma. Immunohistochemical (IHC) staining indicated positive TTF-1, Napsin A, and CK7, and negative P40 and CK5/6. Formalin-fixed paraffin-embedded (FFPE) tumor samples were assessed by DNA next-generation sequencing (NGS, 122 gene panel, Genecast Biotechnology Co., Ltd.) and RNA NGS (29-gene panel, Genecast Biotechnology Co., Ltd.). The results of DNA and RNA sequencing identified an LMO7-ALK (L15, A20) fusion in the patient. The breakpoints of the two genes were chromosome 2 (29446313–29446354) and LMO7 chromosome 13 (76407282-76407322; Figures 2A, B).
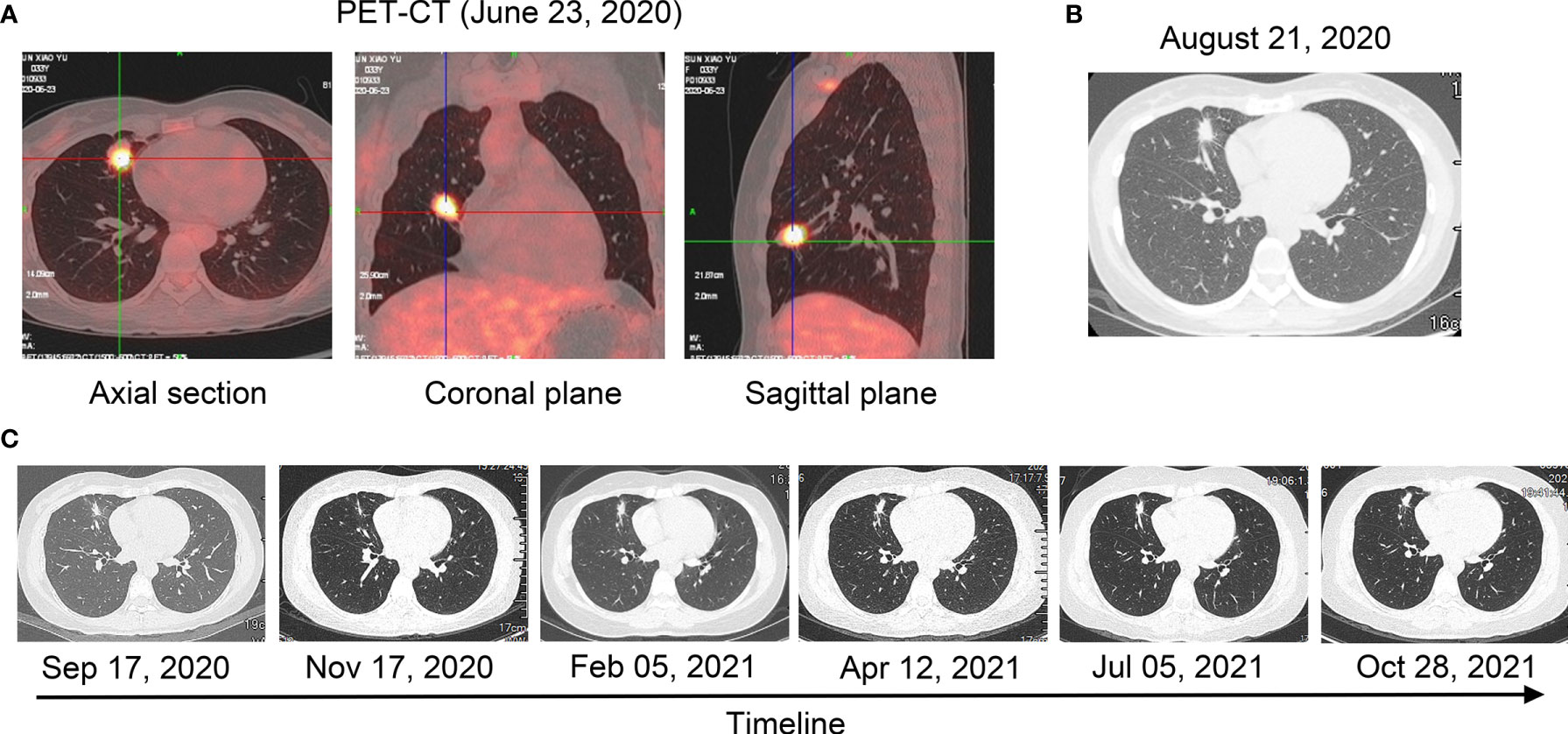
Figure 1 Radiological examinations during the treatment course. (A) PET/CT scan before treatment (23 June 2020). (B) A computer tomography scan after treatment with crizotinib for 6 weeks (21 August 2020). (C) A computer tomography scan after treatment with crizotinib from 17 September 2020 to 28 October 2021.
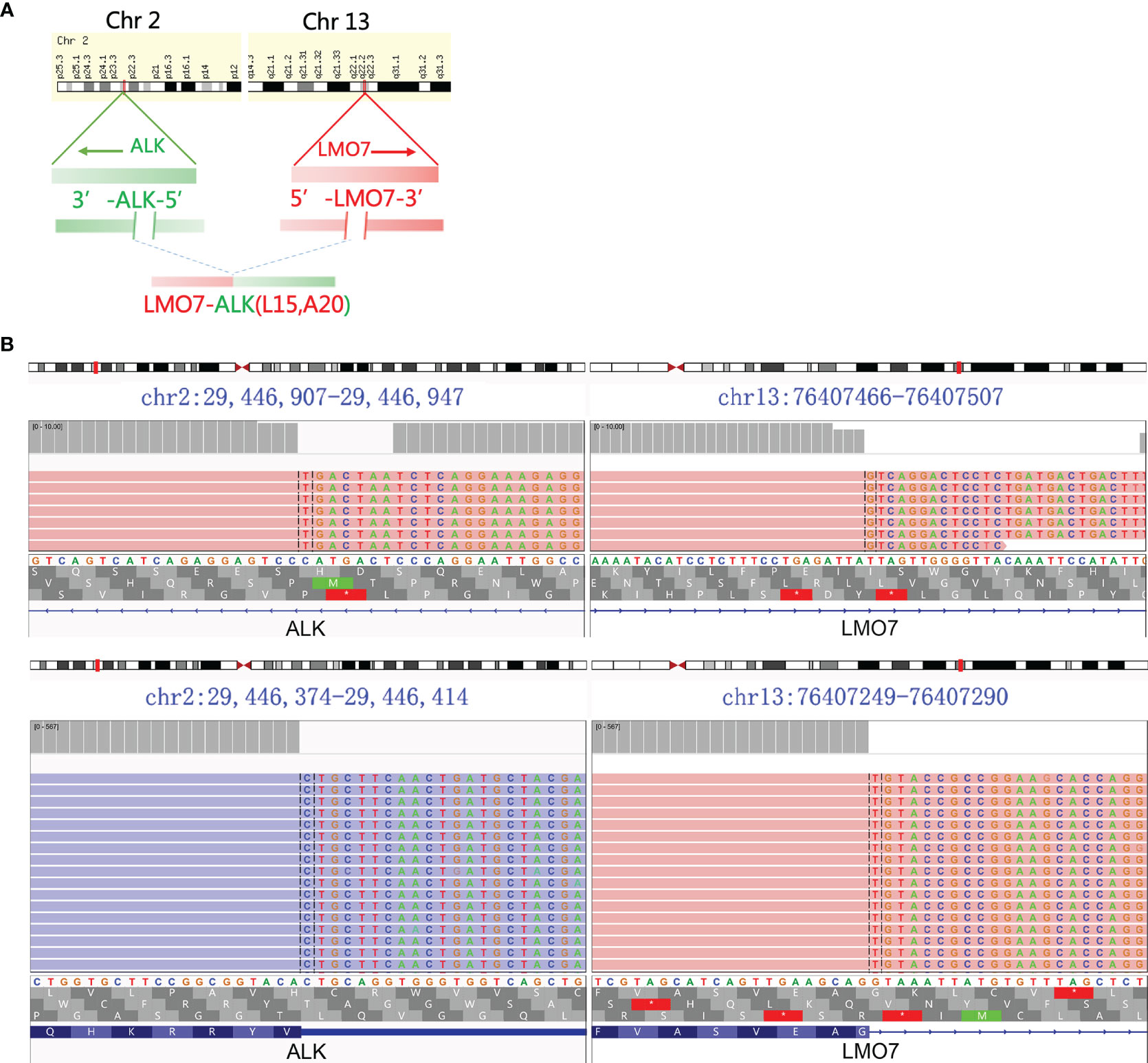
Figure 2 ALK fusion was detected using NGS. (A) Schematic representation of LMO7-ALK (L15, A20). (B) LMO7-ALK (L15, A20) fusion demonstrated by Integrative Genomics Viewed program.
The patient started to receive crizotinib (250 mg, twice a day) on 9 July 2020. After 6 weeks, the CT scan demonstrated reduced tumor size and smaller subcarinal lymph nodes (17 × 12 × 12 mm) compared with the previous examination, and evaluation of therapeutic efficiency indicated partial response (PR, −34.2%) (Figure 1B). A CT scan on 17 September 2020 showed stable disease (SD, −12%) and smaller subcarinal lymph nodes (12 × 10 × 10 mm) (Figure 1C). Follow-up CT scans showed SD (0%) and sizes of subcarinal lymph nodes were almost unchanged until October 2021 (Figure 1C). We conducted ctDNA analysis using DNA NGS (122-gene panel, Genecast Biotechnology Co., Ltd.) with peripheral blood in May 2021, while LMO7-ALK rearrangement was not detected. The PFS for the patients has exceeded 1 year.
This is the report of LMO7-ALK (L15, A20) fusion in NSCLC. The LMO7 (LIM-domain only protein 7) gene is located on chromosome 13q22 while ALK is located on chromosome 2p23 (genecard.org). The fusion transcript was generated by the fusion of LMO7 exon 15 and ALK exon 20. In a previous report, LMO7-BRAF (L6, B9) rearrangement was found in papillary thyroid carcinoma. The fusion protein stimulated ERK1/2 phosphorylation and promoted cell growth in a pattern similar to BRAF (14). This demonstrated that LMO7 may be a functional fusion partner for kinases. The cytoplasmic domain of ALK is encoded by exons 17–26, and the most reported breakpoint of ALK is exon 20 (1). All the functional arrangements are the combination of the 5’-end of the fusion partner and 3’-end of ALK, retaining the entire kinase domain of ALK for activity (15). In our case, the breakpoint of ALK is exon 20 without exception, indicating the retention of the entire kinase domain of ALK, and the fusion protein is likely to be generated from inter-chromosomal arrangement similar to TFG-ALK and KIF5B-ALK (1). The fusion protein of LMO7 to ALK is able to drive carcinogenesis and is considered to behave as an oncogenic alteration that displays a favorable response to crizotinib. The repetitive NGS revealed that the LMO7-ALK fusion is cleared in plasma, which was in accordance with the control of disease.
In previous studies, different ALK fusion variants might have different properties. The short forms of EML4-ALK have later stage and poorer prognosis than the long forms (12, 16), while different fusion partners affect drug sensitivity to ALK TKIs (14). The influences of LMO7 on the intrinsic properties of the fusion protein are still unknown. The patient’s exact response to crizotinib and other ALK TKIs, and possible resistance mechanisms need to be followed up.
An increasing number of novel gene fusions are identified with NGS development and application. DNA and RNA NGSs of tumor tissue samples have been widely used (17). In previous gene detection, gene variations of the tumor tissue from the NSCLC patient were assessed using a DNA NGS and the LMO7-ALK fusion was found. To further verify the result, the RNA NGS of the sample was used and the result was consistent with the DNA NGS. With improving DNA sequencing depth and accuracy, ctDNA sequencing is increasingly applied in gene variation detection (18–20), such as gene fusion, single-nucleotide variations, and copy number variation. Owing to tumor tissue disappearance, LMO7-ALK fusion detection using ctDNA sequencing suggested that there was no tumor cell. In the case, application of DNA and RNA NGS of tumor tissues and ctDNA NGS dynamically revealed variation information of the tumor, which provided precise direction for tumor therapy.
There are limitations for this case. We only confirm that the NSCLC case with LMO7-ALK fusion benefitted from crizotinib therapy. The upstream and downstream molecules in this signaling pathway should also be further illustrated.
In conclusion, LMO7-ALK fusion was verified by the effective treatment of crizotinib in an NSCLC case.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
YY, HZ, and LZ provided the case and drafted the manuscript. YY and LG analyzed data. SS, LG, and ZL reviewed and amended the manuscript. HZ, LG, and BL amended and designed the manuscript. All authors contributed to the article and approved the submitted version.
Authors HZ and LG were employed by Genecast Biotechnology Co., Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the patient and their family for agreeing to publish the report.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.841493/full#supplementary-material
1. Shaw AT, Hsu PP, Awad MM, Engelman JA. Tyrosine Kinase Gene Rearrangements in Epithelial Malignancies. Nat Rev Cancer (2013) 13(11):772–87. doi: 10.1038/nrc3612
2. Ou SI, Zhu VW, Nagasaka M. Catalog of 5' Fusion Partners in Alk-Positive Nsclc Circa 2020. JTO Clin Res Rep (2020) 1(1):100015. doi: 10.1016/j.jtocrr.2020.100015
3. Soda M, Choi YL, Enomoto M, Takada S, Yamashita Y, Ishikawa S, et al. Identification of the Transforming Eml4-Alk Fusion Gene in Non-Small-Cell Lung Cancer. Nature (2007) 448(7153):561–6. doi: 10.1038/nature05945
4. Takeuchi K, Choi YL, Togashi Y, Soda M, Hatano S, Inamura K, et al. Kif5b-Alk, a Novel Fusion Oncokinase Identified by an Immunohistochemistry-Based Diagnostic System for Alk-Positive Lung Cancer. Clin Cancer Res (2009) 15(9):3143–9. doi: 10.1158/1078-0432.CCR-08-3248
5. Togashi Y, Soda M, Sakata S, Sugawara E, Hatano S, Asaka R, et al. Klc1-Alk: A Novel Fusion in Lung Cancer Identified Using a Formalin-Fixed Paraffin-Embedded Tissue Only. PLoS One (2012) 7(2):e31323. doi: 10.1371/journal.pone.0031323
6. Majewski IJ, Mittempergher L, Davidson NM, Bosma A, Willems SM, Horlings HM, et al. Identification of Recurrent Fgfr3 Fusion Genes in Lung Cancer Through Kinome-Centred Rna Sequencing. J Pathol (2013) 230(3):270–6. doi: 10.1002/path.4209
7. Rikova K, Guo A, Zeng Q, Possemato A, Yu J, Haack H, et al. Global Survey of Phosphotyrosine Signaling Identifies Oncogenic Kinases in Lung Cancer. Cell (2007) 131(6):1190–203. doi: 10.1016/j.cell.2007.11.025
8. Schram AM, Chang MT, Jonsson P, Drilon A. Fusions in Solid Tumours: Diagnostic Strategies, Targeted Therapy, and Acquired Resistance. Nat Rev Clin Oncol (2017) 14(12):735–48. doi: 10.1038/nrclinonc.2017.127
9. Chiarle R, Voena C, Ambrogio C, Piva R, Inghirami G. The Anaplastic Lymphoma Kinase in the Pathogenesis of Cancer. Nat Rev Cancer (2008) 8(1):11–23. doi: 10.1038/nrc2291
10. Peters S, Camidge DR, Shaw AT, Gadgeel S, Ahn JS, Kim DW, et al. Alectinib Versus Crizotinib in Untreated Alk-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2017) 377(9):829–38. doi: 10.1056/NEJMoa1704795
11. Mok T, Camidge DR, Gadgeel SM, Rosell R, Dziadziuszko R, Kim DW, et al. Updated Overall Survival and Final Progression-Free Survival Data for Patients With Treatment-Naive Advanced Alk-Positive Non-Small-Cell Lung Cancer in the Alex Study. Ann Oncol (2020) 31(8):1056–64. doi: 10.1016/j.annonc.2020.04.478
12. Noh KW, Lee MS, Lee SE, Song JY, Shin HT, Kim YJ, et al. Molecular Breakdown: A Comprehensive View of Anaplastic Lymphoma Kinase (Alk)-Rearranged Non-Small Cell Lung Cancer. J Pathol (2017) 243(3):307–19. doi: 10.1002/path.4950
13. Li M, An Z, Tang Q, Ma Y, Yan J, Chen S, et al. Mixed Responses to First-Line Alectinib in Non-Small Cell Lung Cancer Patients With Rare Alk Gene Fusions: A Case Series and Literature Review. J Cell Mol Med (2021) 25(19):9476–81. doi: 10.1111/jcmm.16897
14. He H, Li W, Yan P, Bundschuh R, Killian JA, Labanowska J, et al. Identification of a Recurrent Lmo7-Braf Fusion in Papillary Thyroid Carcinoma. Thyroid (2018) 28(6):748–54. doi: 10.1089/thy.2017.0258
15. Childress MA, Himmelberg SM, Chen H, Deng W, Davies MA, Lovly CM. Alk Fusion Partners Impact Response to Alk Inhibition: Differential Effects on Sensitivity, Cellular Phenotypes, and Biochemical Properties. Mol Cancer Res (2018) 16(11):1724–36. doi: 10.1158/1541-7786.MCR-18-0171
16. Christopoulos P, Kirchner M, Endris V, Stenzinger A, Thomas M. Eml4-Alk V3, Treatment Resistance, and Survival: Refining the Diagnosis of Alk(+) Nsclc. J Thorac Dis (2018) 10(Suppl 17):S1989–91. doi: 10.21037/jtd.2018.05.61
17. Izumi H, Matsumoto S, Liu J, Tanaka K, Mori S, Hayashi K, et al. The Clip1-Ltk Fusion Is an Oncogenic Driver in Non-Small-Cell Lung Cancer. Nature (2021) 600(7888):319–23. doi: 10.1038/s41586-021-04135-5
18. Dagogo-Jack I, Brannon AR, Ferris LA, Campbell CD, Lin JJ, Schultz KR, et al. Tracking the Evolution of Resistance to Alk Tyrosine Kinase Inhibitors Through Longitudinal Analysis of Circulating Tumor DNA. JCO Precis Oncol (2018) 2:1–14. doi: 10.1200/PO.17.00160
19. McCoach CE, Blakely CM, Banks KC, Levy B, Chue BM, Raymond VM, et al. Clinical Utility of Cell-Free DNA for the Detection of Alk Fusions and Genomic Mechanisms of Alk Inhibitor Resistance in Non-Small Cell Lung Cancer. Clin Cancer Res (2018) 24(12):2758–70. doi: 10.1158/1078-0432.CCR-17-2588
Keywords: LMO7-ALK fusion, crizotinib, NSCLC, case report, LUAD
Citation: Yang Y, Zheng H, Li Z, Shi S, Zhong L, Gong L and Lan B (2022) LMO7-ALK Fusion in a Lung Adenocarcinoma Patient With Crizotinib: A Case Report. Front. Oncol. 12:841493. doi: 10.3389/fonc.2022.841493
Received: 22 December 2021; Accepted: 18 March 2022;
Published: 19 May 2022.
Edited by:
Petros Christopoulos, Heidelberg University Hospital, GermanyReviewed by:
Haruhiko Sugimura, Hamamatsu University School of Medicine, JapanCopyright © 2022 Yang, Zheng, Li, Shi, Zhong, Gong and Lan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Longlong Gong, Z29uZy5sb25nbG9uZ0BnZW5lY2FzdC5jb20uY24=; Bin Lan, c3RsYW5iaW5AMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.