 Weiqi Li
Weiqi Li Simin Wang2
Simin Wang2 Yuhan He
Yuhan He Li Lin
Li Lin
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol. , 09 August 2022
Sec. Genitourinary Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.697399
Objectives: The objective of the present work was to conduct a systematic review and meta-analysis to assess the association between periodontal disease (PD) and urogenital cancer (UC) risk.
Materials and methods: An electronic search in PubMed, EMBASE, the Cochrane Library, and Web of Science was conducted using MeSH terms to identify cohort studies published before May 17, 2022. Cohort studies examining the association between PD and UC risk were included. We used a random-effects model to summarize the effect sizes with 95% confidence intervals (CIs) of the included studies with PD as the indicator and UC as the outcome.
Results: Eleven cohort studies met the inclusion criteria. Our results suggest that PD patients increases the risk of UC by 1.24-fold (hazard ratio (HR), 1.24; 95% CI, 1.17-1.31; I2, 22.4%). The strength of the sensitivity analysis and cumulative meta-analysis confirmed the reliability of the results.
Conclusion: We found that PD is a potential risk factor for UC. Our results indicate that along with the decrease in the incidence of PD,PD treatment may help prevent UC. We hope that our study will raise awareness of periodontal health, thereby reducing the incidence of UC.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42021244405.
Urogenital cancer (UC) is a general term for cancers of the urogenital system. These include uterine cancer, ovarian cancer, prostate cancer UC and other male and female genital cancers, as well as kidney cancer, bladder cancer and other urologic cancers (1, 2). Cancer of the urogenital system is widely considered due to its high incidence and mortality (3–7). Due to the special function and location of the urogenital, the treatment of cancer often brings great trouble to patients’ lives (4, 8, 9). How to recognize UC and prevent its development and occurrence have become vital issues, and increasing research is focusing on how to prevent risk factors for UC (10–12). A large amount of evidence has confirmed that chronic inflammation may also be a risk factor for UC (13–18).
Periodontal disease (PD)is a common disease often manifests as chronic inflammation that compromises the integrity of periodontal tissues and other tooth-supporting tissues could cause loose teeth and tooth loss, including periodontitis, gingival disease and developmental and acquired deformities and conditions affecting the periodontium (19). PD not only causes a heavy economic burden but also greatly reduces the quality of life of patients (20, 21). From 2009 to 2012, 46% of American adults had periodontitis, and 8.9% had severe periodontitis (22). A variety of systemic diseases and conditions can affect the course of periodontitis or have a negative impact on the periodontal attachment apparatus, PD also affects overall health (23). Close associations of atherosclerosis and rheumatoid arthritis with PD have been widely reported (24–28). Whether PD is a risk factor for cancer has also become a hot topic. Studies have shown that PD increases the risk of pancreatic cancer and breast cancer (29, 30), and PD has been recognized as a risk indicator for gastrointestinal cancer (31). Persistent periodontal infection can lead to the spread of periodontal pathogens to many parts of the body, and the colonization of oral bacteria is closely related to the occurrence and development of cancer in many body parts, including the urogenital system (32–35). Periodontitis may lead to low-grade systemic inflammation and consequently could be associated with UC.
Existing evidence indicates that there may be a correlation between PD and the risk of UC, but the results of epidemiological studies on the correlation between the two are inconsistent (36–46). Considering that no systematic study has summarized the epidemiological results of the effects of PD on UC risk, the objective of the present work was to conduct a systematic review and meta-analysis to assess the association between periodontal disease (PD) and urogenital cancer (UC) risk.
Our meta-analysis was conducted and reported according to the PRISMA 2020 statement (47). The protocol for this systematic review was registered on PROSPERO (CRD42021244405).
Population: Adults; Indicator: Patients with PD; Comparison: Adults without a history of PD; Outcomes: The relationship between PD and UC risk with adjusted effect sizes (odds ratios (ORs)/relative risks (RRs)/hazard ratios (HRs)) and 95% confidence intervals (95% CIs); Study design: Cohort study.
PD diagnoses based on questionnaires, clinical periodontal examinations and radiographic examinations or other credible forms of medical records are acceptable. The diagnosis of UC is accepted in the form of medical records, pathological diagnosis records, and records from the cancer registry.
No full-text article available; Not published in an English-language peer-reviewed journal or studies not written in English; Investigation of tooth loss rather than PD.
A systematic search of the PubMed, EMBASE, Web of Science, and Cochrane Library electronic databases was conducted up to May 17, 2022, to identify research on the correlation between PD and UC risk. We used Medical Subject Headings (MeSH) terms for document retrieval. PD MeSH included periodontal disease, periodontitis, gingivitis, peri-implantitis etc. UC MeSH included Urogenital Neoplasms, Genital Neoplasms, Uterine Neoplasms etc. Details of the complete search strategy can be found in Appendix Table 1.
Articles published by Journal of Clinical Periodontology and Journal of Periodontology from Jan 1,2000 to May 17, 2022, were reviewed. All references of the systematic reviews evaluating the relationship between PD and cancer risk were manually searched (30, 48–54).
If data from multiple studies were derived from the same cohort, we selected the most representative study for data extraction based on follow-up time and data integrity. Two authors independently screened each record and each report retrieved used Endnote (version 20.0.0), if a disagreement occurred, a decision was made through consultation with the third author.
The information and data we extracted from the included studies were as follows: study identification (first author’s last name and published year), study design (cohort design and period), sample (sample characteristics, cohort population and country), length/age (the length of average follow-up durations and the included age of participants), gender, cohort (total number of participants), event (number of UC patients), PD diagnosis, UC diagnosis (diagnosis and the code of International Classification of Diseases), outcomes (incidence or mortality), UC types and periodontal status, effect sizes and their 95% CIs, and adjustment variables. The extracted data are shown in Tables 1, 2.
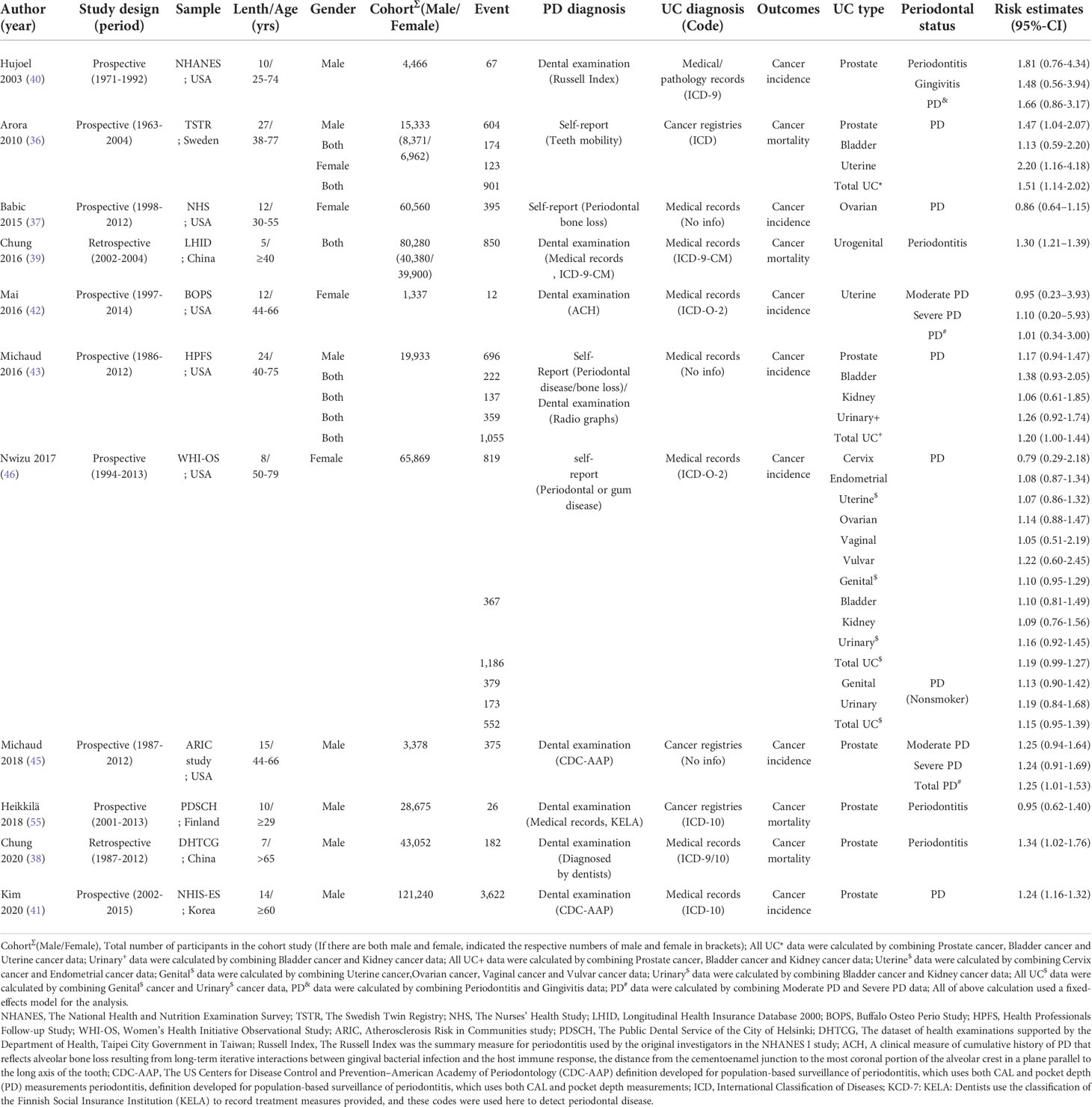
Table 1 Characteristics and quality assessments of the included studies.
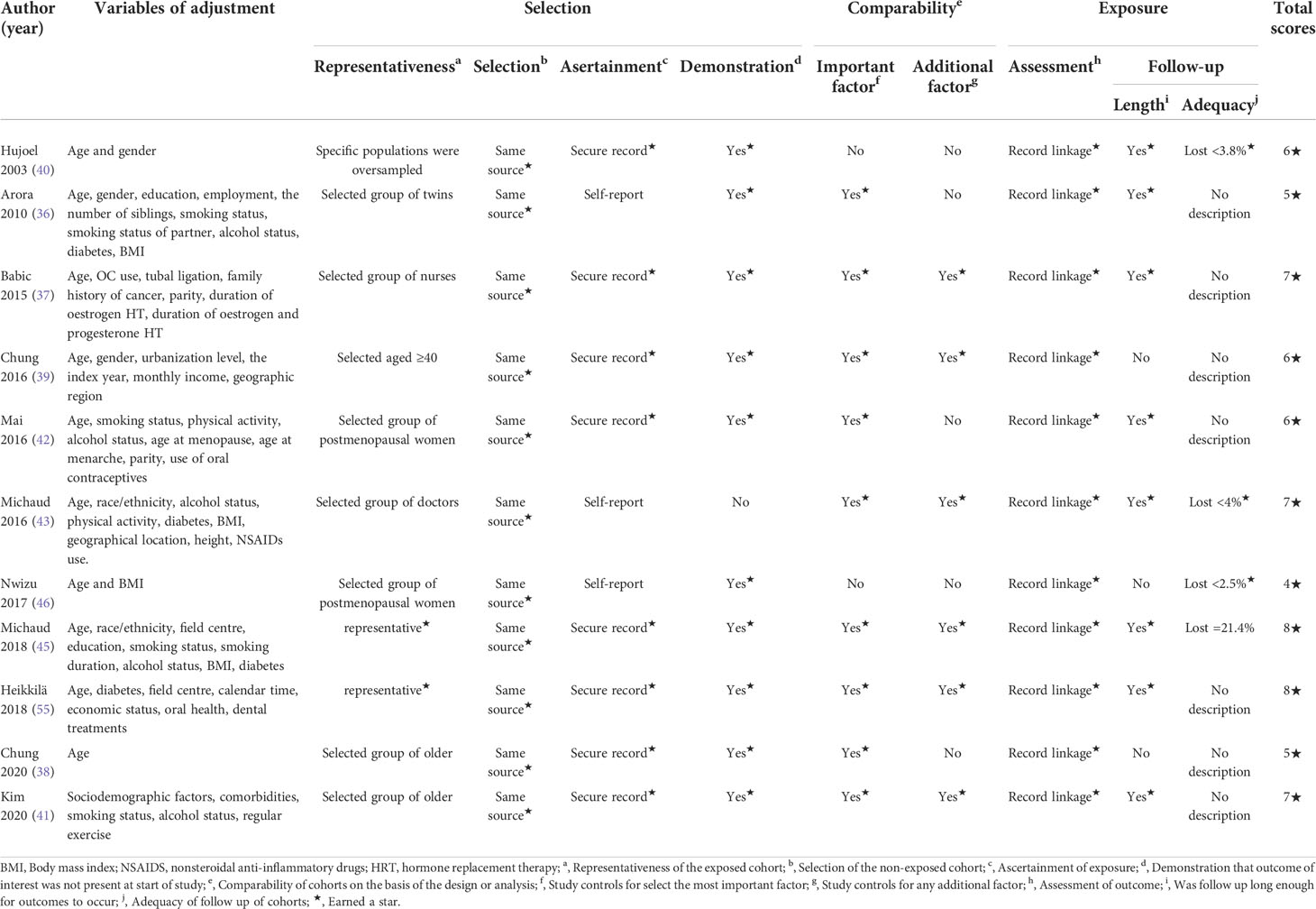
Table 2 The adjusted variables and Newcastle-Ottawa quality assessment scale for cohort studies.
The Newcastle-Ottawa scale (NOS) (28) is widely used to assess the quality of literature in cohort studies. It is based on the semiquantitative principle of a star system, with a total score of nine stars. Studies with 0-3 stars are considered low-quality research with low reliability, while studies with 4-6 stars and 7-9 stars are considered medium- and high-quality research with relatively high reliability.
Considering the small number of studies included, Egger’s test and the trim-and-fill method were carried out to detect publication bias. The trim-and-fill method is a non-parametric statistical method used to estimate the number of missing studies and to assess and correct for publication bias (56).
Since the probability of UC occurrence is very low and all the included studies were observational cohort studies, ORs and RRs were regarded as HRs in our analysis (57, 58). In this meta-analysis, we chose HR as the common correlation measure across studies. The effect sizes and CIs provided by all studies were adjusted for some confounding factors, details could be found in Table 2. Due to different PD diagnoses, UC types and other factors, there was significant clinical heterogeneity. We selected the random-effects model to incorporate the effect sizes and their 95% CIs into the study. Some studies classified PD according to severity. We divided the data according to severity into two groups: Moderate PD (gingivitis) and Severe PD (periodontitis), other studies without classification were pulled into Total PD group. Studies includes multiple sites for UC or studies only overall UC data without subdivision of organs are provided were pulled into total UC group. To improve the reliability of the results, for studies that provided only the respective effect sizes and CIs for different UC types or PD severities but did not provide the total effect size and CI, we combined the data provided using a fixed-effect model to obtain the effect size and CI for total UC and total PD (30). The I² statistic was used to measure the degree of heterogeneity in the meta-analysis (59). We analysed the origin of heterogeneity through subgroup analyses and meta-regressions according to UC types, periodontal status, follow-up duration, study design, outcomes, sex, smoking status, risk of bias and location. The regression coefficient estimates the difference between the intervention effect in each subgroup and a nominated reference subgroup, and the P value of the regression coefficient indicates the presence of statistical significance (48). We excluded one study at a time and then applied the random-effects model to perform a sensitivity analysis of the data to evaluate the robustness of the results. We conducted a cumulative meta-analysis in chronological order to observe the changes in the results over time. Two authors completed the data extraction and analyses; and used the ‘meta’ package in the statistical software R (version 4.0.0) to independently perform all statistical analyses. If a disagreement occurred, a decision was made through consultation with the third author.
Referring to the guidelines (60), we grouped different types of UC into groups for narrative synthesis. With reference to the WHO classification of cancers of the urogenital system. The three types of cancer are further subdivided according to the sources. Female genital cancer includes uterine cancer, ovarian cancer, vaginal cancer and vulvar cancer; male genital cancer is mainly prostate cancer; urologic cancers is divided into kidney cancer and bladder cancer.
Our initial search strategy identified 1,334 records, including 1,324 items retrieved from the databases and 10 items retrieved manually. After removing 182 duplicate studies, the authors confidently scanned the titles and abstracts of 1,152 studies, and 991 studies not reporting an association between PD and UC risk were excluded. 59 articles met the criteria for full-text assessment, and after reading the full texts, 41 records were excluded according to the eligibility criteria. Finally, 11 eligible studies were included in our analysis. Figure 1 shows the search flowchart. The reasons for record exclusion after reading topics and abstracts or the full texts Details can be found in Appendix Tables 2, 3.
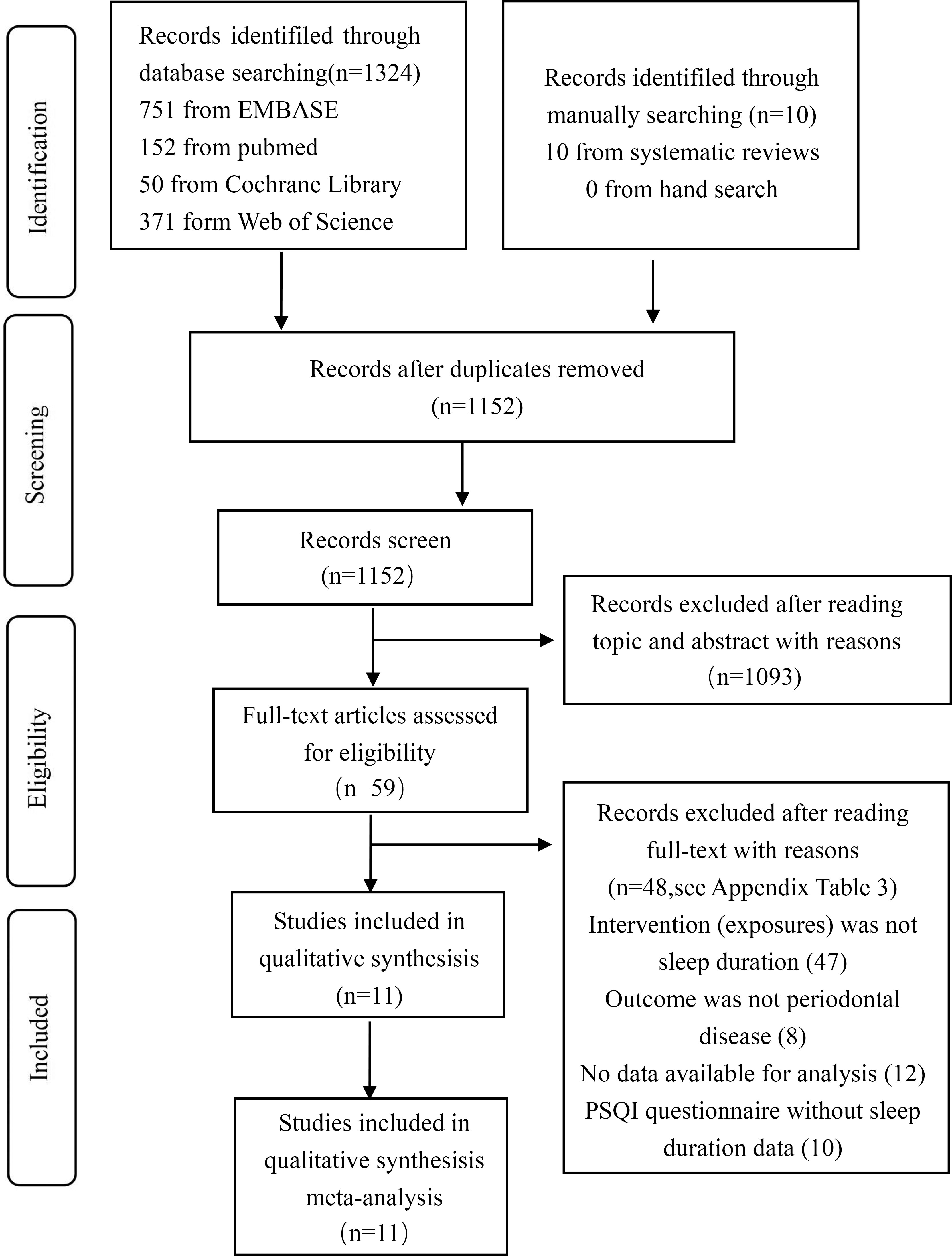
Figure 1 The result of search flowchart.
The included cohort studies were published between 2003 and 2020 by researchers in the United States, Sweden, Finland, South Korea and China. Eleven cohort studies involving 444,123 participants and 7,485 UC patients met the inclusion criteria. The follow-up durations in the included studies ranged from 5 to 27 years. The maximum number of participants in the cohort studies was 121,240, and the minimum number was 1,337. All included studies had a quality score between 4 and 8 stars. Six medium-quality and five high-quality studies were included. Tables 1, 2 list the details of each study. Table 2 shows the complete NOS quality assessment results.
Of the 11 studies, only 2 studies established a diagnosis of PD based on participants’ self-reports (36, 46), and the other 9 provided clear diagnostic criteria (37–43, 45, 55). The diagnosis of UC in four studies was derived from death data from cancer registries (36, 38, 39, 55), and the remaining seven studies were derived from clinical diagnosis in medical records (37, 40–43, 45, 46). Eight studies provided ICD codes for cancer diagnosis (36, 38–42, 46, 55), while the remaining three did not (37, 43, 45).
Except for one study that adjusted only for age (38), the remaining studies adjusted for multiple confounding factors. Four studies adjusted for smoking status, five for alcohol status (36, 41–43, 45), four for diabetes status (36, 43, 45, 55), three for sex (36, 39, 40) and four for body mass index (36, 43, 45, 46). Other adjusted factors included employment (36), the number of siblings (36), physical activity (42), comorbidities (41), regular exercise and sociodemographic factors (41). Details of the variables for which the analyses were adjusted can be found in Table 2.
Of the 11 studies, 4 studies provided the overall effect value of PD and UC risk and its 95% CI, and four other studies investigated the relationship between PD and female genital cancer. We included seven items about male genital cancer and 3 studies that provided data on urologic cancers. We combined data from different studies through random effects models and analysed these data through subgroup analysis and meta regression. See Table 3 for specific data, and the specific studies and data of each group are shown in Appendix Table 5.
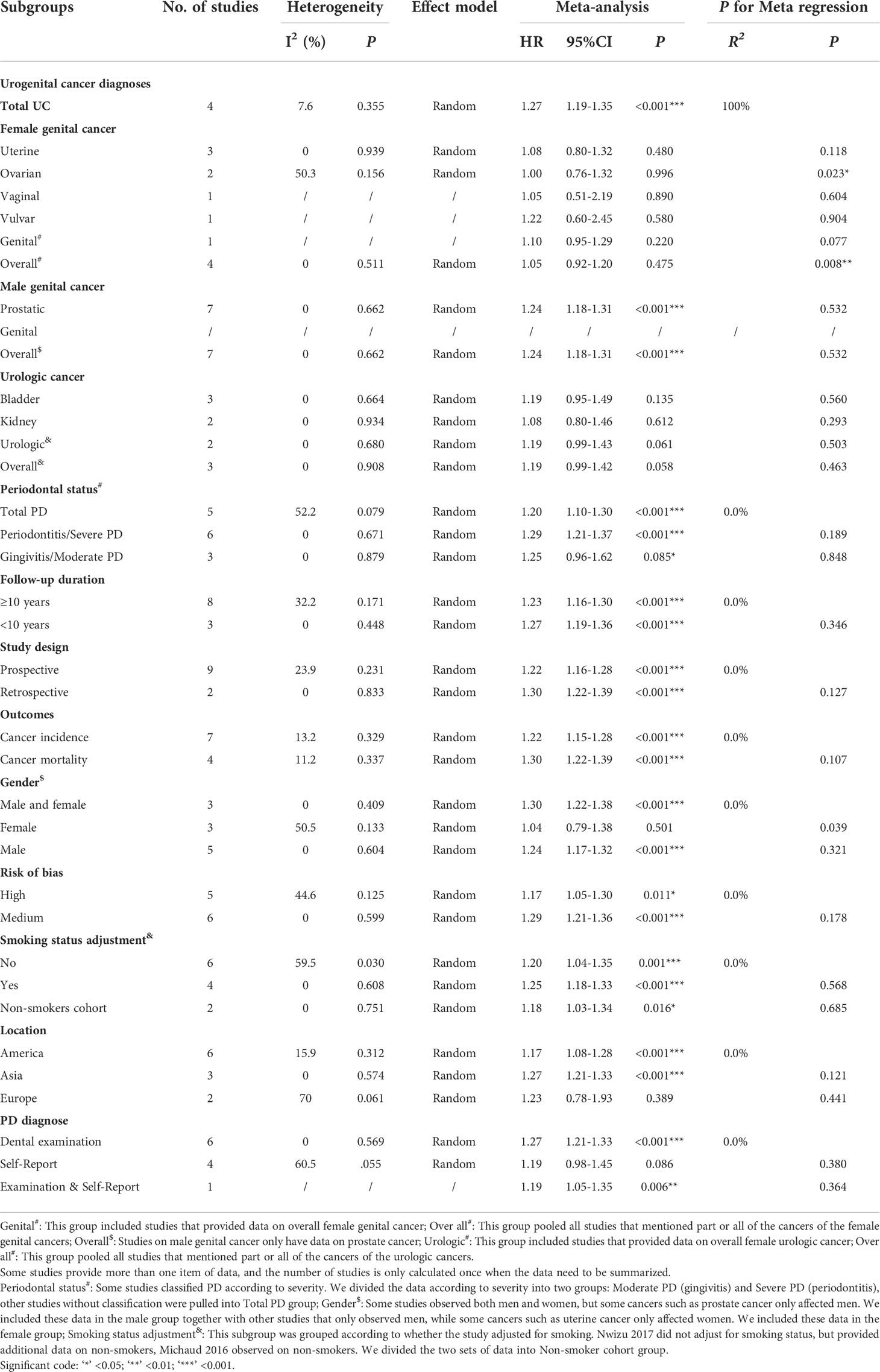
Table 3 Results of subgroup analyses and meta-regression.
Among the four studies, three studies provided cancer data in multiple kinds of urogenital (36, 43, 46). We combined them using a fixed-effect model to obtain UC data. Another study directly provided the overall UC data (39). Two studies involving both males and females found that PD and UC risk were closely related, with significant differences (Arora 2010, HR, 1.51; Chung 2016, HR, 1.30) (36, 39). Another study involved both sexes (Michaud 2016, HR, 1.20) (43), and the study only investigated females (Nuwizu 2017, HR, 1.19) (46) indicated that PD increased the risk of UC, but their results were not significant.
Four studies were included in this section: three mentioned uterine cancer (Arora 2010, HR, 1.20; Mai 2016, HR, 1.01; Nuwizu 2017, HR, 1.07) (36, 42, 46), two involved ovarian cancer (Babic 2015, HR, 0.86; Nuwizu 2017, HR, 1.14) (37, 46) and one study mentioned vaginal cancer (Nuwizu 2017, HR, 1.05) (46) and vulvar cancer (Nuwizu 2017, HR, 1.22). In addition, another study provided overall data on female genital cancer (Nuwizu 2017, HR, 1.10). All the results were not significant.
Seven studies mentioned that data on male genital cancer are all focused on prostate cancer. Four of the studies found that patients with PD were more likely to develop prostate cancer (Arora 2010, HR, 1.47; Michaud 2018, HR, 1.25; Chung 2016, HR, 1.34; Kim 2020, HR, 1.24) (36, 39, 41, 45). The other three studies did not find a significant association (Hujoel 2003, HR, 1.66; Michaud 2016, HR, 1.17; Heikkilä 2018, HR, 0.95) (40, 43, 55).
Research on urologic cancers focuses on bladder cancer and Kidney cancer. Two studies provided data on both bladder cancer (Michaud 2016, HR, 1.38; Nuwizu 2017, HR, 1.10) (43, 46) and kidney cancer (Michaud 2016, HR, 1.06; Nuwizu 2017, HR, 1.19). We used a fixed-effects model to combine the data of the two cancers as the result of urologic cancers (Michaud 2016, HR, 1.26; Nuwizu 2017, HR, 1.16). In addition, another study only provided data on bladder cancer (Arora 2010, HR, 1.13) (36). None of the studies found a clear correlation between PD and urologic cancers.
Our meta-analysis showed that the risk of UC in PD patients was 1.24 times higher than that in patients without PD (HR, 1.24; 95% CI, 1.17-1.31; P < 0.001). The I² statistic showed no heterogeneity (I2 = 22.4%; the heterogeneity P was 0.230). A forest plot incorporating the results of all the studies is shown in Figure 2. After removing each study, the combined effect values were statistically significant. Other details are shown in Figure 3.
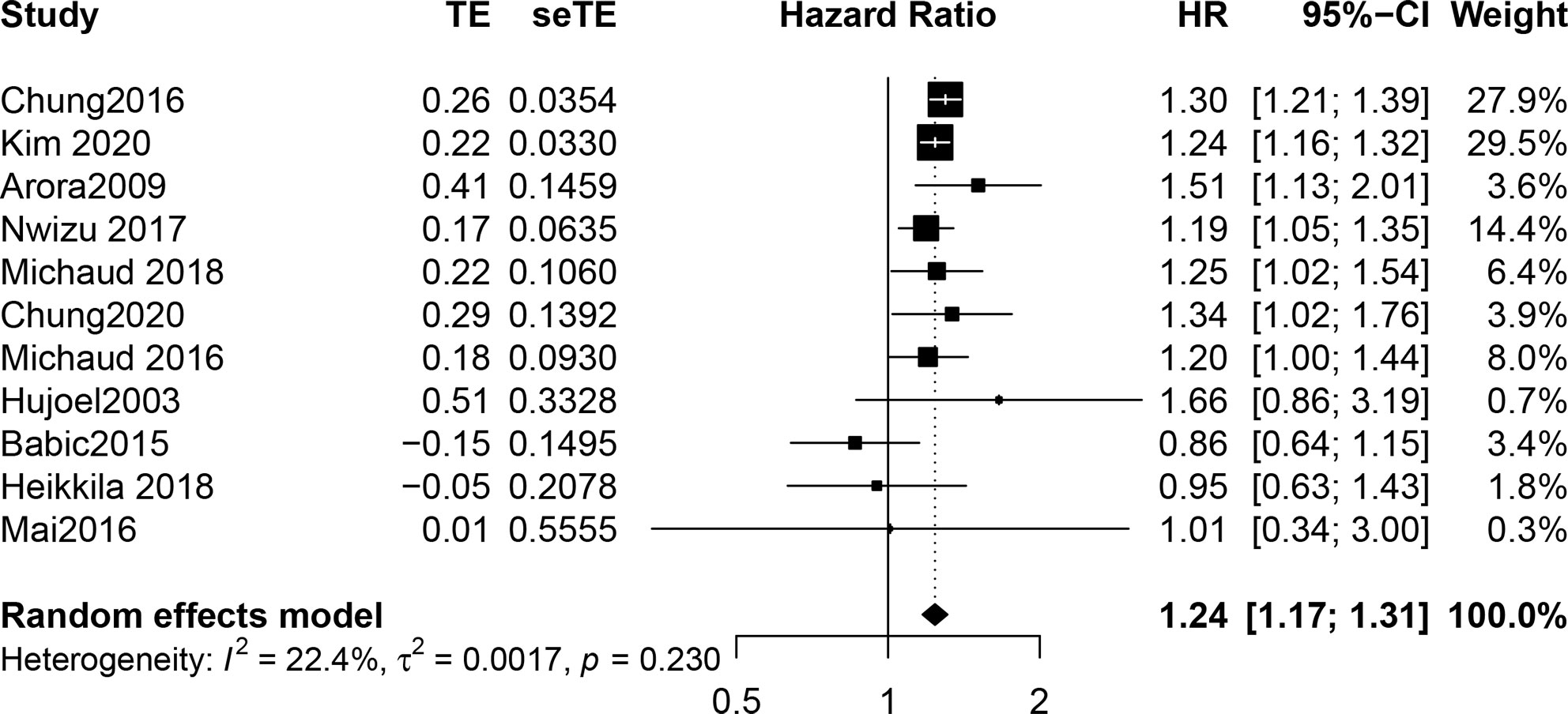
Figure 2 Forest plot incorporating the results of all the studies.
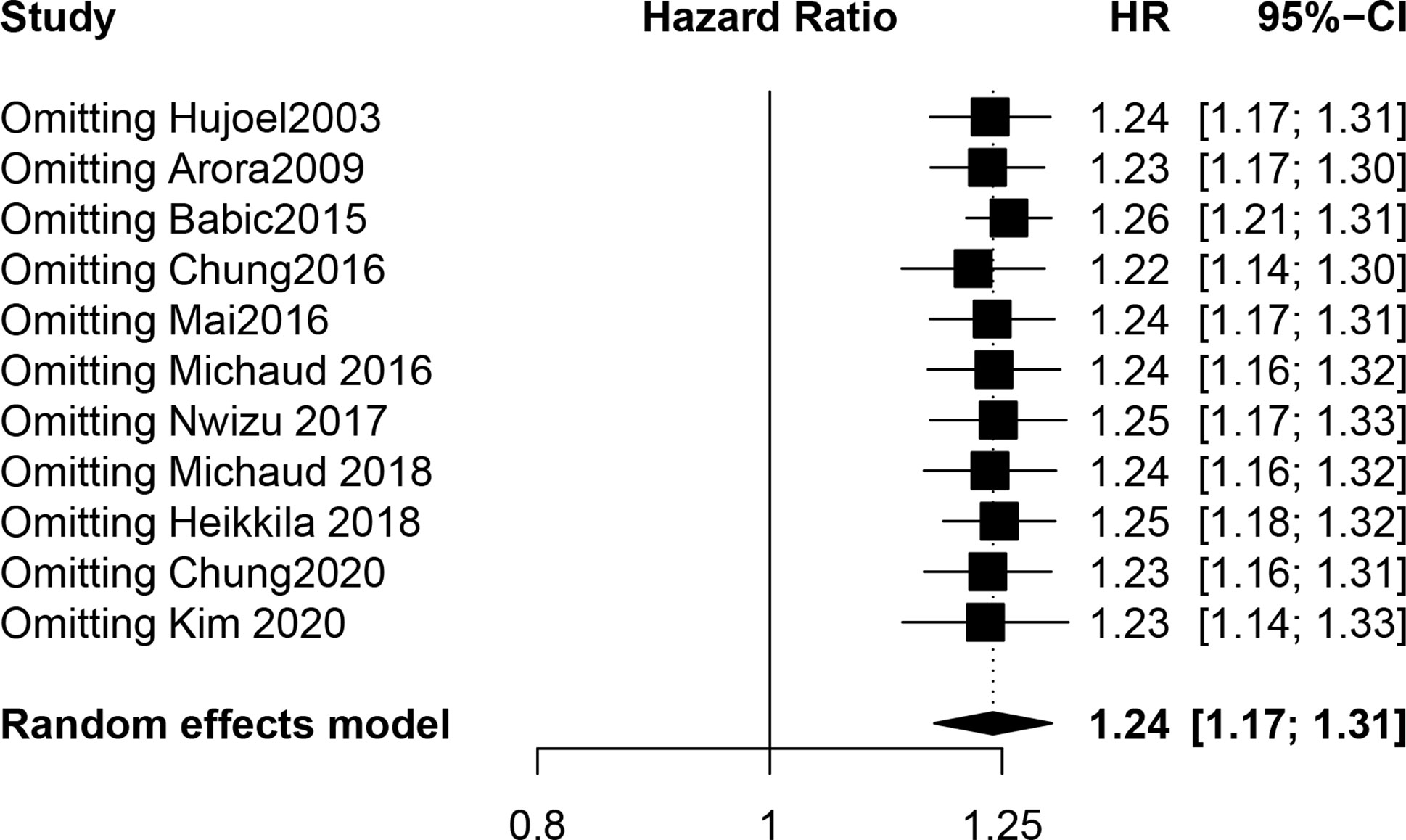
Figure 3 The result of sensitivity analysis.
Subgroup analysis and meta-regression were carried out according to predefined groupings. The results showed that the HRs of each subgroup were ≥ 1.00 but not all results were significant. Random effects model used in data analysis in all subgroups.
According to UC diagnoses, the risk of cancer in PD patients was significantly increased in the study reporting urogenital cancer (HR, 1.27, P < 0.001) and male genital cancer (HR, 1.24, P < 0.001), and there was no significant relationship between PD and female genital cancer (HR, 1.05, P = 0.475) or urologic cancers (HR, 1.19, P = 0.058). The meta-regression results showed that there was a significant difference between UC and Female genital cancer (P = 0.008), as well as UC and ovarian cancer (P = 0.023). More details about the results of subgroup analysis and meta-regression based on urogenital cancer diagnoses are shown in Table 3.
The subgroup analyses according to the follow-up duration, study design, outcomes, risk of bias and smoking status adjustment showed that the results were all similar (HRs, from 1.18 to 1.30) and statistically significant (P < 0.01). According to periodontal status, the HRs of the three groups were similar (total PD, HR, 1.20, P < 0.001; severe PD, HR, 1.29, P < 0.001; moderate PD, HR, 1.25, P = 0.085), and only moderate PD (gingivitis) had no significant correlation with UC. Grouped according to gender, the HR of the study that only observed females was significantly lower than that of the other two groups (male and female, HR, 1.30, P < 0.001; male, HR, 1.28, P = 0.007; female, HR, 1.05, P = 0.501), and there was no significant difference in the results of only the female group. Studies in America and Asia have found a correlation between PD and UC (America, HR, 1.18, P < 0.001; Asia, HR, 1.27, P < 0.001), but Europe has not yet (Europe, HR, 1.22, P = 0.389). The meta-regression results showed that the P value in each group was greater than 0.05. More details about the other results of subgroup analyses and meta-regression are shown in Table 3.
Egger’s test (P = 0.473) indicated no obvious publication bias, and the trim-and-fill method with 2 added studies yielded robust results (P < 0.001, random-effects model). More details about Egger’s test and the trim-and-fill method are shown in Figures 4, 5. The cumulative meta-analysis also showed that our results were stable over time. After cumulative analysis in chronological order, HR point estimates and interval estimates tended to be stable. P < 0.05 was considered statistically significant, and the influence of PD on UC first achieved significance in 2016. Subsequent studies narrowed the range of CIs and improved the reliability of the results. The results of the cumulative meta-analysis are shown in Figure 6.
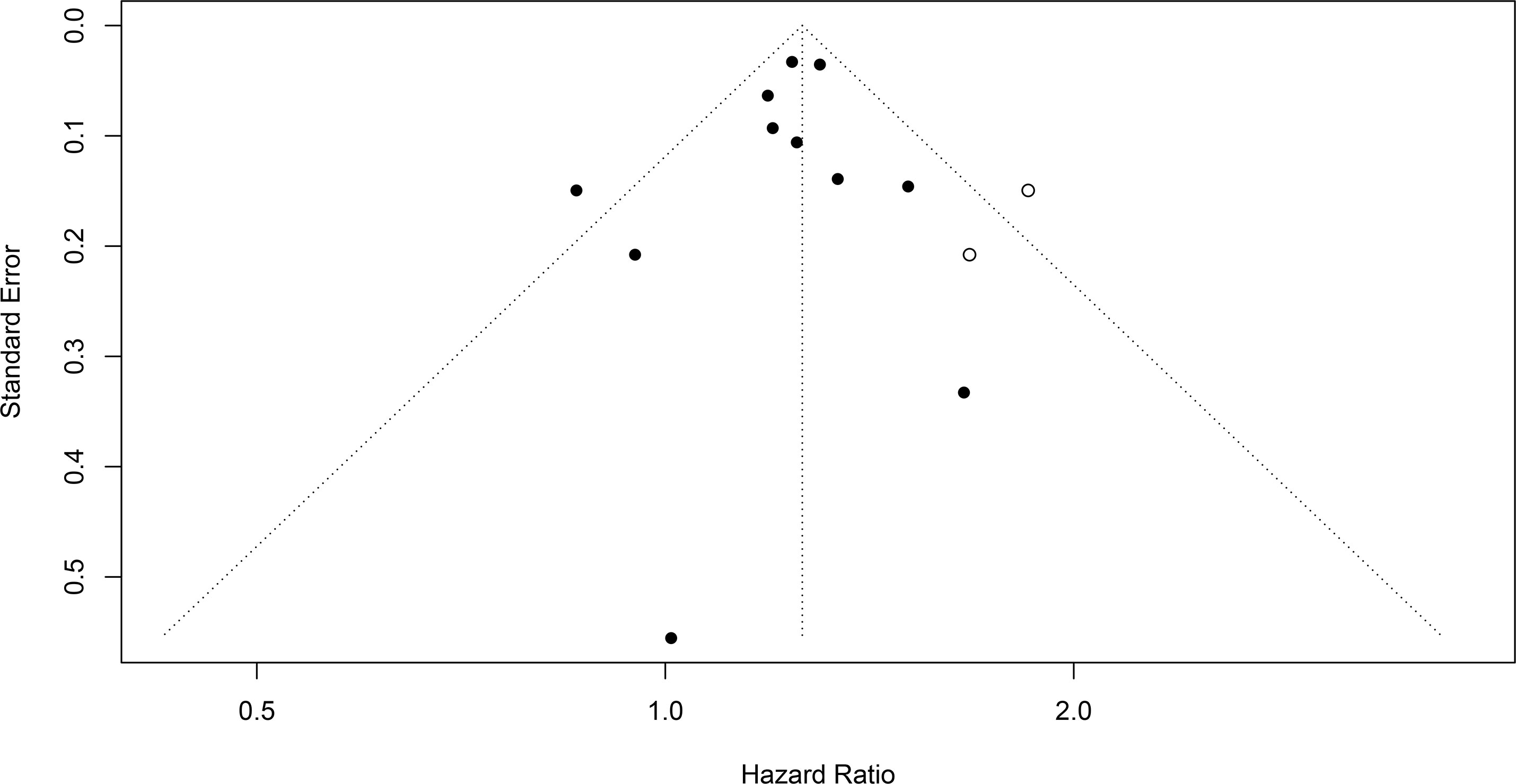
Figure 4 The result of the trim-and-fill method.
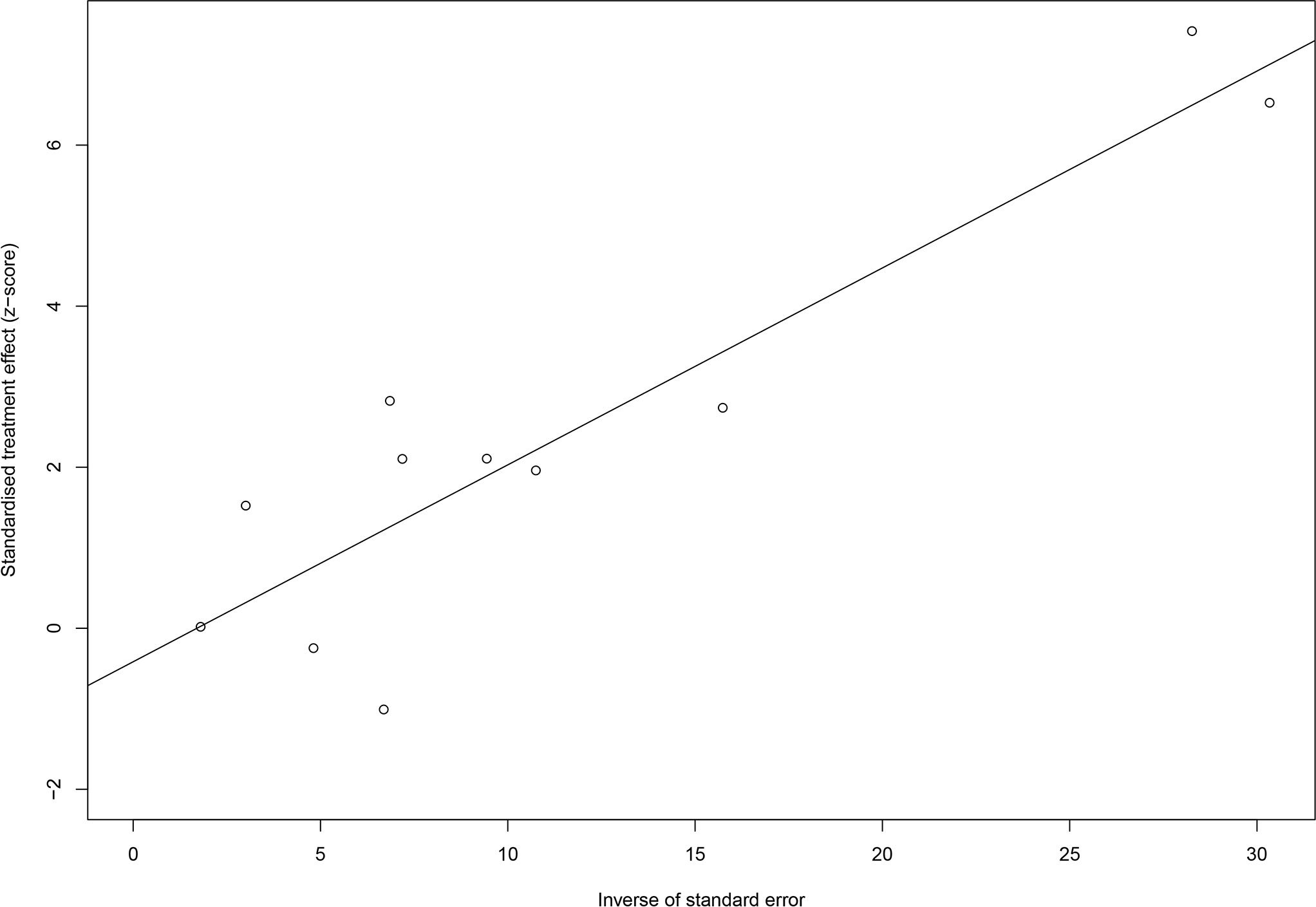
Figure 5 The result of Egger’s test.
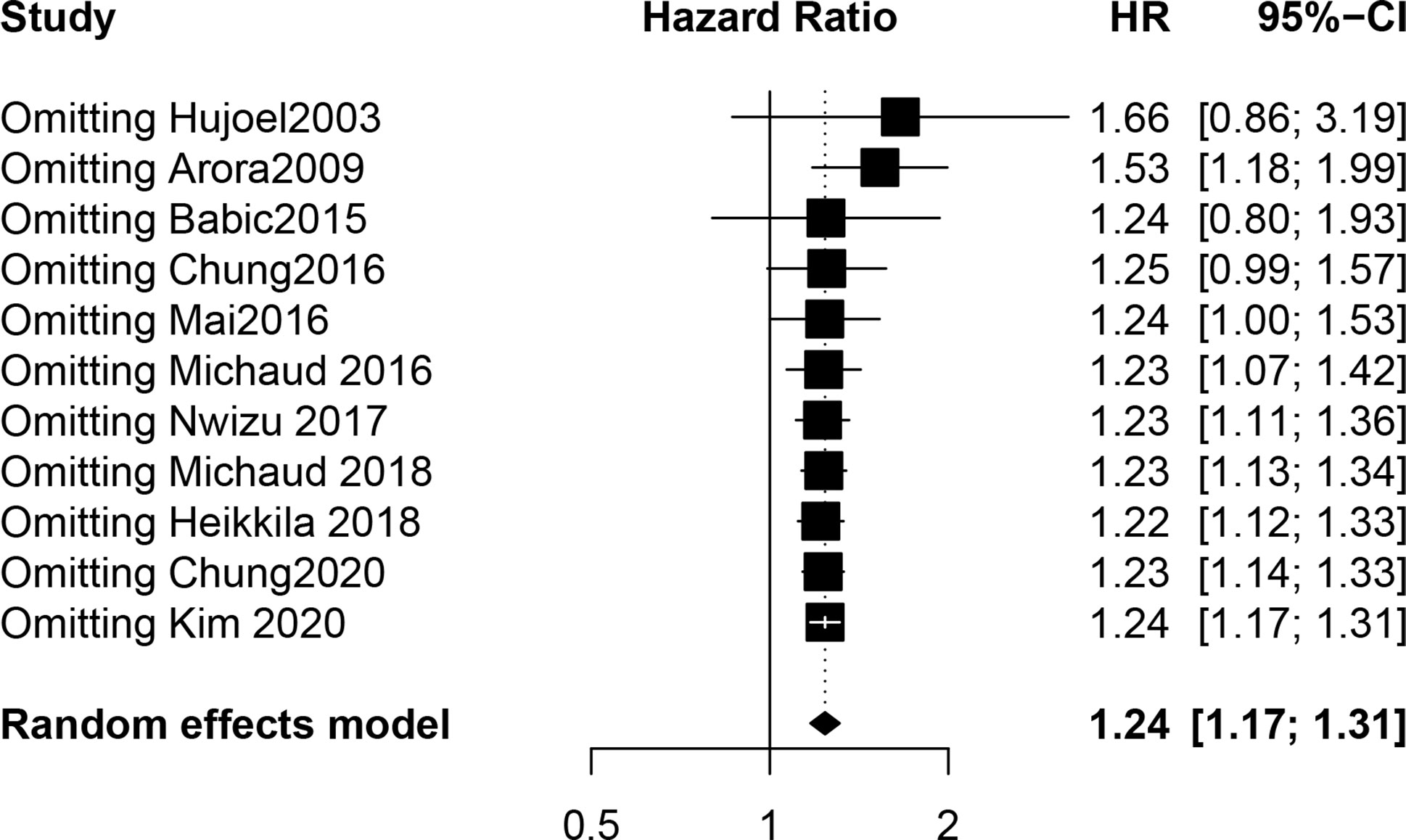
Figure 6 The result of cumulative meta-analysis.
To date, no systematic review or meta-analysis has examined the relationship between PD and UC risk. All eleven studies included in our study were medium- and high-quality cohort studies, and nine were prospective studies. Cohort studies first aim to determine exposure factors and then to explore the results by longitudinal prospective observation. Since exposure factors are evaluated first and then results are observed, this study design is more able to test the causal relationship between a certain factor and a disease. Our meta-analysis of cohort studies can prove the potential causal relationship between PD and UC risk. Our results showed that PD increased the risk of UC by 1.24 times (CI, 1.17-1.31, P < 0.001). The I² statistic was 22.4% and P = 0.230 for heterogeneity; thus, no significant heterogeneity was observed. Subgroup analysis revealed that there were differences between females and other groups according to gender, but the meta-regression analysis found that the difference was not significant. Combining the results of subgroup analysis and meta-regression, we found that there was a significant difference between female genital cancer and UC, which is considered the source of heterogeneity. We believe that the particularity of Female genital cancer is caused by the physiological structure, and the connectivity between the male genital system and the urologic system has caused the results of the two to be closer. The sensitivity analysis, trim-and-fill method and subgroup analysis showed that our research results were reliable. No publication bias was found in Egger’s test. The results of the cumulative meta-analysis indicated that the results tended to be moderate.
Periodontal infection and inflammatory reactions caused by PD correlate with many general diseases (24–28). Many cancers are caused by chronic microbial infections and chronic inflammation damage (61–63). PD and oral bacteria have a strong association with the occurrence and development of cancers in the endocrine system, including the mammary glands and pancreas (29–31, 64). In addition to the chronic inflammatory state caused by cancer, periodontal pathogens may promote cancer by affecting cell proliferation and NF-κB activation and inhibiting apoptosis (63). In addition, periodontal pathogens may release carcinogens (65). The plaque of patients with PD is often not under reasonable control, causing periodontal pathogens to disseminate and accumulate in some parts of the body through the digestive tract, respiratory tract or endocrine system, promoting the development and occurrence of cancer (29–35, 64).
Anaerobic bacteria, such as Fusobacterium and Porphyromonas, are not only pathogens of PD but also pathogenic bacteria of the urinary system (66).A study found that some periodontal pathogens, including Porphyromonas, Fusobacterium and Treponema, existed in the urogenital fluid of patients who had PD with chronic prostatitis and benign urogenital hyperplasia (67). PD and the relationship between its pathogens and chronic kidney disease, including nephritis, have also been widely studied (68–70). The inflammatory status induced by chronic prostatitis and urinary tract infection has been reported to be closely correlated with UC (14, 71–73).In addition, we observed a high correlation between PD and prostate cancer risk (HR, 1.24, P < 0.001), which is a Urogenital System organ specific to male, which we believe explains to some extent why PD is more significantly associated with UC risk in male. Moreover, Fusobacterium was found in the tumours of UC patients (32, 65). We believe that invasion of oral pathogens after epithelial or mucosal traumatic injury may cause urogenital disease development and then have an impact on the subsequent progression of cancer. Although we lack direct evidence of the association between PD and UC, all signs indicate that PD and oral pathogens are inextricably linked to UC.
This meta-analysis has some notable advantages. First, this study was the first meta-analysis in this field. Our study is innovative in exploring the correlation between PD and UC. Second, our study included all studies that met the inclusion criteria, and no publication bias was observed; moreover, the effect sizes and CIs provided by all studies were adjusted for many confounding factors. Third, the studies we included were all cohorts, and the studies had a high level of evidence, suggesting a potential causal relationship between PD and UC risk while minimizing selection and recall bias. Fourth, the average follow-up time in the included studies was more than 10 years, which was long enough to avoid the effects of insufficient follow-up time on the results. Fifth, this study included populations in Europe, Asia and North America, thereby reducing the possible influence of nationality on the results. Finally, our meta-analysis included medium- to high-quality research, increasing the reliability of our results.
While there were strengths, there are naturally many limitations. First, as the clinical definition of PD continues to evolve with the development of the discipline, the diagnostic criteria in different studies were disparate. Even diagnosis in some early studies was based on patient self-reporting, which impacted the heterogeneity of our research. Additionally, it also affects the reliability of the results. Second, although Egger’s test did not indicate bias and the results of the trim-and-fill method were robust, there may still be potential publication bias considering the small number of included studies and articles published in only English. Third, the size of our sample and the number of included studies were small, at least ten observations should be available for each characteristic modelled and when the covariates are unevenly distributed need more. affecting the robustness of the subgroup analyses and meta-regression results. Fourth, confounding factors may have influenced the results. Although each study controlled for some confounding factors, there are still many confounding factors that were not adjusted for in the studies we included, and each study adjusted their confounding factors differently, which not only increased the heterogeneity but also affected the validity of the results. Finally, it was difficult to explore whether there was a difference in the associations between PD and UC with varying severity on account of the limited data provided by the included studies.
Due to the slow progression of UC, most patients do not exhibit significant symptoms, rendering UC difficult to recognize. Therefore, it is important to avoid risk factors that cause UC. PD can be prevented and treated. We can educate people on the correct way to brush their teeth, the harm of smoking and the significance of attending regular dental examinations to decrease PD-associated morbidity. We look forward to helping people realize the importance of maintaining their oral health. With the prevention of PD, we can decrease the risk of UC.
In conclusion, our study shows that the risk of UC in PD patients is increased by 24% compared with people without PD. This study found a link between PD and UC risk, reminding people to pay close attention to PD and the importance of oral health. Of course, our results show only a possible epidemiological correlation between PD and UC, and we do not understand the exact mechanism of the connection between the two. We look forward to finding direct evidence to prove the connection between the two in the future. We also hope that in the future, there will be additional large-scale, multicentre, prospective cohort studies with uniform standards to enrich and expand our research results worldwide.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
WL and SW designed this study. WL and SW performed search and collected data. YZ and YH re-checked data. WL, SL, and DC performed analysis. WL and SL wrote the manuscript. LL reviewed the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by a grant from the National Nature Science Foundation of China (GM 81970942).
The authors would like to thank CDD team for excellent technical support and Professor Dongmei Zhang for critically reviewing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.697399/full#supplementary-material
1. Tagalakis V, Tamim H, Blostein M, Collet JP, Hanley JA, Kahn SR. Use of warfarin and risk of urogenital cancer: a population-based, nested case-control study. Lancet Oncol (2007) 8(5):395–402. doi: 10.1016/S1470-2045(07)70046-3
2. van der Kwast TH, Egevad L, Kristiansen G, Grignon DJ. The international society of urological pathology consultation on molecular pathology of urogenital cancer. Am J Surg Pathol (2020) 44(7):859–61. doi: 10.1097/PAS.0000000000001496
3. Henley SJ, Miller JW, Dowling NF, Benard VB, Richardson LC. Uterine cancer incidence and mortality - united states, 1999-2016. MMWR Morb Mortal Wkly Rep (2018) 67(48):1333–8. doi: 10.15585/mmwr.mm6748a1
4. Jayson GC, Kohn EC, Kitchener HC, Ledermann JA. Ovarian cancer. Lancet (2014) 384(9951):1376–88. doi: 10.1016/S0140-6736(13)62146-7
5. Lenis AT, Lec PM, Chamie K, Mshs MD. Bladder cancer: A review. JAMA. (2020) 324(19):1980–91. doi: 10.1001/jama.2020.17598
7. Rebello RJ, Oing C, Knudsen KE, Loeb S, Johnson DC, Reiter RE, et al. Prostate cancer. Nat Rev Dis Primers. (2021) 7(1):9. doi: 10.1038/s41572-020-00243-0
8. Fizazi K, Kramer G, Eymard JC, Sternberg CN, de Bono J, Castellano D, et al. Quality of life in patients with metastatic prostate cancer following treatment with cabazitaxel versus abiraterone or enzalutamide (CARD): an analysis of a randomised, multicentre, open-label, phase 4 study. Lancet Oncol (2020) 21(11):1513–25. doi: 10.1016/S1470-2045(20)30449-6
9. Mickley A, Kovaleva O, Kzhyshkowska J, Gratchev A. Molecular and immunologic markers of kidney cancer-potential applications in predictive, preventive and personalized medicine. EPMA J (2015) 6:20. doi: 10.1186/s13167-015-0042-2
10. Coughlin SS, Neaton JD, Randall B, Sengupta A. Predictors of mortality from kidney cancer in 332,547 men screened for the multiple risk factor intervention trial. Cancer. (1997) 79(11):2171–7. doi: 10.1002/(SICI)1097-0142(19970601)79:11<2171::AID-CNCR15>3.0.CO;2-T
11. Kaplan SA. Re: benign prostatic hyperplasia is a significant risk factor for bladder cancer in diabetic patients: a population-based cohort study using the national health insurance in Taiwan. J Urol. (2014) 191(1):58–9. doi: 10.1016/j.juro.2013.10.010
12. Bai X, Yi M, Dong B, Zheng X, Wu K. The global, regional, and national burden of kidney cancer and attributable risk factor analysis from 1990 to 2017. Exp Hematol Oncol (2020) 9:27. doi: 10.1186/s40164-020-00181-3
13. De Nunzio C, Kramer G, Marberger M, Montironi R, Nelson W, Schroder F, et al. The controversial relationship between benign prostatic hyperplasia and prostate cancer: the role of inflammation. Eur Urol. (2011) 60(1):106–17. doi: 10.1016/j.eururo.2011.03.055
14. de Vivar Chevez AR, Finke J, Bukowski R. The role of inflammation in kidney cancer. Adv Exp Med Biol (2014) 816:197–234. doi: 10.1007/978-3-0348-0837-8_9
15. Dominguez Gutierrez PR, Kwenda EP, Donelan W, O'Malley P, Crispen PL, Kusmartsev S. Hyal2 expression in tumor-associated myeloid cells mediates cancer-related inflammation in bladder cancer. Cancer Res (2020) 81(3):648–657. doi: 10.1158/0008-5472.CAN-20-1144
16. Savant SS, Sriramkumar S, O'Hagan HM. The role of inflammation and inflammatory mediators in the development, progression, metastasis, and chemoresistance of epithelial ovarian cancer. Cancers (Basel). (2018) 10(8):251. doi: 10.3390/cancers10080251
17. Vignozzi L, Maggi M. Prostate cancer: intriguing data on inflammation and prostate cancer. Nat Rev Urol. (2014) 11(7):369–70. doi: 10.1038/nrurol.2014.143
18. Yang H, Gu J, Lin X, Grossman HB, Ye Y, Dinney CP, et al. Profiling of genetic variations in inflammation pathway genes in relation to bladder cancer predisposition. Clin Cancer Res (2008) 14(7):2236–44. doi: 10.1158/1078-0432.CCR-07-1670
19. Caton J, Armitage G, Berglundh T, Chapple I, Jepsen S, Kornman K, et al. A new classification scheme for periodontal and peri-implant diseases and conditions - introduction and key changes from the 1999 classification. J Clin periodontol (2018), S1–8. doi: 10.1111/jcpe.12935
20. Peres MA, Daly B, Guarnizo-Herreno CC, Benzian H, Watt RG. Oral diseases: a global public health challenge - authors' reply. Lancet. (2020) 395(10219):186–7. doi: 10.1016/S0140-6736(19)32997-6
21. Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol (2015) 15(1):30–44. doi: 10.1038/nri3785
22. Eke PI, Dye BA, Wei L, Slade GD, Thornton-Evans GO, Borgnakke WS, et al. Update on prevalence of periodontitis in adults in the united states: NHANES 2009 to 2012. J Periodontol (2015) 86(5):611–22. doi: 10.1902/jop.2015.140520
23. Jepsen S, Caton J, Albandar J, Bissada N, Bouchard P, Cortellini P, et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Clin periodontol (2018), S219–S29. doi: 10.1111/jcpe.12951
24. Han YW, Wang X. Mobile microbiome: oral bacteria in extra-oral infections and inflammation. J Dent Res (2013) 92(6):485–91. doi: 10.1177/0022034513487559
25. Kebschull M, Demmer RT, Papapanou PN. "Gum bug, leave my heart alone!"–epidemiologic and mechanistic evidence linking periodontal infections and atherosclerosis. J Dent Res (2010) 89(9):879–902. doi: 10.1177/0022034510375281
26. Li C, Lv Z, Shi Z, Zhu Y, Wu Y, Li L, et al. Periodontal therapy for the management of cardiovascular disease in patients with chronic periodontitis. Cochrane Database Syst Rev (2017) 11:CD009197. doi: 10.1002/14651858.CD009197.pub3
27. Lundberg K, Wegner N, Yucel-Lindberg T, Venables PJ. Periodontitis in RA-the citrullinated enolase connection. Nat Rev Rheumatol (2010) 6(12):727–30. doi: 10.1038/nrrheum.2010.139
28. Madianos PN, Bobetsis YA, Offenbacher S. Adverse pregnancy outcomes (APOs) and periodontal disease: pathogenic mechanisms. J Periodontol (2013) 84(4 Suppl):S170–80. doi: 10.1902/jop.2013.1340015
29. Maisonneuve P, Amar S, Lowenfels AB. Periodontal disease, edentulism, and pancreatic cancer: a meta-analysis. Ann Oncol (2017) 28(5):985–95. doi: 10.1093/annonc/mdx019
30. Shao J, Wu L, Leng WD, Fang C, Zhu YJ, Jin YH, et al. Periodontal disease and breast cancer: A meta-analysis of 1,73,162 participants. Front Oncol (2018) 8:601. doi: 10.3389/fonc.2018.00601
31. Zhang Y, Sun C, Song EJ, Liang M, Shi T, Min M, et al. Is periodontitis a risk indicator for gastrointestinal cancers? a meta-analysis of cohort studies. J Clin Periodontol (2020) 47(2):134–47. doi: 10.1111/jcpe.13217
32. Bucevic Popovic V, Situm M, Chow CT, Chan LS, Roje B, Terzic J. The urinary microbiome associated with bladder cancer. Sci Rep (2018) 8(1):12157. doi: 10.1038/s41598-018-29054-w
33. Liss MA, White JR, Goros M, Gelfond J, Leach R, Johnson-Pais T, et al. Metabolic biosynthesis pathways identified from fecal microbiome associated with prostate cancer. Eur Urol. (2018) 74(5):575–82. doi: 10.1016/j.eururo.2018.06.033
34. Ma X, Chi C, Fan L, Dong B, Shao X, Xie S, et al. The microbiome of prostate fluid is associated with prostate cancer. Front Microbiol (2019) 10:1664. doi: 10.3389/fmicb.2019.01664
35. Oresta B, Braga D, Lazzeri M, Frego N, Saita A, Faccani C, et al. The microbiome of catheter collected urine in males with bladder cancer according to disease stage. J Urol. (2021) 205(1):86–93. doi: 10.1097/JU.0000000000001336
36. Arora M, Weuve J, Fall K, Pedersen NL, Mucci LA. An exploration of shared genetic risk factors between periodontal disease and cancers: a prospective co-twin study. Am J Epidemiol. (2010) 171(2):253–9. doi: 10.1093/aje/kwp340
37. Babic A, Poole EM, Terry KL, Tworoger SS. Periodontal bone loss and risk of epithelial ovarian cancer in nurses' health study. Clin Cancer Res (2015) 21(16):POSTER-CTRL-1201. doi: 10.1158/1557-3265.OVCASYMP14-POSTER-CTRL-1201
38. Chung PC, Chan TC. Association between periodontitis and all-cause and cancer mortality: retrospective elderly community cohort study. BMC Oral Health (2020) 20(1):168. doi: 10.1186/s12903-020-01156-w
39. Chung SD, Tsai MC, Huang CC, Kao LT, Chen CH. A population-based study on the associations between chronic periodontitis and the risk of cancer. Int J Clin Oncol (2016) 21(2):219–23. doi: 10.1007/s10147-015-0884-6
40. Hujoel PP, Drangsholt M, Spiekerman C, Weiss NS. An exploration of the periodontitis-cancer association. Ann Epidemiol. (2003) 13(5):312–6. doi: 10.1016/S1047-2797(02)00425-8
41. Kim DH, Jeong SN, Lee JH. Chronic periodontal disease increases risk for prostate cancer in elderly individuals in south Korea: a retrospective nationwide population-based cohort study. J Cancer. (2020) 11(16):4716–23. doi: 10.7150/jca.45369
42. Mai X, LaMonte MJ, Hovey KM, Freudenheim JL, Andrews CA, Genco RJ, et al. Periodontal disease severity and cancer risk in postmenopausal women: the buffalo OsteoPerio study. Cancer Causes Control. (2016) 27(2):217–28. doi: 10.1007/s10552-015-0699-9
43. Michaud DS, Kelsey KT, Papathanasiou E, Genco CA, Giovannucci E. Periodontal disease and risk of all cancers among male never smokers: an updated analysis of the health professionals follow-up study. Ann Oncol (2016) 27(5):941–7. doi: 10.1093/annonc/mdw028
44. Michaud DS, Liu Y, Meyer M, Giovannucci E, Joshipura K. Periodontal disease, tooth loss, and cancer risk in male health professionals: a prospective cohort study. Lancet Oncol (2008) 9(6):550–8. doi: 10.1016/S1470-2045(08)70106-2
45. Michaud DS, Lu J, Peacock-Villada AY, Barber JR, Joshu CE, Prizment AE, et al. Periodontal disease assessed using clinical dental measurements and cancer risk in the ARIC study. J Natl Cancer Inst (2018) 110(8):843–54. doi: 10.1093/jnci/djx278
46. Nwizu NN, Marshall JR, Moysich K, Genco RJ, Hovey KM, Mai X, et al. Periodontal disease and incident cancer risk among postmenopausal women: Results from the women's health initiative observational cohort. Cancer Epidemiol Biomarkers Prev (2017) 26(8):1255–65. doi: 10.1158/1055-9965.EPI-17-0212
47. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
48. Li W, Xu J, Zhang R, Li Y, Wang J, Zhang X, et al. Is periodontal disease a risk indicator for colorectal cancer? a systematic review and meta-analysis. J Clin periodontol (2021) 48(3):336–47. doi: 10.1111/jcpe.13402
49. Maisonneuve P, Amar S, Lowenfels A. Periodontal disease, edentulism, and pancreatic cancer: a meta-analysis. Ann Oncol Off J Eur Soc Med Oncol (2017) 28(5):985–95. doi: 10.1093/annonc/mdx019
50. Shi T, Min M, Sun C, Zhang Y, Liang M, Sun Y. Periodontal disease and susceptibility to breast cancer: A meta-analysis of observational studies. J Clin periodontol (2018) 45(9):1025–33. doi: 10.1111/jcpe.12982
51. Xie W, Jin Y, Leng W, Wang X, Zeng X. Periodontal disease and risk of bladder cancer: A meta-analysis of 298476 participants. Front Physiol (2018) 9:979. doi: 10.3389/fphys.2018.00979
52. Guo Z, Gu C, Li S, Gan S, Li Y, Xiang S, et al. Periodontal disease and the risk of prostate cancer: a meta-analysis of cohort studies. Int Braz J Urol. (2021) 47(6):1120–30. doi: 10.1590/s1677-5538.ibju.2020.0333
53. Pilati SFM, Pilati PVF. Does periodontal disease have an association with prostate cancer? Evid Based Dent (2021) 22(4):140–2. doi: 10.1038/s41432-021-0213-z
54. Yuan S, Fang C, Leng WD, Wu L, Li BH, Wang XH, et al. Oral microbiota in the oral-genitourinary axis: identifying periodontitis as a potential risk of genitourinary cancers. Mil Med Res (2021) 8(1):54. doi: 10.1186/s40779-021-00344-1
55. Heikkilä P, But A, Sorsa T, Haukka J. Periodontitis and cancer mortality: Register-based cohort study of 68,273 adults in 10-year follow-up. Int J Cancer. (2018) 142(11):2244–53. doi: 10.1002/ijc.31254
56. Odone A, Gianfredi V, Vigezzi G, Amerio A, Ardito C, d'Errico A, et al. Does retirement trigger depressive symptoms? a systematic review and meta-analysis. Epidemiol Psychiatr Sci (2021) 30:e77. doi: 10.1017/S2045796021000627
57. Ronksley PE, Brien SE, Turner BJ, Mukamal KJ, Ghali WA. Association of alcohol consumption with selected cardiovascular disease outcomes: a systematic review and meta-analysis. BMJ. (2011) 342:d671. doi: 10.1136/bmj.d671
58. Zhang J, Yu KF. What's the relative risk? a method of correcting the odds ratio in cohort studies of common outcomes. JAMA. (1998) 280(19):1690–1. doi: 10.1001/jama.280.19.1690
59. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327(7414):557–60. doi: 10.1136/bmj.327.7414.557
60. Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. (2020) 368:l6890. doi: 10.1136/bmj.l6890
61. de Bono JS, Guo C, Gurel B, De Marzo AM, Sfanos KS, Mani RS, et al. Prostate carcinogenesis: inflammatory storms. Nat Rev Cancer. (2020) 20(8):455–69. doi: 10.1038/s41568-020-0267-9
62. Pollard J. Bacteria, inflammation and cancer. Nat Rev Immunol (2015) 15(9):528. doi: 10.1038/nri3899
63. Taniguchi K, Karin M. NF-kappaB, inflammation, immunity and cancer: coming of age. Nat Rev Immunol (2018) 18(5):309–24. doi: 10.1038/nri.2017.142
64. Li W, Xu J, Zhang R, Li Y, Wang J, Zhang X, et al. Is periodontal disease a risk indicator for colorectal cancer? a systematic review and meta-analysis. J Clin Periodontol (2021) 48(3):336–47. doi: 10.1111/jcpe.13402
65. Abed J, Maalouf N, Parhi L, Chaushu S, Mandelboim O, Bachrach G. Tumor targeting by fusobacterium nucleatum: A pilot study and future perspectives. Front Cell Infect Microbiol (2017) 7:295. doi: 10.3389/fcimb.2017.00295
66. Brook I. Urinary tract and genito-urinary suppurative infections due to anaerobic bacteria. Int J Urol. (2004) 11(3):133–41. doi: 10.1111/j.1442-2042.2003.00756.x
67. Sandhu JS. Prostate cancer and chronic prostatitis. Curr Urol Rep (2008) 9(4):328–32. doi: 10.1007/s11934-008-0056-6
68. Chen YT, Shih CJ, Ou SM, Hung SC, Lin CH, Tarng DC, et al. Periodontal disease and risks of kidney function decline and mortality in older people: A community-based cohort study. Am J Kidney Dis (2015) 66(2):223–30. doi: 10.1053/j.ajkd.2015.01.010
69. Iwasaki M, Taylor GW, Nesse W, Vissink A, Yoshihara A, Miyazaki H. Periodontal disease and decreased kidney function in Japanese elderly. Am J Kidney Dis (2012) 59(2):202–9. doi: 10.1053/j.ajkd.2011.08.027
70. Kitamura M, Mochizuki Y, Miyata Y, Obata Y, Mitsunari K, Matsuo T, et al. Pathological characteristics of periodontal disease in patients with chronic kidney disease and kidney transplantation. Int J Mol Sci (2019) 20(14):3413. doi: 10.3390/ijms20143413
71. Bayne CE, Farah D, Herbst KW, Hsieh MH. Role of urinary tract infection in bladder cancer: a systematic review and meta-analysis. World J Urol. (2018) 36(8):1181–90. doi: 10.1007/s00345-018-2257-z
72. Stone L. Bladder cancer: Urinary tract infection increases risk. Nat Rev Urol. (2015) 12(1):4. doi: 10.1038/nrurol.2014.343
Keywords: urogenital cancer, periodontal disease, systematic review, meta-analysis, cohort studies
Citation: Li W, Wang S, He Y, Zhang Y, Lin S, Cen D and Lin L (2022) Is periodontal disease a risk indicator for urogenital cancer? A systematic review and meta-analysis of cohort studies. Front. Oncol. 12:697399. doi: 10.3389/fonc.2022.697399
Received: 19 April 2021; Accepted: 13 July 2022;
Published: 09 August 2022.
Edited by:
Alcides Chaux, Universidad del Norte, ParaguayReviewed by:
Francisco Wilker Mustafa Gomes Muniz, Federal University of Pelotas, BrazilCopyright © 2022 Li, Wang, He, Zhang, Lin, Cen and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Li Lin, bGlubGlAY211LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.