 Nicolas Serratrice1
Nicolas Serratrice1 Imène Lameche1
Imène Lameche1 Christian Attieh1
Christian Attieh1 Moussa A Chalah1,2,3
Moussa A Chalah1,2,3 Joe Faddoul1,4
Joe Faddoul1,4 Bilal Tarabay1Rabih Bou-Nassif5
Bilal Tarabay1Rabih Bou-Nassif5 Youssef Ali6Joseph G Mattar1
Youssef Ali6Joseph G Mattar1 François Nataf7
François Nataf7 Samar S Ayache1,2,3,8†
Samar S Ayache1,2,3,8† Georges N Abi Lahoud1,3†*
Georges N Abi Lahoud1,3†*- 1Institut de la Colonne Vertébrale et des Neurosciences (ICVNS), Centre Médico-Chirurgical Bizet, Paris, France
- 2EA 4391, Excitabilité Nerveuse et Thérapeutique, Faculté de Santé, Université Paris Est, Créteil, France
- 3Gilbert and Rose-Marie Chagoury School of Medicine, Lebanese American University, Byblos, Lebanon
- 4Service de Neurochirurgie, Centre Hospitalier de la Côte Basque, Bayonne, France
- 5Department of Neurosurgery, Memorial Sloan Kettering Cancer Center, New York, NY, United States
- 6Institut de Chirurgie Osseuse et de Neurochirurgie, Médipole-Montagard, Avignon, France
- 7Service de Neurochirurgie, Hôpital Lariboisière, Paris, France
- 8Service de Physiologie-Explorations Fonctionnelles, DMU FIxIT, Hôpital Henri Mondor, Créteil, France
Meningiomas arise from arachnoidal cap cells of the meninges, constituting the most common type of central nervous system tumors, and are considered benign tumors in most cases. Their incidence increases with age, and they mainly affect females, constituting 25-46% of primary spinal tumors. Spinal meningiomas could be detected incidentally or be unraveled by various neurological symptoms (e.g., back pain, sphincter dysfunction, sensorimotor deficits). The gold standard diagnostic modality for spinal meningiomas is Magnetic resonance imaging (MRI) which permits their classification into four categories based on their radiological appearance. According to the World Health Organization (WHO) classification, the majority of spinal meningiomas are grade 1. Nevertheless, they can be of higher grade (grades 2 and 3) with atypical or malignant histology and a more aggressive course. To date, surgery is the best treatment where the big majority of meningiomas can be cured. Advances in surgical techniques (ultrasonic dissection, microsurgery, intraoperative monitoring) increase the complete resection rate. Operated patients have a satisfactory prognosis, even in those with poor preoperative neurological status. Adjuvant therapy has a growing role in treating spinal meningiomas, mainly in the case of subtotal resection and tumor recurrence. The current paper reviews the fundamental epidemiological and clinical aspects of spinal meningiomas, their histological and genetic characteristics, and their management, including the various surgical novelties and techniques.
Introduction
Meningiomas are lesions that arise from arachnoidal cap cells, the outer part of the arachnoid layer and villi (1). They usually form dural attachments and are marked by meningothelial hyperplasia (1).
Spinal meningiomas are relatively rare, accounting for approximately 3% of all meningiomas of the central nervous system (CNS) (2) and 25-46% of all primary intraspinal neoplasms (2, 3). 90% of intradural extramedullary spinal tumors are either meningiomas or schwannomas and constitute nearly 25% of primary spinal neoplasia (3).
Spinal meningiomas mainly affect people in their fifth decade of life and are more frequent in women (given their estrogen receptors) (4). In case they occur in young patients, or if they cause multiple lesions, a genetic disorder like neurofibromatosis type 2 (NF2) or aggressive histological subtypes should be suspected (2, 4). Spinal meningiomas most commonly occur in the posterior, posterolateral, or lateral thoracic region, followed by the anterior cervical and lumbosacral regions. The main treatment is surgery, which can be performed in (a) a classical open microsurgical approach in the vast majority of cases, (b) a minimally invasive surgery (MIS), or (c) through an endoscopic intervention (5). The choice of the most appropriate surgical method could be challenging, especially in the case of aggressive meningiomas and in some difficult access tumors (e.g., location anterior to the spinal cord in the thoracic region). For instance, ventral/ventrolateral cervical meningiomas within the upper cervical region, may envelop the vertebral artery (6), and thus require precise presurgical calculations to adopt the safest approach.
The scientific knowledge regarding spinal meningiomas has evolved over the past twenty years. This evolution concerns multiple aspects, including clinical evaluation, molecular and radiological specificities, and microsurgical management techniques. Therefore, the main goal of this paper is to come up with an updated review of spinal meningiomas, with a particular focus on their clinical presentation, biological and imaging aspects, and neurosurgical strategies.
Selection criteria
A review of the literature was carried out using PubMed/Medline and Scopus databases. The following keywords were used: “spinal meningioma” AND (“biology” OR “molecular” OR “genetic” OR “endocrine” OR “imaging” OR “grading” OR “prognosis” OR “surgery” OR “resection” OR “intraoperative monitoring” OR “adjuvant therapy” OR “recurrence” OR “psychology” OR “anxiety” AND “depression”). Original papers published in English and French were included in the analysis. The references of the selected papers were manually scanned in order to identify any additional references. To note, papers on intracranial meningiomas were also scanned and relevant papers were included since some research on spinal meningiomas stem from studies carried out on intracranial meningiomas.
Clinical features
Spinal meningiomas are typically solitary, well-circumcised, slow-growing, intradural extramedullary tumors (Figure 1) (7) that usually respect the surrounding normal tissue (1). Hence, they are often perceived as noninvasive. However, they could be aggressive in some cases by seeding other parts of the CNS or the surgical site.
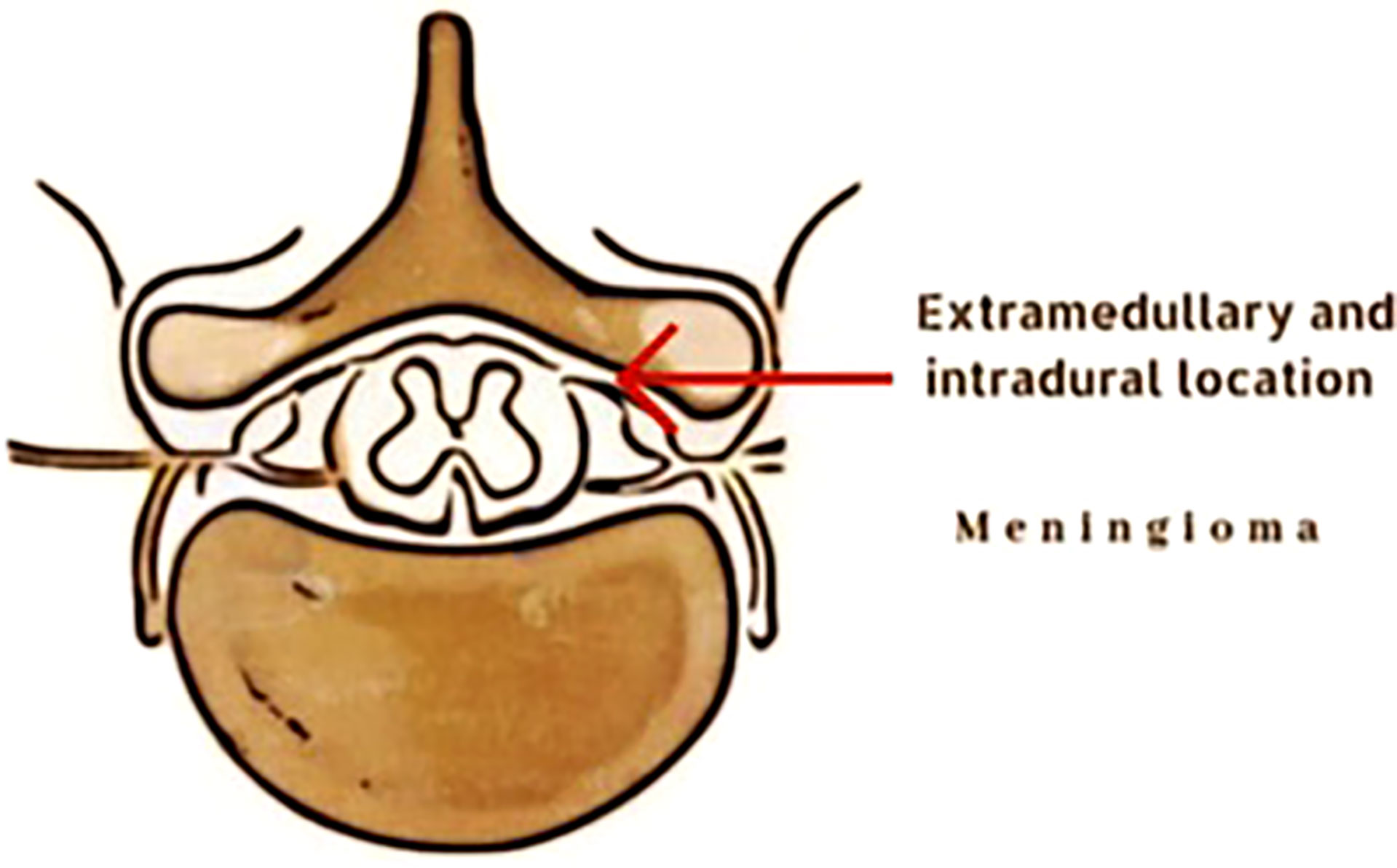
Figure 1 Illustration of extramedullary and intradural location of a spinal meningioma.
As stated above, meningiomas are more frequently seen at the thoracic level and tend to expand slowly without any clinical manifestation initially. Around 9% of cases are asymptomatic and report no complaints (8). At an advanced stage, meningiomas compromise spinal elements, resulting in various neurological symptoms and signs, such as pain, motor, and sensory disturbances, gait abnormality, and sphincter dysfunction. Complaints can vary from one person to another depending on the size of the meningioma and the exact site of the spinal compression (8). Clinical manifestations depend also on the initial size of the spinal canal as large constitutional ones can tolerate the development of large sized tumors while remaining asymptomatic.
The most frequent presentation is pain, ranging from 42% in some case series to as high as 87% in other reports (8, 9). Pain is more frequently described as local or radicular. Apart from pain, patients often report sensory and motor symptoms. Sensory manifestations can have many aspects, such as aching, burning, tingling, numbness, hypoesthesia, paresthesia, and anesthesia. These symptoms can be present in 16% to 84% of cases (4, 10). However, the most alarming sign for patients is motor deficit. It can start as a slight weakness and evolves later into a complete motor deficit. Motor symptoms are present in 33% to 93% of patients with spinal meningiomas (2, 4). Moreover, some patients could complain of gait and balance disturbances in 47% to 93% of cases (8, 11). Finally, sphincter dysfunction is reported in some series but less frequently than other symptoms. Sphincter dysfunction can be seen in 6 to 60% of patients seeking medical opinion (8, 11). A summary of the clinical manifestations is depicted in Table 1.
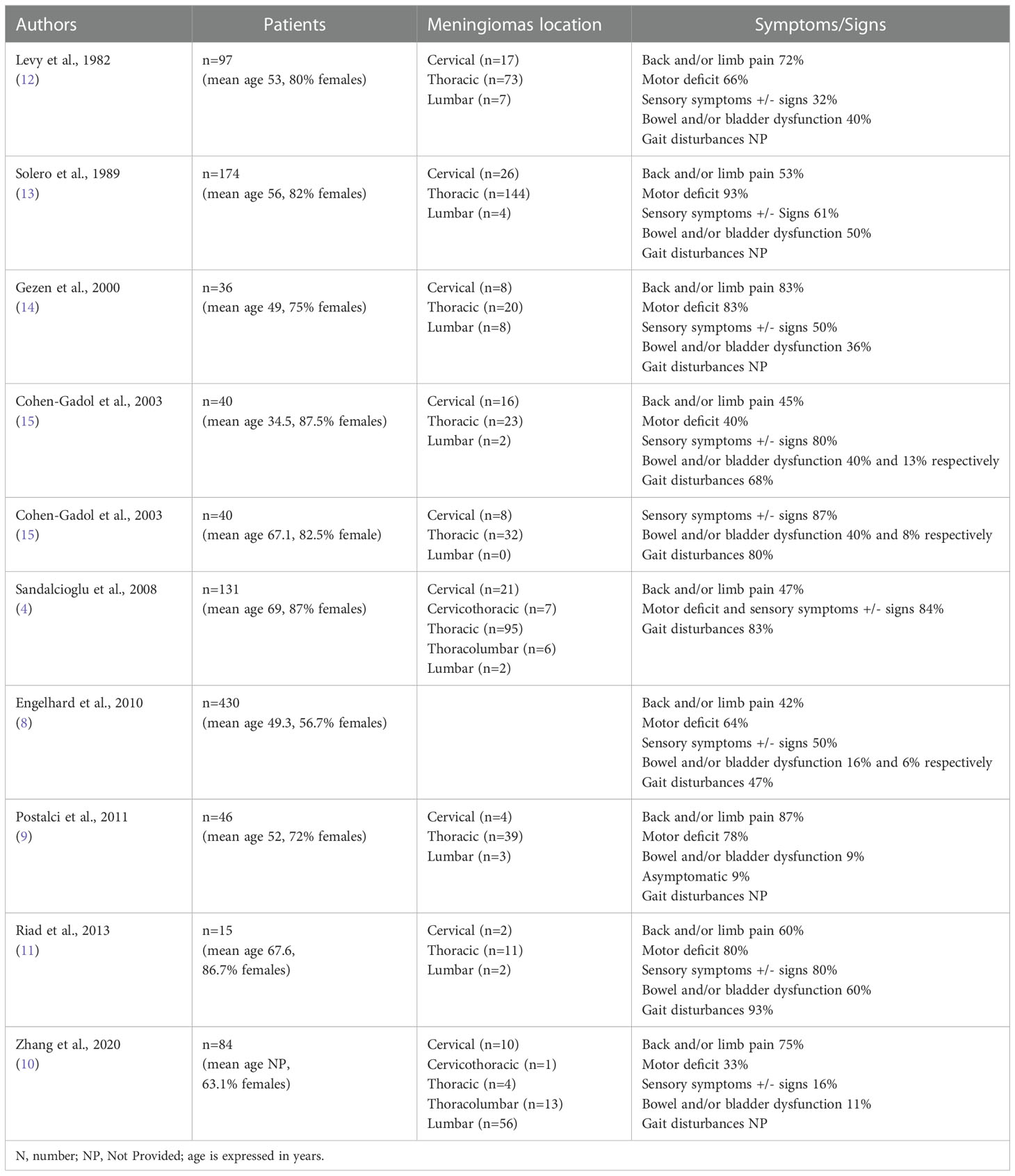
Table 1 Summary of clinical manifestations in spinal meningiomas.
Pathology
Many histological subtypes of meningiomas have been described, among which meningothelial, fibroblastic, and transitional meningiomas are the most frequent ones. The histological analysis of meningiomas defines the histological type and grade of the tumor according to the 2021 World Health Organization (WHO) classification, as illustrated in Figure 2 (16). It classifies meningiomas into three grades, where each grade correlates with different potential for growth, metastatic spread, recurrence, and prognosis.
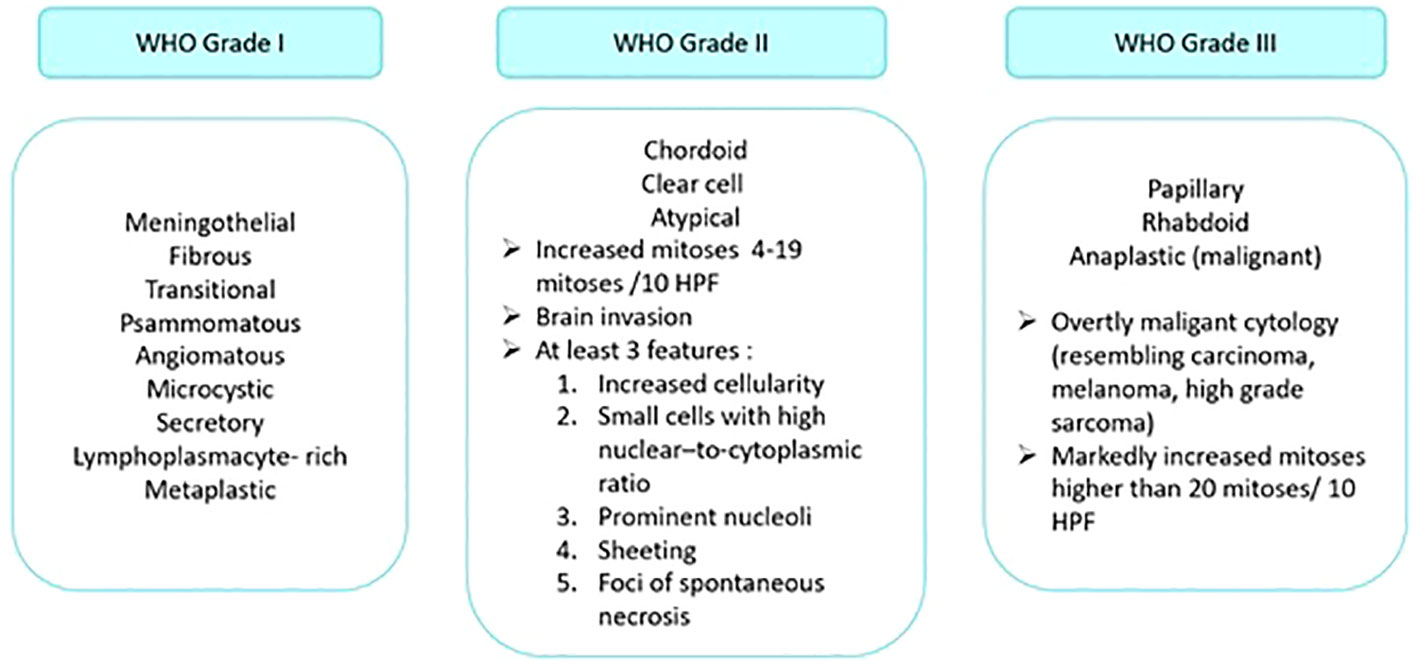
Figure 2 Grading of meningiomas according to the 2021 WHO classification system. HPF: high power field.
Many histologic subtypes are observed in both intracranial and spinal meningiomas. Meningothelial, metaplastic, psammomatous, transitional, atypical, and clear cell subtypes are the most common subtypes of intracranial meningiomas. As for spinal meningiomas, the psammomatous, meningothelial and transitional subtypes distinguish them, and they have a lower risk of recurrence than the intracranial ones for reasons yet to be determined.
The WHO divides meningiomas into three grades from 1 to 3 (benign, atypical and malignant, respectively) based on their malignancy degree (17). In the case of “mixed” tumors, the diagnosis of the dominant histological type (i.e., the type forming more than 50% of the tumor) is retained. However, the presence of a minority contingent with more aggressive potential should be reported.
Genetic alterations
Advances in molecular biology have greatly improved the understanding of the various mechanisms at the origin of meningiomas development. Molecular profiles of spinal meningiomas are similar to their intracranial counterparts (18). These alterations account for 3% of reported cases only. Chromosomal instability is a widespread molecular alteration that characterizes recurrent or poor prognosis meningiomas. Accumulation of cytogenetic aberrations is associated with higher-grade meningiomas and a higher risk of recurrence, which explains why high-grade meningiomas have more altered cytogenetic profiles than benign meningiomas (19). Table 2 summarizes the different gene mutations implicated in meningiomas and their prognosis.
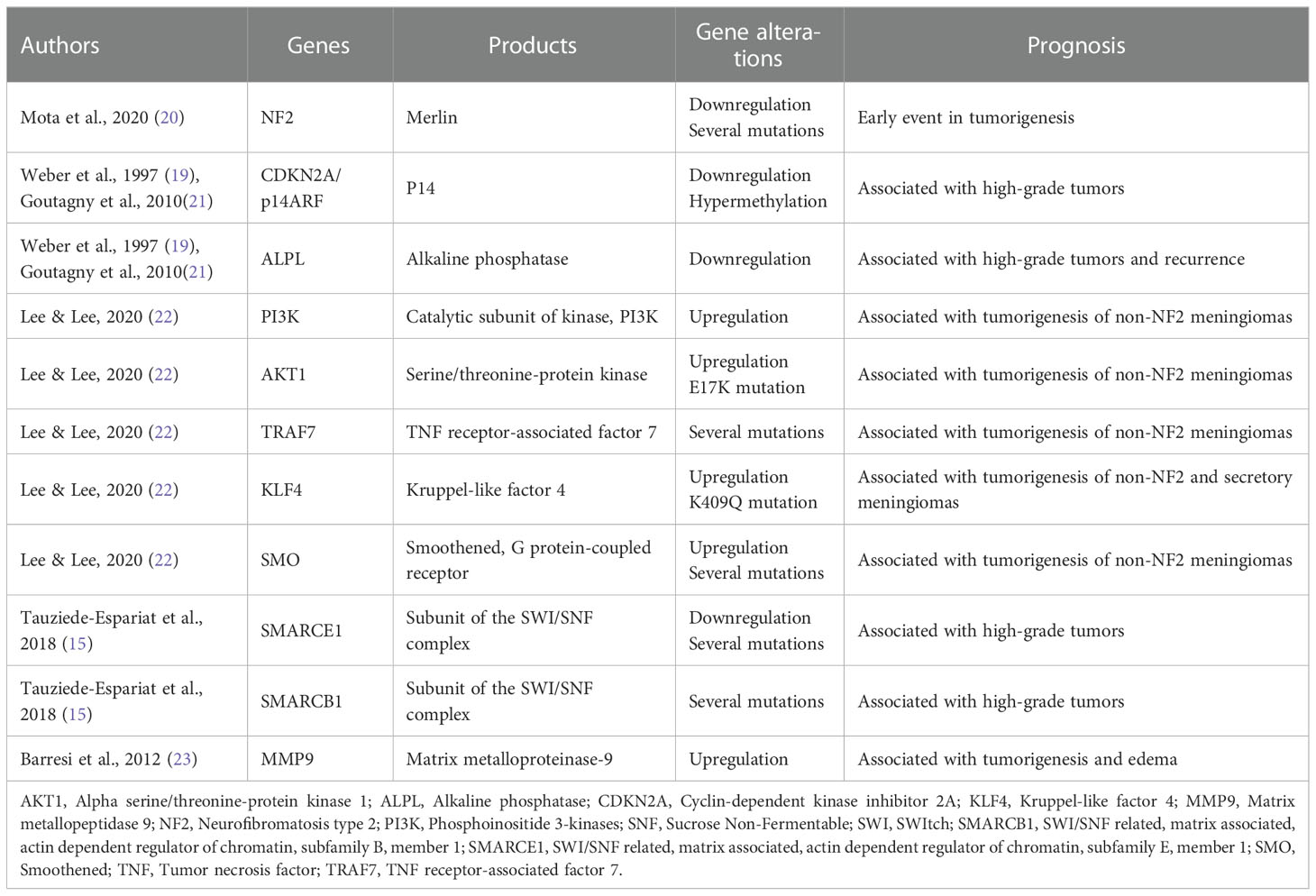
Table 2 Main molecular alteration and their prognosis in meningiomas.
Among the multiple mechanisms of oncogenesis, the increased cell proliferation was considered as the most important one. In brain tumors, the typical immunohistochemically marker Ki-67/MIB-1 for cell proliferation is more predictive of survival than the expression of proliferating cell nuclear antigens p53 and PCNA. In meningiomas, a high expression level of Ki-67 is directly associated with significant worse prognostic, especially with Ki-67 index higher than 4% (24). A close follow-up is recommended in this population.
Chromosomal abnormalities
Among the chromosomal abnormalities found to be related to spinal meningiomas, chromosomal 22q deletion seems to be the most important one (25). In addition, one study on sixteen patients with spinal meningiomas showed an allelic loss of the 1p chromosomal arm - involving several genes such as the ALPL (Alkaline phosphatase) gene - and a homozygous loss of 9p that results in inactivation of tumor suppressor genes such as the CDKN2A (Cyclin-dependent kinase inhibitor 2A) (19, 21). Other chromosomal abnormalities have also been described, such as the loss of 10q and the gain of 5p and 17q (26).
NF2-mutated meningiomas
In Schwann cells, the NF2 gene on chromosome 22q12.2 leads to the production of merlin, a protein also known as schwannomine, that provides myelin insulation for nerves. Merlin is also involved in the regulation of several key signaling pathways implied in cytoskeletal remodeling and cell motility. In addition, this protein is a tumor suppressor that prevents cell proliferation (20). The loss of merlin expression is characteristic of all NF2-associated meningiomas and nearly half of sporadic cases. Mutations in the NF2 gene produce an abnormally shortened protein altering its functional condition (20). NF2 mutation is also known to activate several oncogenic signaling pathways such as PI3K/AKT1 (20).
NF2-non-mutated meningiomas
Approximately 40% of sporadic meningiomas are independent of NF2 inactivation and are linked to other mutations discovered in high-throughput sequencing studies of large cohorts of meningiomas (27). For grade I meningiomas, mutations in AKT1 (v-akt murine thymoma viral oncogene homolog 1, leading to activation of the PI3K pathway), TRAF7 (Tumor necrosis factor receptor-associated factor 7, encoding the pro-apoptotic E3 ubiquitin ligase), KLF4 (Krupple-like factor 4, a pluripotency-inducing transcription factor) and SMO (Smoothened, frizzled family receptor, leading to activation of the Hedgehog pathway) have been identified and appear to be mutually exclusive of NF2 alterations (22). In addition, mutations in the SMARCE1 gene (SWI/SNF related, matrix associated, actin dependent regulator of chromatin, subfamily E, member 1) have been reported in clear cell meningioma, and mutations in the SMARCB1 gene (SWI/SNF related, matrix associated, actin dependent regulator of chromatin, subfamily B, member 1) are involved in multiple meningiomas. These mutations are further associated with tumor location and histological subtype (Tauziede-Espariat et al., 2017). In spinal schwannoma, one study reported a mutation in the large tumor suppressor kinase 1 gene (LATS1), a downstream mediator of NF2, but the clinical relevance of these alterations remains unknown in spinal meningiomas (28).
Other additional mutations
Comparative microarray analysis between spinal and intracranial meningiomas confirmed that spinal meningiomas are associated to a higher rate of chromosome 22 deletion (23). Moreover, 35 genes out of 1555 reported were more highly expressed in spinal than in intracranial meningiomas (23). Barresi et al. reported that spinal meningiomas showed an increased expression of the matrix metalloproteinase family, a group of proteins also involved in cell growth and invasion (23).
Meningiomas and sex hormones
Multiple reasons suggest the association between sexual hormones and the development of meningiomas. Meningiomas are more common in females, even more for spinal meningiomas than intracranial meningiomas, and are positively correlated with breast cancer (29, 30). Most meningiomas express progesterone and somatostatin receptors (31). Spinal meningiomas expressed more androgen receptors (AR+) and estrogen receptors (ER+) than intracranial meningiomas (30).
Many studies have investigated the impact of sex hormone medication, such as oral contraception or hormonal replacement therapy (HRT), on meningiomas development. Results were inconclusive still recently (32–34). A dose-dependent relationship between the incidence and growth of meningiomas and hormonal treatment with progestin cyproterone acetate (CPA) has recently been established (35). A similar but lower risk of meningiomas has been recently reported with the use of chlormadinone acetate and nomegestrol acetate as progestin treatments (35).
Concerning HRT in menopausal patients, evidence from epidemiological studies seem to favor an increased risk of meningiomas in treated patients although a recent study failed to show an increased growth of meningiomas in HRT treated vs. nontreated patients (36). Until larger studies are available, it seems wise to recommend avoiding HRT in patients with meningiomas (37).
Based on studies demonstrating the expression of hormonal receptors in meningiomas, therapies targeting these receptors have been tried but have failed to show an overall favorable clinical outcome in meningioma treatment (37).
To the best of our knowledge, there are no published data on spinal meningiomas in pregnant women. However, data arising from intracranial meningiomas research suggest that the latter may enlarge during pregnancy, as noted by Cushing and Eisenhardt (38). But the rarity of this condition does not allow to clearly define the risk and the need for surgery during pregnancy. Usually, urgent neurosurgery can be indicated during pregnancy in case of neurological symptoms such as motor deficit or visual impairment (39, 40). For asymptomatic meningiomas, a multidisciplinary approach is always useful to better evaluate the pros and cons of surgery during pregnancy and following management both for maternal and fetal health, the aim being, as far as possible, to organize the surgery away from childbirth (41).
Neuroimaging
Magnetic resonance imaging aspect
Magnetic resonance imaging (MRI) is currently the preferred diagnostic modality of intradural spinal tumors (Figure 3). On MRI, most spinal meningiomas show intermediate to hypo intensity on T1-weighted images (WI) and are iso- to hyperintense on T2-WI (42, 43). In fact, on T2-WI, these tumors present with a higher signal than the spinal cord but a lower signal than the surrounding fat tissue (44). They are usually well-circumscribed, with an intermediate to strong homogeneous enhancement after gadolinium injection (45). Tumors with heterogeneous enhancement seldom present with a decreased intratumoral signal on T2-WI due to calcifications, hemorrhage, or necrosis (46).
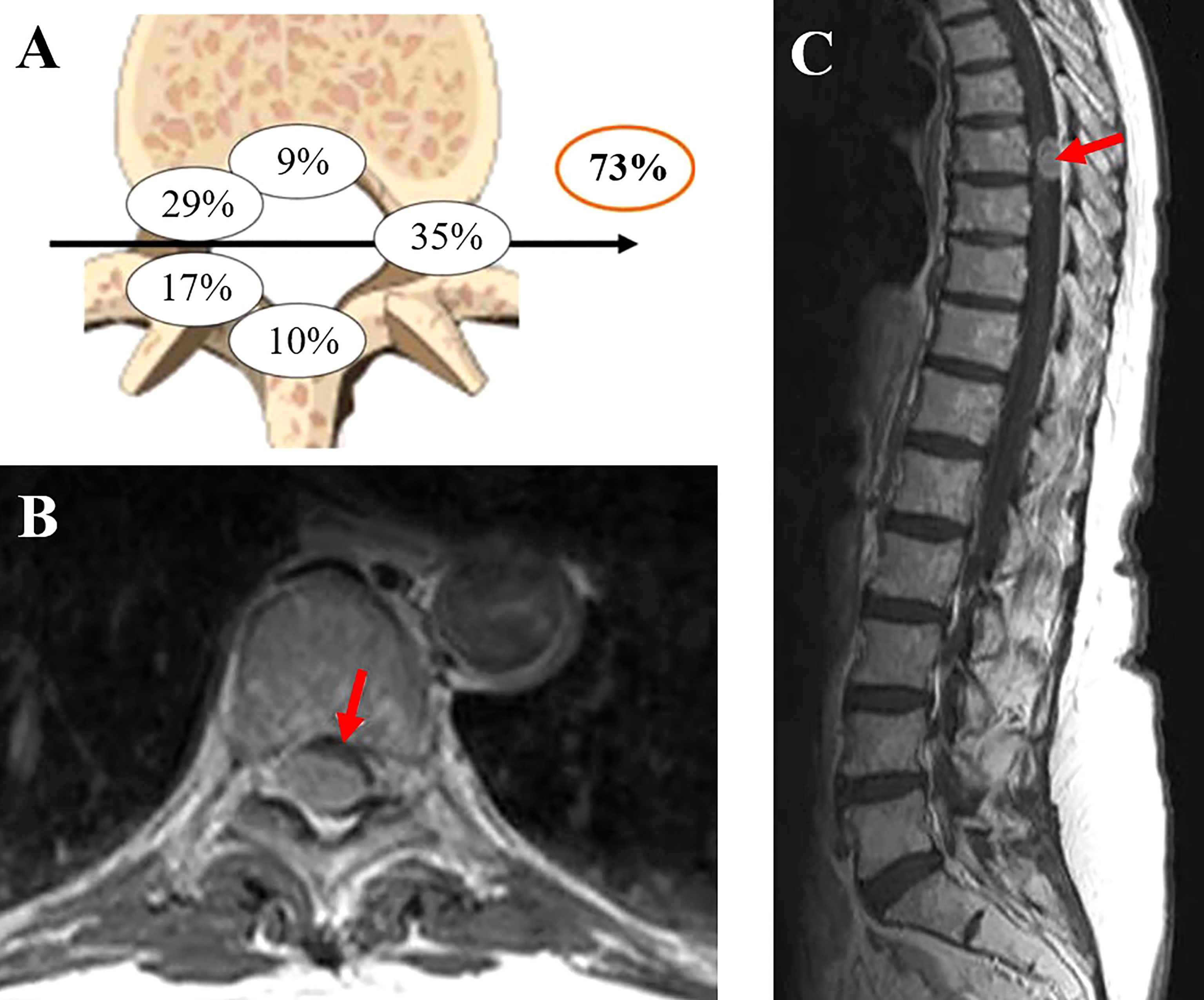
Figure 3 (A) Localization of the dural attachment (73% located ventrally to the dentate ligament). (B, C) Spinal meningioma aspects on MRI. The figure is adapted from reference 4 and reproduced with permission from SNCSC.
Intratumoral calcifications are reported in less than 5% of spinal meningiomas (46) but are associated with poor functional outcomes after surgical resection (4).
Characteristic radiological features
As previously mentioned, spinal meningiomas are most commonly found in the thoracic region, in the lateral and anterolateral aspects of the spinal cord (in front of the denticulate ligament). Although a dural tail is a characteristic feature of meningiomas, it is less frequently seen in spinal than in cranial meningiomas (47).
Radiological classification
Yeo et al. classify spinal meningiomas into four categories depending on their MRI appearance (44): Type A includes tumors with a dural attachment (with and without dural tail) that shows homogeneous enhancement after gadolinium injection; type B consists of oval-shaped tumors with hypo intense component on T2WI; type C consists of “en plaque” meningioma, that grows in a diffuse sheet-like aspect along with the dura mater; and type D for the rest of spinal meningiomas that could not type A, B nor C.
A unique presentation of “en plaque” meningioma
“En plaque” or type C meningioma is a subgroup of spinal meningiomas. It is frequently associated with intramedullary signal changes on T2WI (44), although myelomalacia is a rare finding in spinal meningiomas (47). Moreover, type C meningioma has a larger size at diagnosis compared to well-encapsulated tumors (44). Thus, it has an increased risk of worse surgical outcomes, with postoperative arachnoiditis and higher recurrence rates after surgical resection. This might be explained by the diffuse growth pattern of these tumors, which delays clinical manifestations (44).
Observation
More available neuroimaging modalities as MRI scans facilitated the discovery of incidental meningiomas. These lesions represent of 0.9% to 1.0% of the general population (48). Depending on the growth of the lesions, a follow-up plan is set for every individual patient. Presently, it is agreed that annual MRI scans are recommended in meningiomas of WHO grade 1 for five years. After that period, biannual MRIs can be performed.
During pregnancy, a close follow-up is recommended in patients known to have meningiomas (40).
Management
Unlike intracranial meningiomas, spinal meningiomas do not generally invade the pia and rarely result in spinal cord edema, compared to small intracranial meningiomas that can cause significant vasogenic edema thus becoming symptomatic (49). Spinal meningiomas tend to manifest clinically once they exhibit a direct mass effect on the neural elements (50). For incidentally discovered meningiomas, clinical and radiographical observation is essential to select the best management strategy, even in the case of a documented tumor growing on serial imaging. Several factors should be considered in asymptomatic spinal meningioma before proposing tumor resection. Those factors include the patient’s age, comorbidities, and tumor size.
Surgery
Surgery is the gold standard therapy for spinal meningiomas (51). Pseudomeningoceles or CSF leakage are the most common complications occurring in nearly 4% of cases (52). In neurosurgical practice, spinal meningiomas location and growing patterns may affect surgical results (9). The tumor location in the canal was classified into four types depending on the location of the dural attachment of the tumor and their shape (53): dorsal, lateral and ventral; dumbbell-shaped spinal meningioma being extremely rare. Ventrally attached large tumors causing spinal cord signal changes are linked with poor functional outcomes and increased risk of spinal cord traction during surgery. Severe preoperative impairment (McCormick grades III, IV, and V) that may reflect the plasticity and a vulnerable spinal cord, is significantly related to neurological deterioration postoperatively (54). Location of the meningioma throughout the spine is also important, as lumbar location gives more freedom for gross total resection (GTR) than dorsal or cervical locations, due to the absence of the spinal cord. Thoracic location is most critical as the vascularization of the spinal cord is frail (54).
Surgical removal of dorsal or lateral lesions is usually not difficult, and complete surgical resection can be achieved in 97% of cases (13). Ventrally located are less accessible, and “en plaque” meningiomas may not be removed totally (9).
A posterior midline approach with laminectomy can be used in the majority of dorsal or dorsolateral spinal meningiomas. Bilateral laminectomy, one level above and below the lesion, is usually sufficient for exposure in open surgery for small lesions (6, 55). The integrity of the surrounding vertebral structures should be mandatory to preserve biochemical stability, especially in cases of multilevel laminectomy or facet join disruption (56).
Anterior or anterolateral approaches are exceptional (56, 57), and must be reserved to complex anterior spinal meningiomas, because complications are more frequent, especially for CSF leakage (58). These techniques generally require a corpectomy, preferably with a unilateral approach, which implies a complementary vertebral fixation and fusion for the preservation of biomechanical stability. In some cases of anterolateral localization, when costotransversectomy and pediculectomy are needed to safely access the spinal canal and expose the lateral and anterior parts of the tumor, unilateral instrumented fusion should be done.
Excision of spinal meningiomas follows the Simpson grading (Table 3) regarding the totality of the resection and the treatment of the dural tail attachment (59). One of the most critical surgical steps is to define a dissection plane between the lesion and the neural elements. To access to the anterior compartment, it might be required to separate the dentate ligaments during debulking to ensure a convenient area of manipulation of the spinal cord (7). Tumor excision is accomplished using micro scissors, rongeurs, bipolar cauterization and/or ultrasonic cavitation aspirator (7, 55). Hemostasis of the epidural plexus can be achieved using surgical compression, low-intensity electrocoagulation, or hemostatic agents (55). Dural attachment resection with a patch graft suturing must be systematically performed to limit postoperative complications such as pseudomeningoceles or CSF leakage (52, 60). Finally, Kaplan-Meier survival curves showed that there is no significant difference between Simpson grade I and II, grade II GTR is more convenient in difficult surgical cases where access is difficult and risky (54).
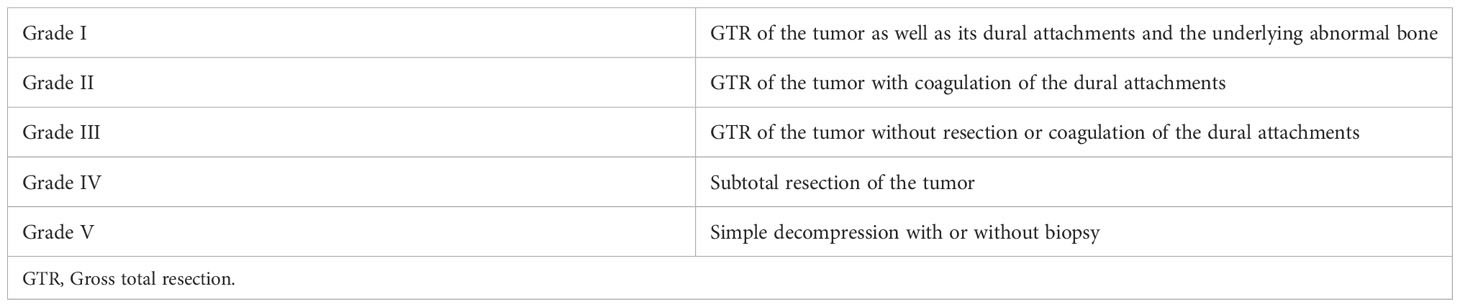
Table 3 Simpson grading in meningiomas.
Minimally-invasive techniques
In 2006, Tredway et al. reported operative success using a mini-invasive hemilaminectomy technique with a tubular retractor system (55), allowing to less manipulation of the spinal cord, thus maintaining vertebral stability, decreasing blood loss and reducing hospitalization period. Since then, numerous reports have confirmed the feasibility and safety of MIS for spinal meningiomas. However, this type of approach can only be used for small lesions limited to maximum two vertebral levels (55), and must be offered to elderly and fragile patients when possible (61). However, there is still not enough evidence to recommend MIS techniques over the classical open surgery (62), because the studies advocating for MIS had small sample sizes and mixed extra- and intra-medullary tumors, resulting in confounding biases. More inspections are needed in the near future to establish specified criteria and indications for the proper usage of MIS in the treatment of spinal meningiomas.
Intraoperative monitoring
Spinal surgery has little margin for error. Therefore, all means must be deployed to preserve the functioning of the spinal pathways and reduce the postsurgical neurological deficit. For this purpose, intraoperative neurophysiological monitoring was first introduced in 1975 by Tamaki and Yamane and has been widely used by spinal surgeons to provide information regarding the extent of tissue manipulation, tissue resection, and preservation of spinal tracts function (2, 56).
Motor evoked potentials (MEP) and somatosensory evoked potentials (SEP) are the two main neuromonitoring tools used during surgery. MEP explore the integrity of the pyramidal tracts and are primarily used in the context of anterior and anterolateral spinal lesions. SEP examine the dorsal columns and are thus mainly used in the case of posterior and posterolateral spinal lesions. The two modalities are frequently combined and offer quick and valuable surgical feedback. Intraoperative SEP and/or MEP deterioration prompt rapid surgical intervention and prevent irreversible sensory and motor pathways damage.
MEP requires stimulation of the pyramidal tracts and response recording through surface electrodes placed over a muscle of interest (for instance, intrinsic hand muscles or tibialis anterior muscle) (63–66). Direct spinal stimulation could elicit muscle responses and has been used by several groups worldwide. However, it is now known that the obtained responses could not accurately reflect the functioning and integrity of central motor pathways. Although these motor responses translate the firing of lower motor neurons, they result from the activation of various spinal tracts, including antidromic activation of dorsal column axons that have collaterals with lower motor neurons (67). Therefore, brain stimulation is recommended to monitor the integrity of corticospinal (pyramidal) tracts (64).
Brain activation could be obtained by applying magnetic or electric stimulation to the scalp. For intraoperative monitoring, electric currents are by far more practical than the magnetic field. They are delivered to the brain through “corkscrew” needles, straight needles, or surface electrodes. The latter consists of electroencephalographic (EEG) cups that could be securely fixed on the scalp (before surgery) using collodium. Anodal stimulation was more efficient than cathodal stimulation in evoking MEP. Stimulating electrodes are placed at specific sites over the motor cortex, such as C3, C4, C1, C2, Cz - 1 cm, and Cz + 6 cm (according to the 10-20 international system of electrode placement). Several montages have been proposed, like hemispheric, interhemispheric, and midline (for review, please refer to 64); each has its advantages and inconveniences that fall outside the scope of this paper and will not be discussed here.
As for SEP, this technique requires stimulation of a peripheral nerve of the upper or lower limb and response recording through electrodes positioned over the primary sensory cortex (65). Recording electrodes consist of either EEG cup electrodes fixed to the scalp using collodium or subcutaneous needle electrodes. The latter provide rapid positioning but could increase the risk of local infection or subcutaneous hemorrhage.
Concerning stimulation, median and posterior tibial nerves are usually used; other peripheral nerves can also be stimulated in certain circumstances; for instance, the ulnar nerve is chosen in lower cervical interventions. The stimuli are rectangular, of 0.2 to 0.3 ms duration, and supramaximal intensity. The latter corresponds to two times the motor threshold or three times the sensory threshold (65).
For both techniques, qualified and experimented personnel is needed to accurately detect any changes in SEP or MEP response, distinguish it from any confounder, and warn the surgical team.
Metastatic spinal meningiomas
The literature regarding spinal meningiomas metastasis is lacking. However, according to data arising from intracranial meningiomas research, extracranial meningioma metastases (EMM) occur in 0.1% of intracranial meningiomas mainly encountered in atypical and anaplastic lesions. Most common sites of metastasis are the lungs and pleura but intraspinal and vertebral EMM also occur in a lesser percentage and are poorly described in the literature. There is no standard treatment protocol for EMM although their presence might worsen the prognosis of the concerned patients (68). EMM occurrence is independent of WHO grading and can be even present before tumor recurrence.
Tumor recurrence
As stated previously, spinal meningiomas are benign tumors with a low recurrence rate independently of the histological grade of the cancer. In general, the recurrence rate in spinal meningiomas tend to be less than in intracranial meningiomas. The recurrence/progression of meningiomas after ten years can reach 13% (2, 69). The incidence was lower for convexity lesions (3%) than parasagittal (18%) and sphenoid ridge (34%) meningiomas. Multiple demographic, clinical and radiological factors have been associated with increased recurrence rates, such as patient age (recurrence rate higher in young patients (below 50)), tumor location (cervical), infiltrating meningioma, En plaque growth, extradural extension, arachnoid scarring, and partial resection (Simpson IV-V grades). Moreover, a recent series reported by Park et al. found that foraminal and thoracic location is associated with a higher recurrence rate (70).
In addition, histological types seem to influence the recurrence risk; for instance, spinal clear cell meningioma was found to have a greater recurrence rate (10).
The importance of dural attachment resection is controversial and contrasting results have been described. For instance, Nakamura et al. found that the recurrence rate was lower for Simpson Grade I than for Simpson Grade II resection (53). In contrast, a low recurrence rate can be found even without dural resection (71). In the same perspective, the add-on value of including the dural tail in the field of radiation therapy is still undetermined. Some data come from the domain of intracranial meningioma, where the radiation of the dural attachment was not found to be beneficial (i.e., it did not reduce the recurrence rate) in a large retrospective series recently reported by Piper etal. (72). A better understanding of the dural tail (or dural attachment) pathophysiology is needed to guide and improve the management of this cancer.
Functional outcomes and complications
Spinal meningiomas are frequently associated with a favorable neurological and functional prognosis (4, 73, 74).
The patients who underwent surgical decompression experienced significant post-operative improvements in Patient Reported Outcomes as measured by the Brief Pain Index and MD Anderson Symptom Inventory (75). However, anterior or calcified lesions, recurrences, cases in which the arachnoid layer has been violated, tumors invading the spinal cord and/or the vascular structures do not have the same favorable outcome (74). Therefore, the preoperative functional and neurological evaluation using the Frankel and the McCormick scales should be carried out before and after surgery (Tables 4, 5). Complications are present due to neurological worsening that can be caused by the surgery itself. This includes spinal epidural hematoma, CSF leakage with or without deep or superficial infections, syringomyelia, and iatrogenic instability (4, 73, 76). In the event of early postoperative neurological deterioration, epidural hematoma should be suspected, and an emergent MRI obtained, in order to rule out this complication, the other possibility being spinal cord ischemia or edema. Epidural hematoma should be evacuated in an urgent manner to obtain rapid and total neurological recovery. In the absence of epidural hematoma and the presence of spinal cord edema, high-dose intravenous steroids should be administered. There are no exact percentages in the literature for these postoperative complications, but all publications agree on their rarity and (i.e., below 5% of cases). CSF leakage is treated by lumbar drainage for 4-5 days and usually resolves without surgical revision. Superficial and deep infections are rare and must be treated with antibiotic therapy and surgical revision when required. Syringomyelia is a late onset complication. If chronic neurological impairment is attributed to the development of the evolving syrinx, subarachnoidal shunting of the cavity through an intracystic catheter should be considered. This complication is usually of bad prognosis. Iatrogenic instability should be considered mainly when back pain remains an issue with the appearance of local kyphosis on control imaging. Instrumented fusion should be considered. It could be done through a minimally invasive navigated percutaneous approach.
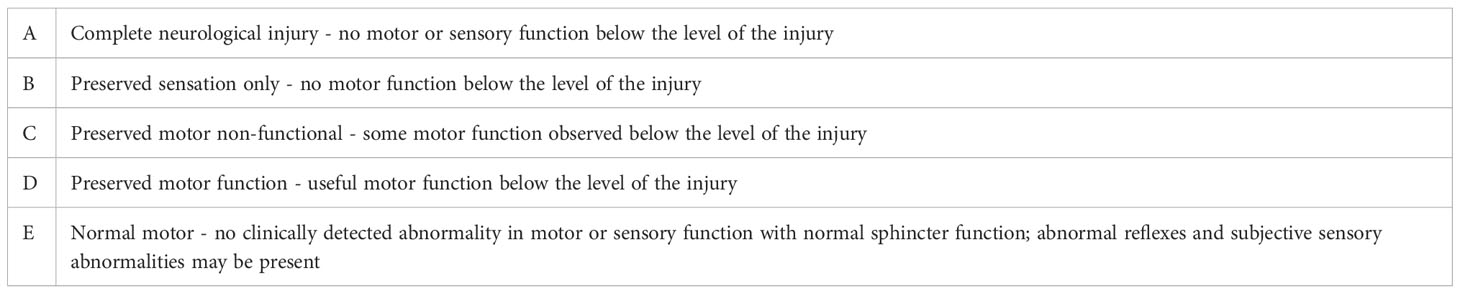
Table 4 Frankel scale evaluating functional outcomes in spinal cord injuries.
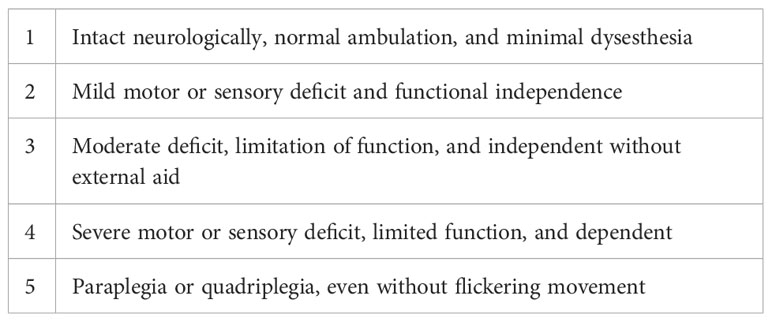
Table 5 McCormick scale evaluating neurological outcomes in spinal cord injuries.
Adjuvant therapy
Surgery remains the primary treatment modality for spinal meningiomas, although radiotherapy may be used as an adjuvant treatment in some cases.
Postoperative radiotherapy role is not well understood yet (14). Radiotherapy and radiosurgery are the two best substitutes for surgery in specific situations described in the literature (77–79).
Both therapeutic strategies are depicted in Table 6. Patients with WHO grade 1 meningiomas do not necessarily need adjuvant treatment after resection that might be sufficient for short-term tumor control (80).
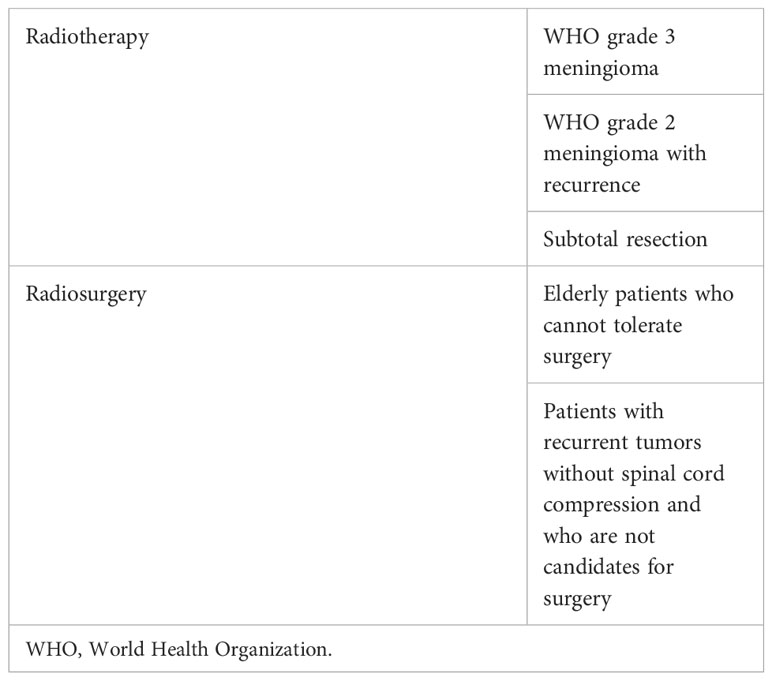
Table 6 Indication for adjuvant treatment in spinal meningiomas.
Upfront radiosurgery is usually not an option, given that small, non-compressive lesions usually require a close observation strategy, and large symptomatic lesions should undergo surgery. It may be used in fragile patients who cannot be operated. In addition, a 2-3 mm margin between the meningioma and the spinal cord is required for an effective tumoricidal dose (81). Thus, stereotactic body radiation therapy (SBRT) can be proposed for operated patients within a safe margin. The definitive SBRT dose consisted of delivering 21 Gray in three fractions. Five-year control rates with stereotactic therapy for meningiomas, varied between 70% and 100% (82). Adjuvant therapy can also be considered in WHO grade 3 meningiomas, given that these lesions are more aggressive and have a higher recurrence rate (83). Image-modulated radiation therapy (IMRT) and conventional fractionated radiation therapy have also been used to treat spinal meningioma, but SBRT is the preferred modality (77).
Chemotherapy is not used in the management of spinal meningiomas. In invasive atypical meningiomas (WHO grade 3), multiple agents have been used, including hydroxyurea, interferon α-2B, long-acting Sandostatin, and even multidrug sarcoma protocols (84). Chemotherapy can also have a role as a salvage therapy in cases of highly aggressive tumors.
Specific situation: Spinal meingioma in pediatric population
When a spinal meningioma is diagnosed in children, a strictly follow-up must be adopted because of the high risk of developing other tumors, particularly in the context of NF2 (52). Complete surgical resection is the primary treatment modality of spinal meningiomas (85). Adjuvant radiotherapy should be recommended only for children with recurrence (85).
Psycho-oncological aspects
Neuropsychiatric symptoms could be observed in oncology wards, including neuro-oncology. They could result either from the direct effect of the tumoral processes affecting the CNS (such in the case of intracranial meningiomas) and/or secondary to the stressful events or the adjustment processes that arise from the announcement of potentially life-threatening conditions and the related workup, surgical interventions, prognosis, and follow-up (86–88). Although these manifestations might affect patients with meningiomas, as in those with other tumors, they remain overlooked and sometimes forgotten. The majority of the few available studies published on this matter focused on intracranial meningiomas and reported the frequent occurrence of fatigue, anxiety, and depression symptoms (89, 90), as well as the lack of effect of pharmacological therapies (Methylphenidate or Modafinil) on these symptoms, compared to placebo in the randomized clinical trials that recruited patients with primary brain tumors including meningiomas (91, 92).
Fewer data are available on this matter in spinal meningiomas and involve anxiety, depression, and quality of life. For instance, in one study that considered patients with intradural extramedullary spinal tumors (of which 31.8% were meningiomas), some (50%) or extreme (14.3%) problems with anxiety and depression according to a quality-of-life questionnaire (EQ-5D-3L) were reported before the surgical intervention; the rates started to decrease from less than 1-month following the surgery to 3-12 months later, but they increased back to baseline values after one-year follow-up (93). Moreover, in another study involving patients with intradural extramedullary spinal tumors, of which 4.2% had meningiomas, 22.9% met the diagnostic and statistical manual of mental disorder criteria (DSM IV-TR) of a psychiatric disorder. In comparison, 37.5% and 12.5% of patients had mild and moderate depression symptoms according to Beck Depression Inventory, respectively (94). Furthermore, in a third study that addressed the previous limitation by including a homogeneous cohort of patients with spinal meningiomas (n=84), some or extreme problems with anxiety and depression were reported by 31% and 3.6% of patients, respectively, according to a quality-of-life questionnaire (EQ-5D-3L; 95). Here, no significant differences in problems related to anxiety and depression were found in gender or neurological status.
These facts warrant more research to further understand this clinical population’s affective and cognitive outcomes. A thorough investigation of these variables would help to (a) understand such outcomes (depression and anxiety symptoms, fear of recurrence, fatigue, coping strategies) and their clinical predictors, (b) subsequently develop specific screening tools to quantify the symptoms and identify patients at risk, and (c) implement psycho-oncological interventions that could be ideally offered in a patient-tailored manner (psychoeducation, psychosocial support, pharmacotherapeutics or psychotherapies if justified) (96). Lastly, informal caregivers of patients with spinal meningiomas seem to be still forgotten (97), and future studies are needed to evaluate and help these “hidden patients” (98), which might contribute to its turn in improving patients’ outcomes.
Conclusion
Spinal meningiomas are intradural, slow-growing tumors, classified as a WHO grade 1 lesion in more than 70% of the cases. There is no histological difference between spinal and intracranial meningiomas.
Since intradural spinal tumors are not frequent, multicenter studies are required to fully understand and materialize the promise of targeted genetic therapies that will widen the treatment options in the future with a better clinical decision-making.
Observation should be implemented when suitable. Surgical treatment is the gold standard solution, with a principal goal of a GTR (Simpson grade I). If this GTR cannot be achieved, a SIMPSON II is advised, if possible, given the low recurrence rates. In cases of the ventral tumor where GTR is hardly achievable, small amounts of the tumor should be left. If interval growth is seen, the residual tumor can be observed and/or treated with adjuvant therapy, mainly SBRT.
Advances in surgical approaches, especially endoscopic and minimally invasive techniques, are still ongoing to minimize the risks with a better postoperative prognosis with a complete resection as a primary treatment modality.
Psycho-oncological interventions might be beneficial in patients presenting with spinal meningiomas. More research is needed to optimize screening and support patients and their informal caregivers.
Author contributions
SA and GL: Conceptualization and methodology. NS, IL, CA, BT, FN, JF, JM, MC, RB-N and YA: Data analysis, writing-original draft preparation. MC and SA: Review and editing. SA and GL: supervision. All authors contributed to the article and approved the submitted version.
Conflict of interest
SA declares having received compensation from ExoNeural Network AB, Sweden. MC declares having received compensation from Janssen Global Services LLC, ExoNeural Network AB, Sweden, and Ottobock, France.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AKT1, alpha serine/threonine-protein kinase 1; ALPL, alkaline phosphatase; AR, androgen receptors; CCA, chlormadinone acetate; CDKN2A, cyclin-dependent kinase inhibitor 2A; CNS, central nervous system; CPA, cyproterone acetate; CSF, cerebrospinal fluid; e.g., exempli gratia; EMM, extracranial meningioma metastases; ER, estrogen receptor; GTR, gross total resection; HRT, hormonal replacement therapy; i.e., id est; IMRT, image-modulated radiation therapy; KLF4, Kruppel like factor 4; LATS1, large tumor suppressor kinase 1; MEP, motor evoked potentials; MIS, minimally invasive surgery; MMP9, matrix metallopeptidase 9; MRI, magnetic resonance imaging; NF2, neurofibromatosis type 2; PCNA, proliferating cell nuclear antigen; PI3K, phosphoinositide 3-kinases; SBRT, stereotactic body radiation therapy; SEP, somatosensory evoked potentials; SMARCB1, SWI/SNF related, matrix associated, actin dependent regulator of chromatin, subfamily B, member 1; SMARCE1, SWI/SNF related, matrix associated, actin dependent regulator of chromatin, subfamily E, member 1; SMO, smoothened; T1-WI, T1-weighted images; T2-WI, T2-weighted images; TRAF7, TNF receptor-associated factor 7; vs., versus; WHO, World Health Organization.
References
1. Perry A, Gutmann DH, Reifenberger G. Molecular pathogenesis of meningiomas. J Neurooncol. (2004) 70(2):183–202. doi: 10.1007/s11060-004-2749-0
2. Ravindra VM, Schmidt MH. Management of spinal meningiomas. Neurosurg Clin N. Am (2016) 27(2):195–205. doi: 10.1016/j.nec.2015.11.010
3. Saraceni C, Harrop JS. Spinal meningioma: chronicles of contemporary neurosurgical diagnosis and management. Clin Neurol Neurosurg (2009) 111(3):221–6. doi: 10.1016/j.clineuro.2008.10.018
4. Sandalcioglu IE, Hunold A, Müller O, Bassiouni H, Stolke D, Asgari S. Spinal meningiomas: critical review of 131 surgically treated patients. Eur Spine J (2008) 17(8):1035–41. doi: 10.1007/s00586-008-0685-y
5. Arima H, Takami T, Yamagata T, Naito K, Abe J, Shimokawa N, et al. Surgical management of spinal meningiomas: A retrospective case analysis based on preoperative surgical grade. Surg Neurol Int (2014) 5(Suppl 7):S333–8. doi: 10.4103/2152-7806.139642
6. Parsa AT, Lee J, Parney IF, Weinstein P, McCormick PC, Ames C. Spinal cord and intradural-extraparenchymal spinal tumors: current best care practices and strategies. J Neurooncol. (2004) 69(1-3):291–318. doi: 10.1023/b:neon.0000041889.71136.62
7. Gottfried ON, Gluf W, Quinones-Hinojosa A, Kan P, Schmidt MH. Spinal meningiomas: surgical management and outcome. Neurosurg Focus. (2003) 14(6):e2. doi: 10.3171/foc.2003.14.6.2
8. Engelhard HH, Villano JL, Porter KR, Stewart AK, Barua M, Barker FG, et al. Clinical presentation, histology, and treatment in 430 patients with primary tumors of the spinal cord, spinal meninges, or cauda equina. J Neurosurg Spine. (2010) 13(1):67–77. doi: 10.3171/2010.3.SPINE09430
9. Postalci L, Tugcu B, Gungor A, Guclu G. Spinal meningiomas: recurrence in ventrally located individuals on long-term follow-up; a review of 46 operated cases. Turk. Neurosurg (2011) 21(4):449–53.
10. Zhang H, Ma L, Shu C, Dong LQ, Ma YQ, Zhou Y. Spinal clear cell meningiomas: Clinical features and factors predicting recurrence. World Neurosurg (2020) 134:e1062–76. doi: 10.1016/j.wneu.2019.11.093
11. Riad H, Knafo S, Segnarbieux F, Lonjon N. Spinal meningiomas: surgical outcome and literature review. Neurochirurgie. (2013) 59(1):30–4. doi: 10.1016/j.neuchi.2012.10.137
13. Solero CL, Fornari M, Giombini S, Lasio G, Oliveri G, Cimino C, et al. Spinal meningiomas: review of 174 operated cases. Neurosurgery. (1989) 25(2):153–60.
14. Gezen F, Kahraman S, Canakci Z, Bedük A. Review of 36 cases of spinal cord meningioma. Spine (2000) 25(6):727–31. doi: 10.1097/00007632-200003150-00013
15. Cohen-Gadol AA, Zikel OM, Koch CA, Scheithauer BW, Krauss WE. Spinal meningiomas in patients younger than 50 years of age: a 21-year experience. J Neurosurg (2003) 98(3 Suppl):258–63.
16. Birzu C, Peyre M, Sahm F. Molecular alterations in meningioma: prognostic and therapeutic perspectives. Curr Opin Oncol (2020) 32(6):613–22. doi: 10.1097/CCO.0000000000000687
17. Holleczek B, Zampella D, Urbschat S, Sahm F, von Deimling A, Oertel J, et al. Incidence, mortality and outcome of meningiomas: A population-based study from Germany. Cancer Epidemiol. (2019) 62:101562. doi: 10.1016/j.canep.2019.07.001
18. Moussalem C, Massaad E, Minassian GB, Ftouni L, Bsat S, Houshiemy MNE, et al. Meningioma genomics: a therapeutic challenge for clinicians. J Integr Neurosci (2021) 20(2):463–9. doi: 10.31083/j.jin2002049
19. Weber RG, Boström J, Wolter M, Baudis M, Collins VP, Reifenberger G, et al. Analysis of genomic alterations in benign, atypical, and anaplastic meningiomas: toward a genetic model of meningioma progression. Proc Natl Acad Sci U. S. A. (1997) 94(26):14719–24. doi: 10.1073/pnas.94.26.14719
20. Mota M, Shevde LA. Merlin regulates signaling events at the nexus of development and cancer. Cell Commun Signal (2020) 18(1):63. doi: 10.1186/s12964-020-00544-7
21. Goutagny S, Yang HW, Zucman-Rossi J, Chan J, Dreyfuss JM, Park PJ, et al. Genomic profiling reveals alternative genetic pathways of meningioma malignant progression dependent on the underlying NF2 status. Clin Cancer Res (2010) 16(16):4155–64. doi: 10.1158/1078-0432.CCR-10-0891
22. Lee YS, Lee YS. Molecular characteristics of meningiomas. J Pathol Transl Med (2020) 54(1):45–63. doi: 10.4132/jptm.2019.11.05
23. Barresi V, Alafaci C, Caffo M, Barresi G, Tuccari G. Clinicopathological characteristics, hormone receptor status and matrix metallo-proteinase-9 (MMP-9) immunohistochemical expression in spinal meningiomas. Pathol Res Pract (2012) 208(6):350–5. doi: 10.1016/j.prp.2012.02.013
24. Liu N, Song SY, Jiang JB, Wang TJ, Yan CX. The prognostic role of ki-67/MIB-1 in meningioma: A systematic review with meta-analysis. Med (Baltimore). (2020) 99(9):e18644. doi: 10.1097/MD.0000000000018644
25. Sayagués JM, Tabernero MD, Maíllo A, Trelles O, Espinosa AB, Sarasquete ME, et al. Microarray-based analysis of spinal versus intracranial meningiomas: different clinical, biological, and genetic characteristics associated with distinct patterns of gene expression. J Neuropathol Exp Neurol (2006) 65(5):445–54. doi: 10.1097/01.jnen.0000229234.13372.d8
26. Boetto J, Peyre M, Kalamarides M. Meningiomas from a developmental perspective: exploring the crossroads between meningeal embryology and tumorigenesis. Acta Neurochir. (Wien). (2021) 163(1):57–66. doi: 10.1007/s00701-020-04650w
27. Youngblood MW, Duran D, Montejo JD, Li C, Omay SB, Özduman K, et al. Correlations between genomic subgroup and clinical features in a cohort of more than 3000 meningiomas. J Neurosurg (2019) 25:1–10. doi: 10.3171/2019.8.JNS191266
28. Kim YH, Ohta T, Oh JE, Le Calvez-Kelm F, McKay J, Voegele C, et al. TP53, MSH4, and LATS1 germline mutations in a family with clustering of nervous system tumors. Am J Pathol (2014) 184(9):2374–81. doi: 10.1016/j.ajpath.2014.05.017
29. Ostrom QT, Patil N, Cioffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the united states in 2013-2017. Neuro Oncol (2020) 22(12 Suppl 2):iv1–iv96. doi: 10.1093/neuonc/noaa200
30. Portet S, Banor T, Bousquet J, Simonneau A, Flores M, Ingrand P, et al. New insights into expression of hormonal receptors by meningiomas. World Neurosurg (2020) 140:e87–96. doi: 10.1016/j.wneu.2020.04.168
31. Miyagishima DF, Moliterno J, Claus E, Günel M. Hormone therapies in meningioma-where are we? J Neurooncol. (2022). doi: 10.1007/s11060-022-04187-1
32. Benson VS, Pirie K, Green J, Casabonne D, Beral V, Million Women Study Collaborators. Lifestyle factors and primary glioma and meningioma tumours in the million women study cohort. Br J Cancer. (2008) 99(1):185–90. doi: 10.1038/sj.bjc.6604445
33. Blitshteyn S, Crook JE, Jaeckle KA. Is there an association between meningioma and hormone replacement therapy? J Clin Oncol (2008) 26(2):279–82. doi: 10.1200/JCO.2007.14.2133
34. Benson VS, Kirichek O, Beral V, Green J. Menopausal hormone therapy and central nervous system tumor risk: large UK prospective study and meta-analysis. Int J Cancer. (2015) 136(10):2369–77. doi: 10.1002/ijc.29274
35. Samoyeau T, Provost C, Roux A, Legrand L, Dezamis E, Plu-Bureau G, et al. Meningioma in patients exposed to progestin drugs: results from a real-life screening program. J Neurooncol. (2022) 160(1):127–36. doi: 10.1007/s11060-022-04124-2
36. Dresser L, Yuen CA, Wilmington A, Walker M, Vogel TJ, Merrell RT, et al. Estrogen hormone replacement therapy in incidental intracranial meningioma: a growth-rate analysis. Sci Rep (2020) 10(1):17960. doi: 10.1038/s41598-020-74344-x
37. Hage M, Plesa O, Lemaire I, Raffin Sanson ML. Estrogen and progesterone therapy and meningiomas. Endocrinology (2022) 163(2):bqab259. doi: 10.1210/endocr/bqab259
38. Chakravarthy V, Kaplan B, Gospodarev V, Myers H, De Los Reyes K, Achiriloaie A. Houdini Tumor: Case report and literature review of pregnancy-associated meningioma. World Neurosurg (2018) 114:e1261–5. doi: 10.1016/j.wneu.2018.03.187
39. Antolínez Ayala VE, García Arias MD, Bautista Vargas SE, Báez Cárdenas LM, Castellanos Peñaranda C. Paraplegia due to spinal meningioma during the third trimester of pregnancy: case report and literature review. Spinal. Cord. Ser Cases. (2021) 7(1):31. doi: 10.1038/s41394-020-00368-0
40. Carbone L, Somma T, Iorio GG, Vitulli F, Conforti A, Raffone A, et al. Meningioma during pregnancy: what can influence the management? a case series and review of the literature. J Matern. Fetal. Neonatal. Med (2022) 35(25):8767–77. doi: 10.1080/14767058.2021.2004585.C
41. Dumitru AE, Panaitescu A, Iancu G, Paslaru FG, Paslaru AC, Gorgan RM, et al. Management strategies and clinical follow-up of pregnant women with intracranial meningioma. J Med Life (2021) 14(1):2–6. doi: 10.25122/jml-2021-0012
42. Liu WC, Choi G, Lee SH, Han H, Lee JY, Jeon YH, et al. Radiological findings of spinal schwannomas and meningiomas: focus on discrimination of two disease entities. Eur Radiol (2009) 19(11):2707–15. doi: 10.1007/s00330-009-1466-7
43. Hoover JM, Morris JM, Meyer FB. Use of preoperative magnetic resonance imaging T1 and T2 sequences to determine intraoperative meningioma consistency. Surg Neurol Int (2011) 2:142. doi: 10.4103/2152-7806.85983
44. Yeo Y, Park C, Lee JW, Kang Y, Ahn JM, Kang HS, et al. Magnetic resonance imaging spectrum of spinal meningioma. Clin Imaging. (2019) 55:100–6. doi: 10.1016/j.clinimag.2019.02.007
45. De Verdelhan O, Haegelen C, Carsin-Nicol B, Riffaud L, Amlashi SF, Brassier G, et al. MR imaging features of spinal schwannomas and meningiomas. J Neuroradiol (2005) 32(1):42–9. doi: 10.1016/s0150-9861(05)83021-4
46. Doita M, Harada T, Nishida K, Marui T, Kurosaka M, Yoshiya S. Recurrent calcified spinal meningioma detected by plain radiograph. Spine (2001) 26(11):E249–52. doi: 10.1097/00007632-200106010-00005
47. Abul-Kasim K, Thurnher MM, McKeever P, Sundgren PC. Intradural spinal tumors: current classification and MRI features. Neuroradiology. (2008) 50(4):301–14. doi: 10.1007/s00234-007-0345-7
48. Goldbrunner R, Stavrinou P, Jenkinson MD, Sahm F, Mawrin C, Weber DC, et al. EANO guideline on the diagnosis and management of meningiomas. Neuro Oncol (2021) 23(11):1821–34. doi: 10.1093/neuonc/noab150
49. Hou J, Kshettry VR, Selman WR, Bambakidis NC. Peritumoral brain edema in intracranial meningiomas: the emergence of vascular endothelial growth factor-directed therapy. Neurosurg Focus. (2013) 35(6):E2. doi: 10.3171/2013.8.FOCUS13301
50. Corell A, Cerbach C, Hoefling N, Björkman-Burtscher IM, Jakola AS. Spinal cord compression in relation to clinical symptoms in patients with spinal meningiomas. Clin Neurol Neurosurg (2021) 211:107018. doi: 10.1016/j.clineuro.2021.107018
51. Jecko V, Weller J, Houston D, Champeaux-Depond C. Epidemiology and survival after spinal meningioma surgery: A nationwide population-based study. Asian Spine J (2022). doi: 10.31616/asj.2021.0213
52. Maiti TK, Bir SC, Patra DP, Kalakoti P, Guthikonda B, Nanda A. Spinal meningiomas: clinicoradiological factors predicting recurrence and functional outcome. Neurosurg Focus. (2016) 41(2):E6. doi: 10.3171/2016.5.FOCUS16163
53. Nakamura M, Tsuji O, Fujiyoshi K, Hosogane N, Watanabe K, Tsuji T, et al. Long-term surgical outcomes of spinal meningiomas. Spine (2012) 37(10):E617–23. doi: 10.1097/BRS.0b013e31824167f1
54. Kobayashi K, Ando K, Matsumoto T, Sato K, Kato F, Kanemura T, et al. Clinical features and prognostic factors in spinal meningioma surgery from a multicenter study. Sci Rep (2021) 11:11630. doi: 10.1038/s41598-021-91225-z
55. Tredway TL, Santiago P, Hrubes MR, Song JK, Christie SD, Fessler RG. Minimally invasive resection of intradural-extramedullary spinal neoplasms. Neurosurgery (2006) 58(1 Suppl):ONS52–8. doi: 10.1227/01.neu.0000192661.08192.1c
56. Misra SN, Morgan HW. Avoidance of structural pitfalls in spinal meningioma resection. Neurosurg Focus. (2003) 14(6):e1. doi: 10.3171/foc.2003.14.6.1
57. Payer M. The anterior approach to anterior cervical meningiomas: review illustrated by a case. Acta Neurochir. (Wien). (2005) 147(5):555–60. doi: 10.1007/s00701-005-0502-x
58. Albanese V, Platania N. Spinal intradural extramedullary tumors. personal experience. J Neurosurg Sci (2002) 46(1):18–24.
59. Simpson D. The recurrence of intracranial meningiomas after surgical treatment. J Neurol Neurosurg Psychiatry (1957) 20(1):22–39. doi: 10.1136/jnnp.20.1.22
60. Iacob G. Spinal meningiomas. personal experience and review of literature. Roman. Neurosurg (2014) 21:146–60.
61. Dauleac C, Leroy HA, Karnoub MA, Obled L, Mertens P, Assaker R. Minimally invasive surgery for intradural spinal meningioma: A new standard? a comparative study between minimally invasive and open approaches. Neurochirurgie. (2022) 68(4):379–85. doi: 10.1016/j.neuchi.2022.01.006
62. Caballero-García J, Linares-Benavides YJ, Leitão ULS, Aparicio-García C, López-Sánchez M. Minimally invasive removal of extra- and intradural spinal tumors using full endoscopic visualization. Global Spine J (2022) 12(1):121–9. doi: 10.1177/2192568220948806
63. Groppa S, Oliviero A, Eisen A, Quartarone A, Cohen LG, Mall V, et al. A practical guide to diagnostic transcranial magnetic stimulation: report of an IFCN committee. Clin Neurophysiol (2012) 123(5):858–82. doi: 10.1016/j.clinph.2012.01.010
64. MacDonald DB, Skinner S, Shils J, Yingling C, American Society of Neurophysiological Monitoring. Intraoperative motor evoked potential monitoring - a position statement by the American society of neurophysiological monitoring. Clin Neurophysiol (2013) 124(12):2291–316. doi: 10.1016/j.clinph.2013.07.025
65. MacDonald DB, Dong C, Quatrale R, Sala F, Skinner S, Soto F, et al. Recommendations of the international society of intraoperative neurophysiology for intraoperative somatosensory evoked potentials. Clin Neurophysiol (2019) 130(1):161–79. doi: 10.1016/j.clinph.2018.10.008
66. Rossini PM, Burke D, Chen R, Cohen LG, Daskalakis Z, Di Iorio R, et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. an updated report from an IFCN committee. Clin Neurophysiol (2015) 126(6):1071–107. doi: 10.1016/j.clinph.2015.02.001
67. Langeloo DD, Journée HL, de Kleuver M, Grotenhuis JA. Criteria for transcranial electrical motor evoked potential monitoring during spinal deformity surgery a review and discussion of the literature. Neurophysiol. clinique. = Clin neurophysiol. (2007) 37(6):431–9. doi: 10.1016/j.neucli.2007.07.007
68. Singh R, Ryan C, Chohan MO, Tisnado J, Hadjigeorgiou GF, Bilsky MH. Intracranial meningioma with vertebral or intraspinal metastasis: report of 2 cases and review of the literature. J Neurosurg Spine. (2016) 25(6):775–81. doi: 10.3171/2016.5.SPINE151457
69. Mirimanoff RO, Dosoretz DE, Linggood RM, Ojemann RG, Martuza RL. Meningioma: analysis of recurrence and progression following neurosurgical resection. J Neurosurg (1985) 62(1):18–24. doi: 10.3171/jns.1985.62.1.0018
70. Park BJ, Dougherty MC, Noeller J, Nourski KV, Gold CJ, Menezes AH, et al. Spinal meningioma in adults: Imaging characteristics, surgical outcomes, and risk factors for recurrence. World Neurosurg (2022) 164:e852-e860. doi: 10.1016/j.wneu.2022.05.054
71. King AT, Sharr MM, Gullan RW, Bartlett JR. Spinal meningiomas: a 20-year review. Br J Neurosurg (1998) 12(6):521–6. doi: 10.1080/02688699844367
72. Piper K, Yu S, Taghvaei M, Fernandez C, Mouchtouris N, Smit RD, et al. Radiation of meningioma dural tail may not improve tumor control rates. Front Surg (2022) 9:908745. doi: 10.3389/fsurg.2022.908745
73. Westwick HJ, Yuh SJ, Shamji MF. Complication avoidance in the resection of spinal meningiomas. World Neurosurg (2015) 83(4):627–34. doi: 10.1016/j.wneu.2014.12.015
74. Raco A, Pesce A, Toccaceli G, Domenicucci M, Miscusi M, Delfini R. Factors leading to a poor functional outcome in spinal meningioma surgery: Remarks on 173 cases. Neurosurgery. (2017) 80(4):602–9. doi: 10.1093/neuros/nyw092
75. Newman WC, Berry-Candelario J, Villavieja J, Reiner AS, Bilsky MH, Laufer I, et al. Improvement in quality of life following surgical resection of benign intradural extramedullary tumors: A prospective evaluation of patient-reported outcomes. Neurosurgery. (2021) 88(5):989–95. doi: 10.1093/neuros/nyaa561
76. McGirt MJ, Garcés-Ambrossi GL, Parker SL, Sciubba DM, Bydon A, Wolinksy JP, et al. Short-term progressive spinal deformity following laminoplasty versus laminectomy for resection of intradural spinal tumors: analysis of 238 patients. Neurosurgery. (2010) 66(5):1005–12. doi: 10.1227/01.NEU.0000367721.73220.C9
77. Gerszten PC, Chen S, Quader M, Xu Y, Novotny J Jr, Flickinger JC. Radiosurgery for benign tumors of the spine using the synergy s with cone-beam computed tomography image guidance. J Neurosurg (2012) 117(Suppl):197–202. doi: 10.3171/2012.8.GKS12981
78. Lee KD, DePowell JJ, Air EL, Dwivedi AK, Kendler A, McPherson CM. Atypical meningiomas: is postoperative radiotherapy indicated? Neurosurg Focus. (2013) 35(6):E15. doi: 10.3171/2013.9.FOCUS13325
79. Saade R, Hessel A, Ginsberg L, Fuller G, Bell D. Primary extradural meningioma presenting as a neck mass: Case report and review of the literature. Head Neck. (2015) 37(8):E92–5.
80. Sun SQ, Cai C, Ravindra VM, Gamble P, Yarbrough CK, Dacey RG, et al. Simpson Grade I-III resection of spinal atypical (World health organization grade II) meningiomas is associated with symptom resolution and low recurrence. Neurosurgery. (2015) 76(6):739–46. doi: 10.1227/NEU.0000000000000720
81. Tseng CL, Eppinga W, Charest-Morin R, Soliman H, Myrehaug S, Maralani PJ, et al. Spine stereotactic body radiotherapy: indications, outcomes, and points of caution. Global Spine J (2017) 7(2):179–97. doi: 10.1177/2192568217694016
82. Kalash R, Glaser SM, Flickinger JC, Burton S, Heron DE, Gerszten PC, et al. Stereotactic body radiation therapy for benign spine tumors: is dose de-escalation appropriate? J Neurosurg Spine. (2018) 29(2):220–5. doi: 10.3171/2017.12.SPINE17920
83. Noh SH, Kim KH, Shin DA, Park JY, Yi S, Kuh SU, et al. Treatment outcomes of 17 patients with atypical spinal meningioma, including 4 with metastases: a retrospective observational study. Spine J (2019) 19(2):276–84. doi: 10.1016/j.spinee.2018.06.006
84. Moazzam AA, Wagle N, Zada G. Recent developments in chemotherapy for meningiomas: a review. Neurosurg Focus. (2013) 35(6):E18. doi: 10.3171/2013.10.FOCUS13341
85. Piątek P, Kwiatkowski S, Milczarek O. Spinal meningiomas in pediatric patients - a case series and literature review. Surg Neurol Int (2022) 13:445. doi: 10.25259/SNI_365_2022
86. Mukand JA, Blackinton DD, Crincoli MG, Lee JJ, Santos BB. Incidence of neurologic deficits and rehabilitation of patients with brain tumors. Am J Phys Med Rehabil. (2001) 80(5):346–50. doi: 10.1097/00002060-200105000-00005
87. Lidstone V, Butters E, Seed PT, Sinnott C, Beynon T, Richards M. Symptoms and concerns amongst cancer outpatients: identifying the need for specialist palliative care. Palliat. Med (2003) 17(7):588–95. doi: 10.1191/0269216303pm814oa
88. Pranckeviciene A, Deltuva VP, Tamasauskas A, Bunevicius A. Association between psychological distress, subjective cognitive complaints and objective neuropsychological functioning in brain tumor patients. Clin Neurol Neurosurg (2017) 163:18–23. doi: 10.1016/j.clineuro.2017.10.007
89. van der Vossen S, Schepers VP, Berkelbach van der Sprenkel JW, Visser-Meily JM, Post MW. Cognitive and emotional problems in patients after cerebral meningioma surgery. J Rehabil Med (2014) 46(5):430–7. doi: 10.2340/16501977-1795
90. Kalasauskas D, Keric N, Abu Ajaj S, von Cube L, Ringel F, Renovanz M. Distress and quality of life do not change over time in patients with operated and conservatively managed intracranial meningioma. Acta Neurochir. (Wien). (2021) 163(12):3417–24. doi: 10.1007/s00701-021-05004-w
91. Boele FW, Douw L, de Groot M, van Thuijl HF, Cleijne W, Heimans JJ, et al. The effect of modafinil on fatigue, cognitive functioning, and mood in primary brain tumor patients: a multicenter randomized controlled trial. Neuro Oncol (2013) 15(10):1420–8. doi: 10.1093/neuonc/not102
92. Reijneveld JC, Klein M. ) the effect of modafinil on fatigue, cognitive functioning, and mood in primary brain tumor patients: a multicenter randomized controlled trial. Neuro Oncol (2013) 15(10):1420–8.
93. Viereck MJ, Ghobrial GM, Beygi S, Harrop JS. Improved patient quality of life following intradural extramedullary spinal tumor resection. J Neurosurg Spine. (2016) 25(5):640–5. doi: 10.3171/2016.4.SPINE151149
94. Luzzati F, Giusti EM, Scotto GM, Perrucchini G, Cannavò L, Castelnuovo G, et al. Quality of life, pain, and psychological factors in patients undergoing surgery for primary tumors of the spine. Support. Care Cancer. (2020) 28(3):1385–93. doi: 10.1007/s00520-019-04965-0
95. Pettersson-Segerlind J, von Vogelsang AC, Fletcher-Sandersjöö A, Tatter C, Mathiesen T, Edström E, et al. Health-related quality of life and return to work after surgery for spinal meningioma: A population-based cohort study. Cancers (Basel). (2021) 13(24):6371. doi: 10.3390/cancers13246371
96. Sperner-Unterweger B. Psychoonkologie - psychosoziale onkologie: Integration in ein onkologisches behandlungskonzept [Psycho-oncology - psychosocial oncology: integration in a concept of oncological treatment]. Nervenarzt. (2011) 82(3):371–8. doi: 10.1007/s00115-010-3163-9
97. Boele FW, Rooney AG, Bulbeck H, Sherwood P. Interventions to help support caregivers of people with a brain or spinal cord tumour. Cochrane Database Syst Rev (2019) 7(7):CD012582. doi: 10.1002/14651858.CD012582.pub2
Keywords: gross total resection (GTR), meningiomas, spinal meningiomas, stereotactic body radiation therapy (SBRT), minimally invasive (MIS), microsurgery (MS), ultrasonic dissection, central nervous system
Citation: Serratrice N, Lameche I, Attieh C, Chalah MA, Faddoul J, Tarabay B, Bou-Nassif R, Ali Y, Mattar JG, Nataf F, Ayache SS and Abi Lahoud GN (2023) Spinal meningiomas, from biology to management - A literature review. Front. Oncol. 12:1084404. doi: 10.3389/fonc.2022.1084404
Received: 30 October 2022; Accepted: 22 December 2022;
Published: 13 January 2023.
Edited by:
Ignazio Gaspare Vetrano, IRCCS Carlo Besta Neurological Institute Foundation, ItalyReviewed by:
Andrea Saladino, IRCCS Carlo Besta Neurological Institute Foundation, ItalyMervyn Lim, National University Hospital, Singapore
Copyright © 2023 Serratrice, Lameche, Attieh, Chalah, Faddoul, Tarabay, Bou-Nassif, Ali, Mattar, Nataf, Ayache and Abi Lahoud. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Georges N Abi Lahoud, aWN2bnNAY2xpbmlxdWUtYml6ZXQuY29t
†These authors have contributed equally to this work