 Jiazhong Ren
Jiazhong Ren Zheng Fu1
Zheng Fu1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Oncol. , 06 January 2023
Sec. Thoracic Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1077777
This article is part of the Research Topic Case Reports in Thoracic Oncology: 2022 View all 42 articles
True thymic hyperplasia (TTH) in children is rare and difficult to distinguish from other thymic tumors such as thymoma and thymic carcinoma. A 3‐year‐old girl underwent an 18F‐fluorodeoxyglucose (18F‐FDG) positron emission tomography (PET)/computed tomography (CT) scan (18F‐FDG PET/CT) and a chest CT scan to evaluate an anterior mediastinal mass. 18F‐FDG PET/CT revealed a mediastinal mass showing heterogeneously increased FDG uptake with a maximum standardized uptake value (SUVmax) of 7.1. Eventually, postoperative pathological diagnosis demonstrated TTH. So far, there are no reports of 18F‐FDG PET/CT imaging of this disease.
True thymic hyperplasia (TTH) usually presents as an anterior mediastinal mass and causes significant challenges in its diagnosis and treatment (1). The enlargement of the thymus occurs most often during infancy and usually spontaneously degenerates after the age of 3 years (2). TTH is the most common benign tumor observed in pediatric patients with tumors following chemotherapy and is essentially a rebound of the thymus gland (3). However, TTH in children is rare, mostly has unknown etiology, and is usually not with any comorbidity (4). Computed tomography (CT) and magnetic resonance imaging (MRI) are mainly used to evaluate thymic lesions. 18F‐fluorodeoxyglucose positron emission tomography/CT (18F‐FDG PET/CT) has an excellent diagnostic value in thymic rebound and can differentiate between thymic hyperplasia (TH), thymoma, and thymic carcinoma (5). However, there are fewer reports on the diagnostic value of 18F‐FDG PET/CT in scanning children with TTH. Here, we describe the case of a child whose diagnosis of TTH was based on a pathological diagnosis after surgical resection, which was supported by CT‐enhanced imaging and an 18F‐FDG PET/CT scan. 18F‐FDG PET/CT is of great value in the preoperative evaluation of pediatric patients with TTH.
A 3‐year‐old girl was admitted to the hospital owing to a 20‐day history of cough and sputum without hemoptysis. Physical examination revealed an anterior chest bulge measuring approximately 6 × 5 cm2, firm in texture, with poor mobility, and with no sternal pressure and rubbing sensation in the chest. She had no other symptoms and no family history of TTH or other diseases. Laboratory tests showed a mildly elevated lactate dehydrogenase (LDH) at 276 U/L (reference range: 38–126 U/L), a white blood cell count of 13.76 × 109/L (reference range: 4–10 × 109/L), and a red blood cell count of 5.09 × 1012/L (reference range: 4–4.5 × 1012/L). However, thyroid‐related laboratory test results were normal. In addition, neuron‐specific enolase (NSE) and human chorionic gonadotropin levels (HCG) were normal. The chest CT scan revealed a well‐defined irregular mass of 17 × 10 × 7.5 cm3 in the right anterior mediastinum, with strip‐like low‐density shadows in the lesion, and a CT value of approximately −67 Hounsfield units, thereby suggesting adipose tissue (Figure 1). The arterial phase showed less vascularity and heterogeneous hypodensity within the lesion (A, white arrow; Figure 1); the venous phase showed persistent hypodensity (B, white arrow; Figure 1) with compression of the cardiac cavity, right main bronchus, and occlusion of the right main bronchus (C, red arrow; Figure 1) ; the compressed right main bronchus and corresponding lung tissue returned to normal (D, black arrow; Figure 1) one week after the patient underwent chest surgery.
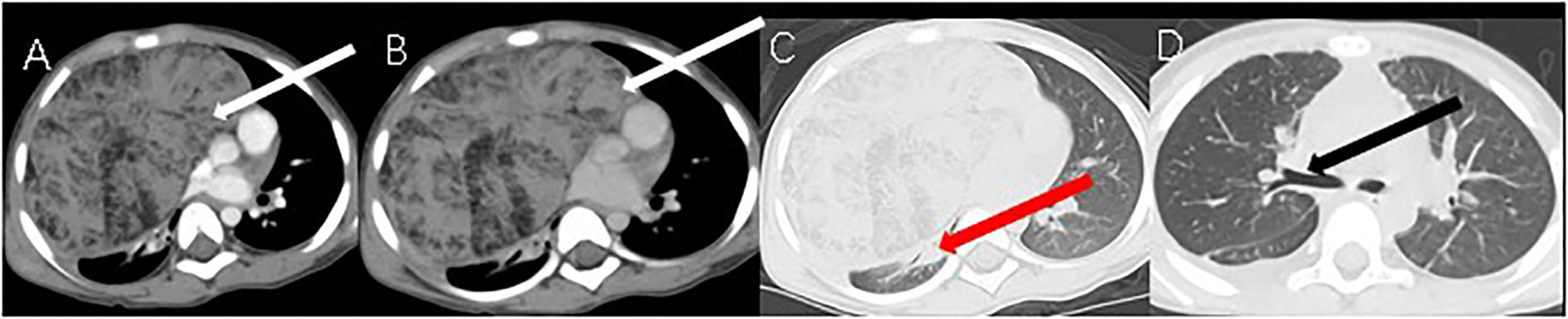
Figure 1 CT images.
After a CT scan of the chest, 18F‐FDG PET/CT was performed owing to concerns that the lesion may be malignant. Coronal PET/CT fusion images (A; Figure 2) show a large, heterogeneous hypermetabolic mass in the right thorax (white arrows; Figure 2), whereas the thyroid was normal and not hypermetabolic (green arrows; Figure 2), thereby suggesting a thymic origin of the mass. In axial images (B: CT; C: PET/CT fusion; D: PET; Figure 2), the uptake of FDG with an SUVmax of 7.1 (white and black arrows; Figure 2) shows that the mass has heterogeneous hyperactivity. Pathological images (E, hematoxylin–eosin stain; original magnification × 100) showed histologically normal thymic tissue consisting of lobules with well‐defined cortical and medullary cells. Immunohistochemical staining was positive for CKpan, CK19, LCA, CD3, TDT, MDM2, and CD1a and negative for CK20, and Desmin. The lesion was eventually diagnosed as TTH, and the patient recovered well during the follow‐up period.
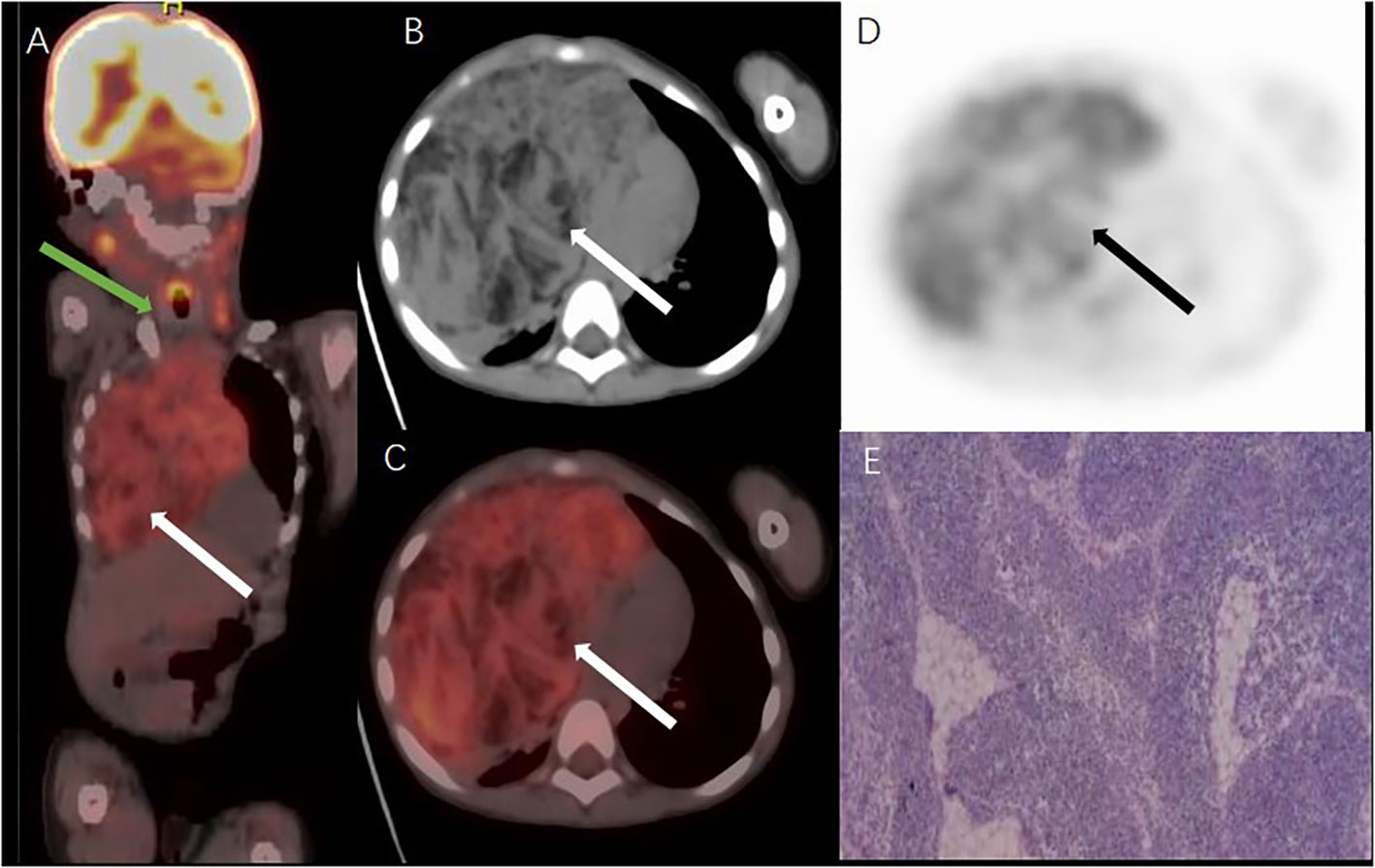
Figure 2 18F FDG PETCT images and pathologic picture.
The thymus is a gland situated in the anterior mediastinum; it is embryologically derived from the pharyngeal pouch of the third and fourth branchial arch (2). Its size varies with age because thymic tissue gradually shrinks and is replaced by adipose tissues. The thymus gland gradually invaginates during the first 3–4 years of life (6).
TH is usually divided into two categories: TTH and lymphatic follicular hyperplasia (LFH) (7). TTH is characterized by a diffused thickening and enlargement of the thymus that exceeds the corresponding upper limit of size or mass in a normal child of the same age but maintains the normal thymic structure and immunohistochemical features (8). TH is often caused by chemotherapy for tumors, thermal burns, or surgery. LFH is characterized by an increase in the number of lymphoid follicles and germinal centers in the thymus, which may be normal or slightly enlarged in size. LFH is associated with several endocrine and autoimmune diseases such as Graves’ disease, myasthenia gravis, and systemic lupus erythematosus (9).
TTH in children is a rare clinical condition, has unknown etiology, and often has no comorbidities. It is often referred to as massive thymic hyperplasia (MTH) because it is characterized by a relatively larger and heavier thymus than the thymus of a healthy individual. The diagnostic features of MTH are as follows: 1. radiographs show gland projection exceeding the cardiac shadow, 2. The thymus weighs several times its expected weight at a specific age, 3. the mass of the thymus is > 2% of the body mass, and 4. pathological test shows normal thymus structure (10). The patient in this case report largely met the above diagnostic criteria.
The most common tumors of the anterior mediastinum in children are tumors of thymic, lymphatic, or germ‐cell origin (11). Tumor markers (alpha‐fetoprotein (AFP), HCG, and NSE) are helpful in the differential diagnosis of some tumors such as germ cell tumors (GCTs). Mediastinal yolk sac tumor is often associated with elevated levels of serum AFP, seminoma with elevated levels of serum HCG, and lymphoma with elevated levels of LDH. MRI or CT scans are often used to evaluate thymic lesions (11, 12). Mediastinal GCTs are mostly teratomas, often containing fatty tissues and calcifications, and are easily diagnosed. Invasion of the thymus by lymphoma usually occurs in the setting of extensive systemic disease. Homogeneous enlargement of the thymus with mediastinal and/or axillary lymph node enlargement is usually diagnosed as lymphoma (13). Previous studies have reported that 18F‐FDG PET/CT can differentiate between benign and malignant thymic tumors but cannot distinguish between aggressive and non‐aggressive thymoma and still relies on morphological examination by CT and MRI or pathological examination (8, 14, 15). In general, benign uptake of physiological thymus or chemotherapy‐induced thymic rebound hyperplasia is less intense on 18F‐FDG PET/CT scans, where SUVmax is approximately 1.0–2.8. In comparison to thymoma and TH, thymic carcinoma shows considerably higher FDG uptake (13).
Although multimodal imaging has an excellent diagnostic value for TTH, MRI can more easily identify mediastinal masses, which are directly contiguous with and follow the same signal features as the main body of the thymus (12). Moreover, MRI is more sensitive in detecting adipose tissue in TTH, which can enable us to accurately deduce the origin and nature of the mass. Therefore, we recommend that MRI should always be preferred in diagnosing pediatric patients if feasible, specifically because it is free of ionizing radiation and is therefore safe for these patients. Unfortunately, due to our inexperience with TTH and the suspicion that the mediastinal mass was malignant as detected by enhanced CT, we selected 18F‐FDG PET/CT instead of MRI for further examination.
In this case report, 18F‐FDG PET/CT scan revealed that there was an increase in the heterogeneous hypermetabolism at the lesion with an SUVmax of 7.1, the lung tissue adjacent to the lesion was only compressed but not invaded, and the patient had no lymph node metastases and distant metastases. Although 18F‐FDG PET/CT has limited diagnostic value for thymic lesions (8, 12), especially in children, in this case report, it helped us to determine that the lesion was benign with no adjacent tissue invasion, which enabled subsequent surgery plans for the patient.
Most previous case reports suggest that treatment of TTH with steroids is usually ineffective; therefore, surgical resection is a better option (6, 10, 16). Finally, the patient underwent complete surgical resection of the mediastinal tumor and recovered well after surgery without any postoperative complications. Therefore, we recommend that surgical resection should be the first option for pediatric patients with TTH because this tumor is non‐invasive to adjacent tissues and easily resectable, and the surgery is free of any postoperative complications.
In conclusion, 18F‐FDG PET/CT is of great value in the preoperative diagnosis and assessment of pediatric patients with TTH. In addition, awareness of these findings is important in the interpretation of PET/CT scans of anterior mediastinal masses in young children.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee of Cancer Hospital Affiliated to Shandong First Medical University. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
JR acquisition of data, drafting of the manuscript; ZF and YZ: revision of the manuscript, supervision. All authors read and critically revised the manuscript for intellectual content and approved the final manuscript.
We thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Mlika M, Yaiche R, Fourti A, Braham E, Houcin Y, Marghli A, et al. Thymic hyperplasia: A study of 46 cases. Ann Pathol (2021) 41:544–8. doi: 10.1016/j.annpat.2021.01.003
2. Hofmann WJ, Mö ller P, Otto HF. Thymic hyperplasia. i. true thymic hyperplasia. review of the literature. Klin Wochenschr (1987) 65:49–52. doi: 10.1007/BF01745472
3. Smith CS, Schoder H, Yeung HW. Thymic extension in the superior mediastinum in patients with thymic hyperplasia: potential cause of false-positive findings on 18F-FDG PET/CT. AJR Am J Roentgenol (2007) 188:1716–21. doi: 10.2214/AJR.06.0552
4. Rice HE, Flake AW, Hori T, Galy A, Verhoogen. RH. Massive thymic hyperplasia: Characterization of a rare mediastinal mass. J Pediatr Surg (1994) 29(12):1561–4. doi: 10.1016/0022-3468(94)90216-x
5. Kawano T, Suzuki A, Ishida A, Takahashi N, Lee J, Tayama Y, et al. The clinical relevance of thymic fluorodeoxyglucose uptake in pediatric patients after chemotherapy. Eur J Nucl Med Mol Imaging (2004) 31:831–6. doi: 10.1007/s00259-004-1466-4
6. Tan Z, Ying LY, Zhang ZW, Li JH, Gao Z, Qi JC. True thymic hyperplasia in an infant. J Pediatr Surg (2010) 45:1711–3. doi: 10.1016/j.jpedsurg.2010.05.001
7. Weis CA, Markl B, Schuster T, Vollert K, Strobel P, Marx A. [True thymic hyperplasia: Differential diagnosis of thymic mass lesions in neonates and children]. Pathologe (2017) 38:286–93. doi: 10.1007/s00292-017-0283-z
8. Nguyen R, Coleman JL, Howard SC, Metzger ML. Watchful waiting for some children with a mediastinal mass: the potential role for (1)(8)F-fluorodeoxyglucose positron emission tomography: A case report and review of the literature. BMC Pediatr (2013) 13:103. doi: 10.1186/1471-2431-13-103
9. Kiwaki T, Tanaka H, Akiyama Y, Akaki M, Tomita M, Kataoka H. A rare association between true thymic hyperplasia and thyroid follicular tumor: A case report. J Med Case Rep (2020) 14:9. doi: 10.1186/s13256-019-2332-0
10. Linegar AG, Odell JA, Fennell WM, Close M, De Groot MK, Casserly DR, et al. Massive thymic hyperplasia. Ann Thorac Surg (1993) 55(5):1197–201. doi: 10.1016/0003-4975(93)90033-e
11. Nariman M, Willi W, Hansjörg S, Martin B, Michael G, Konrad R. Case report: True thymic hyperplasia in a 30-Day-Old boy. Klin Padiatr (2021) 233(6):299–302. doi: 10.1055/a-1557-1427
12. Ka KW, Elisa F, Morand P. F-18 FDG PET/CT study showing cervical extension of thymic tissue. Clin Nucl Med (2008) 33(8):547–8. doi: 10.1097/RLU.0b013e31817dec53
13. Liu Y. Characterization of thymic lesions with f-18 FDG PET-CT: an emphasis on epithelial tumors. Nucl Med Commun (2011) 32:554–62. doi: 10.1097/MNM.0b013e328345b984
14. Tatsuro T, Satoko K, Akiko K, Motoko Y, Akihiko T, Hirohiko K, et al. First description of the role of 18F-FDG-PET/CT as compared to CT, MRI To suspect a case of thymoma in a pediatric patient. Hell J Nucl Med (2012) 15(1):68–9.
15. Ferdinand B, Gupta P, Kramer EL. Spectrum of thymic uptake at 18F-FDG PET. Radiographics (2004) 24(6):1611–6. doi: 10.1148/rg.246045701
Keywords: 18F‐FDG PET/CT, CT, mediastinum, TTH, MTH
Citation: Ren J, Fu Z and Zhao Y (2023) Case report: Imaging findings of true thymic hyperplasia at 18F-FDG PET/CT in an infant. Front. Oncol. 12:1077777. doi: 10.3389/fonc.2022.1077777
Received: 23 October 2022; Accepted: 13 December 2022;
Published: 06 January 2023.
Edited by:
Kohei Fujita, National Hospital Organization Kyoto Medical Center, JapanReviewed by:
Alessandro Boscarelli, Institute for Maternal and Child Health Burlo Garofolo (IRCCS), ItalyCopyright © 2023 Ren, Fu and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yaqing Zhao, YmV0dGVydG9tb3Jyb3cxOEAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.