
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Oncol., 14 December 2022
Sec. Thoracic Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1059999
 Feng Rong*Rui ShiLili HuRan ChenDaoyue WangXiazhi LvYong ZhaoWei HuangYang YangHongyang ZhouKaige Hong
Feng Rong*Rui ShiLili HuRan ChenDaoyue WangXiazhi LvYong ZhaoWei HuangYang YangHongyang ZhouKaige HongBackground: Lung cancer is the leading cause of cancer-related death worldwide, with risk factors such as age and smoking. Low-dose computed tomography screening can reduce lung cancer mortality. However, its effectiveness in Asian populations remains unclear. Most Asian women with lung cancer are non-smokers who have not been screened. We conducted a randomized controlled trial to evaluate the performance of low-dose computed tomography screening in a Chinese population, including high-risk smokers and non-smokers exposed to passive smoking. The baseline data are reported in this study.
Methods: Between May and December 2019, eligible participants were randomized in a ratio of 1:1:1 to a screening (two arms) or control cohort. Non-calcified nodules/masses with a diameter >4 mm on low-dose computed tomography were considered positive findings.
Results: In total, 600 patients (mean age, 59.1 ± 6.9 years) underwent low-dose computed tomography. Women accounted for 31.5% (189/600) of patients; 89.9% (170/189) were non-smokers/passive smokers. At baseline, the incidence of lung cancer was 1.8% (11/600). The incidence of lung cancer was significantly lower in smokers than in female non-smokers/passive smokers (1.0% [4/415] vs. 4.1% [7/170], respectively; P=0.017). Stage 0–I lung cancer accounted for 90.9% (10/11) of cases.
Conclusions: We demonstrate the importance of including active smokers and female non-smokers/passive smokers in lung cancer screening programs. Further studies are needed to explore the risk factors, and long-term cost–benefit of screening Asian non-smoking women.
Clinical trial registration: http://chictr.org.cn/showproj.aspx?proj=39003, identifier ChiCTR1900023197.
Lung cancer is the leading cause of cancer-related death worldwide (1, 2). Most patients with lung cancer have advanced disease that is incurable. With advances in the understanding of the pathogenesis of lung cancer and the emergence of new treatment strategies, such as targeted therapy and immunotherapy, the long-term outcomes of patients with advanced lung cancer have improved significantly. However, the 5-year survival rate of patients with advanced non-small cell lung cancer was <5% in the chemotherapy era, and is only 13.4% in the immunotherapy era (3).
Early diagnosis and treatment of lung cancer through screening can improve outcomes (4). European and American studies (5–7) have shown that low-dose computed tomography (LDCT) screening reduces the risk of mortality by 20% to 26%. The criteria for selecting high-risk individuals for lung cancer screening in Europe and the United States are based on age and smoking history (4, 8, 9). Nevertheless, the effectiveness of lung cancer screening is influenced by race/ethnicity (10). Studies have shown that lung cancer in Asia differs from that in other regions, in terms of risk factors (10, 11), population characteristics (12), imaging manifestations (13), and screening effectiveness (12, 14). For instance, lung cancer detected by screening in Asia is more radiologically characterized by mixed and pure ground-glass nodules (10, 12). Therefore, the performance of LDCT screening for lung cancer in Asian smokers needs to be clarified.
Lung cancer in women is increasing worldwide (1). However, the increase in lung cancer in Asian women is not fully explained by smoking. In China (2) and South Korea (15), the proportion of female smokers has remained stable at 2.0–6.4%. In Asia, the smoking rate among female lung cancer patients is <20%, while in Europe and the United States it reaches 70–85% (16). Non-smoking lung cancer accounts for the majority of Asian female lung cancers. Unfortunately, these patients are not included in LDCT screening programs. For non-smoking women, the focus is on identifying risk factors in those who may benefit from screening (17). Currently, risk factors for lung cancer in non-smoking Asian women are poorly defined (18). Environmental pollutants, such as environmental tobacco smoke (ETS), particulate matter 2.5, and kitchen fumes, may be risk factors for lung cancer (19). In particular, ETS is associated with the high prevalence of female lung cancer in Asia (19).
China is the largest producer and consumer of tobacco (20); 52.1% of adult males are smokers (2). Women may be more susceptible to ETS at home, in the workplace, and in public places (21, 22). Traditional Chinese patriarchal culture may further increase the risk of ETS exposure at home (21, 23). Passive smoking is an important risk factor for lung cancer in non-smoking Chinese women (24). Better understanding of the screening performance in non-smoking women exposed to passive smoking is needed. Some population-based prospective (14, 25) and retrospective (11) screening studies have included women. However, the risk factors were difficult to analyze, or were not focused on ETS. The ongoing TALENT study focuses on non-smokers but has not yet been peer-reviewed or published. More clinical trial data are needed to elucidate the risk factors, inclusion criteria, and efficacy of LDCT screening of non-smoking women for lung cancer.
We conducted a randomized controlled trial to evaluate the performance of LDCT screening in a Chinese population, including high-risk smokers and non-smokers exposed to passive smoking. The baseline data are reported in this study.
The study was approved by the Ethics Committee of Lu’an Hospital of Anhui Medical University, Anhui, China (2019–002–01). The study was registered in the Chinese Clinical Trial Registry (ChiCTR1900023197). All participants provided written informed consent.
This was a prospective, randomized controlled trial that was primarily designed to assess the performance of LDCT lung cancer screening in asymptomatic high-risk populations in mainland China. The secondary aim was to explore the clinical value of inflammatory markers in screening for lung cancer.
From May to December 2019, participants were recruited from a community health center and via advertisements in 16 communities. At the time of randomization, eligible participants had to be between 50 and 75 years of age, with at least one high-risk factor: (1) A smoking history of ≥30 pack-years (current smoker or former smoker with ≤15 years since quitting); (2) A non-smoker exposed to passive smoking at home (from a family member) or in the workplace (from a colleague) for >20 years; and (3) A non-smoker with a family history of lung cancer. Individuals who had been diagnosed with cancer in the last 5 years, a metallic stent/internal fixation in the chest and/or back, a physical condition rendering them unsuitable for examination, or undergone chest computed tomography in the last 12 months were excluded.
Demographic data and medical histories were recorded at enrollment. Before recruitment, SAS 9.2 software (SAS Institute Inc., Cary, NC, USA) was used to generate random sequences, according to the block randomization method (block=9). To maintain blinding, the sequences were kept by someone who did not understand the random sequence generation method and did not participate in recruitment. Signed informed consent forms were submitted to the sequence custodian, who performed the randomization, according to the randomly assigned sequence.
Participants were randomized in a ratio of 1:1:1 to three arms: LDCT1 (three rounds of annual LDCT screening), LDCT2 (three rounds of LDCT screening [at baseline, year 1, and year 3] and blood collection) and control (monitoring and questionnaire follow-ups without interfering with normal medical behavior).
Baseline LDCT screening was performed soon after randomization. When the participant was diagnosed with lung cancer, further LDCT screening was not performed. Spiral computed tomography images were obtained using a 32-detector row scanner (Neosoft, China) with a low-dose setting (120 Kvp, 60 mA), and in overlapping contiguous 1-mm increments, with a 1.25 pitch. The images were reviewed by two radiologists with >10 years of experience. The size of the lung nodules/masses, and the maximum diameter in the axial plane, were measured. If there was a disagreement, a chief radiologist specializing in chest imaging was consulted. Positive findings were reviewed by a team consisting of two medical and one thoracic oncologist.
On LDCT, non-calcified nodules with a diameter of >4 mm were regarded as positive results. The average diameter was used for nodules with a longest diameter of <10 mm. The size and radiological features of non-calcified nodules (diameter >4 mm) were recorded. Abnormalities suggestive of clinically significant conditions, other than lung cancer, were also documented, as were minor abnormalities. Screening results were communicated to the participants within 4 weeks. Positive results were communicated within 2 weeks.
The management of positive screening results was carried out according to the China National Lung Cancer screening guideline with LDCT (2018 version) (26). All complications and medical interventions were documented. Participants completed a semiannual Short-Form 36 questionnaire on vital status, with the help of trained interviewers, via telephone or in-person interviews. Patients were classified according to the 2015 World Health Organization classification of tumors of the lung and staged according to the eighth edition of the Tumor–Node–Metastasis classification for lung cancer (27). Data were entered into an EpiData database.
SPSS for Windows (version 25; SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Continuous variables are presented as mean ± standard deviation or median (interquartile range). Categorical variables are presented as numbers and percentages. Differences in rates between the LDCT and control arms were analyzed using the chi-square or Fisher’s exact test; differences in constituent ratios were analyzed using the Wilcoxon rank sum test. A two-sided P-value <0.05 was considered statistically significant.
In 16 communities, 12,388 questionnaires were administered. A total of 2,198 of the 7,326 respondents, who returned the questionnaires, were eligible for inclusion. In the second questionnaire, 1,136 participants, who met the inclusion criteria, were willing to undergo LDCT screening. According to the predetermined sample size, the first 900 subjects, who provided written informed consent, were randomly assigned to a screening or control arm (Figure 1). As the difference between the LDCT1 and LDCT2 arms mainly lies in the interval between the second and third round of screening, the baseline analysis was a pooled analysis of the two LDCT arms (collectively known as the LDCT group).
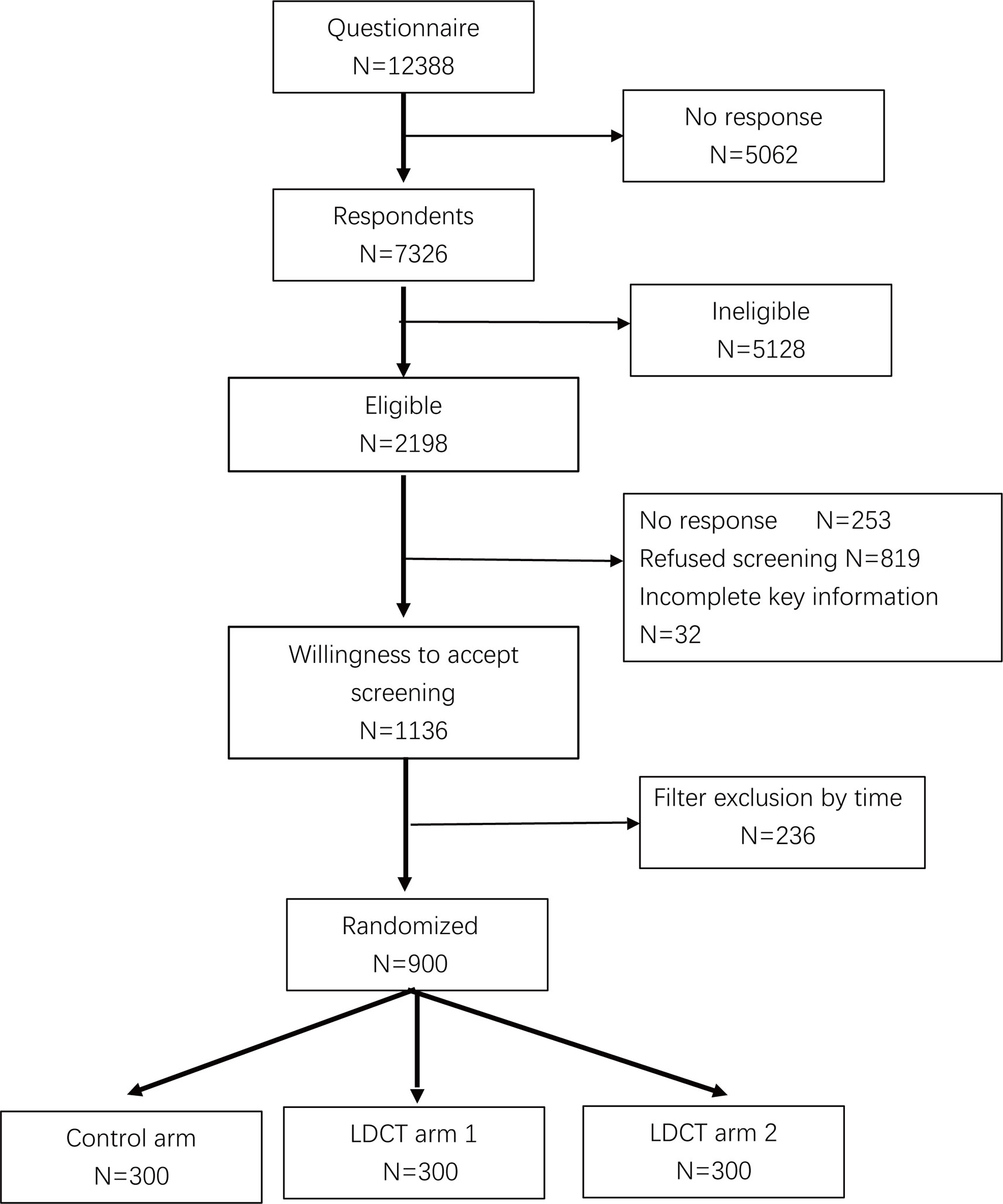
Figure 1 Flowchart of the participants in the trial. LDCT, low-dose computed tomography.
There were no significant differences in baseline characteristics between the LDCT and control groups. In the LDCT group (mean age, 59.1 ± 6.9 years), the mean smoking index was 44.7 ± 20.6 pack-years, 32.0% (192/600) of participants were exposed daily to kitchen fumes, and 8.7% (52/600) had a college degree or higher. Women accounted for 31.9% (287/900) of participants; 92.3% (266/287) of women were non-smokers (Table 1). All participants met the second criteria (exposed to secondhand smoke at home or in the workplace for >20 years) and were included in the study.
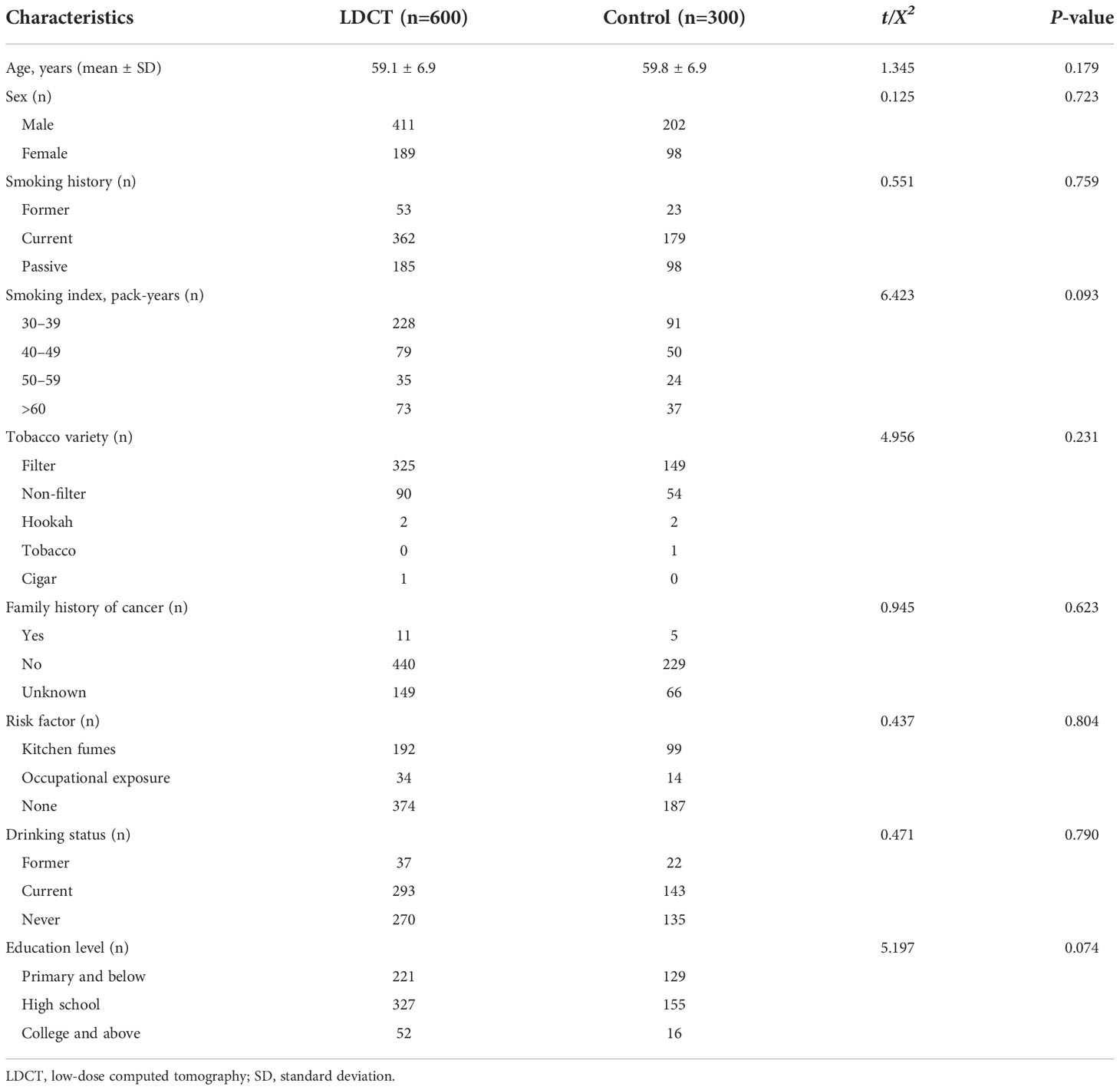
Table 1 Participant characteristics according to study group.
In the LDCT group, 21.8% (131/600) of participants had lesions measuring >4 mm in the chest, with a total of 134 lesions. There were 130 lesions measuring >4 mm in the lung, three in the posterior thymus, and one in the interlobular fissure. A greater number of positive nodules were located in the right lung (67.8%, 88/130) than in the left lung (26.2%, 34/130) (Figure 2 and Table 2). The proportion of participants with subsolid (mixed and pure ground-glass) nodules was 7.7% (46/600); that in the upper lung was higher than that in the middle and lower lung (69.6% [32/46] vs. 6.5% [3/46] and 23.9% [11/46], respectively). (Table 2).

Figure 2 Screening strategy and results of LDCT. LDCT, low-dose computed tomography; LLL, left lower lung; LUL, left upper lung; RLL, right lower lung; RML, right middle lung; RUL, right upper lung.
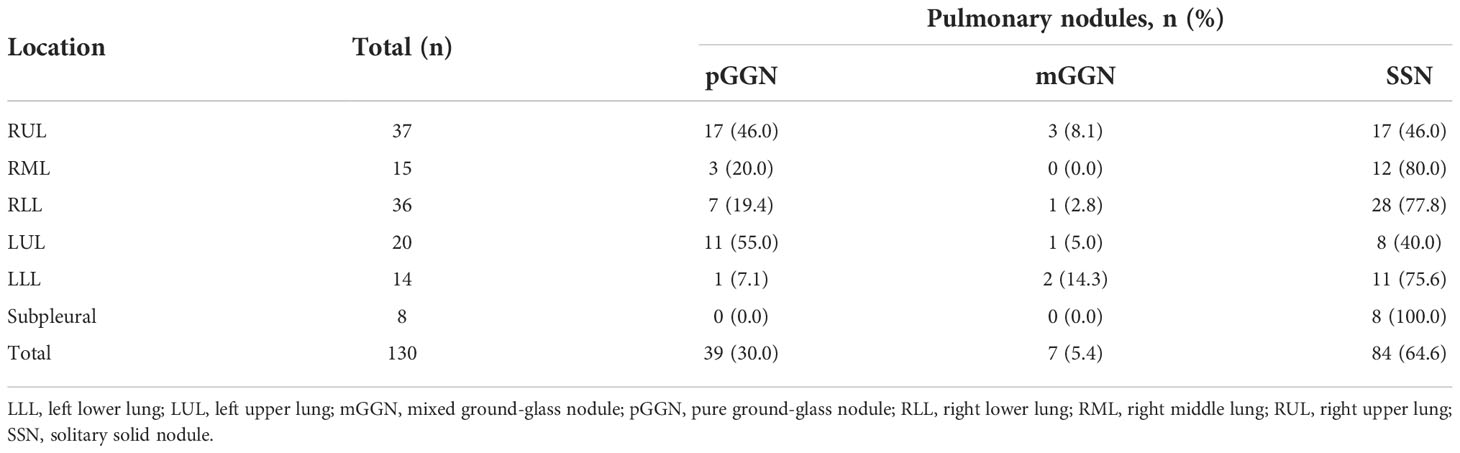
Table 2 Distribution and type of pulmonary nodules (>4 mm).
At baseline, the lung cancer detection rate was 1.8% (11/600). All patients had adenocarcinoma. The detection rate of male lung cancer was 0.7% (3/411), which was significantly lower than that of female lung cancer (4.2%, 8/189) (P=0.006). Among participants who met the 2021 United States Preventive Services Task Force recommendation on lung cancer screening (4), the lung cancer detection rate was 1.0% (4/415), which was significantly lower than that in female non-smokers (4.1%, 7/170) (P=0.017). Stage 0–I lung cancer accounted for 90.9% (10/11) of cases. The proportion of non-smokers was 63.6% (7/11). Female lung cancer accounted for 72.7% (8/11) of cases, of which non-smoking female lung cancer accounted for 87.5% (7/8). There was no significant difference in the diagnosis rate between right and left lung positive nodules (10.2% vs. 5.9%, respectively; P=0.726) (Table 3). None of the participants in the control group were diagnosed with lung cancer in at least one year of follow-up.
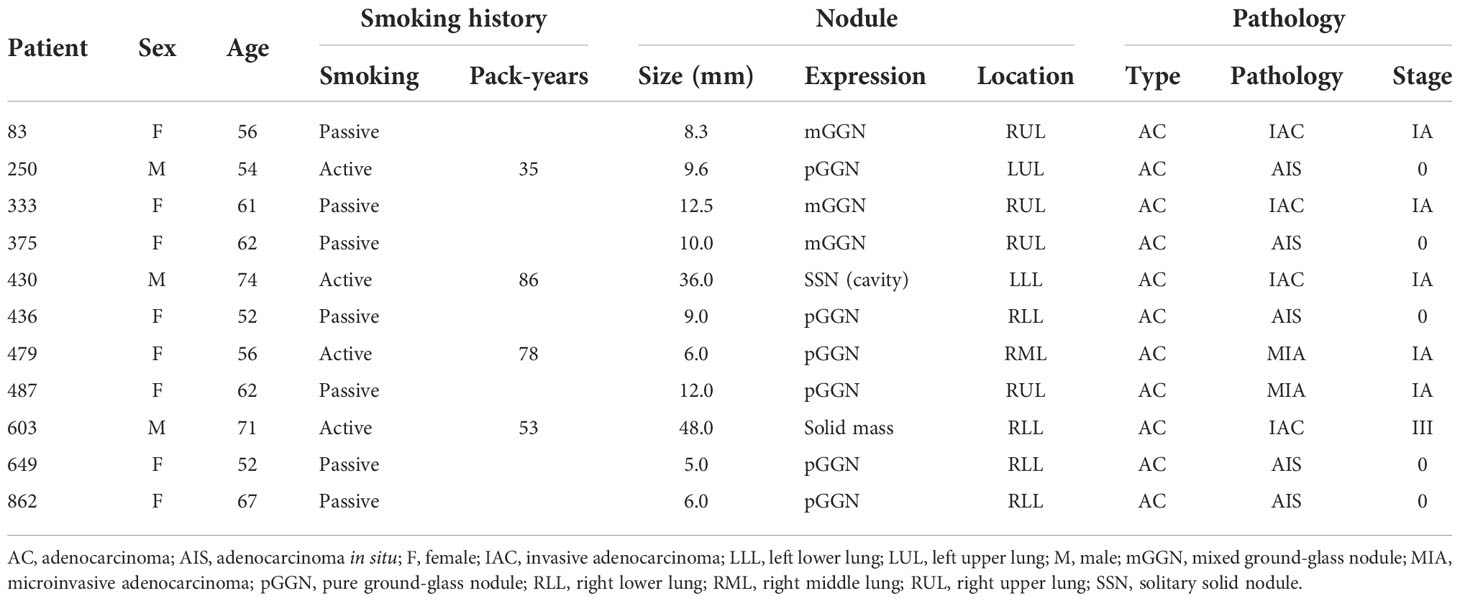
Table 3 Characteristics of patients diagnosed with lung cancer.
In this study, the eligible population included non-smokers other than those who met the 2021 United States Preventive Services Task Force recommendation on lung cancer screening (4). The results showed that the diagnostic rate of lung cancer in female non-smokers was significantly higher than that in smokers. All female non-smokers were passive smokers, suggesting that non-smoking women exposed to passive smoking should be included in Asian high-risk populations for LDCT screening. Our findings add to the evidence regarding the value of LDCT screening in Asia and provide relevant information to optimize and improve the eligibility criteria for LDCT screening in Asian countries.
Age is strongly associated with lung cancer (23). In both men and women, lung cancer is most likely to develop between the ages of 50 and 79 years (28). Mazzone et al. (29) showed that LDCT screening, starting at the age of 50 years and ending at the age of 74–75 years, significantly reduced mortality (hazard ratio: 0.77 [P<0.01] and 0.88 [P=0.005], respectively). In this study, the inclusion age range was 50–75 years. The mean age was approximately 59 years, similar to those in the NLST (5), NELSON (6), and MILD (30) studies (58–61 years). Taking a diameter of >4 mm as the positive standard, the positive rate of 21.8% was comparable to the T0 rates in the NLST (5), LUSI (7), and UKLS (31) studies (22.2–27.3%). A randomized controlled trial in Shanghai, China (14) showed that the detection rate of non-calcified nodules on initial screening was 22.9%, and that the detection rate of non-calcified nodules measuring ≥5 mm was 13.6%, which were lower than the 26.8% (161/600) and 21.2% (127/600) reported in this study, respectively. This may be attributable to the younger population (45–70 years) in the Yang et al. (14) study. Nevertheless, the incidence of lung nodules increases with age (32).
In the NLST (33) and I-ELCAP (34) studies, subsolid nodules were detected in 9.4% and 4.2% of participants at baseline, respectively. Fan et al. (12) showed that the detection rate of subsolid nodules was no more than 8.6% (1,513 nodules in 17,683 subjects) in Shanghai, China. In this study, subsolid nodules accounted for 7.7% of positive nodules. These findings show that the proportion of subsolid nodules detected by screening is similar in China and the United States and Europe. However, early lung cancer is more likely to present as subsolid nodules in Asia. In this study, subsolid nodules (81.8%) were the main manifestations of lung cancer, consistent with other Asian studies (59.0–84.9%) (10, 12). In Western developed countries, the proportion of subsolid nodules detected by screening was lower (35).
The overall detection rate of lung cancer in this study was 1.8%, which was higher than those in the NLST (1.1%) (36) and NELSON (0.9%) (6) studies, with age and smoking history as inclusion criteria. However, it was similar to screening studies of non-smoking women (10, 13, 37). These differences may be due to the inclusion of non-smokers. In this study, the detection rate of smoking lung cancer was 1.0% (4/415), which was consistent with the aforementioned studies. Similar lung cancer detection rates in Asian smokers further support efforts to include high-risk smokers in screening programs.
In this study, the detection rate of lung cancer in smokers was significantly lower than that in female non-smokers exposed to passive smoking (relative risk: 0.23 [95% confidence interval: 0.07–0.79]; P=0.017), consistent with previous studies (10, 37). This difference may be due to the fact that non-smoking female lung cancer patients are more likely to present with ground-glass nodules, and LDCT is advantageous for detecting ground-glass nodules. Non-smoking lung cancer is more common in women, whereas smoking lung cancer does not show significant sex differences (17). This may partially explain the higher detection rate of lung cancer in non-smoking women. The risk factors for lung cancer in Asian women who do not smoke have not been elucidated. However, studies have shown that female non-smoking lung cancer is largely attributed to passive smoking (24, 38). In this study, passive smoking was defined in terms of location (home/workplace) and duration (≥20 years). Forte et al. (18) showed that there was a dose–effect relationship between the duration of exposure to secondhand smoke and lung cancer risk, and that >20 years of passive smoking is the primary determinant of lung cancer risk in women (odds ratio: 1.57 [95% confidence interval: 1.05–2.35]; P<0.01). This may also explain the higher detection rate of lung cancer in non-smoking women in this study compared to other studies. We believe that our quantitative measure of passive smoking is more accurate in practice.
Tobacco use is an important mortality factor for lung cancer (39). However, non-smoking lung cancer is the seventh most prevalent malignancy worldwide (17). In Asia, non-smoking lung cancer accounts for the majority of lung cancers in women (16). Therefore, current European and American criteria for selecting eligible patients, based on age and smoking history, may not be applicable to the Chinese population (40), because they may result in a large number of female lung cancer patients being unable to access screening before the onset of symptoms. Abdel-Rahman (41) showed that non-smokers exposed to passive smoking are at a higher risk of developing and dying from lung cancer. Our study also showed that the lung cancer detection rate was higher in non-smoking women exposed to passive smoking. These findings highlight the need to enroll female passive smokers in Asian lung cancer screening programs.
Stage 0–I lung cancer accounted for 90.9% of all lung cancers examined in this study. Overdiagnosis is one focus of lung cancer screening research. Cancers are deemed to have been overdiagnosed if they would not have progressed to a clinical stage throughout the patient’s lifetime (42). Meanwhile, it is the magnitude of overdiagnosis that changes over time as the follow up period is extended. In Asia, overdiagnosis is an issue for lung cancer screening, because more than 90% of lung cancers screened were cStage 0-I. Most of them are indolent. A study (43) from Taiwan showed that LDCT screening in all female nonsmokers may cause a significant overdiagnosis problem. Therefore, age at detection and the definition of risk factors are crucial for lung cancer screening in Asian female nonsmokers.
Although early lung cancer that manifests as ground-glass nodules is usually indolent (44), it may grow rapidly (13), be less stable than that which manifests as mixed ground-glass nodules (45), and require long-term follow-up (46) and treatment (47). We supported the surgical strategies for pre- and minimally invasive lung adenocarcinoma 3.0 proposed by Zhang et al. (48). With the same opinion as Chen (49), we also agree with Detterbeck regarding the observation standards of GGNs by CT. Considering the long lead time of MIA/AIS (50), psychological burden caused by lesions, repeated computed tomography scans, greater surgical resection, and more intensive postoperative surveillance, a multidisciplinary approach is needed.
This study has several limitations. First, it was a single-center study, which may have resulted in selection bias. To avoid bias, we expanded our outreach in the city’s urban areas through on-site and joint outreach with community primary health care providers. Second, passive smoking, exposure to kitchen fumes, and other risk factors have no formal definition and are difficult to assess. In this study, we used the definition of living or working with a smoker for >20 years. Finally, limited by sample size, this study may be not to show an overall survival benefit of screening. However, during COVID-19 pandemic, large-scale clinical researches would meet many challenges. A well-designed study with a small sample size can also provide high-quality data and evidence for future pool analysis.
In conclusion, we conducted a randomized controlled trial to evaluate the performance of LDCT screening in China, using the NLST and customized passive smoking criteria as inclusion criteria. The results confirmed the higher lung cancer detection rate in non-smoking women exposed to passive smoking than in Asian high-risk smokers. We demonstrated the importance of including active smokers and female passive smokers in lung cancer screening programs in China and provided support for the standardization and practice of lung cancer screening in Asia. Further studies are needed to explore the risk factors, and long-term cost–benefit of screening Asian non-smoking women.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the ethics committee of Lu’an Hospital of Anhui Medical University. The patients/participants provided their written informed consent to participate in this study.
FR, YZ, and RS contributed to study design and implementation. FR supervised the study and wrote the first draft of the manuscript. RS, LH, RC, DW, WH, KH, HZ, YY, and XL contributed to the collection and assembly of data. FR, RC, LH, and DW analyzed and interpreted the data. All authors approved the final manuscript and agree to be accountable for all aspects of the work.
This work was supported by the Key Research and Development Program of Anhui [grant number: 201904a07020006], the Scientific Research Project of Lu’an Hospital of Anhui Medical University [grant number: 2020kykt30], and the Discipline Construction Fund of Lu’an Hospital of Anhui Medical University.
We thank the personnel who participated in the study. We also thank Editage (www.editage.com) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71:209–49. doi: 10.3322/caac.21660
2. Li S, Ma C, Xi B. Tobacco control in China: Still a long way to go. Lancet (2016) 387:1375–6. doi: 10.1016/S0140-6736(16)30080-0
3. Borghaei H, Gettinger S, Vokes EE, Chow LQM, Burgio MA, de Castro Carpeno J, et al. Five-year outcomes from the randomized, phase III trials checkmate 017 and 057: Nivolumab versus docetaxel in previously treated non-small-cell lung cancer. J Clin Oncol (2021) 39:723–33. doi: 10.1200/JCO.20.01605
4. US Preventive Services Task Force, Krist AH, Davidson KW, Mangione CM, Barry MJ, Cabana M, et al. Screening for lung cancer: US preventive services task force recommendation statement. JAMA (2021) 325:962–70. doi: 10.1001/jama.2021.1117
5. National Lung Screening Trial Research Team, Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med (2011) 365:395–409. doi: 10.1056/NEJMoa1102873
6. de Koning HJ, van der Aalst CM, de Jong PA, Scholten ET, Nackaerts K, Heuvelmans MA, et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N Engl J Med (2020) 382:503–13. doi: 10.1056/NEJMoa1911793
7. Becker N, Motsch E, Trotter A, Heussel CP, Dienemann H, Schnabel PA, et al. Lung cancer mortality reduction by LDCT screening-results from the randomized German LUSI trial. Int J Cancer (2020) 146:1503–13. doi: 10.1002/ijc.32486
8. Jaklitsch MT, Jacobson FL, Austin JH, Field JK, Jett JR, Keshavjee S, et al. The American association for thoracic surgery guidelines for lung cancer screening using low-dose computed tomography scans for lung cancer survivors and other high-risk groups. J Thorac Cardiovasc Surg (2012) 144:33–8. doi: 10.1016/j.jtcvs.2012.05.060
9. Mazzone PJ, Silvestri GA, Patel S, Kanne JP, Kinsinger LS, Wiener RS, et al. Screening for lung cancer: CHEST guideline and expert panel report. Chest (2018) 153:954–85. doi: 10.1016/j.chest.2018.01.016
10. Yi CA, Lee KS, Shin MH, Cho YY, Choi YH, Kwon OJ, et al. Low-dose CT screening in an Asian population with diverse risk for lung cancer: A retrospective cohort study. Eur Radiol (2015) 25:2335–45. doi: 10.1007/s00330-015-3620-8
11. Wu FZ, Huang YL, Wu CC, Tang EK, Chen CS, Mar GY, et al. Assessment of selection criteria for low-dose lung screening CT among Asian ethnic groups in Taiwan: From mass screening to specific risk-based screening for non-smoker lung cancer. Clin Lung Cancer (2016) 17:e45–56. doi: 10.1016/j.cllc.2016.03.004
12. Fan L, Wang Y, Zhou Y, Li Q, Yang W, Wang S, et al. Lung cancer screening with low-dose CT: Baseline screening results in shanghai. Acad Radiol (2019) 26:1283–91. doi: 10.1016/j.acra.2018.12.002
13. Zhang Y, Jheon S, Li H, Zhang H, Xie Y, Qian B, et al. Results of low-dose computed tomography as a regular health examination among Chinese hospital employees. J Thorac Cardiovasc Surg (2020) 160:824–831.e4. doi: 10.1016/j.jtcvs.2019.10.145
14. Yang W, Qian F, Teng J, Wang H, Manegold C, Pilz LR, et al. Community-based lung cancer screening with low-dose CT in China: Results of the baseline screening. Lung Cancer (2018) 117:20–6. doi: 10.1016/j.lungcan.2018.01.003
15. Park CK, Kim SJ. Trends and updated statistics of lung cancer in Korea. Tuberc Respir Dis (Seoul) (2019) 82:175–7. doi: 10.4046/trd.2019.0015
16. Lim JU, Han S, Kim HC, Choi CM, Jung CY, Cho DG, et al. Characteristics of female lung cancer in Korea: Analysis of Korean national lung cancer registry. J Thorac Dis (2020) 12:4612–22. doi: 10.21037/jtd-20-1671
17. Kerpel-Fronius A, Tammemägi M, Cavic M, Henschke C, Jiang L, Kazerooni E, et al. Screening for lung cancer in individuals who never smoked: An international association for the study of lung cancer early detection and screening committee report. J Thorac Oncol (2022) 17:56–66. doi: 10.1016/j.jtho.2021.07.031
18. Ni X, Xu N, Wang Q. Meta-analysis and systematic review in environmental tobacco smoke risk of female lung cancer by research type. Int J Environ Res Public Health (2018) 15(7). doi: 10.3390/ijerph15071348
19. Domagala-Kulawik J, Trojnar A. Lung cancer in women in 21th century. J Thorac Dis (2020) 12:4398–410. doi: 10.21037/jtd-20-287
20. World Health Organization. WHO report on the global tobacco epidemic(2017). Available at: http://www.who.int/tobacco/global_report/2017/en/ (Accessed November 5, 2018).
21. Passey ME, Longman JM, Robinson J, Wiggers J, Jones LL. Smoke-free homes: What are the barriers, motivators and enablers? a qualitative systematic review and thematic synthesis. BMJ Open (2016) 6:e010260. doi: 10.1136/bmjopen-2015-010260
22. Mao A. Space and power: Young mothers’ management of smoking in extended families in China. Health Place (2013) 21:102–9. doi: 10.1016/j.healthplace.2013.01.015
23. Blanchard EM, Arnaoutakis K, Hesketh PJ. Lung cancer in octogenarians. J Thorac Oncol (2010) 5:909–16. doi: 10.1097/jto.0b013e3181d89b48
24. Boffetta P. What proportion of lung cancer in never-smokers can be attributed to known risk factors? Int J Cancer (2012) 131:265–75. doi: 10.1002/ijc.27477
25. Li N, Tan F, Chen W, Dai M, Wang F, Shen S, et al. One-off low-dose CT for lung cancer screening in China: A multicentre, population-based, prospective cohort study. Lancet Respir Med (2022) 10:378–91. doi: 10.1016/S2213-2600(21)00560-9
26. Zhou Q, Fan Y, Wang Y, Qiao Y, Wang G, Huang Y, et al. China National lung cancer screening guideline with low-dose computed tomography (2018 version). Chin J Lung Cancer (2018) 21:67–75. doi: 10.3779/j.issn.1009-3419.2018.02.01
27. Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WEE, et al. The IASLC lung cancer staging project: Proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J Thorac Oncol (2016) 11:39–51. doi: 10.1016/j.jtho.2015.09.009
28. Xie L, Qian Y, Liu Y, Li Y, Jia S, Yu H, et al. Distinctive lung cancer incidence trends among men and women attributable to the period effect in shanghai: An analysis spanning 42 years. Cancer Med (2020) 9:2930–9. doi: 10.1002/cam4.2917
29. Mazzone PJ, Silvestri GA, Souter LH, Caverly TJ, Kanne JP, Katki HA, et al. Screening for lung cancer: CHEST guideline and expert panel report. Chest (2021) 160:e427–94. doi: 10.1016/j.chest.2021.06.063
30. Pastorino U, Rossi M, Rosato V, Marchianò A, Sverzellati N, Morosi C, et al. Annual or biennial CT screening versus observation in heavy smokers: 5-year results of the mild trial. Eur J Cancer Prev (2012) 21:308–15. doi: 10.1097/CEJ.0b013e328351e1b6
31. Field JK, Duffy SW, Baldwin DR, Whynes DK, Devaraj A, Brain KE, et al. UK Lung cancer RCT pilot screening trial: Baseline findings from the screening arm provide evidence for the potential implementation of lung cancer screening. Thorax (2016) 71:161–70. doi: 10.1136/thoraxjnl-2015-207140
32. Gould MK, Tang T, Liu IL, Lee J, Zheng C, Danforth KN, et al. Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med (2015) 192:1208–14. doi: 10.1164/rccm.201505-0990OC
33. Yip R, Yankelevitz DF, Hu M, Li K, Xu DM, Jirapatnakul A, et al. Lung cancer deaths in the national lung screening trial attributed to nonsolid nodules. Radiology (2016) 281:589–96. doi: 10.1148/radiol.2016152333
34. Yankelevitz DF, Yip R, Smith JP, Liang M, Liu Y, Xu DM, et al. CT screening for lung cancer: Nonsolid nodules in baseline and annual repeat rounds. Radiology (2015) 277:555–64. doi: 10.1148/radiol.2015142554
35. Henschke CI, Yankelevitz DF, Mirtcheva R, McGuinness G, McCauley D, Miettinen OS, et al. CT screening for lung cancer: Frequency and significance of part-solid and nonsolid nodules. AJR Am J Roentgenol (2002) 178:1053–7. doi: 10.2214/ajr.178.5.1781053
36. Frille A, Hardavella G, Lee R. Lung cancer incidence and mortality with extended follow-up in the national LungScreening trial. Breathe (Sheff) (2020) 16:190322. doi: 10.1183/20734735.0322-2019
37. Luo X, Zheng S, Liu Q, Wang S, Li Y, Shen L, et al. Should nonsmokers be excluded from early lung cancer screening with low-dose spiral computed tomography? community-based practice in shanghai. Transl Oncol (2017) 10:485–90. doi: 10.1016/j.tranon.2017.02.002
38. Du Y, Cui X, Sidorenkov G, Groen HJM, Vliegenthart R, Heuvelmans MA, et al. Lung cancer occurrence attributable to passive smoking among never smokers in China: A systematic review and meta-analysis. Transl Lung Cancer Res (2020) 9:204–17. doi: 10.21037/tlcr.2020.02.11
39. Triphuridet N, Henschke C. Landscape on CT screening for lung cancer in Asia. Lung Cancer (Auckl) (2019) 10:107–24. doi: 10.2147/LCTT.S192643
40. Randhawa SK, Puri V. Commentary: The changing risk paradigm in lung cancer: Are we opening pandora’s box? J Thorac Cardiovasc Surg (2020) 160:836–7. doi: 10.1016/j.jtcvs.2019.12.037
41. Abdel-Rahman O. Incidence and mortality of lung cancer among never smokers in relationship to secondhand smoking: Findings from the PLCO trial. Clin Lung Cancer (2020) 21:415–420.e2. doi: 10.1016/j.cllc.2020.04.009
42. Adami HO, Bretthauer M, Kalager M. Assessment of cancer screening effectiveness in the era of screening programs. Eur J Epidemiol (2020) 35(10):891–7. doi: 10.1007/s10654-020-00684-7
43. Gao W, Wen CP, Wu A, Welch HG. Association of computed tomographic screening promotion with lung cancer overdiagnosis among Asian women. JAMA Intern Med (2022) 182(3):283–90. doi: 10.1001/jamainternmed.2021.7769
44. Kakinuma R, Noguchi M, Ashizawa K, Kuriyama K, Maeshima AM, Koizumi N, et al. Natural history of pulmonary subsolid nodules: A prospective multicenter study. J Thorac Oncol (2016) 11:1012–28. doi: 10.1016/j.jtho.2016.04.006
45. Tang EK, Chen CS, Wu CC, Wu MT, Yang TL, Liang HL, et al. Natural history of persistent pulmonary subsolid nodules: Long-term observation of different interval growth. Heart Lung Circ (2019) 28:1747–54. doi: 10.1016/j.hlc.2018.08.015
46. Lee HW, Jin KN, Lee JK, Kim DK, Chung HS, Heo EY, et al. Long-term follow-up of ground-glass nodules after 5 years of stability. J Thorac Oncol (2019) 14:1370–7. doi: 10.1016/j.jtho.2019.05.005
47. Henschke CI, Wisnivesky JP, Yankelevitz DF, Miettinen OS. Small stage I cancers of the lung: Genuineness and curability. Lung Cancer (2003) 39:327–30. doi: 10.1016/s0169-5002(02)00503-2
48. Zhang Y, Chen Z, Hu H, Chen H. Surgical strategies for pre- and minimally invasive lung adenocarcinoma 3.0: Lessons learned from the optimal timing of surgical intervention. Semin Thorac Cardiovasc Surg (2022) 34:311–4. doi: 10.1053/j.semtcvs.2020.12.009
49. Chen KN. Commentary: Pay attention to low-risk populations for lung cancer, but cautiously interpret ground-glass nodules screened by low-dose computed tomography scan. J Thorac Cardiovasc Surg (2020) 160(3):833–4. doi: 10.1016/j.jtcvs.2019.10.204
Keywords: female lung cancer, low-dose computed tomography, lung cancer screening, passive smoking, randomized controlled trial
Citation: Rong F, Shi R, Hu L, Chen R, Wang D, Lv X, Zhao Y, Huang W, Yang Y, Zhou H and Hong K (2022) Low-dose computed tomography for lung cancer screening in Anhui, China: A randomized controlled trial. Front. Oncol. 12:1059999. doi: 10.3389/fonc.2022.1059999
Received: 02 October 2022; Accepted: 30 November 2022;
Published: 14 December 2022.
Edited by:
Giuseppe Cardillo, San Camillo Forlanini Hospital, Thoracic Surgery, ItalyReviewed by:
Maurizio Infante, Integrated University Hospital Verona, ItalyCopyright © 2022 Rong, Shi, Hu, Chen, Wang, Lv, Zhao, Huang, Yang, Zhou and Hong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feng Rong, d2F6aGwxOTk2QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.