 Yang Yu1,2†
Yang Yu1,2† Chuyun Chen
Chuyun Chen Zheng Zhang
Zheng Zhang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 27 September 2022
Sec. Genitourinary Oncology
Volume 12 - 2022 | https://doi.org/10.3389/fonc.2022.1024342
This article is part of the Research Topic Molecular Mechanism, Diagnosis, and Treatment of Adrenal Tumors View all 6 articles
Objective: To analyze the correlation between metanephrine and normetanephrines (MNs) and subclinical myocardial injuries (SMI) diagnosed by low left ventricular global longitudinal strain (LV GLS) in patients with pheochromocytoma and paraganglioma (PPGL).
Methods: Seventy-six patients who underwent surgery for pheochromocytoma or paraganglioma from September 2017 to April 2022 were examined. All the patients enrolled had normal left ventricular ejection fraction (LVEF) and myocardial injury biomarkers including cardiac troponin I and B-natriuretic peptide. Univariate analysis and multivariate analysis were performed to evaluate the association of MNs and subclinical myocardial injury (SMI)(defined as LV GLS<18).
Results: LV GLS of 13(17.11%) PPGL patients was less than 18. The percentage of patients with elevation of single hormone (metanephrine, normetanephrine, 3-methoxytyramine) or any one of MNs was not significantly correlated with SMI (P=0.987, 0.666, 0.128 and 0.918, respectively). All MNs elevation was associated with SMI (OR: 11.27; 95% CI, 0.94—135.24; P= 0.056). After adjusting for age, All MNs elevation was significantly correlated with SMI (OR: 16.54; 95% CI, 1.22—223.62; P= 0.035).
Conclusion: MNs might be an important factor influencing myocardial function. All MNs elevation might indicate SMI. If all MNs elevated, LV GLS measurement was recommended for PPGL patients to detect SMI in the absence of decrease LVEF or other heart disease in clinical practice.
Pheochromocytomas and paragangliomas (PPGL) are catecholamine-producing neuroendocrine tumor and surgery is the only curative therapy at present. One of the main causes of perioperative complications and death in PPGL patients is myocardial injury, including stress cardiomyopathy, hypertrophic myocardiopathy, dilated cardiomyopathy and myocardial ischemia (1). Therefore, how to identify the myocardial injury early and implement efficacious treatments before surgery are key steps to ensure the safety during the surgery (2). In previous studies, subclinical myocardial injury (SMI) is defined as left ventricular ejection fraction (LVEF) impairment and/or elevation of myocardial injury markers, without any symptoms. This definition emphasizes that the PPGL patients do not show any clinical symptoms. Given that routine examinations before surgery consist of echocardiography and myocardial enzyme test, so called SMI is easily identifiable and attached more attention by the surgeons. Therefore, the patients with PPGL who has normal LVEF, cardiac enzyme, B-natriuretic peptide (BNP) and no symptoms seems more likely to be overlooked in clinical practice, while the cardiac function of these patients seem to be normal, but serious in fact. Recently, left ventricular global longitudinal strain (LV GLS) is given more and more attention and recognized as an accurate and sensitive index in early detection of myocardial injury before LVEF impairment (3). In this retrospective study, SMI was innovatively defined as the patients with normal LVEF, cardiac enzyme, BNP and no symptoms, but with low LV GLS. Early identification and treatment for real SMI would be helpful for perioperation management. Considering preoperative LV GLS measurement is uncommon now and lacking of studies in PPGL, complete echocardiography images before surgery are remeasured and analyzed for LV GLS in this study. Our study aims at examining the correlation between clinical parameters, especially MNs, and SMI with innovative definition in PPGL patients.
Patients who underwent surgery for PPGL from September 2017 to April 2022 in Peking University First Hospital and tested for plasma MNs (including metanephrine (MN), normetanephrine (NMN), 3-methoxytyramine (3-MT)) before surgery were initially enrolled as potential participants (N=262). A retrospective study design was used. The patients who met any of the following criteria were excluded (1): surgery involving non-tumor organs (2); incomplete data abstracted from the electronic medical records (3); missing echocardiography images before surgery or poor image quality (unable to obtain adequate tracking quality in more than two left ventricular (LV) segments during offline strain analysis); (4) complicated with heart disease including catecholamine cardiomyopathy (CC) or LVEF <50%; (5) elevation of cardiac troponin I or hypersensitive troponin I or BNP before surgery. Finally, 76 patients were enrolled. The study protocol was approved by the ethics committee of Peking University First Hospital. Written informed consent for participation was not required and the study was conducted in accordance with the Declaration of Helsinki.
For each patient, we reviewed the medical records to collect information including patient demographics, medical history, the highest systolic blood pressure (SBP) and diastolic blood pressure (DBP) before surgery, biochemical test, and tumor size in postoperative pathologic examination. All biochemical test values were defined to be positive if beyond the upper limit of the normal range. Patients were divided into two groups: no myocardial injury (defined as LV GLS≥18) and SMI (defined as LV GLS<18) (4).
All patients’ echocardiographs before surgery were digitally recorded and remeasured for LV function following the echocardiography core laboratory protocol based on American Society of Echocardiography guidelines (3), with standard commercially available cardiac ultrasonography equipment of several manufacturers. LV GLS was measured offline using exported raw DICOM images and a post processing analysis package (Image-Arena, TOMTEC). Peak segmental strain values from apical 2-, 3-, and 4-chamber views were averaged to calculate peak LV GLS.
15 randomly selected patients’ LV GLS were remeasured by the same observer blinded to previous measurements with 1 week interval, and by a second observer blinded to the first one’s results to assess intra- and inter- observer variability.
Continuous variables were presented as mean ± standard deviation or median [Percentile 25, Percentile 75]. Categorical variables were presented as number with percentage(%). Differences between the two groups were compared using Student’s t-test or the χ2 test. Univariate analysis and multivariate analysis were performed to evaluate the association of MNs and LV GLS. Covariates were included as potential confounders in the adjusted model if P ≤ 0.1. All P values were two-sided and were considered statistically significant if less than 0.05. All analyses were performed with statistical software (Empower(R), www.empowerstats.com; X&Y solutions, Inc., Boston, MA, USA; R [http://www.R-project.org].v4.2.0).
In this retrospective study, the average age was 46.34 ± 15.04 years and 34 (44.74%) of the patients were male. LV GLS in 13(17.11%) patients was less than 18. Additionally, 39 (51.32%) had history of hypertension, 18 (23.68%) had history of diabetes, and 4 (5.33%) had history of stroke. LV GLS in two group were 21.94 ± 2.45 (no myocardial injury), 14.90 ± 1.81 (SMI), respectively. Elevation of single hormone (MN, NMN, 3-MT) was no different in the groups (P=0.987, 0.665 and 0.111, respectively). However, the rate of elevation of all MNs was 1.59% and 15.38% (P=0.020). And there were no differences in other factors among the groups (Table 1).
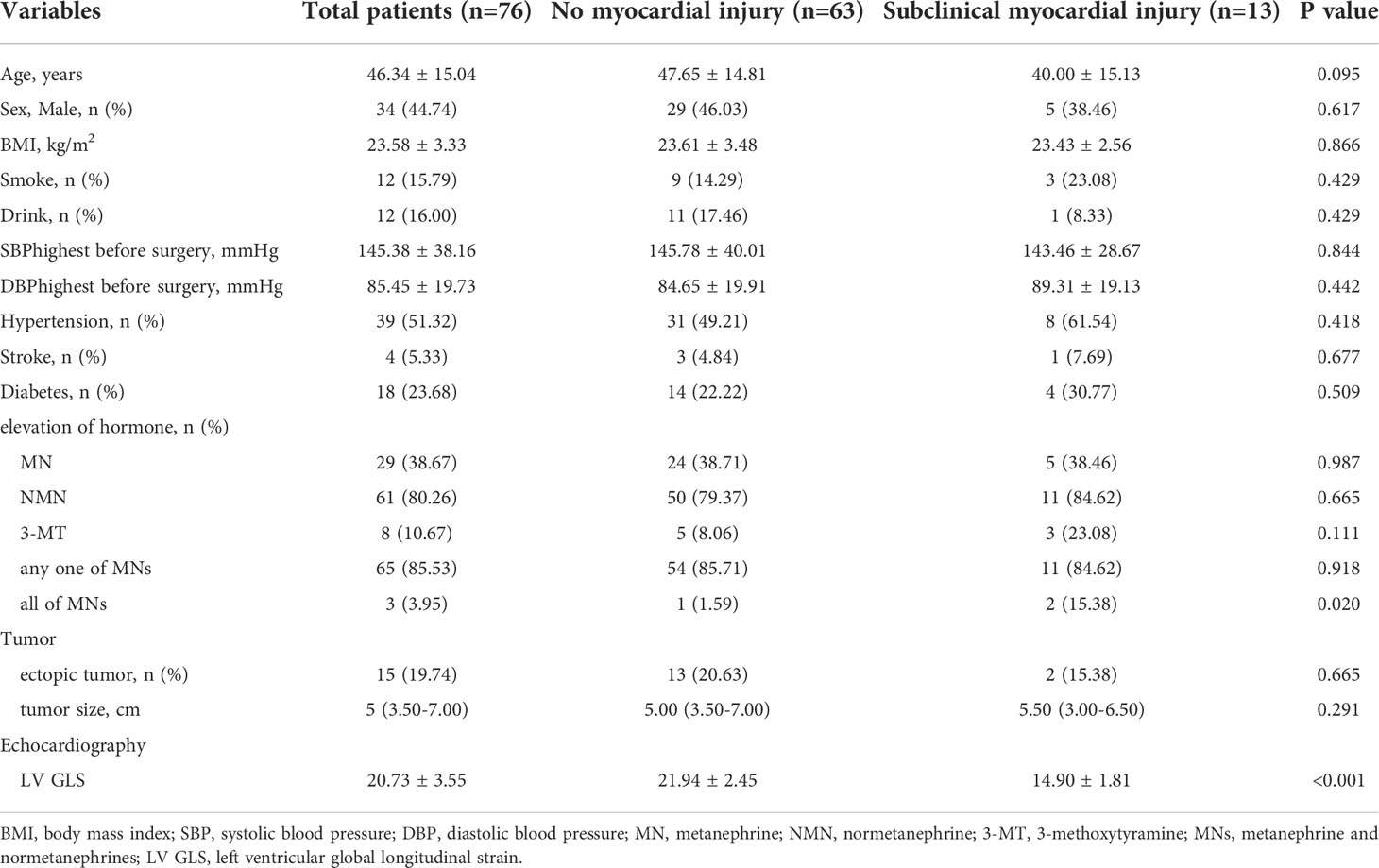
Table 1 Characteristics of all PCGL patients.
Univariate correlations of LV GLS included demographic parameters (age, sex, body mass index, smoke, drink, SBP highest before surgery, DBP highest before surgery, HT, stroke and Diabetes), elevation of hormone (MN, NMN, 3-MT, any one of MNs, all of MNs) and tumor condition (tumor size and ectopic tumor) (Table 2).
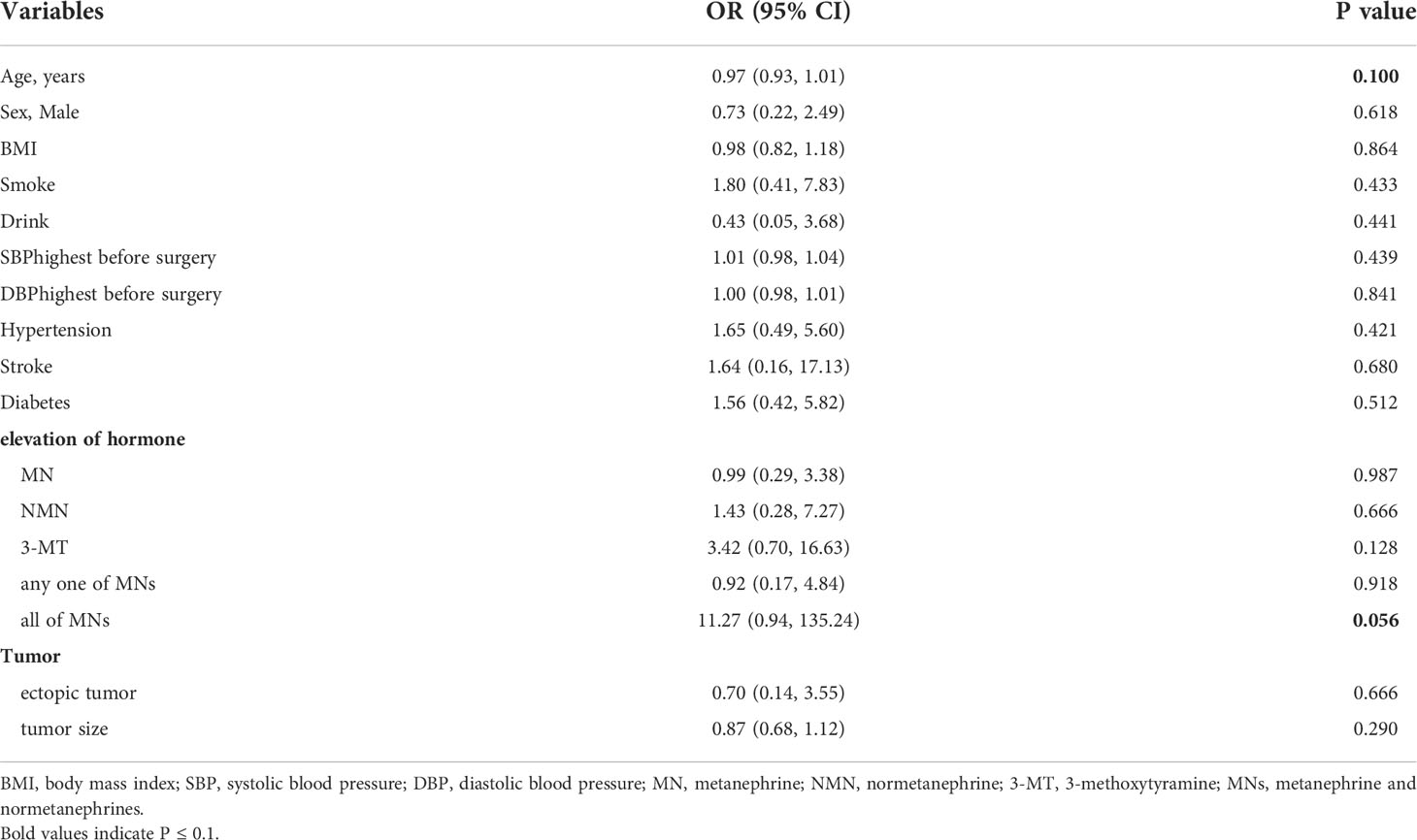
Table 2 Results of univariate analysis.
Overall, elevation of single hormone (MN, NMN, 3-MT) or any one of MNs was not associated with SMI (P=0.987, 0.666, 0.128 and 0.918, respectively). However, compared with patients with no elevation of MNs, the OR for patients with all MNs elevation was 11.27 (95% CI, 0.94—135.24)(P= 0.056).
Given that age was related to LV GLS (5) (OR: 0.97; 95% CI, 0.93—1.01; P= 0.100) and small sample of the study, multiple regression analysis was performed with age adjusted only (Table 3). Elevation of all MNs was associated with SMI (OR: 16.54; 95% CI, 1.22—223.62; P= 0.035), which was in accordance with the results in univariate analysis.
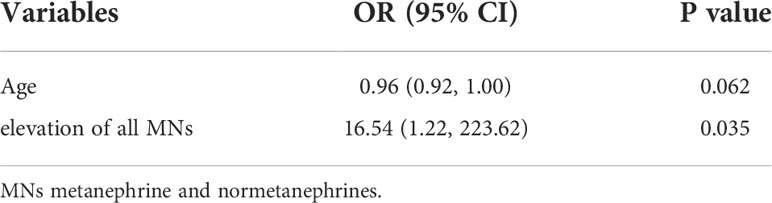
Table 3 Results of multivariate analysis.
The intra- and inter- observer intraclass correlation coefficient (ICC) for LV GLS was 0.968 (95%CI: 0.911 -0.989) and 0.982 (95%CI: 0.949 - 0.994), respectively.
As a severe complication of PPGL, CC was a specific cardiomyopathy disease, influencing the cardiac structure and function due to the circulating catecholamine (CA) beyond physical dosage. It was reported that CA had direct effects on the systolic function of LV myocardium and 8-11% of PPGL patients would develop CC (6–8). Mortality rate of CC patients were high at 33% without surgery (9). Perioperative complications would occur in 20-23% CC patients in spite of adequate preoperative preparation. If CC was missed diagnosis or the patient was not fully prepared for the operation, the incidence of perioperative complications and mortality of PPGL surgery would increase to 67-70% and 6-33%, respectively (10).
Symmetric LV hypertrophy was the main pathological characteristic of CC. Myocarditis was found in about 50-60% of PPGL patients at autopsy, with degeneration, contraction band necrosis, inflammatory cells infiltrating and fibrosis during later period. And sarcomere excess contraction, mitochondria swelling and endoplasmic reticulum dilatation could also be observed clearly under electronic microscope, which were entirely different from coagulative necrosis in myocardial infarction (11). Although different from the pathogenic mechanism of ischemic heart disease, it was uncommon to confirm the diagnosis of CC in the early stage and the diagnosis was made by exclusion of other organic heart disease. CC was mainly manifested as high levels of cardiac injury markers and significant decline of LVEF, which indicated clinical myocardial injury (12). Under this condition, the patients had missed the optimal surgery opportunity, bringing about tremendous challenges for the surgeons to prepare for the operation (13). Meune et al. (2) found that subclinical LV systolic dysfunction actually existed in PPGL patients, while whose echocardiogram report were usually normal at the same time. Their study also showed that subclinical LV systolic dysfunction was related to the circulatory failure during the surgery. Unfortunately, there was no well-defined or standard criterion for SMI in their research. Recently, LV GLS was given more attention and played an essential role in SMI (14). Furthermore, LV GLS was regarded as an accurate and sensitive index in early detection of subclinical alterations in LV longitudinal function, which occured before LVEF impairment, myocardial biomarkers elevation and clinical symptoms (15–17). Therefore, the definition of SMI in this study covered the earliest period of cardiac damage which tended to be ignored usually in clinical practice.
We used TOMTEC in LV GLS measurement in the current study and an absolute number of 18% as the cutoff value according to published literature (3–5). LV GLS of 13 (17.11%) patients was less than 18 in our study, but with normal LVEF and myocardial injury biomarkers. This proportion was firstly reported in our study, indicating that some patients with SMI were overlooked during traditional preoperative procedure. The perioperative risks might have increased in such situations.
Although CA was reported to be associated with myocardial injury in PPGL patients in previous research or hypothesis of mechanism, it was still controversial what risk factors increased the probability of injury. In a 15 cases study, there was no correlation between plasma epinephrine or noradrenaline level and LV structural parameters of echocardiography in 6 LV hypertrophy patients (18). However, noradrenaline was thought to be a risk factor of acute cardial complications in the other study (14). One of the most probable reasons was the episodic secretion of epinephrine, noradrenaline or dopamine, making the tests not necessarily reflecting the plasma concentrations of CA on time (19). Furthermore, myocardial injury might be a chronic pathophysiological process, involving the gradual accumulation of CA (20, 21). MNs, intermediate metabolites of CA, were the most accurate index in reflection of tumor condition and the chronic hormone accumulative process. For a consideration of these problems, only patients who tested for all three MNs (MN, NMN and 3-MT) before surgery were enrolled in our study.
In general, CA could cause myocardial injury through chronic and continuous exposure, overexcitation of receptors and desensitization of beta receptors. Large amounts of studies showed that the mechanisms of different CA acting on myocardial injury seemed to be various. Norepinephrine could augment myocardial oxygen demand, cell death and injury and attenuate cardiac performance, thus leading to systolic heart failure and dilated dilated cardiomyopathy (22). The adrenochrome, which was formed through oxidation of epinephrine by tyrosine (23), induced arrhythmias and sudden cardiac death in anesthetized rats (24). Yates et al. (1) found that dopamine-secreting pheochromocytoma might present with hypotension, on account of the effect on β2-adrenoceptors situated on smooth muscles or peripheral arteries. Based on the above, elevation of single MNs (MN, NMN, 3-MT), any one of MNs and all MNs were all analyzed in our study. The results demonstrated that the co-hypersecretion of three MNS was the only factor associated with SMI. And tomor size was not significant associated with SMI, neither was ectopic tumor, which was consistent with the results of several previous studies (8, 25, 26). Co-hypersecretion of three MNs was first described associated with SMI. This may be partly explained by the inclusion criteria, PPGL patients with completely normal LVEF and myocardial injury biomarker, which was quite different from prior studies. It was speculated that the pathogenic mechanism of SMI was different from clinical myocardial injury. As for the type of CA secretion, in most patients with acute myocardial injury, epinephrine secretion was present (14, 27), revealing that the episodical release of epinephrine might cause sudden cardiac decompensation, as opposed to the persistent storage and release of norepinephrine (28, 29). In this study, it was supposed that co-hypersecretion of three types of CA may cause chronic injury to myocardium in some PPGL patients through various receptors and signal pathways, presenting SMI. On the other hand, sharp rise of certain types of CA may directly cause acute myocardial injury, diagnosed as CC. Although the above hypothesis need further study to confirm, for the patients with co-elevation of three plasma MNs, LV GLS measurement was strongly suggested for the early detection of SMI.
Some limitations could not be ignored in the study. Firstly, inevitable bias existed in the retrospective study. Secondly, based on a small sample, LV GLS<18 patients were few in number. Moreover, lack of postoperative follow-up and echocardiography made it impossible to compare the changes of LV GLS. Lastly, qualitative analysis rather than quantitative analysis was used in the elevation of MNs.
In summary, MNs might be an important factor influencing myocardial function. All MNs elevation might indicate SMI. If all MNs elevated, LV GLS measurement was recommended for PPGL patients to detect SMI in the absence of decrease LVEF or other heart disease in clinical practice.
The datasets presented in this article are not readily available because The data that support the findings of this study are available from the corresponding author upon reasonable request after the request is submitted and formally reviewed and approved by the ethics committee of Peking University First Hospital. Requests to access the datasets should be directed to ZG9jemh6QGFsaXl1bi5jb20=.
The studies involving human participants were reviewed and approved by the ethics committee of Peking University First Hospital. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
ZZ and YiY: conception and design. YY, CC and WH: acquisition of data and critical revision of the manuscript for important intellectual content. YY and CC: analysis and interpretation of data, drafting of the manuscript. ZZ, YZ and YiY: supervision. All authors contributed to the article and approved the submitted version.
This work was supported by the National High Level Hospital Clinical Research Funding (Scientific and Technological Achievements Transformation Incubation Guidance Fund Project of Peking University First Hospital) (2022CX08).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Santos JR, Brofferio A, Viana B, Pacak K. Catecholamine-induced cardiomyopathy in pheochromocytoma: How to manage a rare complication in a rare disease? Horm Metab Res (2019) 51(7):458–69. doi: 10.1055/a-0669-9556
2. Meune C, Bedhemt J, Dousset B, Jude N, Bertagna X, Duboc D, et al. Reduced myocardial contractility assessed by tissue Doppler echocardiography is associated with increased risk during adrenal surgery of patients with increased risk during adrenal surgery of patients with pheochromocytoma: Report of a preliminary study. J Am Soc Eehocardiogr (2006) 19(12):1466–70. doi: 10.1016/j.echo.2006.06.014
3. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr (2015) 28(1):1–39.e14. doi: 10.1016/j.echo.2014.10.003
4. Galderisi M, Cosyns B, Edvardsen T, Cardim N, Delgado V, Di Salvo G, et al. 2016–2018 EACVI scientific documents committee; 2016–2018 EACVI scientific documents committee. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European association of cardiovascular imaging. Eur Heart J Cardiovasc Imaging (2017) 18(12):1301–10. doi: 10.1093/ehjci/jex244
5. D'Elia N, Caselli S, Kosmala W, Lancellotti P, Morris D, Muraru D, et al. Normal global longitudinal strain: An individual patient meta-analysis. JACC Cardiovasc Imaging (2020) 13(1 Pt 1):167–9. doi: 10.1016/j.jcmg.2019.07.020
6. Otusanya O, Goraya H, Iyer P, Landi K, Tibb A, Msaouel P, et al. A vicious cycle of acute catecholamine cardiomyopathy and circulatory collapse secondary to pheochromocytoma. Oxf Med Case Rep (2015) 10:343–5. doi: 10.1093/omcr/omv058
7. Park JH, Kim KS, Sul JY, Shin SK, Kim JH, Lee JH, et al. Prevalence and patterns of left ventricular dysfunction in patients with pheochromocytoma. J Cardiovasc Ultrasound (2011) 19(2):76–82. doi: 10.4250/jcu.2011.19.2.76
8. Giavarini A, Chedid A, Bobrie G, Plouin PF, Hagège A, Amar L, et al. Acute catecholamine cardiomyopathy in patients with phaeochromocytoma or functional paraganglioma. Heart (2013) 99(19):1438–44. doi: 10.1136/heartjnl-2013-304073
9. Dalby MC, Burke M, Radley-smith R, Banner NR. Pheochromocytoma presenting after cardiac transplantation for dilated cardiomyopathy. J Heart Lung Transplant (2001) 20(7):773–5. doi: 10.1016/s1053-2498(00)00233-3
10. Scholten A, Cisco RM, Vriens MR, Cohen JK, Mitmaker EJ, Liu C, et al. Pheochromocytoma crisis is not a surgical emergency. J Clin Endocrinol Metab (2013) 98(2):581–91. doi: 10.1210/jc.2012-3020
11. Miura M, Kawano H, Yoshida T, Yamagata Y, Nakata T, Koga S, et al. The histological features of a myocardial biopsy specimen in a patient in the acute phase of reversible catecholamine-induced cardiomyopathy due to pheochromocytoma. Intern Med (2017) 56(6):665–71. doi: 10.2169/internalmedicine.56.7454
12. Lyon AR, Bossone E, Schneider B, Sechtem U, Citro R, Underwood SR, et al. Current state of knowledge on takotsubo syndrome: A position statement from the taskforce on takotsubo syndrome of the heart failure association of the European society of cardiology. Eur J Heart Fail (2016) 18(1):8–27. doi: 10.1002/ejhf.424
13. Kassim TA, Clarke DD, Mai VQ, Clyde PW, Mohamed Shakir KM. Catecholamine-induced cardiomyopathy. Endocr Pract (2008) 14(9):1137–49. doi: 10.4158/EP.14.9.1137
14. Zhou J, Xuan He, Miao Y, Dai Y. Acute cardiac complications and subclinical myocardial injuries associated with pheochromocytoma and paraganglioma. BMC Cardiovasc Disord (2021) 21(1):203. doi: 10.1186/s12872-021-02013-6
15. Bonsignore A, Marwick TH, Adams SC, Thampinathan B, Somerset E, Amir E, et al. Clinical, echocardiographic, and biomarker associations with impaired cardiorespiratory fitness early after HER2-targeted breast cancer therapy. JACC CardioOncol (2021) 3(5):678–91. doi: 10.1016/j.jaccao.2021.08.010
16. Esmaeilzadeh M, Urzua Fresno CM, Somerset E, Shalmon T, Amir E, Fan CS, et al. A combined echocardiography approach for the diagnosis of cancer therapy-related cardiac dysfunction in women with early-stage breast cancer. JAMA Cardiol (2022) 7(3):330–40. doi: 10.1001/jamacardio.2021.5881
17. Haji K, Huynh Q, Wong C, Stewart S, Carrington M, Marwick TH, et al. Improving the characterization of stage a and b heart failure by adding global longitudinal strain. JACC Cardiovasc Imaging (2022) 15(8):1380–7. doi: 10.1016/j.jcmg.2022.03.007
18. Galetta F, Franzoni F, Bernini G, Poupak F, Carpi A, Cini G, et al. Cardiovascular complications in patients with pheoehromocytoma: A mini review. BioMed Pharmacother (2010) 64(7):505–9. doi: 10.1016/j.biopha.2009.09.014
19. Lenders JW, Pacak K, Walther MM, Linehan WM, Mannelli M, Friberg P, et al. Biochemical diagnosis of pheochromocytoma: Which test is best? JAMA (2002) 287(11):1427–34. doi: 10.1001/jama.287.11.1427
20. Gervais MK, Gagnon A, Henri M, Bendavid Y. Pheochromocytoma presenting as inverted takotsubo cardiomyopathy: A case report and review of the literature. J Cardiovasc Med (Hagerstown) (2015) 16 Suppl 2:S113–117. doi: 10.2459/JCM.0b013e3283356651
21. Eisenhofor G, Keiocr H, Ftibeg P, Mezey E, Huynh TT, Hiremagalur B, et al. Plasma metanephrines are markers of pheochromocytoma produced by catechol-o-methyltransferase within tumors. J Clin Endocrinol Metab (1998) 83(6):2175–85. doi: 10.1210/jcem.83.6.4870
22. Attar MN, Moulik PK, Salem GD, Rose EL, Khaleeli AA. Phaeochromocytoma presenting as dilated cardiomyopathy. Int J Clin Pract (2003) 57(6):547–8.
23. Green DE, Richter D. Adrenaline and adrenochrome. Biochem J (1937) 31(4):596–616. doi: 10.1042/bj0310596
24. Beamish RE, Dhillon KS, Singal PK, Dhalla NS. Protective effect of sulfinpyrazone against catecholamine metabolite adrenochrome-induced arrhythmias. Am Heart J (1981) 102(2):149–52. doi: 10.1016/s0002-8703(81)80001-4
25. Riester A, Weismann D, Quinkler M, Lichtenauer UD, Sommerey S, Halbritter R, et al. Life-threatening events in patients with pheochromocytoma. Eur J Endocrinol (2015) 173(6):757–64. doi: 10.1530/EJE-15-0483
26. Zelinka T, Petrák O, Turková H, Holaj R, Strauch B, Kršek M, et al. High incidence of cardiovascular complications in pheochromocytoma. Hormone Metab Res (2012) 44(5):379–84. doi: 10.1055/s-0032-1306294
27. Gagnon N, Mansour S, Bitton Y, Bourdeau I. Takotsubo-like cardiomyopathy in a large cohort of patients with pheochromocytoma and paraganglioma. Endocr Pract (2017) 23(10):1178–92. doi: 10.4158/EP171930.OR
28. Gupta G, Pacak K AACE, AACE Adrenal Scientific Committee. Adrenal scientific committee. precision medicine: An update on genotype/biochemical phenotype relationships in pheochromocytoma/paraganglioma patients. Endocr Pract (2017) 23(6):690–704. doi: 10.4158/EP161718.RA
Keywords: pheochromocytoma, metanephrine and normetanephrine, subclinical myocardial injury, left ventricular global longitudinal strain, retrospective study
Citation: Yu Y, Chen C, Han W, Zhang Y, Zhang Z and Yang Y (2022) Metanephrine and normetanephrine associated with subclinical myocardial injuries in pheochromocytoma and paraganglioma. Front. Oncol. 12:1024342. doi: 10.3389/fonc.2022.1024342
Received: 21 August 2022; Accepted: 12 September 2022;
Published: 27 September 2022.
Edited by:
Lu Yang, Sichuan University, ChinaReviewed by:
Meng Zhe, Zhongnan Hospital, Wuhan University, ChinaCopyright © 2022 Yu, Chen, Han, Zhang, Zhang and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zheng Zhang, ZG9jemh6QGFsaXl1bi5jb20=; Ying Yang, eWFuZ3lpbmcxNTI3QDE2My5jb20=
†These authors contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.