 Kemin Li
Kemin Li Zhengyu Li
Zhengyu Li- The Department of Obstetrics and Gynecology, West China Second University Hospital of Sichuan University, Chengdu, China
Background: Frailty has been related with poor prognosis of various diseases, including ovarian cancer. We performed a systematic review and meta-analysis to evaluate the association between frailty and long-term survival of patients with ovarian cancer.
Methods: Relevant cohort studies were retrieved by search of PubMed, Embase, Cochrane’s Library, and Web of Science electronic databases. Two authors independently performed literature search, data collection, and statistical analyses. A random-effect model incorporating the possible influence of heterogeneity was used to pool the results.
Results: Nine cohort studies including 2497 women with confirmed diagnosis of ovarian cancer contributed to the meta-analysis, and 536 (21.5%) of them were with high frailty. The median follow-up durations varied between 24 and 69 months. Compared to patients with low or non-frailty, OC patients with high frailty were associated with poor overall survival (risk ratio [RR]: 1.61, 95% confidence interval [CI]: 1.41 to 1.85, p < 0.001; I2 = 0%) and progression-free survival (RR: 1.51, 95% CI: 1.20 to 1.89, p < 0.001; I2 = 0%). Subgroup analyses according to study design, cancer stage, age of patients, scales for frailty evaluation, follow-up duration, and quality score of the included study showed consistent association between high frailty and poor overall survival in women with ovarian cancer (p for subgroup effects all < 0.05). After considering GRADE criteria for strength of the evidence, it was rated low for both the two outcomes.
Conclusion: High frailty may be an independent risk factor of poor survival in women with ovarian cancer. Evaluating frailty may be important for predicting the prognosis and determining the optimal anticancer treatments in women with ovarian cancer.
Systematic Review Registration: https://inplasy.com/, identifier INPLASY202290028.
Introduction
Currently, ovarian cancer (OC) ranks the fifth leading cause of cancer-related mortality of the global population (1, 2). The incidence of OC is generally lower compared to other gynecological cancers (3). However, because the symptoms of OC tend to be non-specific and the effective screening methods for OC are still lacked, patients with OC are likely to be diagnosed at advanced stage, which may be an important reason for the poor prognosis of these patients (4, 5). Surgical resection is the preferred treatment for OC if diagnosed early (6). Although emerging therapies such as poly (ADP-ribose) polymerase (PARP) inhibitors are being developed in maintenance and recurrence treatment settings of epithelial OC with BRCA 1-2 gene mutation (7), for most patients with advanced OC, tumor debulking followed by adjunctive therapy is recommended (6, 8). Many factors have been proposed to influence the prognosis of patients with OC, such as age, cancer stage, grade, histological type, and anticancer treatments etc. (8, 9). However, for some patients with OC, prognostic prediction remains difficult (10, 11), which highlights the importance of the identification of new prognostic factors in patients with OC.
Recent advances in oncogeriatrics suggested the important role of geriatric evaluation for frailty in the risk stratification and optimized management of patients with cancer (12). By definition, frailty refers to a state of age-related decline in biological reserve, decreased ability to maintain physiological balance and increased vulnerability to adverse health events (13, 14). It has been proposed that frailty may be a key factor which affects the therapeutic efficacy and toxicity of anticancer modalities (15, 16). Accordingly, high frailty has been shown to be a predictor of poor survival in patients with some types of cancers, such as lung cancer (17), prostate cancer (18), colorectal cancer (19), and other digestive system tumors (20). However, studies evaluating the correlation between frailty and survival of patients with OC showed inconsistent results (21–29). Some studies suggested that high frailty was associated with poor survival of these patients (22, 24, 25, 27–29), while others failed to show a significant association (21, 23, 26). Therefore, we performed a systematical review and meta-analysis to comprehensively investigate the relationship between frailty and survival of patients with OC.
Materials and methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (30, 31) was followed in designing, performing, and reporting the meta-analysis was in accordance with the recommendations of the Cochrane’s Handbook (32) guideline. The protocol of the meta-analysis has been registered at INPLASY (International Platform of Registered Systematic Review and Meta-analysis Protocols, https://inplasy.com/) with the registration number of INPLASY202290028).
Literature retrieving
Studies were retrieved by search of PubMed, Embase, Cochrane’s Library and Web of Science electronic databases from the inception to April 2, 2022. A combined search term was used, including (1) “frailty” OR “frail”; (2) “ovarian” OR “ovary”; and (3) “cancer” OR “carcinoma” OR “malignancy” OR “tumor” OR “neoplasm”. The search was limited to human studies published in full-length articles. No restriction was applied regarding the language of publication. As a supplementation, we manually checked the citations of the relevant original and review articles for possible studies of interest.
Study selection
The PICOS criteria were used for study inclusion.
P (patients): Adult patients with histologically confirmed diagnosis of OC, regardless of the cancer stage or treatments.
I (exposure): Patients with high frailty at admission. Methods and criteria for defining patients with frailty were consistent with the modalities used in the original studies.
C (control): Patients with low or non-frailty at admission. The evaluating tools and criteria for the frailty were consistent with those applied among the included studies.
O (outcomes): the primary outcome was overall survival (OS), and the secondary outcomes were progression-free survival (PFS), compared between OC patients with high versus low or non-frailty. Generally, OS was defined as the time elapsed from treatment and to the date of death from any cause, while PFS was defined as the interval between initiation of the treatment and the first recurrence or progression event.
S (study design): cohort studies, including prospective and retrospective cohorts;
Reviews, preclinical studies, studies including non-OC patients, studies that did not evaluate frailty, or studies that did not report the survival outcomes were excluded. In addition, studies with follow-up duration within months were also excluded because we did not aim to evaluate the immediate influence of frailty on mortality of patients with OC.
Data collection and quality assessing
Two independent authors conducted literature search and analysis, data collection, and study quality assessment separately. If discrepancies were encountered, they were resolved by discussion with the third author to reach consensus. Data of study information, design characteristics (prospective or retrospective), patient demographic factors, cancer stage, main treatments, scales for the evaluation of frailty, follow-up durations, outcomes reported, and variables adjusted in the regression model for the analysis of the association between frailty and survival outcomes were collected. Quality of the included studies was evaluated via the Newcastle–Ottawa Scale (33) with scoring regarding the criteria for participant selection, comparability of the groups, and the validity of the outcomes. The scale ranged between 1-9 stars, with larger number of stars presenting higher study quality.
Statistical analyses
The main objective was to determine the relative risks of OS and PFS of OC patients with high versus low or non-frailty, which were presented as risk ratios (RRs) and the confidence intervals (CIs). Using the 95% CIs or p values, data of RRs and the standard errors (SEs) could be calculated, and a subsequent logarithmical transformation was conducted to keep stabilized variance and normalized distribution. Between study heterogeneity was estimated with the Cochrane’s Q test and the I2 statistic (34). The between-study heterogeneity was classed as mild (I2 < 25%), moderate (I2 25%~75%), and high (I2 >75%) according to the Cochrane’s Handbook (32). A random-effect model with the DerSimonian & Laird approach was applied to pool the results after incorporating of possible between-study heterogeneity (32). Influencing analyses by excluding one cohort at a time were performed to evaluate the stability of the results (35). Subgroup analyses were also performed to explore the influences of study characteristics on the outcome. By construction of the funnel plots, the publication bias was estimated based on the visual judgement of the symmetry of the plots, supplemented with the Egger’s regression asymmetry test (36). The Grading of recommendation, assessment, development and evaluation (GRADE) methodology was used to evaluate the quality of the body of retrieved evidence (GRADEpro, https://gdt.gradepro.org/app/#projects). The RevMan (Version 5.1; Cochrane Collaboration, Oxford, UK) and Stata (Version 17.0; Stata Corporation, College Station, TX) software were applied for these analyses, and a p < 0.05 suggests statistical significance.
Results
Studies obtained
Figure 1 shows the process of literature analysis. In short, the initial search of the databases retrieved 389 articles, and 321 were left after excluding the duplicated records. Then, an additional 295 articles were excluded since the contents of the titles and abstracts indicated that they were not relevant to the aim of the meta-analysis, which made a total of 26 studies for the full-text review. Finally, after excluding 17 studies through full-text review, nine studies (21–29) were included. The reasons for the removing of the 17 studies are also presented in Figure 1.
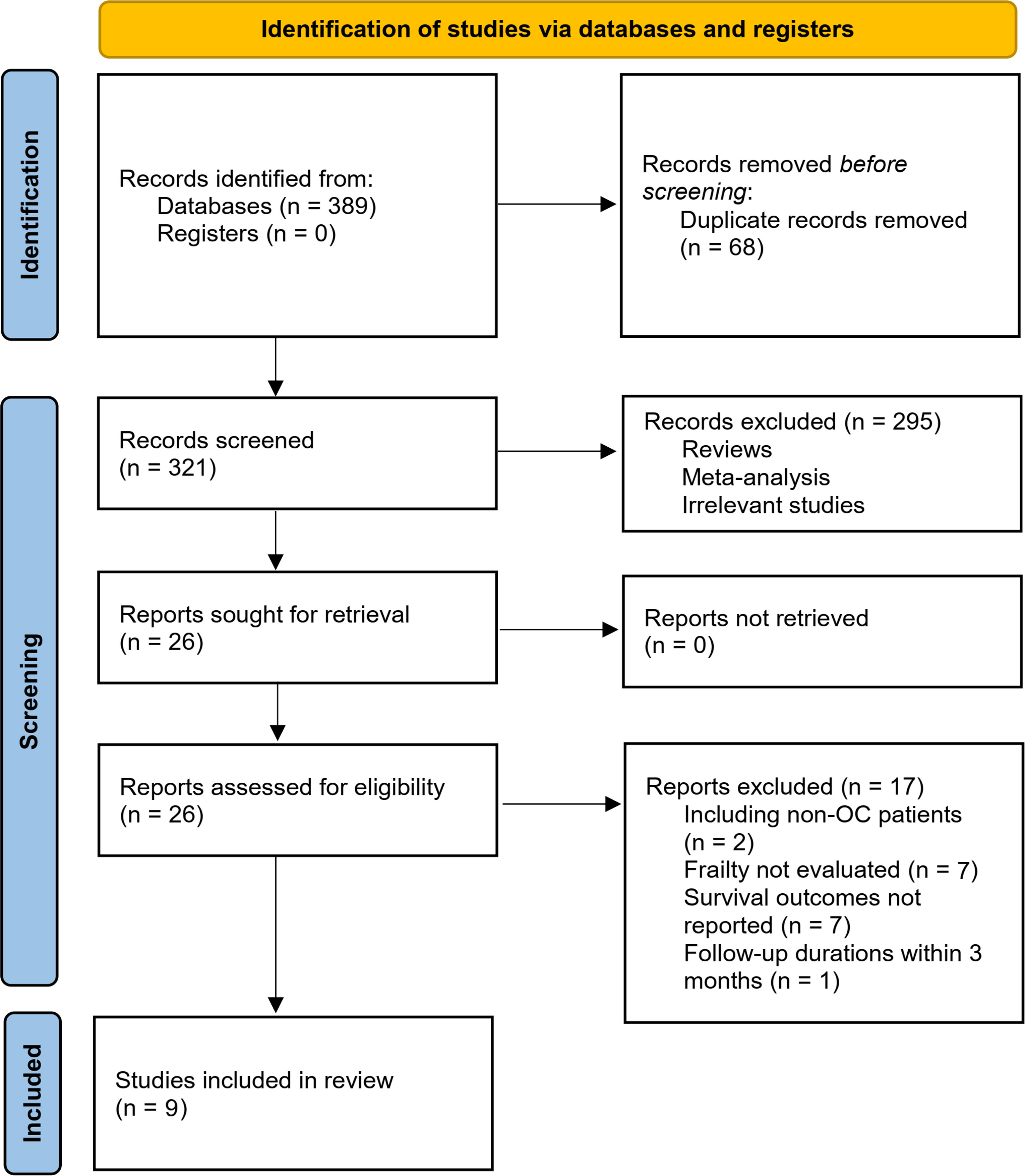
Figure 1 Summarized process of literature search and study identification.
Characteristics of the included studies
As presented in Table 1, nine cohort studies, including two prospective (23, 28) and seven retrospective cohorts (21, 22, 24–27, 29), with 2497 patients with OC contributed to the meta-analysis. These studies were published between 2017 and 2022, and performed in the United States (22, 23, 25, 27, 29), Italy (21), France (24), and Germany (26, 28). All of the studies included patients with confirmed diagnosis of OC, and four studies included older patients only (21, 24, 26, 27). Five studies included patients with stage I-IV OC (21, 23, 24, 26, 28), three studies included patients with stage III-IV OC (22, 25, 27), while the remaining one study included patients with stage II-IV OC (29). Most of the included patients received surgical treatment for OC. Various scales were used for the evaluation of frailty, such as the frailty deficit index (22, 25, 28), the modified frailty index (mFI) (21, 24, 29), the Fried frailty phenotype (23), G-8 score (26), and the memorial Sloan Kettering Frailty Index (27). Accordingly, 536 (21.5%) of the included patients were with high frailty at admission. Among the included studies, three of them compared the survival between patients with high versus low frailty (21, 24, 29), and the other six compared the survival between patients with high versus non-frailty (22, 23, 25–28). The median follow-up durations varied from 24 to 69 months. The OS was reported in all of the nine studies (21–29), while the outcome of PFS was reported in four studies (24–26, 29). Univariate analyses were performed in two studies (21, 24) when the association between frailty and survival outcome was analyzed, while multivariate analyses were performed in seven studies (22, 23, 25–29). Variables such as age, cancer stage, grade, histological type, and concurrent treatments were adjusted in the multivariate models. The NOS of the included studies were 6 to 9 stars, suggesting moderate to good study quality (Table 2).
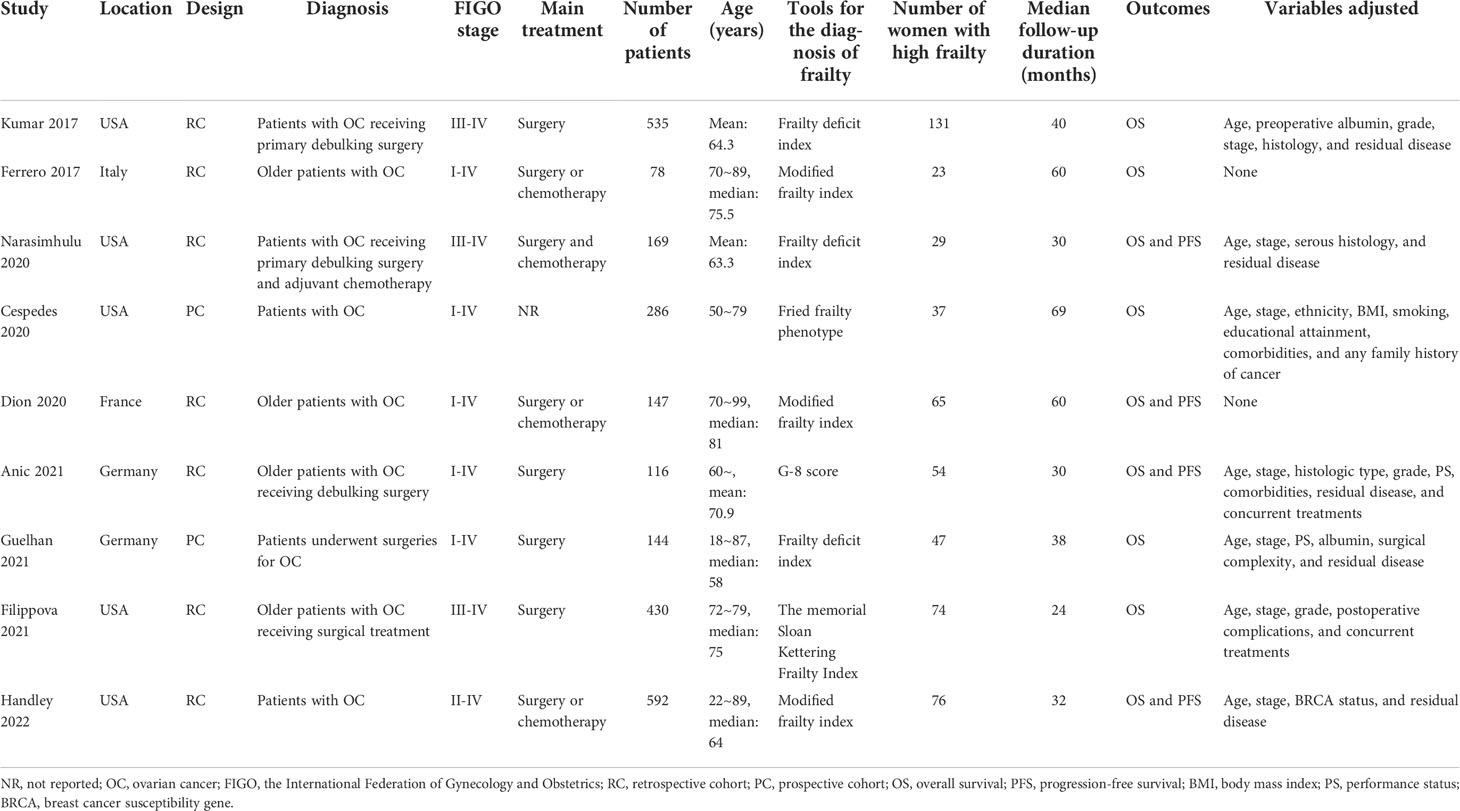
Table 1 Characteristics of the included studies.
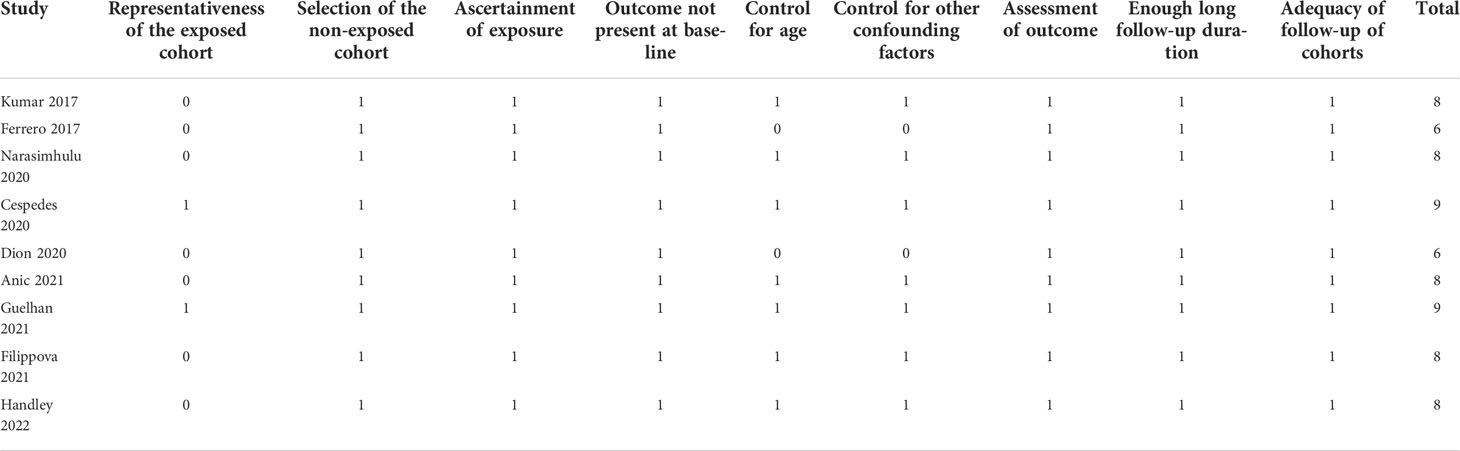
Table 2 Quality evaluation of the included studies.
Frailty and survival of patients with OC
Pooled results with nine studies (21–29) showed that OC patients with high frailty were associated with poor OS compared to low or non-frail patients (RR: 1.61, 95% CI: 1.41 to 1.85, p < 0.001; Figure 2A) with no significant heterogeneity (p for Cochrane’s Q test = 0.95, I2 = 0%). Influencing analyses by omitting one study at a time showed consistent results (RR: 1.58 to 1.67, p all < 0.001; Figure 2B). Subgroup analyses according to study design, cancer stage, age, scale for frailty evaluation, follow-up duration, and quality score of the included study showed consistent association between frailty and poor overall survival in women with ovarian cancer (Table 3, p for subgroup effects all < 0.05). Specifically, subgroup analyses showed consistent association between studies comparing patients with high frailty versus patients with low frailty (RR: 1.76, 95% CI: 1.34 to 2.32, p < 0.001; I2 = 0%) and studies compared to patients with non-frailty (RR: 1.57, 95% CI: 1.34 to 1.84, p < 0.001; I2 = 0%; Table 3). In addition, pooled results with four studies (24–26, 29) also showed that high frailty was associated with poor PFS in patients with OC (RR: 1.51, 95% CI: 1.20 to 1.89, p < 0.001; Figure 3A) with no significant heterogeneity (Cochrane’s Q test = 0.82, I2 = 0%). Similarly, influencing analyses by omitting one study at a time showed consistent results (RR: 1.45 to 1.55, p all < 0.01; Figure 3B).
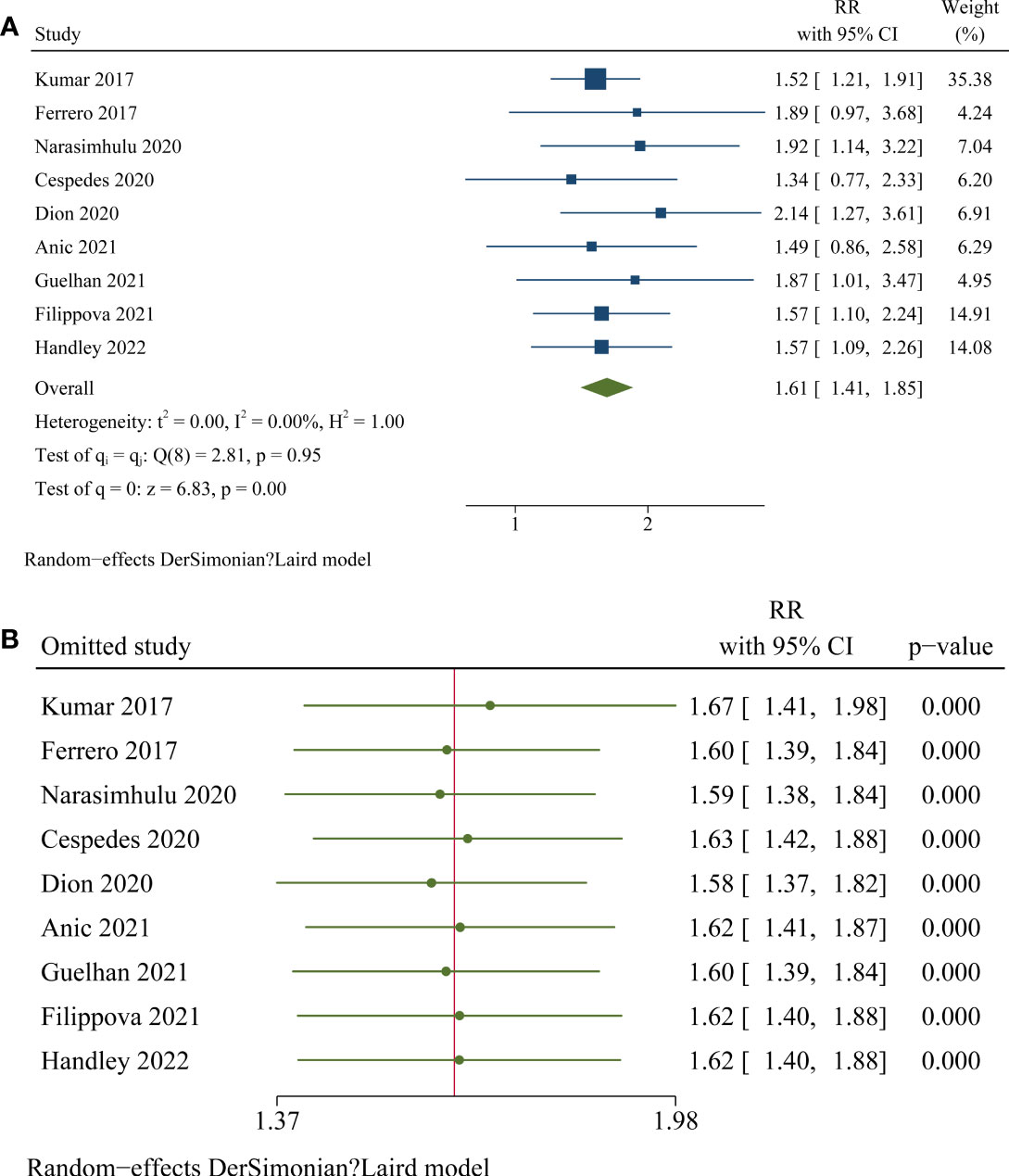
Figure 2 Forest plots for the meta-analyses regarding the association between high frailty and OS in patients with OC. (A), overall meta-analysis; (B), influencing analysis by omitting one study at a time.
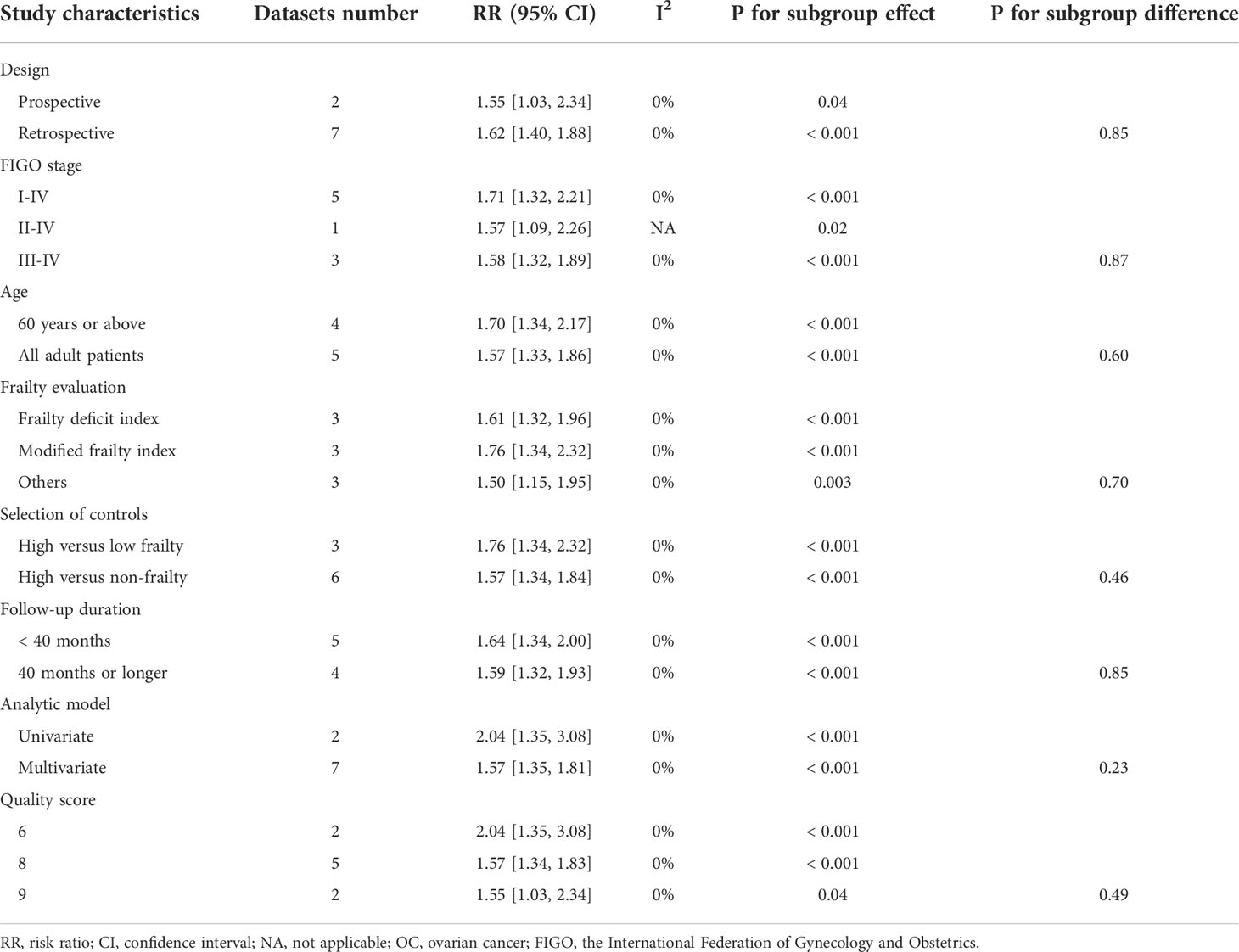
Table 3 Subgroup analyses for the association between frailty and overall survival in patients with OC.
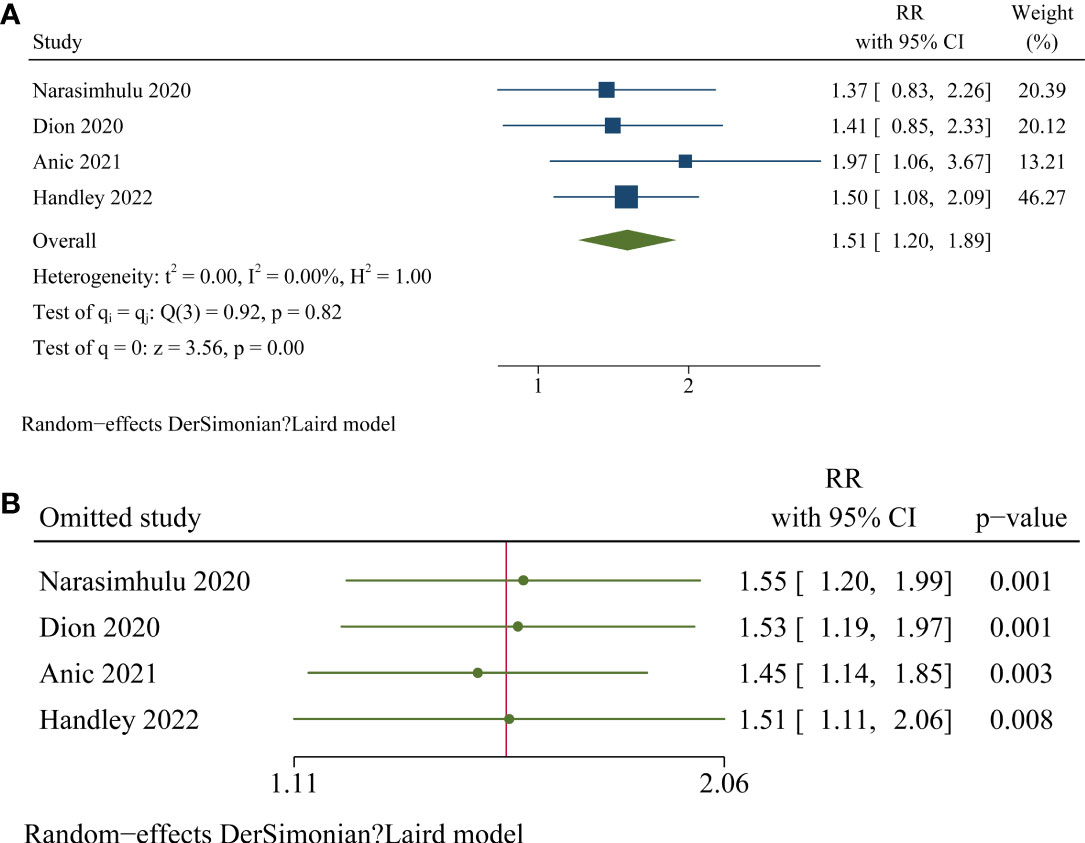
Figure 3 Forest plots for the meta-analyses regarding the association between high frailty and PFS in patients with OC. (A), overall meta-analysis; (B), influencing analysis by omitting one study at a time.
Publication bias
Figure 4 display the funnel plots for the meta-analysis of the association between frailty and OS in patients with OC. Visual inspection revealed symmetry of the plots, reflecting low risks of publication biases. The Egger’s regression tests also showed low risk of publication bias (p = 0.48). The publication bias for the meta-analysis of the association between frailty and PFS was difficult to determine because only four studies were included.
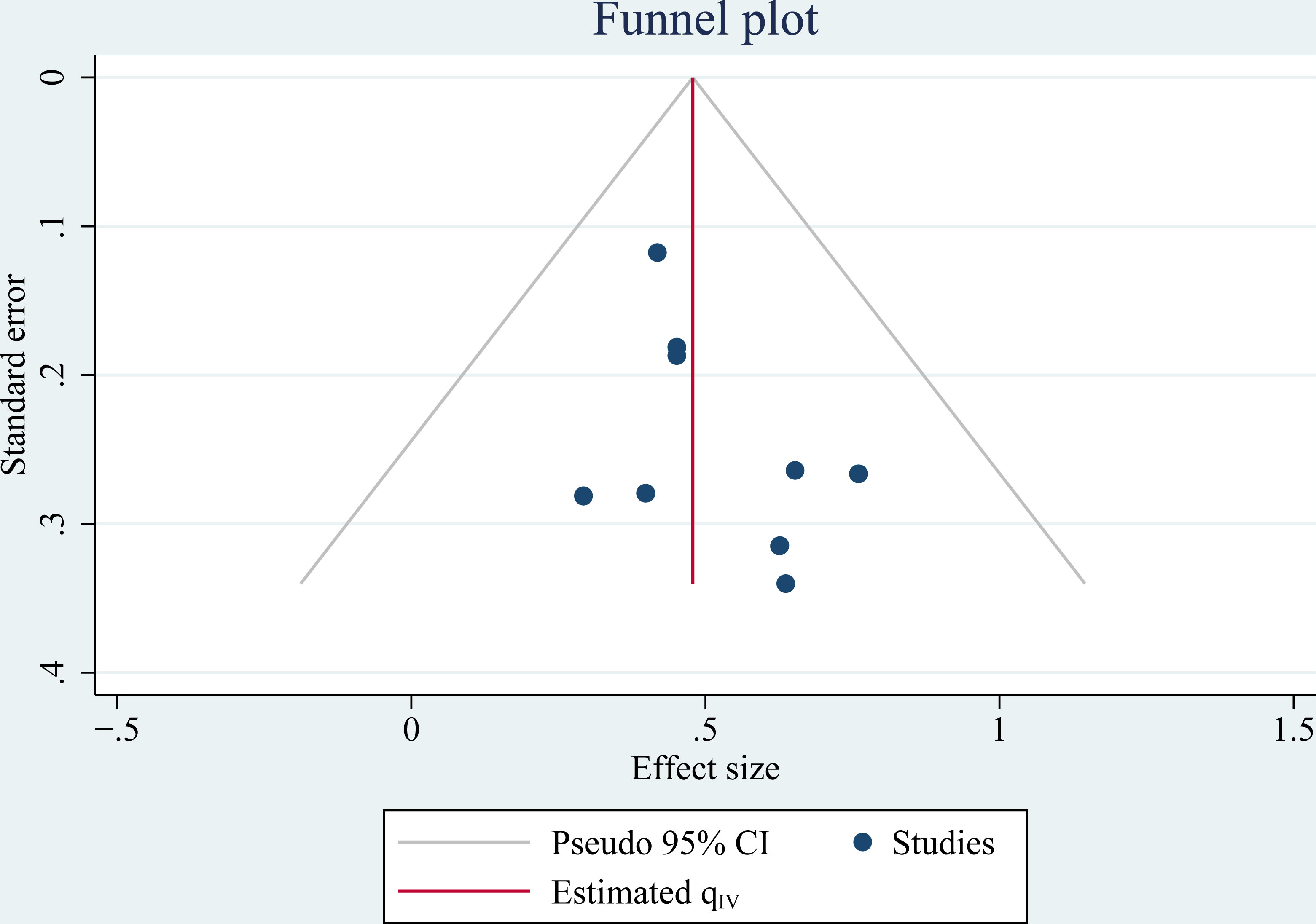
Figure 4 Funnel plots for the publication bias underlying the meta-analysis regarding the association between high frailty and OS in patients with OC.
Evaluation of the evidence
Table 4 provides an overview of the GRADE assessment for the association between frailty and survival of patients with OC. The level of evidence was rated generally low for both the outcomes of OS and PFS.
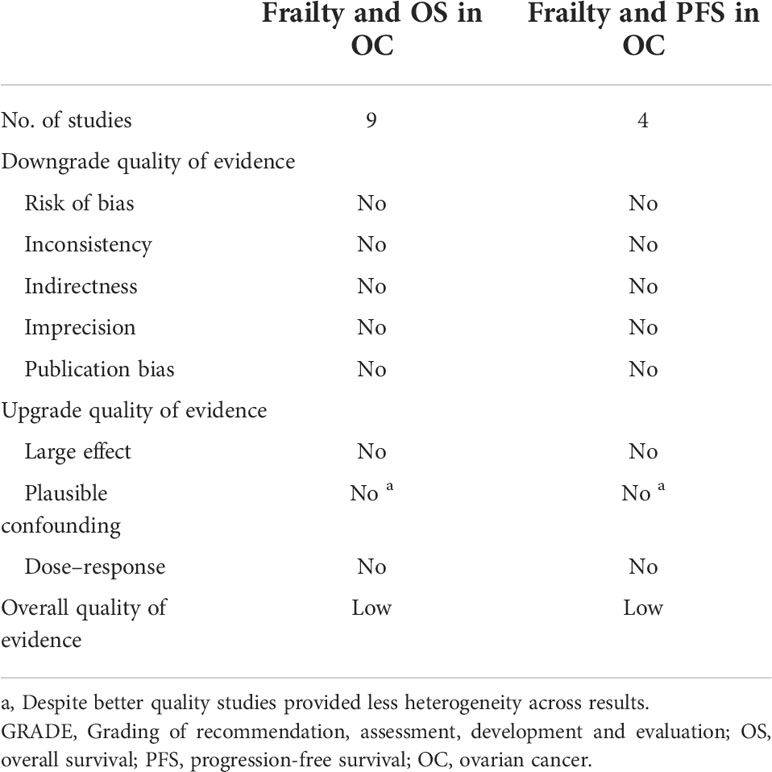
Table 4 Certainty of evidence by GRADE criteria.
Discussion
This systematical review and meta-analysis integrated the findings of nine cohort studies, and the pooled results showed that OC patients with high frailty were associated with poor long-term survival. The results were consistent for outcomes of OS and FPS. Moreover, subsequent sensitivity analyses by omitting one study at a time showed consistent results. In addition, for the meta-analysis of the outcome of OS, subgroup analyses showed that the association between frailty and poor OS in patients with OC was robust and not significantly affected by study characteristics such as study design, cancer stage, patient age, frailty evaluation scale, level of frailty of the controls, follow-up durations, analytic models, and study quality scores. Taken together, these results indicated that frailty may be an important risk factor of the poor long-term survival in patients with OC.
To the best of our knowledge, this is the first systematical review and meta-analysis which evaluated the association between frailty and long-term survival outcomes in patients with OC. The strengths of the meta-analysis included extensive literature searching to incorporate the up-to-date literature evidence, including cohort studies to indicate a longitudinal relationship between frailty and poor survival of patients with OC, and performing multiple sensitivity and subgroup analyses to confirm the robustness of the findings. The findings of the meta-analysis indicated a potential association between high frailty and poor survival of patients with OC. The mechanisms underlying the association may be multifactorial. Biologically, frailty has been associated with chronic inflammation and immunosenescence (37), which has also been involved in the carcinogenesis and invasion of the cancers (38). Besides, people with frailty were at higher risk for sarcopenia (39) and cancer-related cachexia (40), both of which have been related to a poor long-term survival of patients with OC (41). In addition, previous studies have shown that compared to non-frailty patients, OC patients with frailty were more likely to have postoperative morbidity (42, 43) and mortality (44), ICU admission (45), and intolerance for the standard-of-care chemotherapy (46) compared to the none-frailty patients, all of which may lead to poor long-term survival in these patients. Subgroup analyses according to multiple study or patient characteristics showed a consistent association between frailty and poor OS in patients with OC, suggesting a universal role of frailty as a predictor of poor prognosis in OC patients with different ages and cancer stages. Specifically, multiple evaluating scales were used for the evaluation of frailty among the included studies, and the results of subgroup analysis showed a consistent association in different scales. A previous large-scale study in community-dwelling elderly population with different frailty tools showed a similar capacity to detect frailty and a similar prognostic impact (47). Furthermore, the prognostic impact of frailty was also suggested to be similar among the oncologic patients (48). However, further large-scale studies are needed to determine if the prognostic efficacies of different frailty tools are similar in patients with OC.
Results of the meta-analysis also highlighted the significance of geriatric evaluation for frailty in patients with cancer, including those with OC. Besides the importance in prognostic prediction, identification of frailty patients with cancer may be important for the determination of appropriate anticancer modalities in these patients, considering these patients are less tolerable for surgeries and adjuvant therapies and more likely to develop complications and toxicity events. Moreover, geriatric co-management in cancer patients with frailty is also clinical significance, which may increase their tolerability to anticancer treatments and finally improve the clinical outcomes. For example, a previous study showed that in older women with advanced OC and frailty, preoperative/postoperative geriatric and surgical co-management may improve their tolerance to cytoreductive surgery and subsequent postoperative outcomes (49). Similarly, a recent clinical study confirmed that a geriatric assessment and intervention could reduce the serious toxic effects from cancer treatment in older patients with advanced cancer (50). Finally, besides identification of frailty patients with cancer, geriatric evaluation in patients with cancer is also useful to identify the “fit” older cancer patients, who could receive standard anticancer treatment similar to the young patients (51, 52). Collectively, results of the meta-analysis support the incorporating of geriatric evaluation for frailty into the routine management of patients with cancer.
Our study also has limitations. Firstly, as mentioned above, different tools for frailty assessment were used among the included studies, which may contribute to the clinical heterogeneity of the meta-analysis. Besides, the definition of frailty was different even among studies using the same methods. For example, for the three studies using mFI as the evaluating tool for frailty, a high frailty was defined as mFI ≥ 4 (21), a modified Charlson Comorbidity Index [mCCI] score >3 (24), and the adjusted modified frailty index score (amFI) ≥ 2 (29), respectively. Although no statistical heterogeneity was observed and subgroup analyses according to the frailty tools showed consistent results, studies are needed to determine the optimal scales and cutoff values for the determination of cancer patients with high frailty versus low or non-frailty. Moreover, we could not determine if the different histological type of OC may affect the association between frailty and survival because none of the included studies reported the stratified data according to the histological type of the cancer. Studies are warranted in the future to address this issue. Finally, as a meta-analysis based on observational studies, we could not confirm a causative relationship between frailty and poor survival of patients with OC. Clinical studies are needed to determine if intervention targeting frailty in patients with OC could improve the long-term clinical outcomes of these patients.
To sum up, results of this meta-analysis indicate that high frailty may be a risk factor of poor survival in patients with OC. These results highlight the importance of geriatric evaluation for frailty in patients with OC, which may be important for prognostic prediction and determination of the appropriate anticancer treatments for these patients.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
KL and ZL designed the study. KL and RY performed database search, literature review, study quality evaluation, and data collection. KL and ZL performed statistics and interpreted the results. KL drafted the manuscript. ZL critically revised the manuscript. All authors approved the submission of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Xia C, Dong X, Li H, Cao M, Sun D, He S, et al. Cancer statistics in China and united states, 2022: profiles, trends, and determinants. Chin Med J (Engl) (2022) 135(5):584–90. doi: 10.1097/CM9.0000000000002108
2. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin (2022) 72(1):7–33. doi: 10.3322/caac.21708
3. Reid BM, Permuth JB, Sellers TA. Epidemiology of ovarian cancer: a review. Cancer Biol Med (2017) 14(1):9–32. doi: 10.20892/j.issn.2095-3941.2016.0084
4. Lheureux S, Gourley C, Vergote I, Oza AM. Epithelial ovarian cancer. Lancet (2019) 393(10177):1240–53. doi: 10.1016/S0140-6736(18)32552-2
5. Elias KM, Guo J, Bast RC Jr. Early detection of ovarian cancer. Hematol Oncol Clin North Am (2018) 32(6):903–14. doi: 10.1016/j.hoc.2018.07.003
6. Kuroki L, Guntupalli SR. Treatment of epithelial ovarian cancer. BMJ (2020) 371:m3773. doi: 10.1136/bmj.m3773
7. Della Corte L, Foreste V, Di Filippo C, Giampaolino P, Bifulco G. Poly (ADP-ribose) polymerase (PARP) as target for the treatment of epithelial ovarian cancer: what to know. Expert Opin Investig Drugs (2021) 30(5):543–54. doi: 10.1080/13543784.2021.1901882
8. Lheureux S, Braunstein M, Oza AM. Epithelial ovarian cancer: Evolution of management in the era of precision medicine. CA Cancer J Clin (2019) 69(4):280–304. doi: 10.3322/caac.21559
9. Stewart C, Ralyea C, Lockwood S. Ovarian cancer: An integrated review. Semin Oncol Nurs (2019) 35(2):151–6. doi: 10.1016/j.soncn.2019.02.001
10. Slomovitz B, Gourley C, Carey MS, Malpica A, Shih IM, Huntsman D, et al. Low-grade serous ovarian cancer: State of the science. Gynecol Oncol (2020) 156(3):715–25. doi: 10.1016/j.ygyno.2019.12.033
11. Perrone MG, Luisi O, De Grassi A, Ferorelli S, Cormio G, Scilimati A. Translational theragnosis of ovarian cancer: where do we stand? Curr Med Chem (2020) 27(34):5675–715. doi: 10.2174/0929867326666190816232330
12. Minami CA, Cooper Z. The frailty syndrome: A critical issue in geriatric oncology. Crit Care Clin (2021) 37(1):151–74. doi: 10.1016/j.ccc.2020.08.007
13. Huang EY, Lam SC. Review of frailty measurement of older people: Evaluation of the conceptualization, included domains, psychometric properties, and applicability. Aging Med (Milton) (2021) 4(4):272–91. doi: 10.1002/agm2.12177
14. Sobhani A, Fadayevatan R, Sharifi F, Kamrani AA, Ejtahed HS, Hosseini RS, et al. The conceptual and practical definitions of frailty in older adults: a systematic review. J Diabetes Metab Disord (2021) 20(2):1975–2013. doi: 10.1007/s40200-021-00897-x
15. Le Saux O, Falandry C. Toxicity of cancer therapies in older patients. Curr Oncol Rep (2018) 20(8):64. doi: 10.1007/s11912-018-0705-y
16. Crimmin J, Fulop T, Battisti NML. Biological aspects of aging that influence response to anticancer treatments. Curr Opin Support Palliat Care (2021) 15(1):29–38. doi: 10.1097/SPC.0000000000000536
17. Komici K, Bencivenga L, Navani N, D'Agnano V, Guerra G, Bianco A, et al. Frailty in patients with lung cancer: A systematic review and meta-analysis. Chest (2022) 162(2):485–97. doi: 10.1016/j.chest.2022.02.027
18. Liu X, Sun W. Frailty assessment for outcome prediction of patients with prostate cancer receiving radical prostatectomy: A meta-analysis of cohort studies. Clin Nurs Res (2022) 31(6):1136–47. doi: 10.1177/10547738221100350
19. Chen S, Ma T, Cui W, Li T, Liu D, Chen L, et al. Frailty and long-term survival of patients with colorectal cancer: a meta-analysis. Aging Clin Exp Res (2022) 34(7):1485–97. doi: 10.1007/s40520-021-02072-x
20. Ding L, Lu J, Zhu H, Zhu S, Xu X, Hua H, et al. Effects of preoperative frailty on outcomes following surgery among patients with digestive system tumors: A systematic review and meta-analysis. Eur J Surg Oncol (2021) 47(12):3040–8. doi: 10.1016/j.ejso.2021.07.019
21. Ferrero A, Fuso L, Tripodi E, Tana R, Daniele A, Zanfagnin V, et al. Ovarian cancer in elderly patients: Patterns of care and treatment outcomes according to age and modified frailty index. Int J Gynecol Cancer (2017) 27(9):1863–71. doi: 10.1097/IGC.0000000000001097
22. Kumar A, Langstraat CL, DeJong SR, McGree ME, Bakkum-Gamez JN, Weaver AL, et al. Functional not chronologic age: Frailty index predicts outcomes in advanced ovarian cancer. Gynecol Oncol (2017) 147(1):104–9. doi: 10.1016/j.ygyno.2017.07.126
23. Cespedes Feliciano EM, Hohensee C, Rosko AE, Anderson GL, Paskett ED, Zaslavsky O, et al. Association of prediagnostic frailty, change in frailty status, and mortality after cancer diagnosis in the women's health initiative. JAMA Netw Open (2020) 3(9):e2016747. doi: 10.1001/jamanetworkopen.2020.16747
24. Dion L, Mimoun C, Nyangoh Timoh K, Bendifallah S, Bricou A, Collinet P, et al. Ovarian cancer in the elderly: Time to move towards a more logical approach to improve prognosis-a study from the FRANCOGYN group. J Clin Med (2020) 9(5):1339. doi: 10.3390/jcm9051339
25. Narasimhulu DM, McGree ME, Weaver AL, Jatoi A, LeBrasseur NK, Glaser GE, et al. Frailty is a determinant of suboptimal chemotherapy in women with advanced ovarian cancer. Gynecol Oncol (2020) 158(3):646–52. doi: 10.1016/j.ygyno.2020.05.046
26. Anic K, Birkert S, Schmidt MW, Linz VC, Heimes AS, Krajnak S, et al. G-8 geriatric screening tool independently predicts progression-free survival in older ovarian cancer patients irrespective of maximal surgical effort: Results of a retrospective cohort study. Gerontology (2022) 68(10):1101–10. doi: 10.1159/000520328
27. Filippova OT, Tin AL, Alonso J, Vickers AJ, Tew WP, Gardner GJ, et al. Frailty based on the memorial Sloan Kettering frailty index is associated with surgical decision making, clinical trial participation, and overall survival among older women with ovarian cancer. Gynecol Oncol (2021) 161(3):687–92. doi: 10.1016/j.ygyno.2021.03.016
28. Inci MG, Anders L, Woopen H, Richter R, Guzel D, Armbrust R, et al. Frailty index for prediction of surgical outcome in ovarian cancer: Results of a prospective study. Gynecol Oncol (2021) 161(2):396–401. doi: 10.1016/j.ygyno.2021.02.012
29. Handley K, Sood AK, Molin GZD, Westin SN, Meyer LA, Fellman B, et al. Frailty repels the knife: The impact of frailty index on surgical intervention and outcomes. Gynecol Oncol (2022) 166(1):50–6. doi: 10.1016/j.ygyno.2022.05.009
30. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ (2021) 372:n160. doi: 10.1136/bmj.n160
31. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (2021) 372:n71. doi: 10.1136/bmj.n71
32. Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al. Cochrane handbook for systematic reviews of interventions version 6.2. Wiley, London: The Cochrane Collaboration (2021). Available at: www.training.cochrane.org/handbook.
33. Wells GA, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2010). Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
34. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med (2002) 21(11):1539–58. doi: 10.1002/sim.1186
35. Patsopoulos NA, Evangelou E, Ioannidis JP. Sensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. Int J Epidemiol (2008) 37(5):1148–57. doi: 10.1093/ije/dyn065
36. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ (1997) 315(7109):629–34. doi: 10.1136/bmj.315.7109.629
37. Fulop T, McElhaney J, Pawelec G, Cohen AA, Morais JA, Dupuis G, et al. Frailty, inflammation and immunosenescence. Interdiscip Top Gerontol Geriatr (2015) 41:26–40. doi: 10.1159/000381134
38. Zhang X, Meng X, Chen Y, Leng SX, Zhang H. The biology of aging and cancer: Frailty, inflammation, and immunity. Cancer J (2017) 23(4):201–5. doi: 10.1097/PPO.0000000000000270
39. Cruz-Jentoft AJ, Kiesswetter E, Drey M, Sieber CC. Nutrition, frailty, and sarcopenia. Aging Clin Exp Res (2017) 29(1):43–8. doi: 10.1007/s40520-016-0709-0
40. Zhang X, Edwards BJ. Malnutrition in older adults with cancer. Curr Oncol Rep (2019) 21(9):80. doi: 10.1007/s11912-019-0829-8
41. Ubachs J, Ziemons J, Minis-Rutten IJG, Kruitwagen R, Kleijnen J, Lambrechts S, et al. Sarcopenia and ovarian cancer survival: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle (2019) 10(6):1165–74. doi: 10.1002/jcsm.12468
42. Chambers LM, Chalif J, Yao M, Chichura A, Morton M, Gruner M, et al. Modified frailty index predicts postoperative complications in women with gynecologic cancer undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Gynecol Oncol (2021) 162(2):368–74. doi: 10.1016/j.ygyno.2021.05.013
43. Di Donato V, Di Pinto A, Giannini A, Caruso G, D'Oria O, Tomao F, et al. Modified fragility index and surgical complexity score are able to predict postoperative morbidity and mortality after cytoreductive surgery for advanced ovarian cancer. Gynecol Oncol (2021) 161(1):4–10. doi: 10.1016/j.ygyno.2020.08.022
44. Sia TY, Wen T, Cham S, Friedman AM, Wright JD. Effect of frailty on postoperative readmissions and cost of care for ovarian cancer. Gynecol Oncol (2020) 159(2):426–33. doi: 10.1016/j.ygyno.2020.08.024
45. Yao T, DeJong SR, McGree ME, Weaver AL, Cliby WA, Kumar A. Frailty in ovarian cancer identified the need for increased postoperative care requirements following cytoreductive surgery. Gynecol Oncol (2019) 153(1):68–73. doi: 10.1016/j.ygyno.2018.12.025
46. Hay CM, Donovan HS, Campbell GB, Taylor SE, Wang L, Courtney-Brooks M. Chemotherapy in older adult gynecologic oncology patients: Can a phenotypic frailty score predict tolerance? Gynecol Oncol (2019) 152(2):304–9. doi: 10.1016/j.ygyno.2018.11.031
47. Woo J, Leung J, Morley JE. Comparison of frailty indicators based on clinical phenotype and the multiple deficit approach in predicting mortality and physical limitation. J Am Geriatr Soc (2012) 60(8):1478–86. doi: 10.1111/j.1532-5415.2012.04074.x
48. Markar SR, Karthikesalingam A, Low DE. Outcomes assessment of the surgical management of esophageal cancer in younger and older patients. Ann Thorac Surg (2012) 94(5):1652–8. doi: 10.1016/j.athoracsur.2012.06.067
49. Filippova OT, Chi DS, Long Roche K, Sonoda Y, Zivanovic O, Gardner GJ, et al. Geriatric co-management leads to safely performed cytoreductive surgery in older women with advanced stage ovarian cancer treated at a tertiary care cancer center. Gynecol Oncol (2019) 154(1):77–82. doi: 10.1016/j.ygyno.2019.04.683
50. Mohile SG, Mohamed MR, Xu H, Culakova E, Loh KP, Magnuson A, et al. Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): a cluster-randomised study. Lancet (2021) 398(10314):1894–904. doi: 10.1016/S0140-6736(21)01789-X
51. Montroni I, Rostoft S, Spinelli A, Van Leeuwen BL, Ercolani G, Saur NM, et al. GOSAFE - geriatric oncology surgical assessment and functional rEcovery after surgery: early analysis on 977 patients. J Geriatr Oncol (2020) 11(2):244–55. doi: 10.1016/j.jgo.2019.06.017
Keywords: frailty, ovarian cancer, survival, meta-analysis, geriatric assessment
Citation: Li K, Yin R and Li Z (2022) Frailty and long-term survival of patients with ovarian cancer: A systematic review and meta-analysis. Front. Oncol. 12:1007834. doi: 10.3389/fonc.2022.1007834
Received: 31 July 2022; Accepted: 20 September 2022;
Published: 17 October 2022.
Edited by:
Giuseppe Vizzielli, University of Udine, ItalyReviewed by:
Yu Gu, Peking Union Medical College Hospital (CAMS), ChinaLuigi Della Corte, University of Naples Federico II, Italy
Copyright © 2022 Li, Yin and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhengyu Li, emhlbmd5dWxpXzI4NUAxNjMuY29t