
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 11 February 2022
Sec. Breast Cancer
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.827625
 Alberto Ocaña1,2,3*
Alberto Ocaña1,2,3* Jose Ignacio Chacón3,4Lourdes Calvo3,5Antonio Antón3,6Mauro Mansutti7Joan Albanell2,3,8,9María Teresa Martínez2,3,10Ainhara Lahuerta3,11Giancarlo Bisagni12
Jose Ignacio Chacón3,4Lourdes Calvo3,5Antonio Antón3,6Mauro Mansutti7Joan Albanell2,3,8,9María Teresa Martínez2,3,10Ainhara Lahuerta3,11Giancarlo Bisagni12 Begoña Bermejo2,3,10Vladimir Semiglazov13Marc Thill14Arlene Chan15
Begoña Bermejo2,3,10Vladimir Semiglazov13Marc Thill14Arlene Chan15 Serafin Morales3,16Jesús Herranz3Ignacio Tusquets2,3,9Massimo Chiesa3Rosalía Caballero3Pinuccia Valagussa17Giampaolo Bianchini17
Serafin Morales3,16Jesús Herranz3Ignacio Tusquets2,3,9Massimo Chiesa3Rosalía Caballero3Pinuccia Valagussa17Giampaolo Bianchini17 Emilio Alba2,3,18†
Emilio Alba2,3,18† Luca Gianni17†
Luca Gianni17†Background: Derived neutrophil-to-lymphocyte ratio (dNLR) is a biomarker associated with clinical outcome in breast cancer (BC). We analyzed the association of dNLR with pathological complete response (pCR) in triple-negative BC (TNBC) patients receiving neoadjuvant chemotherapy (CT).
Methods: This is a retrospective analysis of two randomized studies involving early stage/locally advanced TNBC patients receiving anthracycline/taxane-based CT+/−carboplatin (GEICAM/2006-03) or nab-paclitaxel/paclitaxel followed by anthracycline regimen (ETNA). dNLR was calculated as the ratio of neutrophils to the difference between total leukocytes and neutrophils in peripheral blood before CT (baseline) and at the end of treatment (EOT). Logistic regression analyses were used to explore dNLR association with pCR.
Results: In total, 308 TNBC patients were analyzed, 216 from ETNA and 92 from GEICAM/2006-03. Baseline median dNLR was 1.61 (interquartile range (IQR): 1.25–2.04) and at EOT 1.53 (IQR: 0.96–2.22). Baseline dNLR showed positive correlation with increased tumor size (p-value = 1e−04). High baseline dNLR, as continuous variable or using median cutoff, was associated with lower likelihood of pCR in univariate analysis. High EOT dNLR as continuous variable or using quartiles was also associated with lower pCR rate in uni- and multivariate analyses.
Conclusions: High baseline and EOT dNLR correlates with lower benefit from neoadjuvant CT in TNBC.
Neoadjuvant chemotherapy is a widely used therapeutic option for the treatment of early-stage or locally advanced breast cancer (1). This is particularly evident for the treatment of HER2-positive breast cancer or the triple-negative breast cancer (TNBC) subtypes in which pathological complete response (pCR) has been shown to be associated with improved clinical outcome (2–5). Further, patients with TNBC or HER2 positive tumors that do not achieve a pCR can be offered additional adjuvant treatment including TDM1 or chemotherapy, respectively, which has demonstrated an improvement in survival (5, 6). For TNBC, although not all clinical studies have confirmed this benefit, residual invasive disease following neoadjuvant chemotherapy is indicative of high risk of relapse and additional adjuvant treatment with capecitabine can contribute to the reduction of this risk (7, 8). Unfortunately, the benefit of neoadjuvant chemotherapy in other subtypes of breast cancer, particularly in the luminal group, is less clear and is restricted to locally advanced cases.
Inflammation as a consequence of the immune response to the tumor is a hallmark of cancer (9). In addition, the presence of an immunogenic activated environment identifies tumors that have a better prognosis and predicts for response to immune checkpoint inhibitors (ICIs) (10, 11). TNBC demonstrates heightened immunogenic activation, but data with ICIs in the advanced disease have demonstrated disappointing results, with only one study showing an increase in overall survival when the population was selected by PD-L1 expression (12). In one study, pembrolizumab in combination with chemotherapy in the neoadjuvant setting slightly reached the prespecified pathological complete response threshold to consider the experimental arm as being beneficial (13) The ability to identify biomarkers that can help to select patients whose tumors are most likely to respond to ICIs in combination with chemotherapy would be clinically important. Although it is known that immunologic transcriptomic signatures can identify immune-active tumors that can better respond to chemotherapy (14), the evaluation of biomarkers which can be more easily implemented is a clinical necessity.
The derived neutrophil-to-lymphocyte ratio (dNLR) is calculated as the ratio of neutrophils to the difference between total leukocytes and neutrophils in peripheral blood (15). Its role to discriminate prognosis has been widely explored and in some indications has already been incorporated in clinical guidelines (e.g., prostate cancer).
It is clear that the use of liquid biopsy to study genomic correlates of the tumor or to indirectly evaluate biomarkers of immune response has gained momentum, demonstrating its utility in different clinical scenarios (16).
Our group and others have explored the role of dNLR in early-stage breast cancer demonstrating its prognostic value (17–19). The role of dNLR in the neoadjuvant setting to predict response to chemotherapy has not been established.
To this end, we evaluated two randomized studies (GEICAM/2006-03-NCT00432172 and ETNA-NCT01822314) which investigated neoadjuvant chemotherapy in operable early stage (>2 cm; node positive) or locally advanced tumors to explore the capability of dNLR to predict response in the TNBC subgroup.
Data from patients who participated in the randomized phase 2 GEICAM/2006-03 (NCT00432172) and phase 3 ETNA (NCT01822314) trials were analyzed retrospectively. Details and main results of the studies were published elsewhere (20–22). Briefly, in the GEICAM/2006-03 trial, HER2-negative patients were selectively treated according to clinical subtypes: triple-negative (TN) patients received standard taxane/anthracycline-based chemotherapy (TA-CT) +/− carboplatin, while luminal patients were randomized to TA-CT vs. hormone therapy (only patients (pts) that received TA-CT +/− carboplatin were considered for this analysis). In the ETNA trial, HER2-negative pts were treated with nab-paclitaxel or paclitaxel followed by anthracyclines. In both studies, pCR in breast and axilla was used to measure treatment response according to Miller&Payne criteria. Analysis of ER, PgR, and HER2 status was carried out in a central laboratory in the two studies. TN subgroup was defined as estrogen receptor (ER) negative, progesterone receptor (PgR) negative, and HER2.
dNLR was calculated from analytical values of peripheral blood collected either before the start of chemotherapy (baseline) or at the end of treatment (EOT). dNLR was calculated as the ratio of the absolute neutrophil number to the difference between absolute total leukocyte and absolute neutrophil counts, a proxy for lymphocyte count (22). Patients without information on neutrophils and leukocytes and patients with leukocyte counts >15 × 109/L were excluded, as this might reflect infectious or hematologic conditions unrelated to breast cancer.
Univariate and multivariate logistic regression analyses were used to explore the association of dNLR with main clinical characteristics and dNLR capability (distributed as a continuous variable, using median cutoff and quartiles) to predict pCR. Multivariate models were adjusted for important clinical variables (treatment, tumor size, lymph nodes, grade, Ki67) and for clinical variables significantly associated (p-value <0.1) with pCR (age, histological type). An optimal cutoff model based on Youden Index was also used to analyze the association of basal dNLR with pCR.
A total of 308 patients with TNBC were included in the analysis, 216 from the ETNA and 92 from the GEICAM/2006-03 study. Both trials evaluated neoadjuvant chemotherapy in early stage (tumor >2 cm and/or node positive) or locally advanced triple-negative and luminal breast cancers. Median age of the analyzed patients was 51 years. Most patients had cT2 disease (n = 227, 73.7%)and cN1 (n = 153, 49.7%) followed by cN0 (n = 133, 43.2%). pCR was achieved in 36.7% (n = 113) of the treated patients. All patients’ characteristics, according to response to chemotherapy (pCR = No/Yes) are described in Table 1.
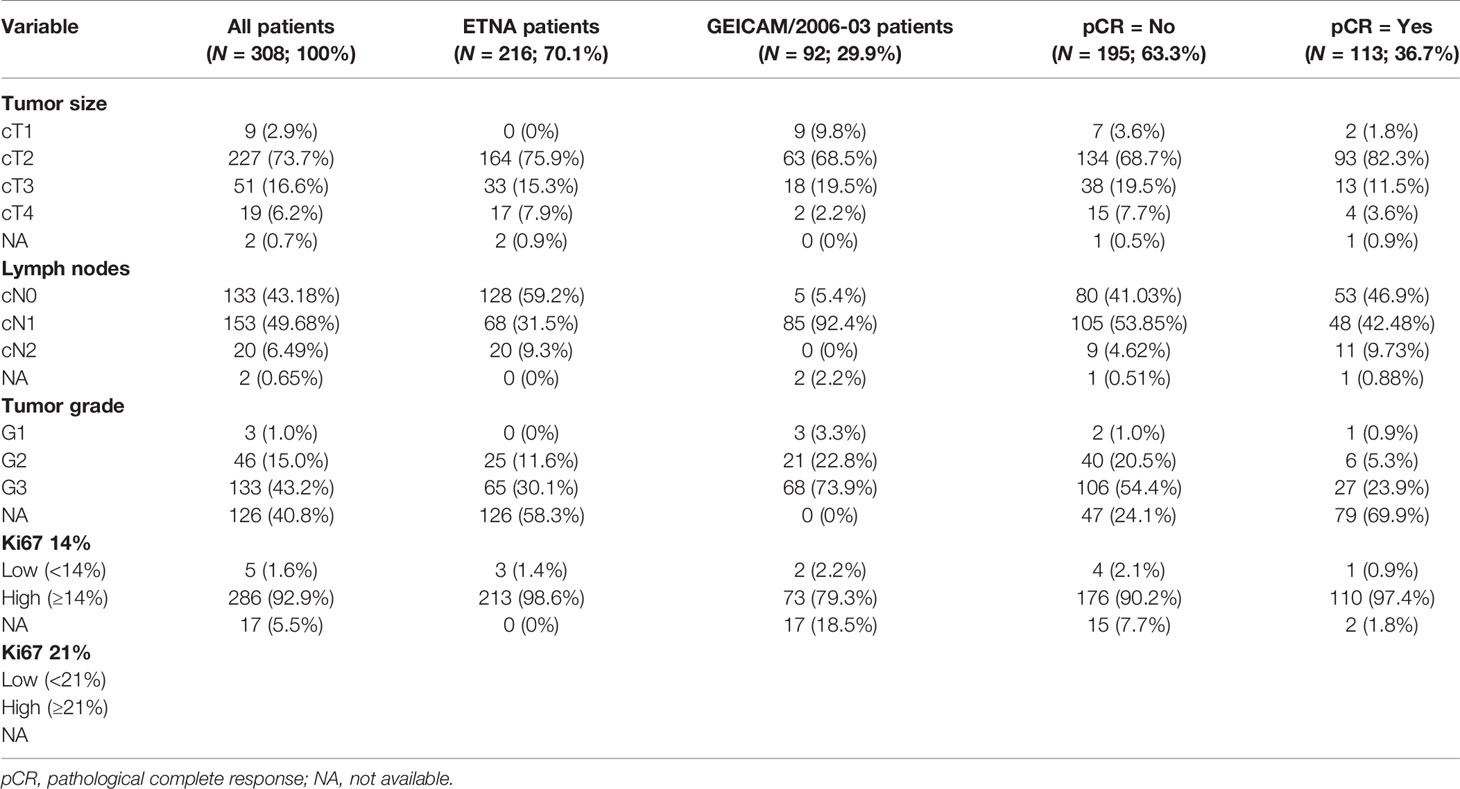
Table 1 Main clinical-pathological patients’ characteristics.
Median baseline dNLR was 1.61 (IQR: 1.25–2.04), and at the EOT 1.53 (IQR: 0.96–2.22) (Figure 1) (Table 2).

Figure 1 dNLR median values before CT (Baseline) and at EOT. dNLR, derived neutrophil-to-lymphocyte ratio; CT, chemotherapy; EOT, end of treatment.
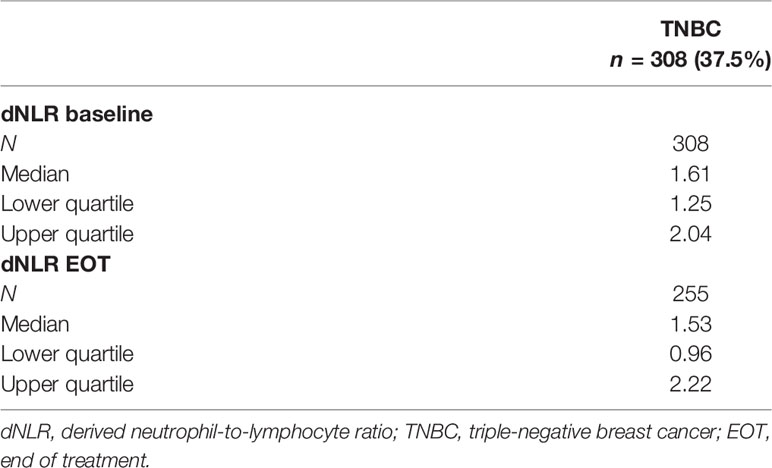
Table 2 dNLR expression in the patients’ population.
Analysis of the association of baseline dNLR with the main clinical features (tumor size, lymph nodes, tumor grade, Ki67) demonstrated a significant correlation only with tumor size (p-value = 1e−04) (Table 3). No significant associations were found between EOT dNLR and clinical features (Table 3).
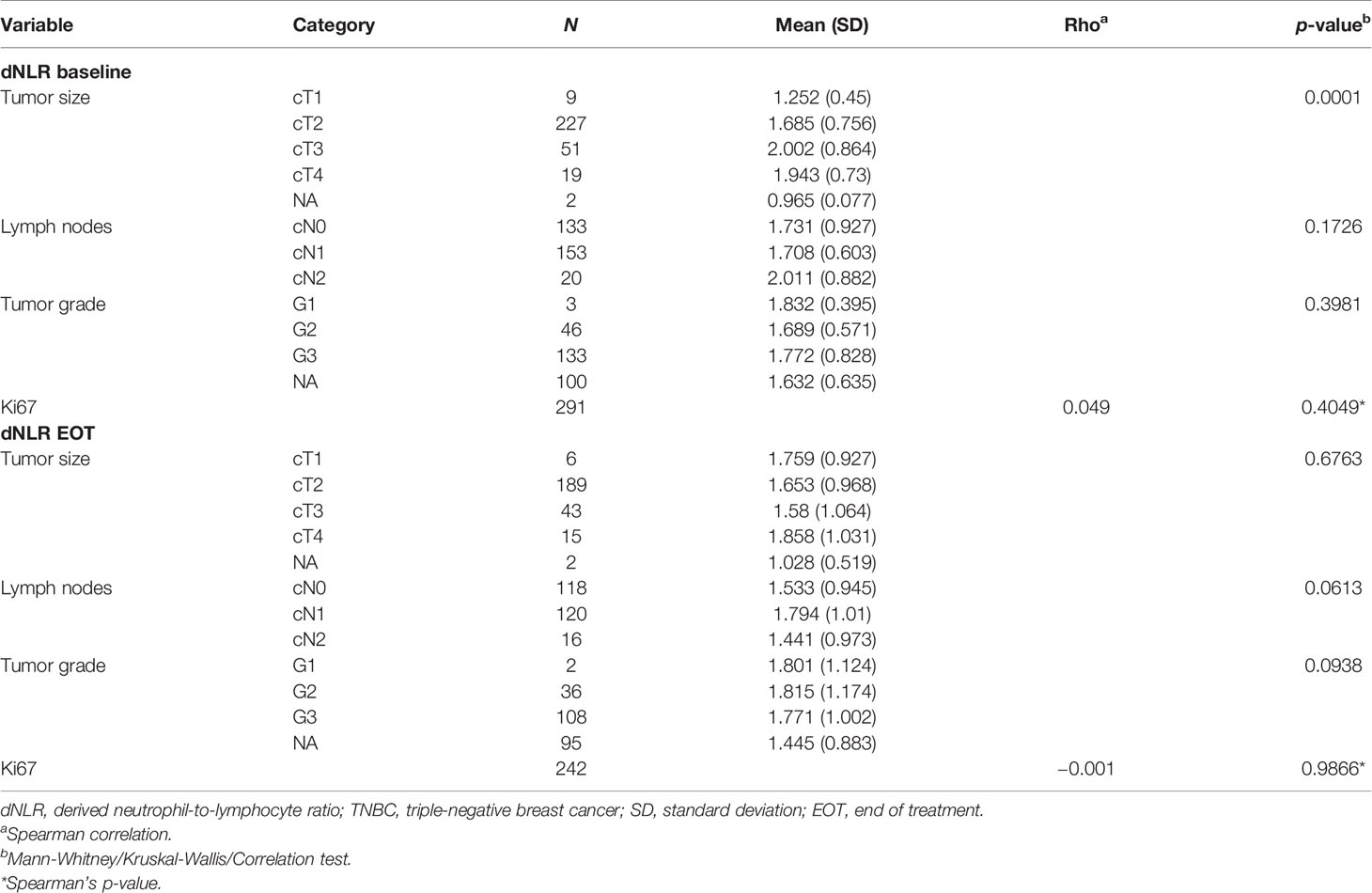
Table 3 Association of dNLR with clinical and pathological parameters in TNBC.
No association was observed between baseline dNLR and EOT dNLR (correlation coefficient: 0.138).
In the univariate analysis, high baseline dNLR level, considered continuous and categorical variable defined by the median cutoff, was associated with a lower likelihood of pCR (OR: 0.709; 95% CI: 0.5–1.006, p-value = 0.0406 and OR: 0.59; 95% CI: 0.37–0.94, p-value = 0.0244, respectively). The association between baseline dNLR quartiles and pCR was only marginally significant (p-value = 0.0706). The association did not retain significance in multivariate analysis after correction for clinical variables (Table 4).
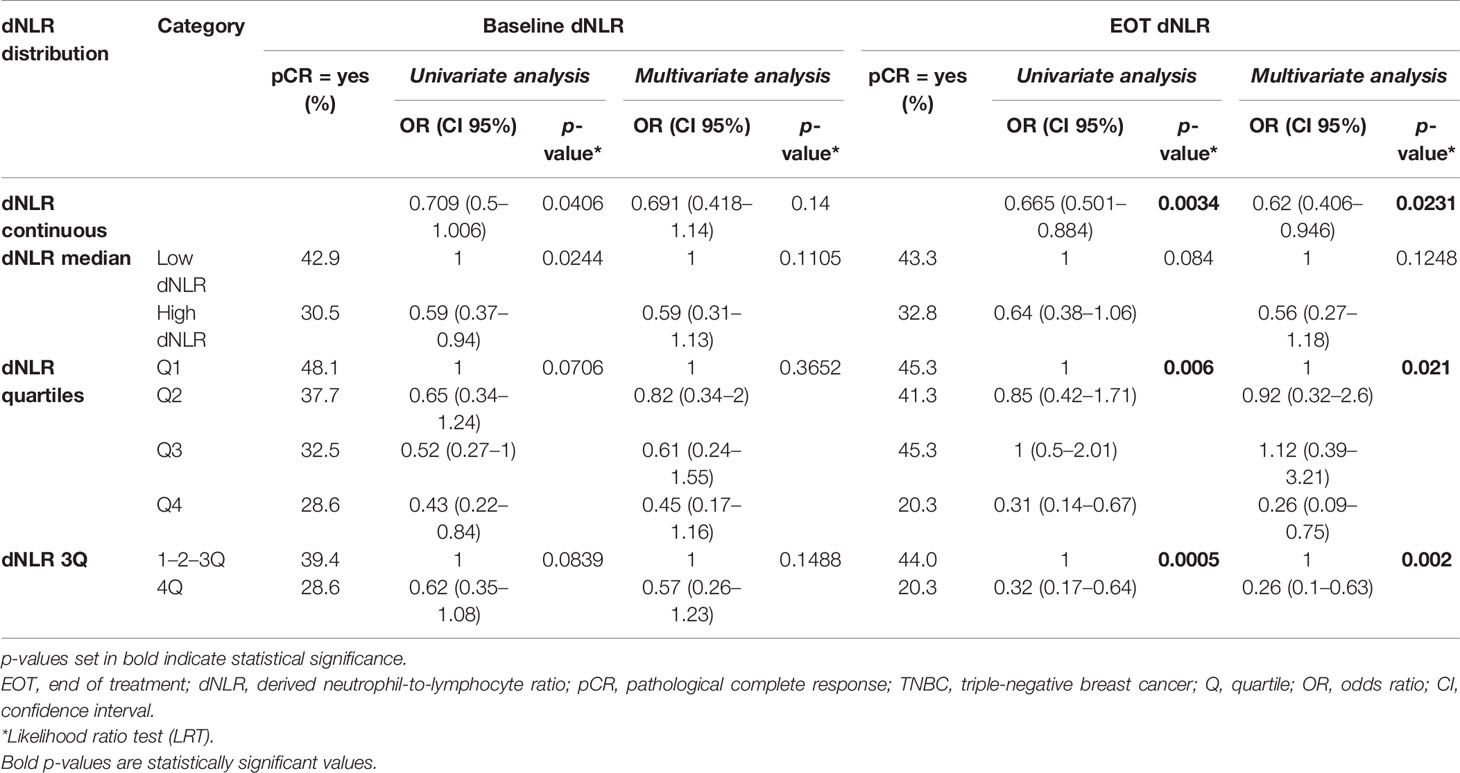
Table 4 Association of baseline and EOT dNLR with pCR in TNBC patients’ population.
High EOT dNLR levels considered a continuous variable was associated with lower likelihood of achieving a pCR, in both univariate (OR: 0.665; 95% CI: 0.501–0.884; p-value = 0.0034) and multivariate (OR: 0.62; 95% CI: 0.406–0.946; p-value = 0.0231) logistic regression analysis. High EOT dNLR defined by the median cutoff demonstrated only a trend for association with lower pCR (OR: 0.64; 95% CI: 0.38–1.06; p-value = 0.084). When EOT dNLR was assessed by quartiles, a significant association between higher dNLR and lower rate of pCR was described in both uni- and multivariate analyses (p-value = 0.006 and 0.021, respectively). This association was driven by the highest quartile as demonstrated by the comparison with the combined lower quartiles (OR: 0.32; 95% CI: 0.17–0.64; p-value = 5e−04 and OR: 0.26; 95% CI: 0.1–0.63; p-value = 0.002, respectively).
An exploratory assessment of dNLR to define the optimal predictive cutoff points was performed: baseline cutoff = 1.715 (OR: 0.65; 95% CI: 0.51–0.82; p-value = 0.035) and EOT dNLR cutoff = 2.231 (OR: 0.43; 95% CI: 0.25–0.74; p-value = 0.0035) (Table 5).

Table 5 Association of baseline and EOT dNLR with pCR in TNBC patients’ population—cutpoint model.
Supplementary Tables S1–S3 describe the variables included in the multivariate logistic regression analysis.
We described a new biomarker related to inflammation and immune response which is associated with a lower likelihood to achieve pCR in patients with TNBC treated with chemotherapy in these two prospective randomized trials. Identification of patients who derive the greatest benefit from chemotherapy is useful to optimize treatment tailoring and therefore the discovery of novel predictive biomarkers that could be easily implemented in the clinic is warranted.
Achieving a pCR has been associated with better clinical outcome particularly for the triple-negative and HER2-positve subtypes (23).
TNBC is the more immune-activated breast cancer subtype, and incorporation of immune checkpoint inhibitors in combination with chemotherapy in high-risk TNBC appears promising and will likely become the new standard of care (24, 25). However, the current unmet need is the precise identification of patients who will most likely benefit from the addition of immune checkpoint therapy to the standard of care.
In the case of TNBC, predictive biomarkers of response to neoadjuvant chemotherapy have been demonstrated both in terms of tumor-infiltrating lymphocytes and transcriptomic signatures (26–28). In our study, dNLR appeared to be another promising easily assessable and reliable biomarker that could be incorporated into the clinical practice and might help to identify those patients with lower benefit from chemotherapy and who might benefit the most from additional treatments.
How chemotherapy can affect inflammation in TN subtype is unclear, but some studies have suggested that it could modulate immune populations therefore influencing treatment efficacy (29). Conversely, systemic inflammation could be associated with different local immune milieu such as the amount of tumor-infiltrating lymphocytes, which are known to influence prognosis and response to chemotherapy.
In this study, no association between dNLR and clinicopathological parameters was observed with the exception of larger tumor size which was associated with high dNLR. To this regard, the association with size can just confirm the more aggressive phenotype recognized by the presence of dNLR.
EOT dNLR as a continuous variable and by quartile distribution was associated with a reduce rate of pCR in TNBC in univariate and multivariate analyses. This finding suggests that administration of chemotherapy may affect the immune system within the tumor, inducing inflammation that somehow could limit the efficacy of the chemotherapy (29). Alternatively, it is known that chemotherapy can stimulate an immunologic cell death, which depends on the tumor type and the specific genomic and stromal microenvironment and could favor the efficacy of chemotherapy (30).
Assessment of dNLR in TNBC using the optimal cutoff showed a negative association with pCR in the Cox regression model at baseline and at the EOT dNLR. This suggests that high baseline dNLR may also be informative as to which patients are less likely to benefit from chemotherapy. Assessment of this biomarker before treatment can be implemented easily, thus potentially allowing its incorporation into management decisions. In this context, integration of liquid biopsy to help the management of our patients is gaining momentum, and the reported analysis here is an example of one of those applications.
We recognize that there are limitations in our analysis. Firstly, this is a retrospective analysis which would need to be confirmed ideally in a prospective clinical trial. Secondly, it is unclear if the observed association of dNLR levels and lower likelihood to response to chemotherapy would be influenced when ICIs are used together with chemotherapy. In this regard, the analysis of dNLR in patients treated with ICIs in combination with chemotherapy in the neoadjuvant setting warrants investigation, as it might identify a subgroup of patients who derive less benefit also from ICIs.
High levels of dNLR correlate with lower likelihood to benefit from chemotherapy in TN tumors receiving neoadjuvant chemotherapy. This finding warrants confirmation in larger retrospective or prospective cohort of patients and in the context of inclusion of ICIs use in the neoadjuvant setting.
Our results suggest that high dNLR levels at baseline and especially at EOT are associated with lower likelihood of achieving a pCR in patients with TNBC treated with neoadjuvant chemotherapy. The reported data should be considered exploratory, and the evaluation in an additional dataset will be necessary to confirm these results. Similarly, future studies should evaluate the role of dNLR to predict response of ICIs in combination with chemotherapy.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Institut Municipal d’Assistencia Sanitaria (IMAS), Paseo Marítimo 25-29, 08003 Barcelona, Parc de Salut Mar, Dr. Aiguader 88, 08003 Barcelona. The patients/participants provided their written informed consent to participate in this study.
Conceptualization: AO, EA, and LG. Methodology: AO and JH. Software: JH, MC, and RC. Validation and formal analysis: JH. Investigation and data curation: AO, JC, LC, AA, MM, MTM, JA, AL, GBis, BB, VS, MT, AC, SM, IT, PV, GBia, EA, and LG. Resources: AO, JC, LC, AA, MM, MTM, JA, AL, GBis, BB, VS, MT, AC, SM, IT, PV, GBia, EA, LG, MC, and RC. Writing—original draft preparation: AO, GBia, EA, MC, and RC. Writing—review and editing and visualization: all authors. Supervision: AO, MC, and RC. Project administration: MC and RC. Funding acquisition: AO.
This analysis was supported by GEICAM Spanish Breast Cancer Group.
AO is currently an employee of Symphogen, Denmark. MM has received honoraria from Pierre Fabre and support for attending meetings and/or travel from Eisai, Novartis, Pfizer, Pierre Fabre, and Roche. He has received advisory board honoraria from Amgen, Astra Zeneca, Eli Lilly, Gentili, MSD Italia, Novartis, Pfizer, and Roche. JA has received advisory board honoraria from Roche, Lilly, Merck, Daiichi-Sankyo/Astrazeneca, and Seagen and a speaker’s honoraria from Pfizer. GBia has received honoraria from Pfizer, Roche, AstraZeneca, Lilly, Novartis, Noepharm Israel, Amgen, MSD, Chugai, Sanofi, Daiichi Sankyo, Eisai, Gilead, Seagen, and Exact Science. EA has received advisory board honoraria from Roche, Novartis, Pfizer, Lilly, BMS, Genomic Health, and Nanostring and support for attending meetings and/or travel from Celgene, as well as investigation grants from Roche, Pfizer, Sysmex, MSD, and Nanostring. LG has received advisory board honoraria from ADC Therapeutics, AstraZeneca, Celgene, Eli Lilly, G1 Therapeutics, Genentech, Genomic Health, Merck Sharp & Dohme, Oncolytics Biotech, Odonate Therapeutics, Onkaido Therapeutics, Roche, Pfizer, Taiho Pharmaceutical, Hexal Sandoz, Seattle Genetics, Synthon, Zymeworks, and Sanofi-Aventis; consultant honoraria for selected programs of Forty Seven (CD47), GENENTA, METIS Precision Medicine, Novartis, Odonate Therapeutics, Revolution Medicines, Synaffix, Zymeworks, Menarini Ricerche, Amgen, and Biomedical Insights; and research support from Zymeworks, Revolution Medicines (his institution). LG is coinventor of “European Patent Application N.12195182.6 and 12196177.5,” titled “PDL-1 expression in anti-HER2 therapy”—Roche (no compensation provided).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We acknowledge the investigators, pathology departments, other staff of the participant sites, the patients, and the GEICAM staff involved in this trial.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.827625/full#supplementary-material
1. Pusztai L, Foldi J, Dhawan A, DiGiovanna MP, Mamounas EP. Changing Frameworks in Treatment Sequencing of Triple-Negative and HER2-Positive, Early-Stage Breast Cancers. Lancet Oncol (2019) 20(7):e390–e6. doi: 10.1016/S1470-2045(19)30158-5
2. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological Complete Response and Long-Term Clinical Benefit in Breast Cancer: The CTNeoBC Pooled Analysis. Lancet (2014) 384(9938):164–72. doi: 10.1016/S0140-6736(13)62422-8
3. Liedtke C, Mazouni C, Hess KR, Andre F, Tordai A, Mejia JA, et al. Response to Neoadjuvant Therapy and Long-Term Survival in Patients With Triple-Negative Breast Cancer. J Clin Oncol (2008) 26(8):1275–81. doi: 10.1200/JCO.2007.14.4147
4. von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA, et al. Definition and Impact of Pathologic Complete Response on Prognosis After Neoadjuvant Chemotherapy in Various Intrinsic Breast Cancer Subtypes. J Clin Oncol (2012) 30(15):1796–804. doi: 10.1200/JCO.2011.38.8595
5. von Minckwitz G, Huang CS, Mano MS, Loibl S, Mamounas EP, Untch M, et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N Engl J Med (2019) 380(7):617–28. doi: 10.1056/NEJMoa1814017
6. Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES, Yokota I, et al. Adjuvant Capecitabine for Breast Cancer After Preoperative Chemotherapy. N Engl J Med (2017) 376(22):2147–59. doi: 10.1056/NEJMoa1612645
7. Lluch A, Barrios CH, Torrecillas L, Ruiz-Borrego M, Bines J, Segalla J, et al. Phase III Trial of Adjuvant Capecitabine After Standard Neo-/Adjuvant Chemotherapy in Patients With Early Triple-Negative Breast Cancer (GEICAM/2003-11_CIBOMA/2004-01). J Clin Oncol (2020) 38(3):203–13. doi: 10.1200/JCO.19.00904
8. Wang X, Wang SS, Huang H, Cai L, Zhao L, Peng RJ, et al. Effect of Capecitabine Maintenance Therapy Using Lower Dosage and Higher Frequency vs Observation on Disease-Free Survival Among Patients With Early-Stage Triple-Negative Breast Cancer Who Had Received Standard Treatment: The SYSUCC-001 Randomized Clinical Trial. Jama (2021) 325(1):50–8. doi: 10.1001/jama.2020.23370
9. Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell (2011) 144(5):646–74. doi: 10.1016/j.cell.2011.02.013
10. Keenan TE, Burke KP, Van Allen EM. Genomic Correlates of Response to Immune Checkpoint Blockade. Nat Med (2019) 25(3):389–402. doi: 10.1038/s41591-019-0382-x
11. Ribas A, Wolchok JD. Cancer Immunotherapy Using Checkpoint Blockade. Science (2018) 359(6382):1350–5. doi: 10.1126/science.aar4060
12. Schmid P, Adams S, Rugo HS, Schneeweiss A, Barrios CH, Iwata H, et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N Engl J Med (2018) 379(22):2108–21. doi: 10.1056/NEJMoa1809615
13. Schmid P, Dent R, O’Shaughnessy J. Pembrolizumab for Early Triple-Negative Breast Cancer. Reply N Engl J Med (2020) 382(26):e108. doi: 10.1056/NEJMoa1910549
14. Pérez-Pena J, Tibor Fekete J, Páez R, Baliu-Piqué M, García-Saenz J, García-Barberán V, et al. A Transcriptomic Immunologic Signature Predicts Favorable Outcome in Neoadjuvant Chemotherapy Treated Triple Negative Breast Tumors. Front Immunol (2019) 10:2802. doi: 10.3389/fimmu.2019.02802
15. Templeton AJ, McNamara MG, Seruga B, Vera-Badillo FE, Aneja P, Ocana A, et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Solid Tumors: A Systematic Review and Meta-Analysis. J Natl Cancer Inst (2014) 106(6):dju124. doi: 10.1093/jnci/dju124
16. Ignatiadis M, Sledge GW, Jeffrey SS. Liquid Biopsy Enters the Clinic - Implementation Issues and Future Challenges. Nat Rev Clin Oncol (2021) 18(5):297–312. doi: 10.1038/s41571-020-00457-x
17. Templeton AJ, Rodríguez-Lescure Á, Ruíz A, Alba E, Calvo L, Ruíz-Borrego M, et al. Prognostic Role for the Derived Neutrophil-to-Lymphocyte Ratio in Early Breast Cancer: A GEICAM/9906 Substudy. Clin Trans Oncol (2018) 20(12):1548–56. doi: 10.1007/s12094-018-1885-5
18. Dirican A, Kucukzeybek BB, Alacacioglu A, Kucukzeybek Y, Erten C, Varol U, et al. Do the Derived Neutrophil to Lymphocyte Ratio and the Neutrophil to Lymphocyte Ratio Predict Prognosis in Breast Cancer? Int J Clin Oncol (2015) 20(1):70–81. doi: 10.1007/s10147-014-0672-8
19. Krenn-Pilko S, Langsenlehner U, Stojakovic T, Pichler M, Gerger A, Kapp KS, et al. The Elevated Preoperative Derived Neutrophil-to-Lymphocyte Ratio Predicts Poor Clinical Outcome in Breast Cancer Patients. Tumor Biol (2016) 37(1):361–8. doi: 10.1007/s13277-015-3805-4
20. Alba E, Chacon JI, Lluch A, Anton A, Estevez L, Cirauqui B, et al. A Randomized Phase II Trial of Platinum Salts in Basal-Like Breast Cancer Patients in the Neoadjuvant Setting. Results From the GEICAM/2006-03, Multicenter Study. Breast Cancer Res Treat (2012) 136(2):487–93. doi: 10.1007/s10549-012-2100-y
21. Gianni L, Mansutti M, Anton A, Calvo L, Bisagni G, Bermejo B, et al. Comparing Neoadjuvant Nab-Paclitaxel vs Paclitaxel Both Followed by Anthracycline Regimens in Women With ERBB2/HER2-Negative Breast Cancer—The Evaluating Treatment With Neoadjuvant Abraxane (ETNA) Trial: A Randomized Phase 3 Clinical Trial. JAMA Oncol (2018) 4(3):302–8. doi: 10.1001/jamaoncol.2017.4612
22. Proctor MJ, McMillan DC, Morrison DS, Fletcher CD, Horgan PG, Clarke SJ. A Derived Neutrophil to Lymphocyte Ratio Predicts Survival in Patients With Cancer. Br J Cancer (2012) 107(4):695–9. doi: 10.1038/bjc.2012.292
23. Spring LM, Fell G, Arfe A, Sharma C, Greenup R, Reynolds KL, et al. Pathologic Complete Response After Neoadjuvant Chemotherapy and Impact on Breast Cancer Recurrence and Survival: A Comprehensive Meta-Analysis. Clin Cancer Res (2020) 26(12):2838–48. doi: 10.1158/1078-0432.CCR-19-3492
24. Schmid P, Cortés J, Dent R, Pusztai L, McArthur HL, Kuemmel S, et al. LBA8_PR - KEYNOTE-522: Phase III Study of Pembrolizumab (Pembro) + Chemotherapy (Chemo) vs Placebo (Pbo) + Chemo as Neoadjuvant Treatment, Followed by Pembro vs Pbo as Adjuvant Treatment for Early Triple-Negative Breast Cancer (TNBC). Ann Oncol (2019) 30:v853–v4. doi: 10.1093/annonc/mdz394.003
25. Loibl S, Schneeweiss A, Huober JB, Braun M, Rey J, Blohmer JU, et al. Durvalumab Improves Long-Term Outcome in TNBC: Results From the Phase II Randomized GeparNUEVO Study Investigating Neodjuvant Durvalumab in Addition to an Anthracycline/Taxane Based Neoadjuvant Chemotherapy in Early Triple-Negative Breast Cancer (TNBC). J Clinic Oncol (2021) 39: (15_suppl):506–. doi: 10.1200/JCO.2021.39.15_suppl.506
26. Zou Y, Zou X, Zheng S, Tang H, Zhang L, Liu P, et al. Efficacy and Predictive Factors of Immune Checkpoint Inhibitors in Metastatic Breast Cancer: A Systematic Review and Meta-Analysis. Ther Adv Med Oncol (2020) 12:1758835920940928. doi: 10.1177/1758835920940928
27. Denkert C, von Minckwitz G, Darb-Esfahani S, Lederer B, Heppner BI, Weber KE, et al. Tumour-Infiltrating Lymphocytes and Prognosis in Different Subtypes of Breast Cancer: A Pooled Analysis of 3771 Patients Treated With Neoadjuvant Therapy. Lancet Oncol (2018) 19(1):40–50. doi: 10.1016/S1470-2045(17)30904-X
28. Callari M, Cappelletti V, D’Aiuto F, Musella V, Lembo A, Petel F, et al. Subtype-Specific Metagene-Based Prediction of Outcome After Neoadjuvant and Adjuvant Treatment in Breast Cancer. Clin Cancer Res (2016) 22(2):337–45. doi: 10.1158/1078-0432.CCR-15-0757
29. Franzoi MA, Romano E, Piccart M. Immunotherapy for Early Breast Cancer: Too Soon, Too Superficial, or Just Right? Ann Oncol (2021) 32(3):323–36. doi: 10.1016/j.annonc.2020.11.022
Keywords: breast cancer, neoadjuvant chemotherapy, DNLR, PCR, immunology
Citation: Ocaña A, Chacón JI, Calvo L, Antón A, Mansutti M, Albanell J, Martínez MT, Lahuerta A, Bisagni G, Bermejo B, Semiglazov V, Thill M, Chan A, Morales S, Herranz J, Tusquets I, Chiesa M, Caballero R, Valagussa P, Bianchini G, Alba E and Gianni L (2022) Derived Neutrophil-to-Lymphocyte Ratio Predicts Pathological Complete Response to Neoadjuvant Chemotherapy in Breast Cancer. Front. Oncol. 11:827625. doi: 10.3389/fonc.2021.827625
Received: 02 December 2021; Accepted: 24 December 2021;
Published: 11 February 2022.
Edited by:
Michael Gnant, Medical University of Vienna, AustriaReviewed by:
Christoph Suppan, Medical University of Graz, AustriaCopyright © 2022 Ocaña, Chacón, Calvo, Antón, Mansutti, Albanell, Martínez, Lahuerta, Bisagni, Bermejo, Semiglazov, Thill, Chan, Morales, Herranz, Tusquets, Chiesa, Caballero, Valagussa, Bianchini, Alba and Gianni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alberto Ocaña, YWxiZXJ0by5vY2FuYUBzYWx1ZC5tYWRyaWQub3Jn; YWxiZXJ0by5vY2FuYUB1Y2xtLmVz
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.