
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 14 December 2021
Sec. Pediatric Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.770523
This article is part of the Research TopicCritical Complications In Pediatric Oncology and Hematopoietic Cell TransplantView all 31 articles
 Ali H. Ahmad1
Ali H. Ahmad1 Brandon D. Brown2
Brandon D. Brown2 Clark R. Andersen3
Clark R. Andersen3 Kris M. Mahadeo4
Kris M. Mahadeo4 Demetrios Petropolous4
Demetrios Petropolous4 José A. Cortes1
José A. Cortes1 Shehla Razvi1
Shehla Razvi1 Mary Katherine Gardner1
Mary Katherine Gardner1 Linette J. Ewing1
Linette J. Ewing1 Rodrigo E. Mejia1*
Rodrigo E. Mejia1*The use of flexible bronchoscopy (FB) with bronchoalveolar lavage (BAL) to diagnose and manage pulmonary complications has been shown to be safe in adult cancer patients, but whether its use is safe in pediatric cancer patients remains unclear. Thus, to describe the landscape of FB outcomes in pediatric cancer patients and to help define the populations most likely to benefit from the procedure, we undertook a retrospective review of FBs performed in patients younger than 21 years treated at our institution from 2002 to 2017. We found that a greater volume of total fluid instilled during BAL was significantly associated with increased probabilities of positive BAL culture (p=0.042), positive bacterial BAL culture (p=0.037), and positive viral BAL culture (p=0.0496). In more than half of the FB cases, findings resulted in alterations in antimicrobial treatment. Our study suggests that for pediatric cancer patients, FB is safe, likely provides diagnostic and/or therapeutic benefits, and has implications for treatment decisions.
Pulmonary complications are common events that result in significant morbidity and mortality for cancer patients of all ages (1–4). The presence of pulmonary infiltrates in cancer patients presents a diagnostic dilemma. The differential diagnosis includes malignant disease, inflammatory response, and infectious disease, the last of which could have a bacterial, viral, or fungal etiology. Noninvasive imaging is of limited utility in differentiating among these diagnoses. Thus, clinicians must often choose among invasive procedures, including flexible bronchoscopy (FB) with bronchoalveolar lavage (BAL), endobronchial ultrasound (EBUS) (5), radial EBUS, robotic bronchoscopy and computed tomography (CT) guided navigation (6), needle aspiration, and open lung biopsy, to yield a diagnosis. Of these options, FB with BAL is uniquely useful as a diagnostic and therapeutic lung examination procedure. Moreover, the BAL fluid obtained during FB provides a sample of the alveolar microenvironment, reflecting the greater respiratory system. This fluid may yield microbes such as bacteria, inflammatory cells such as macrophages, or malignant cells such as leukemic cells, which, if diagnostic, can guide the management of cancer patients with pulmonary infiltrates (7, 8).
In the present study, our primary objective was to describe the diagnostic yield of FB with BAL in pediatric (9) cancer patients. Our secondary objectives were to identify patient demographics that influence the diagnostic yield; determine the safety of FB and describe its short-, medium-, and long-term outcomes; and describe the rate of patients in whom FB results changed clinical management.
We conducted a retrospective chart review of all cancer patients younger than 21 years who underwent FB at MD Anderson from 2002 to 2017. Patients were identified from a database obtained from an electronic medical record query for FBs performed on pediatric patients by different physicians. We obtained discrete data, including cancer diagnosis; age; sex; laboratory values; diagnostic imaging data; pathology and microbiology results; lung biopsy results; antimicrobial treatment at the time of FB and after FB; noninvasive and/or mechanical ventilation data; indication for FB; location of FB; type of airway device or equipment used during bronchoscopy if indicated; specialty of the physician performing FB; number of BALs; volume of BAL fluid instilled; BAL return yield; lung segment and laterality of BAL; complications of FB; type and timing of HSCT; duration of hospitalization and intensive care unit (ICU) stay; and mortality. Patients received platelet transfusions prior to BAL if the platelet count was < 50 K/µL. Patients with a history refractory thrombocytopenia received a platelet transfusion at the time of the FB. If bleeding occurred during FB, patients were given additional platelet transfusions as clinically appropriate. Clotting parameters were requested only for patients with bleeding tendencies prior to the FB.
MD Anderson’s Institutional Review Board approved the study and waived the requirement for informed consent. Protected health information was initially collected, but names and medical record numbers were replaced with study numbers in the analytical file and were not published nor part of the aggregate data. Procedure and treatment dates were retained for analysis.
Information was retained on a password-protected network server. Protocol-specific study numbers were created for each study participant, and collected data were maintained in a secure password-protected database located on a departmental network server housed behind MD Anderson’s firewall. Complete confidentiality was maintained throughout the study and the preparation and submission of the manuscript.
Patient demographics and clinical characteristics were described and analyzed using means and medians for continuous variables and percentages for categorical variables.
Baseline variables were summarized as means with standard deviations or as frequencies with percentages. Rates of overall survival (calculated from the time of FB) at 3, 28 and 180 days were analyzed using the Kaplan-Meier method (10).
Binary outcomes were modeled by mixed effect logistic regression with relation to each continuous or discrete covariate, with a subject block to control for repeated measures. Continuous outcomes were modeled by mixed-effect linear regression with relation to each continuous or discrete covariate. Where appropriate, these linear models were replaced with generalized additive mixed-effect models with penalized splines accommodating nonlinear relations between the outcome and continuous covariates. Model-adjusted differences in outcomes among levels of discrete covariates were estimated with Tukey-adjusted contrasts.
Statistical analyses were performed using R statistical software (11). All statistical tests were two-sided, with alpha=.05. Survival modeling was performed using the “survival” package (12, 13). Differences among discrete variable levels of covariates in the linear and logistic models were estimated using the “emmeans” package; this analysis included adjusted means weighted proportionally to the covariate marginal frequencies. Catseye plots were produced using the “catseyes” package (14–16).
Patient demographics are summarized in Table 1. FB characteristics are summarized in Table 2. During the 16-year study period, 198 pediatric cancer patients underwent a total of 264 fiberoptic FBs (range, 1-6 FBs per patient). The mean patient age at the time of FB was 15.5 ± 5.2 years (range: 1.6-21.0 years). The most common indication for FB was BAL, in 196 (99.0%) patients.
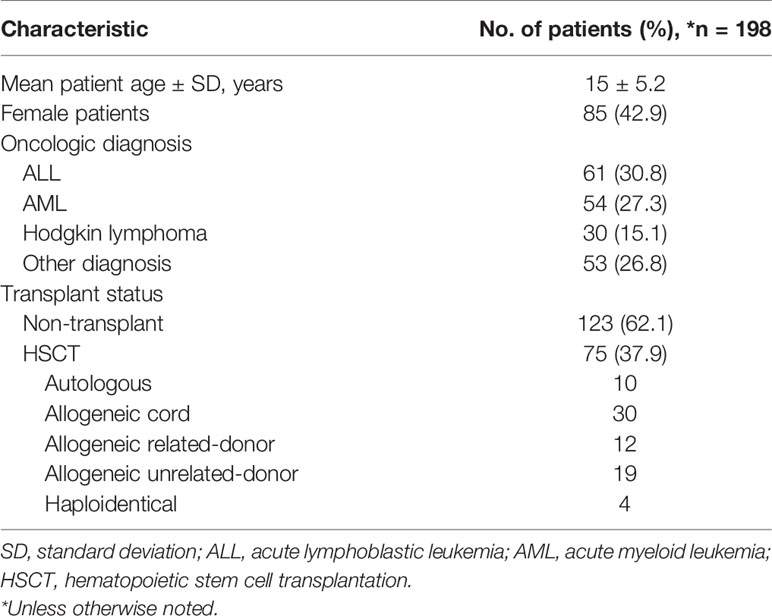
Table 1 Patient demographics.
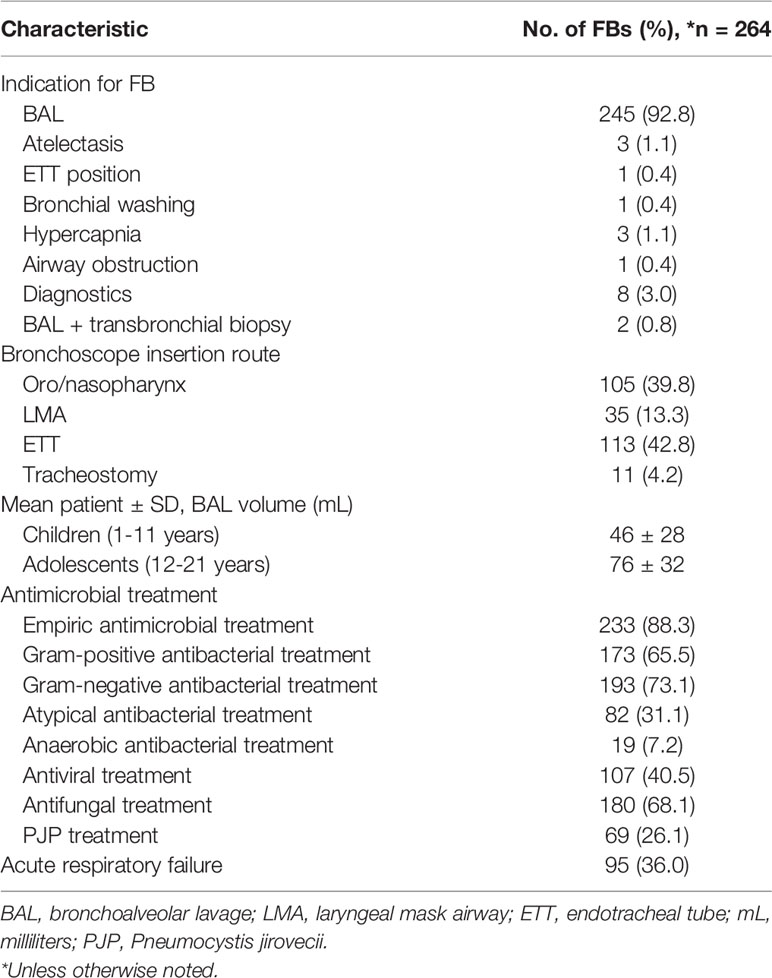
Table 2 Flexible bronchoscopy (FB) characteristics.
The most common underlying oncologic diagnoses were acute lymphoblastic leukemia in 61 (30.8%) patients, acute myelogenous leukemia in 54 (27.3%) patients, and Hodgkin lymphoma in 30 (15.2%) patients. Of the 198 patients included in the study, 75 (37.9%) underwent at least one HSCT.
At least one empiric antimicrobial treatment was initiated before FB in 233 (88.3%) cases. Ninety-five (36.0%) FBs were performed in patients who had acute respiratory failure and were on mechanical ventilation. Thirty-eight (14.4%) FBs were performed in patients who had acute respiratory failure and were on invasive mechanical ventilation with a positive end-expiratory pressure (PEEP) ≥10 cmH20 and a fraction of inspired oxygen (FiO2) ≥0.5.
FB-related complications occurred in 26 (9.8%) cases. In 10 (3.8%) cases, FB-related complications occurred in patients who had acute respiratory failure and were on invasive mechanical ventilation; in 4 (1.5%) cases, the patients had complications while receiving ventilation with a PEEP ≥ 10 cmH20 and a FiO2 ≥ 0.5. Major complications including hypoxia, tachycardia, hypotension and altered mental status occurred in 10 patients (3.8%). Minor complications included transient hypoxia and/or bronchospasm, bleeding and other occurred in 16 patients (6%) (Table 3). The most common major complication was hypoxia in 6 cases (2.3%), requiring ICU admission for non-invasive or invasive mechanical ventilation, with one (0.4%) patient requiring hospital transfer for inhaled nitric oxide. The most common minor complication was self limited bleeding in 5 (1.9%) cases with one patient (0.4%) requiring instillation of epinephrine. No associated mortality occurred as a result of FB.
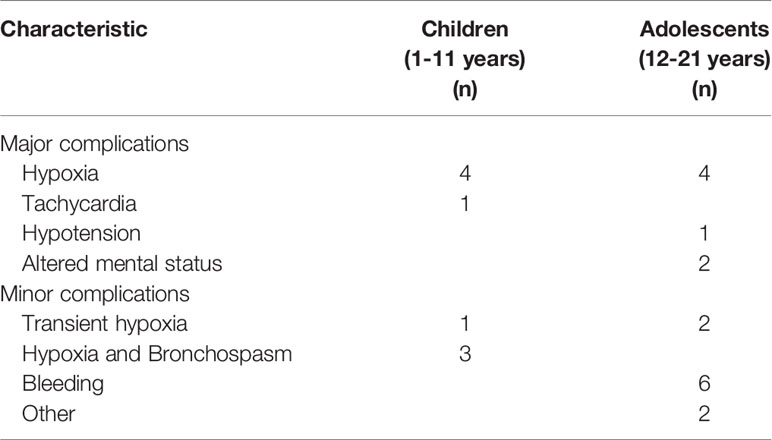
Table 3 Complications.
Clinical data are summarized in Table 4. These are categorized as respiratory function, which details mean ventilator settings and mean PaO2/FiO2 ratio, and bone marrow function, which details mean results of Complete Blood Count (CBC) with differential laboratory data
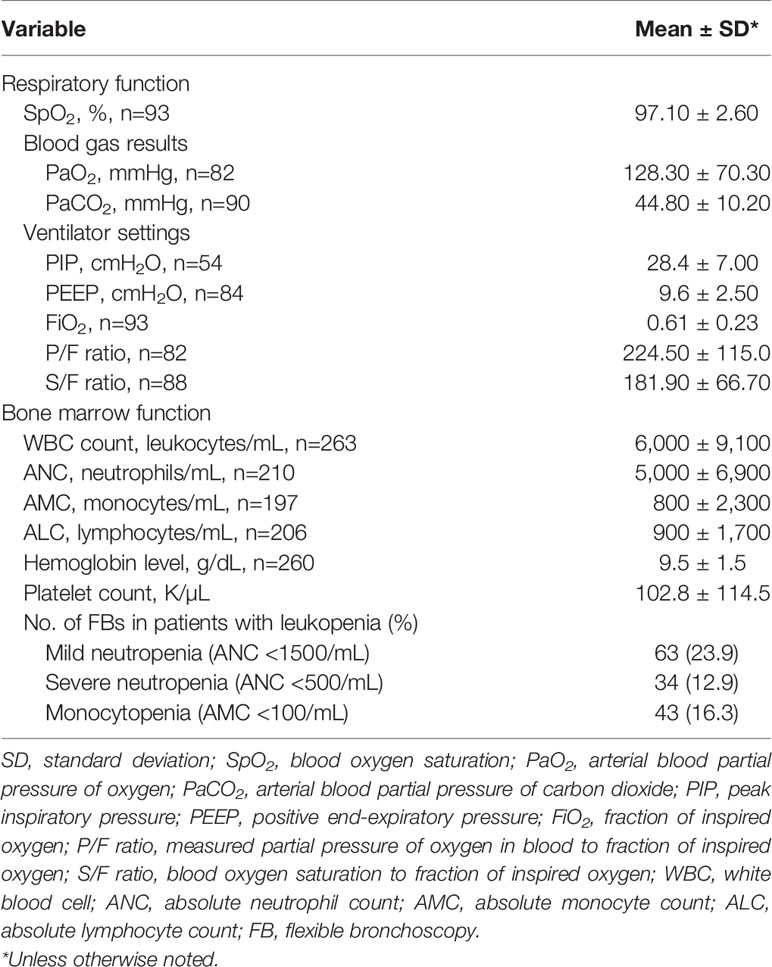
Table 4 Clinical data.
Bronchoscopy results are summarized in Table 5. FB yielded a specific diagnosis in 162 (61.4%) cases. In 4 (1.5%) cases, FB yielded a diagnosis of malignancy consistent with the patient’s underlying disease, including leukemia in 2 (0.8%) cases and metastatic osteosarcoma in 2 (0.8%) cases.
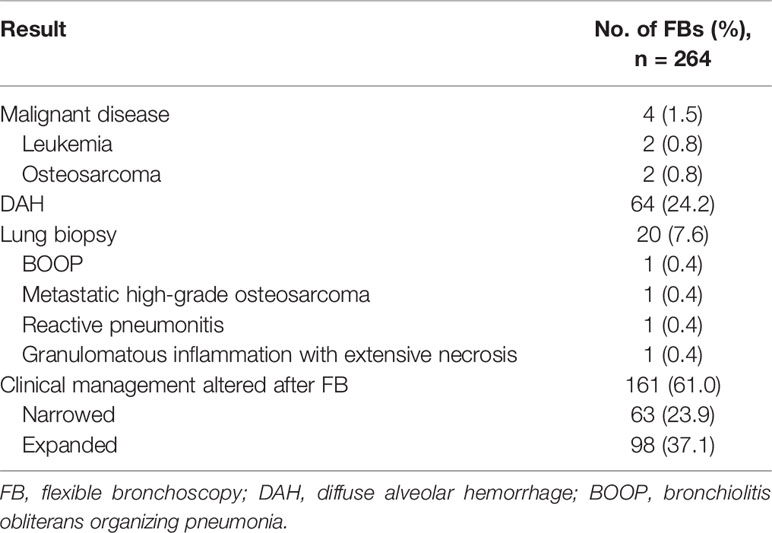
Table 5 Bronchoscopy results.
In 64 (24.2%) FB cases, diffuse alveolar hemorrhage, defined as greater than 20% hemosiderin-laden macrophages present in BAL fluid, was present. Fourteen BALs returned fluid described as bloody.
The most common organisms retrieved from BAL are described in Table 6. In 157 (59.5%) FB cases, BAL yielded positive cultures with single pathogens, including 35 (13.3%) cultures with bacteria, 32 (12.1%) cultures with viruses, 37 (14.0%) cultures with fungi, 3 (1.1%) cultures with PJP, 3 (1.1%) cultures with acid-fast bacilli, and 38 (14.4%) cultures with multiple pathogens. In 6 (2.3%) FB cases, a culture was not obtained.
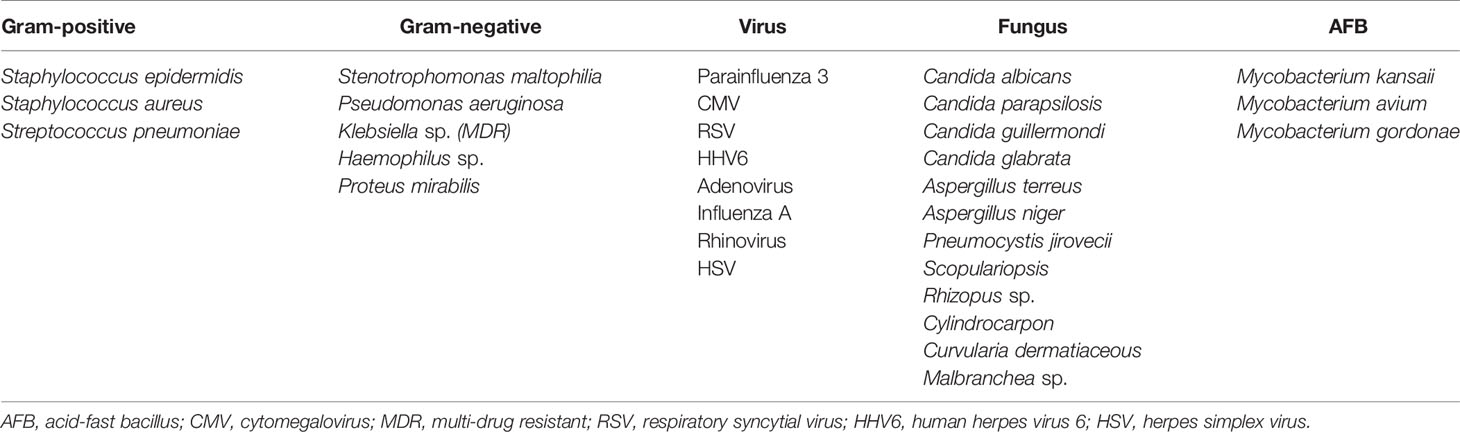
Table 6 Most common organisms retrieved from bronchoalveolar lavage samples.
Lung biopsy, which was performed in 20 (7.6%) FB cases, yielded a variety of diagnoses, including 1 (0.4%) case of bronchiolitis obliterans organizing pneumonia, 1 (0.4%) case of metastatic high-grade osteosarcoma, 1 (0.4%) case of reactive pneumonitis, and 1 (0.4%) case of granulomatous inflammation with extensive necrosis.
The clinical management was altered after FB in 161 of 233 cases (69.1%) of patients receiving empiric antimicrobial therapy. In 63 (27%) cases, antimicrobial therapy was narrowed, and in 98 (42.1%) cases, antimicrobial therapy was expanded.
The mean duration of ICU stay was 17.4 ± 23.0 days, and the mean duration of hospitalization was 30.20 ± 31.50 days. The 3, 28 and 180 day overall survival rates were 99.0%, 86.4%, and 60.1%, respectively (Figure 1).
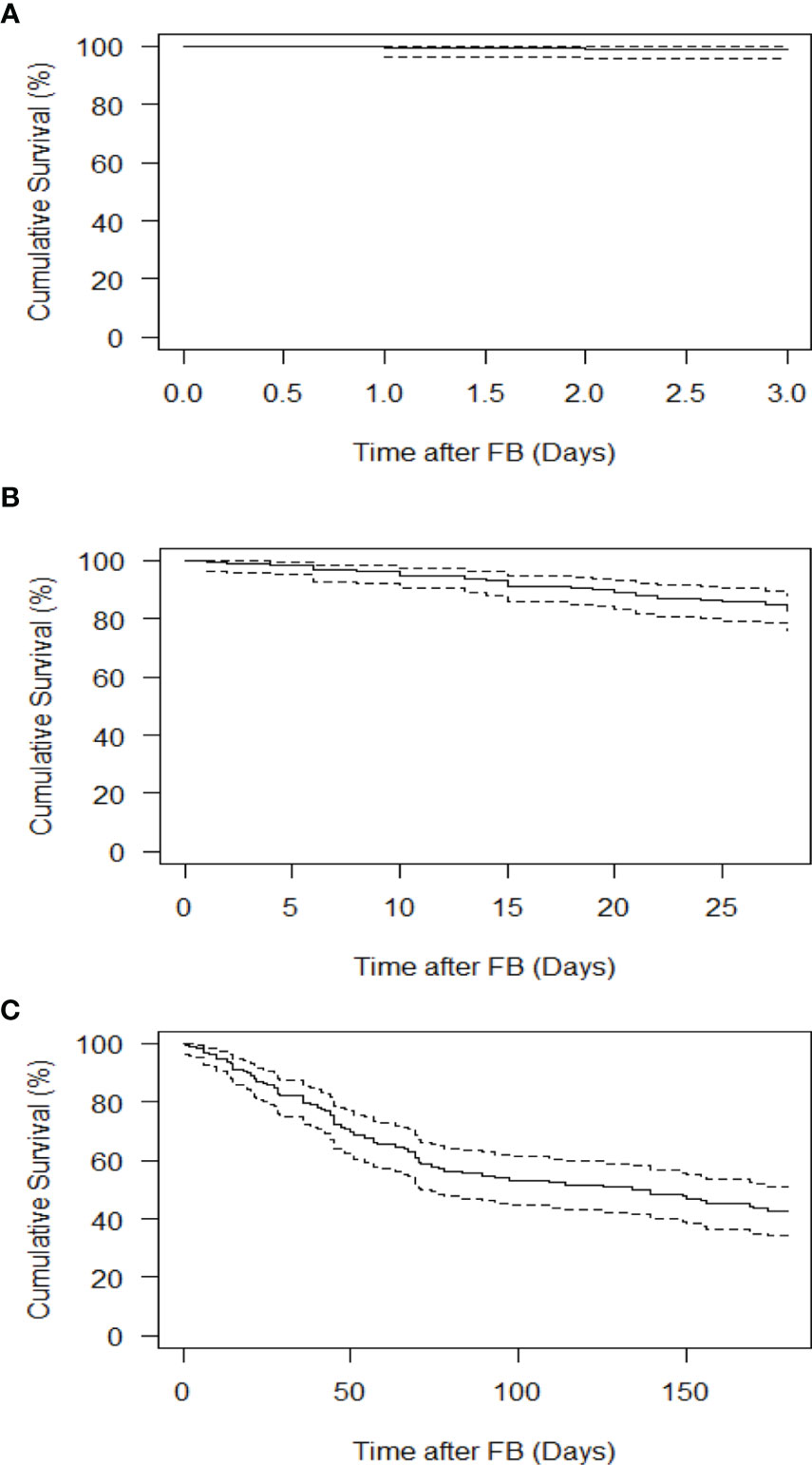
Figure 1 Survival of pediatric and AYA patients undergoing FB. (A) 3 day survival. (B) 28-day survival. (C) 180 day survival. Solid lines indicate the Kaplan-Meier survival curve, while dashed lines indicate 95% confidence intervals.
Increased total fluid instilled during BAL (in mL) was significantly associated with increased probabilities of positive BAL culture (p=0.042, odds ratio [OR]=1.01, 95% confidence interval [CI]=1.00-1.01), positive bacterial BAL culture (p=0.037, OR=1.01, 95% CI=1.01-1.02), and positive viral BAL culture (p=0.0496, OR=1.02, 95% CI=1.01-1.02) (Figures 2A–C) but not positive fungal BAL culture (p=0.38, OR=1.01, 95% CI=1.00-1.01).

Figure 2 Impact of total fluid instilled during BAL on culture results. (A) Probability of positive BAL culture. (B) Probability of positive bacterial BAL culture. (C) Probability of positive viral BAL culture. Regression curves are shown as solid lines, bounded by shaded 95% confidence intervals. Scatterplots show raw patient measures, jittered slightly for clarity.
There was a trend for older age to be associated with an increased probability of positive BAL culture (p=0.062, OR=1.05, 95% CI=1.02-1.08). Older age was significantly associated with an increased probability of positive BAL culture with multiple organisms (p=0.013, OR=1.15, 95% CI=1.09-1.22) and with a higher volume of total fluid instilled during BAL (p<0.0001, slope=2.38, 95% CI=1.39-3.36) (Figure 3). Our study findings did not demonstrate however a correlation between higher positive cultures for any organism from 0-7 days vs. 7-14 days and for subsets for, viral or fungal cultures with days of antibiotics and time of FB (Figure 4).
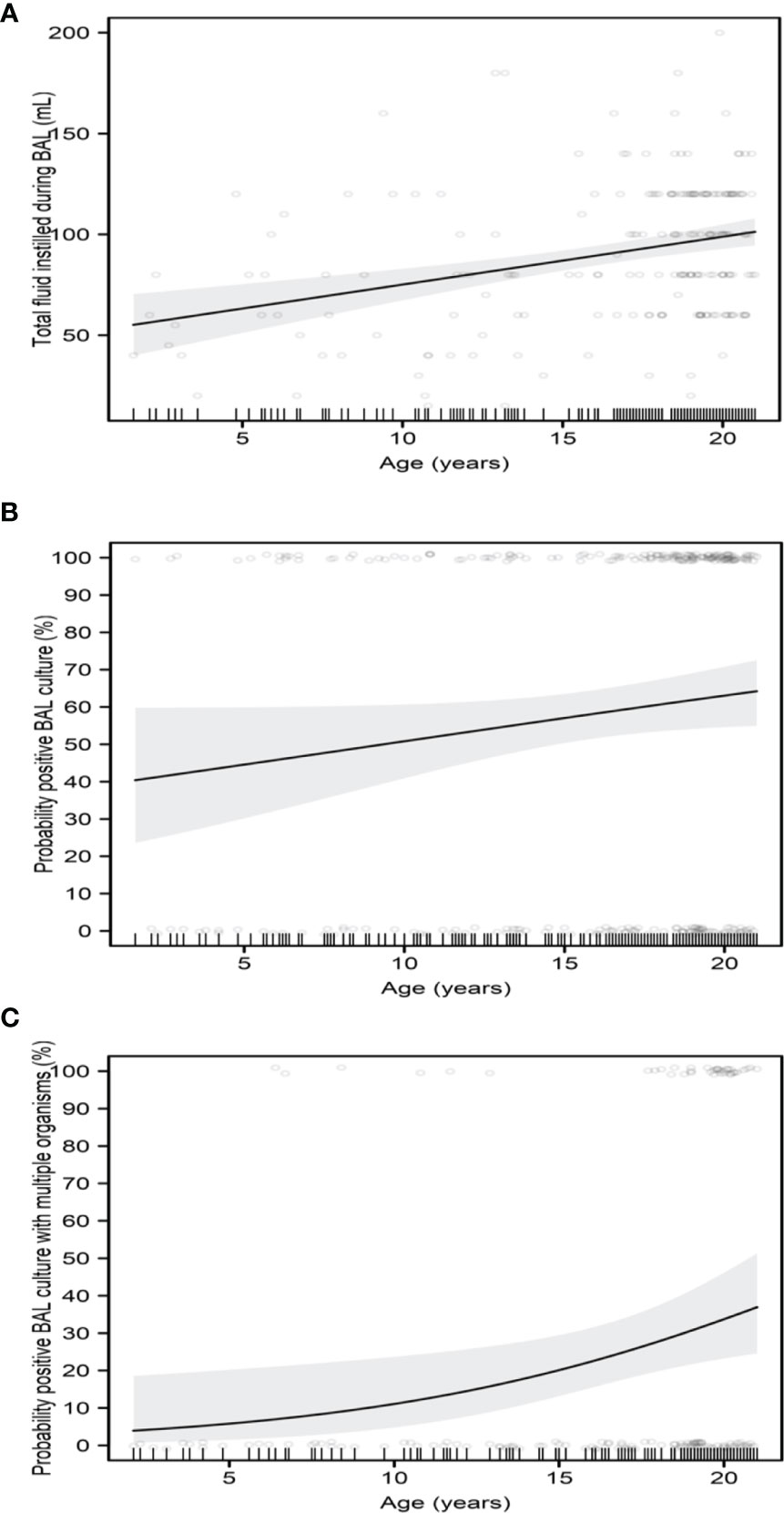
Figure 3 Impact of age on BAL. (A) Total fluid instilled during BAL. (B) Probability of positive BAL culture. (C) Probability of positive BAL culture with multiple organisms. Regression curves are shown as solid lines, bounded by shaded 95% confidence intervals. Scatterplots show raw patient measures, jittered slightly for clarity in the probability plots.
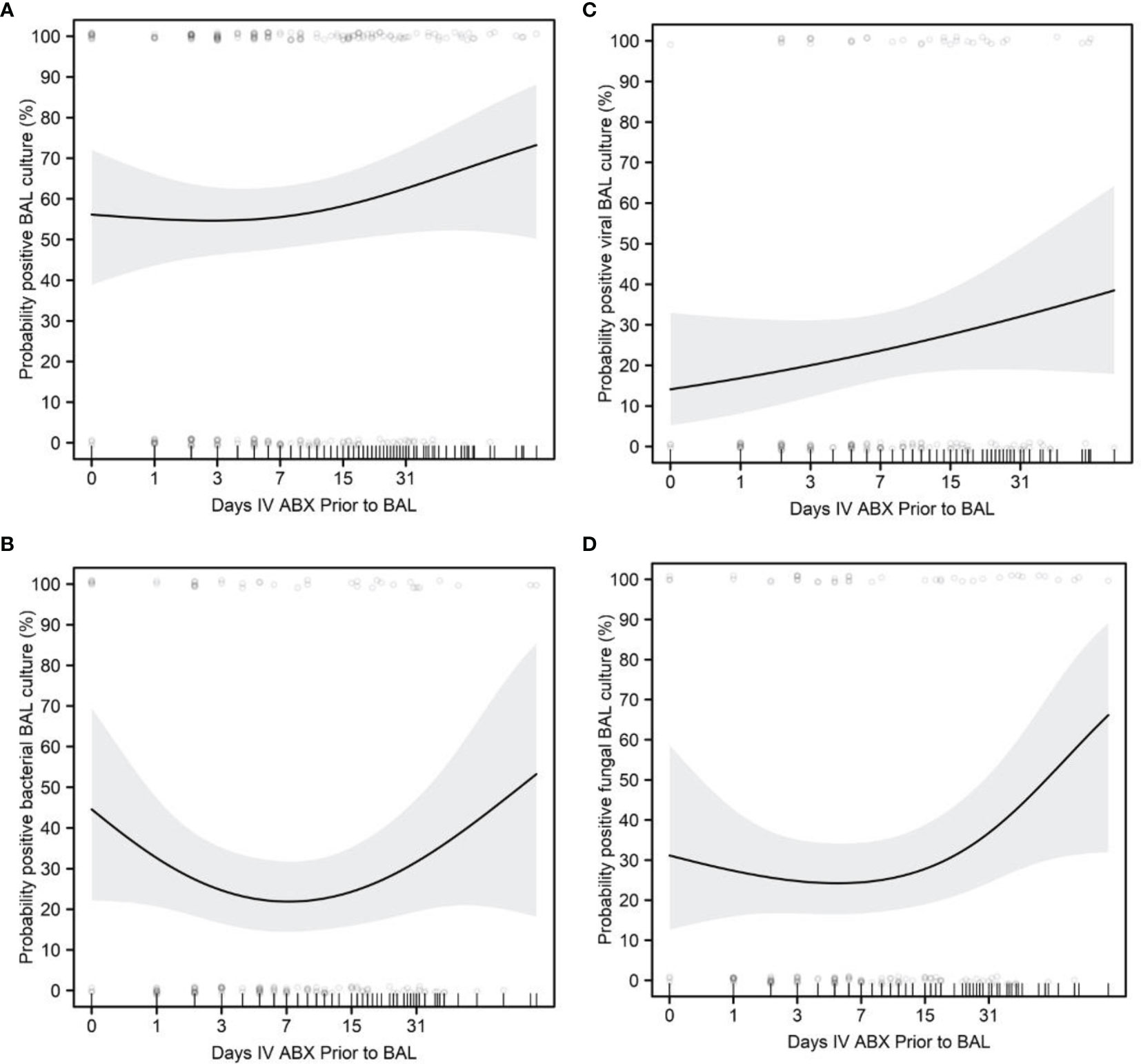
Figure 4 Impact of days of antibiotics and positive BAL cultures. (A) Probability of positive BAL culture. (B) Probability of positive BAL bacterial culture. (C) Probability of positive viral BAL culture. (D) Probability of positive fungal BAL culture. Regression curves are shown as solid lines, bounded by shaded 95% confidence intervals. Scatterplots show raw patient measures, jittered slightly for clarity in the probability plots.
A history of HSCT was significantly associated with an increased probability of positive viral BAL culture (p=0.019, OR=16.84, 95% CI=1.59-178). Among patients with a history of HSCT, those who had received allogeneic unrelated-donor HSCT were the most likely to have a positive viral culture. Patients with a history of autologous HSCT had no positive viral BAL cultures. Longer post-HSCT duration was significantly associated with increased probabilities of positive BAL culture (p=0.017, OR=1.35, 95% CI=1.19-1.53) and positive BAL culture with multiple organisms (p=0.031, OR=1.62, 95% CI=1.3-2.02) (Figure 5).
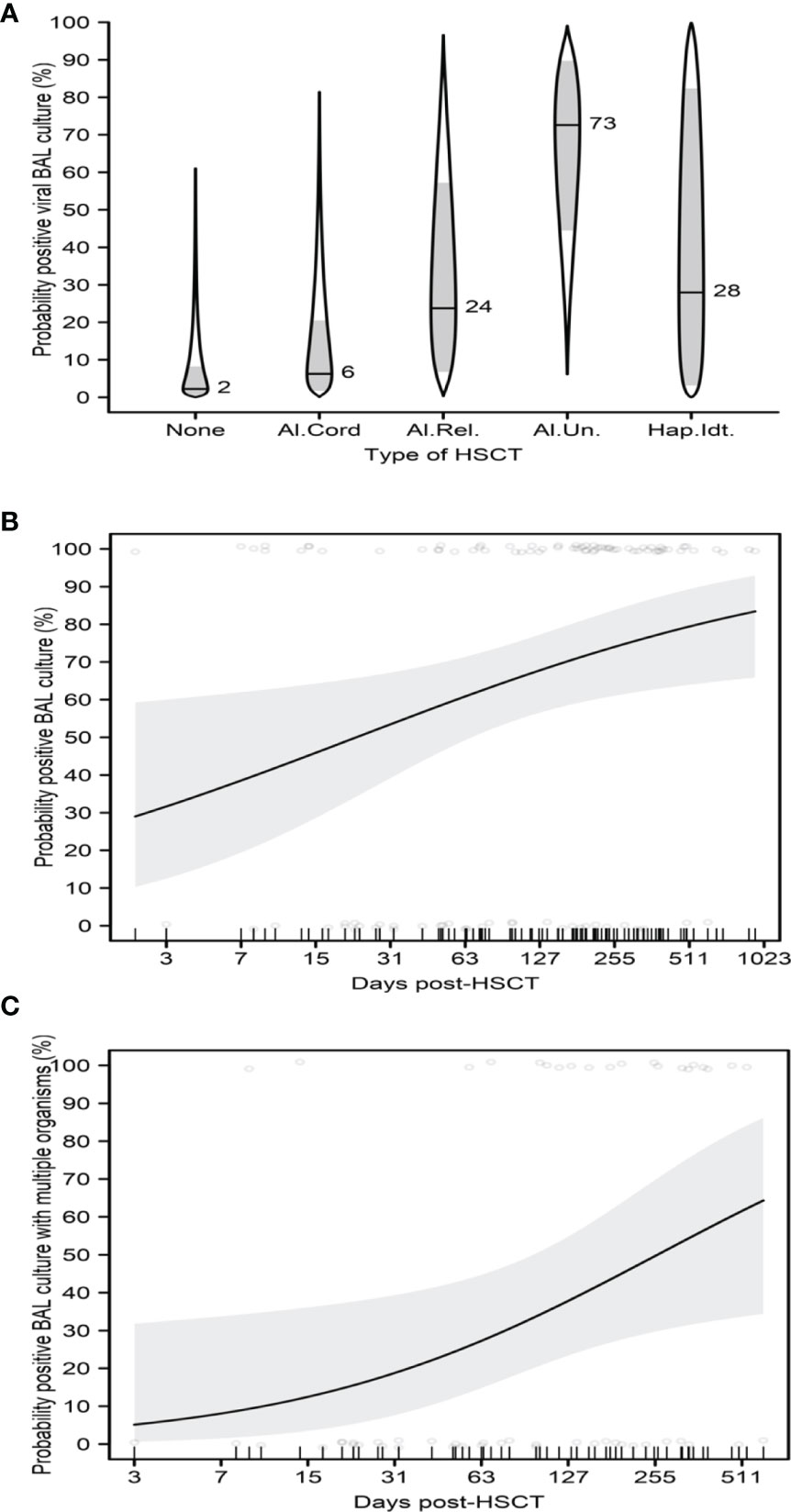
Figure 5 Impact of HSCT on BAL. (A) Probability of positive viral BAL culture with type of HSCT. (B) Probability of positive BAL culture with post-HSCT duration. (C) Probability of positive BAL culture with multiple organisms with post-HSCT duration. (A) shows catseye plots illustrate the normal distributions of the model-adjusted means (horizontal lines, with corresponding numeric percentage probability), with shaded +/- standard error intervals, transformed to the probability scale. In (B, C), regression curves are shown as solid lines, bounded by shaded 95% confidence intervals. Scatterplots show raw patient measures, jittered slightly for clarity.
An ALC <24 cells/mL was significantly associated with a longer duration of antimicrobial therapy prior to BAL (p=0.007, ratio=1.65, 95% CI=1.15-2.35). There was a trend for a lower ANC to be associated with an increased probability of positive fungal BAL culture (p=0.07, OR=0.74, 95% CI=0.62-0.87). There was also a trend for a lower AMC to be associated with an increased probability of positive fungal BAL culture (p=0.055, nonlinear estimated degrees of freedom=1.98).
In the current study, we describe the utility of FB with BAL among 196 pediatric cancer patients. In this, single-center review, we found that an increased total fluid volume instilled during BAL was significantly associated with increased probabilities of positive BAL culture, positive bacterial BAL culture, and positive viral BAL culture in pediatric cancer patients. Furthermore, we found that older patients were more likely to receive a large BAL instillation volume and thus had increased probabilities of a positive BAL culture and a positive BAL culture with multiple organisms. Consensus on fluid instillation, acquisition and processing in children was lacking prior to Ratjen’s (17) and Riedler’s studies (18). In 2000, The European Respiratory Society Task Force on bronchoalveolar lavage in children described a variety of protocols for BAL fluid instillation in pediatric patients (19). One approach is to instill 3 mL/kg divided into three equal aliquots for children weighing less than 20 kg and to instill 3 mL/kg in 20-mL portions for children weighing more than 20 kg (18, 20). Another approach is to adjust the BAL instillation volume according to the child’s functional residual capacity (21). Others use the method applied in adults, which is to instill 2-4 aliquots of the same volume (generally 10-20 mL), regardless of the patient’s body weight and age (22, 23). In our study, children had BAL with 3mL/kg in 10-20mL aliquots while adolescents had 2-5 aliquots of the same volume (20 mL) following best practice guidelines as referenced.
We also found a trend for both neutropenia and monocytopenia to be associated with an increased probability of positive fungal BAL culture. This is consistent with the findings of a prospective multicenter study by Villarroel et al., who found that an ANC ≤500 neutrophils/mL and AMC ≤100 monocytes/mL were each independently associated with an increased probability of invasive fungal disease (24).
In addition, we also found that the type of HSCT was associated with the probability of a positive BAL viral culture; among HSCT patients, those who underwent allogeneic unrelated-donor HSCT were the most likely to have a positive culture. This association could be explained in part by the myeloablative conditioning regimens patients receive in preparation for HSCT, whereas the predominance of allogeneic transplants may be explained by the use of immunomodulators to prevent graft-versus-host disease, each resulting in a relatively greater degree of immunosuppression (25). Our study also showed that longer post-HSCT duration was significantly associated with increased probabilities of both positive BAL culture and positive BAL culture with multiple organisms. This may be explained by the fact that after engraftment, B-cell and CD4 T-cell recover slowly; however, HSCT patients are still at risk for viral and fungal infections as well as infections caused by encapsulated bacteria (26). In addition, our findings support those of prior studies showing that BAL results influence treatment decisions (1, 27). Antimicrobial treatment was altered after more than half (69.1%) of the FB cases in the present study, with treatment narrowed in 27% of cases and treatment expanded in 42.1% of cases. In the cases where antibiotics were expanded, the most common class switch were done in patients with positive BAL cultures, worsening respiratory symptomatology or as a result of overall clinical deterioration. These included class switches from cephalosporins to carbapenems, addition of gram-positive coverage, anaerobic, antiviral, PJP and or atypical organisms’ coverage respectively. In cases where antibiotics were narrowed, the most common class switches were from carbapenems to cephalosporins or as a result of de-escalation of antiviral, PJP, antifungal coverage for patients with negative cultures, improved clinical condition or recommendation from the infectious disease consultant. Although we did not report sensitivities in the study, the data we report reflects subset of oncology and stem cell transplant patients who developed infections following standard prophylaxis strategies. While antimicrobial prophylaxis and therapies against bacterial, viral and fungal infections have improved over time, pediatric cancer and stem cell transplant patients, and perhaps, those in particular with lower respiratory tract infections may not exhibit robust responses to anti-microbial therapies in the absence of host immune defense systems (26, 28, 29).
Our findings did not demonstrate a relationship between timing of FB and diagnostic yield for infectious pathogens or between timing of FB and FB complications. This may be due to the fact that in 88.3% FBs, our subjects were receiving empiric antibiotics at the time of the FB. This is contrary to others findings, which found that as the duration of empiric antimicrobials increased, the BAL yield for positive cultures decreased (30–35).
The complication rate of FB in our study was 9.8%, with the most common complication being hypoxia (5.3%). This complication rate is lower than that described by Efrati et al. (30.6%) (36), but higher than in other studies (7, 37). A proposed pathophysiologic mechanism is that as the pathologic process involving the lung evolves, the parenchyma may become more inflamed, thereby increasing the propensity for complications such as bleeding and pneumothorax (31, 32).
Furthermore, in our study, the 3-day survival rate (99.0%) was higher than the 28-day and 180 day survival rates (86.4% and 60.1%, respectively), which suggests that patients were more likely to die from their disease than from complications related to FB.
Prior studies have also shown that FB with BAL is useful in the evaluation of pulmonary infiltrates in pediatric cancer patients. In a prospective trial of 14 pediatric patients with histories as varied as lymphoid and solid organ malignancies, solid organ transplant, and systemic lupus erythematosus, Pattishall et al. found that FB had a diagnostic yield of 71%, with the most common organisms being PJP, cytomegalovirus (CMV), Candida, and Aspergillus (27). In a retrospective analysis, Efrati et al. compared a cohort of children with cancer or primary immune deficiency (85% of whom previously received broad-spectrum antibiotics) with a control cohort of patients without a malignant diagnosis who underwent FB with BAL during the same period. A diagnosis was obtained in more than 80% of patients in both groups, and a definitive organism was detected in 53% of the patients in the cancer cohort and 18% of the patients in the control group, resulting in treatment alteration rates of 33% and 21%, respectively. Approximately 30% of the patients in the cancer cohort experienced complications, most of which were related to minor desaturations, whereas only 15% of the patients in the control group experienced complications. One cancer patient required mechanical ventilation following the procedure (36). In another retrospective study of FB with BAL in 33 patients with leukemia and pulmonary infiltrates, tracheobronchitis was identified in 51% of patients, endobronchial hypersecretion in 18%, and pulmonary hemorrhage in 21%. BAL cultures were positive in 63% of patients, revealing Candida in 39% of patients and Aspergillus in 9% of patients. There was a trend for early bronchoscopy to be associated with improved overall survival (35). In a recent review of 64 children diagnosed with leukemia, FB with BAL revealed that 56% of patients had positive microbiology results, including bacterial, viral, and fungal infections. Antimicrobial coverage was changed in more than 83% of patients. Approximately 38% of patients who underwent BAL had complications, the most common of which was hypoxia (38). Prior studies report changes in antimicrobial management after BAL (37–39) but won’t comment on prognosis and survival except for three studies in which positive and negative BAL results prompted antimicrobial changes (1, 40) but failed to show improvement in survival (36). Most of these studies, whose numbers of pediatric cancer patients ranged from 14 to 117, were relatively small compared to adult cohort studies (1, 35, 37, 41).
Our study had limitations. First, because this study was an exploratory, retrospective, single-center review, its findings may reflect technical aspects of the performance of FB and/or laboratory analysis that are unique to our institution. Second, while the data obtained via FB led to alteration of antimicrobial management in most cases, it is not clear whether those alterations impacted patient outcomes. The retrospective design of our study did not allow for this analysis. Lastly, the statistical analyses involved multiple testing of associations among the many variables, and no adjustment was made for multiple testing. A larger, multicenter prospective observational trial would attenuate institutional clinical practice influences and have the statistical power necessary to definitively show significant associations.
While acknowledging these limitations, our study also has several strengths. To our knowledge, this is the largest study of BAL in the pediatric oncology and HSCT population and the only BAL study in pediatric cancer patients that reports on total fluid volume instillation having an impact on BAL culture results. Additionally, our observations regarding BAL instillation volume and BAL culture positivity may help inform clinicians’ practice while performing the BAL procedure. Furthermore, the fact that BAL results altered antimicrobial treatment in more than half of the FB cases we observed also informs clinicians of the diagnostic utility of BAL when presented with pneumonias of unclear etiology in pediatric oncology and HSCT patients.
In summary, our study suggests that in pediatric oncology and HSCT patients, FB is safe, provides diagnostic and/or therapeutic benefits, and has implications for treatment decisions. Larger multicenter study evaluating the role of FB in pediatric cancer patients may further elucidate its utility for clinical care in this population.
The raw data supporting the conclusions of this article will be made available by the authors, upon request, without undue reservation.
The studies involving human participants were reviewed and approved by University of Texas MD Anderson Cancer Center Institutional Review Board. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
RM: Fiberoptic bronchoscopies, study conception, data acquisition, analysis, and manuscript writing. AA: Fiberoptic bronchoscopy assistance, data acquisition, analysis, and manuscript writing. BB: Data acquisition, analysis, and manuscript writing. CA: Statistical modeling. JC, SR, MG, and LE: Fiberoptic bronchoscopy assistance. DP and KM: Analysis. All authors contributed to the article and approved the submitted version.
This study was supported in part by the NIH through MD Anderson’s Cancer Center Support Grant (CA16672).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Joe Munch in MD Anderson’s Research Medical Library for editing the manuscript, Jonathan Gill, MD for helping with the protocol submission to IRB; Carlos Jimenez, MD for helping with the study conception and Phillip J. Lum, BBA for his help with data abstraction and database creation.
1. Park JR, Fogarty S, Brogan TV. Clinical Utility of Bronchoalveolar Lavage in Pediatric Cancer Patients. Med Pediatr Oncol (2002) 39(3):175–80. doi: 10.1002/mpo.10130
2. Breuer R, Lossos IS, Berkman N, Or R. Pulmonary Complications of Bone Marrow Transplantation. Respir Med (1993) 87(8):571–9. doi: 10.1016/S0954-6111(05)80259-8
3. Cordonnier C, Bernaudin JF, Bierling P, Huet Y, Vernant JP. Pulmonary Complications Occurring After Allogeneic Bone Marrow Transplantation. A Study of 130 Consecutive Transplanted Patients. Cancer (1986) 58(5):1047–54. doi: 10.1002/1097-0142(19860901)58:5<1047::aid-cncr2820580512>3.0.co;2-y
4. Jules-Elysee K, Stover DE, Yahalom J, White DA, Gulati SC. Pulmonary Complications in Lymphoma Patients Treated With High-Dose Therapy Autologous Bone Marrow Transplantation. Am Rev Respir Dis (1992) 146(2):485–91. doi: 10.1164/ajrccm/146.2.485
5. Anantham D, Koh MS, Ernst A. Endobronchial Ultrasound. Respir Med (2009) 103(10):1406–14. doi: 10.1016/j.rmed.2009.04.010
6. Agrawal A, Hogarth DK, Murgu S. Robotic Bronchoscopy for Pulmonary Lesions: A Review of Existing Technologies and Clinical Data. J Thorac Dis (2020) 12(6):3279–86. doi: 10.21037/jtd.2020.03.35
7. Stokes DC, Shenep JL, Parham D, Bozeman PM, Marienchek W, Mackert PW. Role of Flexible Bronchoscopy in the Diagnosis of Pulmonary Infiltrates in Pediatric Patients With Cancer. J Pediatr (1989) 115(4):561–7. doi: 10.1016/S0022-3476(89)80281-1
8. Zhang Y, Liu Z, Li S, Wang M, Dai D, Jing H, et al. Upregulation of E-Cadherin in Bronchoalveolar Lavage Fluid-Derived Exosomes in Patients With Lung Cancer. Thorac Cancer (2020) 11(1):41–7. doi: 10.1111/1759-7714.13220
9. Hardin AP, Hackell JM, COMMITTEE ON PRACTICE AND AMBULATORY MEDICINE. Age Limit of Pediatrics. Pediatrics (2017) 140(3):e20172151. doi: 10.1542/peds.2017-2151
10. Kaplan ELMP. Nonparametric Estimation From Incomplete Observations. J Am Stat Assoc (1958) 53(282):457–81. doi: 10.1080/01621459.1958.10501452
11. Team RC. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing (2020). Available at: https://www.R-project.org/.
12. Therneau TM, Grambsch PM. Modeling Survival Data: Extending the Cox Model. New York: Springer (2000).
13. Therneau T. A Package for Survival Analysis in R. R Package Version 32-32020. Available at: https://CRAN.R-project.org/package=survival.
14. Lenth RV. Emmeans: Estimated Marginal Means, Aka Least-Squares Means. R Package Version 1462020 . Available at: https://CRAN.R-project.org/package=emmeans.
15. Cumming G. The New Statistics: Why and How. Psychol Sci (2014) 27:7–29. doi: 10.1177/0956797613504966
16. Andersen C. Catseyes: Create Catseye Plots Illustrating the Normal Distribution of the Means. R Package Version 0252020. Available at: https://CRAN.R-project.org/package=catseyes.
17. Ratjen F, Bruch J. Adjustment of Bronchoalveolar Lavage Volume to Body Weight in Children. Pediatr Pulmonol (1996) 21(3):184–8. doi: 10.1002/(SICI)1099-0496(199603)21:3<184::AID-PPUL6>3.0.CO;2-Q
18. Riedler J, Grigg J, Stone C, Tauro G, Robertson CF. Bronchoalveolar Lavage Cellularity in Healthy Children. Am J Respir Crit Care Med (1995) 152(1):163–8. doi: 10.1164/ajrccm.152.1.7599817
19. de Blic J, Midulla F, Barbato A, Clement A, Dab I, Eber E, et al. Bronchoalveolar Lavage in Children. ERS Task Force on Bronchoalveolar Lavage in Children. European Respiratory Society. Eur Respir J (2000) 15(1):217–31. doi: 10.1183/09031936.00.15121700
20. Grigg J, van den Borre C, Malfroot A, Pierard D, Wang D, Dab I. Bilateral Fiberoptic Bronchoalveolar Lavage in Acute Unilateral Lobar Pneumonia. J Pediatr (1993) 122(4):606–8. doi: 10.1016/S0022-3476(05)83547-4
21. de Blic J, McKelvie P, Le Bourgeois M, Blanche S, Benoist MR, Scheinmann P. Value of Bronchoalveolar Lavage in the Management of Severe Acute Pneumonia and Interstitial Pneumonitis in the Immunocompromised Child. Thorax (1987) 42(10):759–65. doi: 10.1136/thx.42.10.759
22. Pingleton SK, Harrison GF, Stechschulte DJ, Wesselius LJ, Kerby GR, Ruth WE. Effect of Location, Ph, and Temperature of Instillate in Bronchoalveolar Lavage in Normal Volunteers. Am Rev Respir Dis (1983) 128(6):1035–7. doi: 10.1164/arrd.1983.128.6.1035
23. Wilmott RW, Kassab JT, Kilian PL, Benjamin WR, Douglas SD, Wood RE. Increased Levels of Interleukin-1 in Bronchoalveolar Washings From Children With Bacterial Pulmonary Infections. Am Rev Respir Dis (1990) 142(2):365–8. doi: 10.1164/ajrccm/142.2.365
24. Villarroel M, Aviles CL, Silva P, Guzman AM, Poggi H, Alvarez AM, et al. Risk Factors Associated With Invasive Fungal Disease in Children With Cancer and Febrile Neutropenia: A Prospective Multicenter Evaluation. Pediatr Infect Dis J (2010) 29(9):816–21. doi: 10.1097/INF.0b013e3181e7db7f
25. Zinter MS, Logan BR, Fretham C, Sapru A, Abraham A, Aljurf MD, et al. Comprehensive Prognostication in Critically Ill Pediatric Hematopoietic Cell Transplant Patients: Results From Merging the Center for International Blood and Marrow Transplant Research (CIBMTR) and Virtual Pediatric Systems (VPS) Registries. Biol Blood Marrow Transplant (2020) 26(2):333–42. doi: 10.1016/j.bbmt.2019.09.027
26. Tomblyn M, Chiller T, Einsele H, Gress R, Sepkowitz K, Storek J, et al. Guidelines for Preventing Infectious Complications Among Hematopoietic Cell Transplant Recipients: A Global Perspective. Preface Bone Marrow Transplant (2009) 44(8):453–5. doi: 10.1038/bmt.2009.254
27. Pattishall EN, Noyes BE, Orenstein DM. Use of Bronchoalveolar Lavage in Immunocompromised Children With Pneumonia. Pediatr Pulmonol (1988) 5(1):1–5. doi: 10.1002/ppul.1950050102
28. Lehrnbecher T, Phillips R, Alexander S, Alvaro F, Carlesse F, Fisher B, et al. Guideline for the Management of Fever and Neutropenia in Children With Cancer and/or Undergoing Hematopoietic Stem-Cell Transplantation. J Clin Oncol (2012) 30(35):4427–38. doi: 10.1200/JCO.2012.42.7161
29. Averbuch D, Orasch C, Cordonnier C, Livermore DM, Mikulska M, Viscoli C, et al. European Guidelines for Empirical Antibacterial Therapy for Febrile Neutropenic Patients in the Era of Growing Resistance: Summary of the 2011 4th European Conference on Infections in Leukemia. Haematologica (2013) 98(12):1826–35. doi: 10.3324/haematol.2013.091025
30. Shannon VR, Andersson BS, Lei X, Champlin RE, Kontoyiannis DP. Utility of Early Versus Late Fiberoptic Bronchoscopy in the Evaluation of New Pulmonary Infiltrates Following Hematopoietic Stem Cell Transplantation. Bone Marrow Transplant (2010) 45(4):647–55. doi: 10.1038/bmt.2009.203
31. Kuehnhardt D, Hannemann M, Schmidt B, Heider U, Possinger K, Eucker J. Therapeutic Implication of BAL in Patients With Neutropenia. Ann Hematol (2009) 88(12):1249–56. doi: 10.1007/s00277-009-0747-1
32. Pereira Gomes JC, Pedreira WL Jr., Araujo EM, Soriano FG, Negri EM, Antonangelo L, et al. Impact of BAL in the Management of Pneumonia With Treatment Failure: Positivity of BAL Culture Under Antibiotic Therapy. Chest (2000) 118(6):1739–46. doi: 10.1378/chest.118.6.1739
33. Hohenadel IA, Kiworr M, Genitsariotis R, Zeidler D, Lorenz J. Role of Bronchoalveolar Lavage in Immunocompromised Patients With Pneumonia Treated With a Broad Spectrum Antibiotic and Antifungal Regimen. Thorax (2001) 56(2):115–20. doi: 10.1136/thorax.56.2.115
34. Bartlett JG. Diagnostic Tests for Agents of Community-Acquired Pneumonia. Clin Infect Dis (2011) 52(Suppl 4):S296–304. doi: 10.1093/cid/cir045
35. Furuya ME, Ramirez-Figueroa JL, Vargas MH, Bernaldez-Rios R, Vazquez-Rosales JG, Rodriguez-Velasco A. Diagnoses Unveiled by Early Bronchoscopy in Children With Leukemia and Pulmonary Infiltrates. J Pediatr Hematol Oncol (2012) 34(8):596–600. doi: 10.1097/MPH.0b013e318240d54b
36. Efrati O, Gonik U, Bielorai B, Modan-Moses D, Neumann Y, Szeinberg A, et al. Fiberoptic Bronchoscopy and Bronchoalveolar Lavage for the Evaluation of Pulmonary Disease in Children With Primary Immunodeficiency and Cancer. Pediatr Blood Cancer (2007) 48(3):324–9. doi: 10.1002/pbc.20784
37. Rizik S, Hakim F, Bentur L, Arad-Cohen N, Kassis I. Bronchoscopy and Bronchoalveolar Lavage in the Diagnosis and Management of Pulmonary Infections in Immunocompromised Children. J Pediatr Hematol Oncol (2018) 40(7):532–5. doi: 10.1097/MPH.0000000000001283
38. Elbahlawan LM, Avent Y, Montoya L, Wilder K, Pei D, Cheng C, et al. Safety and Benefits of Bronchoalveolar Lavage and Lung Biopsy in the Management of Pulmonary Infiltrates in Children With Leukemia. J Pediatr Hematol Oncol (2016) 38(8):597–601. doi: 10.1097/MPH.0000000000000644
39. Efrati O, Sadeh-Gornik U, Modan-Moses D, Barak A, Szeinberg A, Vardi A, et al. Flexible Bronchoscopy and Bronchoalveolar Lavage in Pediatric Patients With Lung Disease. Pediatr Crit Care Med (2009) 10(1):80–4. doi: 10.1097/PCC.0b013e31819372ea
40. Rao U, Piccin A, Malone A, O’Hanlon K, Breatnach F, O’Meara A, et al. Utility of Bronchoalveolar Lavage in the Diagnosis of Pulmonary Infection in Children With Haematological Malignancies. Ir J Med Sci (2013) 182(2):177–83. doi: 10.1007/s11845-012-0852-3
Keywords: bronchoscopy, BAL, pediatric oncology, pediatric critical care, pediatric cancer
Citation: Ahmad AH, Brown BD, Andersen CR, Mahadeo KM, Petropolous D, Cortes JA, Razvi S, Gardner MK, Ewing LJ and Mejia RE (2021) Retrospective Review of Flexible Bronchoscopy in Pediatric Cancer Patients. Front. Oncol. 11:770523. doi: 10.3389/fonc.2021.770523
Received: 04 September 2021; Accepted: 12 November 2021;
Published: 14 December 2021.
Edited by:
Yong-mi Kim, Children’s Hospital of Los Angeles, United StatesReviewed by:
Pierre Goussard, Stellenbosch University, South AfricaCopyright © 2021 Ahmad, Brown, Andersen, Mahadeo, Petropolous, Cortes, Razvi, Gardner, Ewing and Mejia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rodrigo E. Mejia, cm1lamlhQG1kYW5kZXJzb24ub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.