
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 11 November 2021
Sec. Cancer Metabolism
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.762444
This article is part of the Research Topic Novel Insights into the Etiology, Mechanisms, and Treatment of Cancer Cachexia View all 6 articles
 Lara Pozzuto1†
Lara Pozzuto1† Marina Nogueira Silveira1†
Marina Nogueira Silveira1† Maria Carolina Santos Mendes1
Maria Carolina Santos Mendes1 Lígia Traldi Macedo1
Lígia Traldi Macedo1 Felipe Osório Costa1
Felipe Osório Costa1 Carlos Augusto Real Martinez2
Carlos Augusto Real Martinez2 Cláudio Saddy Rodrigues Coy2
Cláudio Saddy Rodrigues Coy2 Ademar Dantas da Cunha Júnior3,4
Ademar Dantas da Cunha Júnior3,4 José Barreto Campello Carvalheira1*
José Barreto Campello Carvalheira1*Body composition performed by computed tomography (CT) impacts on cancer patients’ prognoses and responses to treatment. Myosteatosis has been related to overall survival (OS) and disease-specific survival in colorectal cancer (CRC); however, the independent impact of the association of myosteatosis with prognosis in colon cancer (CC) and rectal cancer (RC) is still unclear. CT was performed at the L3 level to assess body composition features in 227 patients with CRC. Clinical parameters were collected. Overall survival (OS) was the primary outcome, and the secondary outcome was disease-free survival (DFS). Skeletal muscle attenuation and intramuscular adipose tissue area were associated with DFS (p = 0.003 and p = 0.011, respectively) and OS (p < 0.001 and p < 0.001, respectively) in CC patients but not in RC patients. Only the skeletal muscle area was associated with better prognosis related to OS in RC patients (p = 0.009). When CC and RC were analyzed separately, myosteatosis influenced survival negatively in CC patients, worsening DFS survival (hazard ratio [HR], 2.70; 95% confidence interval [CI], 1.07–6.82; p = 0.035) and OS (HR, 5.76; 95% CI, 1.31–25.40; p = 0.021). By contrast, the presence of myosteatosis did not influence DFS (HR, 1.02; 95% CI, 0.52–2.03; p = 0.944) or OS (HR, 0.76; 95% CI, 0.33–1.77; p = 0.529) in RC patients. Our study revealed the interference of myosteatosis in the therapy and survival of patients with CC but not in those with RC, strengthening the value of grouping the two types of cancer in body composition analyses.
Cancer is a condition that affects millions of people and is among the leading causes of death worldwide, with increasing number of cases each year. In 2020, the estimated number of new cases was 19.3 million, with a forecast of up to 30.2 million by 2040 (1). Colorectal cancer (CRC) is among the most incident types of the disease, occupying the third position of highest incidence in both sexes (1, 2).
Body composition impacts cancer patients’ prognosis, the response to treatment, and consequently, the survival of these individuals (3–5). Computed tomography (CT) is an effective and accurate method for identifying body features that may interfere with patient treatment and prognosis (3); indeed, CT scanning is the most suitable method for assessing body composition in cancer patients (6) to predict toxicity, tolerance to treatment, and survival (7, 8). One of the body composition features that can be identified through CT scan is loss of muscle tissue, which can be caused by reduced muscle fiber number and diameter as well as by fat infiltration and collagen deposit into the muscle (9, 10). Intramuscular fat invasion is known as myosteatosis and determines low muscle radiodensity on CT scan (4, 11); this feature can occur in patients with different body mass indexes (12). Importantly, myosteatosis is strongly related to shorter survival in certain cancer patients (5, 13, 14).
Relevant to oncological patients’ survival outcomes, myosteatosis in CRC is also related to patients’ disease-free survival (DFS) and overall survival (OS) (15–18); studies showed that this disorder is related to patients’ postoperative results and treatment (19–22). Notably, McSorley et al. identified that among the parameters of body composition by CT—sarcopenia, myosteatosis, and visceral obesity—only myosteatosis was associated with OS and disease-specific survival, but not independently of inflammatory parameters (15), indicating that the effects of covariables may strongly impact the influence of myosteatosis on survival outcomes. Along these lines, some studies do not take into consideration the cancer clinical stage (CS), generalizing the findings to varying times of the diseases and outcomes (23–25). Furthermore, body composition studies in non-metastatic CRC rarely distinguish colon cancer (CC) and rectal cancer (RC) (15–17, 21, 26).
Although CC and RC have similar pathophysiology, the chemotherapy and radiotherapy approaches for these entities are strikingly different. Therefore, the present study aimed to assess the association of myosteatosis in DFS and OS of patients with non-metastatic CC and RC and how this body composition feature may influence the patients’ therapy.
This retrospective–observational cohort involved patients diagnosed with non-metastatic CRC between January 2010 and December 2017 at the University of Campinas (UNICAMP University Hospital). Information was gathered from electronic or physical medical records from the diagnosis period until the last day of follow-up or death. Inclusion criteria were as follows: histologically confirmed CRC adenocarcinoma; patients submitted to curative-intent surgery; clinical stages (CS) I to III according to the 8th AJCC cancer manual (27); abdominal CT scans performed 3 months before or after the diagnosis and available electronically in the picture archiving and communication system; and availability of key clinical, demographic, and anthropometric data of interest. Patients diagnosed with cancer other than adenocarcinoma or primary cancer at other concomitant sites, patients for whom only low-quality CT was available or contrast CT was unavailable, those in stage IV, those for whom treatment data were not reported, and those with CRC in situ were excluded. The local Institutional Review Board approved this study (CAAE number: 84469318.2.0000.5404), as principles recommended by the Declaration of Helsinki have been respected and obtained a waiver for the consent form.
Computed tomography images were evaluated to obtain the patients’ body composition. CT images were routinely performed for cancer staging, collected weight and height data, and calculated BMI. The images were analyzed using the software viewer Software SliceOMatic V.5.0 (TomoVision, Canada). The standard Hounsfield units (HU) settled for tissues were −29 to 150 for skeletal muscle (SM), −150 to −50 for visceral adipose tissue (VAT), and −190 to –30 for intramuscular adipose tissue (IMAT) and subcutaneous adipose tissue (SAT). Skeletal muscle groups evaluated include the psoas, abdominal, rectus abdominal, and paravertebral muscles (6, 28). Skeletal muscle and subcutaneous or visceral adipose tissue were measured in units of square centimeters (cm²) and normalized for height in square meters (m²) and reported as SM index (SMI), SAT index (SFI), and VAT index (VFI) in cm²/m² units. SM density was measured as the mean radiological tissue attenuation in HU (29, 30). Myosteatosis in patients was determined with cutoff points of <41 HU for patients with BMI ≤24.9 and <33 HU for those with BMI ≥25, according to Martin et al. (12). Two consecutive images of the third lumbar vertebra were acquired, and the image analyzes were performed by two independent evaluators (MS and LP), who were blind to the outcomes under study. Coefficients of variation for the cross-sectional areas analyzed were 1.07%, 1.05%, 1.61%, and 3.57% for SM and SAT, VAT, and IMAT, respectively, and 1.60% for SM density.
Data were retrospectively collected from medical records and entered into the electronic tool REDCap hosted at the University of Campinas (31). Clinical parameters collected included age, sex, BMI, weight loss (less than 5% or more than 5% of the original weight), alcoholism, smoking, Charlson Comorbidity Index, tumor stage, emergency surgery neoadjuvant and adjuvant therapy, biochemical tests, and toxicity data during treatment (according to NCI CTCAE version 5.0) (32).
The primary outcome was overall survival (OS), calculated between the time of diagnosis, and death from any cause. The secondary outcome was disease-free survival (DFS), calculated between the time of diagnosis and disease progression or death from CRC. The date of death was determined from the death certificate’s date attached to the medical record or from information obtained by telephone contact with family members. Living patients were censored on the date of the last follow-up.
Categorical variables were analyzed using χ2 or Fisher’s exact test, when appropriate, and Student’s t-test for continuous variables, presented in the baseline table and the table with characteristics according to the patients’ chemotherapy treatment. Kaplan–Meier curves were created to evaluate the effect of myosteatosis on the survival of patients with CRC, CR, and CC, and the differences between the curves were assessed using log-rank tests. Obtaining hazard ratios (HR) and respective confidence intervals (CI), proportional risk models were performed using Cox regression with 95% CI for disease-free survival and overall survival. In the multivariate analysis, variables with p <0.1 identified in the univariate were used, and adjustments were made in Cox’s multivariate regression analysis for age, Charlson Comorbidity Index (CCI) (33), alcohol consumption, and AJCC stage. Kaplan–Meier curves were created to evaluate the effect of myosteatosis on the survival of patients with CRC, CR, and CC, and the differences between the curves were assessed using log-rank tests. Statistical significance was determined with a two-sided p-value <0.05, and the software used for the analyses was Stata, version 12.0 (StataCorp LP, College Station, United States).
The study cohort included 227 CRC patients, 118 with colon cancer (CC), and 109 with rectal cancer (RC) (Figure 1). Six hundred and four patients were treated for stage I–III CRC, between 2009 and 2017, in our data collection. Of these, 288 patients had CT available for analysis. Patients with missing treatment information (n = 5), lacking CT either at the established time (n = 23) or without contrast (n = 32), and in situ CRC (n = 1) were excluded.
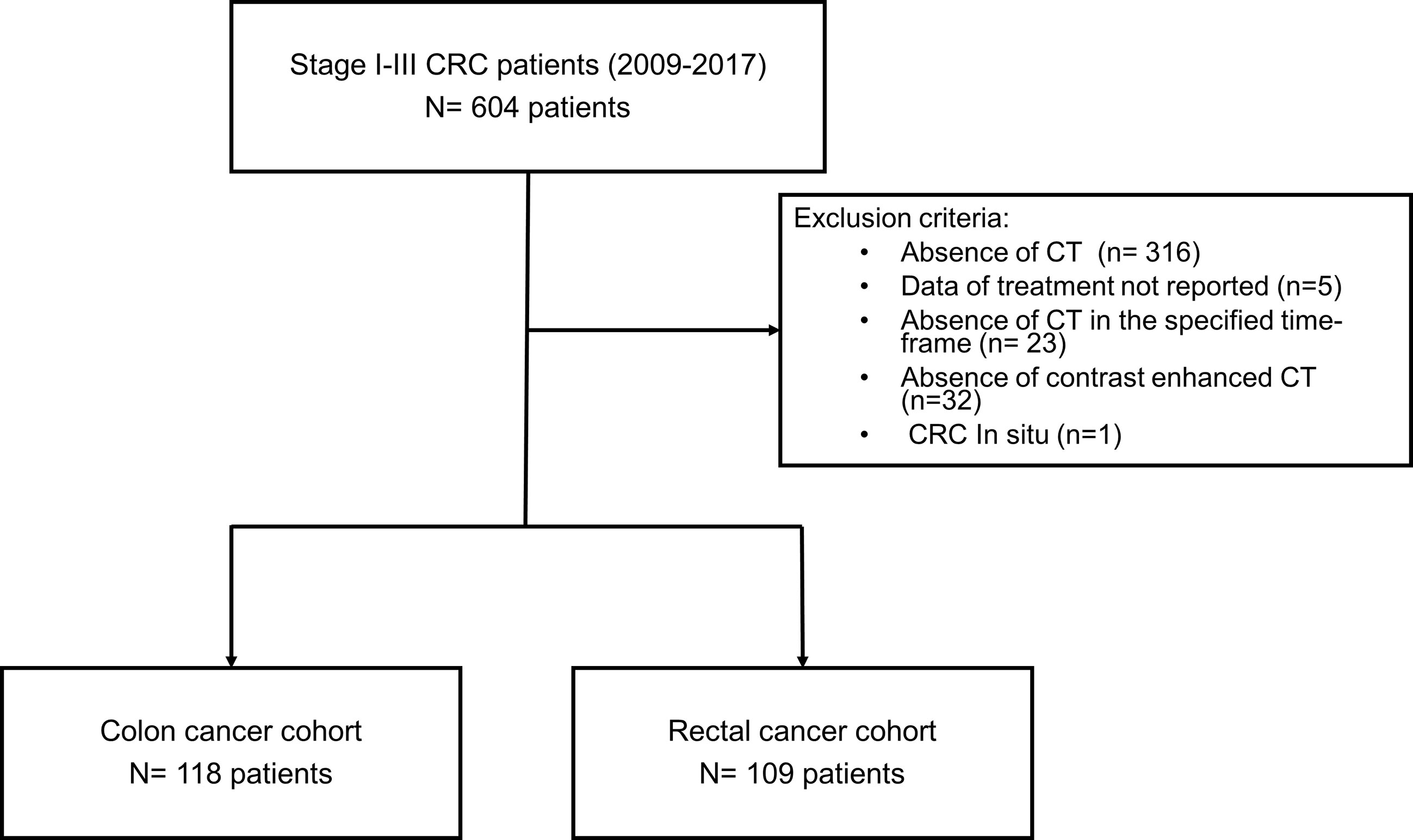
Figure 1 Flow chart showing the inclusion and exclusion process for patients treated for CRC stage I-III.
The clinical and demographic characteristics of the patients, according to the presence of myosteatosis, are described in Table 1 for CC and RC patients. For CC, most patients had less than 65 years, while most significant RC patients with myosteatosis had more than 65 years. Still, myosteatosis was more prevalent in patients older than 65 years in both colon and rectal cancer. CC or RC patients with myosteatosis had the worst Charlson Comorbidity Index.
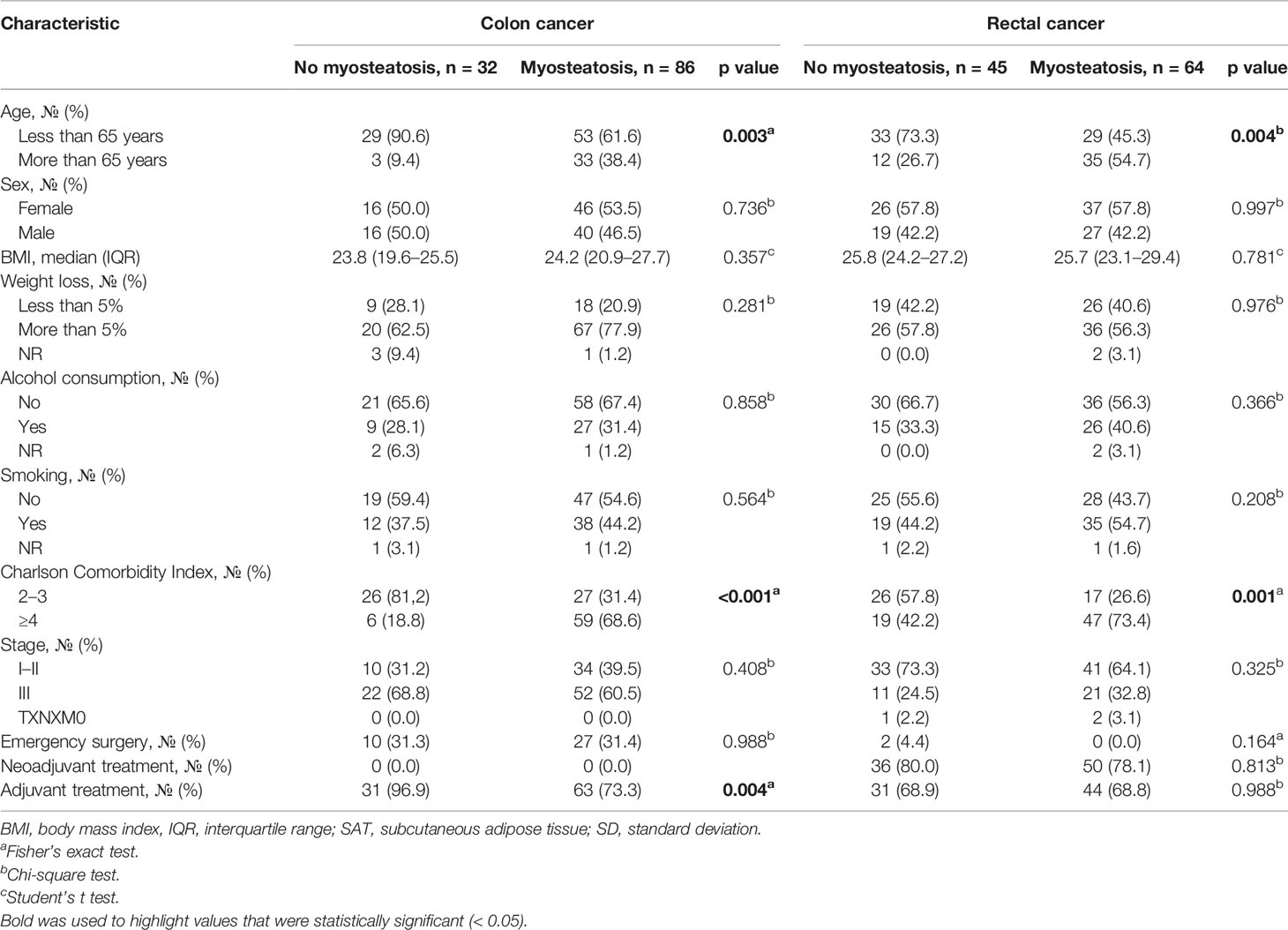
Table 1 Selected demographic and disease characteristics according to myosteatosis of stage I–III colon and rectal cancer patients.
Emergency surgery was performed on 39 (17%) patients, 86 (38%) had neoadjuvant therapy, and 169 (74%) had adjuvant treatment. Interestingly, 97% of patients with CC without myosteatosis were able to undergo adjuvant treatment, while significantly fewer patients undergo adjuvant therapy in the presence of myosteatosis (Table 1).
Among CC patients, just men with myosteatosis showed significant reduction in skeletal muscle area (p = 0.020) and SMI (p = 0.037). On the other hand, all patients with myosteatosis showed significantly larger IMAT area (p < 0.001). Regarding inflammatory parameters, myosteatosis was associated with lower LMR indices (p = 0.013) and higher PLR indices (p = 0.003) (Supplementary Table 1). As for patients with rectal cancer, in contrast, in both males and females, myosteatosis was related to minor skeletal muscle and SMI areas and larger IMAT areas. Besides, myosteatosis was related to higher VAT and VATI areas and SAT attenuation (Supplementary Table 2).
Body composition features associate differently in CC or RC patients. Skeletal muscle attenuation and intramuscular adipose tissue area were associated with disease-free survival and overall survival in CC patients, but not with RC patients. Only SM areas were associated with better prognosis related to OS in RC patients (Tables 2 and 3). Kaplan–Meier curves show that myosteatosis influences survival negatively in CC patients, worsening disease-free survival (hazard ratio [HR], 2.70; 95% confidence interval [CI], 1.07–6.82; p = 0.035) and overall survival (HR, 5.76; 95% CI, 1.31–25.40; p = 0.021) (Figures 2A, B). In opposite, the presence of myosteatosis did not influence DFS (HR, 1.02; 95% CI, 0.52–2.03; p = 0.944) or OS (HR, 0.76; 95% CI, 0.33–1.77; p = 0.529) in RC patients (Figures 3A, B).
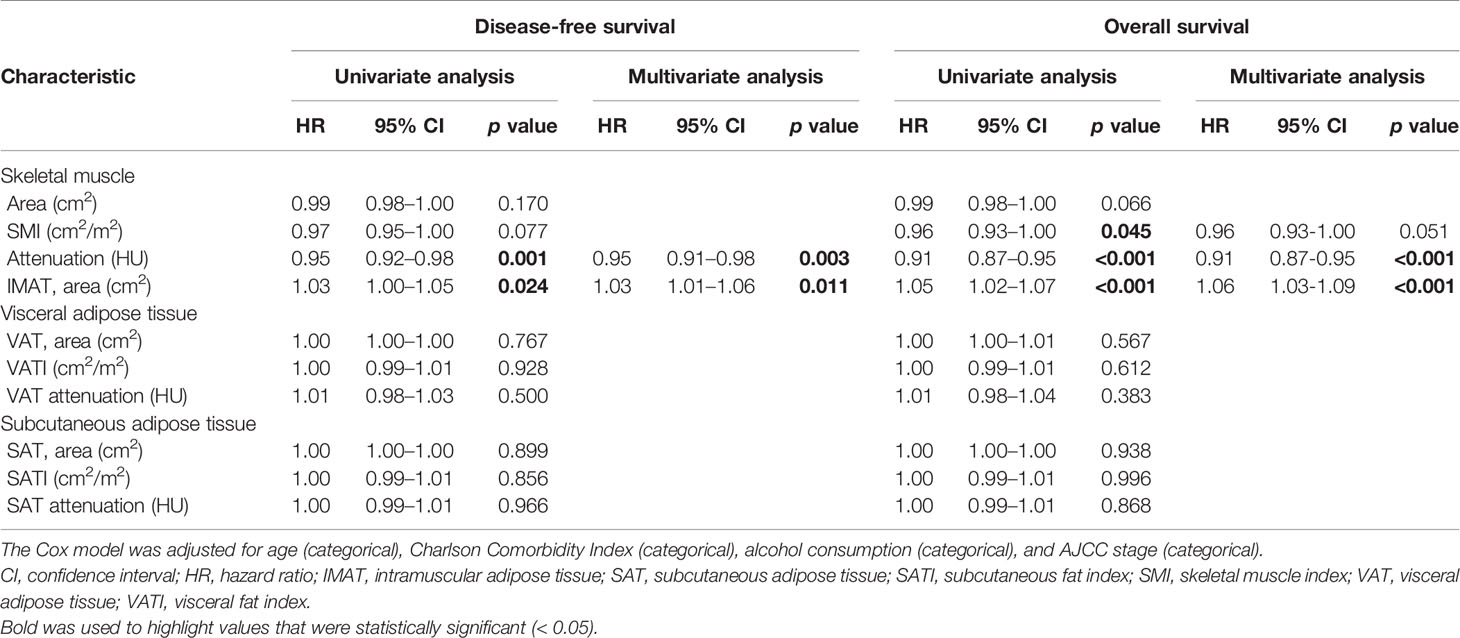
Table 2 Univariate and multivariate COX regression analyses of body composition features of colon cancer patients.
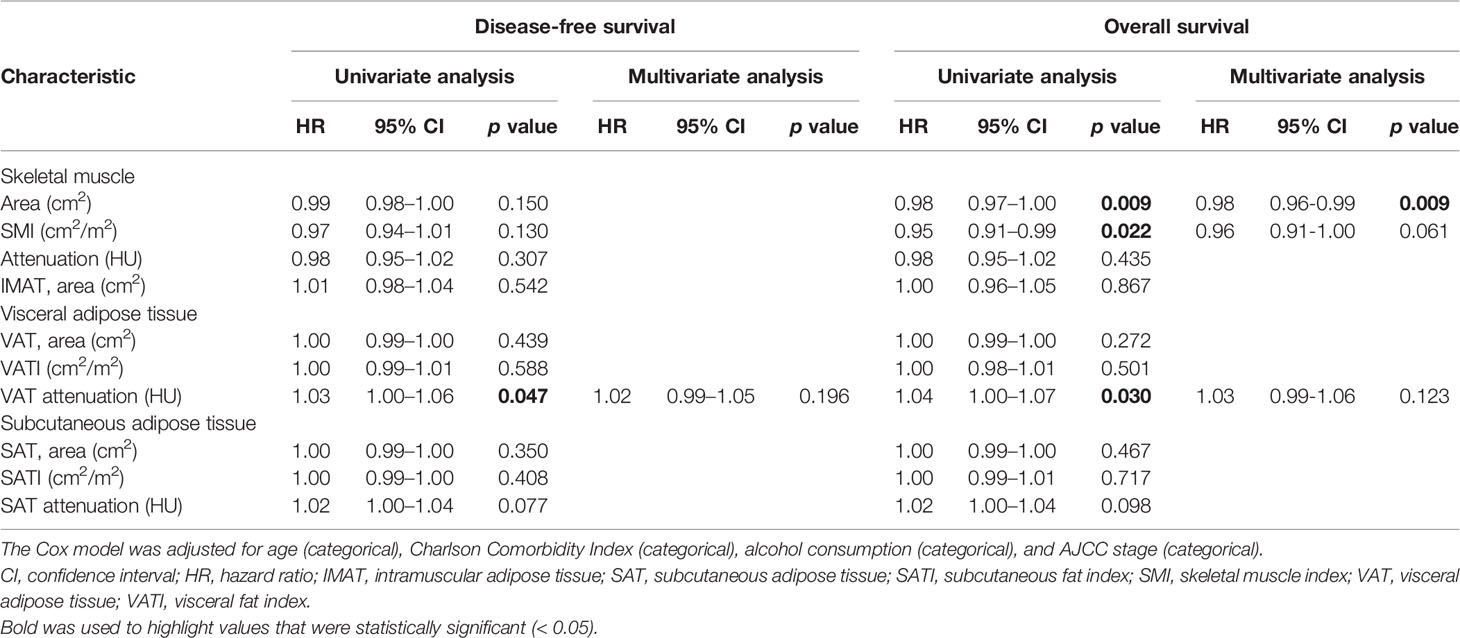
Table 3 Univariate and multivariate COX regression analyses of body composition features of rectal cancer patients.
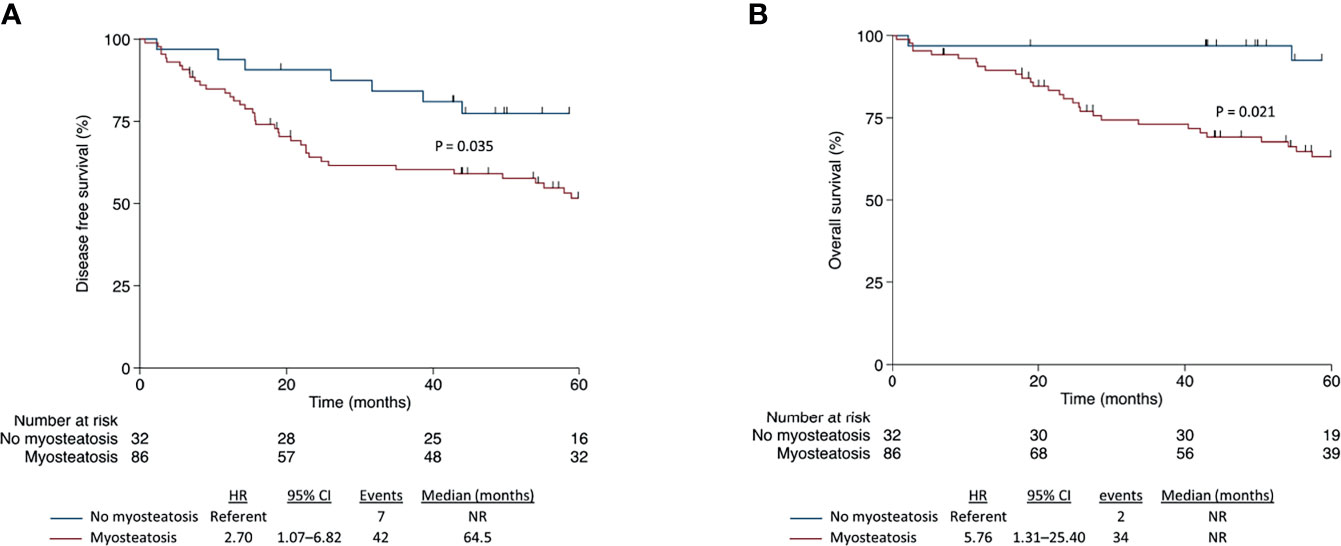
Figure 2 Disease-free survival (A) and overall survival (B) according to myosteatosis in patients with colon cancer.
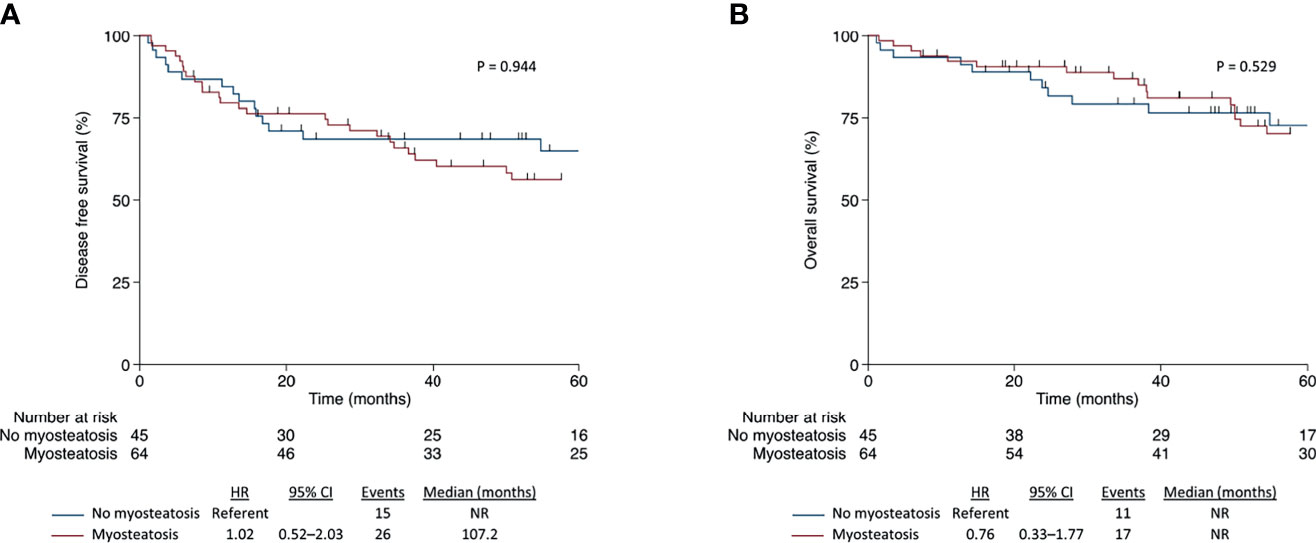
Figure 3 Disease-free survival (A) and overall survival (B) according to myosteatosis in patients with rectal cancer.
Interestingly, we identified that myosteatosis in patients with CC was significantly related to the type of chemotherapy and adjuvant treatment duration. Specifically, fewer patients with CC and myosteatosis were exposed to oxaliplatin, and 55.6% of these patients completed adjuvant regimen, while 80.7% of CC patients without myosteatosis received the preplanned adjuvant treatment (p = 0.031). The presence of myosteatosis affected chemotherapy tolerance predominantly by increasing toxicity-related treatment interruption (p = 0.005). In RC, on the other hand, no statistically significant difference was found between myosteatosis and treatment tolerance, highlighting the differences between patients with CC and those with RC (Table 4).
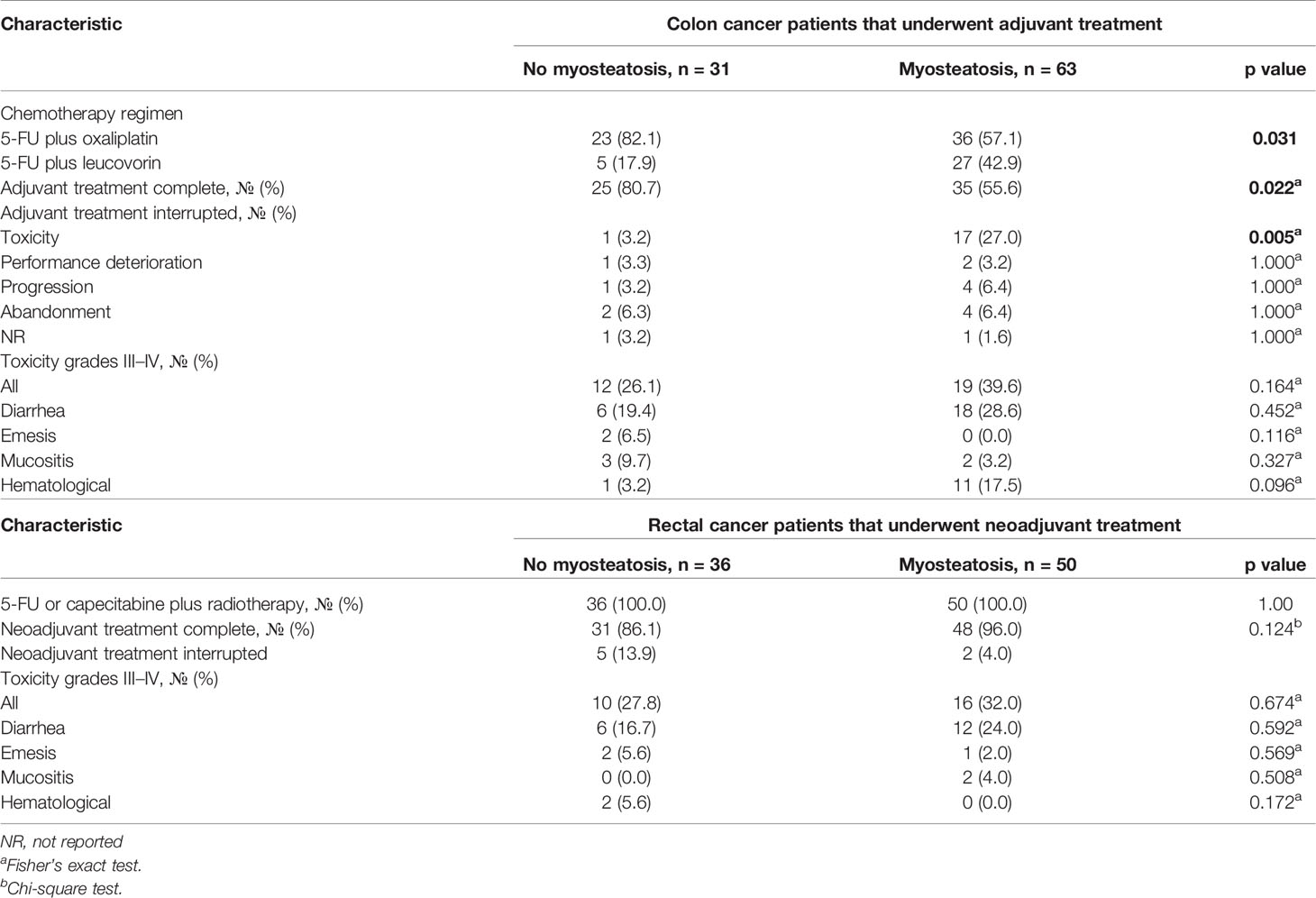
Table 4 Selected adjuvant and neoadjuvant treatment characteristics according to myosteatosis of stage I–III colon and rectal cancer patients, respectively.
Myosteatosis in CC is associated with worse DFS and OS even after adjustments for age, CCI, alcoholism, and CS. In opposite, we did not detect that myosteatosis affected the survival outcomes in the entire population (CRC) or in RC alone. In accordance, myosteatosis prevented the completion rate of adjuvant chemotherapy in CC patients. On the other hand, we did not identify an association between myosteatosis and the completion rate of neoadjuvant systemic chemotherapy (NSC) to RC patients.
Myosteatosis is a factor that negatively affects survival (14, 34–36), and it is associated with increased chemotherapy toxicity (36–38) as well as with increased hospital readmissions due to postoperative complications (13, 22). Our findings extend these data by showing that myosteatosis prevented patients with CC from receiving the entire preplanned adjuvant chemotherapy regimen. In contrast, myosteatosis did not influence the NSC administration in RC patients. Interestingly, in a recent Latin-American-based study with non-metastatic CRC, body composition was not associated with survival outcomes (26), which corroborates the present results in the entire cohort. In aggregate, these data suggest that myosteatosis is a marker of postoperative frailty, which detects patients who performed worse during surgery and thus were unable to complete or even start adjuvant therapy, therefore jeopardizing the opportunity to offer patients a more satisfying quality of life and more prolonged survival.
Although CC and RC have different characteristics about the clinical management, treatment, and outcomes of each disease (25, 39, 40), our study is the first to systematically investigate the effect of myosteatosis on CC and RC separately. Saliently, for patients with stage III CC, adjuvant chemotherapy with fluoropyrimidine combined with oxaliplatin diminishes the risk of relapse and mortality, with a therapy duration that might be abbreviated to 3 months as effective as 6 months, particularly in the lower-risk subgroup and in specific conditions according to limit toxicities, such as sensitive neuropathy or thrombocytopenia (41). Recognizing the visible cost and disability to patients results in surgical complications; current investigations have concentrated on distinguishing modifiable biomarkers to advance perioperative risk stratification and purpose supportive management. We identified that myosteatosis in patients with CC was significantly related to the type of chemotherapy and adjuvant treatment duration. Moreover, the presence of myosteatosis affected chemotherapy tolerance predominantly by increasing toxicity-related treatment interruption. Therefore, the present data suggest that myosteatosis could be a biomarker associated with toxicity, which might be assessed previously to chemotherapy protocol in CC patients. In RC, in contrast, no statistically significant difference was observed between myosteatosis and treatment tolerance, indicating the treatment approach diversity between patients with CC and RC.
The reasons for the different impacts of myosteatosis on CC, RC DFS, and OS are not entirely clear. However, it is essential to observe that the differences between the two tissues begin in their embryonic origin, which generates differences in the local blood flow supply, different metabolic pathways, and consequently differences in tumor development (42). Colon and rectal cancers have different molecular patterns and differentiation profiles; tumor size, malignancy, and the T extension of the invasion are distinct (43–51). Such differences impact cancer treatment, therapy choice, response to therapy, and survival. While neoadjuvant chemotherapy’s efficacy is still under investigation for colon cancer (52), its use has been well established to treat rectal cancer and our negative findings might underline the importance of myosteatosis as a postoperative biomarker for CC using adjuvant chemotherapy. NSC approaches are considered standard of care in numerous other gastrointestinal tumor types such as gastric, esophageal, and pancreatic cancer (53–55), also in RC (56). Interestingly, in a previous study we also did not find a shorter survival in locally advanced esophageal cancer patients with myosteatosis that were not submitted to surgery, reinforcing the idea of myosteatosis as a marker of postoperative frailty (57). Moreover, the benefit of neoadjuvant chemotherapy regimens may be related to increased completion rate of subsequent treatments (58); thus, further studies evaluating myosteatosis as a marker for anticipating the use of chemotherapy in neoadjuvant, instead of in adjuvant setting, is warranted.
In the context of metastatic CRC (mCRC), low muscularity was associated with shorter DFS and OS in most studies (18, 59). However, some studies have not found an effect of sarcopenia at diagnosis on mCRC prognosis, despite the detection of a negative influence in OS caused by muscle mass loss during the chemotherapy period (60, 61). Regarding myosteatosis, the results are also controversial. Myosteatosis is associated with a worse prognosis in patients with mCRC in certain studies (18, 59); others do not find an association (60). Notably, we did not notice any study that assessed CC and CR separately in the metastatic context.
Our study presents key strengths, with a rigorous sample as to the selection and analysis of the CRC. We recognize some limitations in our study which are the retrospective design, the sample number, and the possibility of sealing bias due to the loss of cases due to the lack of CT. Furthermore, we did not have data on dietary intake, physical activity, socioeconomic status, and perioperative care support, which could reasonably have affected SMI, SMD, and outcomes. Therefore, further prospective studies are needed to confirm our findings.
Our study clearly showed the interference of myosteatosis in the treatment and survival of patients with CC, but not in RC, reinforcing the importance of separating the two types of cancer in body composition studies. In addition, myosteatosis in the postsurgical recovery negatively affected for non-indication of adjuvant therapy and contributed to the striking difference we found between CC and CR.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Comitê de Ética em Pesquisa (CEP) da Universidade Estadual de Campinas. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Conceptualization, LP, MS, MM, and JC. Data curation, MS, MM, and JC. Formal analysis, LP, MS, MM, and JC. Funding acquisition, JC. Methodology, LP, MS, and MM. Project administration, JC. Resources, JC. Supervision, MM and JC. Visualization, MS, LM, FC, CM, CC, and AC. Writing—original draft, LP, MS, MM, FC, and AC. Writing—review and editing, LP, MS, MM, LM, CM, CC, AC, and JC. All authors contributed to the article and approved the submitted version.
This research was funded by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), grant number 2018/23428-0.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Sandra Regina Branbilla for administrative and technical support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.762444/full#supplementary-material
1. Wild CP, Weiderpass E, BW S. World Cancer Report: Cancer Research for Cancer Prevention. IARC L, editor. France: International Agency for Research on Cancer (IARC) (2020).
2. Ministério da Saúde - Instituto Nacional de Câncer José Alencar Gomes da Silva. Síntese De Resultados E Comentários. In: Estimativa 2020. Incidência de Câncer no Brasil. Rio de Janeiro (RJ: INCA (2019). p. 33–52.
3. Gibson DJ, Burden ST, Strauss BJ, Todd C, Lal S. The Role of Computed Tomography in Evaluating Body Composition and the Influence of Reduced Muscle Mass on Clinical Outcome in Abdominal Malignancy: A Systematic Review. Eur J Clin Nutr (2015) 69(10):1079–86. doi: 10.1038/ejcn.2015.32
4. Aleixo GFP, Shachar SS, Nyrop KA, Muss HB, Malpica L, Williams GR. Myosteatosis and Prognosis in Cancer: Systematic Review and Meta-Analysis. Crit Rev Oncol Hematol (2020) 145:102839. doi: 10.1016/j.critrevonc.2019.102839
5. Lee CM, Kang J. Prognostic Impact of Myosteatosis in Patients With Colorectal Cancer: A Systematic Review and Meta-Analysis. J Cachexia Sarcopenia Muscle (2020) 11(5):1270–82. doi: 10.1002/jcsm.12575
6. Mourtzakis M, Prado CM, Lieffers JR, Reiman T, McCargar LJ, Baracos VE. A Practical and Precise Approach to Quantification of Body Composition in Cancer Patients Using Computed Tomography Images Acquired During Routine Care. Appl Physiol Nutr Metab (2008) 33(5):997–1006. doi: 10.1139/H08-075
7. Almasaudi AS, Dolan RD, McSorley ST, Horgan PG, Edwards C, McMillan DC. Relationship Between Computed Tomography-Derived Body Composition, Sex, and Post-Operative Complications in Patients With Colorectal Cancer. Eur J Clin Nutr (2019) 73:1450–57. doi: 10.1038/s41430-019-0414-0
8. Cushen SJ, Power DG, Teo MY, MacEneaney P, Maher MM, McDermott R, et al. Body Composition by Computed Tomography as a Predictor of Toxicity in Patients With Renal Cell Carcinoma Treated With Sunitinib. Am J Clin Oncol (2017) 40(1):47–52. doi: 10.1097/coc.0000000000000061
9. Delmonico MJ, Harris TB, Lee JS, Visser M, Nevitt M, Kritchevsky SB, et al. Alternative Definitions of Sarcopenia, Lower Extremity Performance, and Functional Impairment With Aging in Older Men and Women. J Am Geriatr Soc (2007) 55(5):769–74. doi: 10.1111/j.1532-5415.2007.01140.x
10. Martin A, Freyssenet D. Phenotypic Features of Cancer Cachexia-Related Loss of Skeletal Muscle Mass and Function: Lessons From Human and Animal Studies. J Cachexia Sarcopenia Muscle (2021) 12(2):252–73. doi: 10.1002/jcsm.12678
11. Addison O, Marcus RL, Lastayo PC, Ryan AS. Intermuscular Fat: A Review of the Consequences and Causes. Int J Endocrinol (2014) 2014:309570. doi: 10.1155/2014/309570
12. Martin L, Birdsell L, Macdonald N, Reiman T, Clandinin MT, McCargar LJ, et al. Cancer Cachexia in the Age of Obesity: Skeletal Muscle Depletion Is a Powerful Prognostic Factor, Independent of Body Mass Index. J Clin Oncol (2013) 31(12):1539–47. doi: 10.1200/JCO.2012.45.2722
13. Martin L, Gioulbasanis I, Senesse P, Baracos VE. Cancer-Associated Malnutrition and CT-Defined Sarcopenia and Myosteatosis Are Endemic in Overweight and Obese Patients. JPEN J Parenter Enteral Nutr (2020) 44(2):227–38. doi: 10.1002/jpen.1597
14. Findlay M, Brown C, De Abreu Lourenço R, White K, Bauer J. Sarcopenia and Myosteatosis in Patients Undergoing Curative Radiotherapy for Head and Neck Cancer: Impact on Survival, Treatment Completion, Hospital Admission and Cost. J Hum Nutr Diet (2020) 33:811–21. doi: 10.1111/jhn.12788
15. McSorley ST, Black DH, Horgan PG, McMillan DC. The Relationship Between Tumour Stage, Systemic Inflammation, Body Composition and Survival in Patients With Colorectal Cancer. Clin Nutr (2017) 37(4):1279–85. doi: 10.1016/j.clnu.2017.05.017
16. Hopkins JJ, Reif RL, Bigam DL, Baracos VE, Eurich DT, Sawyer MB. The Impact of Muscle and Adipose Tissue on Long-Term Survival in Patients With Stage I to III Colorectal Cancer. Dis Colon Rectum (2019) 62(5):549–60. doi: 10.1097/DCR.0000000000001352
17. Aro R, Mäkäräinen-Uhlbäck E, Ämmälä N, Rautio T, Ohtonen P, Saarnio J, et al. The Impact of Sarcopenia and Myosteatosis on Postoperative Outcomes and 5-Year Survival in Curatively Operated Colorectal Cancer Patients - A Retrospective Register Study. Eur J Surg Oncol (2020) 46(9):1656–62. doi: 10.1016/j.ejso.2020.03.206
18. Cunha LPD, Silveira MN, Mendes MCS, Costa FO, Macedo LT, Siqueira NDSD, et al. Sarcopenia as an Independent Prognostic Factor in Patients With Metastatic Colorectal Cancer: A Retrospective Evaluation. Clin Nutr ESPEN (2019) 32:107–12. doi: 10.1016/j.clnesp.2019.04.004
19. Malietzis G, Currie AC, Athanasiou T, Johns N, Anyamene N, Glynne-Jones R, et al. Influence of Body Composition Profile on Outcomes Following Colorectal Cancer Surgery. Br J Surg (2016) 103(5):572–80. doi: 10.1002/bjs.10075
20. Prado CM, Baracos VE, McCargar LJ, Mourtzakis M, Mulder KE, Reiman T, et al. Body Composition as an Independent Determinant of 5-Fluorouracil-Based Chemotherapy Toxicity. Clin Cancer Res (2007) 13(11):3264–8. doi: 10.1158/1078-0432.ccr-06-3067
21. Malietzis G, Johns N, Al-Hassi HO, Knight SC, Kennedy RH, Fearon KC, et al. Low Muscularity and Myosteatosis Is Related to the Host Systemic Inflammatory Response in Patients Undergoing Surgery for Colorectal Cancer. Ann Surg (2016) 263(2):320–5. doi: 10.1097/SLA.0000000000001113
22. Xiao J, Caan BJ, Cespedes Feliciano EM, Meyerhardt JA, Peng PD, Baracos VE, et al. Association of Low Muscle Mass and Low Muscle Radiodensity With Morbidity and Mortality for Colon Cancer Surgery. JAMA Surg (2020) 155(10):942–9. doi: 10.1001/jamasurg.2020.2497
23. Giani A, Famularo S, Riva L, Tamini N, Ippolito D, Nespoli L, et al. Association Between Specific Presurgical Anthropometric Indexes and Morbidity in Patients Undergoing Rectal Cancer Resection. Nutrition (2020) 75-76:110779. doi: 10.1016/j.nut.2020.110779
24. Heus C, Bakker N, Verduin WM, Doodeman HJ, Houdijk APJ. Impact of Body Composition on Surgical Outcome in Rectal Cancer Patients, a Retrospective Cohort Study. World J Surg (2019) 43(5):1370–6. doi: 10.1007/s00268-019-04925-z
25. Boer BC, de Graaff F, Brusse-Keizer M, Bouman DE, Slump CH, Slee-Valentijn M, et al. Skeletal Muscle Mass and Quality as Risk Factors for Postoperative Outcome After Open Colon Resection for Cancer. Int J Colorectal Dis (2016) 31(6):1117–24. doi: 10.1007/s00384-016-2538-1
26. Cárcamo L, Peñailillo E, Bellolio F, Miguieles R, Urrejola G, Zúñiga A, et al. Computed Tomography-Measured Body Composition Parameters Do Not Influence Survival in Non-Metastatic Colorectal Cancer. ANZ J Surg (2021) 91:E298–306. doi: 10.1111/ans.16708
27. Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to Build a Bridge From a Population-Based to a More "Personalized" Approach to Cancer Staging. CA Cancer J Clin (2017) 67(2):93–9. doi: 10.3322/caac.21388
28. Mitsiopoulos N, Baumgartner RN, Heymsfield SB, Lyons W, Gallagher D, Ross R. Cadaver Validation of Skeletal Muscle Measurement by Magnetic Resonance Imaging and Computerized Tomography. J Appl Physiol (1985) (1998) 85(1):115–22. doi: 10.1152/jappl.1998.85.1.115
29. Heymsfield SB, Wang Z, Baumgartner RN, Ross R. Human Body Composition: Advances in Models and Methods. Annu Rev Nutr (1997) 17:527–58. doi: 10.1146/annurev.nutr.17.1.527
30. Heymsfield SB, Smith R, Aulet M, Bensen B, Lichtman S, Wang J, et al. Appendicular Skeletal Muscle Mass: Measurement by Dual-Photon Absorptiometry. Am J Clin Nutr (1990) 52(2):214–8. doi: 10.1093/ajcn/52.2.214
31. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J BioMed Inform (2019) 95:103208. doi: 10.1016/j.jbi.2019.103208
32. SERVICES, U.S.D.O.H.A.H. Common Terminology Criteria for Adverse Events (CTCAE) V5.0. Rockville: N.C.I. National Institutes of Health (2017). Available at: https://ctep.cancer.gov/.
33. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J Chronic Dis (1987) 40(5):373–83. doi: 10.1016/0021-9681(87)90171-8
34. Sueda T, Takahasi H, Nishimura J, Hata T, Matsuda C, Mizushima T, et al. Impact of Low Muscularity and Myosteatosis on Long-Term Outcome After Curative Colorectal Cancer Surgery: A Propensity Score-Matched Analysis. Dis Colon Rectum (2018) 61(3):364–74. doi: 10.1097/dcr.0000000000000958
35. Srpcic M, Jordan T, Popuri K, Sok M. Sarcopenia and Myosteatosis at Presentation Adversely Affect Survival After Esophagectomy for Esophageal Cancer. Radiol Oncol (2020) 54(2):237–46. doi: 10.2478/raon-2020-0016
36. Murnane LC, Forsyth AK, Koukounaras J, Pilgrim CH, Shaw K, Brown WA, et al. Myosteatosis Predicts Higher Complications and Reduced Overall Survival Following Radical Oesophageal and Gastric Cancer Surgery. Eur J Surg Oncol (2021) 47(9):2295–303. doi: 10.1016/j.ejso.2021.02.008
37. Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, et al. Chemoradiotherapy After Surgery Compared With Surgery Alone for Adenocarcinoma of the Stomach or Gastroesophageal Junction. N Engl J Med (2001) 345(10):725–30. doi: 10.1056/NEJMoa010187
38. Dijksterhuis WPM, Pruijt MJ, van der Woude SO, Klaassen R, Kurk SA, van Oijen MGH, et al. Association Between Body Composition, Survival, and Toxicity in Advanced Esophagogastric Cancer Patients Receiving Palliative Chemotherapy. J Cachexia Sarcopenia Muscle (2019) 10(1):199–206. doi: 10.1002/jcsm.12371
39. Cercek A, Roxburgh CSD, Strombom P, Smith JJ, Temple LKF, Nash GM, et al. Adoption of Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer. JAMA Oncol (2018) 4(6):e180071. doi: 10.1001/jamaoncol.2018.0071
40. Cunningham D, Atkin W, Lenz HJ, Lynch HT, Minsky B, Nordlinger B, et al. Colorectal Cancer. Lancet (2010) 375(9719):1030–47. doi: 10.1016/s0140-6736(10)60353-4
41. Grothey A, Sobrero AF, Shields AF, Yoshino T, Paul J, Taieb J, et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N Engl J Med (2018) 378(13):1177–88. doi: 10.1056/NEJMoa1713709
42. Pocard M, Salmon RJ, Muleris M, Remvikos Y, Bara J, Dutrillaux B, et al. [Two Colons–Two Cancers? Proximal or Distal Adenocarcinoma: Arguments for a Different Carcinogenesis]. Bull Cancer (1995) 82(1):10–21.
43. Labianca R, Nordlinger B, Beretta GD, Mosconi S, Mandala M, Cervantes A, et al. Early Colon Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol (2013) 24(Suppl 6):vi64–72. doi: 10.1093/annonc/mdt354
44. Flemer B, Lynch DB, Brown JM, Jeffery IB, Ryan FJ, Claesson MJ, et al. Tumour-Associated and Non-Tumour-Associated Microbiota in Colorectal Cancer. Gut (2017) 66(4):633–43. doi: 10.1136/gutjnl-2015-309595
45. Thomas LA, Veysey MJ, French G, Hylemon PB, Murphy GM, Dowling RH. Bile Acid Metabolism by Fresh Human Colonic Contents: A Comparison of Caecal Versus Faecal Samples. Gut (2001) 49(6):835–42. doi: 10.1136/gut.49.6.835
46. Benedix F, Kube R, Meyer F, Schmidt U, Gastinger I, Lippert H, et al. Comparison of 17,641 Patients With Right- and Left-Sided Colon Cancer: Differences in Epidemiology, Perioperative Course, Histology, and Survival. Dis Colon Rectum (2010) 53(1):57–64. doi: 10.1007/DCR.0b013e3181c703a4
47. Gonzalez EC, Roetzheim RG, Ferrante JM, Campbell R. Predictors of Proximal vs. Distal Colorectal Cancers. Dis Colon Rectum (2001) 44(2):251–8. doi: 10.1007/BF02234301
48. Meguid RA, Slidell MB, Wolfgang CL, Chang DC, Ahuja N. Is There a Difference in Survival Between Right- Versus Left-Sided Colon Cancers? Ann Surg Oncol (2008) 15(9):2388–94. doi: 10.1245/s10434-008-0015-y
49. Gao XH, Yu GY, Gong HF, Liu LJ, Xu Y, Hao LQ, et al. Differences of Protein Expression Profiles, KRAS and BRAF Mutation, and Prognosis in Right-Sided Colon, Left-Sided Colon and Rectal Cancer. Sci Rep (2017) 7(1):7882. doi: 10.1038/s41598-017-08413-z
50. Yamauchi M, Morikawa T, Kuchiba A, Imamura Y, Qian ZR, Nishihara R, et al. Assessment of Colorectal Cancer Molecular Features Along Bowel Subsites Challenges the Conception of Distinct Dichotomy of Proximal Versus Distal Colorectum. Gut (2012) 61(6):847–54. doi: 10.1136/gutjnl-2011-300865
51. Minoo P, Zlobec I, Peterson M, Terracciano L, Lugli A. Characterization of Rectal, Proximal and Distal Colon Cancers Based on Clinicopathological, Molecular and Protein Profiles. Int J Oncol (2010) 37(3):707–18. doi: 10.3892/ijo_00000720
52. Cheong CK, Nistala KRY, Ng CH, Syn N, Chang HSY, Sundar R, et al. Neoadjuvant Therapy in Locally Advanced Colon Cancer: A Meta-Analysis and Systematic Review. J Gastrointest Oncol (2020) 11(5):847–57. doi: 10.21037/jgo-20-220
53. Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, et al. Perioperative Chemotherapy With Fluorouracil Plus Leucovorin, Oxaliplatin, and Docetaxel Versus Fluorouracil or Capecitabine Plus Cisplatin and Epirubicin for Locally Advanced, Resectable Gastric or Gastro-Oesophageal Junction Adenocarcinoma (FLOT4): A Randomised, Phase 2/3 Trial. Lancet (2019) 393(10184):1948–57. doi: 10.1016/S0140-6736(18)32557-1
54. van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, et al. Preoperative Chemoradiotherapy for Esophageal or Junctional Cancer. N Engl J Med (2012) 366(22):2074–84. doi: 10.1056/NEJMoa1112088
55. Rangarajan K, Pucher PH, Armstrong T, Bateman A, Hamady Z. Systemic Neoadjuvant Chemotherapy in Modern Pancreatic Cancer Treatment: A Systematic Review and Meta-Analysis. Ann R Coll Surg Engl (2019) 101(7):453–62. doi: 10.1308/rcsann.2019.0060
56. Sauer R, Liersch T, Merkel S, Fietkau R, Hohenberger W, Hess C, et al. Preoperative Versus Postoperative Chemoradiotherapy for Locally Advanced Rectal Cancer: Results of the German CAO/ARO/AIO-94 Randomized Phase III Trial After a Median Follow-Up of 11 Years. J Clin Oncol (2012) 30(16):1926–33. doi: 10.1200/JCO.2011.40.1836
57. Gabiatti CTB, Martins MCL, Miyazaki DL, Silva LP, Lascala F, Macedo LT, et al. Myosteatosis in a Systemic Inflammation-Dependent Manner Predicts Favorable Survival Outcomes in Locally Advanced Esophageal Cancer. Cancer Med (2019) 8(16):6967–76. doi: 10.1002/cam4.2593
58. Xu JZ, Wang WQ, Zhang SR, Xu HX, Wu CT, Qi ZH, et al. Neoadjuvant Therapy Is Essential for Resectable Pancreatic Cancer. Curr Med Chem (2019) 26(40):7196–211. doi: 10.2174/0929867325666180413101722
59. Charette N, Vandeputte C, Ameye L, Bogaert CV, Krygier J, Guiot T, et al. Prognostic Value of Adipose Tissue and Muscle Mass in Advanced Colorectal Cancer: A Post Hoc Analysis of Two non-Randomized Phase II Trials. BMC Cancer (2019) 19(1):134. doi: 10.1186/s12885-019-5319-8
60. Blauwhoff-Buskermolen S, Versteeg KS, de van der Schueren MA, den Braver NR, Berkhof J, Langius JA, et al. Loss of Muscle Mass During Chemotherapy Is Predictive for Poor Survival of Patients With Metastatic Colorectal Cancer. J Clin Oncol (2016) 34(12):1339–44. doi: 10.1200/JCO.2015.63.6043
Keywords: skeletal muscle radiodensity, cancer, survival, computerized tomography, sarcopenia, skeletal muscle mass
Citation: Pozzuto L, Silveira MN, Mendes MCS, Macedo LT, Costa FO, Martinez CAR, Coy CRS, da Cunha Júnior AD and Carvalheira JBC (2021) Myosteatosis Differentially Affects the Prognosis of Non-Metastatic Colon and Rectal Cancer Patients: An Exploratory Study. Front. Oncol. 11:762444. doi: 10.3389/fonc.2021.762444
Received: 21 August 2021; Accepted: 22 October 2021;
Published: 11 November 2021.
Edited by:
Puneeth Iyengar, University of Texas Southwestern Medical Center, United StatesReviewed by:
Fanghui Chen, Nanjing Agricultural University, ChinaCopyright © 2021 Pozzuto, Silveira, Mendes, Macedo, Costa, Martinez, Coy, da Cunha Júnior and Carvalheira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Barreto Campello Carvalheira, amJjY0B1bmljYW1wLmJy
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.