
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 19 October 2021
Sec. Radiation Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.753768
This article is part of the Research Topic Insights in Radiation Oncology: 2021/2022 View all 12 articles
 Tilman Bostel1,2*†
Tilman Bostel1,2*† Sati Akbaba1,2†
Sati Akbaba1,2† Daniel Wollschläger3Tristan Klodt1,2Laura Oebel1,2Arnulf Mayer1,2Sophia Drabke1,2Tanja Sprave4,5Jürgen Debus6,7Robert Förster8Harald Rief9
Daniel Wollschläger3Tristan Klodt1,2Laura Oebel1,2Arnulf Mayer1,2Sophia Drabke1,2Tanja Sprave4,5Jürgen Debus6,7Robert Förster8Harald Rief9 Alexander Rühle4,5
Alexander Rühle4,5 Anca-Ligia Grosu4,5
Anca-Ligia Grosu4,5 Heinz Schmidberger1,2
Heinz Schmidberger1,2 Nils H. Nicolay4,5
Nils H. Nicolay4,5Background and Purpose: To compare two validated spinal instability scores regarding the stabilizing effects and skeletal-related events (SREs) of palliative radiotherapy (RT) in patients with spinal bone metastases (SBM).
Materials and Methods: Two hundred eighty-two osteolytic SBM of lung or breast cancer patients were analyzed for stability before and following RT based on the Spinal Instability Neoplastic Score (SINS) or the Taneichi score. Score concordance was quantified by absolute agreement and Cohen’s kappa coefficient. SREs were defined as fractures or local progression after RT. OS was quantified as the time between the start of RT and death from any cause.
Results: At 3 and 6 months after RT, 35 and 50% of initially unstable SBM were re-stabilized according to SINS in patients still alive. Corresponding Taneichi score-based stabilization proportions were 25 and 46%, respectively. Comparison of both stability scores showed high absolute agreement for all time-points (range 71–78%, kappa range 0.35–0.44). SRE occurred more frequently in initially unstable SBM compared to stable SBM according to SINS (14 vs. 5%), but no such association could be shown for the Taneichi-based instability criterion. Poor general condition of patients was negatively associated with SINS-measured re-stabilization after 6 months, but no predictive factor for re-stabilization could be found for the Taneichi score.
Conclusions: Despite the relatively high agreement between both stabilization scores, the SINS should be considered the standard for future studies on the stabilization effects of RT in SBM.
Spinal bone metastases (SBM) occur in up to 80% of patients with advanced solid tumors (1, 2). Affected patients often suffer from severe pain, movement restrictions, and/or neurological deficits. Radiotherapy (RT) is a key treatment for symptomatic SBM (3). In addition to the elimination of pain symptoms and restoration of skeletal function, instability of SBM with impending or manifest fractures represents another frequent indication for palliative RT. Unstable SBM not only affect spinal statics but may also threaten the integrity of the spinal cord and the branching nerves with potentially significant negative impact on the patients’ quality of life (4, 5). However, stability assessment of the spinal column is a major challenge in clinical practice and is often only carried out on the basis of clinical experience. This may result in under- or overdiagnosis of spinal instability, making communication between physicians of different disciplines very difficult, and leading to inconsistent therapeutic approaches. For this reason, the Spinal Instability Neoplastic Score (SINS) was introduced in 2010 by the Spinal Oncology Study Group and has since become the most adopted stability score for assessing SBM (6). Based on six categories, the SINS is a highly reliable tool to classify the stability of metastatically affected vertebral bodies into stable, potentially unstable, and unstable lesions (7). For unstable vertebral bodies, the SINS gives a clear recommendation for a stabilizing surgery and postoperative RT. In the case of potentially unstable vertebral body metastases, palliative RT is often preferred to surgery, especially for patients with poor prognosis. Unfortunately, there are only very limited SINS-based data on the effect of RT in unstable SBM (8). Instead, the data available so far are mainly based on the Taneichi score, which has also been validated (9–15).
Therefore, this retrospective study aimed to assess pre- and post-RT stability of spinal metastases using the SINS and Taneichi score, in order to verify their agreement, establish potential predictive factors for stability, and analyze skeletal-related events (SRE) and overall survival (OS) following RT.
A total of 221 patients with a median age of 63 years (range 34–88 years) and osteolytic SBM of the thoracic or lumbar spine with underlying breast (38%) or bronchial carcinoma (62%) were included in this retrospective study. All patients received one or more palliative RT at the University Hospitals of Mainz and Heidelberg between 2006 and 2012. The required patient data were taken from the medical records and cancer registers of the participating centers. The diagnosis of SBM was based on imaging techniques such as CT, MRI, or bone scintigraphy. As inclusion criteria, the spinal metastases had to have an osteolytic phenotype and be located in the thoracic or lumbar spine. This analysis has been approved by the independent ethics committees of the medical faculties of the universities of Heidelberg and Mainz (Heidelberg: S-513/2012, Mainz: 2020-15282).
At baseline, as well as 3 and 6 months after palliative RT, the stability of metastatically affected vertebral bodies was assessed by CT imaging using the SINS and Taneichi scores. The Taneichi score is only validated for osteolytic bone metastases in the thoracic and lumbar spinal column. It is based purely on radiological criteria (degree of vertebral body destruction, involvement of the costovertebral joint and/or pedicle) to identify spinal lesions that have a very high risk of impending vertebral body collapse. The SINS, on the other hand, is validated for bone metastases of any phenotype throughout the entire spinal column. It is based on six criteria (location, type of pain, type of lesions, spinal alignment, presence of vertebral compression fractures, affection of posterolateral elements) to classify the affected vertebral bodies as stable, potentially unstable, and unstable. In this analysis, the instability criteria of the original publication were used (6, 16), i.e., all vertebral body metastases that were classified as at least potentially unstable (≥7 points) according to SINS or had a fracture risk of at least 50% according to Taneichi Score were evaluated as unstable. For both scores, the shift in stability from (potentially) unstable to stable and from stable to (potentially) unstable was independently determined by a board-certified radiologist in patients still alive at the time of evaluation. Furthermore, SREs after palliative RT were assessed, defined as new fractures or progressive sintering of SBM-affected vertebral bodies, or the need for re-irradiation. In the case of multiple bone metastases in a vertebral body or within the target volume, only the most severe lesion was evaluated. If several spinal regions were irradiated in a given patient, each region was evaluated separately in our analysis. A pain response was documented based on reduction of ≥2 points on the 10-point visual analogue scale according to the international consensus criteria (17). For partial and complete pain response to RT, the SINS criterion “type of pain” was rated with 1 and 0 points in our analysis, respectively.
Radiation treatment planning was based on planning CT examinations and, in the case of paravertebral tumor spread, supplemented with MRI scans. The radiation dose was administered via one or more dorsal or oblique dorsal photon fields (6 or 18 MV photon energy). The planning target volume (PTV) included the metastatically affected vertebral body or bodies and the adjacent intervertebral discs, and in most cases also the caudally and cranially adjacent vertebral bodies. Palliative RT was indicated if SBM caused pain symptoms, spinal instability, or neurological deficits. None of the patients in this analysis received additional surgery or other invasive procedures.
Overall survival (OS) was defined as the period from the beginning of first RT until death from any cause and estimated using the Kaplan-Meier method. Group differences in OS after first RT were assessed using the log-rank test. Logistic regression using generalized estimating equations was used to test whether the probability of stable lesions according to SINS and Taneichi score changed from baseline to 3 and 6 months after RT. Logistic regression using generalized estimating equations was used to test the association between the occurrence of any SRE and baseline instability of SBM. Association of prognostic factors “age at RT”, “tumor histology”, “KPS <70 vs. ≥70”, and “fractures prior to RT” with the SINS and Taneichi scores at 3 and 6 months post-RT was tested using separate univariate mixed ordinal logistic regression models. The concordance of the SINS and Taneichi scores in the patient cohort was checked using absolute agreement, and with Cohen’s kappa coefficient. Statistical analysis was done using the R statistical environment, version 4.0.2 (R Core Team 2020, Vienna, Austria). P values of p < 0.05 were considered statistically significant.
A total of 221 patients with 282 target volumes and 792 SBM (range 1–14 metastases per patient) of lung and breast carcinomas that were treated with palliative RT were assessed according to SINS and Taneichi score. Median follow-up after RT was 10.9 months (range 0.1–100.6 months). Further detailed information on patient and treatment characteristics is provided in Table 1.
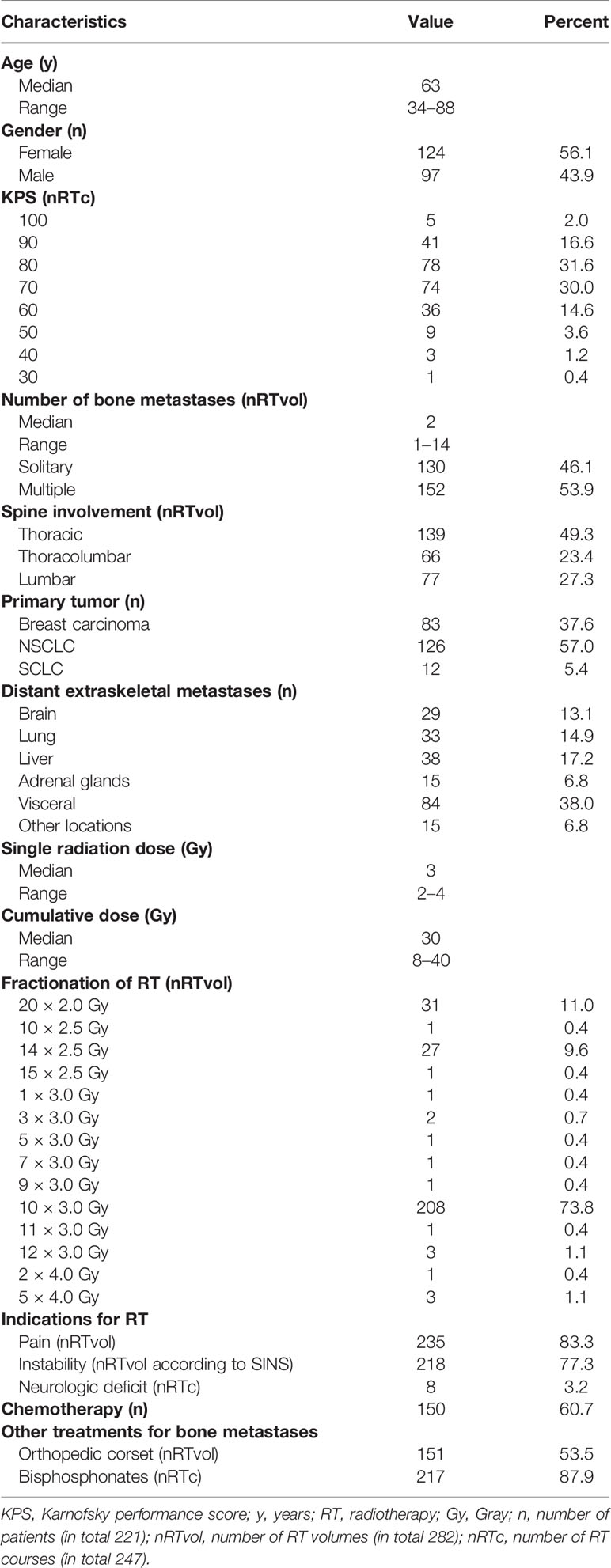
Table 1 Patients’ and treatment characteristics.
Most patients exhibited unstable SBM prior to RT according to the SINS (217/282 SBM; 77%) and Taneichi score (224/282 SBM; 79%), respectively. The majority of these lesions (SINS: 88%, Taneichi: 82%) were associated with pain before the start of irradiation. In patients still alive at 3 and 6 months after RT, the change from baseline in the proportion of stable SBM was statistically significant (p < 0.001) at each time point with 35% (50/143) and 50% (52/104) of the primarily unstable SBM becoming stabilized according to SINS. Our analysis showed no statistically significant differences in the stabilization proportion between SBM of lung and breast cancer patients (see Tables 2, 3A, and 3B).
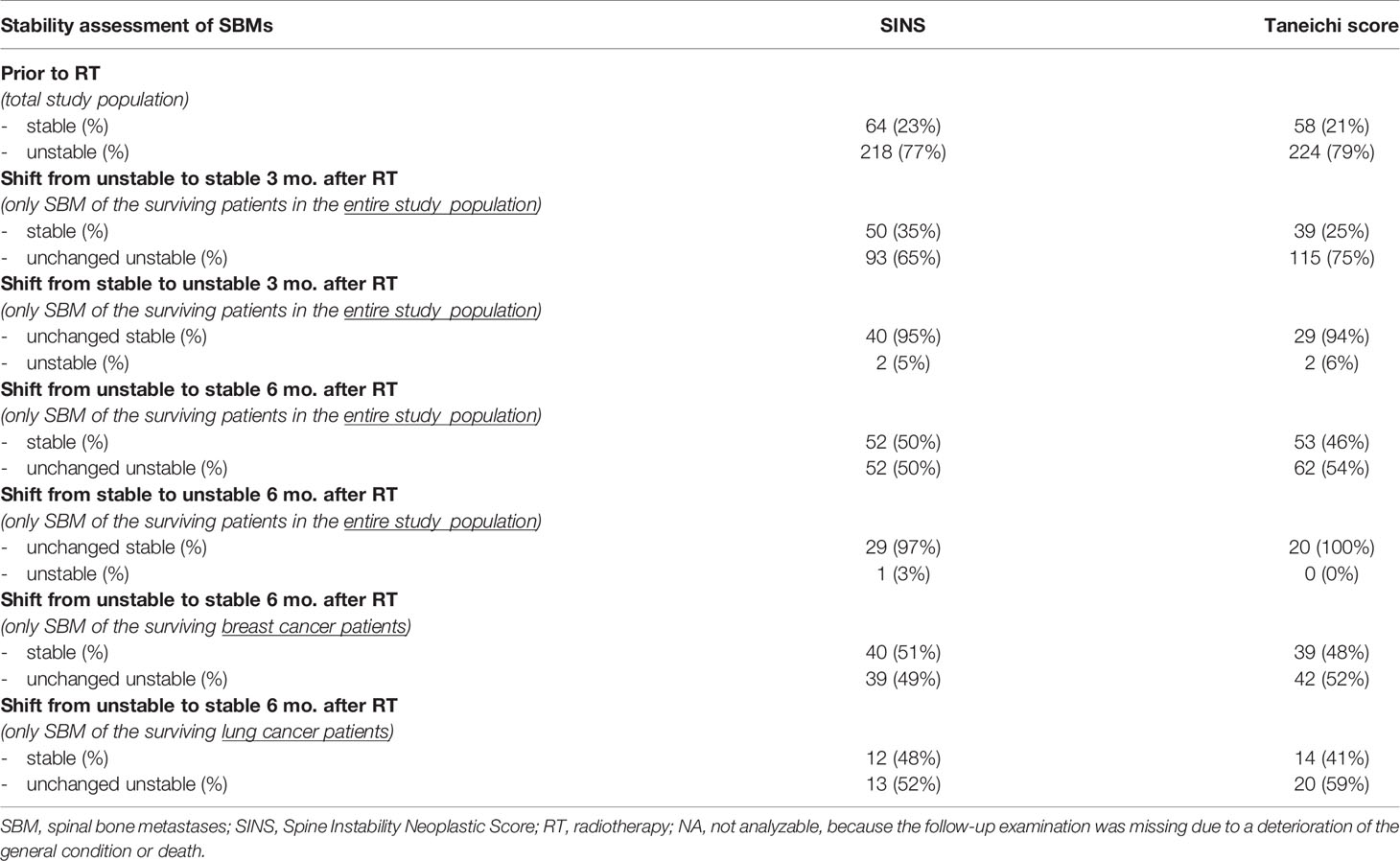
Table 2 Radiogenic changes in vertebral body stability according to SINS and Taneichi Score.
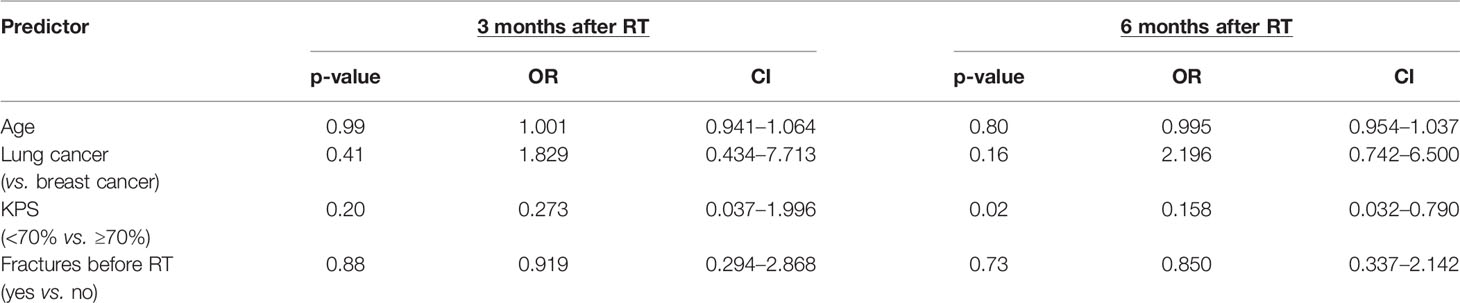
Table 3A Univariate analysis of prognostic factors related to stabilization of initially unstable SBM according to SINS.
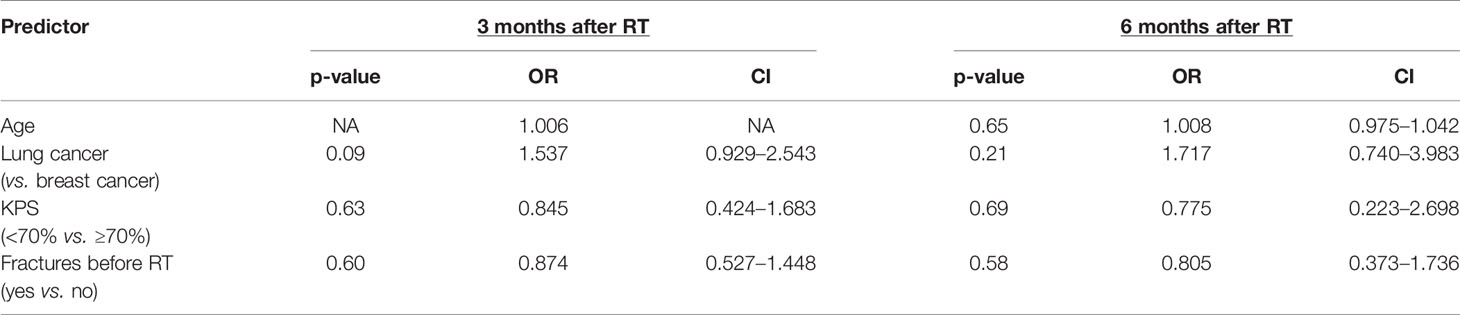
Table 3B Univariate analysis of prognostic factors related to stabilization of initially unstable SBM according to Taneichi score.
Prior to RT, the average SINS was 8.3 [standard deviation (SD) 2.3, range 3–15]. After palliative RT, the average SINS decreased to 6.7 (SD 2.4, range 2–12) after 3 months and to 6.0 (SD 2.2, range 1–12) after 6 months. According to the Taneichi score, the corresponding 3- and 6-month stabilization proportions were 25% (39/154 SBM) and 46% (53/115 SBM), respectively, representing a statistically significant change from baseline (p < 0.001 for each time point; see Table 4). The exact distribution of Taneichi scores before and after palliative RT is summarized in detail in Table 4.
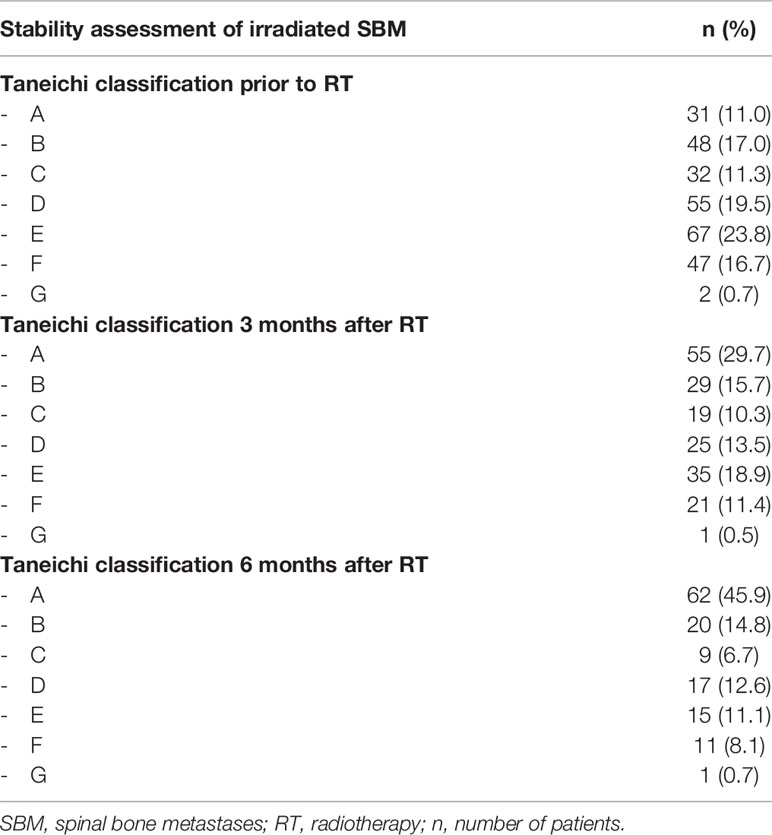
Table 4 Stability assessment of irradiated SBM before and after palliative RT according to the Taneichi score.
Our analysis showed only slightly different 3- and 6-month stabilization proportions of SBM in breast and lung cancer patients who were still alive at the time of evaluation (see Table 2). Taking into account patients who died, the SINS-based stabilization proportions of SBM in the entire study population at 3 and 6 months after palliative RT were only 23% (50/217) and 24% (52/217), respectively. The corresponding Taneichi-based stabilization proportions were 17% (39/224) and 24% (53/224). The different survival prognosis of breast and lung cancer patients had a substantial impact on stabilization probability of primary unstable SBM. In breast cancer patients, the 6-month stabilization probability was 43% (40/93 SBM) and 41% (39/96 SBM) according to the SINS and Taneichi scores, while in lung cancer patients the corresponding values for both scores were only 10 and 11% (SINS: 12/124 SBM, Taneichi: 14/128 SBM).
In our analysis, the SINS criteria “type of lesions”, “type of pain”, and “presence of vertebral compression fractures” were decisive for the change in stability assessment of primary unstable SBM, while the scores in the other SINS criteria remained stable over time. Regarding the “type of lesions” criterion, recalcification was responsible for an improvement in the SINS stability category (i.e., shift from potentially unstable to stable) in 56% of initially unstable osteolytic SBM 3 months after RT (28/50; mixed type of lesions 50%, blastic lesions 6%, no recalcification 44%) and 81% of SBM 6 months after RT (42/52; mixed type of lesions 62%, blastic lesions 19%, no recalcification 19%), respectively. Regarding the “type of pain” criterion, an improvement of the stability due to an RT-induced pain response was present in 75% of symptomatic primary unstable SBM in our analysis (117/157; partial response 40%, complete response 35%).
A shift in stability from stable to (potentially) unstable according to both scores was only rarely observed following RT (see Table 2). In SINS, a Karnofsky Performance Score of less than 70% had a statistically significant association with worse stabilization probability in the univariate mixed ordinal logistic regression for patients still alive 6 months after palliative RT (see Table 3A); in contrast, no predictive factors could be identified for the Taneichi Score in patients still alive 3 and 6 months after palliative RT that could prospectively predict stabilization of primarily unstable SBM (see Table 3B).
When comparing the two stability scores, absolute agreement both before and at 3 and 6 months after RT was high (78, 71, and 73%, respectively), but Cohen’s kappa coefficients were low due to inhomogeneous marginal frequencies (0.35, 0,41 and 0,44, respectively).
Pathologic fractures were detected in 38% of SBM prior to RT (106/282). Up to 6 months after RT, new fractures and progressive sintering of pre-existing fractures within the vertebral bodies were observed in 3% (8/282) and 8% of SBM (22/282), respectively. According to SINS and Taneichi Score, the majority of these post-RT fractures were already initially assessed unstable (90 and 87%, respectively).
Most patients with post-RT fractures received osteoprotective therapy with bisphosphonates or RANK ligand inhibitors (90%) and had already been provided with a corset (66%) before the fracture. Associated pain was reported in 67% of post-RT fractures (20/30 SBM). In addition to post-RT fractures, three SBMs were locally progressive at follow-up with a need for re-irradiation due to new neurological deficits, resulting in an overall SRE proportion of 12% (33/282 target volumes). The presence of an initial pathological fracture in the irradiated area resulted in increased SRE proportions compared to unfractured metastatic lesions (21 vs. 6%). Furthermore, SINS-based initial vertebral body instability was significantly associated with the occurrence of SRE after palliative RT (p = 0.046, OR 3.38, 95% CI 1.02–11.22, Wald test), which was the case in 14% of primary unstable SBM (30/217) compared to only 5% of primary stable SBM (3/65). In contrast, this association could not be shown for the Taneichi-based instability criterion (p = 0.22, OR 1.97, 95% CI 0.66–5.81, Wald test).
For the entire study population, median OS after first palliative RT of SBM amounted to 4.8 months (95% CI 3.8–6.0 months); the corresponding 6-, 12-, and 24-month OS was 42% (95% CI 36–49%), 29% (95% CI 23–35%), and 12% (95% CI 8–17%), respectively. Our analysis showed significantly worse OS after first RT for patients with Karnofsky Performance Scores below 70% compared to patients with scores of ≥70% (p < 0.001) (see Figure 1).
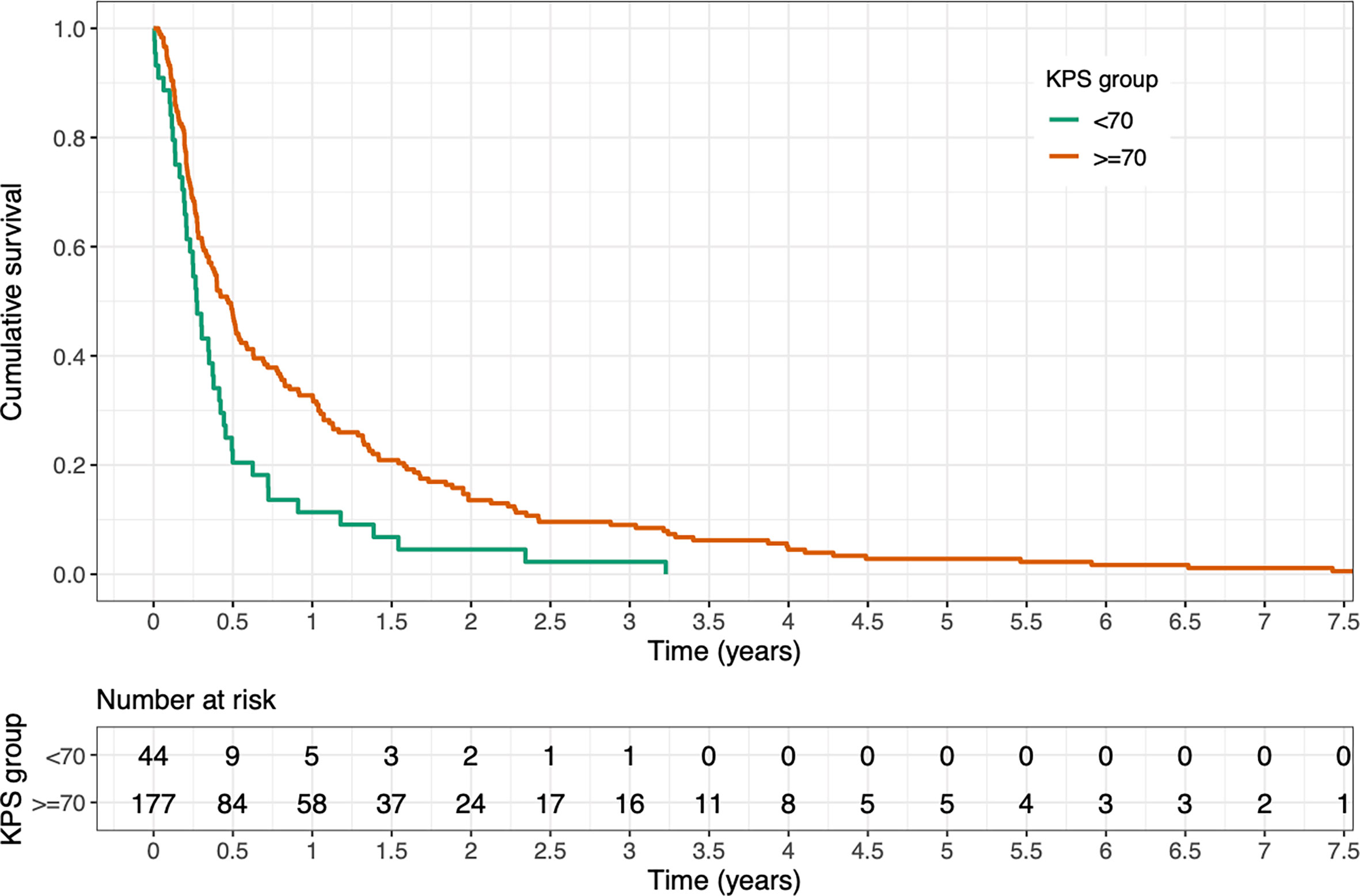
Figure 1 Kaplan-Meier estimate of overall survival (OS) after first radiotherapy stratified by Karnofsky Performance Score (KPS) <70 vs. ≥70. OS was significantly better for patients with a KPS of ≥70% (p < 0.001, log-rank test).
Tumor histology was significantly associated with OS after palliative RT of SBM, with breast cancer patients having a considerably better prognosis than lung cancer patients (p < 0.001, median OS 12.9 months vs. 3.2 months) (see Figure 2).
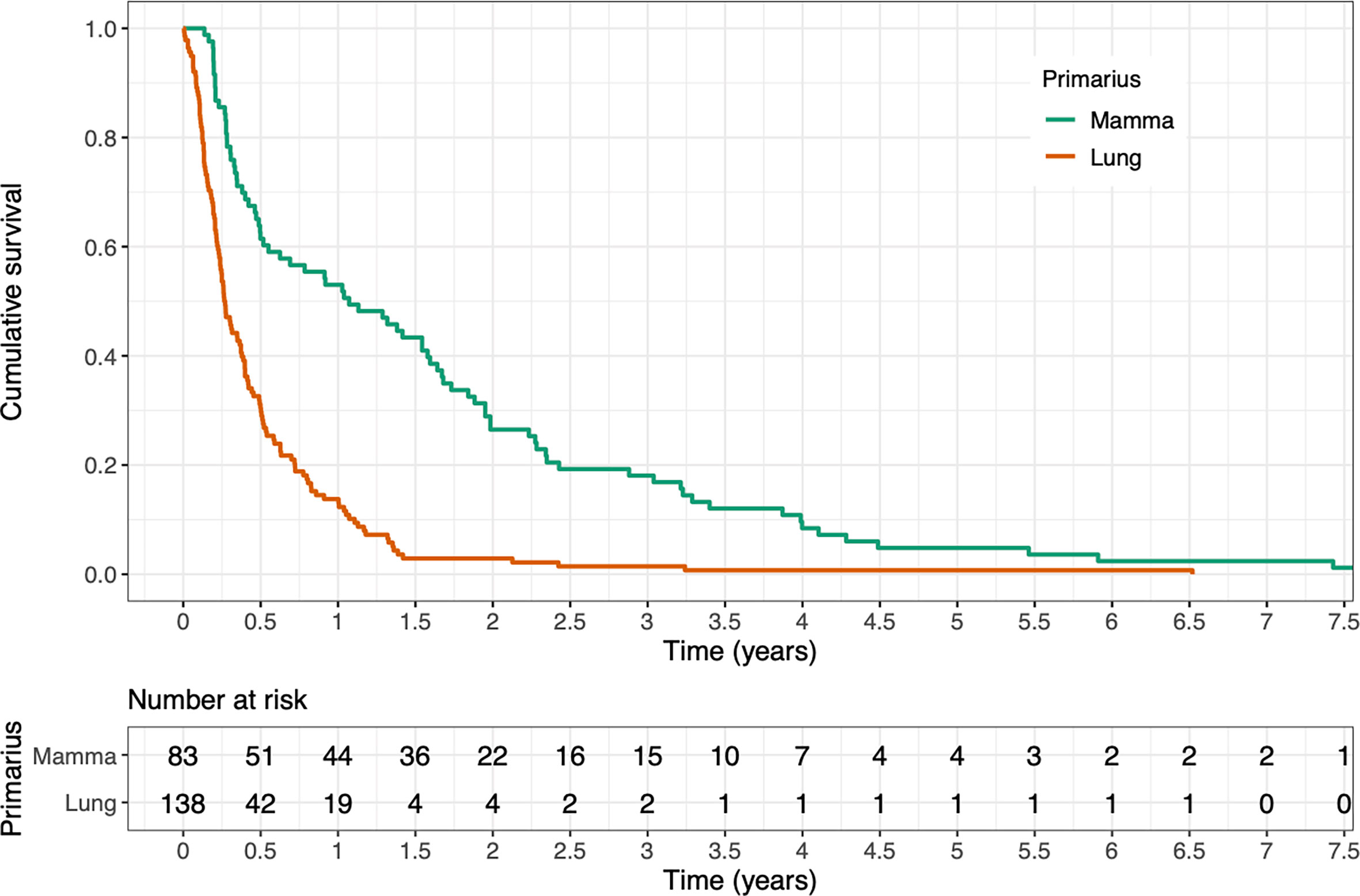
Figure 2 Kaplan-Meier estimate of overall survival after first radiotherapy stratified by tumor histology. OS was significantly better for breast cancer patients compared to lung cancer patients (p < 0.001, log-rank test).
Vertebral instability of SBM represents a key indication for palliative RT, which aims to support recalcification and to improve bone stability. Despite the clinical significance, data on RT-induced stabilization of primarily unstable SBM are limited (18). In particular, the role of stability scores in the context of assessing radiation-induced stabilization remains largely unknown (8).
In our dataset, palliative RT of primarily unstable SBM rarely lead to stabilization in lung cancer patients, whereas nearly half of unstable SBM of breast cancer patients re-stabilized within 6 months after RT. Regarding OS after RT, our evaluation showed significant differences between patients with osseous metastatic lung and breast cancer (median OS 12.9 months vs. 3.2 months). Consequently, the likelihood of stabilization of primarily unstable SBM depends to a large extent on the prognosis of the patients, as recalcification of osteolytic SBM is not expected before 3–6 months after palliative RT (19).
Thus, the relevance of stabilization of unstable SBM is higher for patients with a median OS exceeding 6 months. In our study, tumor histology and the Karnofsky Performance Score were found to be the crucial prognostic factors for OS, which is consistent with the results of previous studies predicting OS in patients with bone metastases (20, 21). Differences in recalcification and stabilization rates between different tumor entities are to a large extent due to the different prognoses, but other factors may also play important roles, such as the individual radiation sensitivity of the respective tumor cell types, the individual tumor microenvironment, the radiation dose or simultaneous systemic treatments. To date, the exact underlying mechanism of radiation-induced recalcification of osteolytic bone metastases remains incompletely understood.
For patients with a low chance of achieving bone stability 6 months after conventional palliative RT, alternative approaches to improve metastatic spinal stability may be considered. For such situations, further dose escalation in the bone metastases through simultaneous integrated boost (i.e., hypofractionated ablative radiotherapy) or even stereotactic body radiotherapy (SBRT) may be promising options. Dose escalation strategies have the potential to improve stabilization in patients with unstable SBM, particularly in patients with good life expectancy and SBM from tumor entities with a relatively low chance of bone stability at 6 months or those with oligometastatic disease. However, potential benefits of SBRT must be balanced against the increased risk of side effects such as fractures or neurologic deficits (22, 23). Surgical stabilization options may also become more relevant to patients. However, compared to SBRT or conventional palliative RT, surgery may interrupt necessary systemic treatments for a considerable time due to perioperative comorbidities.
In assessing vertebral body stability, our analysis showed a relatively good agreement between the SINS and Taneichi scores, with slightly better stabilization rates as assessed by the SINS. This is primarily explained by the inclusion of clinical assessment parameters. Therefore, improved stability scores in our evaluation were also measured by the SINS in case of only a pain response in the absence of recalcification. Nevertheless, our study has shown that previously reported stabilizing effects of palliative RT, based on the Taneichi Score, can be transferred relatively well to the SINS (9, 11, 13, 14, 16, 18, 24). In spinally metastasized head-and-neck tumors, a recent publication assessed stability also on the basis of the SINS (8).
For the SINS, a Karnofsky Performance Score of less than 70% had a statistically significant negative association with the probability of stabilization in our analysis for patients still alive at 6 months after palliative RT. This can be potentially explained by a reduced physical activity of patients with reduced performance, which could negatively impact bony mineralization. In contrast to the results of a recently published study, we could not identify any predictive factors for the Taneichi score in patients still alive at 3 and 6 months after palliative RT that could predict stabilization of primarily unstable SBM (24).
In our study population, pathologic fractures of unstable SBM were shown to be a common clinical problem before starting irradiation. After palliative RT, SRE occurred in 12% of irradiated SBM due to new fractures (3%), progressive fractures (8%), and local progression with the need for re-irradiation (1%). Most post-RT fractures occurred in patients with initial fractures and unstable SBM, and two-thirds of patients with a post-RT fracture reported associated pain. In the literature, secondary fractures, spinal cord compression, and re-irradiation rates after palliative multifractional RT were reported in 2–5, 4–6, and 7–9% of cases, respectively (25–28). The higher number of fractures in our study population can be explained by the high proportion of initially complicated SBM that were not adequately considered in the landmark studies and large literature reviews (25–28).
The presence of a pathologic fracture prior to RT resulted in an increase of SRE in our analysis compared to unfractured metastatic bone (21 vs. 6%). Furthermore, SINS-based initial vertebral instability was found to be significantly associated with the occurrence of SRE, whereas no such association could be demonstrated for Taneichi-based vertebral instability.
Our study has some limitations, especially considering the retrospective character of this patient cohort. For instance, data on clinical factors that may influence bone stabilization and fracture probability such as, e.g., osteoporosis, medication or physical activity could not be systematically collected in our cohort. Furthermore, patients’ quality of life could not be assessed retrospectively and requires further prospective investigation. Our evaluation did not include cervical and sacral SBM, as the Taneichi Score is only validated for osteolytic thoracic and lumbar SBM.
For this analysis, we intentionally included only patients who had not received RT in recent years to exclude potential effects of modern systemic therapies such as immunotherapy on bony remineralization. Thus, as a result of improved survival, SRE and stabilization rates of patients with more recently treated unstable SBM may be higher than reported here. Therefore, the current analysis intends to serve as baseline examination for subsequent histology-specific stability analyses of SBM irradiated in recent years.
In summary, the choice of radiation dose and fractionation should take into account not only the therapeutic goal but also clinical factors such as patients’ general condition and comorbidities, the extent of metastatic disease, and the overall prognosis of the patients, since significant recalcification of osteolytic SBM can first be detected at 3–6 months after palliative RT. The results of our retrospective evaluation support the urgent need to initiate prospective studies to systematically assess irradiation effects and complication rates (SRE) as a function of initial SINS-based vertebral body instability in the era of modern systemic therapies.
Our analysis showed a relatively high agreement between two widely available clinical stabilization scores. The data published so far based on the Taneichi score can therefore be transferred relatively well to the SINS. However, compared to the SINS, the Taneichi Score has some important limitations (i.e., validation only for osteolytic SBM and thoracolumbar lesions), so the SINS should be further considered in future studies on the stabilization effects and complications of palliative RT in SBM. In this regard, initial vertebral body instability according to SINS and pre-existing fractures seemed to increase the risk for SRE after RT.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the independent ethics committees of the medical faculties of the universities of Heidelberg and Mainz (Heidelberg: S-513/2012, Mainz: 2020-15282). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
TB and SA equally contributed to this manuscript. TB, SA, and NN developed and planned the retrospective analysis. DW is responsible for statistical considerations/basis of the analysis. TB, SA, TK, LO, AM, SD, TS, JD, RF, HR, AR, A-LG, HS, and NN participated in data collection and/or interpretation of the results. TB wrote the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Jessica Lüder, Pia Fischer, and Alex Diwo for participating in data collection.
1. Mundy GR. Metastasis to Bone: Causes, Consequences and Therapeutic Opportunities. Nat Rev Cancer (2002) 2(8):584–93. doi: 10.1038/nrc867
2. Nielsen OS. Palliative Radiotherapy of Bone Metastases: There Is Now Evidence for the Use of Single Fractions. Radiother Oncol: J Eur Soc Ther Radiol Oncol (1999) 52(2):95–6. doi: 10.1016/s0167-8140(99)00109-7
3. Lutz S, Balboni T, Jones J, Lo S, Petit J, Rich SE, et al. Palliative Radiation Therapy for Bone Metastases: Update of an ASTRO Evidence-Based Guideline. Pract Radiat Oncol (2017) 7(1):4–12. doi: 10.1016/j.prro.2016.08.001
4. Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, et al. Direct Decompressive Surgical Resection in the Treatment of Spinal Cord Compression Caused by Metastatic Cancer: A Randomised Trial. Lancet (2005) 366(9486):643–8. doi: 10.1016/S0140-6736(05)66954-1
5. Rades D, Segedin B, Conde-Moreno AJ, Garcia R, Perpar A, Metz M, et al. Radiotherapy With 4 Gy X 5 Versus 3 Gy X 10 for Metastatic Epidural Spinal Cord Compression: Final Results of the SCORE-2 Trial (ARO 2009/01). J Clin Oncol: Off J Am Soc Clin Oncol (2016) 34(6):597–602. doi: 10.1200/JCO.2015.64.0862
6. Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, et al. A Novel Classification System for Spinal Instability in Neoplastic Disease: An Evidence-Based Approach and Expert Consensus From the Spine Oncology Study Group. Spine (2010) 35(22):E1221–9. doi: 10.1097/BRS.0b013e3181e16ae2
7. Fourney DR, Frangou EM, Ryken TC, Dipaola CP, Shaffrey CI, Berven SH, et al. Spinal Instability Neoplastic Score: An Analysis of Reliability and Validity From the Spine Oncology Study Group. J Clin Oncol: Off J Am Soc Clin Oncol (2011) 29(22):3072–7. doi: 10.1200/JCO.2010.34.3897
8. Bostel T, Ruhle A, Rackwitz T, Mayer A, Klodt T, Oebel L, et al. The Role of Palliative Radiotherapy in the Treatment of Spinal Bone Metastases From Head and Neck Tumors-A Multicenter Analysis of a Rare Event. Cancers (Basel) (2020) 12(7):1950. doi: 10.3390/cancers12071950
9. Bostel T, Forster R, Schlampp I, Sprave T, Bruckner T, Nicolay NH, et al. Spinal Bone Metastases in Colorectal Cancer: A Retrospective Analysis of Stability, Prognostic Factors and Survival After Palliative Radiotherapy. Radiat Oncol (2017) 12(1):115. doi: 10.1186/s13014-017-0852-6
10. Bostel T, Forster R, Schlampp I, Wolf R, Serras AF, Mayer A, et al. Stability, Prognostic Factors and Survival of Spinal Bone Metastases in Malignant Melanoma Patients After Palliative Radiotherapy. Tumori (2016) 102(2):156–61. doi: 10.5301/tj.5000382
11. Foerster R, Habermehl D, Bruckner T, Bostel T, Schlampp I, Welzel T, et al. Spinal Bone Metastases in Gynecologic Malignancies: A Retrospective Analysis of Stability, Prognostic Factors and Survival. Radiat Oncol (2014) 9:194. doi: 10.1186/1748-717X-9-194
12. Foerster R, Hees K, Bruckner T, Bostel T, Schlampp I, Sprave T, et al. Survival and Stability of Patients With Urothelial Cancer and Spinal Bone Metastases After Palliative Radiotherapy. Radiol Oncol (2018) 52(2):189–94. doi: 10.1515/raon-2017-0038
13. Rief H, Bischof M, Bruckner T, Welzel T, Askoxylakis V, Rieken S, et al. The Stability of Osseous Metastases of the Spine in Lung Cancer–a Retrospective Analysis of 338 Cases. Radiat Oncol (2013) 8(1):200. doi: 10.1186/1748-717X-8-200
14. Schlampp I, Rieken S, Habermehl D, Bruckner T, Forster R, Debus J, et al. Stability of Spinal Bone Metastases in Breast Cancer After Radiotherapy: A Retrospective Analysis of 157 Cases. Strahlenther Onkol (2014) 190(9):792–7. doi: 10.1007/s00066-014-0651-z
15. Schlampp I, Lang H, Forster R, Wolf R, Bostel T, Bruckner T, et al. Stability of Spinal Bone Metastases and Survival Analysis in Renal Cancer After Radiotherapy. Tumori (2015) 101(6):614–20. doi: 10.5301/tj.5000370
16. Taneichi H, Kaneda K, Takeda N, Abumi K, Satoh S. Risk Factors and Probability of Vertebral Body Collapse in Metastases of the Thoracic and Lumbar Spine. Spine (Phila Pa 1976) (1997) 22(3):239–45. doi: 10.1097/00007632-199702010-00002
17. Chow E, Hoskin P, Mitera G, Zeng L, Lutz S, Roos D, et al. Update of the International Consensus on Palliative Radiotherapy Endpoints for Future Clinical Trials in Bone Metastases. Int J Radiat Oncol Biol Phys (2012) 82(5):1730–7. doi: 10.1016/j.ijrobp.2011.02.008
18. Sprave T, Hees K, Bruckner T, Foerster R, Bostel T, Schlampp I, et al. The Influence of Fractionated Radiotherapy on the Stability of Spinal Bone Metastases: A Retrospective Analysis From 1047 Cases. Radiat Oncol (2018) 13(1):134. doi: 10.1186/s13014-018-1082-2
19. Koswig S, Budach V. Remineralization and Pain Relief in Bone Metastases After After Different Radiotherapy Fractions (10 Times 3 Gy vs. 1 Time 8 Gy). A Prospective Study. Strahlenther Onkol (1999) 175(10):500–8. doi: 10.1007/s000660050061
20. Bollen L, Jacobs WCH, van der Linden YM, van der Hel O, Taal W, Dijkstra PDS. A Systematic Review of Prognostic Factors Predicting Survival in Patients With Spinal Bone Metastases. Eur Spine J (2018) 27(4):799–805. doi: 10.1007/s00586-017-5320-3
21. Rades D, Haus R, Schild SE, Janssen S. Prognostic Factors and a New Scoring System for Survival of Patients Irradiated for Bone Metastases. BMC Cancer (2019) 19(1):1156. doi: 10.1186/s12885-019-6385-7
22. Sahgal A, Atenafu EG, Chao S, Al-Omair A, Boehling N, Balagamwala EH, et al. Vertebral Compression Fracture After Spine Stereotactic Body Radiotherapy: A Multi-Institutional Analysis With a Focus on Radiation Dose and the Spinal Instability Neoplastic Score. J Clin Oncol (2013) 31(27):3426–31. doi: 10.1200/JCO.2013.50.1411
23. Garg AK, Shiu AS, Yang J, Wang XS, Allen P, Brown BW, et al. Phase 1/2 Trial of Single-Session Stereotactic Body Radiotherapy for Previously Unirradiated Spinal Metastases. Cancer (2012) 118(20):5069–77. doi: 10.1002/cncr.27530
24. Bostel T, Forster R, Schlampp I, Sprave T, Akbaba S, Wollschlager D, et al. Stability and Survival Analysis of Elderly Patients With Osteolytic Spinal Bone Metastases After Palliative Radiotherapy: Results From a Large Multicenter Cohort. Strahlenther Onkol (2019) 195(12):1074–85. doi: 10.1007/s00066-019-01482-1
25. Steenland E, Leer JW, van Houwelingen H, Post WJ, van den Hout WB, Kievit J, et al. The Effect of a Single Fraction Compared to Multiple Fractions on Painful Bone Metastases: A Global Analysis of the Dutch Bone Metastasis Study. Radiother Oncol (1999) 52(2):101–9. doi: 10.1016/S0167-8140(99)00110-3
26. Hartsell WF, Scott CB, Bruner DW, Scarantino CW, Ivker RA, Roach M 3rd, et al. Randomized Trial of Short- Versus Long-Course Radiotherapy for Palliation of Painful Bone Metastases. J Natl Cancer Inst (2005) 97(11):798–804. doi: 10.1093/jnci/dji139
27. Chow E, Harris K, Fan G, Tsao M, Sze WM. Palliative Radiotherapy Trials for Bone Metastases: A Systematic Review. J Clin Oncol (2007) 25(11):1423–36. doi: 10.1200/JCO.2006.09.5281
Keywords: spinal bone metastases, instability, radiotherapy, SINS, skeletal-related events
Citation: Bostel T, Akbaba S, Wollschläger D, Klodt T, Oebel L, Mayer A, Drabke S, Sprave T, Debus J, Förster R, Rief H, Rühle A, Grosu A-L, Schmidberger H and Nicolay NH (2021) Comparative Analyses of Two Established Scores to Assess the Stability of Spinal Bone Metastases Before and After Palliative Radiotherapy. Front. Oncol. 11:753768. doi: 10.3389/fonc.2021.753768
Received: 05 August 2021; Accepted: 21 September 2021;
Published: 19 October 2021.
Edited by:
Dinesh Thotala, Washington University in St. Louis, United StatesReviewed by:
Yingming Sun, Fujian Medical University, ChinaCopyright © 2021 Bostel, Akbaba, Wollschläger, Klodt, Oebel, Mayer, Drabke, Sprave, Debus, Förster, Rief, Rühle, Grosu, Schmidberger and Nicolay. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tilman Bostel, dGlsbWFuLmJvc3RlbEB1bmltZWRpemluLW1haW56LmRl
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.