
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 09 September 2021
Sec. Thoracic Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.729765
This article is part of the Research TopicWomen in Thoracic Oncology: 2021View all 14 articles
 Greta Alì1†
Greta Alì1† Iosè Di Stefano2†Anello Marcello Poma2Stefano Ricci3Agnese Proietti1Federico Davini4Marco Lucchi5Franca Melfi4
Iosè Di Stefano2†Anello Marcello Poma2Stefano Ricci3Agnese Proietti1Federico Davini4Marco Lucchi5Franca Melfi4 Gabriella Fontanini2*
Gabriella Fontanini2*Delta-like protein 3 (DLL3) is a protein of the Notch pathway, and it is a potential therapeutic target for high-grade lung neuroendocrine tumors (NETs), i.e., small cell lung carcinoma (SCLC) and large cell neuroendocrine carcinoma (LCNEC). However, DLL3 prevalence in lung NETs and its association with clinicopathological characteristics and prognosis remained unclear. We analyzed the immunohistochemical expression of DLL3 and its prognostic role in a consecutive series of 155 surgically resected lung NETs, including typical carcinoid (TC), atypical carcinoid (AC), LCNEC, and SCLC patients. The DLL3 expression was categorized as high (>50% positive tumor cells) or low (<50%). In addition, tumors were categorized by H-score (i.e., percentage of positive cells by staining intensity, ≥150 vs. <150). DLL3 staining was positive in 99/155 (64%) samples, and high DLL3 expression was frequently observed in high-grade tumors. In detail, 46.9% and 75% of SCLC and 48.8% and 53.7% of LCNEC specimens showed a high DLL3 expression by using H-score and percentage of positive tumor cells, respectively. Regarding low-grade NETs, only 4.9% and 12.2% TCs and 19.5% and 24.4% ACs had high DLL3 expression considering H-score and percentage of positive tumor cells, respectively. High DLL3 expression was associated with advanced American Joint Committee on Cancer (AJCC) stage, peripheral location, and chromogranin A expression in high-grade tumors (p < 0.05). In low-grade NETs, high DLL3 expression was associated with female sex, peripheral location, a higher number of mitoses, higher Ki-67 index, presence of necrosis, and pleural infiltration (p < 0.05). No association was observed between high DLL3 expression and overall survival (OS) and disease-free survival (DFS) in high-grade NETs, whereas high DLL3 expression was associated with lower DFS in ACs (p = 0.01). In conclusion, our study demonstrated a high prevalence of DLL3 expression in high-grade lung NET patients and its association with aggressive clinicopathological features. These findings confirm that DLL3 could represent a useful biomarker for target therapy in high-grade tumors. Our results also suggest that the DLL3 expression could identify a subset of AC tumors with more aggressive behavior, thus providing the basis for new therapeutic options in this group of patients.
Neuroendocrine (NE) tumors (NETs) are a heterogeneous group of neoplasms found most commonly in the lung and in the gastrointestinal tract (1, 2). The 2021 WHO classification of lung tumors identifies four distinct histological variants of lung NETs by using diagnostic criteria similar to those used since the 1999 WHO classification. These lung NETs have been categorized as typical carcinoid (TC), atypical carcinoid (AC), large cell NE carcinoma (LCNEC), and small cell lung carcinoma (SCLC); and they are differentiated on the basis of mitotic rate, presence of necrosis, and cytomorphological details, which allow to distinguish between low-grade (TC and AC) and high-grade (LCNEC and SCLC) tumors (3–5).
Low-grade NETs of the lung have a favorable prognosis compared with the more common high-grade NETs, i.e., LCNECs and SCLCs (6, 7).
The correct classification of lung NETs allows to select the most effective treatment regimen; surgery is often curative for both TC and AC, and for LCNECs. On the contrary, surgery is rarely used for SCLC patients, who are generally treated with chemotherapy. However, the rapid acquisition of chemoresistance in these patients and the substantial lack of alternative treatment options contribute to clinical failures (8–10). In carcinoid patients with metastatic disease, adjuvant therapy should be considered only in selected cases, since no studies have convincingly proved a benefit in terms of risk of local or distant recurrence (11–13). Therefore, more effective therapies and predictive biomarkers are needed both in carcinoid tumor patients who are not curable with surgery alone and in high-grade pulmonary NE carcinoma patients.
Delta-like protein 3 (DLL3), a member of the Notch family, has been identified as an inhibitory ligand of the Notch signalling pathway. DLL3 might function as an oncogenic driver in high-grade NETs, not only in the lung (14) but also in the gastrointestinal area (15), where DLL3 appears to be a downstream transcriptional target of the Achaete-scute homolog 1 (ASCL1) transcription factor (16–20). In particular, DLL3 is frequently expressed in the cell membrane of high-grade NETs, and it has low to no expression in most normal tissue (21); therefore, DLL3 could represent a potential therapeutic target in these tumors. Recently, some preclinical and clinical studies have used rovalpituzumab tesirine (Rova-T), a humanized monoclonal antibody against DLL3 in SCLCs (22–24). In these studies, the DLL3 expression seemed to identify patients who are more likely to achieve a response and a better long-term benefit after treatment with Rova-T (23, 24). Other DLL3-targeting agents, such as T cell-redirecting therapies and immuno-oncology therapies (AMG 757 and AMG 119), may have a high effect and specificity for DLL3-positive SCLC tumor cells (25–27).
For these reasons, recent studies have focused on the immunohistochemical DLL3 expression in lung NETs. However, most of them concern high-grade neoplasms, whereas few data are available for carcinoid tumors (23, 24, 28–32). In this study, we analyzed the immunohistochemical expression of DLL3 in a cohort of 155 patients with lung NETs including TCs, ACs, SCLCs, and LCNECs. This cohort included only limited-stage lung NETs treated with surgery; and for all cases, clinicopathological characteristics and prognostic factors were retrospectively reviewed. The aim of this paper was to investigate clinical features that might be associated with the DLL3 expression and to explore the prognostic role of this marker in pulmonary NETs.
This study was approved by the Ethics Committee “Comitato Etico di Area Vasta Nord Ovest” (CEAVNO) for Clinical Experimentation. A total of 155 lung NET specimens were retrospectively collected from the archives of the Operative Unit of Pathological Anatomy III of the University Hospital of Pisa. In detail, we collected 41 TC, 41 AC, 41 LCNEC, and 32 SCLC samples obtained from patients who had been submitted to surgical resection at the Unit of Thoracic Surgery of the University Hospital of Pisa from December 2007 to December 2019. Participation in this study required informed consent. Patients did not receive neoadjuvant chemotherapy nor radiation therapy. Clinical information, including sex, age, smoking status, disease-free survival (DFS), and overall survival (OS) were reviewed for each patient.
All tumor samples were formalin-fixed and paraffin-embedded (FFPE). The most representative paraffin block of tumor was selected for immunohistochemical analysis for each case. Histological diagnoses and pathological features were obtained by two pathologists (GA and ID), according to the WHO 2015 histological and immunohistochemical criteria (4).
In detail, the NET specimens were evaluated for growth patterns (organoid, trabecular, follicular, palisading, rosette, spindle-cell, and diffuse lymphoma-like), mitosis number per 2 mm2, presence of necrosis and its pattern (absent, punctate, extensive, and geographic), vascular invasion (none, present focal, present extended), and tumor-infiltrating lymphocytes (TILs), both intra-tumoral and stromal lymphocytes (none <1%, focal <10%, moderate <50%, and diffused ≥50%). In detail, the presence of necrosis was determined by semiquantitative analysis evaluating necrosis percentage in the tumor area. We also evaluated the immunohistochemical expression of the NE markers (chromogranin A, synaptophysin, and CD56). At least one positive NE marker was required for diagnosis. Furthermore, the immunohistochemical results for thyroid transcription factor 1 (TTF1) and Ki-67 proliferative index were available for all samples. The NE markers, Ki-67, and TTF1 were scored as negative or positive (negative, weakly 1+, moderately 2+, or strongly 3+), as described before (33). Ki-67 was evaluated as the percentage of positively stained tumor cell-nuclei.
For each tumor sample, data concerning site, size, lymph node (LN) status, pleural involvement, and stage were also collected. For all lung NETs, the eighth edition of the TNM classification was applied for pathological staging (34).
DFS was calculated from the date of tumor resection and diagnosis to the date of either disease recurrence including local recurrence or metastasis; otherwise, data were censored at the time of last follow-up or death. OS was calculated from the date of tumor resection to the date of death, or data were censored at the last follow-up.
DLL3 immunohistochemical analysis was performed on 4-µm-thick tissue sections that were deparaffinized in xylene and rehydrated using a graded series of ethanol solutions. The sections were then subjected to immunohistochemical staining with anti-DLL3 antibody, Rabbit Monoclonal Primary Antibody (clone SP347) (Ventana Medical Systems, Inc. Tucson, AZ, USA) by incubating the sections at 36°C for 32 min. Analysis was conducted with the BenchMark ULTRA semiautomated staining instrument (Ventana Medical Systems) using the OptiView DAB IHC Detection Kit (Ventana Medical Systems). Following a series of washes, the sections were counterstained with Hematoxylin II for 4 min and with Bluing Reagent (Ventana Medical Systems) for 4 min, dehydrated by passages in ethanol with increasing concentration from 70% to 100%, and then mounted.
In all cases, immunohistochemical evaluation was performed independently by two pathologists (GA and ID) who were blinded to all the clinical and pathological data. Selected cases were discussed with a third pathologist (GF) for confirmation. In our study, DLL3 expression was scored for any cytoplasmic and/or membranous staining at any intensity in total tumor cells. In literature, the evaluation of DLL3 immunohistochemical expression has widely varied by using different scores and thresholds for defining positivity (21–23, 28–30, 32, 35). Therefore, in our study, DLL3 positivity was determined based on the proportion of cells expressing DLL3 out of the total number of cells defining the level of expression of DLL3. Subsequently, we categorized DLL3 staining by using the following threshold for DLL3 scoring, which is used in the first clinical trial (23): high expression (>50% positive tumor cells) or low expression (<50%). We also determined the staining intensity as weak (1), intermediate (2), and strong (3) for each sample (Figure 1). Therefore, in order to determine the best evaluation system for DLL3 expression and to take in account the different intensities of the staining we observed in our samples, we further evaluated the DLL3 immunohistochemical results by a semiquantitative approach used to assign an H-score to tumor samples. H-score was calculated by multiplying the percentage of positive cells by the predominant staining intensity, with 300 possible values (0–300), as previously described (22, 29). As well as for the score based on the proportion of DLL3 positive cells, the tumors were ranked according to the median theoretical value as high DLL3 expressors (H-score ≥150) and low DLL3 expressors (H-score <150) by using H-score.
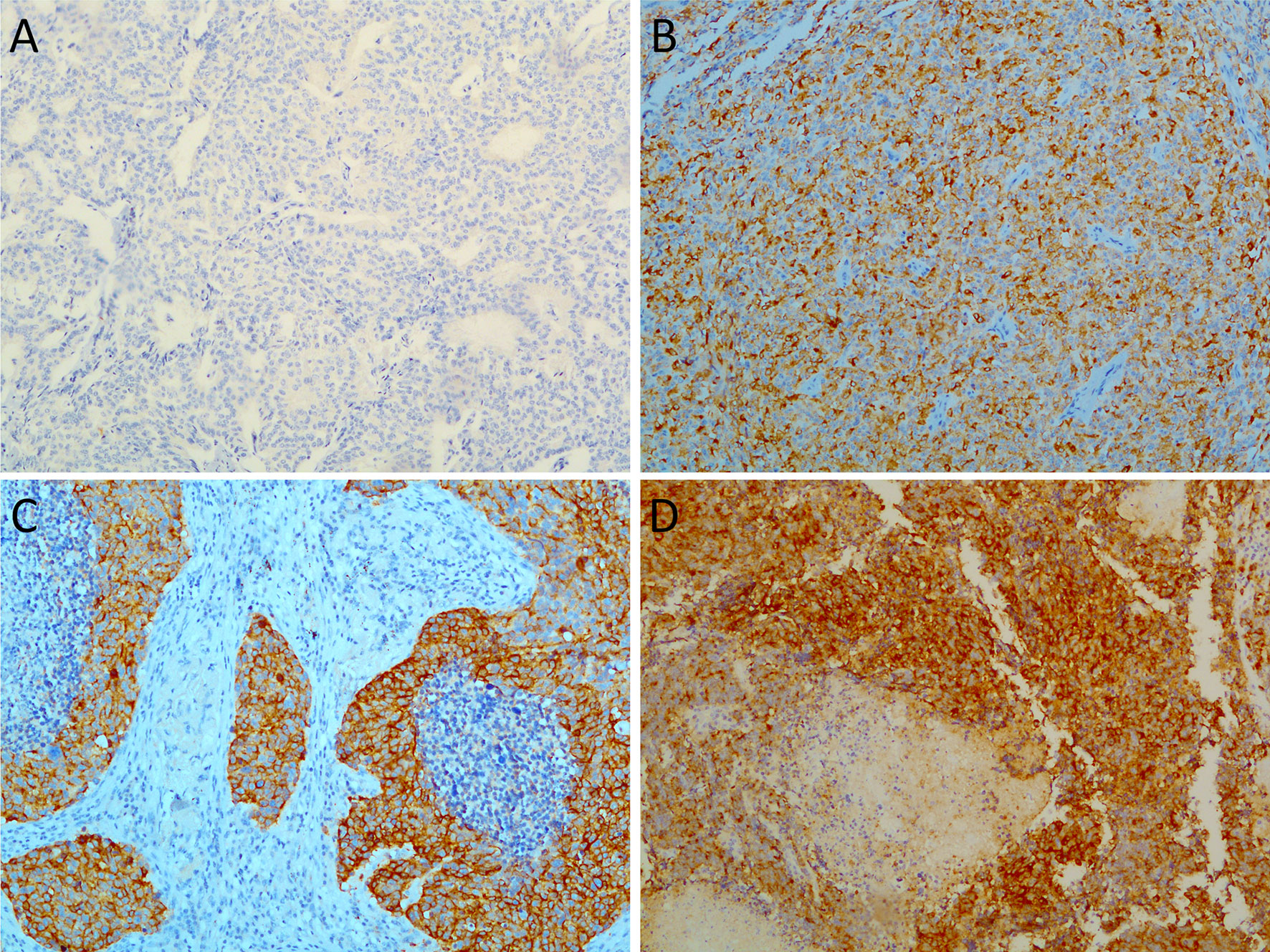
Figure 1 Representative images showing variable percentages of delta-like protein 3 (DLL3) immunohistochemical staining in lung neuroendocrine tumors: (A) typical carcinoid DLL3 negative; (B) a case of atypical carcinoid showing combined cytoplasmic and membranous staining with moderate intensity; (C) large cell neuroendocrine carcinoma with strong and diffuse DLL3 staining; (D) high immunohistochemical expression level of DLL3 in a small cell lung carcinoma specimen. Magnification, ×20.
Pearson’s chi-squared test or Fisher’s exact test was used for categorical variables. Continuous variables were analyzed by the Mann–Whitney or the Kruskal–Wallis tests, and by the Dunn test for multiple comparisons with the Benjamini–Hochberg correction. Survival curves were computed by the Kaplan–Meier method. Cox’s proportional hazard model was used for both univariate and multivariate analyses. All analyses were performed in R environment (version 4.0.2, https://www.r-project.org/, last accessed in January 2021).
A p-value below 0.05 was considered significant.
The present study included 155 patients with lung NETs, 41 (26.5%) TCs, 41 (26.5%) ACs, 41 (26.5%) LCNECs, and 32 (20.5%) SCLCs. Clinicopathological characteristics of patients and morphological findings are summarized in Table 1.
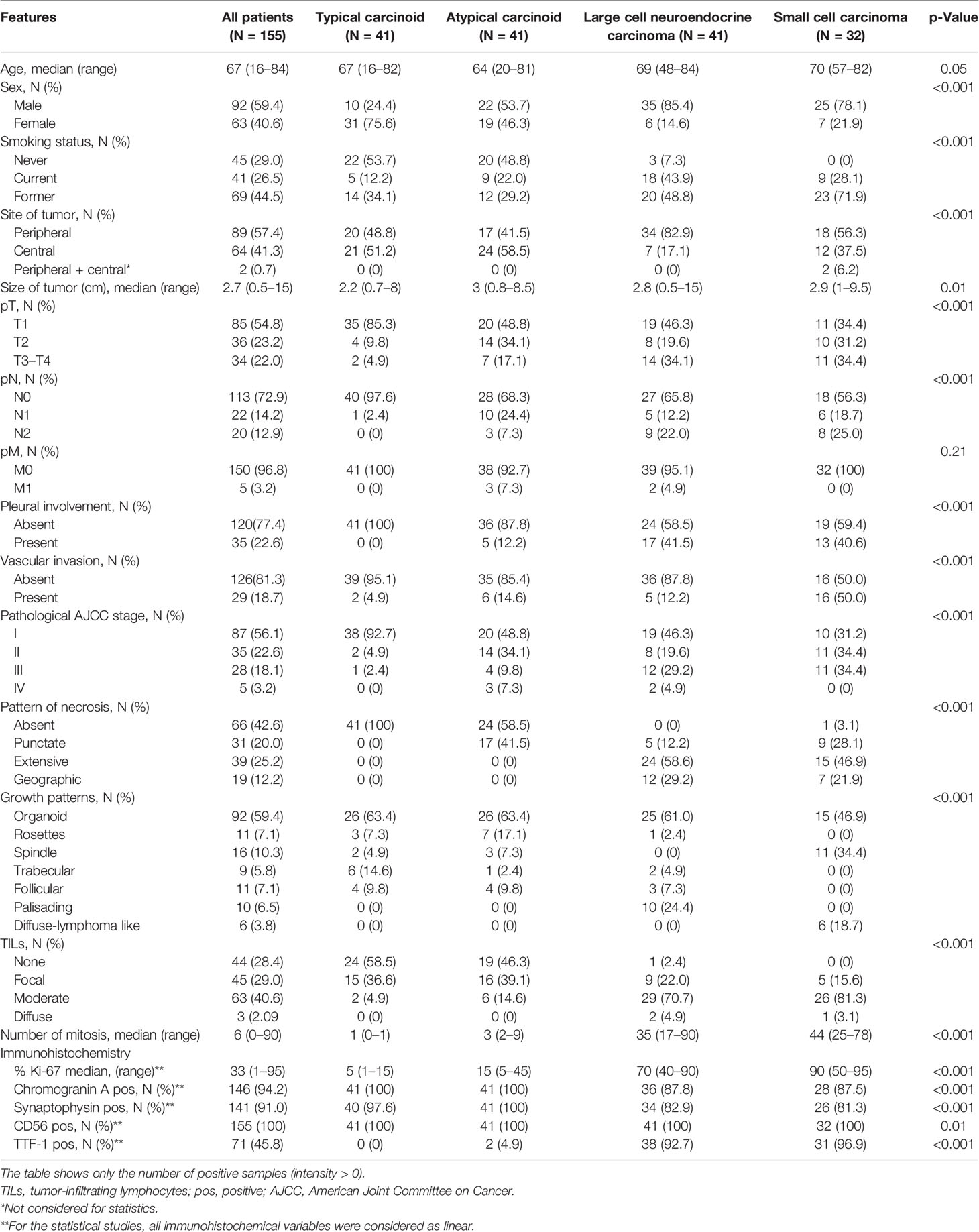
Table 1 Clinicopathological characteristics of patients with lung neuroendocrine tumors.
Patients with high-grade LCNEC and SCLC tumors were more frequently males and smokers. High-grade NETs were more often peripheral. SCLCs, LCNECs, and ACs were larger than TC tumors.
Patients with TC were more often pT1 without regional LN involvement.
Therefore, TC tumors were more commonly resected at stage I (N = 38; 92.7%) in contrast to other histotypes. As regards pleural involvement, high-grade NETs often presented invasion of the pleura, and SCLC showed more frequent vascular invasion than all the other NETs.
Necrosis presence and mitosis number were used as criteria to differentiate the different lung NETs (4). No TC tumors had necrosis, while some AC tumors had punctate necrosis (N = 17; 41.5%), and almost all high-grade NETs showed extensive or geographic necrosis. As expected, the Ki-67 index value was significantly higher in LCNECs and SCLCs compared with low-grade NETs.
With regard to architectural patterns, organoid was the most frequent pattern in low-grade NETs (TCs and ACs) and in LCNECs. The peripheral palisading pattern was observed only in LCNECs; similarly, the diffused lymphoma-like pattern was observed only in SCLCs. High-grade NETs presented significantly more TILs than low-grade tumors.
DLL3 staining was positive in 99/155 (64%) samples, and high DLL3 expression was frequently observed in high-grade tumors. In particular, 20/41 (48.8%) LCNECs and 15/32 (46.9%) SCLCs showed a DLL3 H-score ≥150, whereas only 2/41 (4.9%) TCs and 8/41 (19.5%) ACs had an H-score as high as 150. Considering the percentage of tumor cells, 22/41 (53.7%) LCNECs, 24/32 (75%) SCLCs, 5/41 (12.2%) TCs, and 10/41 (24.4%) ACs showed more than 50% of stained tumor cells (Figures 2A, B). There were no significant differences in DLL3 expression within low-grade and high-grade tumors. Detailed DLL3 immunohistochemistry (IHC) results are shown in Table 2.
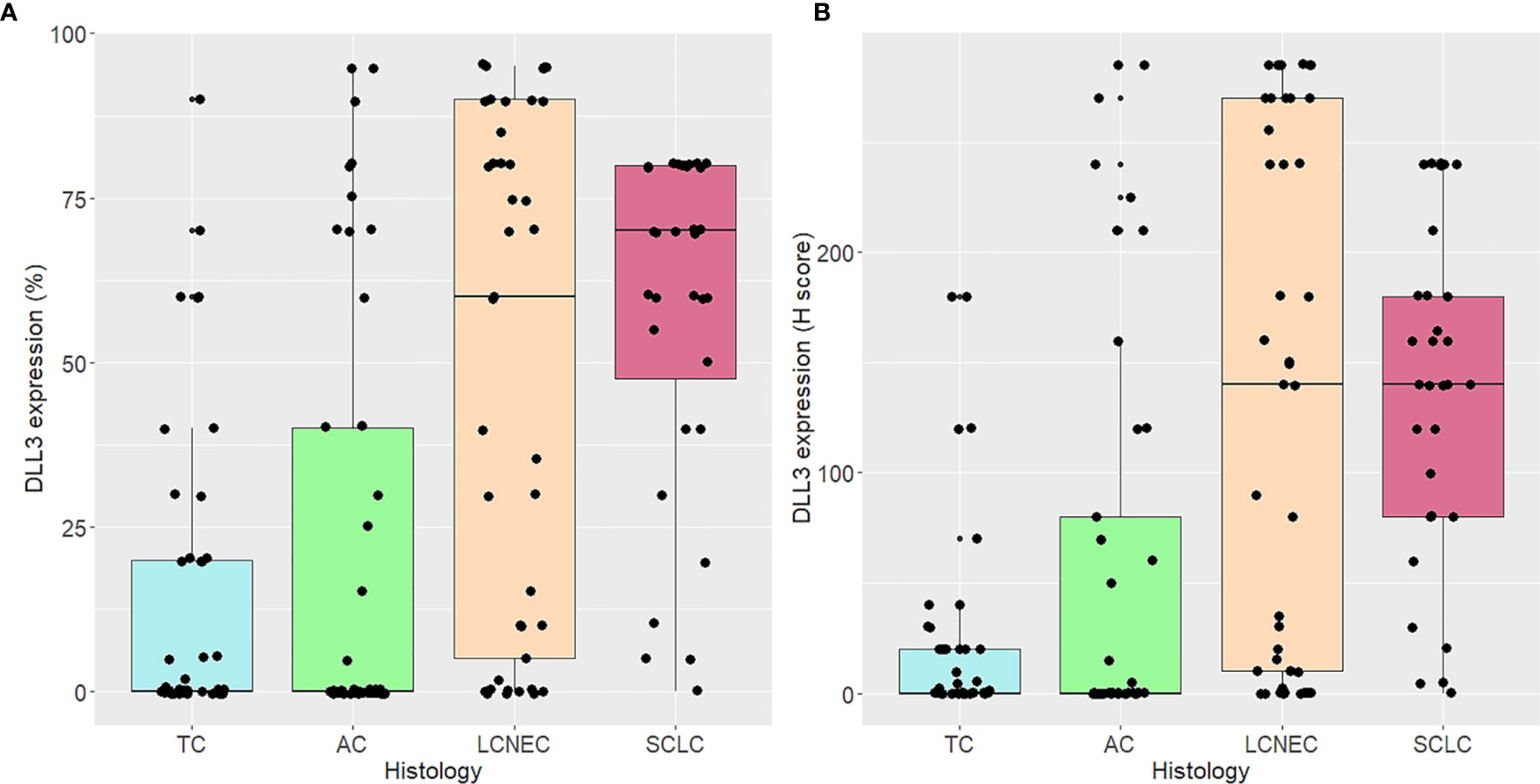
Figure 2 Delta-like protein 3 (DLL3) expression according to histological types. DLL3 expression is indicated as percentage of tumor cells (A) and H-score (B).
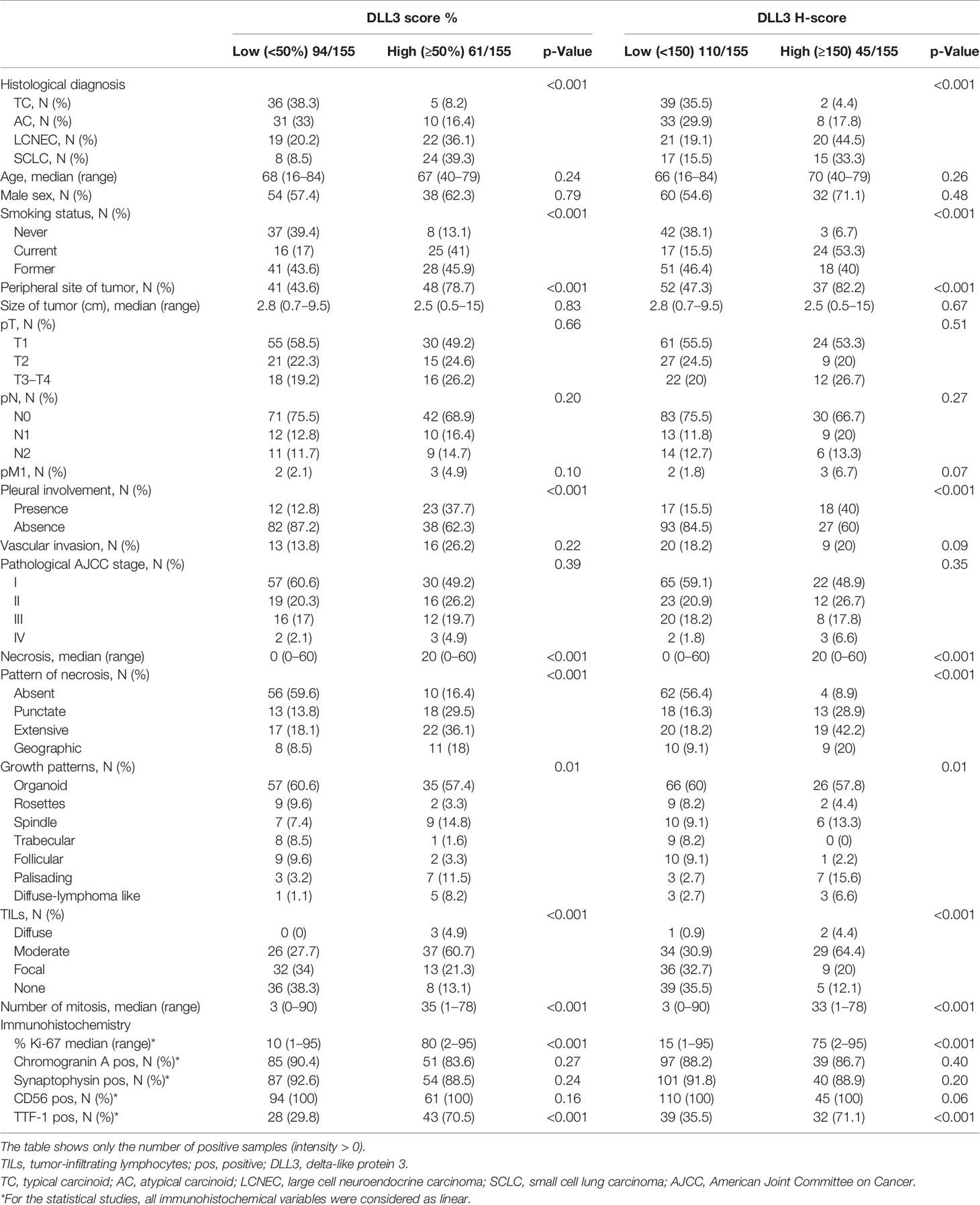
Table 2 Demographics and clinical and pathological features of all neuroendocrine tumors based on high DLL3 expression.
The association between DLL3 expression and clinicopathological patient characteristics and morphological findings is summarized in Table 2.
Overall, patients with high DLL3 expression were more frequently smokers, both current and former; high DLL3 expression was also associated with peripheral tumors.
Considering high- and low-grade tumors as separate groups (Tables 3 and 4), the high DLL3 expression was again associated with the peripheral site of the neoplasm (p = 0.01 for high-grade and p < 0.001 for low-grade tumors). In the high-grade neoplasm group, high DLL3 H-score was associated with advanced pathological American Joint Committee on Cancer (AJCC) stage and younger age.
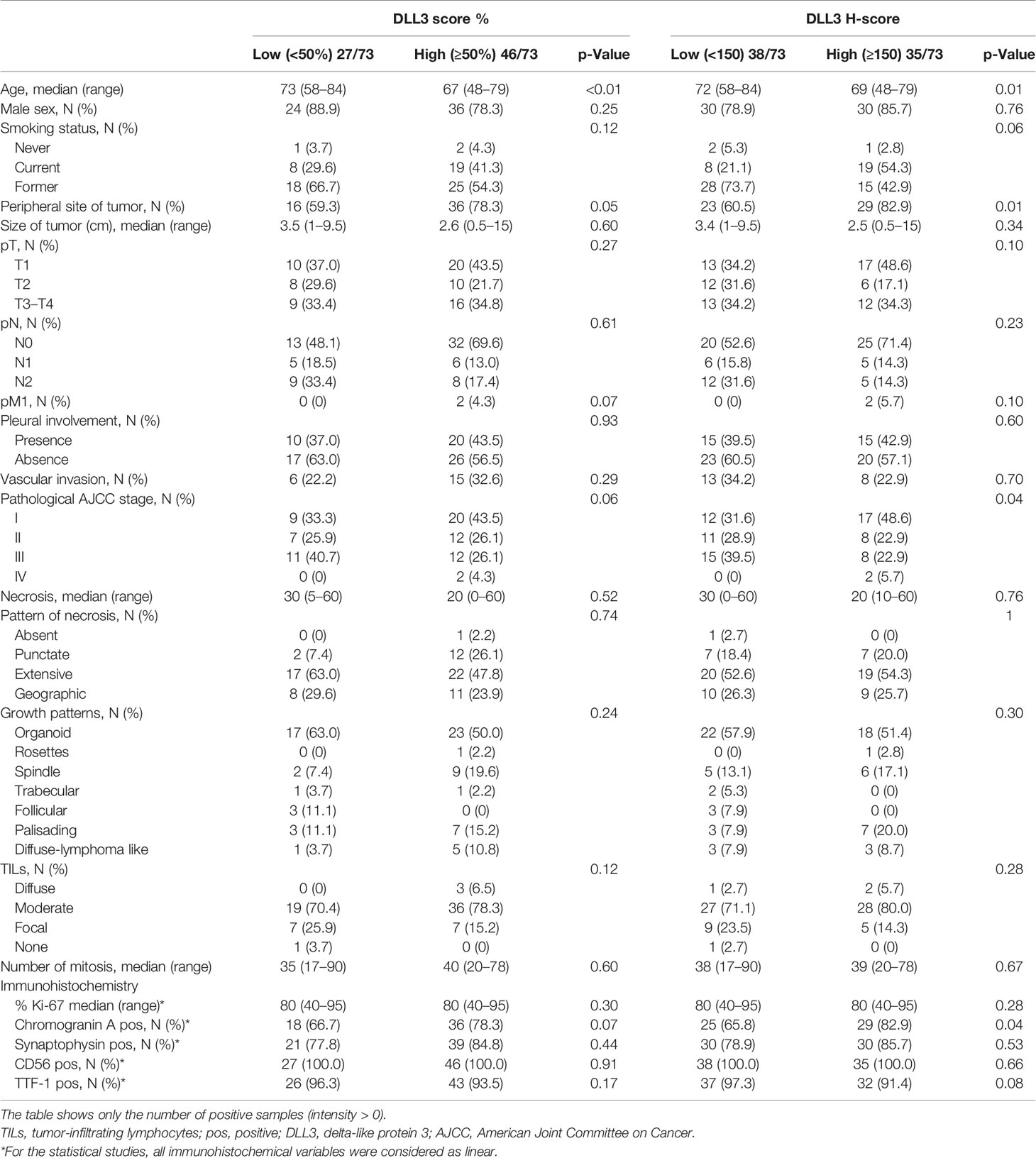
Table 3 Demographics and clinical and pathological features of high-grade neuroendocrine tumors (73/155) based on high DLL3 expression.
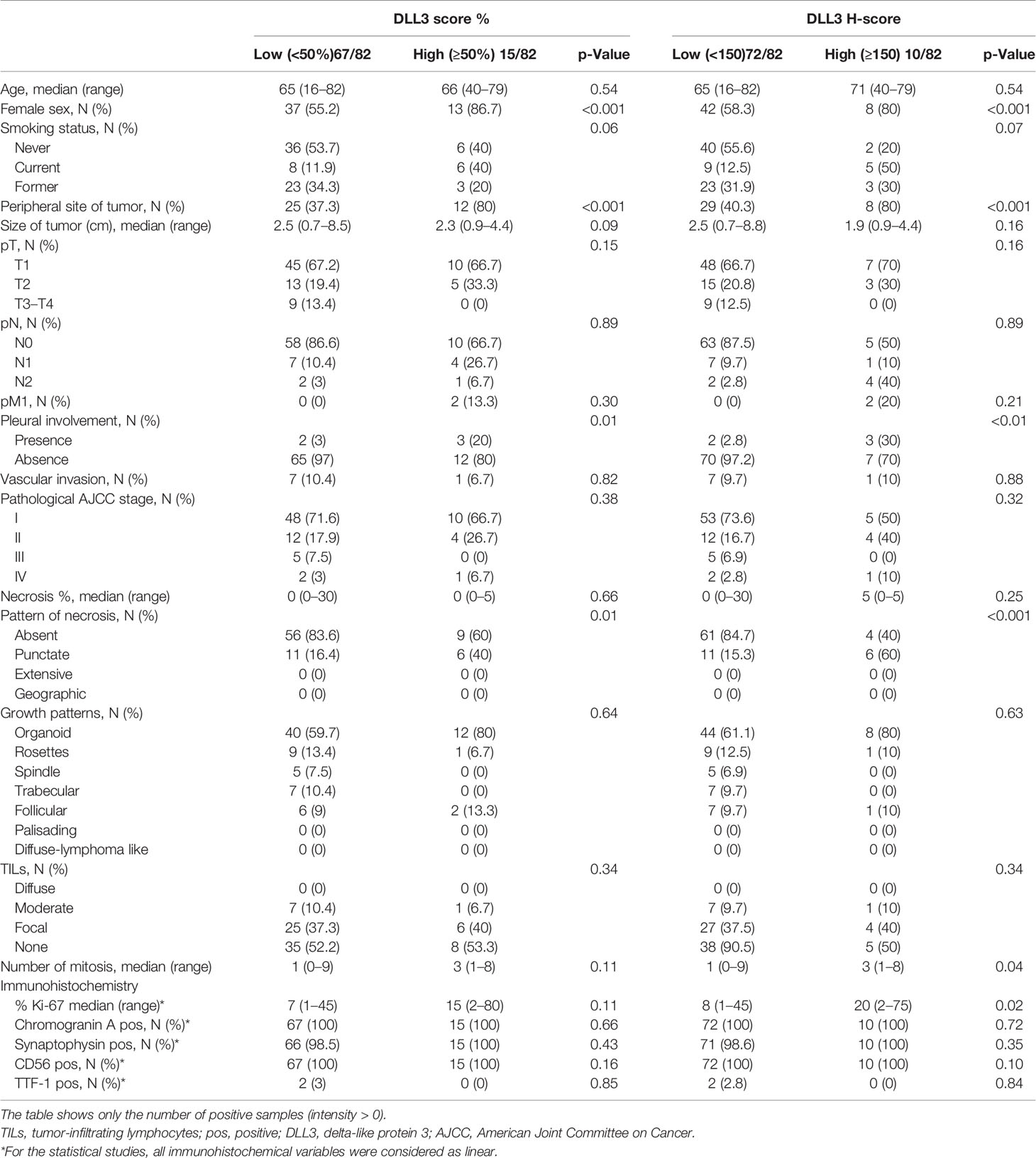
Table 4 Demographics and clinical and pathological features of low-grade neuroendocrine tumors (82/155) based on high DLL3 expression.
In the low-grade neoplasm group, the DLL3 expression was higher in females (p < 0.001). The high DLL3 expression correlated with histological parameters typically associated with high-grade NETs such as high mitosis number (p < 0.001), Ki-67 index (p < 0.0001), and presence of necrosis (p < 0.001). These correlations hold true for the low-grade tumor group, while no significant associations were observed between the DLL3 expression and these variables in the high-grade group.
A greater DLL3 expression was also observed in tumors with visceral pleura infiltration, where 23/35 (65.7%) had ≥50% positive tumor cells and 18/35 (51.4%) had H-score ≥150. On the other hand, considering cases with no pleural involvement, 82/120 (68.3%) had <50% positive tumor cells and 93/120 (77.5%) had H-score <150. These findings were confirmed in the low-grade group of tumors.
The high DLL3 expression in all samples correlates with the presence of moderate or diffuse TIL infiltration (p < 0.001), palisading growth pattern (p = 0.01), and positive TTF-1 immunohistochemical staining (p < 0.001).
Among the neoplasms with high DLL3 expression, 40/61 (65.6% using percentage value) and 31/45 (68.9% using H-score) presented a moderate-to-severe inflammatory infiltrate.
In the high-grade neoplasm group (total = 73), DLL3 H-score positively correlated with chromogranin A expression (p = 0.04).
The prognostic value of DLL3 was tested using an H-score cutoff of 150. Overall, the high DLL3 expression is associated with lower OS (p = 0.001) and DFS (p < 0.001) (Figure 3). Similarly, in low-grade tumors, the high DLL3 expression correlates with poorer DFS (p < 0.01) (Figure 4). As expected, the majority of adverse events in low-grade tumors occurred in AC patients. We tested the prognostic impact of DLL3 in this histological category, and again, the high DLL3 expression predicted a worse DFS (p = 0.01). To better understand the prognostic impact of DLL3, we tested it in multivariate settings, including histology and AJCC stage. DLL3 H-score (cutoff 150) showed a suggestive trend for poor DFS (p = 0.06, hazard ratio (HR) = 1.90, 95% CI 0.98–3.70), independently of the other parameters.
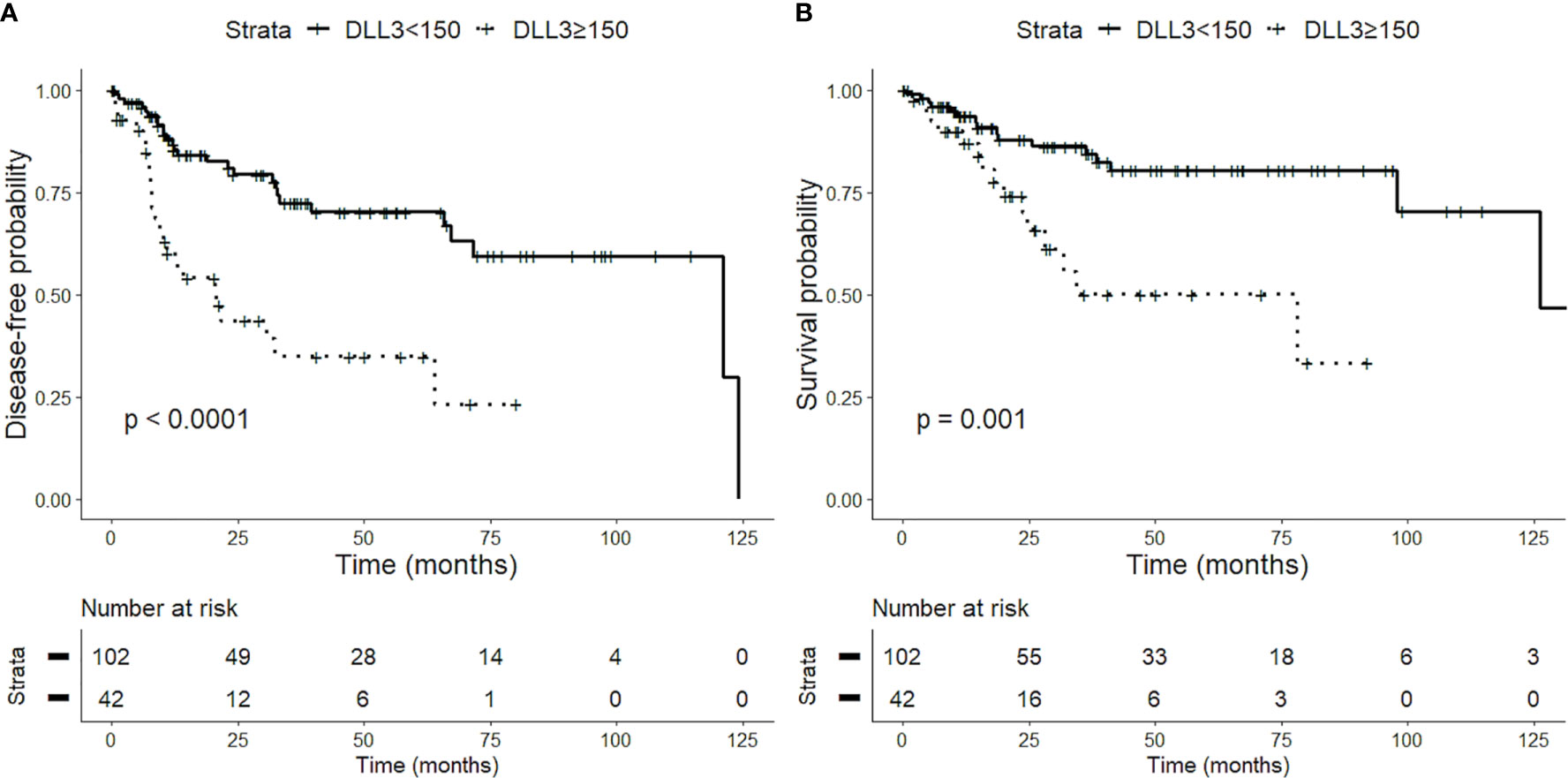
Figure 3 Impact of delta-like protein 3 (DLL3) expression on prognosis of patients with lung neuroendocrine tumors. High levels of DLL3 expression (H-score > 150) are associated with a worse disease-free survival (DFS) (A) and overall survival (OS) (B).
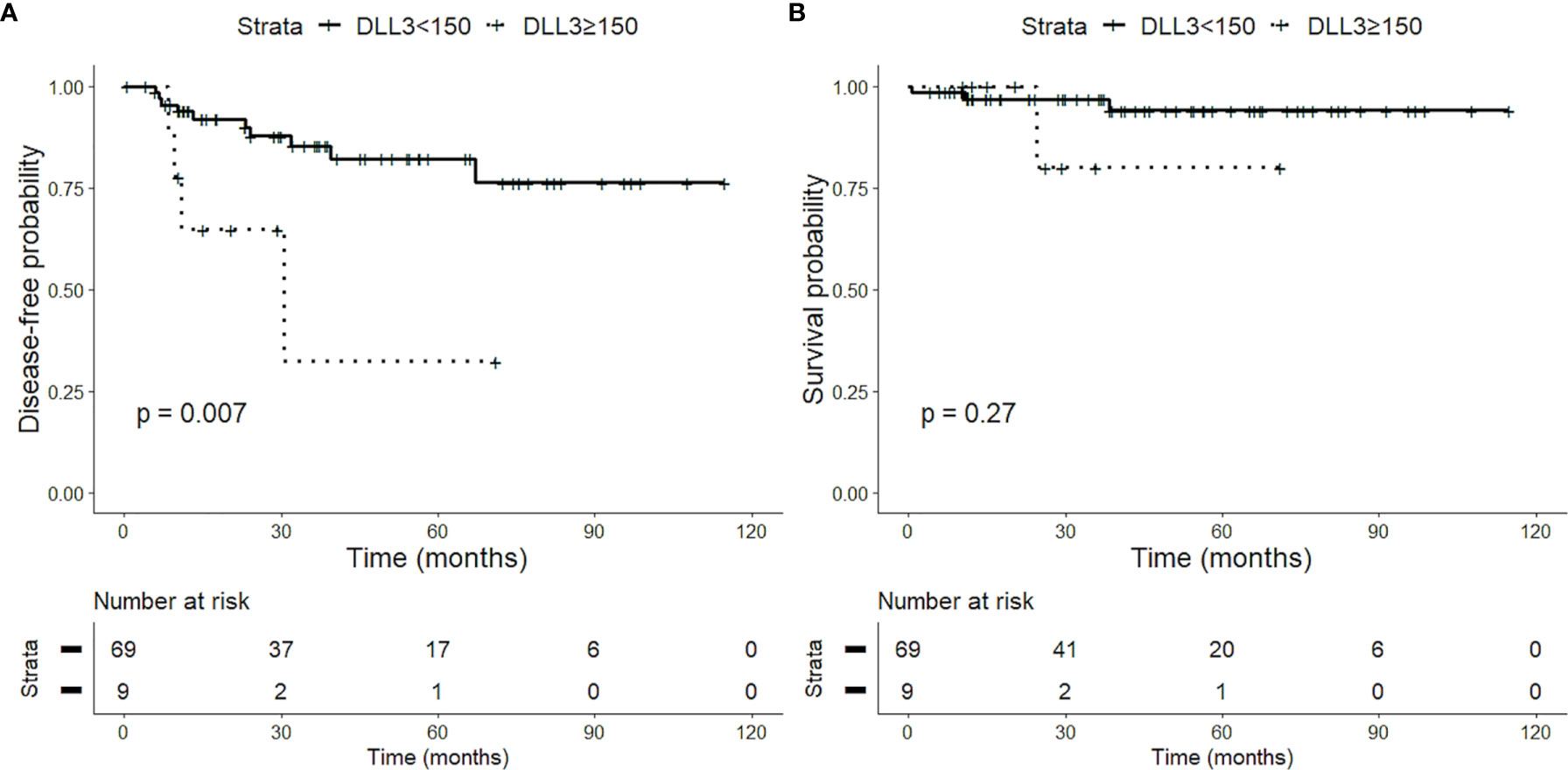
Figure 4 Impact of delta-like protein 3 (DLL3) staining on prognosis of patients with low-grade lung neuroendocrine tumors. High DLL3 expression (H-score > 150) is associated with a reduced disease-free survival (DFS) (A) but not with overall survival (OS) (B), probably due to the low number of events.
In the last few years, DLL3 has been identified as a novel therapeutic target gene mostly in SCLCs, but also in LCNECs (23, 36). Moreover, the literature data have demonstrated a relationship between DLL3 expression and sensitivity of platinum-based adjuvant chemotherapy, suggesting a predictive role of the DLL3 expression (37).
To the best of our knowledge, this is the first article investigating the DLL3 immunohistochemical expression and its prognostic role in a consecutive series of limited-stage lung NETs treated with surgery and including all four histological types (TCs, ACs, LCNECs, and SCLCs).
Higher DLL3 expression was more frequent in high-grade neoplasms. In detail, 46.9% and 75% of SCLC specimens showed a high DLL3 expression by using H-score and percentage of positive tumor cells, respectively. Our DLL3 prevalence data are consistent with those in the literature, showing that the DLL3 protein is highly expressed in SCLCs (21–23, 30, 35, 38, 39).
However, two studies reported a high DLL3 expression in only 32% of SCLCs (28). These discrepancies could depend on technical differences, on DLL3 score computation, and on the analysis of bioptic specimens.
We also demonstrated a high DLL3 expression in 48.8% of LCNECs by using H-score and 53.7% of LCNECs by using percentages of positive tumor cells, comparable with previous studies in LCNECs (29, 35). Only Ogawa and colleagues found lower rates of DLL3 expression (37.1% of LCNECs) by immunohistochemistry, but the results of their data could be due to the non-homogeneous study cohort, which included pure and combined LCNECs as well as different antibody clones (37).
The DLL3 expression has not been fully elucidated in lung carcinoid tumors. In our study, among the low-grade NETs, 20%–25% of ACs and 5%–12% of TCs—assessed by H-score and percentage of positive tumor cells, respectively—have high DLL3 expression. Only two other studies explored the DLL3 immunohistochemical expression in low-grade NETs. Alcala et al. reported a high expression in 40% of carcinoid samples (31); however, the authors included 20 low-grade NE neoplasms without specifying the TC and AC proportion, nor the DLL3 immunohistochemical expression cutoff used. The other study by Xie et al. showed higher DLL3 immunoreactivity in 37% of AC and 32.8% of TC samples by using the cutoff of >50% positive tumor cells to define the high DLL3 expression (30). However, we do not have a straightforward explanation for the DLL3 prevalence discrepancies observed in carcinoid cohorts. For this reason, the DLL3 expression in low-grade NETs needs to be evaluated in larger cohorts in order to define the possible prognostic-therapeutic role in this category of tumors.
The association between DLL3 expression and clinicopathological characteristics has not been thoroughly explored, and it is still largely uncertain. In our study, in the entire cohort, NE neoplasms with high DLL3 expression more often belonged to smoking patients. The neoplasms were mainly peripheral, and more than half of the high DLL3 expression neoplasms had pleural infiltration at microscopic evaluation. Samples with high immunoreactivity had higher numbers of mitosis, higher Ki-67 index, and greater necrosis; moreover, they generally presented palisade growth pattern and moderate-to-severe TILs and expressed TTF-1.
As regards high-grade NETs, those with high DLL3 expression tended to have advanced AJCC stage, peripheral location, and chromogranin A expression. The association of DLL3 expression with more aggressive tumor behavior was also found in patients with other high-grade tumor types, such as endometrial carcinoma, lung adenocarcinoma, and small cell bladder cancer (40–42), as well as in SCLC patients (39). However, other studies did not find any association between DLL3 expression and clinicopathological characteristics in high-grade NE lung tumors (28, 37, 38).
As regards low-grade NETs, neoplasms with high DLL3 expression frequently belonged to female patients, as previously described (30), and generally presented with a peripheral location. Interestingly, high DLL3 expression was also associated with aggressive histological characteristics, such as a higher number of mitoses, higher Ki-67 index, presence of punctate necrosis, and greater predisposition to pleural infiltration.
As regards survival data, high DLL3 expression was associated with lower OS and DFS in the entire cohort. The significant association with lower DFS was confirmed also independently of the histology and AJCC stage, which are the most useful prognostic indices. The association between high DLL3 expression and lower OS and DFS suggests that this marker might be associated with more aggressive tumors, even if this association has not been confirmed for high-grade tumors. The high proportion of patients with positive DLL3 tumor expression, despite the absence of prognostic implications, confirms previous results in SCLC and LCNEC patients (28, 37–39). A study by Huang et al. (43) found an association between high level of the DLL3 expression and low progression-free survival (PFS) and OS rates in biopsy from primary tumors and metastatic LNs in advanced SCLC patients. However, a larger multicenter study, evaluating DLL3 expression in biopsy samples collected from 1,073 SCLC patients with limited and extensive stage disease, did not find any association between DLL3 expression and survival data (32). Therefore, the DLL3 prognostic role needs to be further investigated in biopsy from SCLC patients, which represent the most frequent type of specimen in these patients. Only Xie and collaborators observed a significant association between high DLL3 expression and better OS and small size of tumors in both SCLC and AC patients, suggesting that the DLL3 expression might represent a favorable prognostic factor in lung NETs. However, in their study, only a relatively small percentage of lung NETs had low expression of DLL3. Therefore, prognostic data need to be interpreted with caution (30).
The DLL3 expression has not yet been associated with OS in low-grade NETs. We observed a significant association between high DLL3 expression and lower DFS in ACs. This finding as well as the association between DLL3 expression and aggressive histological characteristics suggests that DLL3 expression could identify a subgroup of ACs with worse prognosis and more clinically aggressive behavior.
Several recent studies suggest the existence of low-grade lung NETs with proliferative capacities higher than those currently accepted for TC and AC (5, 44, 45). These cases could be the lung equivalent of gastro-entero-pancreatic (GEP) NET G3. This new category has a prognostic and therapeutic significance: G3 NETs show a more aggressive behavior than G1–G2 NETs and a lower response rate to platinum-based chemotherapy, which remains a therapeutic signature of NE carcinomas (46). However, actually, this entity is not included in lung NET classification since only a limited number of cases have been reported so far, with different terminologies, different inclusion criteria, and few therapeutic information; and more data about these cases are needed. In this context, DLL3 expression could add useful prognostic information to histological subtyping in low-grade lung NETs.
Cardnell and collaborators found a correlation between TTF1 and DLL3 expression in SCLCs, suggesting that TTF1 could be used as a surrogate marker for DLL3 (47). However, we did not observe this association in high-grade tumors, which confirms previous results from the literature (29). In accordance with previous reports (29, 37), we observed a significant correlation between higher DLL3 expression and increased staining intensity of chromogranin A in high-grade tumors, which supported the hypothesis that the DLL3 expression is related to NE differentiation and could promote NE tumorigenesis in high-grade lung NETs.
Several limitations associated with the present study should be mentioned. Firstly, this was a retrospective, non-randomized single-center study that concerned only resected specimens. However, in clinical practice, the vast majority of SCLCs are diagnosed by biopsy procedure without any need for subsequent surgery resection. Nevertheless, we evaluated DLL3 expression by using a homogeneous cohort composed of only surgically resected pulmonary NETs. Our results thus need to be confirmed in a prospective cohort, by evaluating the DLL3 expression in biopsies from SCLC patients. Our cohort selection may also have led to a bias to evaluate the association between DLL3 expression and prognosis (OS and DFS) in SCLC patients, since the better outcome of the early-stage SCLC patients in our study. However, our results are similar to those of other studies that used biopsies of SCLC to assess for DLL3 expression (23, 32). Secondly, although our report is referred to a large series in terms of surgically resected SCLCs, the overall number of TCs, ACs, and LCNECs is relatively small; and further validation studies should be warranted.
However, despite these limitations, our study demonstrated a high prevalence of DLL3 expression in high-grade lung NET patients and its association with aggressive clinicopathological features. These findings confirm that DLL3 could represent a useful biomarker for target therapy in high-grade tumors. Our results also suggest that the DLL3 expression could identify a subset of ACs tumors with more aggressive behavior, thus providing the basis for new therapeutic options in this group of patients.
The original contributions presented in the study are included in the article/supplementary files. Further inquiries can be directed to the corresponding author.
The study was approved by the Ethics Committee “Comitato Etico di Area Vasta Nord Ovest” (CEAVNO) for Clinical experimentation. Informed written consent for publication was not asked, since no data that can potentially and clearly identify patients were used and reported in the manuscript.
Conception of the work and result interpretation: GA, IDS, and GF. Immunohistochemistry and data analysis: AMP, SR, and AP. Sample collections and result interpretation: FD, ML, and FM. Pathological diagnosis: GA, IDS, and GF. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One Hundred Years After "Carcinoid": Epidemiology of and Prognostic Factors for Neuroendocrine Tumors in 35,825 Cases in the United States. J Clin Oncol (2008) 26(18):3063–72. doi: 10.1200/JCO.2007.15.4377
2. Dasari A, Shen C, Halperin D, Zhao B, Zhou S, Xu Y, et al. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol (2017) 3(10):1335–42. doi: 10.1001/jamaoncol.2017.0589
3. Travis W, Colby T, Corrin B, Shimosato Y, Brambilla E. In collaboration with Sobin LH and Pathologists From 14 Countries. WHO International Histological Classification of Tumours. In: Histological Typing of Lung and Pleural Tumours. New York: Springer-Verlag (1999).
4. Travis WD BE, Burke AP, Marx A, Nicholson AG. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. 4th ed. Lyon, France: International Agency for Research on Cancer (2015).
5. Board WCoTE. Thoracic Tumours. Lyon (France): International Agency for Research on Cancer (2021).
6. Filosso PL, Falcoz PE, Solidoro P, Pellicano D, Passani S, Guerrera F, et al. The European Society of Thoracic Surgeons (ESTS) Lung Neuroendocrine Tumors (NETs) Database. J Thorac Dis (2018) 10(Suppl 29):S3528–S32. doi: 10.21037/jtd.2018.04.104
7. Rekhtman N. Neuroendocrine Tumors of the Lung: An Update. Arch Pathol Lab Med (2010) 134(11):1628–38. doi: 10.1043/2009-0583-RAR.1
8. Ramirez RA, Chauhan A, Gimenez J, Thomas KEH, Kokodis I, Voros BA. Management of Pulmonary Neuroendocrine Tumors. Rev Endocr Metab Disord (2017) 18(4):433–42. doi: 10.1007/s11154-017-9429-9
9. Fasano M, Della Corte CM, Papaccio F, Ciardiello F, Morgillo F. Pulmonary Large-Cell Neuroendocrine Carcinoma: From Epidemiology to Therapy. J Thorac Oncol (2015) 10(8):1133–41. doi: 10.1097/JTO.0000000000000589
10. Wang S, Zimmermann S, Parikh K, Mansfield AS, Adjei AA. Current Diagnosis and Management of Small-Cell Lung Cancer. Mayo Clin Proc (2019) 94(8):1599–622. doi: 10.1016/j.mayocp.2019.01.034
11. Hung YP. Neuroendocrine Tumors of the Lung: Updates and Diagnostic Pitfalls. Surg Pathol Clin (2019) 12(4):1055–71. doi: 10.1016/j.path.2019.08.012
12. Caplin ME, Baudin E, Ferolla P, Filosso P, Garcia-Yuste M, Lim E, et al. Pulmonary Neuroendocrine (Carcinoid) Tumors: European Neuroendocrine Tumor Society Expert Consensus and Recommendations for Best Practice for Typical and Atypical Pulmonary Carcinoids. Ann Oncol (2015) 26(8):1604–20. doi: 10.1093/annonc/mdv041
13. Uprety D, Halfdanarson TR, Molina JR, Leventakos K. Pulmonary Neuroendocrine Tumors: Adjuvant and Systemic Treatments. Curr Treat Options Oncol (2020) 21(11):86. doi: 10.1007/s11864-020-00786-0
14. Furuta M, Kikuchi H, Shoji T, Takashima Y, Kikuchi E, Kikuchi J, et al. DLL3 Regulates the Migration and Invasion of Small Cell Lung Cancer by Modulating Snail. Cancer Sci (2019) 110(5):1599–608. doi: 10.1111/cas.13997
15. Matsuo K, Taniguchi K, Hamamoto H, Ito Y, Futaki S, Inomata Y, et al. Delta-Like 3 Localizes to Neuroendocrine Cells and Plays a Pivotal Role in Gastrointestinal Neuroendocrine Malignancy. Cancer Sci (2019) 110(10):3122–31. doi: 10.1111/cas.14157
16. Chapman G, Sparrow DB, Kremmer E, Dunwoodie SL. Notch Inhibition by the Ligand DELTA-LIKE 3 Defines the Mechanism of Abnormal Vertebral Segmentation in Spondylocostal Dysostosis. Hum Mol Genet (2011) 20(5):905–16. doi: 10.1093/hmg/ddq529
17. Bray SJ. Notch Signalling in Context. Nat Rev Mol Cell Biol (2016) 17(11):722–35. doi: 10.1038/nrm.2016.94
18. George J, Lim JS, Jang SJ, Cun Y, Ozretic L, Kong G, et al. Comprehensive Genomic Profiles of Small Cell Lung Cancer. Nature (2015) 524(7563):47–53. doi: 10.1038/nature14664
19. Crabtree JS, Singleton CS, Miele L. Notch Signaling in Neuroendocrine Tumors. Front Oncol (2016) 6:94. doi: 10.3389/fonc.2016.00094
20. George J, Walter V, Peifer M, Alexandrov LB, Seidel D, Leenders F, et al. Integrative Genomic Profiling of Large-Cell Neuroendocrine Carcinomas Reveals Distinct Subtypes of High-Grade Neuroendocrine Lung Tumors. Nat Commun (2018) 9(1):1048. doi: 10.1038/s41467-018-03099-x
21. Huang RSP, Holmes BF, Powell C, Marati RV, Tyree D, Admire B, et al. Delta-Like Protein 3 Prevalence in Small Cell Lung Cancer and DLL3 (SP347) Assay Characteristics. Arch Pathol Lab Med (2019) 143(11):1373–7. doi: 10.5858/arpa.2018-0497-OA
22. Saunders LR, Bankovich AJ, Anderson WC, Aujay MA, Bheddah S, Black K, et al. A DLL3-Targeted Antibody-Drug Conjugate Eradicates High-Grade Pulmonary Neuroendocrine Tumor-Initiating Cells In Vivo. Sci Transl Med (2015) 7(302):302ra136. doi: 10.1126/scitranslmed.aac9459
23. Rudin CM, Pietanza MC, Bauer TM, Ready N, Morgensztern D, Glisson BS, et al. Rovalpituzumab Tesirine, a DLL3-Targeted Antibody-Drug Conjugate, in Recurrent Small-Cell Lung Cancer: A First-in-Human, First-in-Class, Open-Label, Phase 1 Study. Lancet Oncol (2017) 18(1):42–51. doi: 10.1016/S1470-2045(16)30565-4
24. Morgensztern D, Besse B, Greillier L, Santana-Davila R, Ready N, Hann CL, et al. Efficacy and Safety of Rovalpituzumab Tesirine in Third-Line and Beyond Patients With DLL3-Expressing, Relapsed/Refractory Small-Cell Lung Cancer: Results From the Phase II TRINITY Study. Clin Cancer Res (2019) 25(23):6958–66. doi: 10.1158/1078-0432.CCR-19-1133
25. Owen DH, Giffin MJ, Bailis JM, Smit MD, Carbone DP, He K. DLL3: An Emerging Target in Small Cell Lung Cancer. J Hematol Oncol (2019) 12(1):61. doi: 10.1186/s13045-019-0745-2
26. Giffin MJ, Cooke K, Lobenhofer EK, Estrada J, Zhan J, Deegen P, et al. AMG 757, A Half-Life Extended, DLL3-Targeted Bispecific T-Cell Engager, Shows High Potency and Sensitivity in Preclinical Models of Small-Cell Lung Cancer. Clin Cancer Res (2021) 27(5):1526–37. doi: 10.1158/1078-0432.CCR-20-2845
27. Owonikoko TK, Borghaei H. Immunotherapy of Lung Cancer. J Thorac Dis (2018) 10(Suppl 3):S395–S6. doi: 10.21037/jtd.2018.01.142
28. Tanaka K, Isse K, Fujihira T, Takenoyama M, Saunders L, Bheddah S, et al. Prevalence of Delta-Like Protein 3 Expression in Patients With Small Cell Lung Cancer. Lung Cancer (2018) 115:116–20. doi: 10.1016/j.lungcan.2017.11.018
29. Hermans BCM, Derks JL, Thunnissen E, van Suylen RJ, den Bakker MA, Groen HJM, et al. DLL3 Expression in Large Cell Neuroendocrine Carcinoma (LCNEC) and Association With Molecular Subtypes and Neuroendocrine Profile. Lung Cancer (2019) 138:102–8. doi: 10.1016/j.lungcan.2019.10.010
30. Xie H, Boland JM, Maleszewski JJ, Aubry MC, Yi ES, Jenkins SM, et al. Expression of Delta-Like Protein 3 is Reproducibly Present in a Subset of Small Cell Lung Carcinomas and Pulmonary Carcinoid Tumors. Lung Cancer (2019) 135:73–9. doi: 10.1016/j.lungcan.2019.07.016
31. Alcala N, Leblay N, Gabriel AAG, Mangiante L, Hervas D, Giffon T, et al. Integrative and Comparative Genomic Analyses Identify Clinically Relevant Pulmonary Carcinoid Groups and Unveil the Supra-Carcinoids. Nat Commun (2019) 10(1):3407. doi: 10.1038/s41467-019-11276-9
32. Rojo F, Corassa M, Mavroudis D, Aysim Büge Öz, Biesma B, Brcic L, et al. International Real-World Study of DLL3 Expression in Patients With Small Cell Lung Cancer. Lung Cancer (2020) 147:237–43. doi: 10.1016/j.lungcan.2020.07.026
33. Liu L, Wei J, Teng F, Zhu Y, Xing P, Zhang J, et al. Clinicopathological Features and Prognostic Analysis of 247 Small Cell Lung Cancer With Limited-Stage After Surgery. Hum Pathol (2021) 108:84–92. doi: 10.1016/j.humpath.2020.11.007
34. Brierley JD, Wittekind C, Gospodarowicz MK. TNM Classification of Malignant Tumours. Oxford, UK: Wiley Blackwell (2017).
35. Brcic L, Kuchler C, Eidenhammer S, Pabst D, Quehenberger F, Gazdar AF, et al. Comparison of Four DLL3 Antibodies Performance in High Grade Neuroendocrine Lung Tumor Samples and Cell Cultures. Diagn Pathol (2019) 14(1):47. doi: 10.1186/s13000-019-0827-z
36. Lashari BH, Vallatharasu Y, Kolandra L, Hamid M, Uprety D. Rovalpituzumab Tesirine: A Novel DLL3-Targeting Antibody-Drug Conjugate. Drugs R D (2018) 18(4):255–8. doi: 10.1007/s40268-018-0247-7
37. Ogawa H, Sakai Y, Nishio W, Fujibayashi Y, Nishikubo M, Nishioka Y, et al. DLL3 Expression is a Predictive Marker of Sensitivity to Adjuvant Chemotherapy for Pulmonary LCNEC. Thorac Cancer (2020) 11(9):2561–9. doi: 10.1111/1759-7714.13574
38. Tendler S, Kanter L, Lewensohn R, Ortiz-Villalon C, Viktorsson K, De Petris L. The Prognostic Implications of Notch1, Hes1, Ascl1, and DLL3 Protein Expression in SCLC Patients Receiving Platinum-Based Chemotherapy. PloS One (2020) 15(10):e0240973. doi: 10.1371/journal.pone.0240973
39. Furuta M, Sakakibara-Konishi J, Kikuchi H, Yokouchi H, Nishihara H, Minemura H, et al. Analysis of DLL3 and ASCL1 in Surgically Resected Small Cell Lung Cancer (Hot1702). Oncologist (2019) 24(11):e1172–e9. doi: 10.1634/theoncologist.2018-0676
40. Wang J, Zhang K, Liu Z, Wang T, Shi F, Zhang Y, et al. Upregulated Delta-Like Protein 3 Expression Is a Diagnostic and Prognostic Marker in Endometrial Cancer: A Retrospective Study. Med (Baltimore) (2018) 97(51):e13442. doi: 10.1097/MD.0000000000013442
41. Liu ZY, Wu T, Li Q, Wang MC, Jing L, Ruan ZP, et al. Notch Signaling Components: Diverging Prognostic Indicators in Lung Adenocarcinoma. Med (Baltimore) (2016) 95(20):e3715. doi: 10.1097/MD.0000000000003715
42. Koshkin VS, Garcia JA, Reynolds J, Elson P, Magi-Galluzzi C, McKenney JK, et al. Transcriptomic and Protein Analysis of Small-Cell Bladder Cancer (SCBC) Identifies Prognostic Biomarkers and DLL3 as a Relevant Therapeutic Target. Clin Cancer Res (2019) 25(1):210–21. doi: 10.1158/1078-0432.CCR-18-1278
43. Huang J, Cao D, Sha J, Zhu X, Han S. DLL3 is Regulated by LIN28B and miR-518d-5p and Regulates Cell Proliferation, Migration and Chemotherapy Response in Advanced Small Cell Lung Cancer. Biochem Biophys Res Commun (2019) 514(3):853–60. doi: 10.1016/j.bbrc.2019.04.130
44. Volante M, Mete O, Pelosi G, Roden AC, Speel AJM, Uccella S. Molecular Pathology of Well-Differentiated Pulmonary and Thymic Neuroendocrine Tumors: What Do Pathologists Need to Know? Endocr Pathol (2021) 32(1):154–68. doi: 10.1007/s12022-021-09668-z
45. Marchiò C, Gatti G, Massa F, Bertero L, Filosso P, Pelosi G, et al. Distinctive Pathological and Clinical Features of Lung Carcinoids With High Proliferation Index. Virchows Arch (2017) 471(6):713–20. doi: 10.1007/s00428-017-2177-0
46. Klimstra D, Kloppel G, La Rosa Salas B. The WHO Classification of Tumours Editorial (Ed.), Classification of Neuroendocrine Neoplasms of the Digestive System. In: WHO Classification of Digestive System Tumours, 5th ed. Lyon: IARC Press (2019). p. 16–21.
47. Cardnell RJ, Li L, Sen T, Bara R, Tong P, Fujimoto J, et al. Protein Expression of TTF1 and cMYC Define Distinct Molecular Subgroups of Small Cell Lung Cancer With Unique Vulnerabilities to Aurora Kinase Inhibition, DLL3 Targeting, and Other Targeted Therapies. Oncotarget (2017) 8(43):73419–32. doi: 10.18632/oncotarget.20621
Keywords: lung neuroendocrine tumors, delta-like protein 3, immunohistochemistry, prognosis, biomarker
Citation: Alì G, Di Stefano I, Poma AM, Ricci S, Proietti A, Davini F, Lucchi M, Melfi F and Fontanini G (2021) Prevalence of Delta-Like Protein 3 in a Consecutive Series of Surgically Resected Lung Neuroendocrine Neoplasms. Front. Oncol. 11:729765. doi: 10.3389/fonc.2021.729765
Received: 23 June 2021; Accepted: 13 August 2021;
Published: 09 September 2021.
Edited by:
Elena Levantini, Beth Israel Deaconess Medical Center and Harvard Medical School, United StatesReviewed by:
Vincenzo L’Imperio, University of Milano-Bicocca, ItalyCopyright © 2021 Alì, Di Stefano, Poma, Ricci, Proietti, Davini, Lucchi, Melfi and Fontanini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gabriella Fontanini, Z2FicmllbGxhLmZvbnRhbmluaUBtZWQudW5pcGkuaXQ=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.