 Si-Cong Ma1,2‡
Si-Cong Ma1,2‡ Hong-Bo Zhu3‡Jian Wang1Yan-Pei Zhang1,2Xue-Jun Guo1
Hong-Bo Zhu3‡Jian Wang1Yan-Pei Zhang1,2Xue-Jun Guo1 Li-Li Long1Ze-Qin Guo1De-Hua Wu1
Li-Li Long1Ze-Qin Guo1De-Hua Wu1 Zhong-Yi Dong1*†Xue Bai1*
Zhong-Yi Dong1*†Xue Bai1*- 1Department of Radiation Oncology, Nanfang Hospital, Southern Medical University, Guangzhou, China
- 2Information Management and Big Data Center, Nanfang Hospital, Southern Medical University, Guangzhou, China
- 3Department of Oncology, The First Affiliated Hospital of University of South China, Hengyang, China
Purpose: Despite the success of targeted therapy in c-ros oncogene 1 (ROS1)-rearranged cancers, especially non-small cell lung cancer (NSCLC), the clinical significance of ROS1 de novo mutation has not yet been understood. We sought to elucidate the predictive effect of ROS1 mutation for immune checkpoint inhibitor (ICI) therapy in melanoma.
Methods: The Cancer Genome Atlas [TCGA (n = 10967)] and Memorial Sloan Kettering Cancer Center [MSK (n = 10,945)] datasets, as well as two clinical cohorts of melanoma received ICI [CA209-038 (n = 73) and MEL-IPI (n = 110)], were included to explore the prevalence, prognostic effect, and immunotherapeutic predictive effect of ROS1 mutation in melanoma. Overall survival (OS) was defined as the primary outcome.
Results: Overall, melanoma accounted for the highest proportion of ROS1 mutation (~20%) which made up the majority (~95%) of the ROS1-alterated cases. Remarkably, ROS1 mutation yielded longer OS from ICI than the wild-type counterpart in the MSK melanoma population [hazard ratio (HR) 0.47, 95% confidence interval (CI) 0.30–0.74], and two external melanoma cohorts (CA209-038: HR 0.42, 95% CI 0.20–0.89; MEL-IPI: HR 0.55, 95% CI 0.34–0.91), without affecting the prognosis of patients. Elevated tumor mutational burden and enrichment of DNA damage repair was observed in ROS1 mutated patients, providing an explanation for the favorable responses to ICI therapy. Precisely, ROS1 mutation in non-protein tyrosine kinase (PTK) domain but not PTK mutation was responsible for the immunotherapy-specific responses of the ROS1 mutated patients in melanoma.
Conclusions: Collectively, ROS1 mutation, specifically the non-PTK mutation, is a potential predictor of ICI therapy in melanoma, which is distinct from the well-established role of ROS1 rearrangement for targeted therapy in NSCLC.
Highlights
● Melanoma accounted for the highest proportion of ROS1 mutation which made up the majority of the ROS1-alterated cases.
● ROS1 mutation served as a favorable predictor for immune checkpoint therapy but not a prognostic factor in melanoma.
● ROS1 mutation was correlated with elevated tumor antigenicity and genomic instability.
● The non-PTK domain was the specific site of ROS1 mutation that determine the favorable responses to immune checkpoint therapy in melanoma.
Introduction
The c-ros oncogene 1 (ROS1) gene has aroused great research interest for its role as an oncogenic driver of malignancies, as well as its untapped potential for novel therapeutic targets (1). It encodes a receptor tyrosine kinase with a tyrosine kinase domain located in the intracellular C-terminal (2). Long-term efforts have been devoted to develop tyrosine kinase inhibitors targeting the continuously activated ROS1 proteins resulted by chromosomal rearrangements, and crizotinib has received approval of the U.S. Food and Drug Administration (FDA) for ROS1-rearranged cancers (3). Nonetheless, almost all previous studies focused specifically on ROS1-rearranged non-small cell lung cancer (NSCLC), which only makes up a tiny percentage of patients (4). The focus on ROS1-rearranged NSCLC on the one hand contributes to the tremendous success of tyrosine kinase inhibitors targeting the ROS1 rearrangement, whereas on the other hand leads to the neglect of the therapeutic potential behind the ROS1 alterations other than rearrangement, particularly de novo mutation that accounts for a larger proportion.
With the unprecedented progress of immune checkpoint inhibitors (ICIs), immunotherapy has altered the treatment paradigm and gradually become the mainstay of the treatment for advanced cancers, especially melanoma (5, 6). Identifying marker of significance to predict responses to ICI therapy has become a key challenge in study and clinical practice of immunotherapy because of the heterogeneity of ICI effectiveness seen among patients in the clinical work (7–11). Given the relatively modest predictive power of the routinely applied immunotherapeutic biomarkers, such as PD-L1, growing studies have been committed to search for clues from gene mutation (8, 12–14). Recent advances have expanded the role of oncogenic driver genes from targeted therapy to immunotherapy, including STK11, EGFR and KRAS (14–16); however, for our knowledge, there were few studies on variations other than rearrangement concerning ROS1, and what role the ROS1 mutation would act in ICI treatment of melanoma has not yet been elucidated to date. Therefore, the purpose of our study was to explore the predictive value of ROS1 mutation, instead of rearrangement, for the efficacy of ICI treatment in melanoma.
Methods
Study Populations
Clinical and genomic data of pan-cancer patients from The Cancer Genome Atlas (TCGA, n = 10,967) and Memorial Sloan Kettering Cancer Center (MSK, n = 10,945) were retrieved from cBioPortal (http://www.cbioportal.org/). Among the MSK dataset, 1,661 patients were treated with anti-programmed cell death-1 (PD-1) alone or in combination with anti-Cytotoxic Lymphocyte Antigen-4 (CTLA-4). Additionally, two clinical cohorts of melanoma received anti-PD-1 (CA209-038, n = 73) or anti-CTLA-4 therapy (MEL-IPI, n = 110), along with their corresponding DNA sequencing data, were collected from previously published studies (17, 18). This study was approved by the Institutional Ethical Review Boards of Nanfang Hospital. Patients included in the clinical cohorts have provided signed informed consent in accordance with their corresponding clinical study protocols.
Study Design
A flow chart showing the study design was demonstrated in Supplementary Figure 1. In this study, we first conducted a pan-cancer analysis in the TCGA and the MSK datasets to explore the prevalence of ROS1 mutation in various cancers. Then, an exploratory analysis was performed to investigate the predictive value of ROS1 mutation in the MSK ICI-treated population, as well as the prognostic value in the non-ICI treated population. The predictive significance of ROS1 mutation for ICI therapy in melanoma was furtherly validated in the CA209-038 and the MEL-IPI cohorts. The correlation of ROS1 mutation status with tumor mutational burden (TMB) was analyzed, and pathway enrichment analysis according to ROS1 mutation status was conducted to elucidate the potential mechanism. Moreover, immunotherapy-specific survival outcomes were compared between patients harboring ROS1 mutation in or out of the tyrosine kinase domain to identify the exact mutation sites that predict efficacy of ICI therapy. Overall survival (OS) was defined as the primary outcome in this study.
Genomic Analysis
Patients in the TCGA dataset, as well as the CA209-038 and the MEL-IPI cohorts were molecularly profiled with whole exome sequencing (WES), while those in the MSK dataset underwent Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT), a targeted next-generation sequencing assay (19). TMB was calculated as the absolute count of non-synonymous mutations (including nonsense, missense, nonstop, frame shift, in frame, splice site, and translation start site mutations) by WES, or mutations per megabase by MSK-IMPACT. Tyrosine kinase domain of ROS1 was identified and visualized within a lollipop chart using cBioportal (20).
Pathway Enrichment and Network Analysis With RNA Sequencing Data
RNA sequencing data of TCGA melanoma dataset obtained from cBioportal was preprocessed and normalized using RNA-Seq by Expectation Maximization (RSEM) (20, 21). Patients were classified into subgroups according to ROS1 mutation status. Gene Set Enrichment Analysis (GSEA) was conducted with the java-based GSEA v4.0.3 application to compare the activity of biological processes or pathways between ROS1 mutation and wild-type (22), using the C2 curated gene sets downloaded from the Molecular Signatures Database (MSigDB) (23). Nominal P value evaluated the statistical significance of the enrichment score of a certain pathway or biological process, while false discovery rate (FDR), which was adjusted for gene set size, was estimated to represent the false positive probability. Normalized enrichment score (NES) was used to compare analysis results across gene sets (22). Molecular interaction network was built using STRING (version 11.0), with a minimum required interaction score of 0.99 (24).
Statistical Analysis
GraphPad Prism (version 8.0.1) or R (version 3.6.1) were used for statistical analyses. Survival analyses were performed using the Kaplan–Meier method with log-rank test. Kaplan–Meier survival curves were plotted using GraphPad Prism or the R packages survival and surminer; hazard ratios (HRs) with 95% confidence intervals (CIs) were reported. Differential analysis of ROS1 mutation versus wild-type was conducted using the R package limma. TMB and gene expression were compared between subgroups using unpaired t-test. All P values were two-sided, and P ≤0.05 was considered statistically significant.
Results
Frequent ROS1 Mutation in Melanoma
In total, we included 10,967 patients from TCGA and 10,945 patients from MSK, among which 1,661 patients were treated with ICI, for genomic analysis evaluating the prevalence of ROS1 mutation across various cancers (Figure 1). Overall, patients with melanoma harbored a predominant prevalence of ROS1 mutation, with proportions of 25.0 and 14.8% respectively in the TCGA and the MSK datasets (Figures 1A, B). Specifically, for the ICI-treated patients of the MSK dataset, ROS1 mutation was detected in 20.0% of melanoma patients, and the high mutation frequency was also confirmed within different subtypes of melanoma, including cutaneous melanoma, head and neck mucosal melanoma, and melanoma of unknown primary (Figure 1C). Notably, ROS1 mutation accounted for the majority of the ROS1-alterated melanoma cases in both datasets (TCGA: 94.6%; MSK: 94.7%). In contrast, ROS1 fusion only accounted for a small fraction of patients in NSCLC (<2% in both datasets), and even rare in other tumor types (Figures 1A, B).

Figure 1 Prevalence of ROS1 mutation across various cancers. Frequencies of ROS1 alterations (including mutation, fusion, amplification, deep deletion, and multiple alterations) in various cancer types in (A) the TCGA and (B) the MSK datasets, and (C) detailed cancer subtypes in the MSK ICI-treated population were illustrated. TCGA, The Cancer Genome Atlas; MSK, Memorial Sloan Kettering; ICI, immune checkpoint inhibitor.
ROS1 Mutation Predicts Efficacy of Immunotherapy in Melanoma
Given the high prevalence of ROS1 mutation in melanoma, we first explored its predictive value for risk stratification of melanoma patients received ICI treatment in the MSK dataset. Remarkably, in the total MSK ICI-treated population, patients harboring ROS1 mutation obtained longer OS compared to both the fusion subgroup and the wild-type subgroup (P <0.001, Figure 2A). Specifically, for the ICI-treated melanoma population, survival prospects consistently favored ROS1 mutation than its wild-type counterpart (HR 0.47, 95% CI 0.30–0.74; P = 0.009, Figure 2B).
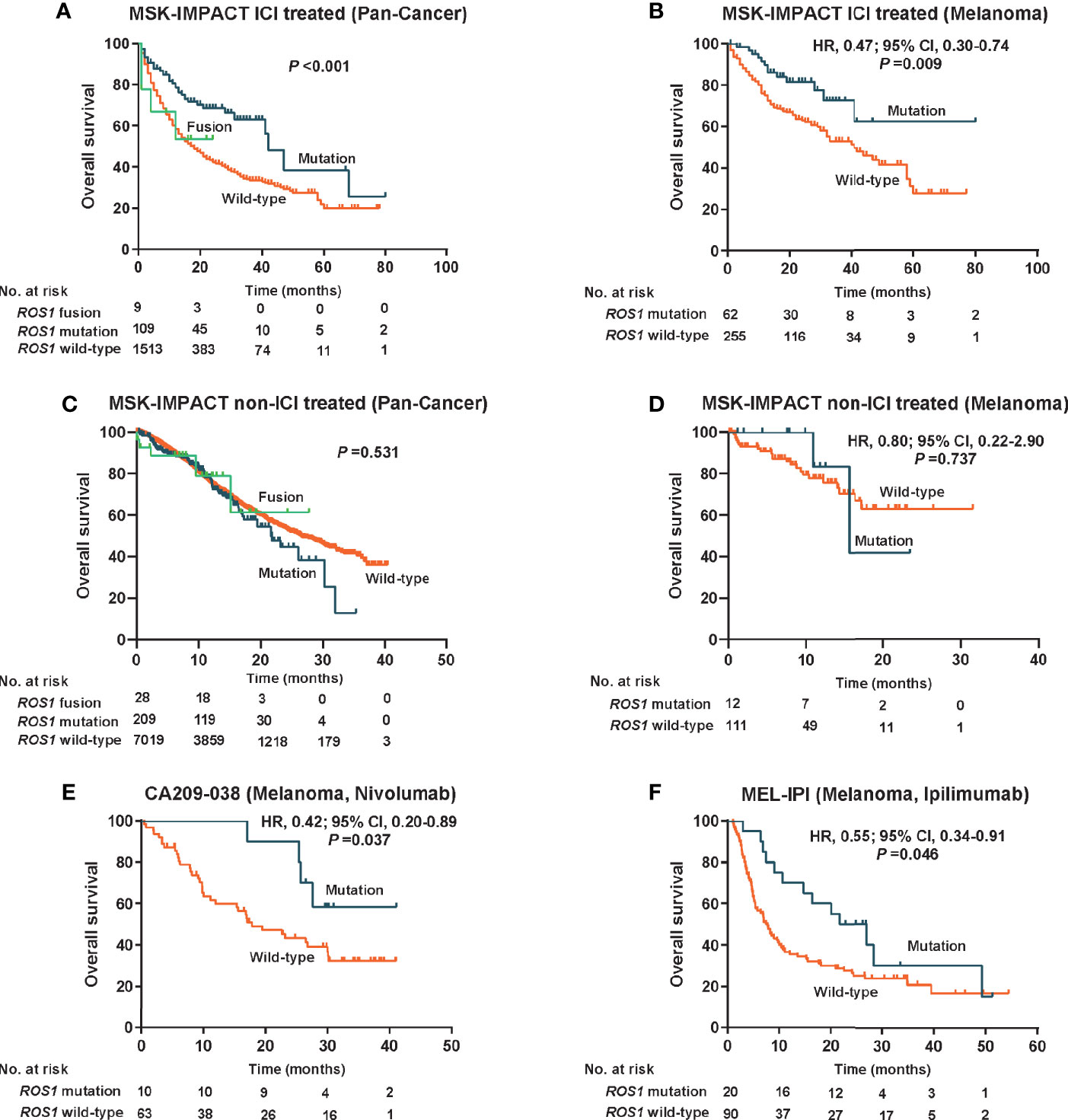
Figure 2 Predictive value for immune checkpoint inhibitors therapy and prognostic effect of ROS1 mutation. Kaplan–Meier curves of overall survival in (A) the pooled MSK ICI-treated population, (B) the MSK ICI-treated melanoma population, (C) the pooled MSK non-ICI treated population, (D) the MSK non-ICI treated melanoma population, (E) the CA209-038 cohort of melanoma received nivolumab, and (F) the MEL-IPI cohort of melanoma received ipilimumab. MSK, Memorial Sloan Kettering; HR, hazard ratio; CI, confidence interval; ICI, immune checkpoint inhibitor.
To clarify whether the predictive effect of ROS1 mutation on immunotherapy was affected by the prognostic effect itself, we evaluated the impact of ROS1 mutation on prognosis in the non-ICI treated population from the MSK dataset. Generally, no significant difference in OS was observed among the ROS1 mutation, the wild-type, and the fusion subgroups in the pooled population (P = 0.531, Figure 2C); likewise, as for the non-ICI treated melanoma patients, ROS1 mutation demonstrated similar OS as the wild-type counterpart (HR 0.80, 95% CI 0.22–2.90; P = 0.737, Figure 2D). A consistent finding seen in the TCGA melanoma population (HR 1.15, 95% CI 0.80–1.65; P = 0.463, Supplementary Figure 2) further confirmed that ROS1 mutation serves as a potential predictive biomarker of ICI treatment for melanoma, without affecting the prognosis of patients.
Moreover, external validation of the predictive significance of ROS1 mutation was conducted in two independent ICI-treated melanoma cohorts. Of note, the presence of ROS1 mutation was associated with long-term survival prospects and increased likelihood of responses to nivolumab in terms of OS in the CA209-038 cohort (HR 0.42, 95% CI 0.20–0.89; P = 0.037, Figure 2E). The pronounced clinical benefits derived from ROS1 mutation versus wild type were furtherly confirmed in the MEL-IPI cohort of melanoma treated with ipilimumab (HR 0.55, 95% CI 0.34–0.91; P = 0.046, Figure 2F).
ROS1 Mutation Correlates With Upregulated Tumor Antigenicity and DNA Damage Repair
To investigate the potential mechanism behind the predictive power of ROS1 mutation for ICI therapy, correlation analysis between ROS1 mutation status and TMB was performed. For the total population, patients with ROS1 mutation harbored significantly higher TMB than ROS1 fusion and wild-type patients in both the TCGA and MSK cohorts (all P <0.001, Figures 3A, B). In parallel, ROS1 mutation was associated with higher TMB relative to the wild-type counterpart in the melanoma population (all P <0.001, Figures 3A, B). Equivalent findings were also seen in the MSK ICI-treated patients (all P <0.001, Figure 3C), providing an explanation for the favorable responses of ROS1-mutated patients to ICI therapy.
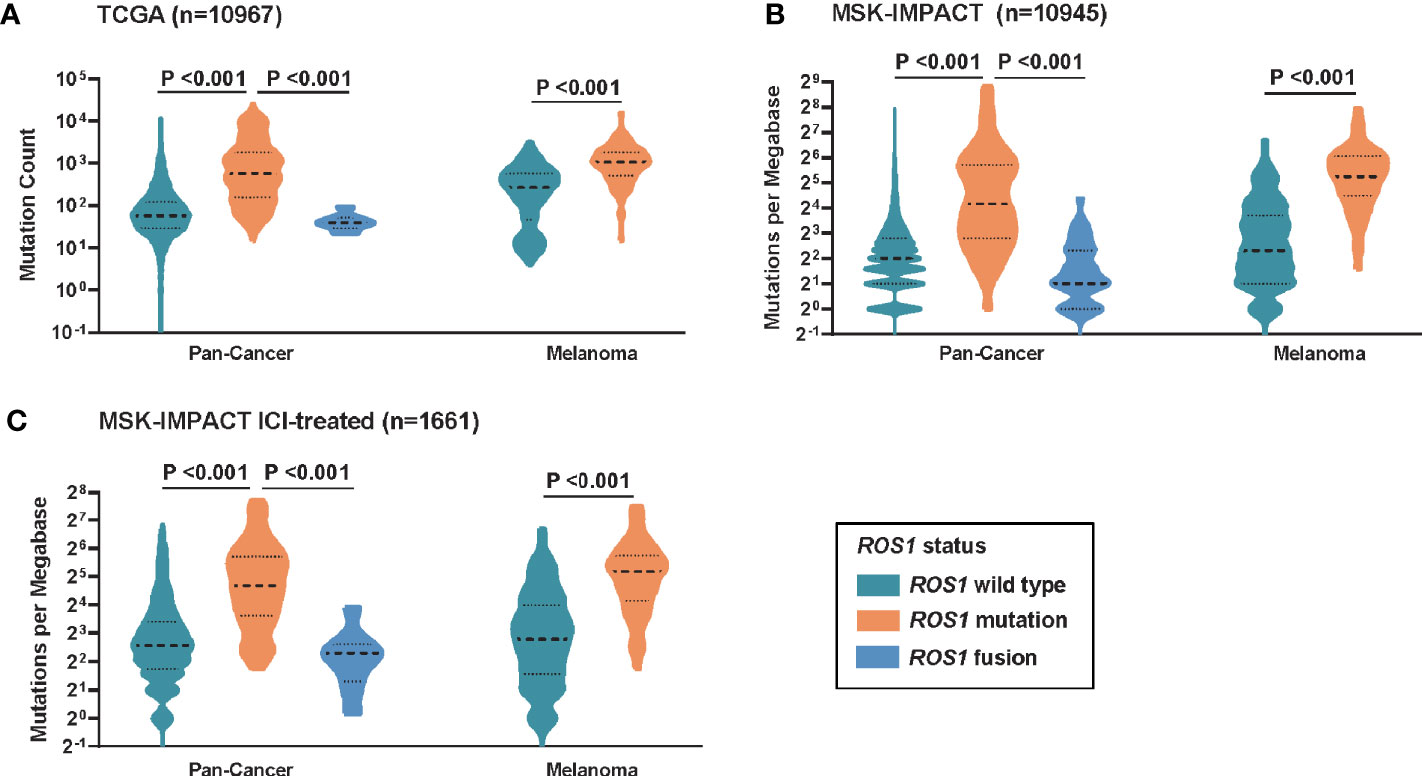
Figure 3 Correlation between ROS1 mutation status and tumor mutational burden. Distribution of TMB in the total population and the melanoma population in (A) the TCGA dataset, (B) the MSK dataset, and (C) the MSK ICI-treated population. TCGA, The Cancer Genome Atlas; MSK, Memorial Sloan Kettering; ICI, immune checkpoint inhibitor; TMB, tumor mutational burden.
Furthermore, we performed GSEA to explain, from the perspective of transcriptomics, the immunotherapy-specific responses of ROS1 mutation versus wild-type using the RNA sequencing data of the TCGA melanoma dataset (Figure 4A and Supplementary Table 1). We observed significant enrichment of DNA damage repair (DDR)-related pathways in the subgroup with ROS1 mutation compared to the wild-type counterpart, including BRCA-centered network, ATP pathway, DNA repair pathway, and mismatch repair pathway (Figures 4B–E), indicative of an upregulation of the activity of DDR-related pathways secondary to the accumulation of gene damage and the elevated tumor antigenicity in the ROS1 mutated population. As a contrast, expression levels of immune checkpoint genes (e.g., PDCD1, CD274, and CTLA4) were not associated with ROS1 mutation status (Supplementary Figure 3). These finding suggest that favorable responsiveness of ROS1 mutation to ICI therapy was specifically attributed to the elevated tumor antigenicity instead of the expression changes in immune checkpoint molecules.
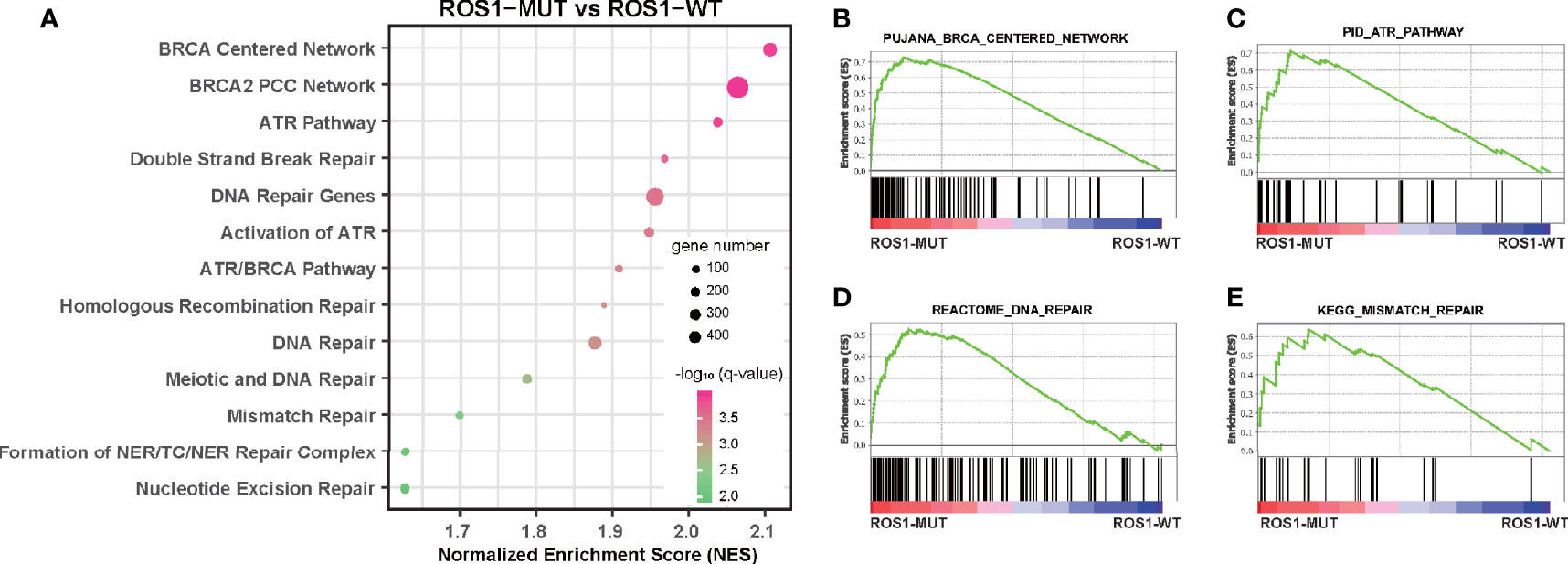
Figure 4 Gene set enrichment analysis of ROS1 mutation versus wild-type. (A) Bubble plot showing the enrichment of DNA damage repair-related pathways in ROS1 mutation patients relative to wild-type patients in the TCGA melanoma dataset. Enrichment plots of ROS1 mutation versus wild-type regarding (B) BRCA centered network, (C) ATR pathway, (D) DNA repair, and (E) mismatch repair. FDR, false discovery rate; MUT, mutation; WT, wild-type; TCGA, The Cancer Genome Atlas.
Non-Tyrosine Kinase Mutation of ROS1 as the Precise Subtype of Immunotherapy-Specific Responses
Given that patients harboring ROS1 fusion, which involves the protein tyrosine kinase (PTK) domain, responded unfavorably to ICI therapy (Figure 2A), we wonder whether de novo mutation of ROS1 within the PTK domain might also compromise the immunotherapy-specific responses. Therefore, we divided ROS1 mutated patients into subgroups according to mutation location. Mutations within the PTK domain (amino acid sites from 1,947 to 2,215) were assigned as PTK mutations, whereas those not in this scope were assigned as non-PTK mutation (Figure 5A).
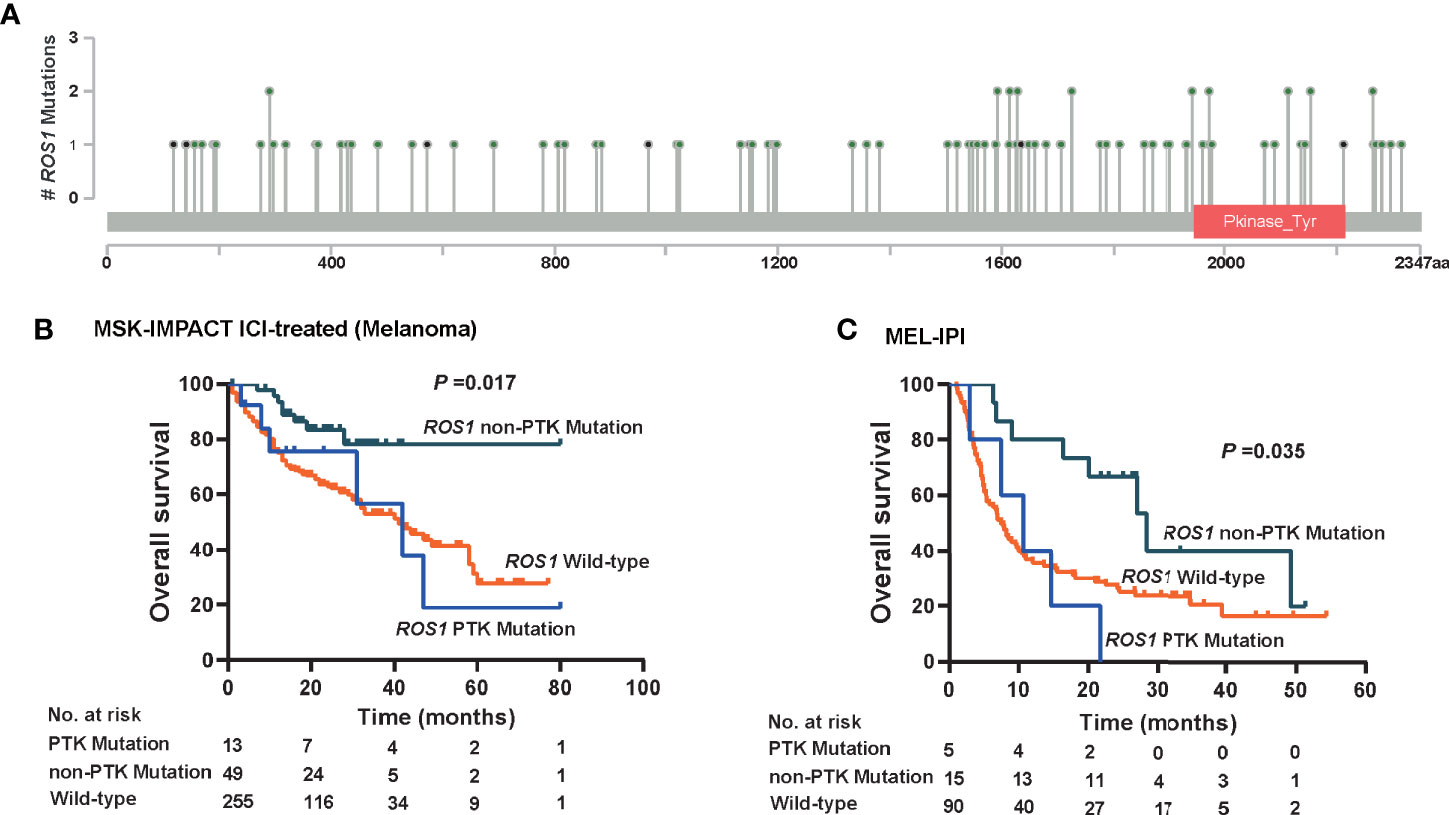
Figure 5 Immunotherapeutic predictive effect of ROS1 mutation in or out of the protein tyrosine kinase domain. (A) Lollipop chart showing the location of the protein tyrosine kinase (PTK) domain of the ROS1 gene, and mutation number of each position in the MSK ICI-treated melanoma dataset. Kaplan–Meier curves of overall survival in (B) the MSK ICI-treated melanoma population, and (C) the MEL-IPI cohort of melanoma received ipilimumab. MSK, Memorial Sloan Kettering; ICI, immune checkpoint inhibitor.
Approximately, non-PTK mutation accounted for ~75% of ROS1 mutation in melanoma patients, namely 79.0% (n = 49) in the MSK ICI-treated melanoma population and 75.0% (n = 15) in the MEL-IPI cohort (Figures 5B, C). It is noteworthy that non-PTK mutation of ROS1 yielded significantly prolonged OS relative to both ROS1 PTK mutation and wild type in the MSK ICI-treated melanoma population (P = 0.017, Figure 5B). In a similar vein, OS was longer in the ROS1 non-PTK mutation arm relative to the ROS1 PTK mutation arm and the ROS1 wild-type arm in the MEL-IPI cohort (P = 0.035, Figure 5C). Taken together, these results indicate that non-PTK mutation of ROS1 is the precise mutation subtype that predicts efficacy of ICI therapy.
Discussion
In this genetic association study, we demonstrated a relatively high mutation frequency of ROS1 in pan-cancer especially melanoma. Notably, ROS1 mutation served as a favorable predictor for ICI therapy but not a prognostic factor in melanoma, whereas ROS1 fusion and wild-type patients derived limited benefits from ICI therapy, potentially attributed to the relatively elevated tumor antigenicity and genomic instability in ROS1 mutated patients. Furthermore, we identified the non-PTK domain as the specific sites of ROS1 mutation that determine the favorable responses to ICI therapy in melanoma.
As a well-known driver gene, ROS1 has long been studied; however, to the best of our knowledge, almost all the studies concerning on ROS1 alterations revolved around chromosomal rearrangement (1, 3, 4). Admittedly, ROS1 targeted inhibitors, represented by crizotinib, achieved tremendous success in ROS1-fusion cancers especially NSCLC (3, 4), but actually, rearrangement just accounts for a fairly small proportion of patients, less than 2% in NSCLC, and even lower in other malignancies (1, 25). Therefore, the effective population of the ROS1 inhibitors was quite limited. Even worse, the resistance to ROS1 inhibitors, owing to the mutation of the kinase domain or activation of bypass pathways, makes the circumstances more pickle (26). In these regards, broader investigation probing into the function of ROS1 alterations, other than rearrangement, is warranted to devise new therapeutic strategies for cancers.
Herein, we identified ROS1 mutation as a predictor for ICI therapy, enabling people to re-examine the value of the gene as another therapeutic target. Compared with ROS1 rearrangement in targeted therapy, ROS1 mutation plays a positive role in ICI therapy. More importantly, it accounts for much greater number of patients than rearrangement, which means more beneficiaries could be identified for precision therapy. Interestingly, ROS1 fusion and wild type were both found to yield a relatively poor response to ICI therapy, potentially attributed to the low mutational burden which has been shown by previous studies to associate with low neoantigenicity, thus hindering the activity of immune system against tumors (27); hence it was reasonable to recommend those patients with ROS1 mutation to receive ICI therapy, whereas those with ROS1 fusion still to receive targeted therapy. Consequently, our finding of ROS1 mutation in ICI therapy was a strong complement for the treatment of patients with ROS1 alterations.
Elucidation of the molecular mechanisms of genomics instability and DNA damage repair have pioneered a new avenue for cancer treatment (28); recent studies on the association between gene damage and tumor neoantigenicity have laid the DNA repair processes and DNA damage checkpoints of an important position in ICI-based immunotherapy (27, 29). Our study suggested an enrichment of DDR-related processes and damage sensor protein-centered pathways in the ROS1 mutated population, represented by upregulation of gene expression of BRCA1/2, ATR, and ATM (Supplementary Figure 4). Network interaction analysis of ROS1 mutation versus wild-type also revealed an enrichment of DNA repair-related molecules (Supplementary Figure 5). On this ground, it is envisioned that patients harboring ROS1 mutation are intrinsically characterized with a hyper mutation status with accumulated genomics instability and gene damage that increased tumor mutational burden, which in turn triggers the secondary activation of DDR-related pathways as well as the resultant immune surveillance at the meantime. In contrast, there was no significant enrichment of biological processes concerning epithelial-mesenchymal transition for ROS1 mutated subgroup versus the wild-type counterpart, indicative of the irrelevance between ROS1 mutation and metastasis (Supplementary Figure 6).
As ROS1 mutations are quite heterogeneous, whether mutations in distinct gene loci confer differential responses to ICI therapy is of significance to explore. To this end, we have classified them based on the mutation location, namely mutations in PTK domain and those in non-PTK domain, so as to identify the exact mutation sites of immunotherapy-specific responses. Interestingly, our data illustrated that it was those patients harboring non-PTK mutation instead of PTK mutation that derived significant efficacy benefits from ICI therapy than the wild-type counterparts. With the aforementioned finding, we proposed that the use of ICI might be an ideal treatment option for patients harboring ROS1 mutation in the non-PTK domain.
This study does have several limitations. First of all, the specific molecular mechanism behind the predictive significance of non-PTK mutation of ROS1 have not been fully characterized, so more comprehensive biological mechanisms are still to be elucidated in future studies. In addition, as a multicohort study, heterogeneity among cohorts is inevitable; still, despite this objective fact, our results demonstrate consistent tendency across cohorts, which in a sense reflects the credibility of the conclusions. Lastly, due to the retrospective nature of the post hoc analysis, it is still necessary to verify the predictive value of ROS1 mutation, specifically the non-PTK mutation, for ICI therapy in prospective clinical trials.
Conclusions
In conclusion, we for the first time reveal the positive predictive value of ROS1 mutation, characterized with increased tumor antigenicity and gene damage, for ICI therapy in melanoma, which is distinct from the well-established role of ROS1 rearrangement for targeted therapy in NSCLC. Moreover, non-PTK mutation is identified as the precise mutation subtype of immunotherapy-specific responses. Further elucidation of the biological mechanisms and validation in future prospective studies are needed before its application in the clinical practice.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found here: http://www.cbioportal.org/.
Ethics Statement
The study was approved by the Nanfang Hospital, Southern Medical University. The patients/participants included in the clinical cohorts have provided signed informed consent in accordance with their corresponding clinical study protocols.
Author Contributions
Study design: XB, Z-YD, D-HW. Data collection: S-CM, XB, JW, and X-JG. Data analysis and interpretation: Z-YD, S-CM, XB, H-BZ, JW, Y-PZ, L-LG, and Z-QG. Writing of the manuscript: S-CM, XB, and Y-PZ. Revision of the manuscript: Z-YD, D-HW, XB, H-BZ, JW, X-JG, L-LG, and Z-QG. Statistical analysis: Z-YD, S-CM, and H-BZ. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the National Natural Science Foundation for Young Scientists of China (Grant Nos. 81802863 and 81902353), the Natural Science Foundation of Guangdong Province (Grant No. 2018030310285), the Outstanding Youths Development Scheme of Nanfang Hospital, Southern Medical University (Grant No. 2017J003 and 2020J011), and the College Students’ Innovative Entrepreneurial Training Plan Program (Grant Nos. 202012121001 and S202012121065).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.666145/full#supplementary-material
Supplementary Figure 1 | Flow chart of the study design. ICI, immune checkpoint inhibitor; TMB, tumor mutational burden; MSK, Memorial Sloan Kettering; TCGA, The Cancer Genome Atlas.
Supplementary Figure 2 | Kaplan Meier curves according to overall survival of ROS1 MUT versus WT in non-ICI treated melanoma patients from the TCGA melanoma dataset. MUT, mutation; WT, wild-type; ICI, immune checkpoint inhibitor; TCGA, The Cancer Genome Atlas.
Supplementary Figure 3 | Gene expression levels of (A) inhibitory receptors within the PD-1 pathway, and (B) other immune checkpoint molecules in The Cancer Genome Atlas (TCGA) melanoma dataset according to the mutation status of ROS1.
Supplementary Figure 4 | Gene expression levels of representative genes within DNA damage repair-related and damage sensor protein-centered pathways in The Cancer Genome Atlas (TCGA) melanoma dataset according to the mutation status of ROS1.
Supplementary Figure 5 | Network analysis for ROS1 downstream mechanisms in TCGA melanoma dataset. (A) Volcano plot showing differential analysis of ROS1 mutation versus wild-type; those genes with P<0.01 were retained for network establishment. (B) Interaction network with a minimum required interaction score of 0.99. (C) BRCA-centered subnetwork. DNA repair-related molecules were color coded within the network. MUT, mutation; WT, wild-type; TCGA, The Cancer Genome Atlas.
Supplementary Figure 6 | Enrichment plots of ROS1 mutation versus wild-type in biological processes concerning metastasis or epithelial-mesenchymal transition (EMT). NES, normalized enrichment score; FDR, false discovery rate.
Abbreviations
ICI, immune checkpoint inhibitor; TCGA, The Cancer Genome Atlas; MSK, Memorial Sloan Kettering; PD-1, programmed cell death-1; CTLA-4, Cytotoxic Lymphocyte Antigen-4; TMB, tumor mutational burden; DDR, DNA damage repair; PTK, protein tyrosine kinase; HR, hazard ratio; CI, confidence interval, NSCLC, non-small cell lung cancer; FDA, Food and Drug Administration.
References
1. Lin JJ. And Shaw at Recent Advances in Targeting ROS1 in Lung Cancer. J Thorac Oncol (2017) 12(11):1611–25. doi: 10.1016/j.jtho.2017.08.002
2. Davies KD, Doebele RC. Molecular Pathways: ROS1 Fusion Proteins in Cancer. Clin Cancer Res (2013) 19(15):4040–5. doi: 10.1158/1078-0432.Ccr-12-2851
3. Shaw AT, Ou SH, Bang YJ, Camidge DR, Solomon BJ, Salgia R, et al. Crizotinib in ROS1-Rearranged Non-Small-Cell Lung Cancer. N Engl J Med (2014) 371(21):1963–71. doi: 10.1056/NEJMoa1406766
4. Shaw AT, Riely GJ, Bang YJ, Kim DW, Camidge DR, Solomon BJ, et al. Crizotinib in ROS1-Rearranged Advanced Non-Small-Cell Lung Cancer (NSCLC): Updated Results, Including Overall Survival, From PROFILE 1001. Ann Oncol (2019) 30(7):1121–6. doi: 10.1093/annonc/mdz131
5. Weber JS, D’Angelo SP, Minor D, Hodi FS, Gutzmer R, Neyns B, et al. Nivolumab Versus Chemotherapy in Patients With Advanced Melanoma Who Progressed After Anti-CTLA-4 Treatment (CheckMate 037): A Randomised, Controlled, Open-Label, Phase 3 Trial. Lancet Oncol (2015) 16(4):375–84. doi: 10.1016/s1470-2045(15)70076-8
6. Tawbi HA, Forsyth PA, Algazi A, Hamid O, Hodi FS, Moschos SJ, et al. Combined Nivolumab and Ipilimumab in Melanoma Metastatic to the Brain. N Engl J Med (2018) 379(8):722–30. doi: 10.1056/NEJMoa1805453
7. Gibney GT, Weiner LM. And Atkins Mb Predictive Biomarkers for Checkpoint Inhibitor-Based Immunotherapy. Lancet Oncol (2016) 17(12):e542–51. doi: 10.1016/s1470-2045(16)30406-5
8. Cao R, Yang F, Ma SC, Liu L, Zhao Y, Li Y, et al. Development and Interpretation of a Pathomics-Based Model for the Prediction of Microsatellite Instability in Colorectal Cancer. Theranostics (2020) 10(24):11080–91. doi: 10.7150/thno.49864
9. Litchfield K, Reading JL, Puttick C, Thakkar K, Abbosh C, Bentham R, et al. Meta-Analysis of Tumor- and T Cell-Intrinsic Mechanisms of Sensitization to Checkpoint Inhibition. Cell (2021) 184(3):596–614.e14. doi: 10.1016/j.cell.2021.01.002
10. Osorio JC, Arbour KC, Le DT, Durham JN, Plodkowski AJ, Halpenny DF, et al. Lesion-Level Response Dynamics to Programmed Cell Death Protein (Pd-1) Blockade. J Clin Oncol (2019) 37(36):3546–55. doi: 10.1200/jco.19.00709
11. Ma S-C, Tang X-R, Long L-L, Bai X, Zhou J-G, Duan Z-J, et al. Integrative Evaluation of Primary and Metastatic Lesion Spectrum to Guide Anti-PD-L1 Therapy of Non-Small Cell Lung Cancer: Results From Two Randomized Studies. OncoImmunology (2021) 10(1):1909296. doi: 10.1080/2162402X.2021.1909296
12. Braun DA, Hou Y, Bakouny Z, Ficial M, Sant’ Angelo M, Forman J, et al. Interplay of Somatic Alterations and Immune Infiltration Modulates Response to PD-1 Blockade in Advanced Clear Cell Renal Cell Carcinoma. Nat Med (2020) 26(6):909–18. doi: 10.1038/s41591-020-0839-y
13. Sun H, Liu SY, Zhou JY, Xu JT, Zhang HK, Yan HH, et al. Specific TP53 Subtype as Biomarker for Immune Checkpoint Inhibitors in Lung Adenocarcinoma. EBioMedicine (2020) 60:102990. doi: 10.1016/j.ebiom.2020.102990
14. Bai X, Wu DH, Ma SC, Wang J, Tang XR, Kang S, et al. Development and Validation of a Genomic Mutation Signature to Predict Response to PD-1 Inhibitors in Non-Squamous NSCLC: A Multicohort Study. J Immunother Cancer (2020) 8(1):e000381. doi: 10.1136/jitc-2019-000381
15. Dong ZY, Zhong WZ, Zhang XC, Su J, Xie Z, Liu SY, et al. Potential Predictive Value of TP53 and KRAS Mutation Status for Response to PD-1 Blockade Immunotherapy in Lung Adenocarcinoma. Clin Cancer Res (2017) 23(12):3012–24. doi: 10.1158/1078-0432.Ccr-16-2554
16. Skoulidis F, Goldberg ME, Greenawalt DM, Hellmann MD, Awad MM, Gainor JF, et al. Stk11/Lkb1 Mutations and PD-1 Inhibitor Resistance in KRAS-Mutant Lung Adenocarcinoma. Cancer Discovery (2018) 8(7):822–35. doi: 10.1158/2159-8290.Cd-18-0099
17. Riaz N, Havel JJ, Makarov V, Desrichard A, Urba WJ, Sims JS, et al. Tumor and Microenvironment Evolution During Immunotherapy With Nivolumab. Cell. (2017) 171(4):934–49.e16. doi: 10.1016/j.cell.2017.09.028
18. Van Allen EM, Miao D, Schilling B, Shukla SA, Blank C, Zimmer L, et al. Genomic Correlates of Response to CTLA-4 Blockade in Metastatic Melanoma. Science. (2015) 350(6257):207–11. doi: 10.1126/science.aad0095
19. Cheng DT, Mitchell TN, Zehir A, Shah RH, Benayed R, Syed A, et al. Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (Msk-Impact): A Hybridization Capture-Based Next-Generation Sequencing Clinical Assay for Solid Tumor Molecular Oncology. J Mol Diagn (2015) 17(3):251–64. doi: 10.1016/j.jmoldx.2014.12.006
20. Cerami E, Gao J, Dogrusoz U, Gross BE, Sumer SO, Aksoy BA, et al. The Cbio Cancer Genomics Portal: An Open Platform for Exploring Multidimensional Cancer Genomics Data. Cancer Discov (2012) 2(5):401–4. doi: 10.1158/2159-8290.Cd-12-0095
21. Li B. And Dewey Cn RSEM: Accurate Transcript Quantification From RNA-Seq Data With or Without a Reference Genome. BMC Bioinf (2011) 12:323. doi: 10.1186/1471-2105-12-323
22. Subramanian A, Tamayo P, Mootha VK, Mukherjee S, Ebert BL, Gillette MA, et al. Gene Set Enrichment Analysis: A Knowledge-Based Approach for Interpreting Genome-Wide Expression Profiles. Proc Natl Acad Sci USA (2005) 102(43):15545–50. doi: 10.1073/pnas.0506580102
23. Liberzon A, Birger C, Thorvaldsdóttir H, Ghandi M, Mesirov JP. And Tamayo P the Molecular Signatures Database (Msigdb) Hallmark Gene Set Collection. Cell Syst (2015) 1(6):417–25. doi: 10.1016/j.cels.2015.12.004
24. Szklarczyk D, Gable AL, Lyon D, Junge A, Wyder S, Huerta-Cepas J, et al. String V11: Protein-Protein Association Networks With Increased Coverage, Supporting Functional Discovery in Genome-Wide Experimental Datasets. Nucleic Acids Res (2019) 47(D1):D607–13. doi: 10.1093/nar/gky1131
25. Pietrantonio F, Di Nicolantonio F, Schrock AB, Lee J, Tejpar S, Sartore-Bianchi A, et al. Alk, ROS1, and NTRK Rearrangements in Metastatic Colorectal Cancer. J Natl Cancer Inst (2017) 109(12):djx089. doi: 10.1093/jnci/djx089
26. McCoach CE, Le AT, Gowan K, Jones K, Schubert L, Doak A, et al. Resistance Mechanisms to Targeted Therapies in ROS1(+) and ALK(+) Non-Small Cell Lung Cancer. Clin Cancer Res (2018) 24(14):3334–47. doi: 10.1158/1078-0432.Ccr-17-2452
27. Cristescu R, Mogg R, Ayers M, Albright A, Murphy E, Yearley J, et al. Pan-Tumor Genomic Biomarkers for PD-1 Checkpoint Blockade-Based Immunotherapy. Science (2018) 362(6411):eaar3593. doi: 10.1126/science.aar3593
28. Sancar A, Lindsey-Boltz LA, Unsal-Kaçmaz K. And Linn S Molecular Mechanisms of Mammalian Dna Repair and the DNA Damage Checkpoints. Annu Rev Biochem (2004) 73:39–85. doi: 10.1146/annurev.biochem.73.011303.073723
Keywords: ROS1 mutation, immune checkpoint inhibitor, melanoma, tyrosine kinase domain, tumor mutational burden
Citation: Ma S-C, Zhu H-B, Wang J, Zhang Y-P, Guo X-J, Long L-L, Guo Z-Q, Wu D-H, Dong Z-Y and Bai X (2021) De Novo Mutation in Non-Tyrosine Kinase Domain of ROS1 as a Potential Predictor of Immune Checkpoint Inhibitors in Melanoma. Front. Oncol. 11:666145. doi: 10.3389/fonc.2021.666145
Received: 01 March 2021; Accepted: 25 May 2021;
Published: 17 June 2021.
Edited by:
Nihal Ahmad, University of Wisconsin-Madison, United StatesReviewed by:
Gagan Chhabra, University of Wisconsin-Madison, United StatesJasmine George, Medical College of Wisconsin, United States
Copyright © 2021 Ma, Zhu, Wang, Zhang, Guo, Long, Guo, Wu, Dong and Bai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xue Bai, YmFpeHVleGp4akAxNjMuY29t; Zhong-Yi Dong, ZG9uZ3p5MTMxN0Bmb3htYWlsLmNvbQ==
†ORCID: Zhong-Yi Dong, orcid.org/0000-0001-9967-0060
‡These authors have contributed equally to this work